Critical Analysis of Safety and Quality Issues in Healthcare
VerifiedAdded on 2023/06/11
|17
|4820
|345
AI Summary
This report presents a critical analysis of safety and quality issues in healthcare based on a given case scenario. It includes identification of issues, summary of literature, safety culture analysis, and actions to deal with the issues.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Assignment 2 1
Healthcare Assignment
Healthcare Assignment
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Assignment 2 2
Contents
Introduction.................................................................................................................................................3
Main Discussions........................................................................................................................................4
Task 1 identify the quality and safety issues raised.................................................................................4
Task 2 Summary of what is known about each issue type based on review of the quality and safety
literature..................................................................................................................................................5
Task 3 Analysis of the safety culture.......................................................................................................7
Task 4 Actions to deal with the issues identified from this scenario......................................................10
Task 5 Choose one of the medication management issues identified in the scenario and using the Plan-
Do-Check-Act cycle as your framework describe your plan for investigating the issue, identifying
potential solutions and testing these......................................................................................................12
Conclusion.................................................................................................................................................14
References.................................................................................................................................................15
Contents
Introduction.................................................................................................................................................3
Main Discussions........................................................................................................................................4
Task 1 identify the quality and safety issues raised.................................................................................4
Task 2 Summary of what is known about each issue type based on review of the quality and safety
literature..................................................................................................................................................5
Task 3 Analysis of the safety culture.......................................................................................................7
Task 4 Actions to deal with the issues identified from this scenario......................................................10
Task 5 Choose one of the medication management issues identified in the scenario and using the Plan-
Do-Check-Act cycle as your framework describe your plan for investigating the issue, identifying
potential solutions and testing these......................................................................................................12
Conclusion.................................................................................................................................................14
References.................................................................................................................................................15

Assignment 2 3
Introduction
The patient safety and quality are at the heart of the most of the hospitals, clinics, and nursing
care centers in the Australian Healthcare Systems because of increasing competitive of the
healthcare service providers and higher health safety and quality expectations from the patients.
This report presents the critical analysis of the safety and quality issues in the case of Dad cared
by his carer, Mum who supplies the lists of the medicines to the doctor of the emergency
department. The report will critically analyze the safety and quality issues in the patient’s care
and summary of the issues raisedalong with causes, incidence, factors, and actions. It will also
analyze the safety issues in the workplace culture of the hospital, actions to address the issues,
and PDCA cycle use to implement a suitable solution for managing the issue effectively and
efficiently(Department of Health, 2013). This overall analysis is based on the given case
scenario.
Introduction
The patient safety and quality are at the heart of the most of the hospitals, clinics, and nursing
care centers in the Australian Healthcare Systems because of increasing competitive of the
healthcare service providers and higher health safety and quality expectations from the patients.
This report presents the critical analysis of the safety and quality issues in the case of Dad cared
by his carer, Mum who supplies the lists of the medicines to the doctor of the emergency
department. The report will critically analyze the safety and quality issues in the patient’s care
and summary of the issues raisedalong with causes, incidence, factors, and actions. It will also
analyze the safety issues in the workplace culture of the hospital, actions to address the issues,
and PDCA cycle use to implement a suitable solution for managing the issue effectively and
efficiently(Department of Health, 2013). This overall analysis is based on the given case
scenario.
Assignment 2 4
Main Discussions
Task 1 identify the quality and safety issues raised
The quality and safety issues are related to the improvement of the patients’ security and quality
care practices by the service staffs after following the safety and health guidelines. The quality
and safety issues were raised because of the human errors by the service staffs working in the
hospital, like not attending the emergent patient (dad) for treating effectively as per the National
Hospital standards. Dad’s experiences (patient) regarding the hospital service quality could not
said be ‘satisfied’ because of the problems in the hospital staffs service delivery, hospital
culture, communicational problems, the lacks of the sufficient staffs, and missing the emergent
medicine by Mum. The quality and safety issues were raised due to the unrealistic service
expectations by the service staffs (Department of Health, 2013).
The main issues were related to the poor management of the service staffs to patient problems
and complaints. Some of the service staffs of the hospital not acted up to follow up the patient’s
complaints that were due to the senior hospital staffs delegated the complaints to others for
resolution with no ending outcomes. Some hospital staffs were aware and concerned about the
patient’s health problems, but they didn’t follow up the Dad’s family complaints because of
other casual and irresponsible service staffs. Some hospital staffs didn’t understand the
responsibility toward the patient by not following the standards of safety and quality of care.
These service staffs not acted on the patient’s actual complaints by stating that the Dad relates
to Frequent Flyer family with unrealistic service standard and unexpected outcomes (Parker,
2009). The staff kept its favor by stating that the patient’s service expectations are never-ending
or unsatisfactory because the dad always comes regularly to the hospital with his wife to
Main Discussions
Task 1 identify the quality and safety issues raised
The quality and safety issues are related to the improvement of the patients’ security and quality
care practices by the service staffs after following the safety and health guidelines. The quality
and safety issues were raised because of the human errors by the service staffs working in the
hospital, like not attending the emergent patient (dad) for treating effectively as per the National
Hospital standards. Dad’s experiences (patient) regarding the hospital service quality could not
said be ‘satisfied’ because of the problems in the hospital staffs service delivery, hospital
culture, communicational problems, the lacks of the sufficient staffs, and missing the emergent
medicine by Mum. The quality and safety issues were raised due to the unrealistic service
expectations by the service staffs (Department of Health, 2013).
The main issues were related to the poor management of the service staffs to patient problems
and complaints. Some of the service staffs of the hospital not acted up to follow up the patient’s
complaints that were due to the senior hospital staffs delegated the complaints to others for
resolution with no ending outcomes. Some hospital staffs were aware and concerned about the
patient’s health problems, but they didn’t follow up the Dad’s family complaints because of
other casual and irresponsible service staffs. Some hospital staffs didn’t understand the
responsibility toward the patient by not following the standards of safety and quality of care.
These service staffs not acted on the patient’s actual complaints by stating that the Dad relates
to Frequent Flyer family with unrealistic service standard and unexpected outcomes (Parker,
2009). The staff kept its favor by stating that the patient’s service expectations are never-ending
or unsatisfactory because the dad always comes regularly to the hospital with his wife to
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Assignment 2 5
diagnose and treat the health problems and raises questions on the service quality of the
hospital.
