Health Information Management
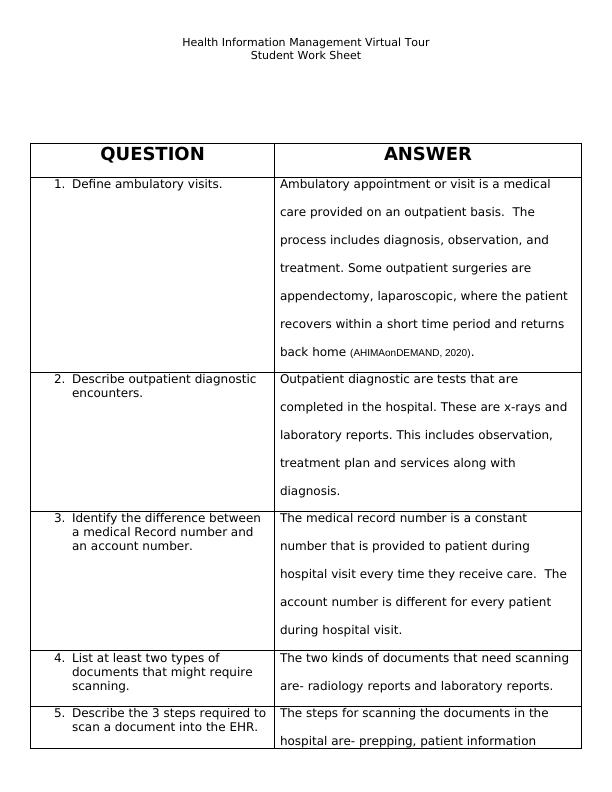
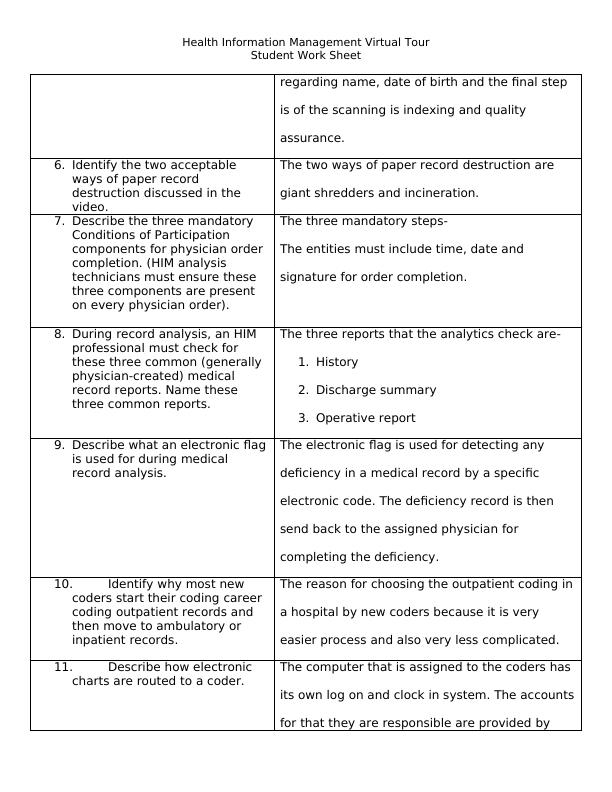
Take a virtual tour of a real HIM department at Sinclair Memorial Hospital in Ohio and answer questions about ambulatory visits, outpatient diagnostic encounters, medical record numbers, account numbers, scanning documents, paper record destruction, physician order completion, common medical record reports, electronic flags, coding career progression, electronic chart routing, and credentials required for coders.
Added on 2022-08-16
About This Document
Watch this video tour of an HIM department and complete the Virtual Tour Worksheet. See file for the Tour Worksheet
Health Information Management
Take a virtual tour of a real HIM department at Sinclair Memorial Hospital in Ohio and answer questions about ambulatory visits, outpatient diagnostic encounters, medical record numbers, account numbers, scanning documents, paper record destruction, physician order completion, common medical record reports, electronic flags, coding career progression, electronic chart routing, and credentials required for coders.
Added on 2022-08-16

End of preview
Want to access all the pages? Upload your documents or become a member.