Health Economics Assignment: NHS, QALYs, and Health Equity Analysis
VerifiedAdded on 2023/01/16
|12
|3804
|60
Homework Assignment
AI Summary
This health economics assignment addresses key concepts in healthcare, including consumer and provider moral hazard, and the role of asymmetric information in market failures. It explores capitation as a payment method for doctors, outlining its advantages and disadvantages. The assignment further delves into cost analysis, differentiating between direct, investment, overhead, and per diem costs, and provides a calculation of incremental cost-effectiveness ratios (ICER). The assignment also discusses the use of Quality-Adjusted Life Years (QALYs) in evaluating healthcare interventions, and examines the concepts of equity in healthcare and the fair innings argument. The assignment provides a detailed analysis of various factors that affect healthcare and discusses the importance of opportunity cost, and the methods for evaluating cost-effectiveness.

HEALTH ECONOMICS 1
HEALTH ECONOMICS – MMB725020
Name:
Tutor:
Course:
Date:
HEALTH ECONOMICS – MMB725020
Name:
Tutor:
Course:
Date:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH ECONOMICS 2
Health Economics.
QUESTION 1.
a. Moral hazard is caused by numerous economic theories. Firstly, economic theory is
founded upon the theory that persons perform in their own greatest economic interests. It
is therefore absolutely sensible that for indemnified services, when the marginal cost of
health services is reduced the patient will lean towards consuming more. In actual fact,
researches have frequently proved that after monitoring for medical status, those who
have medical insurance continuously visit the hospital for health services as compared to
those who are not assured. Secondly, moral hazard in medical insurance is the
discrimination of facts realised between the sick and providers or rather the physicians.
The providers through expert training and expertise they have a vast and voluminous
information concerning curing choices, dangers and diagnoses, none of which is totally
passed to the sick. Clients may not own adequate evidence to even decide whether an
incident of care is suitable. This adds to moral hazard in that sick who are reasonably
unaware concerning their choices must put considerable faith in doctors.
b. First, information failure transpires in instances where the entire associates in a fiscal
interchange possess little or no knowledge of the required evidence. Second, information
failure occurs when one member in an economic exchange is more conversant and
acquire more information than the other, a condition known as problem of asymmetric
information. In the two cases above there is a possibility of misallocation of limited
resources, which lead to buyers compensating with little or excess money and businesses
making little or excess. Government may contribute to market failure by introducing
treatment barriers hence limiting the new entrants into the healthcare market. This type of
intervention by government cause the market to become sluggish in competition thereby
increasing the price of services and goods in the heathcare market. If there is no
intervention by the government it leads to burdening the residents due to high cost of
services and medical related goods.
Physicians overcome the sick with informational evidences and provide cure that
frequently are unnecessary.
Medics do not involve sick adequately and fail to offer meaningful care.
Admitted sick person request avoidable cure based on social media conversations.
Health Economics.
QUESTION 1.
a. Moral hazard is caused by numerous economic theories. Firstly, economic theory is
founded upon the theory that persons perform in their own greatest economic interests. It
is therefore absolutely sensible that for indemnified services, when the marginal cost of
health services is reduced the patient will lean towards consuming more. In actual fact,
researches have frequently proved that after monitoring for medical status, those who
have medical insurance continuously visit the hospital for health services as compared to
those who are not assured. Secondly, moral hazard in medical insurance is the
discrimination of facts realised between the sick and providers or rather the physicians.
The providers through expert training and expertise they have a vast and voluminous
information concerning curing choices, dangers and diagnoses, none of which is totally
passed to the sick. Clients may not own adequate evidence to even decide whether an
incident of care is suitable. This adds to moral hazard in that sick who are reasonably
unaware concerning their choices must put considerable faith in doctors.
b. First, information failure transpires in instances where the entire associates in a fiscal
interchange possess little or no knowledge of the required evidence. Second, information
failure occurs when one member in an economic exchange is more conversant and
acquire more information than the other, a condition known as problem of asymmetric
information. In the two cases above there is a possibility of misallocation of limited
resources, which lead to buyers compensating with little or excess money and businesses
making little or excess. Government may contribute to market failure by introducing
treatment barriers hence limiting the new entrants into the healthcare market. This type of
intervention by government cause the market to become sluggish in competition thereby
increasing the price of services and goods in the heathcare market. If there is no
intervention by the government it leads to burdening the residents due to high cost of
services and medical related goods.
Physicians overcome the sick with informational evidences and provide cure that
frequently are unnecessary.
Medics do not involve sick adequately and fail to offer meaningful care.
Admitted sick person request avoidable cure based on social media conversations.
HEALTH ECONOMICS 3
The cigarette company, who does not notify cigarette smoker of the factual
medical threats of smoking.
c. Capitation is a type of a medical care remuneration structure in which a physician and
other medics fraternity in hospital is rewarded a fixed amount per sick for an agreed
duration of time medics association.
