Hepatitis C in Egypt: Epidemiology, Risks, Trends, and Future Outlook
VerifiedAdded on 2021/04/21

1
Hepatitis C in Egypt
Name
Institution
Paraphrase This Document
HEPATITIS C IN EGYPT
Task 1: Key characteristic of the HEPATITIS C infection
Hepatitis C implies inflammation of the liver caused by drugs, viruses, autoimmune
diseases, and alcohol. The pathogens (bloodborne) associated with hepatitis C is called HCV.
HCV results in severe, lasting liver damage alongside death (potentially). HCV was identified in
the year 1989. Most hepatitis C infection (50 to 85%) turns to chronic thereby leading to liver
disease. Hepatitis C infection is characteristically mild at initial phases, and it is usually not
diagnosed till it has triggered substantial liver damage. The cycle of this illness from infection to
significant damage to the liver takes twenty years and more (Abdel-Hamid et al., 2007).
The HCV is a bloodborne virus. The mode of transmission can be injection of drug use
via the injection equipment sharing; the reutilization/insufficient medical equipment
sterilization (esp. syringes); alongside the unscreened blood and associated products’
transfusion. It can further be sexually transmitted and able to be passed from an infected
mother to the baby; nevertheless, these modes remain less common (Nouroz, Shaheen,
Mujtaba & Noreen, 2015). The HCV host is the human liver. It enters the host cell via the
interactions of a coordinated pathway of sexual co-receptor that are yet to be elucidated
entirely.
Human symptomology: The Hepatitis C’s incubations is usually two weeks to six months.
After the first infection, nearly 80 percent of the individual don’t display any symptoms. Acutely
