International Journal of Social Psychiatry Impact Factor
VerifiedAdded on 2022/09/07
|8
|7638
|19
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
International Journal of
Social Psychiatry
2016, Vol. 62(2) 133 –140
© The Author(s) 2015
Reprints and permissions:
sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/0020764015607550
isp.sagepub.com
E CAMDEN SCHIZOPH
Introduction
Cross-cultural comparison tests the boundaries of
knowledge and stretches methodological parameters,
highlights important similarities and differences and
promotes institutional and intercultural exchange and
understanding (Matsumoto & Van de Vijver, 2011). This
article looks at these matters in relation to the concept
The social and community opportunities
profile social inclusion measure: Structural
equivalence and differential item
functioning in community mental
health residents in Hong Kong
and the United Kingdom
Peter John Huxley1, Kara Chan2, Marcus Chiu3, Yanni Ma2,
Sarah Gaze4 and Sherrill Evans5
Abstract
Introduction: China’s future major health problem will be the management of chronic diseases – of which
health is a major one. An instrument is needed to measure mental health inclusion outcomes for mental he
in Hong Kong and mainland China as they strive to promote a more inclusive society for their citizens and
disadvantaged groups.
Aim: To report on the analysis of structural equivalence and item differentiation in two mentally unhealthy
healthy sample in the United Kingdom and Hong Kong.
Method: The mental health sample in Hong Kong was made up of non-governmental organisation (NGO) r
meeting the selection/exclusion criteria (being well enough to be interviewed, having a formal psychiatric d
living in the community). A similar sample in the United Kingdom meeting the same selection criteria was o
a community mental health organisation, equivalent to the NGOs in Hong Kong. Exploratory factor analysis
regression were conducted.
Results: The single-variable, self-rated ‘overall social inclusion’ differs significantly between all of the sam
we would expect from previous research, with the healthy population feeling more included than the seriou
illness (SMI) groups. In the exploratory factor analysis, the first two factors explain between a third and hal
variance, and the single variable which enters into all the analyses in the first factor is having friends to vis
the regression models were significant; however, in Hong Kong sample, only one-fifth of the total variance
Conclusion: The structural findings imply that the social and community opportunities profile–Chin
(SCOPE-C) gives similar results when applied to another culture. As only one-fifth of the variance of ‘overal
was explained in the Hong Kong sample, it may be that the instrument needs to be refined using different
items within the structural domains of inclusion.
Keywords
Severe mental illness, social exclusion, health assessment, social policy
1 Centre for Mental Health and Society, School of Social Sciences,
Bangor University, Bangor, Wales
2 School of Communication, Hong Kong Baptist University, Kowloon
Tong, Hong Kong
3 Department of Social Work, Faculty of Arts & Social Sciences,
National University of Singapore, Singapore
607550 ISP0010.1177/0020764015607550International Journal of Social Psychiatry Huxley et al.
research-article 2015
Original Article
4 School of Medicine, Swansea University, Swansea, Wales
5Independent Consultant, Pembrokeshire, Wales
Corresponding author:
Peter John Huxley, Centre for Mental Health and Society, School of Soc
Sciences, Bangor University, College Road, Bangor, Wales LL57 2DG.
Email: P.Huxley@bangor.ac.uk
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
Social Psychiatry
2016, Vol. 62(2) 133 –140
© The Author(s) 2015
Reprints and permissions:
sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/0020764015607550
isp.sagepub.com
E CAMDEN SCHIZOPH
Introduction
Cross-cultural comparison tests the boundaries of
knowledge and stretches methodological parameters,
highlights important similarities and differences and
promotes institutional and intercultural exchange and
understanding (Matsumoto & Van de Vijver, 2011). This
article looks at these matters in relation to the concept
The social and community opportunities
profile social inclusion measure: Structural
equivalence and differential item
functioning in community mental
health residents in Hong Kong
and the United Kingdom
Peter John Huxley1, Kara Chan2, Marcus Chiu3, Yanni Ma2,
Sarah Gaze4 and Sherrill Evans5
Abstract
Introduction: China’s future major health problem will be the management of chronic diseases – of which
health is a major one. An instrument is needed to measure mental health inclusion outcomes for mental he
in Hong Kong and mainland China as they strive to promote a more inclusive society for their citizens and
disadvantaged groups.