Advantages of Capitation.
i. Handling this type of structure can be stress-free and an economical structure
since the sole event in keeping trajectory of medics are the total registered
associates. Paper work is minimised.
ii. Revenue inflow is more foreseeable for physicians and participants have
more expected medical attention expenses.
iii. Precautionary attention is a durable emphasis due to the fact that it is cheap
for medics than to cure intricate and prolonged medical problem in future.
iv. Avoidable involvements, checks and attention are restricted due to doctor’s
intention to cut down cost and capitalize on improving the gains. Sick
persons should worry less on catering for additional checks.
Disadvantages of Capitation.
i. Suppliers may be attracted to only agree to take enhanced sick due to lower
the expenses and increase in the gains.
ii. To raise productivity, a health practitioner can initiate plans that keenly
eliminate measures to which the sick can be permitted.
iii. Doctors admit many patients thereby have no time to take reasonable care to
the sick.
QUESTION 2
i. Direct costs.
a. workforce expenses and commodities.
Straight expenses involving resource usage like specialised workforce and commodities
that are expected to be used within short period of time are usually candid to evaluate.
Workforce expenses are most frequent and estimated in elements of time and
The cigarette company, who does not notify cigarette smoker of the factual
medical threats of smoking.
c. Capitation is a type of a medical care remuneration structure in which a physician and
other medics fraternity in hospital is rewarded a fixed amount per sick for an agreed
duration of time medics association.
Advantages of Capitation.
i. Handling this type of structure can be stress-free and an economical structure
since the sole event in keeping trajectory of medics are the total registered
associates. Paper work is minimised.
ii. Revenue inflow is more foreseeable for physicians and participants have
more expected medical attention expenses.
iii. Precautionary attention is a durable emphasis due to the fact that it is cheap
for medics than to cure intricate and prolonged medical problem in future.
iv. Avoidable involvements, checks and attention are restricted due to doctor’s
intention to cut down cost and capitalize on improving the gains. Sick
persons should worry less on catering for additional checks.
Disadvantages of Capitation.
i. Suppliers may be attracted to only agree to take enhanced sick due to lower
the expenses and increase in the gains.
ii. To raise productivity, a health practitioner can initiate plans that keenly
eliminate measures to which the sick can be permitted.
iii. Doctors admit many patients thereby have no time to take reasonable care to
the sick.
QUESTION 2
i. Direct costs.
a. workforce expenses and commodities.
Straight expenses involving resource usage like specialised workforce and commodities
that are expected to be used within short period of time are usually candid to evaluate.
Workforce expenses are most frequent and estimated in elements of time and
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
HEALTH ECONOMICS 4
commodities of the quantities utilized. Consumable are products consumed by persons
and firms that must be substituted frequently due to their wearing and tearing ability or
rather they get finished up easily. They are also referred to as the elements of an end
goods which is used up or forever transformed in the procedure of built-up they include
chemicals among others components.
b. Investment expenses
Investment expenses which include the property, structures and apparatus need
exceptional attention. Such expenses originate from a point in time but the properties
are likely to be used for a longer time. This implies that, the value of the best forgone
alternative is spread over time. They include;
i. Autonomous investment spending it does not depend on the present
demand for products. This spending is not prepared with the gains
reason. They include government projects like construction of roads
and bridges.
ii. Financial investment refers to the spending prepared on the acquisition of
shares, bonds among other securities.
iii. Real investment refers to the expenditure made on the acquisition and
making of new capital goods. These investments rise the GDP of a
country.
iv. Gross investment refers to the whole spending incurred on obtaining new
assets such as land, machinery.
c. Overhead costs
Overheads cost indicate the cost that are frequently distributed between departments
in a hospital and single department may use different amounts of similar resource.
Thus, problems may occur when computing costs for shared resources.
d. Per diem costs.
When evaluating costs involving to a cure, a precise number can only be derived by
estimating resource usage for each sick person. Conversely, sick-based estimate is
costly and difficulties may come up when trying to allocate joint costs.
commodities of the quantities utilized. Consumable are products consumed by persons
and firms that must be substituted frequently due to their wearing and tearing ability or
rather they get finished up easily. They are also referred to as the elements of an end
goods which is used up or forever transformed in the procedure of built-up they include
chemicals among others components.
b. Investment expenses
Investment expenses which include the property, structures and apparatus need
exceptional attention. Such expenses originate from a point in time but the properties
are likely to be used for a longer time. This implies that, the value of the best forgone
alternative is spread over time. They include;
i. Autonomous investment spending it does not depend on the present
demand for products. This spending is not prepared with the gains
reason. They include government projects like construction of roads
and bridges.
ii. Financial investment refers to the spending prepared on the acquisition of
shares, bonds among other securities.
iii. Real investment refers to the expenditure made on the acquisition and
making of new capital goods. These investments rise the GDP of a
country.
iv. Gross investment refers to the whole spending incurred on obtaining new
assets such as land, machinery.
c. Overhead costs
Overheads cost indicate the cost that are frequently distributed between departments
in a hospital and single department may use different amounts of similar resource.