symptomatic individuals could manifest fever, declined appetite, nausea, fatigue, abdominal
pain, vomiting, joint pain, grey-colored faeces, dark urine, and jaundice (Mohamoud, Mumtaz,
Riome, Miller & Abu-Raddad, 2013).
It is lymphotrophic illness associated with two distinct kinds of arthritis-rheumatoid and
intermittent monoarticular/oligoarticular non-destructive one. The former arthritis-like picture,
albeit milder, and seldom linked to erosions. The latter affects huge-and medium-sized joints,
usually with mixed cryoglobulinemia. HCV could coexist alongside JIA; albeit no pediatric
studies evidence (Mohamoud, Mumtaz, Riome, Miller & Abu-Raddad, 2013).
The HCV infection leads to immunity. It is bizarrely useful in creating a lasting infection,
feasibly mediated by the impaired immune response to the virus infection. It affects immune
cells like macrophages, T cells and B cells. HCV core entails immunomodulatory function that
suppresses the immune response of the host. This changed function of immune cells triggered
by HCV accounts for the inefficient immune response to the virus (Mohamoud, Mumtaz, Riome,
Miller & Abu-Raddad, 2013).
Task 2: Hepatitis C Epidemiology in Egypt
HCV Prevalence in General Population:
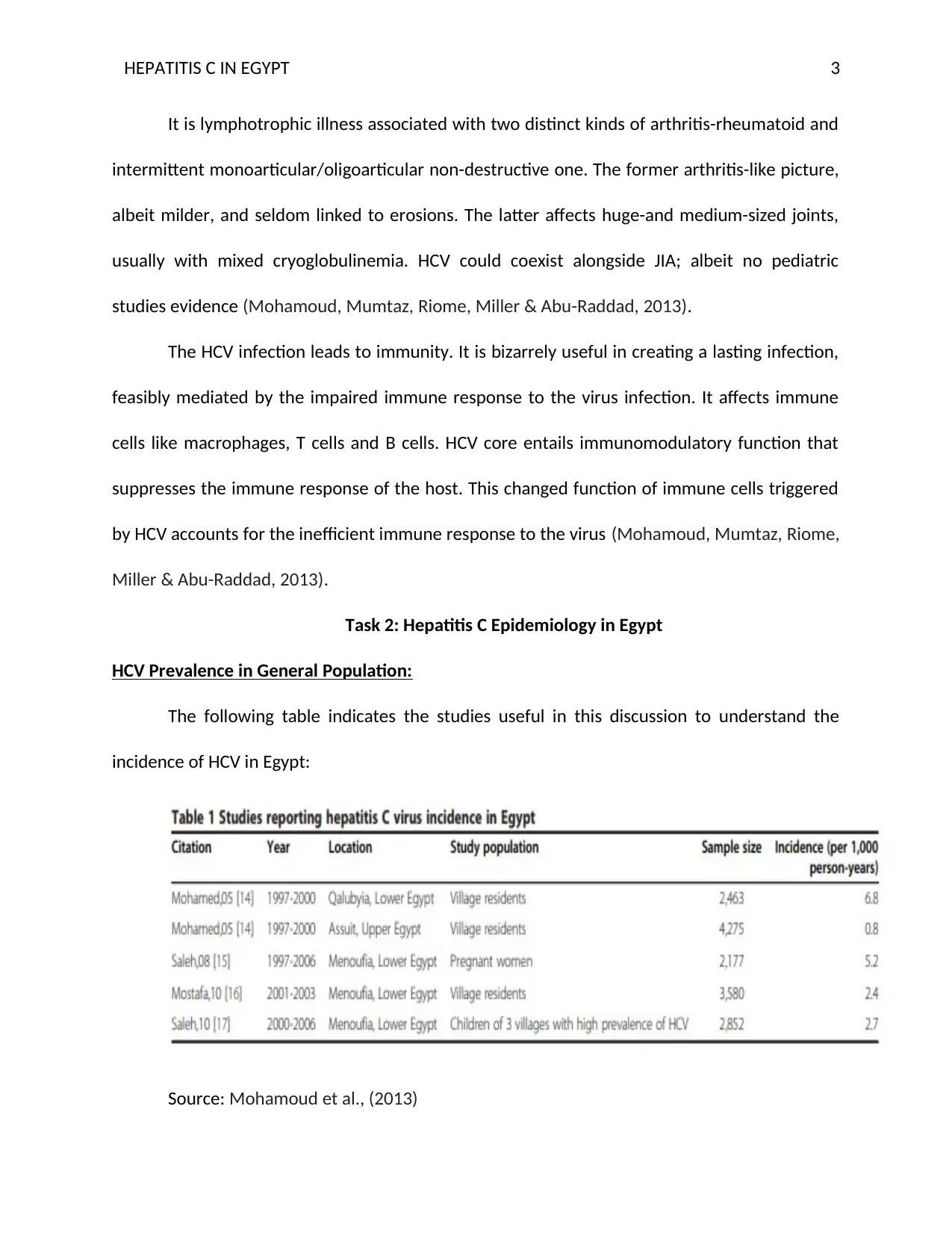
The following table indicates the studies useful in this discussion to understand the
incidence of HCV in Egypt:
Source: Mohamoud et al., (2013)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
There is an extremely high HCV prevalence (up to 41% in some studies) in Egypt. The
incidence, overall, seems to surge suddenly with age whereby the uppermost rates identified
amongst over 40 years. Higher prevalence is also noted in blood donors who are paid alongside