Aim: To report on the analysis of structural equivalence and item differentiation in two mentally unhealthy
healthy sample in the United Kingdom and Hong Kong.
Method: The mental health sample in Hong Kong was made up of non-governmental organisation (NGO) r
meeting the selection/exclusion criteria (being well enough to be interviewed, having a formal psychiatric d
living in the community). A similar sample in the United Kingdom meeting the same selection criteria was o
a community mental health organisation, equivalent to the NGOs in Hong Kong. Exploratory factor analysis
regression were conducted.
Results: The single-variable, self-rated ‘overall social inclusion’ differs significantly between all of the sam
we would expect from previous research, with the healthy population feeling more included than the seriou
illness (SMI) groups. In the exploratory factor analysis, the first two factors explain between a third and hal
variance, and the single variable which enters into all the analyses in the first factor is having friends to vis
the regression models were significant; however, in Hong Kong sample, only one-fifth of the total variance
Conclusion: The structural findings imply that the social and community opportunities profile–Chin
(SCOPE-C) gives similar results when applied to another culture. As only one-fifth of the variance of ‘overal
was explained in the Hong Kong sample, it may be that the instrument needs to be refined using different
items within the structural domains of inclusion.
Keywords
Severe mental illness, social exclusion, health assessment, social policy
1 Centre for Mental Health and Society, School of Social Sciences,
Bangor University, Bangor, Wales
2 School of Communication, Hong Kong Baptist University, Kowloon
Tong, Hong Kong
3 Department of Social Work, Faculty of Arts & Social Sciences,
National University of Singapore, Singapore
607550 ISP0010.1177/0020764015607550International Journal of Social Psychiatry Huxley et al.
research-article 2015
Original Article
4 School of Medicine, Swansea University, Swansea, Wales
5Independent Consultant, Pembrokeshire, Wales
Corresponding author:
Peter John Huxley, Centre for Mental Health and Society, School of Soc
Sciences, Bangor University, College Road, Bangor, Wales LL57 2DG.
Email: P.Huxley@bangor.ac.uk
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

134 International Journal of Social Psychiatry 62(2)
of social inclusion in the United Kingdom and Hong
Kong (HK).
A considerable amount of the literature about social
inclusion is actually about social exclusion (e.g. Leff &
Warner, 2006), and some treat social inclusion as if it is only
the converse of social exclusion (Wright & Stickley, 2013).
Repper and Perkins (2003) among others take the view that
social exclusion focuses on negatives and deficits, whereas
social inclusion is about affirmative action to address those
factors that lead to exclusion. In the United States, this
change in focus has taken place over the past 10 years
(Boushey, Fremstad, Gragg, & Waller, 2007). Social inclu-
sion has been defined in the European Union (EU) as
A process which ensures that those at risk of poverty and
social exclusion gain the opportunities and resources
necessary to participate fully in economic, social and cultural
life and to enjoy a standard of living and wellbeing that is
considered normal in the society in which they live. It ensures
that they have greater participation in decision-making which
affects their lives and access to their fundamental rights (as
defined in the Charter of Fundamental Rights of the EU).
(Council for the European Union, 2003)
The aim of the social inclusion policy in the EU is ‘to pre-
vent and eradicate poverty and exclusion and promote the
integration and participation of all into economic and
social life’ (Commission of the European Communities,
2000). In 2008, Mental Health Europe produced a descrip-
tive report from 27 member states (including Scotland and
Ireland, but not England or Wales) on the outcome of its
work programme on social inclusion for people with men-
tal health problems (Mental Health Europe, 2008)
Curran, Burchardt, Knapp, Mcdaid, and Li (2007) identi-
fied two broad schools of thought in the social inclusion lit-
erature. The first may be called a rights-based approach in
which social inclusion reflects the rights as a member or a
citizen of a particular group, community, society or country.
The second approach starts from the assumption that social
inclusion is the opportunity to participate in key functions or
activities of the society in question. This approach is a
development of the traditional concerns of social science
and especially social policy: measuring poverty and multi-
ple deprivation (Gordon, 2000; Townsend, 1979). Rights-
based conceptions of social inclusion may be particularly
important in the context of mental health, as a denial of
rights and/or access to the means to realise entitlements has
historically been a feature of the treatment of people with
mental illness. Conceptions of social inclusion based on par-
ticipation are also important, however, especially where
comparisons with the general population are sought.