Thus, problems may occur when computing costs for shared resources.
d. Per diem costs.
When evaluating costs involving to a cure, a precise number can only be derived by
estimating resource usage for each sick person. Conversely, sick-based estimate is
costly and difficulties may come up when trying to allocate joint costs.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH ECONOMICS 5
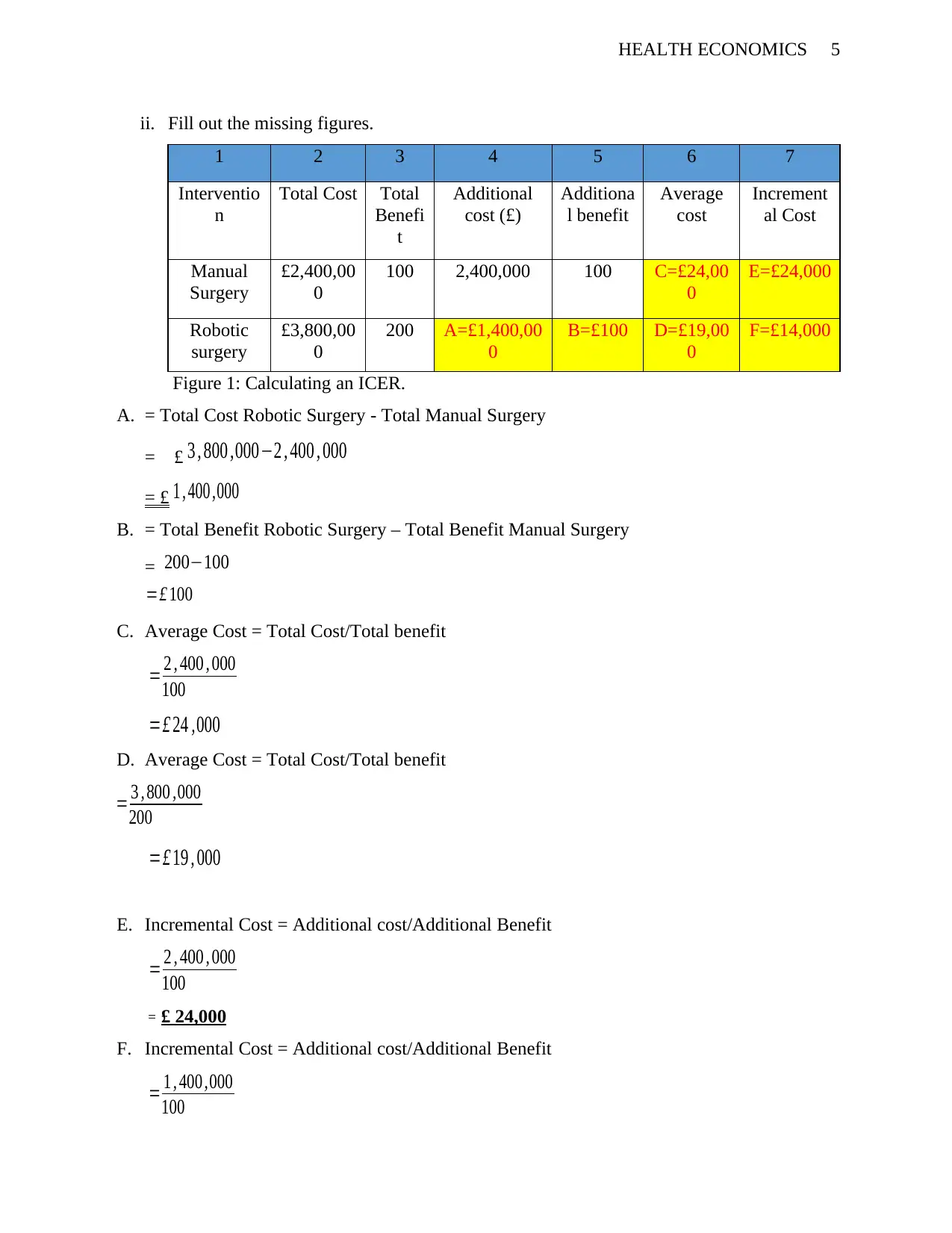
ii. Fill out the missing figures.
1 2 3 4 5 6 7
Interventio
n
Total Cost Total
Benefi
t
Additional
cost (£)
Additiona
l benefit
Average
cost
Increment
al Cost
Manual
Surgery
£2,400,00
0
100 2,400,000 100 C=£24,00
0
E=£24,000
Robotic
surgery
£3,800,00
0
200 A=£1,400,00
0
B=£100 D=£19,00
0
F=£14,000
Figure 1: Calculating an ICER.
