Indigenous Health and Structural Inequality
VerifiedAdded on 2020/06/06
|8
|2245
|43
AI Summary
This assignment delves into the critical issue of Indigenous health in Australia, focusing on the pervasive impact of structural inequities. It analyzes various factors contributing to health disparities, including social determinants of health, historical trauma, and systemic racism. The document explores solutions and strategies aimed at addressing these inequalities and promoting equitable health outcomes for Indigenous communities.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Health Equity in Aboriginal and Strait
Islander Young Males
Islander Young Males
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
TABLE OF CONTENTS
1. INTRODUCTION.......................................................................................................................1
2. Brief description of the group.............................................................................................1
3. Structural determinants in provision of Public Health Services.........................................1
4. Influence of Culture and beliefs in accessing the public health services...........................2
5. Evaluating the influence of acceptance and accessibility in public health and services....3
6. Practical ways in which the public health services could be improved.............................4
CONCLUSION................................................................................................................................5
REFERENCES................................................................................................................................6
1. INTRODUCTION.......................................................................................................................1
2. Brief description of the group.............................................................................................1
3. Structural determinants in provision of Public Health Services.........................................1
4. Influence of Culture and beliefs in accessing the public health services...........................2
5. Evaluating the influence of acceptance and accessibility in public health and services....3
6. Practical ways in which the public health services could be improved.............................4
CONCLUSION................................................................................................................................5
REFERENCES................................................................................................................................6
1. INTRODUCTION
Aboriginal and Torres Islander people are the first citizen in Australian region. The
traditional definitions of these people were based on the colour which have been replaced with
modern definition which emphasis on the ancestry and identification. They constitute diverse
Aboriginal nation which have their own language and tradition (Tsey and et. al., 2011). They
reside on the offshore islands of Australia and Tasmania. Whereas the Torres Strait people reside
in the islands of Torres Strait, Queensland and Papua New Guinea. Health equity is a discipline
which focuses on studying the causes in the quality of healthcare among diversified population
(Adams and et. al., 2012). This report focuses on understanding the health equity in aboriginal
and strait islander young males and find out the best strategies to overcome the inequities.
2. Brief description of the group
The Aboriginal and Torres Islander are both described as indigenous. This term identifies
have evolved under law which identifies the relation of aboriginal people will the particular
territory. These people are treated to be the descendants of the country. These people have a
diverse social, economic and political characteristics. According to the 2001 census there were
548,370 inhabitants. 33% of these people are residing in capital city areas where as 73% of the
population lives outside the capital city areas. A whopping 60% of the male population are under
the age of 25. The major areas of residence of Indigenous Australians are New South Wales,
Queensland, Western Australia and Tasmania (Atkinson, 2016). They believe in passing their
cultural heritage from one generation to another. In form of knowledge, arts and rituals. The
recent research conducted proved that 11% of these people use their cultural language at home.
3. Structural determinants in provision of Public Health Services
The structural determinants are the determinants which takes into account the age, family
structure, education, income and social support. There are some public health services which are
specially designed to provide the public health facilities to the indigenous people which can
further carried out keeping in mind the structural determinants (Australia’s frightening health-
wealth gap, 2017). There can be seen a rise of 15% in the government expenses for the
indigenous people. In this case the people under the age group of 25% is the highest. The level of
education of these people is 25% in capital cities and 8% in outside area compare to 46% and
35% in non- indigenous population. These young males face an unemployment rate of over 20%
1
Aboriginal and Torres Islander people are the first citizen in Australian region. The
traditional definitions of these people were based on the colour which have been replaced with
modern definition which emphasis on the ancestry and identification. They constitute diverse
Aboriginal nation which have their own language and tradition (Tsey and et. al., 2011). They
reside on the offshore islands of Australia and Tasmania. Whereas the Torres Strait people reside
in the islands of Torres Strait, Queensland and Papua New Guinea. Health equity is a discipline
which focuses on studying the causes in the quality of healthcare among diversified population
(Adams and et. al., 2012). This report focuses on understanding the health equity in aboriginal
and strait islander young males and find out the best strategies to overcome the inequities.