family replacement blood donors as opposed to unpaid ones. Higher prevalence is also pointed
out among the male blood donors as opposed to the female group (El-Hawary et al., 2007).
The rural-drawn blood donors had a higher prevalence as opposed to urban regions. The
village residents showed high prevalence rates of about twenty percent higher than that of the
national average. Like blood donors, the village counterparts show higher prevalence among
males as opposed to female colleagues. The rate of prevalence in children aged 0 to 19 ranges
between 7 and 9.90 percent. People between 20 and 39 years had prevalence rate increased to
27.6 percent from that of children while it more than doubled among the villagers above 40
years (Mohamoud, Mumtaz, Riome, Miller & Abu-Raddad, 2013).
Among the pregnant women, about 8 percent prevalence rate was reported in Benha
and Assuit whereas it was as high as fifteen percent in the Nile Delta rural region. Among the
rural school children, the prevalence rate average was approximately 4 percent for children
who attend outpatient clinics (Estes, 2015). Among the tourism worker, fire brigade personnel
and army recruits recorded higher prevalence.
Paraphrase This Document
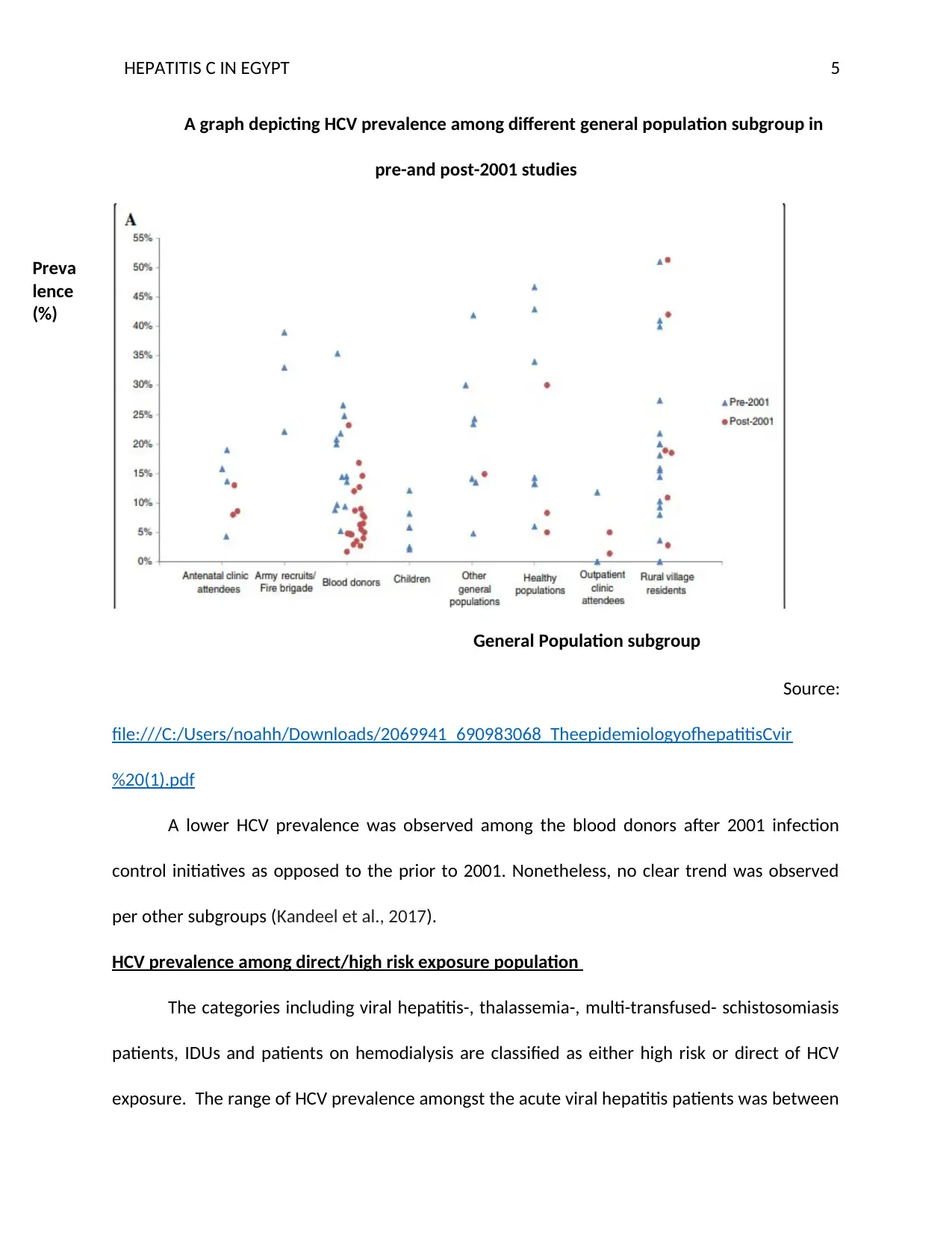
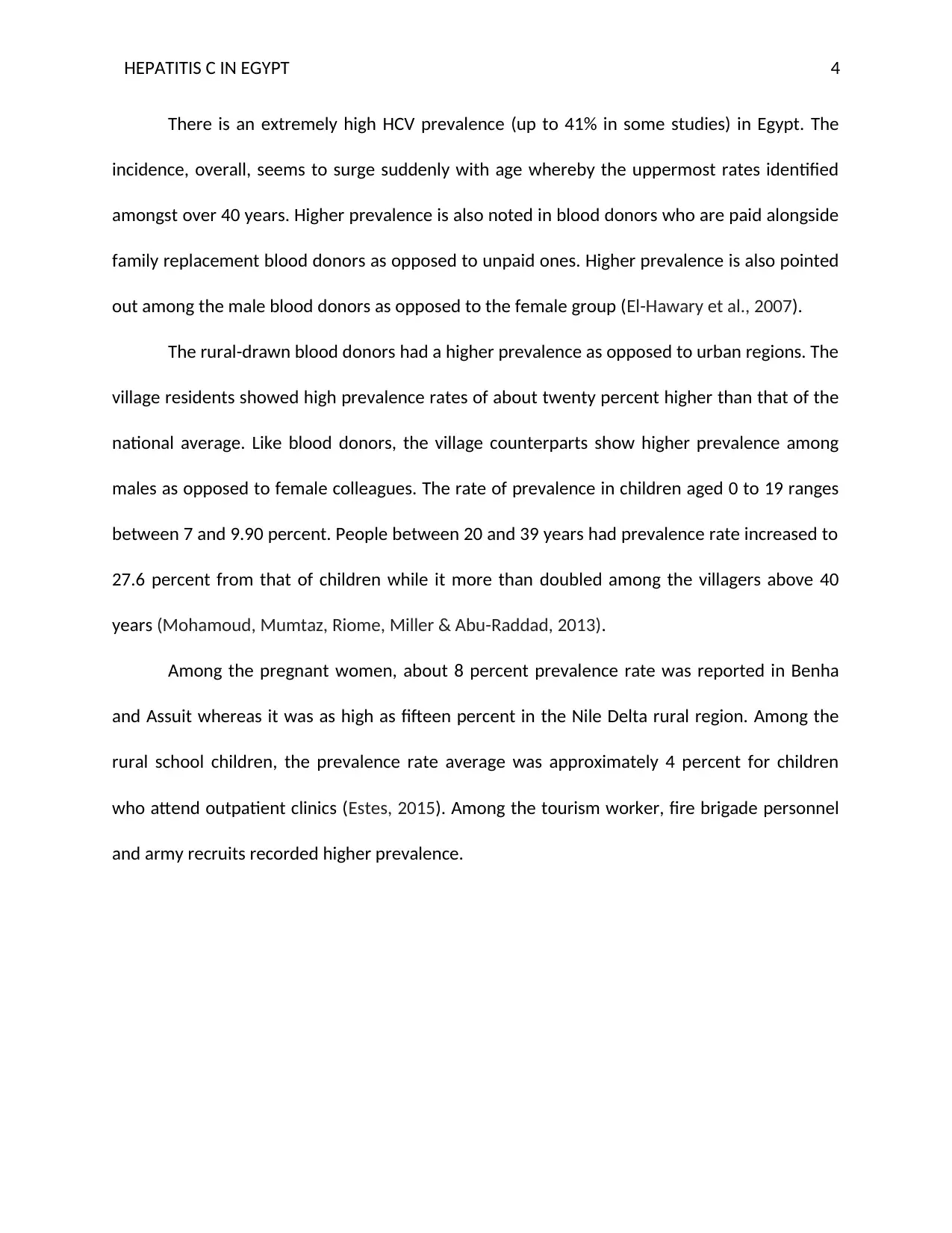
A graph depicting HCV prevalence among different general population subgroup in
pre-and post-2001 studies
Source:
file:///C:/Users/noahh/Downloads/2069941_690983068_TheepidemiologyofhepatitisCvir
%20(1).pdf
A lower HCV prevalence was observed among the blood donors after 2001 infection
control initiatives as opposed to the prior to 2001. Nonetheless, no clear trend was observed
per other subgroups (Kandeel et al., 2017).