A. = Total Cost Robotic Surgery - Total Manual Surgery
= £ 3 , 800 ,000−2 , 400 , 000
= £ 1 , 400 ,000
B. = Total Benefit Robotic Surgery – Total Benefit Manual Surgery
= 200−100
C. Average Cost = Total Cost/Total benefit
= 2 , 400 , 000
100
=£ 24 ,000
D. Average Cost = Total Cost/Total benefit
=£ 19 , 000
E. Incremental Cost = Additional cost/Additional Benefit
= 2 , 400 , 000
100
= £ 24,000
F. Incremental Cost = Additional cost/Additional Benefit
= 1 , 400 ,000
100
=£ 100
= 3 , 800 ,000
200
ii. Fill out the missing figures.
1 2 3 4 5 6 7
Interventio
n
Total Cost Total
Benefi
t
Additional
cost (£)
Additiona
l benefit
Average
cost
Increment
al Cost
Manual
Surgery
£2,400,00
0
100 2,400,000 100 C=£24,00
0
E=£24,000
Robotic
surgery
£3,800,00
0
200 A=£1,400,00
0
B=£100 D=£19,00
0
F=£14,000
Figure 1: Calculating an ICER.
A. = Total Cost Robotic Surgery - Total Manual Surgery
= £ 3 , 800 ,000−2 , 400 , 000
= £ 1 , 400 ,000
B. = Total Benefit Robotic Surgery – Total Benefit Manual Surgery
= 200−100
C. Average Cost = Total Cost/Total benefit
= 2 , 400 , 000
100
=£ 24 ,000
D. Average Cost = Total Cost/Total benefit
=£ 19 , 000
E. Incremental Cost = Additional cost/Additional Benefit
= 2 , 400 , 000
100
= £ 24,000
F. Incremental Cost = Additional cost/Additional Benefit
= 1 , 400 ,000
100
=£ 100
= 3 , 800 ,000
200
HEALTH ECONOMICS 6
=£14,000
iii. Average cost per QALY is total cost per unit of the total benefits while the Incremental
cost per QALY is the additional cost per unit of additional benefit. Incremental cost per
QALY is highly recommended because it is a measure of additional benefit as compared
to the average cost per QALY which is basically the rate of cost per unit of benefit.
iv. Opportunity cost.
The concept of opportunity cost is can be defined as the value of the best next foregone
alternative. Since resources are limited as compared to human requirement, the usage of a
resources in one way inhibits their usage in other way. The opportunity cost of spending
in a healthcare intervention is greatest reflected by the health benefits which is life of
years saved and quality adjusted life years (QALYs) increased that can be realised when
the money consumed on the next best alternative. Opportunity cost can be evaluated
straight with cost effectiveness. Opportunity cost can be measured right with cost
efficiency. When two or more participants are associated cost value efficiency analysis
creates the opportunity cost of the different uses of resources explicit. Although the
concept of opportunity cost is important, improper deductions can lead to problems in
relating the concept. First, the research viewpoint is serious since it decides which prices
and things to consist of in the assessment. A general viewpoint includes all the costs and
benefits irrespective of who gains them.
QUESTION 3.
i. The results from cures and other health-inducing happenings have two basic
constituents, the quantity and the quality of life. A QALY which is the acronym for a
quality adjusted life-year, which holds both of these constituents and is the arithmetic
creation of life expectancy and an estimate of the quality of the outstanding life-years.
The National Institute for Health and Clinical Excellence describes the QALY as an
estimate of an individual’s span of life weighted by evaluation of their health-
connected quality of life. The Quality adjusted life year offers a joint currency for
estimating the level of health achievement that resulted from healthcare interventions
and when joined with the costs linked with the interventions can be used to evaluate
=£14,000
iii. Average cost per QALY is total cost per unit of the total benefits while the Incremental
cost per QALY is the additional cost per unit of additional benefit. Incremental cost per
QALY is highly recommended because it is a measure of additional benefit as compared
to the average cost per QALY which is basically the rate of cost per unit of benefit.
iv. Opportunity cost.
The concept of opportunity cost is can be defined as the value of the best next foregone
alternative. Since resources are limited as compared to human requirement, the usage of a
resources in one way inhibits their usage in other way. The opportunity cost of spending
in a healthcare intervention is greatest reflected by the health benefits which is life of
years saved and quality adjusted life years (QALYs) increased that can be realised when
the money consumed on the next best alternative. Opportunity cost can be evaluated
straight with cost effectiveness. Opportunity cost can be measured right with cost
efficiency. When two or more participants are associated cost value efficiency analysis
creates the opportunity cost of the different uses of resources explicit. Although the
concept of opportunity cost is important, improper deductions can lead to problems in
relating the concept. First, the research viewpoint is serious since it decides which prices
and things to consist of in the assessment. A general viewpoint includes all the costs and
benefits irrespective of who gains them.