The senior management favored the staffs by reporting to CEO, Karol that the problems were
actually caused due to expectations of the high standards of care by Dad and his family
members. Along with this, Dad has the chronic illness and complex health problem that require
time to cure. Additionally, the problems with dad were occurred due to the staff lacking and
busy ward staff in Emergency department that were attending other patients. The staff said that
it is not possible for them to attend Dad all the time by not following other patients. The lack of
staffing and high workload also enforced the staff for not attending Dad properly. Dad’s family
is not agreed to understand the current staffing problems and extra work pressure on the
employed staffs(Ashcroft, Morecroft, Parker, &Noyce, 2005).The regular ward staff and
emergency staffs were not fully aware of the health problemsof Dad despite knowing his health
complexities as his wife was keenly involved in her husband’s care. The changing medication
pattern prescribed by the doctor and not proper medications by Mum every time is also another
reason for the complex health problems to Dad’s health. Along with his, Carol found herself
frustrated and irritable because of disinterested responses from the hospital staffs.
Task 2 Summary of what is known about each issue type based on review of the quality and
safety literature
The safety culture and leadership development issue is related to providing the safety and
standardized health care to the patients through the supportive workforce culture. The current
organizational culture or workplace conditions in the hospital are not good because of the not
sufficient service staffs, low staffs’ commitment and low morale, less productive staffs, and the
lack of teamwork and shared care service practices for providing better treatment to the
diagnose and treat the health problems and raises questions on the service quality of the
hospital.
The senior management favored the staffs by reporting to CEO, Karol that the problems were
actually caused due to expectations of the high standards of care by Dad and his family
members. Along with this, Dad has the chronic illness and complex health problem that require
time to cure. Additionally, the problems with dad were occurred due to the staff lacking and
busy ward staff in Emergency department that were attending other patients. The staff said that
it is not possible for them to attend Dad all the time by not following other patients. The lack of
staffing and high workload also enforced the staff for not attending Dad properly. Dad’s family
is not agreed to understand the current staffing problems and extra work pressure on the
employed staffs(Ashcroft, Morecroft, Parker, &Noyce, 2005).The regular ward staff and
emergency staffs were not fully aware of the health problemsof Dad despite knowing his health
complexities as his wife was keenly involved in her husband’s care. The changing medication
pattern prescribed by the doctor and not proper medications by Mum every time is also another
reason for the complex health problems to Dad’s health. Along with his, Carol found herself
frustrated and irritable because of disinterested responses from the hospital staffs.
Task 2 Summary of what is known about each issue type based on review of the quality and
safety literature
The safety culture and leadership development issue is related to providing the safety and
standardized health care to the patients through the supportive workforce culture. The current
organizational culture or workplace conditions in the hospital are not good because of the not
sufficient service staffs, low staffs’ commitment and low morale, less productive staffs, and the
lack of teamwork and shared care service practices for providing better treatment to the
Assignment 2 6
patient(Waterson, Griffiths, Stride, Murphy, &Hignett, 2010). The lack of adequate training, the
lack of coordination, trust, and teamwork, the low staff’s commitment, poor or ineffective
management support, and the lack of the disciplined activities contribute to occurrence for the
workplace culture problems in the Hospital. To deal with this problem, the senior management
should reinforce a supportive and learning culture that encourages the doctors, supervisors, and
nursing staffs to work interactively by informing each other about the patients’ health
complexities, medications, and treatment required.
The Medication chart prescribed by the doctors could be followed by the service staffs, like
Mum to ensure the ethical working practices in order to give the right kind of medicinesby
looking the Wristband for the scheduled treatment and care practices to the patient (Singla,
Kitch, Weissman, & Campbell, 2006). The hospital is required to ensure an improved
information infrastructure by using the information and communication technologies for
ensuring the high communication level, scheduled training and learning programs for educating
the staffs, and effective workforce planning to measure the proper staffing requirements to
employ in the hospital for meeting all patients’ needs.
The rigid complaint settlement procedure is another issue that is caused from the casual staffs not
following the complaints of Dad’s family members because the working staffs not accepting
their own fault, the working staff find Dad and his family member blame for this and stand
responsible for their critical health problems. This was contributed by the busier and low morale
staffs who were troubled with the staffing problems. It was not possible for the staffs to meet the
care standards of Dad and his family because of higher expectations from them that couldn’t be
met with the current staffing and service facilities. The busier staff in Emergency department
didn’t understand their primary responsibility toward Dad’s critical illness and serious health
patient(Waterson, Griffiths, Stride, Murphy, &Hignett, 2010). The lack of adequate training, the
lack of coordination, trust, and teamwork, the low staff’s commitment, poor or ineffective
management support, and the lack of the disciplined activities contribute to occurrence for the
workplace culture problems in the Hospital. To deal with this problem, the senior management
should reinforce a supportive and learning culture that encourages the doctors, supervisors, and
nursing staffs to work interactively by informing each other about the patients’ health
complexities, medications, and treatment required.
The Medication chart prescribed by the doctors could be followed by the service staffs, like
Mum to ensure the ethical working practices in order to give the right kind of medicinesby
looking the Wristband for the scheduled treatment and care practices to the patient (Singla,
Kitch, Weissman, & Campbell, 2006). The hospital is required to ensure an improved
information infrastructure by using the information and communication technologies for
ensuring the high communication level, scheduled training and learning programs for educating
the staffs, and effective workforce planning to measure the proper staffing requirements to
employ in the hospital for meeting all patients’ needs.
The rigid complaint settlement procedure is another issue that is caused from the casual staffs not
following the complaints of Dad’s family members because the working staffs not accepting
their own fault, the working staff find Dad and his family member blame for this and stand
responsible for their critical health problems. This was contributed by the busier and low morale
staffs who were troubled with the staffing problems. It was not possible for the staffs to meet the
care standards of Dad and his family because of higher expectations from them that couldn’t be
met with the current staffing and service facilities. The busier staff in Emergency department
didn’t understand their primary responsibility toward Dad’s critical illness and serious health
Assignment 2 7
concerns and spent time in attending other patients. Some service staffs of them stated the
medication change is responsible for his daily health problems because his carer, Mum always
likely to change the medicines (Reader, Gillespie, & Roberts, 2013). Mum was also found faulty
for missing some medicines, prescribed by the doctor because she didn’t look at the medication
chart. Sometimes, Mum was found faulty for writing down the medicines at the end of list that
could not be read or seen by medicines department or chemists. Due to missing of medicines and
improper schedules for medicines, caused only because of the human errors by the service staffs,
as a result Dad had to suffer from the health complexities and had to come to the hospital on
daily basis.