HCV prevalence among direct/high risk exposure population
The categories including viral hepatitis-, thalassemia-, multi-transfused- schistosomiasis
patients, IDUs and patients on hemodialysis are classified as either high risk or direct of HCV
exposure. The range of HCV prevalence amongst the acute viral hepatitis patients was between
Preva
lence
(%)
General Population subgroup
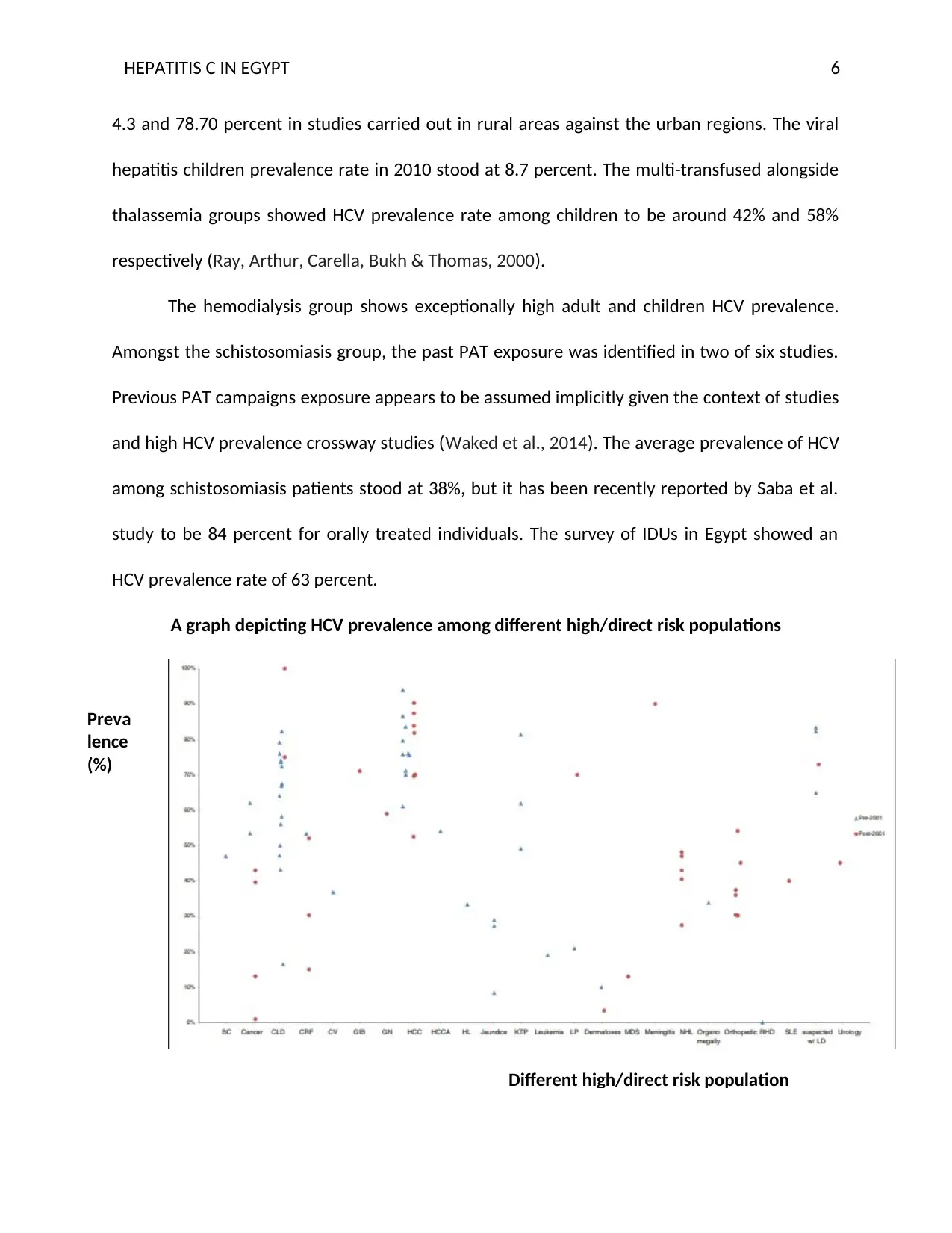
4.3 and 78.70 percent in studies carried out in rural areas against the urban regions. The viral
hepatitis children prevalence rate in 2010 stood at 8.7 percent. The multi-transfused alongside
thalassemia groups showed HCV prevalence rate among children to be around 42% and 58%
respectively (Ray, Arthur, Carella, Bukh & Thomas, 2000).