QUESTION 3.
i. The results from cures and other health-inducing happenings have two basic
constituents, the quantity and the quality of life. A QALY which is the acronym for a
quality adjusted life-year, which holds both of these constituents and is the arithmetic
creation of life expectancy and an estimate of the quality of the outstanding life-years.
The National Institute for Health and Clinical Excellence describes the QALY as an
estimate of an individual’s span of life weighted by evaluation of their health-
connected quality of life. The Quality adjusted life year offers a joint currency for
estimating the level of health achievement that resulted from healthcare interventions
and when joined with the costs linked with the interventions can be used to evaluate
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
HEALTH ECONOMICS 7
their relation value from an economic viewpoint. The quantity of life is conveyed in
terms of life expectancy, it is an old-fashioned estimation that is generally recognised
and has few difficulties of appraisal people are either alive or dead. Quality of life,
describes a complete variety of diverse aspects of individuals lives not just their
medical status. Even limiting the attention to an individual’s health-linked quality of
life will end in a number of proportions involving both physical and mental capacity.
ii. Benefits QALY
They are types of medical status index, founded on population-level information that
estimate medical gains to permit for economic evaluation of different medical
interventions. A QALY is the arithmetic results of life expectancy weighted by an
estimate of the quality of the outstanding life-years to reach a single index value. The
utility figure is zero for dead and the figure for one year of faultless-health life
expectancy is equal to one. The cost per QALY does not discuss the cost of cure but
the cost of the outcome which may be in years or quality gained or lost. Markets
favour consumers with buying power. The health industry is a free market, controlled
by purchaser preference and demand the arrival of new dealers and exit of non-
performing dealers. Within the health market, elasticity is propelled by the evidence
of purchaser independence, in which buyers have information about every good,
hence they can select a vast variety of choices available. In a free market, no one
manufacturer can influence the market price of a goods.
iii. Equity in healthcare
Several factors affect health comprising of genetic factors, which implies that
complete equality of well-being is not attainable. Balancing health can be regarded as
paternalistic because it does not permit a person favourites such as the choice to
smoke. horizontal equity means the equity between individual with the similar
medical care needs while vertical equity means to individual with uneven medical
needs and should get dissimilar medical care. This is to say, vertical equity can be
acceptable in healthcare if ethically applicable factors apply. Though, morally
inappropriate factors are not grounds for vindicating vertical equity. Commissioners
their relation value from an economic viewpoint. The quantity of life is conveyed in
terms of life expectancy, it is an old-fashioned estimation that is generally recognised
and has few difficulties of appraisal people are either alive or dead. Quality of life,
describes a complete variety of diverse aspects of individuals lives not just their
medical status. Even limiting the attention to an individual’s health-linked quality of
life will end in a number of proportions involving both physical and mental capacity.
ii. Benefits QALY
They are types of medical status index, founded on population-level information that
estimate medical gains to permit for economic evaluation of different medical
interventions. A QALY is the arithmetic results of life expectancy weighted by an
estimate of the quality of the outstanding life-years to reach a single index value. The
utility figure is zero for dead and the figure for one year of faultless-health life
expectancy is equal to one. The cost per QALY does not discuss the cost of cure but
the cost of the outcome which may be in years or quality gained or lost. Markets
favour consumers with buying power. The health industry is a free market, controlled
by purchaser preference and demand the arrival of new dealers and exit of non-
performing dealers. Within the health market, elasticity is propelled by the evidence
of purchaser independence, in which buyers have information about every good,
hence they can select a vast variety of choices available. In a free market, no one
manufacturer can influence the market price of a goods.
iii. Equity in healthcare
Several factors affect health comprising of genetic factors, which implies that
complete equality of well-being is not attainable. Balancing health can be regarded as
paternalistic because it does not permit a person favourites such as the choice to
smoke. horizontal equity means the equity between individual with the similar
medical care needs while vertical equity means to individual with uneven medical
needs and should get dissimilar medical care. This is to say, vertical equity can be
acceptable in healthcare if ethically applicable factors apply. Though, morally
inappropriate factors are not grounds for vindicating vertical equity. Commissioners
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH ECONOMICS 8
of health care are always confronted with choices concerning equity, mainly as a
result of the necessity to rank and eventually ration health care to imitate to budgetary
limitations. Common practice today is for commissioners to device importance
setting rules for the fair sharing of health care resources, mostly based on the
difference among properly applicable and inappropriate factors. Thus, not all ethical
choices will please all and hence any decision-making method concerning importance
setting should be about attaining an accord and reliability rather than essentially
attaining the correct response.
iv. Fair inning
The fair innings discussion holds that for Medicare resources to be shared equally
every individual should get adequate Medicare services to offer them with a chance
living in upright medical condition for an average length of years. What institutes a
average length of years is frequently clearly shown as lifespan at confinement but this
standard miss the mark to offer sufficient base for the equal sharing of Medicare
through and between generations. A more suitable standard for the normal life span is
the notion that the human life span is biologically limited.
v. National Institute for Health and Care Excellence firmly applies the cost-effective
threshold to make its care coverage approvals for the country's National Health
Service.