Curran argues that social inclusion is widely agreed to
be
•• Relative to a given society (place and time);
•• Multidimensional (whether those dimensions are
conceived in terms of rights or key activities);
•• Dynamic (because inclusion is a process rather than
a state);
•• Mtilayered (in the sense that its causes operate at
individual, familial, communal, societal and even
global levels).
Cultural contexts
Hong Kong, officially known as Hong Kong Special
Administrative Region of the People’s Republic of China,
is a city state with a high degree of autonomy on the south-
ern coast of China at the Pearl River Estuary and the South
China Sea. HK has 7 million inhabitants over a land mass
of over 400 square miles. In all, 94% of the current popula-
tion of HK are ethnic Chinese. A major part of HK’s
Cantonese-speaking majority originated from the neigh-
bouring Canton province (now Guangdong), migrating to
HK during the 1960s. On the whole, HK psychiatry has
been fashioned close to the British model in terms of its
legal framework, guiding theoretical principles, diagnosis
and management of psychiatric disorders and types of ser-
vice delivery (Ungvari & Chiu, 2004). These aspects of
mental health have not changed since 1997, when HK
became a Special Administrative Region of China. From
its inception in 1967, when the first halfway house opened,
community-based residential rehabilitation has mainly
been the task of non-governmental organisation (NGO) in
collaboration with the Department of Social Welfare and
aided by the psychiatric services.
Over the last 10 years, there has been increasing activity
to improve the disability rights and well-being of the
Chinese population, and this has taken place against a very
gradual shift from collectivism to individualism
(Luhrmann, 2014; Steele & Lynch, 2013). Fisher and Jing
(2008) argue that despite strong statements on disability
rights in Chinese legislation since 1990, the independent
living policy falls short of the social inclusion goals
expected from such a policy commitment. They conclude
that minimum income support and the introduction of
social services are slowly addressing the social inclusion
of disabled people in China.
The World Bank has suggested that China’s major
health challenge for the future is the care and treatment of
people with non-communicable chronic physical and men-
tal diseases. In Toward a Healthy and Harmonious Life in
China (Wang, Marquez, & Langenbrunner, 2011), the
World Bank urged China to step up efforts to tackle its ris-
ing tide of non-communicable diseases (NCDs), warning
of not only the social but also the economic consequences
of inaction. NCDs are China’s number 1 health threat, con-
tributing to more than 80% of the country’s 10·3 million
annual deaths and nearly 70% of its total disease burden.
In HK, where social services are considered one of the
most well developed when compared to other parts of
China, the inclusion spirit has never been stronger. In
2011, the Community Investment and Inclusion Fund
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
of social inclusion in the United Kingdom and Hong
Kong (HK).
A considerable amount of the literature about social
inclusion is actually about social exclusion (e.g. Leff &
Warner, 2006), and some treat social inclusion as if it is only
the converse of social exclusion (Wright & Stickley, 2013).
Repper and Perkins (2003) among others take the view that
social exclusion focuses on negatives and deficits, whereas
social inclusion is about affirmative action to address those
factors that lead to exclusion. In the United States, this
change in focus has taken place over the past 10 years
(Boushey, Fremstad, Gragg, & Waller, 2007). Social inclu-
sion has been defined in the European Union (EU) as
A process which ensures that those at risk of poverty and
social exclusion gain the opportunities and resources
necessary to participate fully in economic, social and cultural
life and to enjoy a standard of living and wellbeing that is
considered normal in the society in which they live. It ensures
that they have greater participation in decision-making which
affects their lives and access to their fundamental rights (as
defined in the Charter of Fundamental Rights of the EU).
(Council for the European Union, 2003)
The aim of the social inclusion policy in the EU is ‘to pre-
vent and eradicate poverty and exclusion and promote the
integration and participation of all into economic and
social life’ (Commission of the European Communities,
2000). In 2008, Mental Health Europe produced a descrip-
tive report from 27 member states (including Scotland and
Ireland, but not England or Wales) on the outcome of its
work programme on social inclusion for people with men-
tal health problems (Mental Health Europe, 2008)
Curran, Burchardt, Knapp, Mcdaid, and Li (2007) identi-
fied two broad schools of thought in the social inclusion lit-
erature. The first may be called a rights-based approach in
which social inclusion reflects the rights as a member or a
citizen of a particular group, community, society or country.
