Indigenous Health Disparities in Australia
VerifiedAdded on 2020/02/24
|12
|2744
|274
AI Summary
This assignment explores the significant health disparities experienced by Indigenous peoples in Australia. It delves into the impact of perceived discrimination, distrust in healthcare systems, limited social capital, and unhealthy behaviors on their well-being. The analysis emphasizes the crucial role of cultural competency in healthcare delivery and examines existing policies aimed at closing the gap in health outcomes between Indigenous and non-Indigenous Australians. Relevant literature, including research articles and reports from organizations like the Australian Institute of Health and Welfare (AIHW), is cited to support the arguments.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: NURSING ASSIGNMENT
Nursing assignment
Name of the student:
Name of the University:
Author’s note
Nursing assignment
Name of the student:
Name of the University:
Author’s note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1NURSING ASSIGNMENT
Topic- Reflection on the cultural diversity in Australia and health issue of Aboriginal and
Torres Strait Islanders
Use of sociological imagination template to reflect on feelings, thoughts and observation
related to the topic
The sociological imagination (SI) template is a term described by a sociologist named
Wright Mills as the awareness of the association or link between personal experience and wider
events in society. The use of imaginative thought and reflection related to an event facilitates
sociological imagination and understanding one’s connection with the wider social realities
(Giddens et al., 2016). Hence, this wider method of sociological analysis helps to focus not just
on personal issues but also on the wider issues faced by certain group in society. Germov, (2014)
states that linking one’s personal problem and social functions with societal problem support
collective action to address any change. By using the sociological imagination template, the
historical, cultural, structural and critical factors related to a social problem can be effectively
analysed. Applying this template in reflective task helps to link personal trouble to public issues.
Topic- Reflection on the cultural diversity in Australia and health issue of Aboriginal and
Torres Strait Islanders
Use of sociological imagination template to reflect on feelings, thoughts and observation
related to the topic
The sociological imagination (SI) template is a term described by a sociologist named
Wright Mills as the awareness of the association or link between personal experience and wider
events in society. The use of imaginative thought and reflection related to an event facilitates
sociological imagination and understanding one’s connection with the wider social realities
(Giddens et al., 2016). Hence, this wider method of sociological analysis helps to focus not just
on personal issues but also on the wider issues faced by certain group in society. Germov, (2014)
states that linking one’s personal problem and social functions with societal problem support