According to NICE, the choice to endorse a medical technology that has an
incremental cost effective ratio below £10,000 is usually based on cost-effective.
Above that criterion, other standard is expected to come into play which include
uncertainty, innovation and stakeholder point of view on quality of life gains.
QUESTION 4
PART A
i. Cost vs Consequences Analysis.
of health care are always confronted with choices concerning equity, mainly as a
result of the necessity to rank and eventually ration health care to imitate to budgetary
limitations. Common practice today is for commissioners to device importance
setting rules for the fair sharing of health care resources, mostly based on the
difference among properly applicable and inappropriate factors. Thus, not all ethical
choices will please all and hence any decision-making method concerning importance
setting should be about attaining an accord and reliability rather than essentially
attaining the correct response.
iv. Fair inning
The fair innings discussion holds that for Medicare resources to be shared equally
every individual should get adequate Medicare services to offer them with a chance
living in upright medical condition for an average length of years. What institutes a
average length of years is frequently clearly shown as lifespan at confinement but this
standard miss the mark to offer sufficient base for the equal sharing of Medicare
through and between generations. A more suitable standard for the normal life span is
the notion that the human life span is biologically limited.
v. National Institute for Health and Care Excellence firmly applies the cost-effective
threshold to make its care coverage approvals for the country's National Health
Service.
According to NICE, the choice to endorse a medical technology that has an
incremental cost effective ratio below £10,000 is usually based on cost-effective.
Above that criterion, other standard is expected to come into play which include
uncertainty, innovation and stakeholder point of view on quality of life gains.
QUESTION 4
PART A
i. Cost vs Consequences Analysis.
HEALTH ECONOMICS 9
It is a organised explanation and estimation of a fixed involvement qualities intended for
consideration during decision making.
The technique fails to recommend a judgment rule.
Offers evidence to judges and opinion maker decide their choice.
Demerit is that weighing of dissimilar features is left to person’s judgement making
which include:
- Rise in well-being of choice maker.
- The choice by person might cannot be in the best interest of the sick.
Cost vs Benefit Analysis
They are procedures a corporate would use to analyse financial decisions. Fiscal figures
on expenses and results hence permitting judgment of projects through the whole
economy.
The real-world problem of fiscal estimation of paybacks and the importance of difficult
health issue engaging a dollar worth on human life hinders the usage of Cost Benefit
Analysis.
CBA permits the evaluation of essential figures. For instance, if benefits are greater than
costs the intervention is worth proceeding with it.
Cost vs Utility Analysis
It uses a non-fiscal shared metric that permit judgements through the medical segment.
For instance, comparing varying medications.
Metric is a blend of lifespan and value of life expectancy referred to as Quality adjusted
life year and Disability adjusted life year.
It might not capture inter medical segment assessments totally and Some medical
involvements have other effects which must be willingly itemized as ideas to the
judgement process
It requires studies to measure utility or disability weights.
ii. The National Institute for Health and Clinical Excellence’s technology appraisal of
drugs for Alzheimer’s disease, a major discussion point was whether the costs falling
It is a organised explanation and estimation of a fixed involvement qualities intended for
consideration during decision making.
The technique fails to recommend a judgment rule.
Offers evidence to judges and opinion maker decide their choice.
Demerit is that weighing of dissimilar features is left to person’s judgement making
which include:
- Rise in well-being of choice maker.
- The choice by person might cannot be in the best interest of the sick.
Cost vs Benefit Analysis
They are procedures a corporate would use to analyse financial decisions. Fiscal figures
on expenses and results hence permitting judgment of projects through the whole
economy.
The real-world problem of fiscal estimation of paybacks and the importance of difficult
health issue engaging a dollar worth on human life hinders the usage of Cost Benefit
Analysis.
CBA permits the evaluation of essential figures. For instance, if benefits are greater than
costs the intervention is worth proceeding with it.
Cost vs Utility Analysis
It uses a non-fiscal shared metric that permit judgements through the medical segment.
For instance, comparing varying medications.
Metric is a blend of lifespan and value of life expectancy referred to as Quality adjusted
life year and Disability adjusted life year.