The second approach starts from the assumption that social
inclusion is the opportunity to participate in key functions or
activities of the society in question. This approach is a
development of the traditional concerns of social science
and especially social policy: measuring poverty and multi-
ple deprivation (Gordon, 2000; Townsend, 1979). Rights-
based conceptions of social inclusion may be particularly
important in the context of mental health, as a denial of
rights and/or access to the means to realise entitlements has
historically been a feature of the treatment of people with
mental illness. Conceptions of social inclusion based on par-
ticipation are also important, however, especially where
comparisons with the general population are sought.
Curran argues that social inclusion is widely agreed to
be
•• Relative to a given society (place and time);
•• Multidimensional (whether those dimensions are
conceived in terms of rights or key activities);
•• Dynamic (because inclusion is a process rather than
a state);
•• Mtilayered (in the sense that its causes operate at
individual, familial, communal, societal and even
global levels).
Cultural contexts
Hong Kong, officially known as Hong Kong Special
Administrative Region of the People’s Republic of China,
is a city state with a high degree of autonomy on the south-
ern coast of China at the Pearl River Estuary and the South
China Sea. HK has 7 million inhabitants over a land mass
of over 400 square miles. In all, 94% of the current popula-
tion of HK are ethnic Chinese. A major part of HK’s
Cantonese-speaking majority originated from the neigh-
bouring Canton province (now Guangdong), migrating to
HK during the 1960s. On the whole, HK psychiatry has
been fashioned close to the British model in terms of its
legal framework, guiding theoretical principles, diagnosis
and management of psychiatric disorders and types of ser-
vice delivery (Ungvari & Chiu, 2004). These aspects of
mental health have not changed since 1997, when HK
became a Special Administrative Region of China. From
its inception in 1967, when the first halfway house opened,
community-based residential rehabilitation has mainly
been the task of non-governmental organisation (NGO) in
collaboration with the Department of Social Welfare and
aided by the psychiatric services.
Over the last 10 years, there has been increasing activity
to improve the disability rights and well-being of the
Chinese population, and this has taken place against a very
gradual shift from collectivism to individualism
(Luhrmann, 2014; Steele & Lynch, 2013). Fisher and Jing
(2008) argue that despite strong statements on disability
rights in Chinese legislation since 1990, the independent
living policy falls short of the social inclusion goals
expected from such a policy commitment. They conclude
that minimum income support and the introduction of
social services are slowly addressing the social inclusion
of disabled people in China.
The World Bank has suggested that China’s major
health challenge for the future is the care and treatment of
people with non-communicable chronic physical and men-
tal diseases. In Toward a Healthy and Harmonious Life in
China (Wang, Marquez, & Langenbrunner, 2011), the
World Bank urged China to step up efforts to tackle its ris-
ing tide of non-communicable diseases (NCDs), warning
of not only the social but also the economic consequences
of inaction. NCDs are China’s number 1 health threat, con-
tributing to more than 80% of the country’s 10·3 million
annual deaths and nearly 70% of its total disease burden.
In HK, where social services are considered one of the
most well developed when compared to other parts of
China, the inclusion spirit has never been stronger. In
2011, the Community Investment and Inclusion Fund
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from

Huxley et al. 135
funded projects to the tune of more than 30 million HK
dollars. Nevertheless, there is a lack of a valid measure to
evaluate the objective of improved social inclusion in HK.
Not only will developing a valid inclusion measure help to
augment the evidence base about the inclusion of ethnic
groups and disabled groups, but it may also be used to
demonstrate the inclusion efficacy of service programmes.
Such a development could have the great potential for pro-
gramme evaluation at local (HK) level and for extended
application to mainland China and other Chinese commu-
nities where inclusion/exclusion issues remain very chal-
lenging (Blaxland, Fisher, & Shang, 2015).