collective action to address any change. By using the sociological imagination template, the
historical, cultural, structural and critical factors related to a social problem can be effectively
analysed. Applying this template in reflective task helps to link personal trouble to public issues.
2NURSING ASSIGNMENT
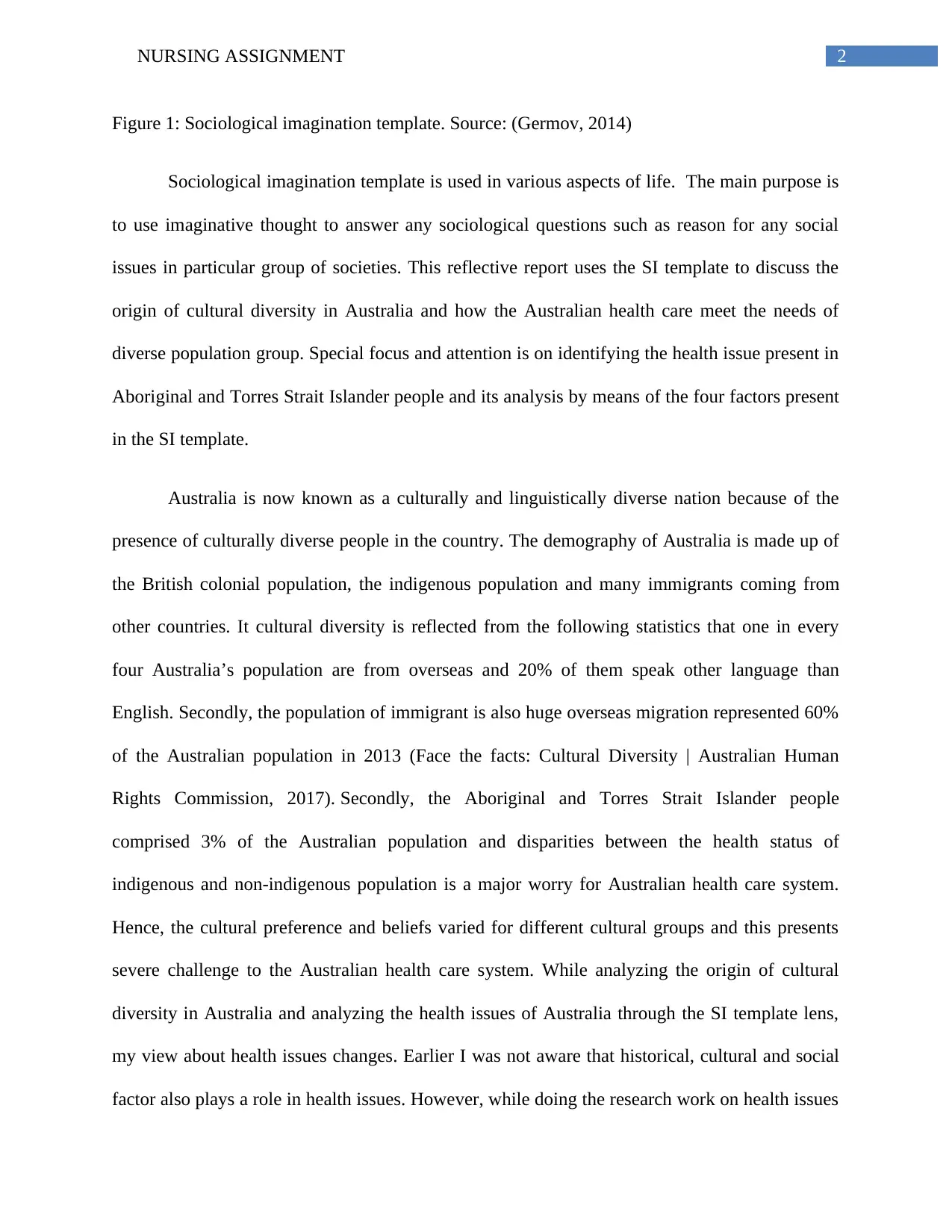
Figure 1: Sociological imagination template. Source: (Germov, 2014)
Sociological imagination template is used in various aspects of life. The main purpose is
to use imaginative thought to answer any sociological questions such as reason for any social
issues in particular group of societies. This reflective report uses the SI template to discuss the
origin of cultural diversity in Australia and how the Australian health care meet the needs of
diverse population group. Special focus and attention is on identifying the health issue present in
Aboriginal and Torres Strait Islander people and its analysis by means of the four factors present
in the SI template.
Australia is now known as a culturally and linguistically diverse nation because of the
presence of culturally diverse people in the country. The demography of Australia is made up of
the British colonial population, the indigenous population and many immigrants coming from
other countries. It cultural diversity is reflected from the following statistics that one in every
four Australia’s population are from overseas and 20% of them speak other language than
English. Secondly, the population of immigrant is also huge overseas migration represented 60%
of the Australian population in 2013 (Face the facts: Cultural Diversity | Australian Human
Rights Commission, 2017). Secondly, the Aboriginal and Torres Strait Islander people
comprised 3% of the Australian population and disparities between the health status of
indigenous and non-indigenous population is a major worry for Australian health care system.
Hence, the cultural preference and beliefs varied for different cultural groups and this presents
severe challenge to the Australian health care system. While analyzing the origin of cultural
diversity in Australia and analyzing the health issues of Australia through the SI template lens,
my view about health issues changes. Earlier I was not aware that historical, cultural and social
factor also plays a role in health issues. However, while doing the research work on health issues
Figure 1: Sociological imagination template. Source: (Germov, 2014)
Sociological imagination template is used in various aspects of life. The main purpose is
to use imaginative thought to answer any sociological questions such as reason for any social
issues in particular group of societies. This reflective report uses the SI template to discuss the
origin of cultural diversity in Australia and how the Australian health care meet the needs of
diverse population group. Special focus and attention is on identifying the health issue present in
Aboriginal and Torres Strait Islander people and its analysis by means of the four factors present
in the SI template.