It might not capture inter medical segment assessments totally and Some medical
involvements have other effects which must be willingly itemized as ideas to the
judgement process
It requires studies to measure utility or disability weights.
ii. The National Institute for Health and Clinical Excellence’s technology appraisal of
drugs for Alzheimer’s disease, a major discussion point was whether the costs falling
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
HEALTH ECONOMICS 10
on caregivers should be included as well as costs to the National Health Service. The
main disagreement for accepting a preventive viewpoint is that the budget for the
National Health Service is meant to be for improving health. Thus, the applicable
attention in assessing interventions is the opportunity cost on the Medicare budget.
Economic evaluation relates the costs and significances of other courses of action.
The cost efficiency of an interference or programme is measured to ensure maximum
health improvement from the limited obtainable resources. If resources are used for
intrusions that are not cost operational, the populace as a total gains fewer health
benefits. Hence, a balance must be struck among effective distribution of resources on
the one hand and a reasonable distribution of those resources on the other. Public
health approvals should be founded on the balance between the projected cost of each
interference and the probable health benefits. Approvals should not be made on the
ground of the total cost or the resource impact of implementing them. Therefore, if
the proof proposes that an intercession offers health benefits and the cost per
individual of doing so is recommended even if it would be costly to carry on with the
project through the entire populace.
PART B.
i. Willing to pay. (WTP)
The objective of Willing to pay is to estimate the comparable difference for the
product in question. Comparable difference is the suitable estimate when an
individual must buy goods such as an upgrading the environmental quality. Both
compensating and comparable variation can be produced by asking an individual to
report a willingness to pay amount. For example, the person may be asked to report
his WTP to obtain the good or to avoid the loss of the good. Legally, WTP is well-
defined as the amount that must be taken away from an individual revenue while
keeping his utility constant.
ii. Strengths and weaknesses of Willing to pay
Strengths.
a. The method is most reliable if firm procedures are followed.
on caregivers should be included as well as costs to the National Health Service. The
main disagreement for accepting a preventive viewpoint is that the budget for the
National Health Service is meant to be for improving health. Thus, the applicable
attention in assessing interventions is the opportunity cost on the Medicare budget.
Economic evaluation relates the costs and significances of other courses of action.
The cost efficiency of an interference or programme is measured to ensure maximum
health improvement from the limited obtainable resources. If resources are used for
intrusions that are not cost operational, the populace as a total gains fewer health
benefits. Hence, a balance must be struck among effective distribution of resources on
the one hand and a reasonable distribution of those resources on the other. Public
health approvals should be founded on the balance between the projected cost of each
interference and the probable health benefits. Approvals should not be made on the
ground of the total cost or the resource impact of implementing them. Therefore, if
the proof proposes that an intercession offers health benefits and the cost per
individual of doing so is recommended even if it would be costly to carry on with the
project through the entire populace.
PART B.
i. Willing to pay. (WTP)
The objective of Willing to pay is to estimate the comparable difference for the
product in question. Comparable difference is the suitable estimate when an
individual must buy goods such as an upgrading the environmental quality. Both
compensating and comparable variation can be produced by asking an individual to
report a willingness to pay amount. For example, the person may be asked to report
his WTP to obtain the good or to avoid the loss of the good. Legally, WTP is well-
defined as the amount that must be taken away from an individual revenue while
keeping his utility constant.
ii. Strengths and weaknesses of Willing to pay
Strengths.
a. The method is most reliable if firm procedures are followed.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH ECONOMICS 11
b. The only method obtainable to a researcher who is looking for non-use values.
c. Figures usually includes consumer surplus.
d. Gives net values, hence there is no need to deduct cost
e. Is best used to quantify environmental benefits that have no market value.
f. Focuses on ex-ante valuation.
g. Involves direct estimation of willingness to pay and willingness to accept.
h. Allows for valuation of a variety of different environmental goods.
Some of these weaknesses of the include:
a. People find it hard to distinct environmental values from wider values.
b. Has quite a number of biasness.
c. It also has reliability issues.
d. Low income and standard of living are a very big problem on WTP.
e. Equally has ethical issues especially in developing countries
f. There is the disagreement over whether people would actually pay the amounts as
stated in interviews.
iii. Quality adjusted life years and willingness to pay are substitute estimates of the value
of decreases in medical risk that are frequently used in assessing environmental,
health and safety practices. Although both approaches are based on personal choices,
the essential expectations vary. The dissimilar bases yield systematically diverse
results about the comparative value of decreasing health and mortality risks to
persons that vary in age, medical conditions, income among other factors. The choice
of which technique to use is influenced by decisions about what restrictions should be
placed on person’s choice. The QALY and WTP frameworks have common
resemblances both are acceptable as on behalf of the choices of persons and both are
summed through persons to signify the social value of a change in medical risk. The
dissimilarities may lead to varying assumptions about whether a policy raise or
lowers aggregate health risk.