To avoid this issue or finding solution to this issue, there should be a controlled disciplined
procedure to take action against such irresponsible or casual staffs, like Mum who didn’t
understand her responsibility toward the safety treatment and emergency careof Dad. The senior
management can suspend such type of staff or terminate for the temporary unemployment. This
disciplined action could change in the behaviors, practices, and service quality of the staffs
(Schnitzer, Kuhlmey, & Adolph, 2012). Along with this, a medication chart is needed to provide
and instruct the nursing staffs to follow the medicine chart while giving medicines to the patients
as per their scheduled prescriptions in the chart. There should be an effective reporting system
for following the customers’ complaints and investigate into the matter for finding the root cause
and immediately take an appropriate action so that the number of complaints could be
minimized.
Task 3 Analysis of the safety culture
The assessment of the safety culture is an increasing interest among the healthcare organizations
for managing the risks effectively. Manchester Patient Safety Framework (MaPSaF) is associated
concerns and spent time in attending other patients. Some service staffs of them stated the
medication change is responsible for his daily health problems because his carer, Mum always
likely to change the medicines (Reader, Gillespie, & Roberts, 2013). Mum was also found faulty
for missing some medicines, prescribed by the doctor because she didn’t look at the medication
chart. Sometimes, Mum was found faulty for writing down the medicines at the end of list that
could not be read or seen by medicines department or chemists. Due to missing of medicines and
improper schedules for medicines, caused only because of the human errors by the service staffs,
as a result Dad had to suffer from the health complexities and had to come to the hospital on
daily basis.
To avoid this issue or finding solution to this issue, there should be a controlled disciplined
procedure to take action against such irresponsible or casual staffs, like Mum who didn’t
understand her responsibility toward the safety treatment and emergency careof Dad. The senior
management can suspend such type of staff or terminate for the temporary unemployment. This
disciplined action could change in the behaviors, practices, and service quality of the staffs
(Schnitzer, Kuhlmey, & Adolph, 2012). Along with this, a medication chart is needed to provide
and instruct the nursing staffs to follow the medicine chart while giving medicines to the patients
as per their scheduled prescriptions in the chart. There should be an effective reporting system
for following the customers’ complaints and investigate into the matter for finding the root cause
and immediately take an appropriate action so that the number of complaints could be
minimized.
Task 3 Analysis of the safety culture
The assessment of the safety culture is an increasing interest among the healthcare organizations
for managing the risks effectively. Manchester Patient Safety Framework (MaPSaF) is associated
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Assignment 2 8
with the safety culture for allowing the safe and healthy workplace practices in the hospital to
treat the patients efficiently by ensuring their quality care and safety. The organizational working
culture in the hospital could not be said safe and standardized because of the lack of proper staffs
for attending the patients effectively. Different staffs have different views, opinions, and thinking
about the patient’s safety. Some staffs among them feel high workloads due to attending of a
large number of patients. Along with this, in the hospital, the working staffs are busier because
of lacking proper staffs in handling the patient(Lawton, R., McEachan, R.R., & Giles S.J, 2012).
MaPSaf is related to access and strengthen the safety culture through the standardized care
practices in the hospital.
The different dimensions of this framework could be applied to the case scenario for ensuring the
safety and quality working practices in the organization. The nine dimensions include Overall
commitment to safety through the continuous improvement, Priority to the patient safety, System
errors and Individual responsibility, Recording and evaluating the Patients’ safety incidents and
the best practices, learning and effective change to the organization, Communication about the
safety management, Proper management and safety issues, Staff education and training, and
Team working. The lack of the staff management, ineffective leadership, and low morale and
low staff engagement in the patient safety are main causes for the patient safety problems in the
hospital. According to MaPSaF, there are five levels of cultures in the healthcare organizations
including pathological, reactive, bureaucratic, proactive, and generative. The hospital should
have a reactive culture that will include always taking the patients’ safety seriously with the
appropriate response and do something or taking suitable action when we have an
incident(Pham, Aswani, & Rosen, 2012). According to this, the patient’s safety should be given
high priority by taking an immediate action rather than waiting for other staffs or delaying the
with the safety culture for allowing the safe and healthy workplace practices in the hospital to
treat the patients efficiently by ensuring their quality care and safety. The organizational working
culture in the hospital could not be said safe and standardized because of the lack of proper staffs
for attending the patients effectively. Different staffs have different views, opinions, and thinking
about the patient’s safety. Some staffs among them feel high workloads due to attending of a
large number of patients. Along with this, in the hospital, the working staffs are busier because
of lacking proper staffs in handling the patient(Lawton, R., McEachan, R.R., & Giles S.J, 2012).
MaPSaf is related to access and strengthen the safety culture through the standardized care
practices in the hospital.