2. Brief description of the group
The Aboriginal and Torres Islander are both described as indigenous. This term identifies
have evolved under law which identifies the relation of aboriginal people will the particular
territory. These people are treated to be the descendants of the country. These people have a
diverse social, economic and political characteristics. According to the 2001 census there were
548,370 inhabitants. 33% of these people are residing in capital city areas where as 73% of the
population lives outside the capital city areas. A whopping 60% of the male population are under
the age of 25. The major areas of residence of Indigenous Australians are New South Wales,
Queensland, Western Australia and Tasmania (Atkinson, 2016). They believe in passing their
cultural heritage from one generation to another. In form of knowledge, arts and rituals. The
recent research conducted proved that 11% of these people use their cultural language at home.
3. Structural determinants in provision of Public Health Services
The structural determinants are the determinants which takes into account the age, family
structure, education, income and social support. There are some public health services which are
specially designed to provide the public health facilities to the indigenous people which can
further carried out keeping in mind the structural determinants (Australia’s frightening health-
wealth gap, 2017). There can be seen a rise of 15% in the government expenses for the
indigenous people. In this case the people under the age group of 25% is the highest. The level of
education of these people is 25% in capital cities and 8% in outside area compare to 46% and
35% in non- indigenous population. These young males face an unemployment rate of over 20%
1
which means they rely on the public health services provided to them. Young indigenous males
face bigger challenges than the indigenous population. Young males have suffered a disruption
in their background due to the continuous alcohol and sexual abuse. The maximum provision of
the health facilities is to be done for the younger male as it carries a large part of the population.
The general health of these people categorised into fair and poor. The main diseases faced by
these people are asthma and long term health problems which is 17% more than the non-
indigenous people.
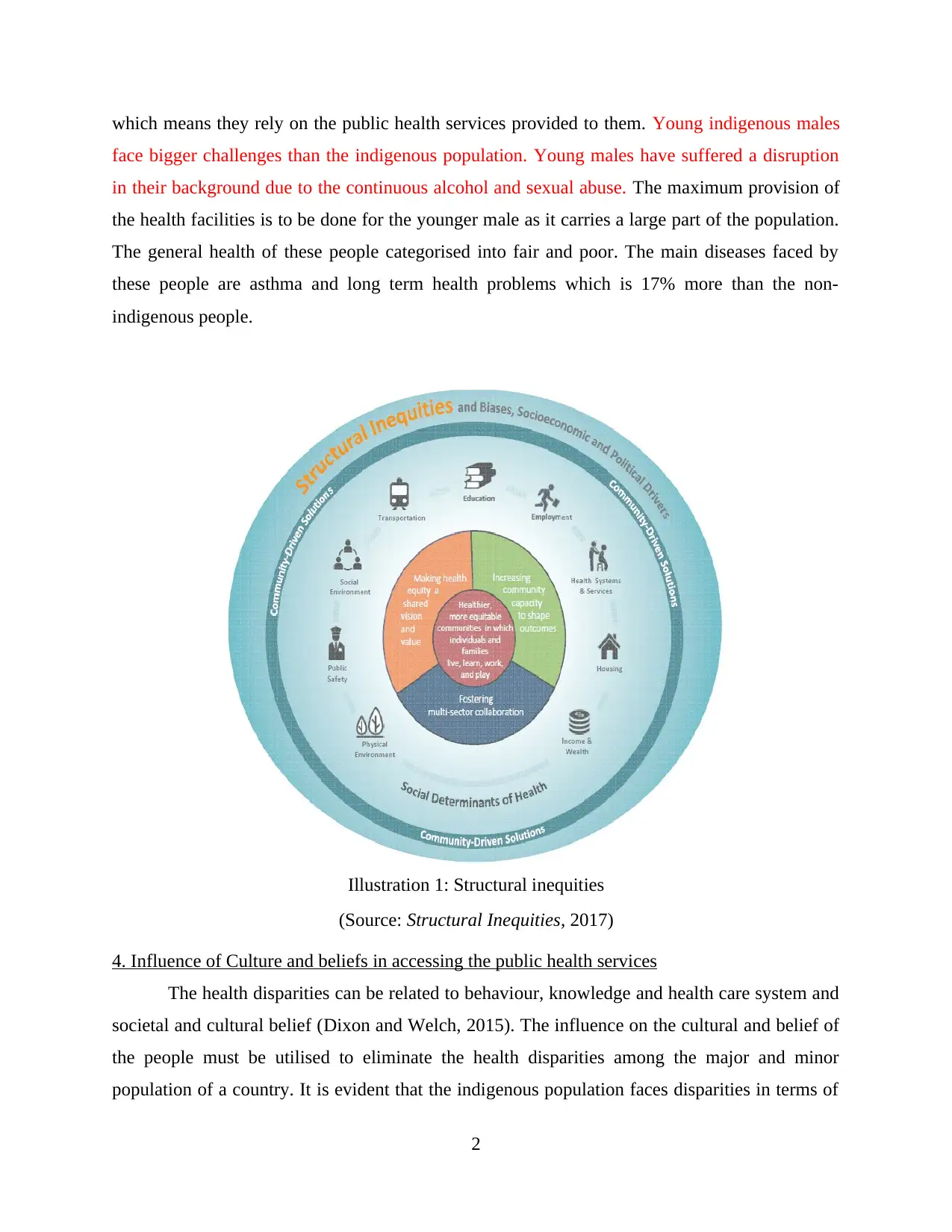
(Source: Structural Inequities, 2017)
4. Influence of Culture and beliefs in accessing the public health services
The health disparities can be related to behaviour, knowledge and health care system and
societal and cultural belief (Dixon and Welch, 2015). The influence on the cultural and belief of
the people must be utilised to eliminate the health disparities among the major and minor
