Jacksonville State University ANP DNP Program H&P Note: Abdominal Pain
VerifiedAdded on 2022/09/28
|4
|1087
|21
Homework Assignment
AI Summary
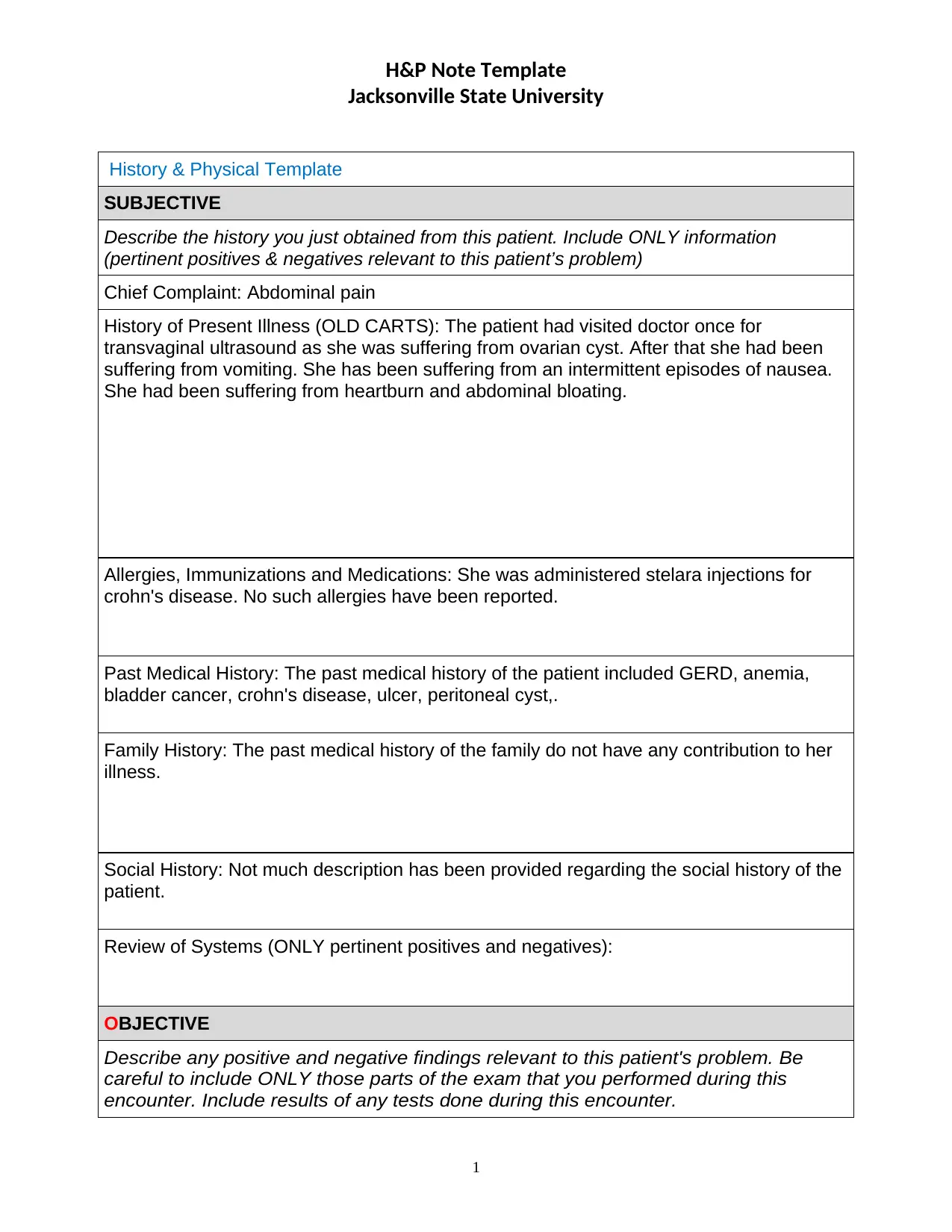
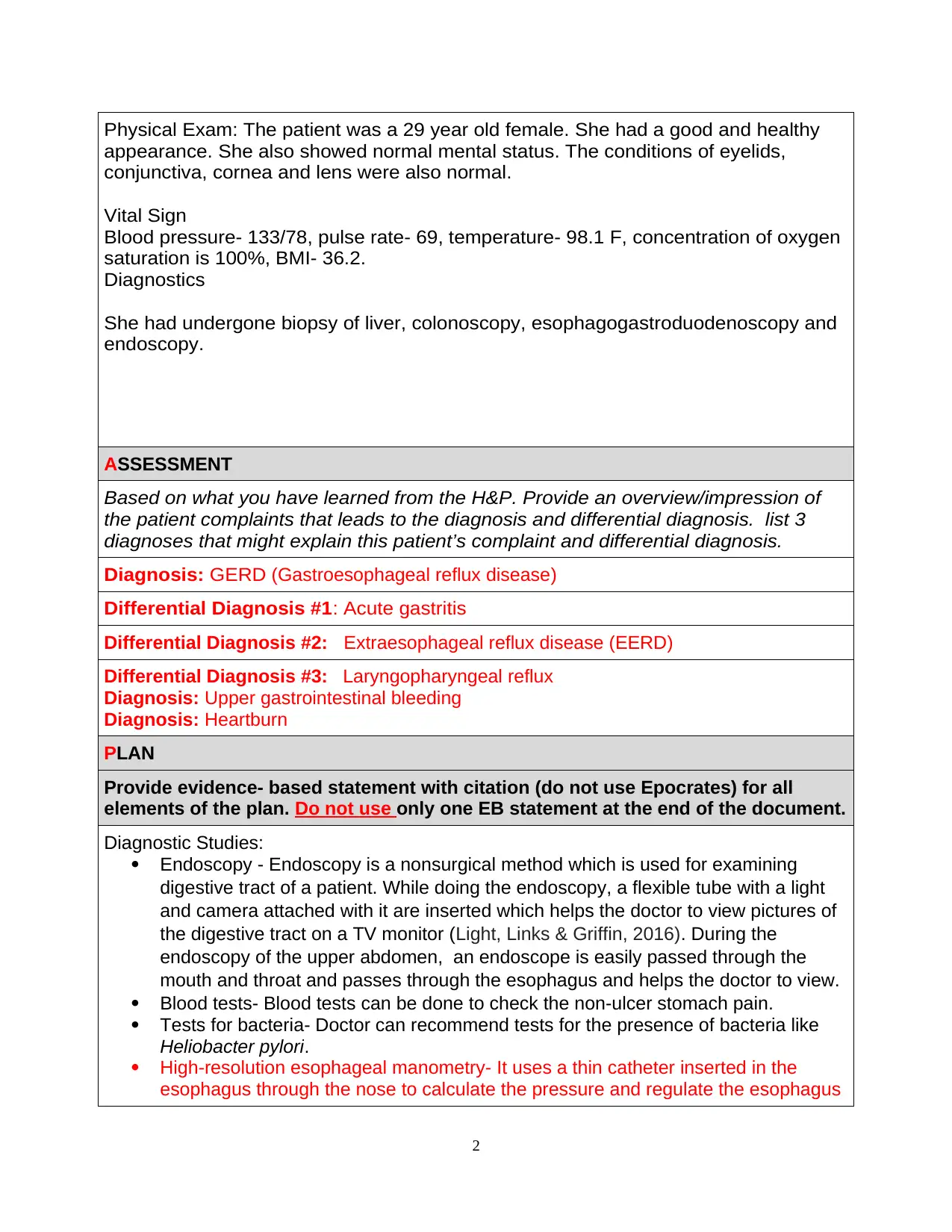
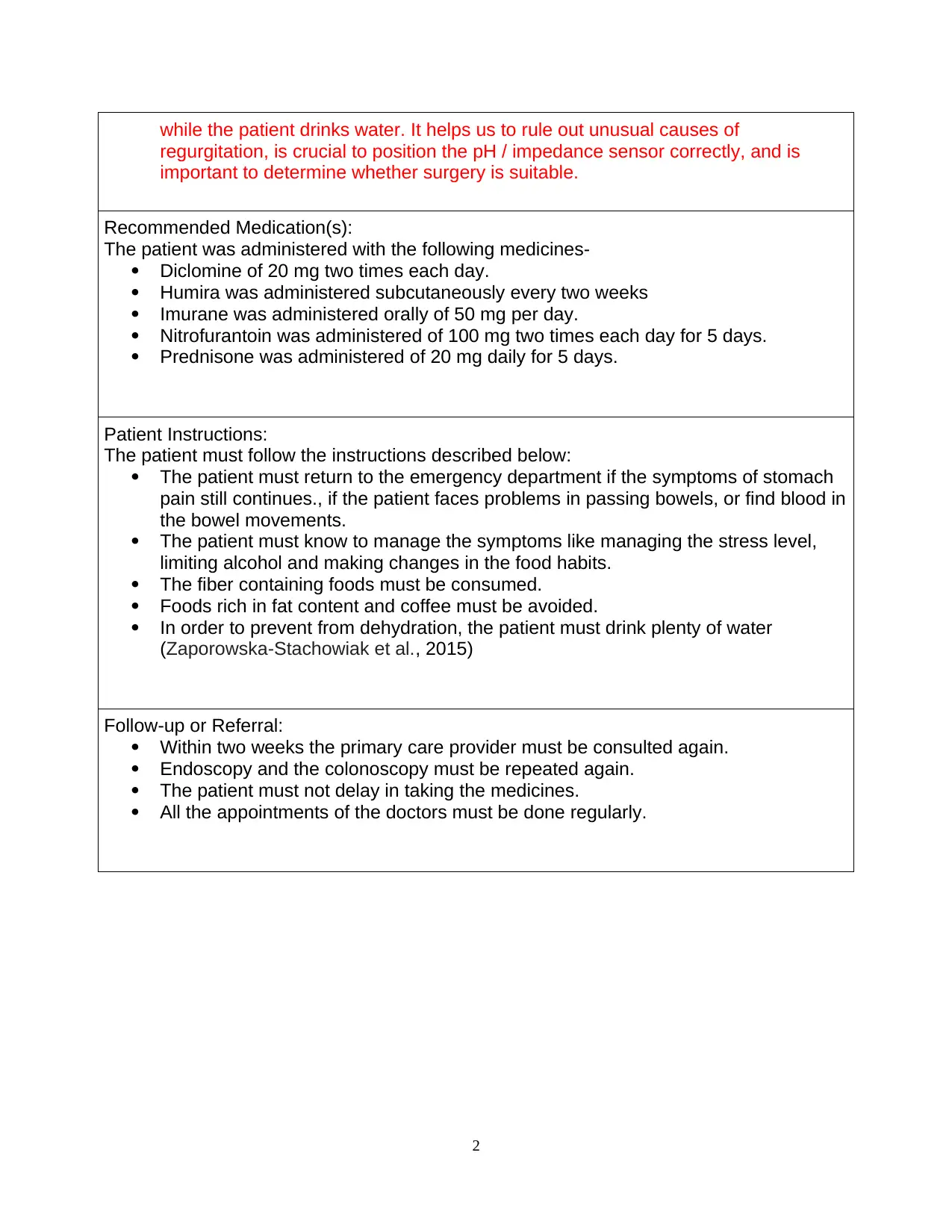
This document presents a detailed H&P (History and Physical) note for a 29-year-old female patient experiencing abdominal pain. The subjective section details the patient's history, including chief complaints, history of present illness (OLD CARTS), allergies, medications, past medical history (GERD, Crohn's disease, etc.), and review of systems. The objective section outlines the physical exam findings, including vital signs and diagnostic results from procedures like endoscopy and blood tests. The assessment provides a diagnosis of GERD, along with differential diagnoses such as acute gastritis, and EERD, and upper gastrointestinal bleeding. The plan section includes evidence-based statements with citations for diagnostic studies (endoscopy, blood tests) and recommended medications (Diclomine, Humira, Imurane, Nitrofurantoin, Prednisone). It also provides patient instructions and follow-up recommendations. The assignment is a comprehensive analysis of a patient case, demonstrating the student's understanding of diagnosis, treatment, and patient management.
1 out of 4
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.