Cross-cultural measurement issues
Interest in cross-cultural measurement issues has grown
rapidly since the turn of the century. Although psycholo-
gists have taken the lead on measurement issues
(Matsumoto & Van de Vijver, 2011), social work research-
ers have recognised the importance of developing cross-
cultural measurement for the profession, especially for
work with minority and immigrant groups (Tran, 2009)
including marginalised Asian immigrants (Willgerodt,
Kataoka-Yahiro, Kim, & Ceria, 2005). Both professions
recognise the same bias and equivalence issues in cross-
cultural measurement (Matsumoto & Van de Vijver,
2011; Tran, 2009).
Issues of equivalence.There are many types of cross-cultural
research. Herdman, Fox-Rushby, and Badia (1998) listed 19
types; others have suggested that there are perhaps as many
as 50 (Johnson, Shavitt, & Holbrook, 2011). Most authors
agree on five or six fundamental ones: these include concep-
tual, item, semantic, operational, metric or measurement
unit, structural and functional equivalence (Berg, Jahnsen,
Holm, & Hussain, 2003; Herdman et al., 1998; Lee & Jung,
2006; Mahler, Jank, Reuschenbach, & Szecsenyi, 2009;
Matsumoto & Van de Vijver, 2011; Streiner & Norman,
2008; Tran, 2009; Van Widenfelt, Treffers, De Beurs, Siebe-
link, & Koudijs, 2005).
In essence, these look at whether the construct is con-
ceptualised in the same way in different cultures, whether
it consists of the same constituent elements and whether its
relation with other constructs is the same. Structure-
oriented studies (such as reported here) focus mainly on
the consistency of relationships among variables and
between measures in more than one culture. Fischer and
Fontaine (2011) distinguish four levels of equivalence:
functional, structural, metric and full score equivalence.
They define structural equivalence as ‘the same underly-
ing dimensions emerge and item responses are not trivially
related to these dimensions in each of the cultural groups’.
It has been suggested that there has been a misguided
pre-occupation with scales rather than the concepts being
scaled and too much reliance on unsubstantiated claims of
conceptual equivalence between them (Bowden & Fox-
Rushby, 2003). The same issue arises in relation to the
cross-cultural adaptation of health-related quality of life
(HRQOL) instruments (Cheung & Thumboo, 2006). The
approach we take to the question of conceptual equiva-
lence between cultures is universalist rather than absolutist
(Herdman et al., 1998). This approach does not make the
prior assumption that constructs will be the same across
cultures and, consequently, implies a need to establish
whether the concept exists and is interpreted similarly in
the two settings.
The development of social and community
opportunities profile–Chinese version
In previous work, we have reported on the conceptual
equivalence of the concept in the United Kingdom and in
HK (Chan, Evans, Ng, Chiu, & Huxley, 2014). A focus
group study involving concept mapping was conducted in
HK during September to October 2012. The objective of the
study was to investigate how the concepts of social inclu-
sion are understood by HK residents. Seven groups of 61
participants (38 females and 23 males) were interviewed,
including separate groups of non-professional workers at a
service centre, senior centre users, a mixed group of parents
as well as community residents, persons with severe mental
illness, professional social service providers, communica-
tion studies students and social work students. Six major
themes were identified by these groups: (1) material
resources and wealth, (2) work, (3) social (dis)harmony and
diversity, (4) discrimination, (5) communication and (6)
participation in activities. HK respondents gave more prom-
inence to issues of stigma and discrimination than UK
respondents, so further items were introduced into the social
and community opportunities profile–Chinese version
(SCOPE-C). Translation and back translation of the other
SCOPE domains were undertaken as per the research proto-
col. As a result, certain variables within domains were
replaced by HK-specific items and codes based upon the
HK population census questions and coding.
The SCOPE-C was then pilot tested for acceptability
and clarity among a group of professionals and NGO
patients. No further amendments were deemed necessary.
The SCOPE-C was then applied to the sample of NGO
patients at baseline and 2 weeks later to assess test–retest
reliability and then again after 6 months to assess change.
The main mental health sample in HK was made up of
NGO patients meeting the selection/exclusion criteria (see
section ‘Method’). A similar sample in the United Kingdom
meeting the same selection criteria was obtained from a
community mental health organisation, equivalent to the
NGOs in HK. In both samples, the main diagnosis was
psychosis, and individuals were still receiving psychiatric
services while resident in the community. The mental
health samples were collected contemporaneously in late
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
funded projects to the tune of more than 30 million HK
dollars. Nevertheless, there is a lack of a valid measure to
evaluate the objective of improved social inclusion in HK.