population of a country. It is evident that the indigenous population faces disparities in terms of
2
Illustration 1: Structural inequities
face bigger challenges than the indigenous population. Young males have suffered a disruption
in their background due to the continuous alcohol and sexual abuse. The maximum provision of
the health facilities is to be done for the younger male as it carries a large part of the population.
The general health of these people categorised into fair and poor. The main diseases faced by
these people are asthma and long term health problems which is 17% more than the non-
indigenous people.
(Source: Structural Inequities, 2017)
4. Influence of Culture and beliefs in accessing the public health services
The health disparities can be related to behaviour, knowledge and health care system and
societal and cultural belief (Dixon and Welch, 2015). The influence on the cultural and belief of
the people must be utilised to eliminate the health disparities among the major and minor
population of a country. It is evident that the indigenous population faces disparities in terms of
2
Illustration 1: Structural inequities
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
income, health disparity and social status. Young males are a victim of drug, depression and
cultural dispersion. The policy makers can provide quality health service and intervention to
shorten the gap between indigenous and non- indigenous people. Matching the cultural
characteristics of the indigenous people will help and promote the acceptance and provision of
health programs. The cultural factors, belief and attitudes can be used as a tool to filter the
information received (Donald and et. al., 2013). In developing effective health communication
programs require active involvement of the cultural and social beliefs. The social determinants
such as circumstances in which people have born, grow, work and live are believed to be the root
causes of the health inequities in the young indigenous males. Young Aboriginal and Torres
Strait and Islander males faced with number of health and social issues that are:
Child and domestic abuse
High suicide rates
Drug and alcohol abuse
Detention of juveniles (constitutes 90% of the young males)
5. Evaluating the influence of acceptance and accessibility in public health and services
1. Inter-cultural communication
Inter-cultural communication is essential in a nation where different cultures reside. This
is important to facilitate communication with resident foreigner male people. A health operator
who is to provide health services to these people requires adequate tools and competences to
facilitate effective interaction overcoming the language and cultural distances. The knowledge of
the culture is important as it to fulfil the health needs of a person.