The hemodialysis group shows exceptionally high adult and children HCV prevalence.
Amongst the schistosomiasis group, the past PAT exposure was identified in two of six studies.
Previous PAT campaigns exposure appears to be assumed implicitly given the context of studies
and high HCV prevalence crossway studies (Waked et al., 2014). The average prevalence of HCV
among schistosomiasis patients stood at 38%, but it has been recently reported by Saba et al.
study to be 84 percent for orally treated individuals. The survey of IDUs in Egypt showed an
HCV prevalence rate of 63 percent.
A graph depicting HCV prevalence among different high/direct risk populations
Preva
lence
(%)
Different high/direct risk population
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Source:
file:///C:/Users/noahh/Downloads/2069941_690983068_TheepidemiologyofhepatitisCvir
%20(1).pdf
No distinguished trend discernible in HCV prevalence distribution in pre- and post- 2001
per subgroups (Mohamoud, Mumtaz, Riome, Miller & Abu-Raddad, 2013).
Prevalence of HCV among people at direct/intermediate risk of exposure
Categories include diabetic patients, hospitalized groups, hospital outpatient attendees,
STI patients, household contacts of index cases or HCV positive cases, periodontal illness
patients, population working in chosen occupation and prisoners (Sievert et al., 2011). Higher
prevalence was noted in diabetic children than adults in Egypt than other nations. Patients
attending hospital showed higher prevalence ranging between 0 to 72.8 percent.
HCV prevalence among special clinical groups
Prevalence of HCV stood high crossways all groups. Non-Hodgkin’s lymphoma (NHL)
patients’ prevalence show about 41 percent whereas it was 39 percent among orthopedic
patients and HCC (hepatocellular carcinoma) recorded between 61.0% and 90.30% prevalence
rate with the lower rate being observed in urban as opposed to rural. No unique pattern was
discernible in HCV prevalence distribution in pre-and post-2001 per special clinical subgroups
(Mohamoud, Mumtaz, Riome, Miller & Abu-Raddad, 2013).
Time and Trend Analysis
Some studies have used both general population model alongside direct or high-risk
groups in the analysis. In regards to the former model, 26 of 87 general population types of
research lacked data gathering year (Mohamoud, Mumtaz, Riome, Miller & Abu-Raddad, 2013).
Paraphrase This Document
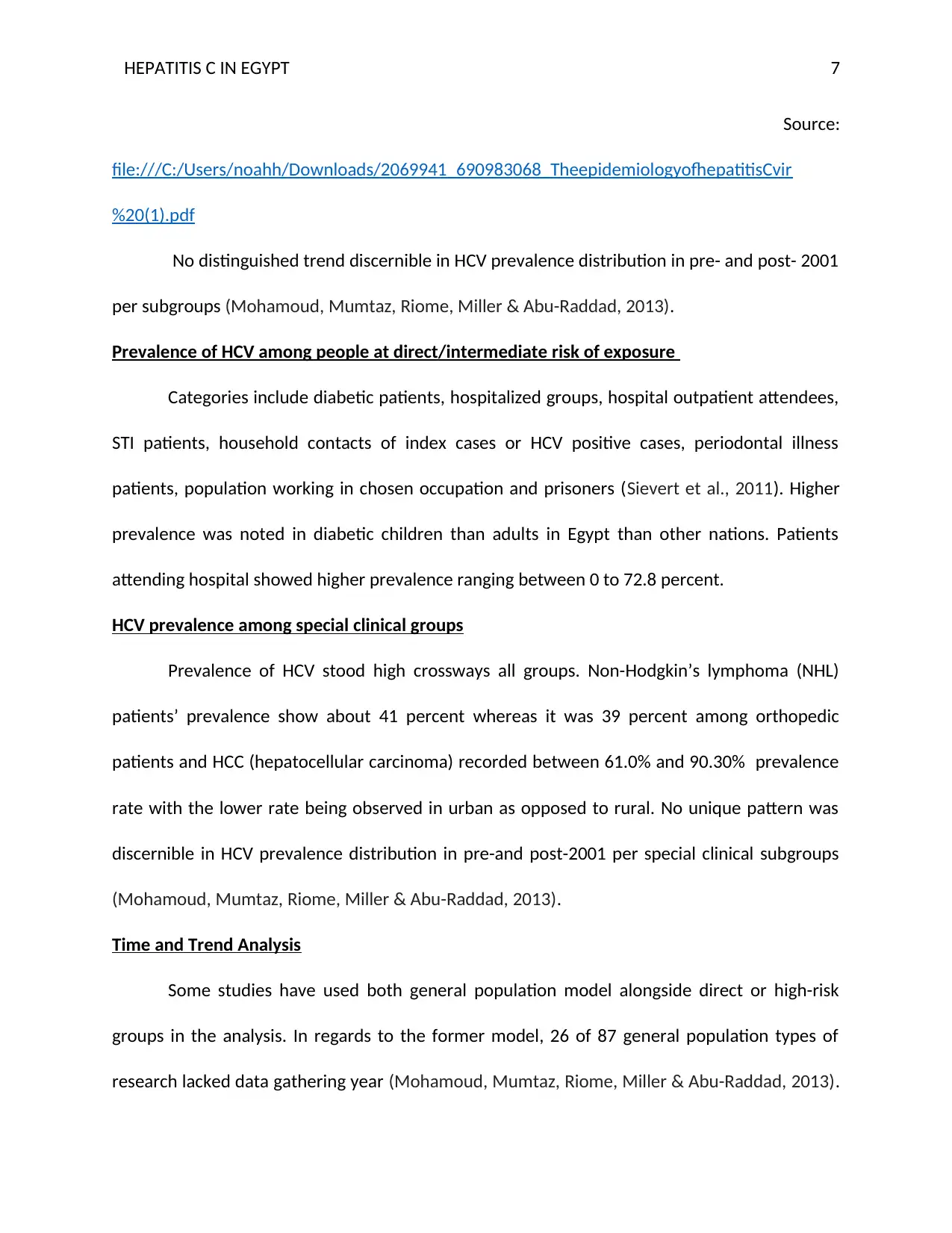
The outcome of their t-test (paired) recognizes a man variation of 3.10 years (95.0% Confidence
Interval: 2.60 to 3.60) between the publication year and data gathering year for researches with
each value. The authors applied time lag in the estimation of data gathering year for studies
lacking values. In separate univariate linear regression examination of every subgroup, blood
donors singly showed a statistically significant alteration in the prevalence of HCV over time
(Nafeh, et al., 2000). In multivariate linear regression examination for merged general
population subgroups, no proof of a statistically drop in the HCV prevalence was observed over
time.