Australia is now known as a culturally and linguistically diverse nation because of the
presence of culturally diverse people in the country. The demography of Australia is made up of
the British colonial population, the indigenous population and many immigrants coming from
other countries. It cultural diversity is reflected from the following statistics that one in every
four Australia’s population are from overseas and 20% of them speak other language than
English. Secondly, the population of immigrant is also huge overseas migration represented 60%
of the Australian population in 2013 (Face the facts: Cultural Diversity | Australian Human
Rights Commission, 2017). Secondly, the Aboriginal and Torres Strait Islander people
comprised 3% of the Australian population and disparities between the health status of
indigenous and non-indigenous population is a major worry for Australian health care system.
Hence, the cultural preference and beliefs varied for different cultural groups and this presents
severe challenge to the Australian health care system. While analyzing the origin of cultural
diversity in Australia and analyzing the health issues of Australia through the SI template lens,
my view about health issues changes. Earlier I was not aware that historical, cultural and social
factor also plays a role in health issues. However, while doing the research work on health issues
3NURSING ASSIGNMENT
in this group and comparing their culture with mine, I realized that human diversity and cultural
background contributes to many social issues. After doing this task, I realize the need to respect
the dignity of each individual despite cultural background and my own responsibility to do to
good to the society and the people around it.
Reflective writing based on SI template
Historical factors:
My country of origin is Nepal, which is a developing country with multidimensional
heritage consisting of ethnic, tribal and other social groups. The culture of the country is mainly
influenced by Tibetan, Indian and Mongolian culture. Being a Buddhist myself, I have always
paid focused on refraining from any violence and mental conduct. I come from a middle class
family and for use mental health and spiritual well-being is more important that other pleasures
in life. My own cultural beliefs and norm has been the reason for what I am today. My cultural
beliefs shaped my judgment and decision making regarding all important choices in life such as
health choices, employment choices and relationship choices. Although my country has different
tribal groups, however I never got the opportunity to work with them closely and understand the
issues facing them in daily life.
Similar to my country, Australia is also a multicultural country with about 60% of
immigrant population. Net increase in overseas migration significantly contributes to the growth
in Australian population. The first inhabitant of Australia, the Aboriginal and Torres Strait
Islander people came to Australia because of famine, floods, oppression and brutal political
regimen in their own countries (Census: Aboriginal and Torres Strait Islander population, 2017).
Many other past historical events led to the transformation of Australia into a culturally diverse
in this group and comparing their culture with mine, I realized that human diversity and cultural
background contributes to many social issues. After doing this task, I realize the need to respect
the dignity of each individual despite cultural background and my own responsibility to do to
good to the society and the people around it.
Reflective writing based on SI template
Historical factors:
My country of origin is Nepal, which is a developing country with multidimensional
heritage consisting of ethnic, tribal and other social groups. The culture of the country is mainly
influenced by Tibetan, Indian and Mongolian culture. Being a Buddhist myself, I have always
paid focused on refraining from any violence and mental conduct. I come from a middle class
family and for use mental health and spiritual well-being is more important that other pleasures
in life. My own cultural beliefs and norm has been the reason for what I am today. My cultural
beliefs shaped my judgment and decision making regarding all important choices in life such as
health choices, employment choices and relationship choices. Although my country has different
tribal groups, however I never got the opportunity to work with them closely and understand the
issues facing them in daily life.
Similar to my country, Australia is also a multicultural country with about 60% of
immigrant population. Net increase in overseas migration significantly contributes to the growth
in Australian population. The first inhabitant of Australia, the Aboriginal and Torres Strait
Islander people came to Australia because of famine, floods, oppression and brutal political
regimen in their own countries (Census: Aboriginal and Torres Strait Islander population, 2017).
Many other past historical events led to the transformation of Australia into a culturally diverse
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4NURSING ASSIGNMENT
nation. Before the European settlement, many migrant came to Australia as an explorer.
However, after the enactment of the White Australian policy in 1901, restriction was imposed on
migration of non-European Australians. This was aimed to promote British cultural identity and
exclude people who did not fit the European culture of Australian society. However, post 1973,
multicultural policies was implemented again by the Labor government and now it has
holistically embraced people from all cultures and origins (Connell & McManus,
2016). However, the presence of multicultural environment has given many threats to policy
makers and public health department. The Australian government prepared themselves to address
this challenge too. For example, the Assimilation policy was implemented to encourage new
arrivals to embrace cultural practices of country (Moorcroft, 2016). The health care department
focused on increasing the cultural competency of health care workers to address the disparities in
health between the indigenous and non-indigenous population group (Clifford et al., 2015).
