Comparative Analysis: Healthcare Systems of Australia, Canada, Sweden
VerifiedAdded on 2022/11/18
|9
|2457
|191
Report
AI Summary
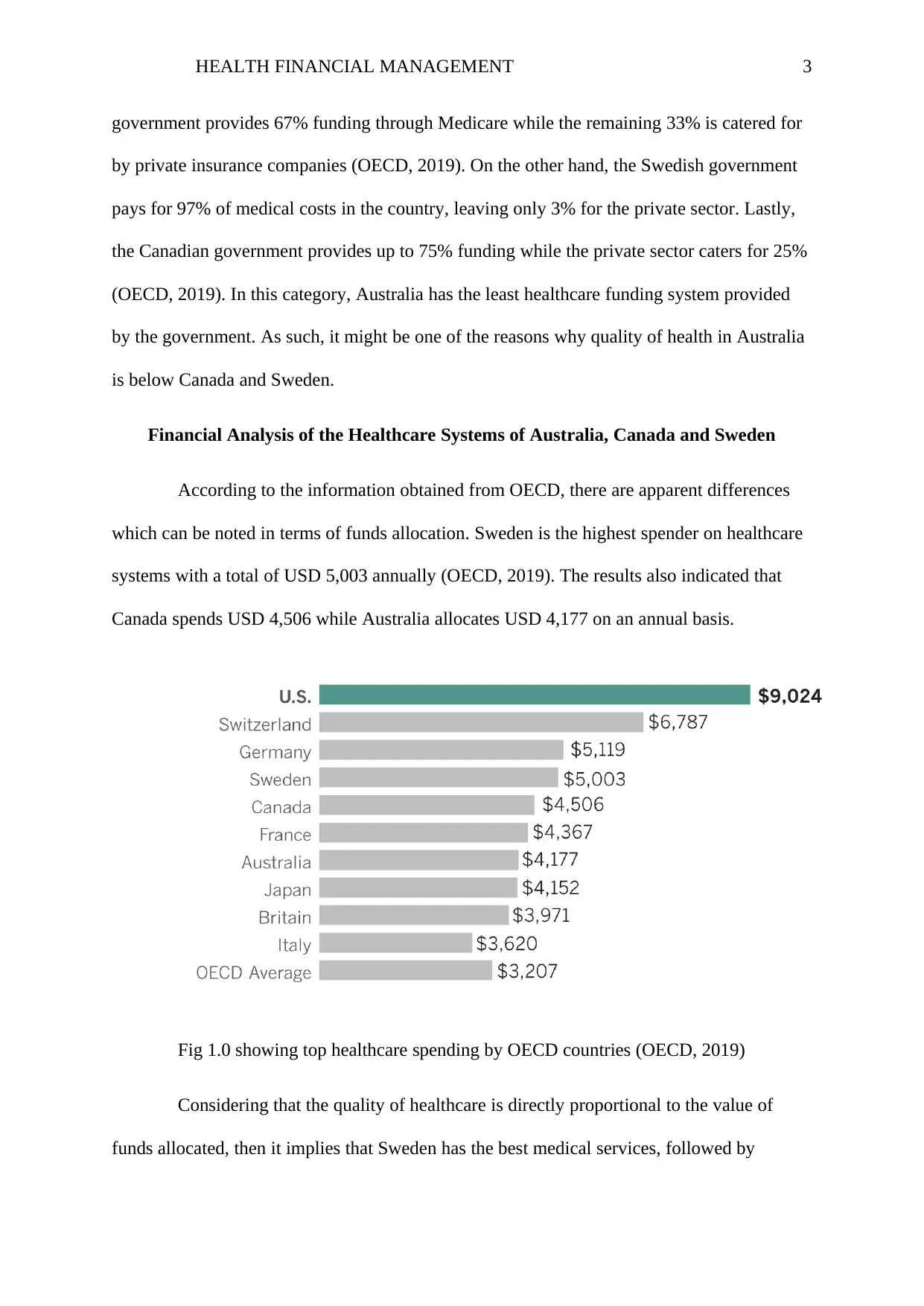
This report provides a comprehensive comparative analysis of the healthcare systems in Australia, Canada, and Sweden, focusing on their financial management. It examines the funding structures, including government allocations, private insurance, and direct payments, highlighting the roles of Medicare in Australia and universal healthcare in Canada and Sweden. The report delves into financial performance measures, such as healthcare spending per capita and the proportion of GDP allocated to healthcare, revealing that Sweden spends the most, followed by Canada, and then Australia. It also discusses the performance of these systems, considering factors like practitioner fees, specialist fees, and emergency services. The report further analyzes the financial implications for citizens, including taxation, medical levies, and insurance premiums, and identifies key challenges, such as demographic changes, the mix of private and public funding, and technological costs. Finally, it offers recommendations to improve efficiency, promote public funding, and standardize healthcare packages to enhance service delivery and achieve better healthcare outcomes in these countries. The report concludes that adjustments to the Medicare program can help Australia achieve the level of healthcare provision seen in Sweden and Canada.

1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.