Not only will developing a valid inclusion measure help to
augment the evidence base about the inclusion of ethnic
groups and disabled groups, but it may also be used to
demonstrate the inclusion efficacy of service programmes.
Such a development could have the great potential for pro-
gramme evaluation at local (HK) level and for extended
application to mainland China and other Chinese commu-
nities where inclusion/exclusion issues remain very chal-
lenging (Blaxland, Fisher, & Shang, 2015).
Cross-cultural measurement issues
Interest in cross-cultural measurement issues has grown
rapidly since the turn of the century. Although psycholo-
gists have taken the lead on measurement issues
(Matsumoto & Van de Vijver, 2011), social work research-
ers have recognised the importance of developing cross-
cultural measurement for the profession, especially for
work with minority and immigrant groups (Tran, 2009)
including marginalised Asian immigrants (Willgerodt,
Kataoka-Yahiro, Kim, & Ceria, 2005). Both professions
recognise the same bias and equivalence issues in cross-
cultural measurement (Matsumoto & Van de Vijver,
2011; Tran, 2009).
Issues of equivalence.There are many types of cross-cultural
research. Herdman, Fox-Rushby, and Badia (1998) listed 19
types; others have suggested that there are perhaps as many
as 50 (Johnson, Shavitt, & Holbrook, 2011). Most authors
agree on five or six fundamental ones: these include concep-
tual, item, semantic, operational, metric or measurement
unit, structural and functional equivalence (Berg, Jahnsen,
Holm, & Hussain, 2003; Herdman et al., 1998; Lee & Jung,
2006; Mahler, Jank, Reuschenbach, & Szecsenyi, 2009;
Matsumoto & Van de Vijver, 2011; Streiner & Norman,
2008; Tran, 2009; Van Widenfelt, Treffers, De Beurs, Siebe-
link, & Koudijs, 2005).
In essence, these look at whether the construct is con-
ceptualised in the same way in different cultures, whether
it consists of the same constituent elements and whether its
relation with other constructs is the same. Structure-
oriented studies (such as reported here) focus mainly on
the consistency of relationships among variables and
between measures in more than one culture. Fischer and
Fontaine (2011) distinguish four levels of equivalence:
functional, structural, metric and full score equivalence.
They define structural equivalence as ‘the same underly-
ing dimensions emerge and item responses are not trivially
related to these dimensions in each of the cultural groups’.
It has been suggested that there has been a misguided
pre-occupation with scales rather than the concepts being
scaled and too much reliance on unsubstantiated claims of
conceptual equivalence between them (Bowden & Fox-
Rushby, 2003). The same issue arises in relation to the
cross-cultural adaptation of health-related quality of life
(HRQOL) instruments (Cheung & Thumboo, 2006). The
approach we take to the question of conceptual equiva-
lence between cultures is universalist rather than absolutist
(Herdman et al., 1998). This approach does not make the
prior assumption that constructs will be the same across
cultures and, consequently, implies a need to establish
whether the concept exists and is interpreted similarly in
the two settings.
The development of social and community
opportunities profile–Chinese version
In previous work, we have reported on the conceptual
equivalence of the concept in the United Kingdom and in
HK (Chan, Evans, Ng, Chiu, & Huxley, 2014). A focus
group study involving concept mapping was conducted in
HK during September to October 2012. The objective of the
study was to investigate how the concepts of social inclu-
sion are understood by HK residents. Seven groups of 61
participants (38 females and 23 males) were interviewed,
including separate groups of non-professional workers at a
service centre, senior centre users, a mixed group of parents
as well as community residents, persons with severe mental
illness, professional social service providers, communica-
tion studies students and social work students. Six major
themes were identified by these groups: (1) material
resources and wealth, (2) work, (3) social (dis)harmony and
diversity, (4) discrimination, (5) communication and (6)
participation in activities. HK respondents gave more prom-
inence to issues of stigma and discrimination than UK
respondents, so further items were introduced into the social
and community opportunities profile–Chinese version
(SCOPE-C). Translation and back translation of the other
SCOPE domains were undertaken as per the research proto-
col. As a result, certain variables within domains were
replaced by HK-specific items and codes based upon the
HK population census questions and coding.