Time and trend analysis
Source:
file:///C:/Users/noahh/Downloads/2069941_690983068_TheepidemiologyofhepatitisCvir
%20(1).pdf
In the latter model, 25 of 46 direct/ high-risk group studies lacked data gathering year.
The outcome of t-test (paired) acknowledged a 3.30 years mean variation (95.0% Confidence
Interval: 4.0-2.60) between data collection and publication year. The time lag was applied in
estimating data gathering year for researches without values (Miller & Abu-Raddad, 2010).
None of proof of a statistically significant drop in incidence of HCV over time per high-risk
subgroup as a whole.
Task 3: HCV Epidemiology Expectation in Next Ten Years
Egypt has already launched an HCV treatment programs utilizing direct-acting antivirals
(DAAs). 5 conceivable programme scale-up together with sustainability scenarios for the
prevention of HCV in Egypt assessment helps determine the future of HCV in case no further
strategies are implemented. The analysis showcases that there is a declining trend in the
prevalence of Egypt’s HCV. However, from the literature reveals that the HCV prevalence will
persist to a substantial degree for decades if Egypt does not control it by interventions
(Mohamoud, Mumtaz, Riome, Miller & Abu-Raddad, 2013).
The assessment reveals that crossways the five programme scenarios, 1.75M to 5.6M
treatments stood subsequently administered by year 2030 (Ayoub & Abu Raddad, 2017). The‐
reduction in HCV incidence or the yearly quantity of new infections by 2030 varied between 20
to 99.0%. The programme-attached decrease in the rate of occurrence of new infections a
susceptible individual a year ranged between eighteen and ninety-nine percent.
The number of averted infection varied between 42,393 and 469,599 and prevalence of
chronic infections hit as low as 2.80% to 0.1%. The prevalence increase rate reductions year by
year ranged between 7 and 15 percent in 1st ten years of programme in many scenarios. In
2030, the coverage of treatment hovered between 24.90% and 98.80%, and the treatment
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
quantity needed to prevent a single unique infection hovered between 12.10 and 9.50
(Mohamoud, Mumtaz, Riome, Miller & Abu-Raddad, 2013).
The projected target for the year 2030 might never be accomplished in the absence of
treatment up-scaling to 365,000 a year alongside sustaining it for ten years. To sum up, the DAA
scale-up shall have a substantial and instant influence on the incidence of HCV in Egypt.
Elimination of HCV prevalence remains feasible by the year 2030 only if Egypt commits
adequate resources to programme scale-up alongside sustainability. The treatment of HCV as
prevention is a practical and potent approach to prevention (Mohamoud, Mumtaz, Riome,
Miller & Abu-Raddad, 2013).
The implication of different scale-up scenarios and sustainability assessment performed
by Ayoub & Abu Raddad (2017) for the HCV-Tasp in Egypt presents a clear picture of HCV‐
prevalence in the coming ten years without new interventions. The forecasted epidemiologic,
programming as well as health economics measures illustrate that HCV-TasP remains a
compelling and potent prevention intervention which can result in the elimination by the year
2030.
Egypt has the rare opportunity currently to avert 500, 000 new HCV infections and
remove HCV and much of HCV’s illness sequelae by the year 2030. This will only be
accomplished by scaling-up as well as sustaining Egypt recently launched treatment
programme, DAA.
Paraphrase This Document
REFERENCES
Abdel-Hamid, M., El-Daly, M., Molnegren, V., El-Kafrawy, S., Abdel-Latif, S., Esmat, G., ... &
Widell, A. (2007). Genetic diversity in hepatitis C virus in Egypt and possible association
with hepatocellular carcinoma. Journal of general virology, 88(5), 1526-1531.
Ayoub, H. H., & Abu‐Raddad, L. J. (2017). Impact of treatment on hepatitis C virus transmission
and incidence in Egypt: A case for treatment as prevention. Journal of viral
hepatitis, 24(6), 486-495.