The different dimensions of this framework could be applied to the case scenario for ensuring the
safety and quality working practices in the organization. The nine dimensions include Overall
commitment to safety through the continuous improvement, Priority to the patient safety, System
errors and Individual responsibility, Recording and evaluating the Patients’ safety incidents and
the best practices, learning and effective change to the organization, Communication about the
safety management, Proper management and safety issues, Staff education and training, and
Team working. The lack of the staff management, ineffective leadership, and low morale and
low staff engagement in the patient safety are main causes for the patient safety problems in the
hospital. According to MaPSaF, there are five levels of cultures in the healthcare organizations
including pathological, reactive, bureaucratic, proactive, and generative. The hospital should
have a reactive culture that will include always taking the patients’ safety seriously with the
appropriate response and do something or taking suitable action when we have an
incident(Pham, Aswani, & Rosen, 2012). According to this, the patient’s safety should be given
high priority by taking an immediate action rather than waiting for other staffs or delaying the
Assignment 2 9
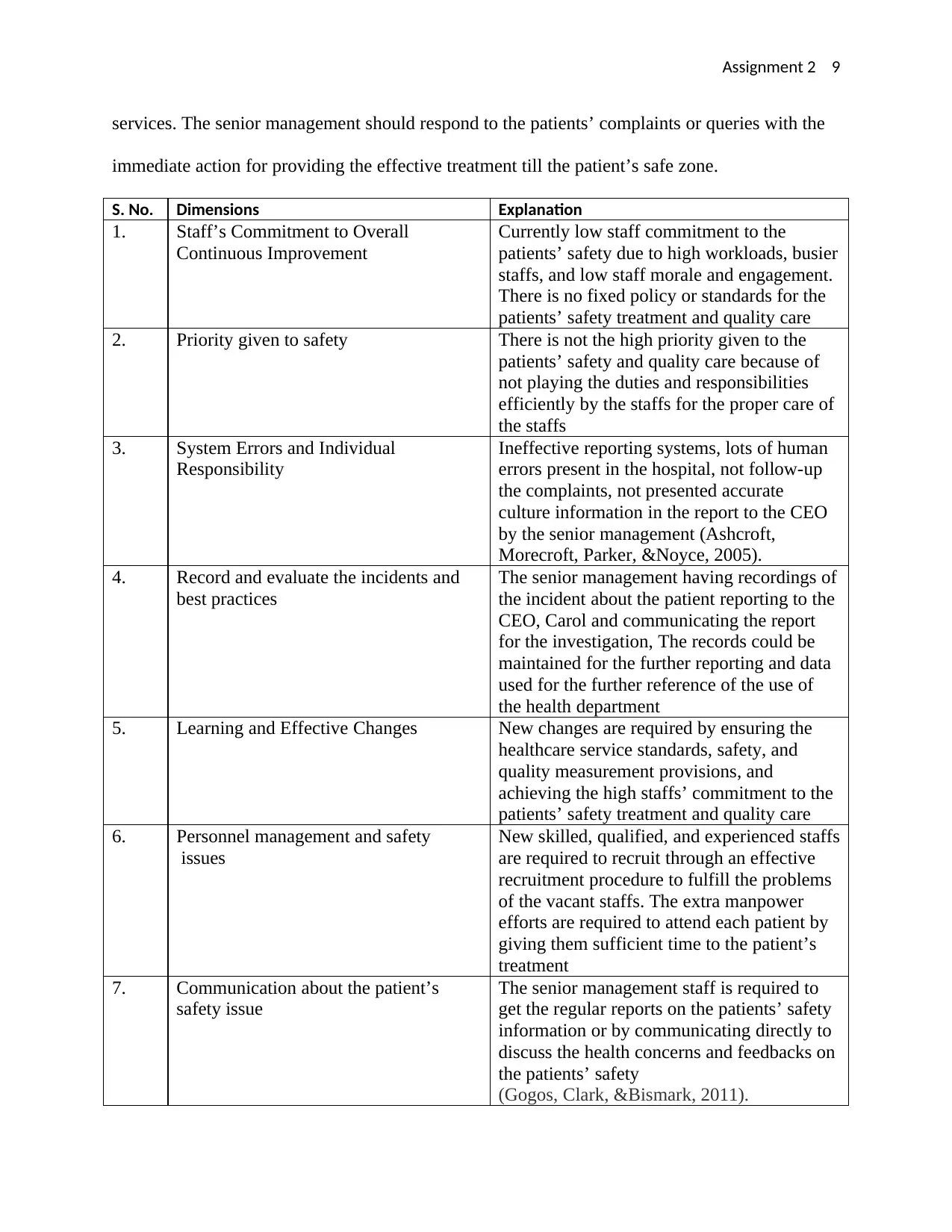
services. The senior management should respond to the patients’ complaints or queries with the
immediate action for providing the effective treatment till the patient’s safe zone.
S. No. Dimensions Explanation
1. Staff’s Commitment to Overall
Continuous Improvement
Currently low staff commitment to the
patients’ safety due to high workloads, busier
staffs, and low staff morale and engagement.
There is no fixed policy or standards for the
patients’ safety treatment and quality care
2. Priority given to safety There is not the high priority given to the
patients’ safety and quality care because of
not playing the duties and responsibilities
efficiently by the staffs for the proper care of
the staffs
3. System Errors and Individual
Responsibility
Ineffective reporting systems, lots of human
errors present in the hospital, not follow-up
the complaints, not presented accurate
culture information in the report to the CEO
by the senior management (Ashcroft,
Morecroft, Parker, &Noyce, 2005).
4. Record and evaluate the incidents and
best practices
The senior management having recordings of
the incident about the patient reporting to the
CEO, Carol and communicating the report
for the investigation, The records could be
maintained for the further reporting and data
used for the further reference of the use of
the health department
5. Learning and Effective Changes New changes are required by ensuring the
healthcare service standards, safety, and
quality measurement provisions, and
achieving the high staffs’ commitment to the
patients’ safety treatment and quality care
6. Personnel management and safety
issues
New skilled, qualified, and experienced staffs
are required to recruit through an effective
recruitment procedure to fulfill the problems
of the vacant staffs. The extra manpower
efforts are required to attend each patient by
giving them sufficient time to the patient’s
treatment
7. Communication about the patient’s
safety issue
The senior management staff is required to
get the regular reports on the patients’ safety
information or by communicating directly to
discuss the health concerns and feedbacks on
the patients’ safety
(Gogos, Clark, &Bismark, 2011).
services. The senior management should respond to the patients’ complaints or queries with the
immediate action for providing the effective treatment till the patient’s safe zone.
S. No. Dimensions Explanation
1. Staff’s Commitment to Overall
Continuous Improvement
Currently low staff commitment to the
patients’ safety due to high workloads, busier
staffs, and low staff morale and engagement.
There is no fixed policy or standards for the
patients’ safety treatment and quality care
2. Priority given to safety There is not the high priority given to the
patients’ safety and quality care because of
not playing the duties and responsibilities
efficiently by the staffs for the proper care of
the staffs
3. System Errors and Individual
Responsibility
Ineffective reporting systems, lots of human
errors present in the hospital, not follow-up
the complaints, not presented accurate
culture information in the report to the CEO
by the senior management (Ashcroft,
Morecroft, Parker, &Noyce, 2005).
4. Record and evaluate the incidents and
best practices
The senior management having recordings of
the incident about the patient reporting to the
CEO, Carol and communicating the report
for the investigation, The records could be
maintained for the further reporting and data
used for the further reference of the use of
the health department
5. Learning and Effective Changes New changes are required by ensuring the
healthcare service standards, safety, and
quality measurement provisions, and
achieving the high staffs’ commitment to the
patients’ safety treatment and quality care
6. Personnel management and safety
issues
New skilled, qualified, and experienced staffs
are required to recruit through an effective
recruitment procedure to fulfill the problems
of the vacant staffs. The extra manpower
efforts are required to attend each patient by
giving them sufficient time to the patient’s
treatment
7. Communication about the patient’s
safety issue
The senior management staff is required to
get the regular reports on the patients’ safety
information or by communicating directly to
discuss the health concerns and feedbacks on
the patients’ safety
(Gogos, Clark, &Bismark, 2011).