The SCOPE-C was then pilot tested for acceptability
and clarity among a group of professionals and NGO
patients. No further amendments were deemed necessary.
The SCOPE-C was then applied to the sample of NGO
patients at baseline and 2 weeks later to assess test–retest
reliability and then again after 6 months to assess change.
The main mental health sample in HK was made up of
NGO patients meeting the selection/exclusion criteria (see
section ‘Method’). A similar sample in the United Kingdom
meeting the same selection criteria was obtained from a
community mental health organisation, equivalent to the
NGOs in HK. In both samples, the main diagnosis was
psychosis, and individuals were still receiving psychiatric
services while resident in the community. The mental
health samples were collected contemporaneously in late
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from

136 International Journal of Social Psychiatry 62(2)
2013 and early 2014. Previous papers (Chan, Chiu, Evans,
Huxley, & Ng, 2015; Chan, Evans, Chiu, Huxley, & Ng,
2014; Chan et al., 2014; Chan, Huxley, Chiu, Evans, &
Ma, 2015) have reported on the development of the instru-
ment and aspects of validity and reliability:
•• The similarities and shared understanding of the
model of social inclusion in focus group samples in
the United Kingdom and HK;
•• The high reliability and validity of the SCOPE-C in
the HK sample;
•• The relationship between health and the experience
of discrimination and inclusion in the HK sample.
Present study aims
The aim of this article is to report on the analysis of struc-
tural equivalence and item differentiation in two mentally
unhealthy samples and one healthy sample.
Method
Samples
The main SCOPE-C mental health sample in HK was
made up of NGO patients meeting the selection/exclusion
criteria (being well enough to be interviewed, having a for-
mal psychiatric diagnosis and living in the community
under NGO supervision). A similar sample in the United
Kingdom meeting the same selection criteria was obtained
from a community mental health organisation, equivalent
to the NGOs in HK. In both samples, the main diagnosis
was psychosis, and individuals were still receiving psychi-
atric services while resident in the community. The main
healthy population sample in the United Kingdom was col-
lected from SCOPE interviews with individuals in a repre-
sentative sample of households across the United Kingdom
collected in 2011 (Huxley et al., 2011).
Analysis
For an understanding of structural equivalence, exploratory
factor analysis has been advocated and principal components
analysis proposed as a data reduction technique. Using
Procrustean rotation (Fischer & Fontaine, 2011), the factor
structure can be rotated towards the theoretically expected
structure. It is an alternative to confirmatory factor analysis
(CFA) in complex data sets.
Differential item functioning (DIF; item bias) can be
assessed using analysis of variance (Van de Vijver &
Leung, 2011) or logistic regression. These two statistical
techniques were applied to the data.
Results
Comparison of samples
While the age and gender items could represent sampling
bias, the other variables could also be seen as representing
cultural differences (Table 1).
‘Overall social inclusion’ (OSI) results
The following analysis compares the three samples in
terms of their response to a single overall inclusion ques-
tion: ‘ overall, how do you feel about the extent to which
you are included in society?’ We have reported the analysis
of variance result, but the Kruskal–Wallis test gave the
same result (Table 2).
From this analysis, we are able to say that overall social
inclusion (OSI) differs significantly between all of the
samples, in the way we would expect from previous
research, with the healthy population feeling more included
than the SMI groups.
Structural equivalence: factor analysis results
Next, we look at the structural equivalence using factor analy-
sis, the rotated factor patterns in each sample and the item
loadings. Many of the variables included in Tables 3–5
are either of the form ‘how satisfied are you with your partici-
pation/engagement in’ (e.g. opportunities to enhance your
income (Satisfaction with opportuntities (SO) income)) or per-
ception of the range of opportunities available in the area (e.g.
to find suitable work (Perceived opportunities (PO) work)).
Identical variables were entered into all three analyses.
Table 1. Baseline socio-demographic variables for individuals in the three populations (UK mentally ill sample (UK SMI),
Kong mentally ill sample (HK SMI) and UK general population).