QUESTION 5
i. MB/MC
Program A = £140/2000
b. The only method obtainable to a researcher who is looking for non-use values.
c. Figures usually includes consumer surplus.
d. Gives net values, hence there is no need to deduct cost
e. Is best used to quantify environmental benefits that have no market value.
f. Focuses on ex-ante valuation.
g. Involves direct estimation of willingness to pay and willingness to accept.
h. Allows for valuation of a variety of different environmental goods.
Some of these weaknesses of the include:
a. People find it hard to distinct environmental values from wider values.
b. Has quite a number of biasness.
c. It also has reliability issues.
d. Low income and standard of living are a very big problem on WTP.
e. Equally has ethical issues especially in developing countries
f. There is the disagreement over whether people would actually pay the amounts as
stated in interviews.
iii. Quality adjusted life years and willingness to pay are substitute estimates of the value
of decreases in medical risk that are frequently used in assessing environmental,
health and safety practices. Although both approaches are based on personal choices,
the essential expectations vary. The dissimilar bases yield systematically diverse
results about the comparative value of decreasing health and mortality risks to
persons that vary in age, medical conditions, income among other factors. The choice
of which technique to use is influenced by decisions about what restrictions should be
placed on person’s choice. The QALY and WTP frameworks have common
resemblances both are acceptable as on behalf of the choices of persons and both are
summed through persons to signify the social value of a change in medical risk. The
dissimilarities may lead to varying assumptions about whether a policy raise or
lowers aggregate health risk.
QUESTION 5
i. MB/MC
Program A = £140/2000
HEALTH ECONOMICS 12
= 0.07
MB/MC
Program B = £360/3500
= 0.10
From the data above and considering the values of the calculation it is apparent that
the resource should be moved from Program A to B. This is because the value of the
benefit that is anticipated to be gained from program B is greater than the benefit that
would be foregone from program A when relocating all its resources to Program B.
ii. One would stop reallocation process when dividing MB/MC gives one at that
particular point the program budgeting and marginal analysis is at equilibrium and
there will be no essence of reallocating process.
iii. The best accessible information is later recycled to estimate the price and outputs for
each of the program as indicated on the table. Productions should be measured in
relations to willingly accessible estimates, for instance, sums of sick attended. This
technique, as a result, offers a mechanism to decide the cost is that is expended and
the results realised. It is projected only to offer the framework for assessment. The
appraisal recognised five working sub-groups for sustenance the appraisal, as defined
below. Information from each of these clusters was abridged and then joined and
compared into summary booklets for each enterprise. During this summary procedure
the appraisal teams approved that a scoring system was necessary to assist guide the
panel. A traffic lighting structure was decided as the most suitable and visually
operative system. Each of the suggestion appraisal sub-teams applied a traffic lighting
evaluation system to their particular stream of suggestion and then a complete traffic
lighting rating was allocated to each program founded upon all the accessible
suggestion assembled by the different groups. The complete traffic lighting rating had
the results indicated as Red, based on available suggestion and discussion, this
intercession was questionable to bring a populace health benefit and option should be
discovered to attain these health goals. Amber, bigger suggestion requires to be based
for the impact of this program at a population level and there are components of the
program that required considerable revision or there is inadequate suggestion
= 0.07
MB/MC
Program B = £360/3500
= 0.10
From the data above and considering the values of the calculation it is apparent that
the resource should be moved from Program A to B. This is because the value of the
benefit that is anticipated to be gained from program B is greater than the benefit that
would be foregone from program A when relocating all its resources to Program B.
ii. One would stop reallocation process when dividing MB/MC gives one at that
particular point the program budgeting and marginal analysis is at equilibrium and
there will be no essence of reallocating process.
iii. The best accessible information is later recycled to estimate the price and outputs for
each of the program as indicated on the table. Productions should be measured in
relations to willingly accessible estimates, for instance, sums of sick attended. This
technique, as a result, offers a mechanism to decide the cost is that is expended and
the results realised. It is projected only to offer the framework for assessment. The
appraisal recognised five working sub-groups for sustenance the appraisal, as defined
below. Information from each of these clusters was abridged and then joined and
compared into summary booklets for each enterprise. During this summary procedure
the appraisal teams approved that a scoring system was necessary to assist guide the
panel. A traffic lighting structure was decided as the most suitable and visually
operative system. Each of the suggestion appraisal sub-teams applied a traffic lighting
evaluation system to their particular stream of suggestion and then a complete traffic
lighting rating was allocated to each program founded upon all the accessible
suggestion assembled by the different groups. The complete traffic lighting rating had
the results indicated as Red, based on available suggestion and discussion, this
intercession was questionable to bring a populace health benefit and option should be
discovered to attain these health goals. Amber, bigger suggestion requires to be based
for the impact of this program at a population level and there are components of the
program that required considerable revision or there is inadequate suggestion
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.