HNN108: Research Evidence Annotation and Clinical Nursing Practice
VerifiedAdded on 2023/06/09
|16
|3417
|365
Report
AI Summary
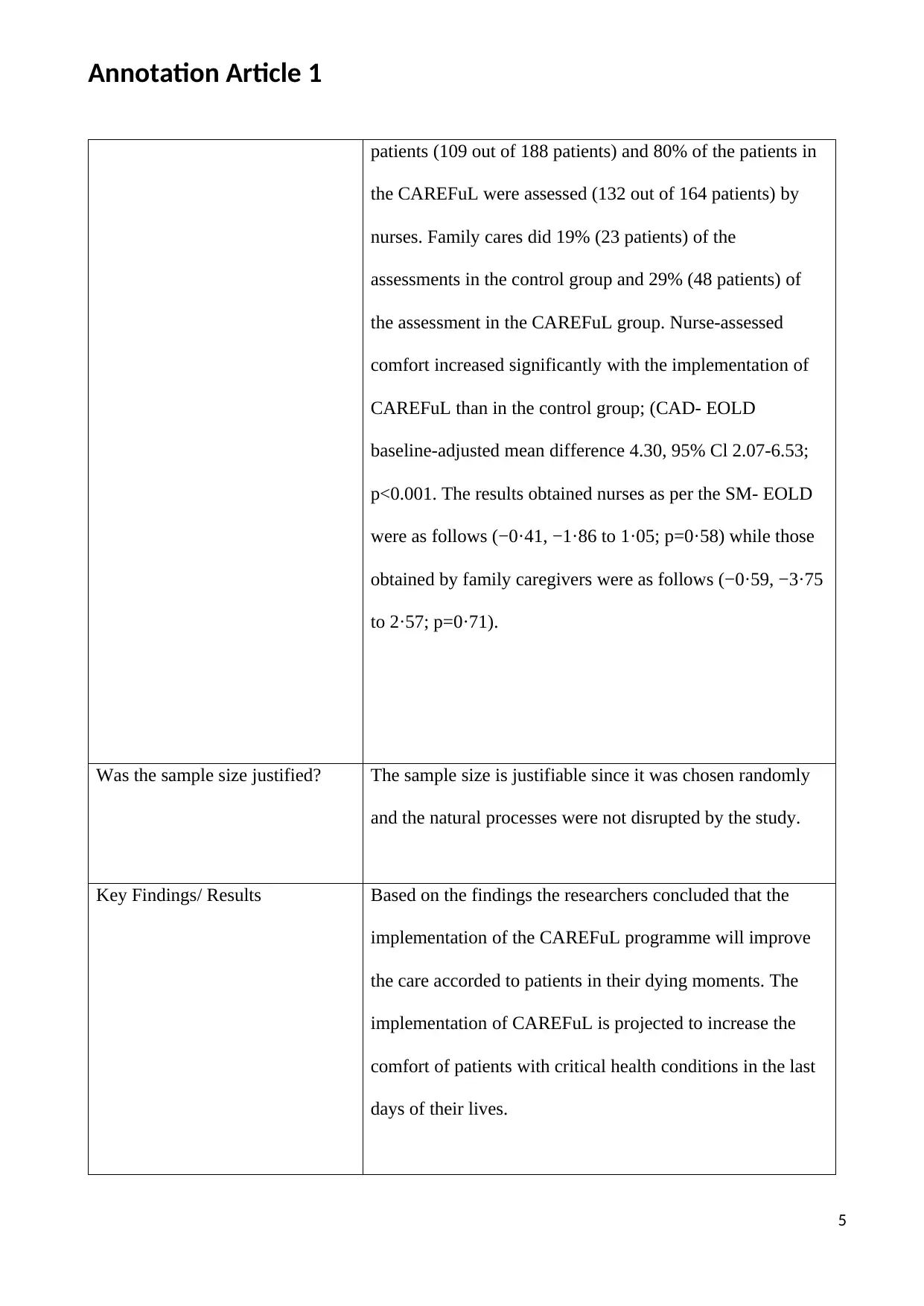
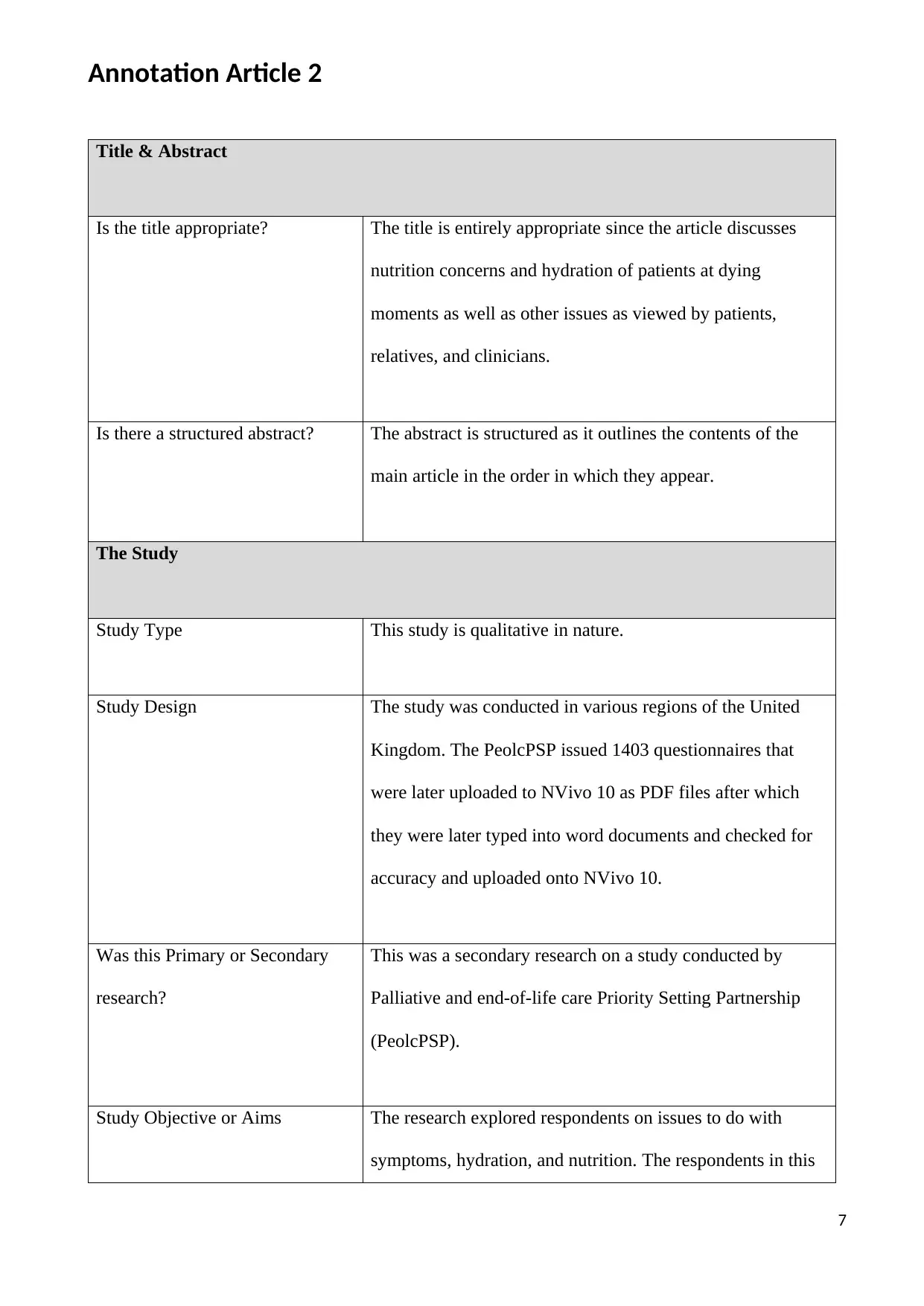
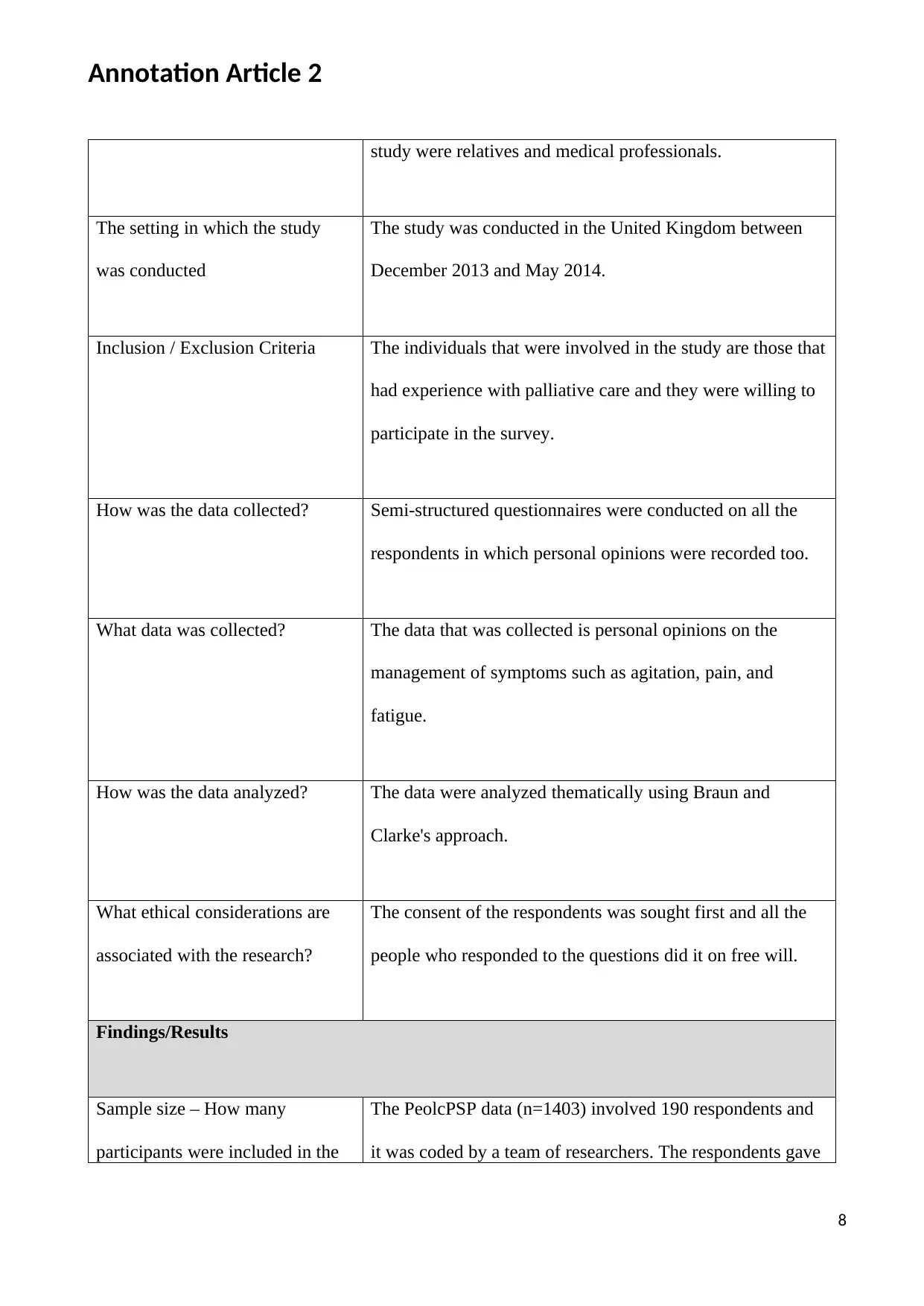
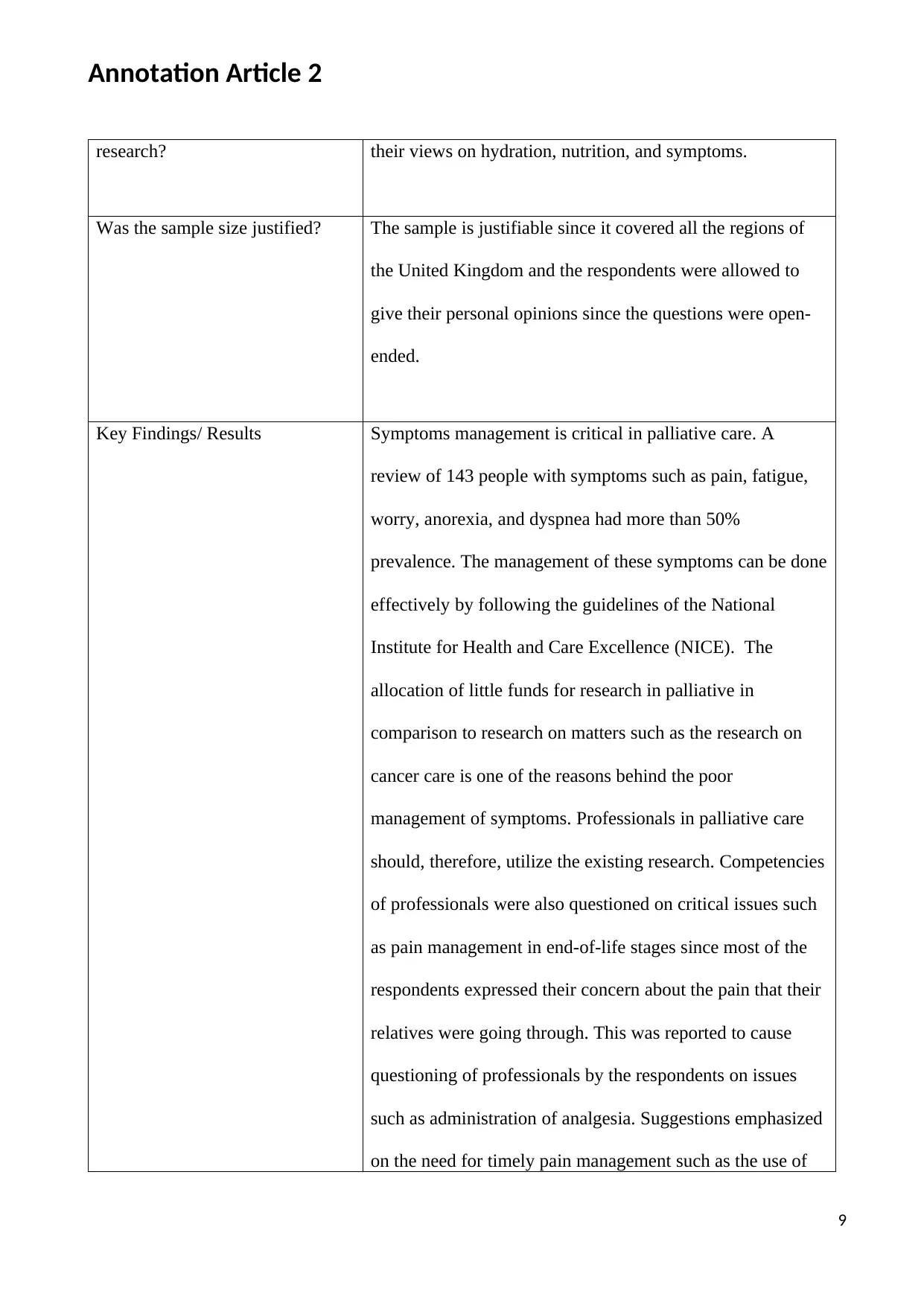
This report analyzes two peer-reviewed articles concerning symptom management in palliative and end-of-life care. The first article focuses on the CAREFuL program, a comprehensive intervention implemented in Belgian hospitals to improve the comfort of dying patients in geriatric wards. It employed a quantitative approach, comparing intervention and control groups to assess the program's impact on patient comfort, as measured by nurse and family caregiver assessments. The second article explores patient, relative, and clinician perspectives on symptom management in the UK, utilizing a qualitative study design with semi-structured questionnaires to gather data on issues like nutrition, hydration, and pain. The findings highlight the importance of effective symptom management, the need for more research, and the role of communication and the care environment in enhancing patient comfort. The report emphasizes the need for improved symptom management, the role of research and clinical guidelines, and the importance of patient-centered care in palliative settings. The report summarizes the research methodology, findings, and implications for nursing practice, including the application of evidence-based interventions to improve patient outcomes and reduce distress.

1 out of 16
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.