2. Health professional behaviour
Health professional are the people who are given the task to work with the local
communities in a region. These professionals are responsible in raising the awareness about the
various illnesses and diseases. The death rate of indigenous is twice compared to people of
Australian region (Eades, 2011). The infant mortality rate is 11 deaths per 1000 births and the
most importantly the life expectancy of these people is 56 years compared to Australian male is
77 years. The difference in health condition are of major concern. The health professional can
3
cultural dispersion. The policy makers can provide quality health service and intervention to
shorten the gap between indigenous and non- indigenous people. Matching the cultural
characteristics of the indigenous people will help and promote the acceptance and provision of
health programs. The cultural factors, belief and attitudes can be used as a tool to filter the
information received (Donald and et. al., 2013). In developing effective health communication
programs require active involvement of the cultural and social beliefs. The social determinants
such as circumstances in which people have born, grow, work and live are believed to be the root
causes of the health inequities in the young indigenous males. Young Aboriginal and Torres
Strait and Islander males faced with number of health and social issues that are:
Child and domestic abuse
High suicide rates
Drug and alcohol abuse
Detention of juveniles (constitutes 90% of the young males)
5. Evaluating the influence of acceptance and accessibility in public health and services
1. Inter-cultural communication
Inter-cultural communication is essential in a nation where different cultures reside. This
is important to facilitate communication with resident foreigner male people. A health operator
who is to provide health services to these people requires adequate tools and competences to
facilitate effective interaction overcoming the language and cultural distances. The knowledge of
the culture is important as it to fulfil the health needs of a person.
2. Health professional behaviour
Health professional are the people who are given the task to work with the local
communities in a region. These professionals are responsible in raising the awareness about the
various illnesses and diseases. The death rate of indigenous is twice compared to people of
Australian region (Eades, 2011). The infant mortality rate is 11 deaths per 1000 births and the
most importantly the life expectancy of these people is 56 years compared to Australian male is
77 years. The difference in health condition are of major concern. The health professional can
3
effectively communicate about the diseases and can raise awareness about certain illnesses which
are in big numbers. Educate them about the government’s health care programs and equips these
people with strategies which can help improve their standard of life. The matriarchal structure
have adversely affected the development of young islander males. The importance of the role
played by men needs to be restored in order to fulfil the requirements of the family. Professional
s needs to evaluate the status of young males and engage them to restore their identity in the
society.
3. Service structure, organisation and functioning
The public service is responsible for management and funding of health service to the
citizens. There are more than 220 public hospitals which caters the medical needs of people. The
expenditure on health services is 5% higher than that of non- indigenous people. The extra
expenditure is required to reduce the health inequity between these communities. The indigenous
people use more public health services due to their negligible income (Hinkson and Harris,
2012). The young males are reluctant in accepting and availing the public health service as they
believe that these are for old people and the another big reason is that they are ashamed in
availing the public health services. The Aboriginal and Torres Strait Islander services have
established to cater the needs of these people but they are not aware about the health people
visiting their community.
6. Practical ways in which the public health services could be improved
The link between the public health service and health outcomes of the people could be
improved with application of these strategies.
AHW can promote the use of public health services by educating young males through
schools and youth groups.
Providing the alternate to alcohol and drugs by organising recreational activities such as
sports, hunting trips and addressing the drug problems.
The provision of contraceptives to young males can help protect them form sexually
transmitted infections and HIV. Providing adequate information and establishing regular
health check-ups for the young indigenous males.
Supporting mental health so that they males are able to build their identity and self-
esteem can help them in progressing.
4
are in big numbers. Educate them about the government’s health care programs and equips these
people with strategies which can help improve their standard of life. The matriarchal structure
have adversely affected the development of young islander males. The importance of the role
played by men needs to be restored in order to fulfil the requirements of the family. Professional
s needs to evaluate the status of young males and engage them to restore their identity in the
society.