El‐Akel, W., El‐Sayed, M. H., El Kassas, M., El‐Serafy, M., Khairy, M., Elsaeed, K., ... & Shaker, M.
K. (2017). National treatment programme of hepatitis C in Egypt: Hepatitis C virus model
of care. Journal of viral hepatitis, 24(4), 262-267.
Elgharably, A., Gomaa, A. I., Crossey, M. M., Norsworthy, P. J., Waked, I., & Taylor-Robinson, S.
D. (2017). Hepatitis C in Egypt–past, present, and future. International journal of general
medicine, 10, 1.
El-Hawary, M. A., El-Raziky, M. S., Esmat, G., Soliman, H., Abouzied, A., El-Raziky, M., ... & El-
Karaksy, H. (2007). Assessment of hepatic fibrosis in pediatric cases with hepatitis C
virus in Egypt. World Journal of Gastroenterology: WJG, 13(20), 2846.
Estes, C., Abdel‐Kareem, M., Abdel‐Razek, W., Abdel‐Sameea, E., Abuzeid, M., Gomaa, A., ... &
Waked, I. (2015). Economic burden of hepatitis C in Egypt: the future impact of highly
effective therapies. Alimentary pharmacology & therapeutics, 42(6), 696-706.
Kandeel, A., Genedy, M., El‐Refai, S., Funk, A. L., Fontanet, A., & Talaat, M. (2017). The
prevalence of hepatitis C virus infection in Egypt 2015: implications for future policy on
prevention and treatment. Liver International, 37(1), 45-53.
Kouyoumjian, S. P., Chemaitelly, H., & Abu-Raddad, L. J. (2018). Characterizing hepatitis C virus
epidemiology in Egypt: systematic reviews, meta-analyses, and meta-
regressions. Scientific reports, 8(1), 1661.
Lehman, E. M., & Wilson, M. L. (2009). Epidemic hepatitis C virus infection in Egypt: estimates of
past incidence and future morbidity and mortality. Journal of viral hepatitis, 16(9), 650-
658.
Miller, F. D., & Abu-Raddad, L. J. (2010). Evidence of intense ongoing endemic transmission of
hepatitis C virus in Egypt. Proceedings of the National Academy of Sciences, 107(33),
14757-14762.
Mohamoud, Y. A., Mumtaz, G. R., Riome, S., Miller, D., & Abu-Raddad, L. J. (2013). The
epidemiology of hepatitis C virus in Egypt: a systematic review and data synthesis. BMC
infectious diseases, 13(1), 288.
Nafeh, M. A., Medhat, A., Shehata, M., Mikhail, N. N., Swifee, Y., Abdel-Hamid, M., ... & Sallam,
I. (2000). Hepatitis C in a community in Upper Egypt: I. Cross-sectional survey. The
American journal of tropical medicine and hygiene, 63(5), 236-241.
Nouroz, F., Shaheen, S., Mujtaba, G., & Noreen, S. (2015). An overview on hepatitis C virus
genotypes and its control. Egyptian Journal of Medical Human Genetics, 16(4), 291-298.
Ray, S. C., Arthur, R. R., Carella, A., Bukh, J., & Thomas, D. L. (2000). Genetic epidemiology of
hepatitis C virus throughout Egypt. The Journal of infectious diseases, 182(3), 698-707.
Sievert, W., Altraif, I., Razavi, H. A., Abdo, A., Ahmed, E. A., AlOmair, A., ... & Elshazly, M. (2011).
A systematic review of hepatitis C virus epidemiology in Asia, Australia and Egypt. Liver
International, 31(s2), 61-80.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

Waked, I., Doss, W., El-Sayed, M. H., Estes, C., Razavi, H., Shiha, G., ... & Esmat, G. (2014). The
current and future disease burden of chronic hepatitis C virus infection in Egypt. Arab J
Gastroenterol, 15(2), 45-52.
Paraphrase This Document
Part 2: Public Summary
Egypt has the highest prevalence rate (14.70%) of HCV than any other nation in the
world. The HCV cycle from infection to significant damage to the liver takes twenty years or
more. The pathogen (bloodborne virus) causing Hepatitis C is called HCV. The primary mode of
transmission of HCV is through sharing of injection equipment like syringes.
The host of HCV is the human liver, and the virus enters through a coordinated pathway
of partially elucidated sexual co-receptor. The human pathology for symptomatic people
includes fever, reduced appetite, and fatigue. The HCV infection leads to immunity as it creates
permanent infection after attacking immune cells including T cells, macrophages and B cells.
The incidence of HCV falls in the bracket of 0.8 to 6.8 for every 1000 person-years. HCV
prevalence among the pregnant individuals ranges between 5 and 15 percent. The prevalence
of HCV among the blood donors ranged between 5 and 25 percent while it ranges between 0
and 40 percent for the general population cohorts (Kouyoumjian, Chemaitelly & Abu-Raddad,
2018). Among the multi-transfused patients, it varies between 10 and 55% while among the
dialysis patients, the range was between 50 and 90 percent. Among the high-risk group, HCV
ranges between 10 and 85 percent.