Cultural factors:
My own cultural beliefs and preferences has influences my views about society and
health. In my home country, I have found that local people do not believe on the biomedical
approach to health and their perception is that illness and pain is linked to the supernatural
elements. Hence, they mostly prefer spiritual intervention to address their pain and suffering due
to diseases. Different health beliefs and cultural norms also affect the disease management
process and adherence to medication in patients. For instance, some people do not take
medications and believe in worship and prayers for protection from disease and illness. Some
prefer to seek cure through spiritual means (Wasti, S. P. (2011). However, for me biomedical
approach to health is important because my professional education in the health care fields have
strengthened my rational regarding the efficacy of biomedical cause of illness and treating
nation. Before the European settlement, many migrant came to Australia as an explorer.
However, after the enactment of the White Australian policy in 1901, restriction was imposed on
migration of non-European Australians. This was aimed to promote British cultural identity and
exclude people who did not fit the European culture of Australian society. However, post 1973,
multicultural policies was implemented again by the Labor government and now it has
holistically embraced people from all cultures and origins (Connell & McManus,
2016). However, the presence of multicultural environment has given many threats to policy
makers and public health department. The Australian government prepared themselves to address
this challenge too. For example, the Assimilation policy was implemented to encourage new
arrivals to embrace cultural practices of country (Moorcroft, 2016). The health care department
focused on increasing the cultural competency of health care workers to address the disparities in
health between the indigenous and non-indigenous population group (Clifford et al., 2015).
Cultural factors:
My own cultural beliefs and preferences has influences my views about society and
health. In my home country, I have found that local people do not believe on the biomedical
approach to health and their perception is that illness and pain is linked to the supernatural
elements. Hence, they mostly prefer spiritual intervention to address their pain and suffering due
to diseases. Different health beliefs and cultural norms also affect the disease management
process and adherence to medication in patients. For instance, some people do not take
medications and believe in worship and prayers for protection from disease and illness. Some
prefer to seek cure through spiritual means (Wasti, S. P. (2011). However, for me biomedical
approach to health is important because my professional education in the health care fields have
strengthened my rational regarding the efficacy of biomedical cause of illness and treating
5NURSING ASSIGNMENT
diseases. However, my choices in life are influences by my cultural beliefs and norms too as I do
not will to cross them.
While working in Australia, I came to know about the multicultural diversity of the
nation. Multiculturalism in Australia is high because of diversity in language, people and culture
if residents. The Australian Government has readily embraced multiculturalism by implementing
immigration policies, preventing discrimination and promoting equality for all. However,
despite such efforts, the difference in cultural beliefs and values has had an impact on health
outcome of different cultural group too.
For example, great disparity in health outcome between indigenous and the non-
indigenous Australians have been found. Life expectancy and mortality rate is an important
indicator of health outcome and life expectancy in Aboriginals were found to be lower than 10.6
years compared to the non-indigenous population in 2010-2012 (Life expectancy (AIHW),
2017). . The inequality in health status between indigenous and non-indigenous Australians is
also reflected from the high rate of infant mortality, poor health and poor education and
employment in Aboriginal and Torres Strait Islander people. Cancer and Circulatory disease was
a major cause of death in the group between 2007 and 2011. The disadvantage was also seen due
to risky behaviors lie smoking, poor nutrition, alcohol consumptions and physical inactivity.
Remoteness and poor access to health was also found to increase the health disparity (Indigenous
health (AIHW), 2017). Discrimination and negative experience in health care services also
affected the use of health service among the indigenous people. Hence, I think that focusing on
the social model of health care will be important for a multicultural nation like Australia because
this will help to focus on cultural, environment, economic and social influence on health and
reduce the gap in health outcome of different cultural groups too (Aver & Patterson, 2017).
diseases. However, my choices in life are influences by my cultural beliefs and norms too as I do
not will to cross them.
While working in Australia, I came to know about the multicultural diversity of the
nation. Multiculturalism in Australia is high because of diversity in language, people and culture
if residents. The Australian Government has readily embraced multiculturalism by implementing
immigration policies, preventing discrimination and promoting equality for all. However,
despite such efforts, the difference in cultural beliefs and values has had an impact on health
outcome of different cultural group too.