Assignment 2 10
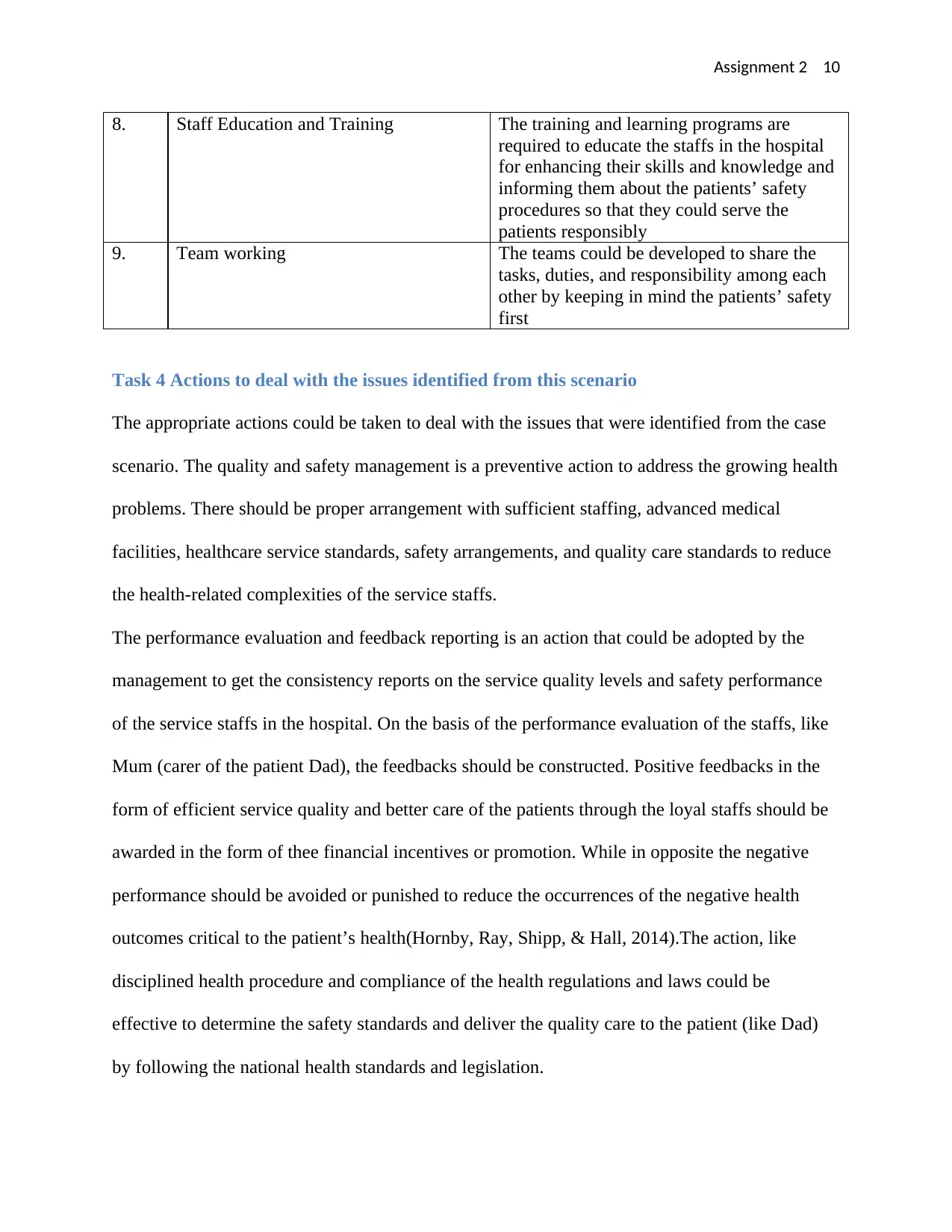
8. Staff Education and Training The training and learning programs are
required to educate the staffs in the hospital
for enhancing their skills and knowledge and
informing them about the patients’ safety
procedures so that they could serve the
patients responsibly
9. Team working The teams could be developed to share the
tasks, duties, and responsibility among each
other by keeping in mind the patients’ safety
first
Task 4 Actions to deal with the issues identified from this scenario
The appropriate actions could be taken to deal with the issues that were identified from the case
scenario. The quality and safety management is a preventive action to address the growing health
problems. There should be proper arrangement with sufficient staffing, advanced medical
facilities, healthcare service standards, safety arrangements, and quality care standards to reduce
the health-related complexities of the service staffs.
The performance evaluation and feedback reporting is an action that could be adopted by the
management to get the consistency reports on the service quality levels and safety performance
of the service staffs in the hospital. On the basis of the performance evaluation of the staffs, like
Mum (carer of the patient Dad), the feedbacks should be constructed. Positive feedbacks in the
form of efficient service quality and better care of the patients through the loyal staffs should be
awarded in the form of thee financial incentives or promotion. While in opposite the negative
performance should be avoided or punished to reduce the occurrences of the negative health
outcomes critical to the patient’s health(Hornby, Ray, Shipp, & Hall, 2014).The action, like
disciplined health procedure and compliance of the health regulations and laws could be
effective to determine the safety standards and deliver the quality care to the patient (like Dad)
by following the national health standards and legislation.
8. Staff Education and Training The training and learning programs are
required to educate the staffs in the hospital
for enhancing their skills and knowledge and
informing them about the patients’ safety
procedures so that they could serve the
patients responsibly
9. Team working The teams could be developed to share the
tasks, duties, and responsibility among each
other by keeping in mind the patients’ safety
first
Task 4 Actions to deal with the issues identified from this scenario
The appropriate actions could be taken to deal with the issues that were identified from the case
scenario. The quality and safety management is a preventive action to address the growing health
problems. There should be proper arrangement with sufficient staffing, advanced medical
facilities, healthcare service standards, safety arrangements, and quality care standards to reduce
the health-related complexities of the service staffs.