3. Service structure, organisation and functioning
The public service is responsible for management and funding of health service to the
citizens. There are more than 220 public hospitals which caters the medical needs of people. The
expenditure on health services is 5% higher than that of non- indigenous people. The extra
expenditure is required to reduce the health inequity between these communities. The indigenous
people use more public health services due to their negligible income (Hinkson and Harris,
2012). The young males are reluctant in accepting and availing the public health service as they
believe that these are for old people and the another big reason is that they are ashamed in
availing the public health services. The Aboriginal and Torres Strait Islander services have
established to cater the needs of these people but they are not aware about the health people
visiting their community.
6. Practical ways in which the public health services could be improved
The link between the public health service and health outcomes of the people could be
improved with application of these strategies.
AHW can promote the use of public health services by educating young males through
schools and youth groups.
Providing the alternate to alcohol and drugs by organising recreational activities such as
sports, hunting trips and addressing the drug problems.
The provision of contraceptives to young males can help protect them form sexually
transmitted infections and HIV. Providing adequate information and establishing regular
health check-ups for the young indigenous males.
Supporting mental health so that they males are able to build their identity and self-
esteem can help them in progressing.
4
Community Engagement: The health outcomes could be improved by involving or
encouraging the participation of indigenous young males. Suppprting their well- being of
males emotionally and physically will help in providing equal chances of development.
Including them in the formal structure so that ATSI have a better understanding of their
problems (Hunter, 2007).
Delivery of primary health care programs ensures better long term health of the
indigenous people. These programs will detect the chronic diseases at the treatable stage.
Community favouring approaches: the approaches adopted should able to provide
organised service and medical services to dispersed population.
Multidisciplinary approaches: the approach not only cater the medical needs but also
focuses on providing employment and other opportunities which help them physically,
economically and socially (Hunter, 2016).
Evidence based approaches: the evidence reflect the current circumstances. Which can be
considered to develop quality improvement programs and adapting to the local conditions
of these people.
CONCLUSION
The availability and accessibility for the indigenous people is confined to a limited
number. The government have formed ATSI to look after the need of the people in Aboriginal
and Torres Strait Island. The health equity between the people indigenous and non- indigenous
people is rising. The average health expectancy and the number of infant mortality rate is higher
than Australians. The level of inter- cultural communication and the health professional are still
not able to achieve the desired results. The government need to adopt various interactive and
inclusive programs. Such as community development, multidisciplinary approaches so that there
is minimum health issues faced by these people and economic and social justice can be restored
in the country.
5
encouraging the participation of indigenous young males. Suppprting their well- being of
males emotionally and physically will help in providing equal chances of development.
Including them in the formal structure so that ATSI have a better understanding of their
problems (Hunter, 2007).
Delivery of primary health care programs ensures better long term health of the
indigenous people. These programs will detect the chronic diseases at the treatable stage.
Community favouring approaches: the approaches adopted should able to provide
organised service and medical services to dispersed population.
Multidisciplinary approaches: the approach not only cater the medical needs but also
focuses on providing employment and other opportunities which help them physically,
economically and socially (Hunter, 2016).
Evidence based approaches: the evidence reflect the current circumstances. Which can be
considered to develop quality improvement programs and adapting to the local conditions
of these people.
CONCLUSION
The availability and accessibility for the indigenous people is confined to a limited
number. The government have formed ATSI to look after the need of the people in Aboriginal
and Torres Strait Island. The health equity between the people indigenous and non- indigenous
people is rising. The average health expectancy and the number of infant mortality rate is higher
than Australians. The level of inter- cultural communication and the health professional are still
not able to achieve the desired results. The government need to adopt various interactive and
inclusive programs. Such as community development, multidisciplinary approaches so that there
is minimum health issues faced by these people and economic and social justice can be restored
in the country.
5
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
REFERENCES
Books and Journals
Adams, K. and et. al., 2012. Use of participatory research and photo‐voice to support urban
Aboriginal healthy eating. Health & social care in the community. 20(5). pp.497-505.
Atkinson, J., 2016. Violence against Aboriginal women: reconstitution of community law-the
way forward.[This article is reproduced from Aboriginal Law Bulletin v. 2, no. 46,
October 1990 p. 6-9.]. Indigenous Law Bulletin. 6(27). p.13.