For example, great disparity in health outcome between indigenous and the non-
indigenous Australians have been found. Life expectancy and mortality rate is an important
indicator of health outcome and life expectancy in Aboriginals were found to be lower than 10.6
years compared to the non-indigenous population in 2010-2012 (Life expectancy (AIHW),
2017). . The inequality in health status between indigenous and non-indigenous Australians is
also reflected from the high rate of infant mortality, poor health and poor education and
employment in Aboriginal and Torres Strait Islander people. Cancer and Circulatory disease was
a major cause of death in the group between 2007 and 2011. The disadvantage was also seen due
to risky behaviors lie smoking, poor nutrition, alcohol consumptions and physical inactivity.
Remoteness and poor access to health was also found to increase the health disparity (Indigenous
health (AIHW), 2017). Discrimination and negative experience in health care services also
affected the use of health service among the indigenous people. Hence, I think that focusing on
the social model of health care will be important for a multicultural nation like Australia because
this will help to focus on cultural, environment, economic and social influence on health and
reduce the gap in health outcome of different cultural groups too (Aver & Patterson, 2017).
6NURSING ASSIGNMENT
Structural factors:
I come from a middle class family and my cultural value of respect and doing no harm to
people has helped me to achieve many things in life. I have always maintained a good
relationship with my family and taken their views before taking any decisions in life. In health
choices too, although I follow the biomedical approach to health, however I incorporate my
Buddhist cultural element of maintaining mental peace to promote health and well-being. Hence,
my personality and my interaction with society is dependent a lot on my cultural and religious
beliefs.
While working in Australia, I have found that biomedical model of health care is more
dominant in their health care system. All health care process and service is relies on the
biomedical model. However, as there are a large number of culturally diverse people in the
country, I feel that focusing just on the biomedical model will not help to address the health
issues of the indigenous population. Reports have shown that the cultural beliefs. experience of
discrimination and negative experiences of colonization are the major reason for health
disadvantage in Aboriginal and Torres Strait Islander people. Cultural gap has been the reason
for poor access and use of health services. Language gap has also prevented establishing
therapeutic relationship with these people (Mitrou et al., 2014). Hence, Australia has now started
focusing delivering culturally sensitive care by improving the cultural competency of staff and
addressing the social and health disadvantage factors in their life. The adaption of social model
in health delivery facilitates taking many preventive measures to reduce negative health outcome
in indigenous population.
Critical factors:
Structural factors:
I come from a middle class family and my cultural value of respect and doing no harm to
people has helped me to achieve many things in life. I have always maintained a good
relationship with my family and taken their views before taking any decisions in life. In health
choices too, although I follow the biomedical approach to health, however I incorporate my
Buddhist cultural element of maintaining mental peace to promote health and well-being. Hence,
my personality and my interaction with society is dependent a lot on my cultural and religious
beliefs.
While working in Australia, I have found that biomedical model of health care is more
dominant in their health care system. All health care process and service is relies on the
biomedical model. However, as there are a large number of culturally diverse people in the
country, I feel that focusing just on the biomedical model will not help to address the health
issues of the indigenous population. Reports have shown that the cultural beliefs. experience of
discrimination and negative experiences of colonization are the major reason for health
disadvantage in Aboriginal and Torres Strait Islander people. Cultural gap has been the reason
for poor access and use of health services. Language gap has also prevented establishing
therapeutic relationship with these people (Mitrou et al., 2014). Hence, Australia has now started
focusing delivering culturally sensitive care by improving the cultural competency of staff and
addressing the social and health disadvantage factors in their life. The adaption of social model
in health delivery facilitates taking many preventive measures to reduce negative health outcome
in indigenous population.
Critical factors:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7NURSING ASSIGNMENT
Cultural values have not made my life difficult. This is because I have balanced based on
my knowledge and insight regarding the benefits of different social element and processes in
society. This has helped me to manage my health concerns and profession decisions too. The
Australian health care is also focusing a lot on social model of care to address health disparities
in a multicultural environment. In response to the closing the gap policy, there has been a focus
on improving cultural competency to improve the quality and effectiveness of care for
indigenous people (Cultural competency in the delivery of health services for Indigenous people,
2017).