The performance evaluation and feedback reporting is an action that could be adopted by the
management to get the consistency reports on the service quality levels and safety performance
of the service staffs in the hospital. On the basis of the performance evaluation of the staffs, like
Mum (carer of the patient Dad), the feedbacks should be constructed. Positive feedbacks in the
form of efficient service quality and better care of the patients through the loyal staffs should be
awarded in the form of thee financial incentives or promotion. While in opposite the negative
performance should be avoided or punished to reduce the occurrences of the negative health
outcomes critical to the patient’s health(Hornby, Ray, Shipp, & Hall, 2014).The action, like
disciplined health procedure and compliance of the health regulations and laws could be
effective to determine the safety standards and deliver the quality care to the patient (like Dad)
by following the national health standards and legislation.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Assignment 2 11
There should be an effective complaint settlement procedure to hear the patients’ complaints by
following them and listening their concerns or issues attentively. After this, the senior healthcare
manager is required to investigate into the matter by employing a supervisory panel to
investigate the matter and after this, an appropriate decision will be taken based on prioritizing
the patient’s health and safety. The blamed service staffs will be terminated or deducted some
payment in his/her monthly salary account. A safety culture will be developed that will foster the
teamwork, group performance, shared tasks, informed decisions, and added responsibilities that
will be effective to attend the serious patients by another staff in the absence of the relevant staff
members in this employment team.This culture will promote the health and safety practices
greatly by determining the safety measurements and treatment standards for the patients in the
hospital(Kirk, Parker, Claridge, Esmail, & Marshall, 2007). Additionally, new service staffs with
skills and adequate competences will be hired through the effective recruitment and selection
procedures to recruit the talent, experienced, and high performing doctors and nursing staffs who
understand the patients’ critical healthcare issues and accordingly to provide the emergency
treatment as per the current patients’ conditions and service needs.
The standard clinical practices by using the professional ethical code of conduct and CSR
reporting could be considered for maintaining the accountability, transparency, and materiality of
the hospital care services through the right kind of information and regular reporting from the
nursing staffs to the senior management and from where it should be reefed to the CEO for the
final review. The CSR and ethical practices will assist in the better treatment and individualized
care of the patients. The care staffs found in any corrupted activities will be withdrawn from the
immediate effect through the suspension order from the CEO without giving notice to such
employees(Law, Zimmerman, Baker, & Smith, 2010). The Medication management is an action
There should be an effective complaint settlement procedure to hear the patients’ complaints by
following them and listening their concerns or issues attentively. After this, the senior healthcare
manager is required to investigate into the matter by employing a supervisory panel to
investigate the matter and after this, an appropriate decision will be taken based on prioritizing
the patient’s health and safety. The blamed service staffs will be terminated or deducted some
payment in his/her monthly salary account. A safety culture will be developed that will foster the
teamwork, group performance, shared tasks, informed decisions, and added responsibilities that
will be effective to attend the serious patients by another staff in the absence of the relevant staff
members in this employment team.This culture will promote the health and safety practices
greatly by determining the safety measurements and treatment standards for the patients in the
hospital(Kirk, Parker, Claridge, Esmail, & Marshall, 2007). Additionally, new service staffs with
skills and adequate competences will be hired through the effective recruitment and selection
procedures to recruit the talent, experienced, and high performing doctors and nursing staffs who
understand the patients’ critical healthcare issues and accordingly to provide the emergency
treatment as per the current patients’ conditions and service needs.
The standard clinical practices by using the professional ethical code of conduct and CSR
reporting could be considered for maintaining the accountability, transparency, and materiality of
the hospital care services through the right kind of information and regular reporting from the
nursing staffs to the senior management and from where it should be reefed to the CEO for the
final review. The CSR and ethical practices will assist in the better treatment and individualized
care of the patients. The care staffs found in any corrupted activities will be withdrawn from the
immediate effect through the suspension order from the CEO without giving notice to such
employees(Law, Zimmerman, Baker, & Smith, 2010). The Medication management is an action
Assignment 2 12
to ensure the right kind of medicines prescribed by the doctors by following the Medication
Chart to attend the patient, like Dad and give the right kind of medicines for the scheduled
treatment and quality care of the patient.
Task 5 Choose one of the medication management issues identified in the scenario and
using the Plan-Do-Check-Act cycle as your framework describe your plan for investigating
the issue, identifying potential solutions and testing these
Medication management is an important part of the healthcare service policy that includes use of
the right kind of medicines as per medication chart and schedules in the most of the hospitals in
the Australian healthcare industry. The case scenario involved different medication management
issues including the improper medication schedule, missing medicines in the list for the medicine
department, not added other or new medicine as per the schedule change for treating other
problem, and writing down the medicines at bottom in the list by Mum that is not seen by the
medicine department or drug store. The missing of the medicines is a medication management
issue that is identified as an important intervention, caused from higher incident of human errors
(mistakes of staff, Mum) and creates the health problems for Dad. PDCA cycle is used to deal
with this intervention or issue that involves four steps- planning, doing, acting, and checking for
developing an effective plan to investigate the root cause of the medication issue and potential
solutions to deal with the issue (New South Wales Government, 2015).
The planning for this will include the preparation of the medical chart for specifying the
particular medicines to a particular patient. It will also include the workforce planning, like
employing a Medical safety and Quality Unit (MSQU),pharmacy barcode scanning, user-applied
labeling, and the National Impatient Medication Chart. The doing phase will include working on
the medication chart, specifying and providing the specific medicine matching the wristband of
to ensure the right kind of medicines prescribed by the doctors by following the Medication
Chart to attend the patient, like Dad and give the right kind of medicines for the scheduled
treatment and quality care of the patient.
Task 5 Choose one of the medication management issues identified in the scenario and
using the Plan-Do-Check-Act cycle as your framework describe your plan for investigating
the issue, identifying potential solutions and testing these
Medication management is an important part of the healthcare service policy that includes use of
the right kind of medicines as per medication chart and schedules in the most of the hospitals in
the Australian healthcare industry. The case scenario involved different medication management
issues including the improper medication schedule, missing medicines in the list for the medicine
department, not added other or new medicine as per the schedule change for treating other
problem, and writing down the medicines at bottom in the list by Mum that is not seen by the
medicine department or drug store. The missing of the medicines is a medication management
issue that is identified as an important intervention, caused from higher incident of human errors
(mistakes of staff, Mum) and creates the health problems for Dad. PDCA cycle is used to deal
with this intervention or issue that involves four steps- planning, doing, acting, and checking for
developing an effective plan to investigate the root cause of the medication issue and potential
solutions to deal with the issue (New South Wales Government, 2015).
The planning for this will include the preparation of the medical chart for specifying the
particular medicines to a particular patient. It will also include the workforce planning, like
employing a Medical safety and Quality Unit (MSQU),pharmacy barcode scanning, user-applied
labeling, and the National Impatient Medication Chart. The doing phase will include working on
the medication chart, specifying and providing the specific medicine matching the wristband of
Assignment 2 13
the patient, scanning of the bar code on the medicines before giving the patients, hiring of the
high-risk machines and employment of the competent staff who understand the patients’
medicines properly(Reader, Gillespie, &Mannell, 2014).The checking phase will include
revising the medicines of the suffered patient with the hospital medication chart and matching
the medicine schedules of the patient (Dad) with the chart. It will also include checking of the
barcode on the medicines, linking the requirements for the user-applied labeling, and checking of
the high-risks or emergent medicines by MSQU department.