Dixon, J. and Welch, N., 2015. Researching the rural–metropolitan health differential using the
‘social determinants of health’. Australian Journal of Rural Health. 8(5). pp.254-260.
Donald, M. and et. al., 2013. The Queensland Young People's Mental Health Survey Report.
Public Health Services, Queensland Health, GPO Box 48, Brisbane, Queensland,
Australia, 4001.
Eades, S.J., 2011. Reconciliation, social equity and Indigenous health. Aboriginal and Islander
Health Worker Journal. 24(3). p.3.
Hinkson, M. and Harris, A., 2001. Aboriginal Sydney: a guide to important places of the past
and present. Canberra: Aboriginal Studies Press.
Hunter, E., 2012. ‘Best intentions’ lives on: untoward health outcomes of some contemporary
initiatives in Indigenous affairs. Australian & New Zealand Journal of Psychiatry. 36(5).
pp.575-584.
Hunter, E., 2016. Disadvantage and discontent: A review of issues relevant to the mental health
of rural and remote Indigenous Australians. Australian Journal of Rural Health. 15(2).
pp.88-93.
Schwab, R.G., 2015. Twenty years of policy recommendations for indigenous education:
overview and research implications. Australian National University, Centre for
Aboriginal Economic Policy Research.
Tsey, K. and et. al., 2011. Indigenous men taking their rightful place in society? A preliminary
analysis of a participatory action research process with Yarrabah men's health group.
Australian Journal of Rural Health. 10(6). pp.278-284.
Online
Australia’s frightening health-wealth gap. 2017 [online]. Available
through:<http://www.adelaidenow.com.au/lifestyle/health/australias-frightening-
healthwealth-gap/news-story/7f30190e661c978537720a1db3b49188>.[Accessed on 9th
October 2017].
6
Books and Journals
Adams, K. and et. al., 2012. Use of participatory research and photo‐voice to support urban
Aboriginal healthy eating. Health & social care in the community. 20(5). pp.497-505.
Atkinson, J., 2016. Violence against Aboriginal women: reconstitution of community law-the
way forward.[This article is reproduced from Aboriginal Law Bulletin v. 2, no. 46,
October 1990 p. 6-9.]. Indigenous Law Bulletin. 6(27). p.13.
Dixon, J. and Welch, N., 2015. Researching the rural–metropolitan health differential using the
‘social determinants of health’. Australian Journal of Rural Health. 8(5). pp.254-260.
Donald, M. and et. al., 2013. The Queensland Young People's Mental Health Survey Report.
Public Health Services, Queensland Health, GPO Box 48, Brisbane, Queensland,
Australia, 4001.
Eades, S.J., 2011. Reconciliation, social equity and Indigenous health. Aboriginal and Islander
Health Worker Journal. 24(3). p.3.
Hinkson, M. and Harris, A., 2001. Aboriginal Sydney: a guide to important places of the past
and present. Canberra: Aboriginal Studies Press.
Hunter, E., 2012. ‘Best intentions’ lives on: untoward health outcomes of some contemporary
initiatives in Indigenous affairs. Australian & New Zealand Journal of Psychiatry. 36(5).
pp.575-584.
Hunter, E., 2016. Disadvantage and discontent: A review of issues relevant to the mental health
of rural and remote Indigenous Australians. Australian Journal of Rural Health. 15(2).
pp.88-93.
Schwab, R.G., 2015. Twenty years of policy recommendations for indigenous education:
overview and research implications. Australian National University, Centre for
Aboriginal Economic Policy Research.
Tsey, K. and et. al., 2011. Indigenous men taking their rightful place in society? A preliminary
analysis of a participatory action research process with Yarrabah men's health group.
Australian Journal of Rural Health. 10(6). pp.278-284.
Online
Australia’s frightening health-wealth gap. 2017 [online]. Available
through:<http://www.adelaidenow.com.au/lifestyle/health/australias-frightening-
healthwealth-gap/news-story/7f30190e661c978537720a1db3b49188>.[Accessed on 9th
October 2017].
6
1 out of 8
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.