Alignment with ACU graduate attributes
By research on the topic of origins of cultural diversity in Australia and the health issues
specific to the Aboriginal and Torres Strait Islander people, I came to know about the great
cultural gap between indigenous and non-indigenous Australian. Before doing this reflective
assignment, I was not aware about the hardship experienced by this group and how their past
experience had an impact on health. However, while researching on the cause of negative health
outcome in Aboriginal people in Australia, I was shocked to know that they were victim of brutal
political regimen in their own country. Secondly, after migrating to Australia, hardship continued
for them due to cultural shock, discrimination and poor experience in health care service. Lack of
access to proper housing, employment and employment also played a role in negative health
outcome (Chen, D., & Yang, T. C. (2014).. After doing their reflecting writing, I have more
respect for this people and in future, my outlook towards migrant people will not remain the
change. I will always approach them with dignity and do my best to understand their cultural
views and preferences while interacting with them in my professional life.
Cultural values have not made my life difficult. This is because I have balanced based on
my knowledge and insight regarding the benefits of different social element and processes in
society. This has helped me to manage my health concerns and profession decisions too. The
Australian health care is also focusing a lot on social model of care to address health disparities
in a multicultural environment. In response to the closing the gap policy, there has been a focus
on improving cultural competency to improve the quality and effectiveness of care for
indigenous people (Cultural competency in the delivery of health services for Indigenous people,
2017).
Alignment with ACU graduate attributes
By research on the topic of origins of cultural diversity in Australia and the health issues
specific to the Aboriginal and Torres Strait Islander people, I came to know about the great
cultural gap between indigenous and non-indigenous Australian. Before doing this reflective
assignment, I was not aware about the hardship experienced by this group and how their past
experience had an impact on health. However, while researching on the cause of negative health
outcome in Aboriginal people in Australia, I was shocked to know that they were victim of brutal
political regimen in their own country. Secondly, after migrating to Australia, hardship continued
for them due to cultural shock, discrimination and poor experience in health care service. Lack of
access to proper housing, employment and employment also played a role in negative health
outcome (Chen, D., & Yang, T. C. (2014).. After doing their reflecting writing, I have more
respect for this people and in future, my outlook towards migrant people will not remain the
change. I will always approach them with dignity and do my best to understand their cultural
views and preferences while interacting with them in my professional life.
8NURSING ASSIGNMENT
9NURSING ASSIGNMENT
Reference
Avery, N., & Patterson, S. (2017). Physical Health in Public Mental Health Care: A Qualitative
Study Employing the COM‐B Model of Behaviour to Describe Views and Practices of
Australian Psychologists. Australian Psychologist.
Census: Aboriginal and Torres Strait Islander population. (2017). Abs.gov.au. Retrieved 4
September 2017, from
http://www.abs.gov.au/ausstats/abs@.nsf/MediaRealesesByCatalogue/02D50FAA9987D
6B7CA25814800087E03?OpenDocument
Chen, D., & Yang, T. C. (2014). The pathways from perceived discrimination to self-rated
health: an investigation of the roles of distrust, social capital, and health behaviors. Social
science & medicine, 104, 64-73.
Clifford, A., McCalman, J., Bainbridge, R., & Tsey, K. (2015). Interventions to improve cultural
competency in health care for Indigenous peoples of Australia, New Zealand, Canada and
the USA: a systematic review. International Journal for Quality in Health Care, 27(2),
89-98.
Connell, J., & McManus, P. (2016). Rural revival?: place marketing, tree change and regional
migration in Australia. Routledge.
Cultural competency in the delivery of health services for Indigenous people. (2017). Retrieved 4
September 2017, from
http://www.aihw.gov.au/uploadedFiles/ClosingTheGap/Content/Our_publications/2015/
ctgc-ip13.pdf
Reference
Avery, N., & Patterson, S. (2017). Physical Health in Public Mental Health Care: A Qualitative
Study Employing the COM‐B Model of Behaviour to Describe Views and Practices of
Australian Psychologists. Australian Psychologist.
Census: Aboriginal and Torres Strait Islander population. (2017). Abs.gov.au. Retrieved 4
September 2017, from
http://www.abs.gov.au/ausstats/abs@.nsf/MediaRealesesByCatalogue/02D50FAA9987D
6B7CA25814800087E03?OpenDocument
Chen, D., & Yang, T. C. (2014). The pathways from perceived discrimination to self-rated
health: an investigation of the roles of distrust, social capital, and health behaviors. Social
science & medicine, 104, 64-73.