The final step, acting phase will include providing drugs to the patient by checking his wrist
band, looking attentively at the medication chart and giving each dose of medicine as per
schedule prescribed by the doctor. It will also include the medication safety self-assessmentthat
is related to the development of processes and tools designed to facilitate the effective
monitoring and evaluation of the medication management that will highlight the opportunities to
bring further improvement in the missing of the medicines.The VTE prevention programs will
assist the clinical teams and healthcare service facilities to implement the robust programs and
processes for the prevention of the wrong medicines or missing medicines(Runciman, Hibbert, &
Thomson, 2009). The application of PDCA Cycle will bring major improvement in practicing
safer medication management for giving right drugs including the emergent and high-risk
medicines to the patient, Dad for the quick treatment of the current or emergent health problem.
the patient, scanning of the bar code on the medicines before giving the patients, hiring of the
high-risk machines and employment of the competent staff who understand the patients’
medicines properly(Reader, Gillespie, &Mannell, 2014).The checking phase will include
revising the medicines of the suffered patient with the hospital medication chart and matching
the medicine schedules of the patient (Dad) with the chart. It will also include checking of the
barcode on the medicines, linking the requirements for the user-applied labeling, and checking of
the high-risks or emergent medicines by MSQU department.
The final step, acting phase will include providing drugs to the patient by checking his wrist
band, looking attentively at the medication chart and giving each dose of medicine as per
schedule prescribed by the doctor. It will also include the medication safety self-assessmentthat
is related to the development of processes and tools designed to facilitate the effective
monitoring and evaluation of the medication management that will highlight the opportunities to
bring further improvement in the missing of the medicines.The VTE prevention programs will
assist the clinical teams and healthcare service facilities to implement the robust programs and
processes for the prevention of the wrong medicines or missing medicines(Runciman, Hibbert, &
Thomson, 2009). The application of PDCA Cycle will bring major improvement in practicing
safer medication management for giving right drugs including the emergent and high-risk
medicines to the patient, Dad for the quick treatment of the current or emergent health problem.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Assignment 2 14
Conclusion
The PDCA cycle is used to deliver an effective solution to the medication intervention in the
form of missing medication issue through different stages (plan, do, check, and act). This process
provided a platform to bring improvement in the medication management for supplying the right
medicines to the patient. The safety and quality issues, like staffing management problems,
ineffective complaint redressal procedure, rigid information flow and inefficient reporting
system, and errors in the medication by the service staffs were also discussed along with the
contributory factors, effects, causes, action plans, and incidents for the issues. The cultural safety
issues were caused due to the leadership development issues, the lack of the learning culture,
ineffective information system management infrastructure, communicational problems, staffing
management issues, and the lack of scheduled reporting and performance evaluation system.
Finally, the action plans for addressing the workplace culture concerns were suggested in order
to provide the right kind of treatment with the quality care by ensuring the safety of the patient
from the high-risk zone.
Conclusion
The PDCA cycle is used to deliver an effective solution to the medication intervention in the
form of missing medication issue through different stages (plan, do, check, and act). This process
provided a platform to bring improvement in the medication management for supplying the right
medicines to the patient. The safety and quality issues, like staffing management problems,
ineffective complaint redressal procedure, rigid information flow and inefficient reporting
system, and errors in the medication by the service staffs were also discussed along with the
contributory factors, effects, causes, action plans, and incidents for the issues. The cultural safety
issues were caused due to the leadership development issues, the lack of the learning culture,
ineffective information system management infrastructure, communicational problems, staffing
management issues, and the lack of scheduled reporting and performance evaluation system.
Finally, the action plans for addressing the workplace culture concerns were suggested in order
to provide the right kind of treatment with the quality care by ensuring the safety of the patient
from the high-risk zone.
Assignment 2 15
References
Ashcroft, D.M., Morecroft, C., Parker, D., &Noyce, P.R. (2005). ‘Safety culture assessment in
community pharmacy: development, face validity, and feasibility of the Manchester
Patient Safety Assessment Framework’, Quality and Safety in Health Care, Vol. 14(6),
pp. 417-421.
Department of Health (2013).Delivering high quality, effective, compassionate care: Developing
the right people with the right skills and the right values. Mandate from Government to
HEE: Retrieved From:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/
203332/29257_29 00971_Delivering_Accessible.pdf.
Flin, R., Burns, C., Mearns, K., Yule, S., & Robertson, E.M. (2006).‘Measuring safety climate in
healthcare’, Quality and Safety in Health Care, Vol. 15(2), pp. 109-115.
Gogos, A.J., Clark, R.B., &Bismark, M.M., (2011). ‘When informed consent goes poorly: a
descriptive study of medical negligence claims and patient complaints’, Journal of
Medicine Science, Vol. 195, pp.340–344.
Hornby P., Ray D.K., Shipp P.J., & Hall, T.L. (2014).Guidelines for Health Manpower
Planning: A course book. Retrieved
From: www.whqlibdoc.who.int/publications/9241541563_%28p1-p188%29.pdf.
Källberg, A.S., Göransson, K.E., &Östergren, J., (2013). ‘Medical errors and complaints in
emergency department care in Sweden as reported by care providers, healthcare staff, and
patients–a national review’, European Journal of Emergency Medicine, Vol. 20, pp. 33-
38.
References
Ashcroft, D.M., Morecroft, C., Parker, D., &Noyce, P.R. (2005). ‘Safety culture assessment in
community pharmacy: development, face validity, and feasibility of the Manchester
Patient Safety Assessment Framework’, Quality and Safety in Health Care, Vol. 14(6),
pp. 417-421.
Department of Health (2013).Delivering high quality, effective, compassionate care: Developing
the right people with the right skills and the right values. Mandate from Government to
HEE: Retrieved From:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/
203332/29257_29 00971_Delivering_Accessible.pdf.
Flin, R., Burns, C., Mearns, K., Yule, S., & Robertson, E.M. (2006).‘Measuring safety climate in
healthcare’, Quality and Safety in Health Care, Vol. 15(2), pp. 109-115.
Gogos, A.J., Clark, R.B., &Bismark, M.M., (2011). ‘When informed consent goes poorly: a
descriptive study of medical negligence claims and patient complaints’, Journal of
Medicine Science, Vol. 195, pp.340–344.