The prevalence of HCV varies broadly among other clinical groups and groups at
intermediate risk. The parenteral anti-schistosomal therapy appears to be the risk factors
alongside transfusions, surgical procedures, and injections. The time trend analysis outcome
shows no evidence of statistically significant plunge in the prevalence of HCV over time. Egypt
appears to be increasingly confronted with the burden of HCV illness of historical degrees which
isolates it from other countries (El‐Akel et al., 2017).
A massive epidemic of HCV seems to have taken place at the national level with
significant transmission persisting to date. There is a need for Egypt to have HCV prevention as
a national priority. The country’s policymakers alongside public health besides medical care
stakeholders must introduce as well as implement additional measures that target the HCV
transmission routes to prevent its increasing prevalence.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
REFERENCES
Abdel-Hamid, M., El-Daly, M., Molnegren, V., El-Kafrawy, S., Abdel-Latif, S., Esmat, G., ... &
Widell, A. (2007). Genetic diversity in hepatitis C virus in Egypt and possible association
with hepatocellular carcinoma. Journal of general virology, 88(5), 1526-1531.
Ayoub, H. H., & Abu‐Raddad, L. J. (2017). Impact of treatment on hepatitis C virus transmission
and incidence in Egypt: A case for treatment as prevention. Journal of viral
hepatitis, 24(6), 486-495.
El‐Akel, W., El‐Sayed, M. H., El Kassas, M., El‐Serafy, M., Khairy, M., Elsaeed, K., ... & Shaker, M.
K. (2017). National treatment programme of hepatitis C in Egypt: Hepatitis C virus model
of care. Journal of viral hepatitis, 24(4), 262-267.
Elgharably, A., Gomaa, A. I., Crossey, M. M., Norsworthy, P. J., Waked, I., & Taylor-Robinson, S.
D. (2017). Hepatitis C in Egypt–past, present, and future. International journal of general
medicine, 10, 1.
El-Hawary, M. A., El-Raziky, M. S., Esmat, G., Soliman, H., Abouzied, A., El-Raziky, M., ... & El-
Karaksy, H. (2007). Assessment of hepatic fibrosis in pediatric cases with hepatitis C
virus in Egypt. World Journal of Gastroenterology: WJG, 13(20), 2846.
Estes, C., Abdel‐Kareem, M., Abdel‐Razek, W., Abdel‐Sameea, E., Abuzeid, M., Gomaa, A., ... &
Waked, I. (2015). Economic burden of hepatitis C in Egypt: the future impact of highly
effective therapies. Alimentary pharmacology & therapeutics, 42(6), 696-706.
Kandeel, A., Genedy, M., El‐Refai, S., Funk, A. L., Fontanet, A., & Talaat, M. (2017). The
prevalence of hepatitis C virus infection in Egypt 2015: implications for future policy on
prevention and treatment. Liver International, 37(1), 45-53.
Paraphrase This Document
Kouyoumjian, S. P., Chemaitelly, H., & Abu-Raddad, L. J. (2018). Characterizing hepatitis C virus
epidemiology in Egypt: systematic reviews, meta-analyses, and meta-
regressions. Scientific reports, 8(1), 1661.
Lehman, E. M., & Wilson, M. L. (2009). Epidemic hepatitis C virus infection in Egypt: estimates of
past incidence and future morbidity and mortality. Journal of viral hepatitis, 16(9), 650-
658.
Miller, F. D., & Abu-Raddad, L. J. (2010). Evidence of intense ongoing endemic transmission of
hepatitis C virus in Egypt. Proceedings of the National Academy of Sciences, 107(33),
14757-14762.
Mohamoud, Y. A., Mumtaz, G. R., Riome, S., Miller, D., & Abu-Raddad, L. J. (2013). The
epidemiology of hepatitis C virus in Egypt: a systematic review and data synthesis. BMC
infectious diseases, 13(1), 288.
Nafeh, M. A., Medhat, A., Shehata, M., Mikhail, N. N., Swifee, Y., Abdel-Hamid, M., ... & Sallam,
I. (2000). Hepatitis C in a community in Upper Egypt: I. Cross-sectional survey. The
American journal of tropical medicine and hygiene, 63(5), 236-241.
Nouroz, F., Shaheen, S., Mujtaba, G., & Noreen, S. (2015). An overview on hepatitis C virus
genotypes and its control. Egyptian Journal of Medical Human Genetics, 16(4), 291-298.
Ray, S. C., Arthur, R. R., Carella, A., Bukh, J., & Thomas, D. L. (2000). Genetic epidemiology of
hepatitis C virus throughout Egypt. The Journal of infectious diseases, 182(3), 698-707.
Sievert, W., Altraif, I., Razavi, H. A., Abdo, A., Ahmed, E. A., AlOmair, A., ... & Elshazly, M. (2011).
A systematic review of hepatitis C virus epidemiology in Asia, Australia and Egypt. Liver
International, 31(s2), 61-80.

Waked, I., Doss, W., El-Sayed, M. H., Estes, C., Razavi, H., Shiha, G., ... & Esmat, G. (2014). The
current and future disease burden of chronic hepatitis C virus infection in Egypt. Arab J
Gastroenterol, 15(2), 45-52.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
© 2024 | Zucol Services PVT LTD | All rights reserved.