Clifford, A., McCalman, J., Bainbridge, R., & Tsey, K. (2015). Interventions to improve cultural
competency in health care for Indigenous peoples of Australia, New Zealand, Canada and
the USA: a systematic review. International Journal for Quality in Health Care, 27(2),
89-98.
Connell, J., & McManus, P. (2016). Rural revival?: place marketing, tree change and regional
migration in Australia. Routledge.
Cultural competency in the delivery of health services for Indigenous people. (2017). Retrieved 4
September 2017, from
http://www.aihw.gov.au/uploadedFiles/ClosingTheGap/Content/Our_publications/2015/
ctgc-ip13.pdf
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10NURSING ASSIGNMENT
Face the facts: Aboriginal and Torres Strait Islander Peoples | Australian Human Rights
Commission. (2017). Humanrights.gov.au. Retrieved 4 September 2017, from
https://www.humanrights.gov.au/education/face-facts/face-facts-aboriginal-and-torres-
strait-islander-peoples
Face the facts: Cultural Diversity | Australian Human Rights Commission.
(2017). Humanrights.gov.au. Retrieved 4 September 2017, from
https://www.humanrights.gov.au/face-facts-cultural-diversity
Germov, J. (2014). Imagining health problems as social issues. In Second opinion: An
introduction to health sociology (5th ed.). (Chapter 1). South Melbourne: Oxford
University Press.
Giddens, A., Duneier, M., Appelbaum, R. P., & Carr, D. S. (2016). Introduction to sociology.
WW Norton.
Indigenous health (AIHW). (2017). Aihw.gov.au. Retrieved 4 September 2017, from
http://www.aihw.gov.au/australias-health/2014/indigenous-health/
Life expectancy (AIHW). (2017). Aihw.gov.au. Retrieved 4 September 2017, from
http://www.aihw.gov.au/deaths/life-expectancy/
Mitrou, F., Cooke, M., Lawrence, D., Povah, D., Mobilia, E., Guimond, E., & Zubrick, S. R.
(2014). Gaps in Indigenous disadvantage not closing: a census cohort study of social
determinants of health in Australia, Canada, and New Zealand from 1981–2006. BMC
Public Health, 14(1), 201.
Face the facts: Aboriginal and Torres Strait Islander Peoples | Australian Human Rights
Commission. (2017). Humanrights.gov.au. Retrieved 4 September 2017, from
https://www.humanrights.gov.au/education/face-facts/face-facts-aboriginal-and-torres-
strait-islander-peoples
Face the facts: Cultural Diversity | Australian Human Rights Commission.
(2017). Humanrights.gov.au. Retrieved 4 September 2017, from
https://www.humanrights.gov.au/face-facts-cultural-diversity
Germov, J. (2014). Imagining health problems as social issues. In Second opinion: An
introduction to health sociology (5th ed.). (Chapter 1). South Melbourne: Oxford
University Press.
Giddens, A., Duneier, M., Appelbaum, R. P., & Carr, D. S. (2016). Introduction to sociology.
WW Norton.
Indigenous health (AIHW). (2017). Aihw.gov.au. Retrieved 4 September 2017, from
http://www.aihw.gov.au/australias-health/2014/indigenous-health/
Life expectancy (AIHW). (2017). Aihw.gov.au. Retrieved 4 September 2017, from
http://www.aihw.gov.au/deaths/life-expectancy/
Mitrou, F., Cooke, M., Lawrence, D., Povah, D., Mobilia, E., Guimond, E., & Zubrick, S. R.
(2014). Gaps in Indigenous disadvantage not closing: a census cohort study of social
determinants of health in Australia, Canada, and New Zealand from 1981–2006. BMC
Public Health, 14(1), 201.
11NURSING ASSIGNMENT
Moorcroft, H. (2016). Paradigms, paradoxes and a propitious niche: conservation and Indigenous
social justice policy in Australia. Local Environment, 21(5), 591-614.
Wasti, S. P. (2011). In what way do Nepalese cultural factors affect adherence to antiretroviral
treatment in Nepal?. Health Science Journal.
Moorcroft, H. (2016). Paradigms, paradoxes and a propitious niche: conservation and Indigenous
social justice policy in Australia. Local Environment, 21(5), 591-614.
Wasti, S. P. (2011). In what way do Nepalese cultural factors affect adherence to antiretroviral
treatment in Nepal?. Health Science Journal.
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.