Hornby P., Ray D.K., Shipp P.J., & Hall, T.L. (2014).Guidelines for Health Manpower
Planning: A course book. Retrieved
From: www.whqlibdoc.who.int/publications/9241541563_%28p1-p188%29.pdf.
Källberg, A.S., Göransson, K.E., &Östergren, J., (2013). ‘Medical errors and complaints in
emergency department care in Sweden as reported by care providers, healthcare staff, and
patients–a national review’, European Journal of Emergency Medicine, Vol. 20, pp. 33-
38.
Assignment 2 16
Kirk, S., Parker, D., Claridge, T., Esmail, A., & Marshall, M. (2007). ‘Patient safety culture in
primary care: developing a theoretical framework for practical use’, Quality and Safety in
Healthcare, Vol. 16(4), pp. 313-320.
Law, P.M., Zimmerman, R., Baker, R.G., & Smith, T. (2010).‘Assessment of Safety Culture
Maturity in a Hospital Setting’, Healthcare Quarterly, Vol. 13, pp. 110-115.
Lawton, R., McEachan, R.R., & Giles S.J. (2012).‘Development of an evidence-based
framework of factors contributing to patient safety incidents in hospital settings: a
systematic review’, Biomedical Journal of Quality and Safety in Healthcare, Vol. 21,
pp.369–380.
New South Wales Government (2015).Medication Quality and Safety.Retrieved
From:http://www.cec.health.nsw.gov.au/patient-safety-programs/medication-safety/
medication-safety-and-quality.
Parker, D. (2009). ‘Managing risk in healthcare: understanding your safety culture using the
Manchester Patient Safety Framework (MaPSaF)’, Journal of Nursing Management, Vol.
17(2), pp.2018-2022.
Pham, J.C., Aswani, M.S., & Rosen, M. (2012). ‘Reducing medical errors and adverse events’,
Annual Review in Medicine Science, Vol. 63, pp. 447–463.
Reader, W.T., Gillespie, A., &Roberts, J. (2013).Patient Complaints in Healthcare Systems: A
Systematic Review and Coding Taxonomy. Retrieved From:
http://qualitysafety.bmj.com/content/early/2014/05/29/bmjqs-2013-002437.
Reader, T., Gillespie, A., &Mannell, J. (2014).‘Patient neglect in the 21st century healthcare
institutions: a community health psychology perspective’, Journal of Health Psychology,
Vol. 19, pp.137–148.
Kirk, S., Parker, D., Claridge, T., Esmail, A., & Marshall, M. (2007). ‘Patient safety culture in
primary care: developing a theoretical framework for practical use’, Quality and Safety in
Healthcare, Vol. 16(4), pp. 313-320.
Law, P.M., Zimmerman, R., Baker, R.G., & Smith, T. (2010).‘Assessment of Safety Culture
Maturity in a Hospital Setting’, Healthcare Quarterly, Vol. 13, pp. 110-115.
Lawton, R., McEachan, R.R., & Giles S.J. (2012).‘Development of an evidence-based
framework of factors contributing to patient safety incidents in hospital settings: a
systematic review’, Biomedical Journal of Quality and Safety in Healthcare, Vol. 21,
pp.369–380.
New South Wales Government (2015).Medication Quality and Safety.Retrieved
From:http://www.cec.health.nsw.gov.au/patient-safety-programs/medication-safety/
medication-safety-and-quality.
Parker, D. (2009). ‘Managing risk in healthcare: understanding your safety culture using the
Manchester Patient Safety Framework (MaPSaF)’, Journal of Nursing Management, Vol.
17(2), pp.2018-2022.
Pham, J.C., Aswani, M.S., & Rosen, M. (2012). ‘Reducing medical errors and adverse events’,
Annual Review in Medicine Science, Vol. 63, pp. 447–463.
Reader, W.T., Gillespie, A., &Roberts, J. (2013).Patient Complaints in Healthcare Systems: A
Systematic Review and Coding Taxonomy. Retrieved From:
http://qualitysafety.bmj.com/content/early/2014/05/29/bmjqs-2013-002437.
Reader, T., Gillespie, A., &Mannell, J. (2014).‘Patient neglect in the 21st century healthcare
institutions: a community health psychology perspective’, Journal of Health Psychology,
Vol. 19, pp.137–148.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Assignment 2 17
Runciman, W., Hibbert, P., & Thomson, R.(2009). ‘Towards an international classification for
patient safety: key concepts and terms’, International Journal of Quality in Health Care,
Vol. 21, pp.18–26.
Schnitzer, S., Kuhlmey, A., & Adolph, H., (2012). ‘Complaints as indicators of health care
shortcomings: which groups of patients are affected?’ International Journal of Quality in
Health Care, Vol. 24, pp. 476–482.
Singla, A.K., Kitch, B.T., Weissman, J.S., & Campbell, E.G. (2006). ‘Assessing Patient Safety
Culture: A Review and Synthesis of the Measurement Tools’, Journal of Patient Safety,
Vol. 2, pp. 105-115.
Waterson, P., Griffiths, P., Stride, C., Murphy, J., &Hignett, S. (2010). ‘Psychometric properties
of the Hospital Survey on Patient Safety Culture: findings from the UK’, Quality and
Safety in Healthcare.Retrieved From:
http://qualitysafety.bmj.com/content/early/2010/03/04/qshc.2008.031625.
Runciman, W., Hibbert, P., & Thomson, R.(2009). ‘Towards an international classification for
patient safety: key concepts and terms’, International Journal of Quality in Health Care,
Vol. 21, pp.18–26.
Schnitzer, S., Kuhlmey, A., & Adolph, H., (2012). ‘Complaints as indicators of health care
shortcomings: which groups of patients are affected?’ International Journal of Quality in
Health Care, Vol. 24, pp. 476–482.
Singla, A.K., Kitch, B.T., Weissman, J.S., & Campbell, E.G. (2006). ‘Assessing Patient Safety
Culture: A Review and Synthesis of the Measurement Tools’, Journal of Patient Safety,
Vol. 2, pp. 105-115.
Waterson, P., Griffiths, P., Stride, C., Murphy, J., &Hignett, S. (2010). ‘Psychometric properties
of the Hospital Survey on Patient Safety Culture: findings from the UK’, Quality and
Safety in Healthcare.Retrieved From:
http://qualitysafety.bmj.com/content/early/2010/03/04/qshc.2008.031625.
1 out of 17
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.