UK SMI
(n = 43)
HK SMI
(n = 168)
UK general
population
(n = 212)
Chi-squared
(df)
p
Age: proportion under 50 years 48% 59% 41% 12.71 (2) .002
Gender: (%) female 56% 52% 57.5% 1.03 (2) NS
Long-term limiting illness or disability: (%) yes91.7% 49.4% 32.7% 50.16 (2) <.001
In any form of work: % yes 9% 60% 91% 137.75 (2) <.001
Car ownership: % yes 14% 0% 86% 191.64 (2) <.001
SMI: serious mental illness; HK: Hong Kong; df: degrees of freedom.
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
2013 and early 2014. Previous papers (Chan, Chiu, Evans,
Huxley, & Ng, 2015; Chan, Evans, Chiu, Huxley, & Ng,
2014; Chan et al., 2014; Chan, Huxley, Chiu, Evans, &
Ma, 2015) have reported on the development of the instru-
ment and aspects of validity and reliability:
•• The similarities and shared understanding of the
model of social inclusion in focus group samples in
the United Kingdom and HK;
•• The high reliability and validity of the SCOPE-C in
the HK sample;
•• The relationship between health and the experience
of discrimination and inclusion in the HK sample.
Present study aims
The aim of this article is to report on the analysis of struc-
tural equivalence and item differentiation in two mentally
unhealthy samples and one healthy sample.
Method
Samples
The main SCOPE-C mental health sample in HK was
made up of NGO patients meeting the selection/exclusion
criteria (being well enough to be interviewed, having a for-
mal psychiatric diagnosis and living in the community
under NGO supervision). A similar sample in the United
Kingdom meeting the same selection criteria was obtained
from a community mental health organisation, equivalent
to the NGOs in HK. In both samples, the main diagnosis
was psychosis, and individuals were still receiving psychi-
atric services while resident in the community. The main
healthy population sample in the United Kingdom was col-
lected from SCOPE interviews with individuals in a repre-
sentative sample of households across the United Kingdom
collected in 2011 (Huxley et al., 2011).
Analysis
For an understanding of structural equivalence, exploratory
factor analysis has been advocated and principal components
analysis proposed as a data reduction technique. Using
Procrustean rotation (Fischer & Fontaine, 2011), the factor
structure can be rotated towards the theoretically expected
structure. It is an alternative to confirmatory factor analysis
(CFA) in complex data sets.
Differential item functioning (DIF; item bias) can be
assessed using analysis of variance (Van de Vijver &
Leung, 2011) or logistic regression. These two statistical
techniques were applied to the data.
Results
Comparison of samples
While the age and gender items could represent sampling
bias, the other variables could also be seen as representing
cultural differences (Table 1).
‘Overall social inclusion’ (OSI) results
The following analysis compares the three samples in
terms of their response to a single overall inclusion ques-
tion: ‘ overall, how do you feel about the extent to which
you are included in society?’ We have reported the analysis
of variance result, but the Kruskal–Wallis test gave the
same result (Table 2).
From this analysis, we are able to say that overall social
inclusion (OSI) differs significantly between all of the
samples, in the way we would expect from previous
research, with the healthy population feeling more included
than the SMI groups.
Structural equivalence: factor analysis results
Next, we look at the structural equivalence using factor analy-
sis, the rotated factor patterns in each sample and the item
loadings. Many of the variables included in Tables 3–5
are either of the form ‘how satisfied are you with your partici-
pation/engagement in’ (e.g. opportunities to enhance your
income (Satisfaction with opportuntities (SO) income)) or per-
ception of the range of opportunities available in the area (e.g.
to find suitable work (Perceived opportunities (PO) work)).
Identical variables were entered into all three analyses.
Table 1. Baseline socio-demographic variables for individuals in the three populations (UK mentally ill sample (UK SMI),
Kong mentally ill sample (HK SMI) and UK general population).
UK SMI
(n = 43)
HK SMI
(n = 168)
UK general
population
(n = 212)
Chi-squared
(df)
p
Age: proportion under 50 years 48% 59% 41% 12.71 (2) .002
Gender: (%) female 56% 52% 57.5% 1.03 (2) NS
Long-term limiting illness or disability: (%) yes91.7% 49.4% 32.7% 50.16 (2) <.001
In any form of work: % yes 9% 60% 91% 137.75 (2) <.001
Car ownership: % yes 14% 0% 86% 191.64 (2) <.001
SMI: serious mental illness; HK: Hong Kong; df: degrees of freedom.
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Huxley et al. 137
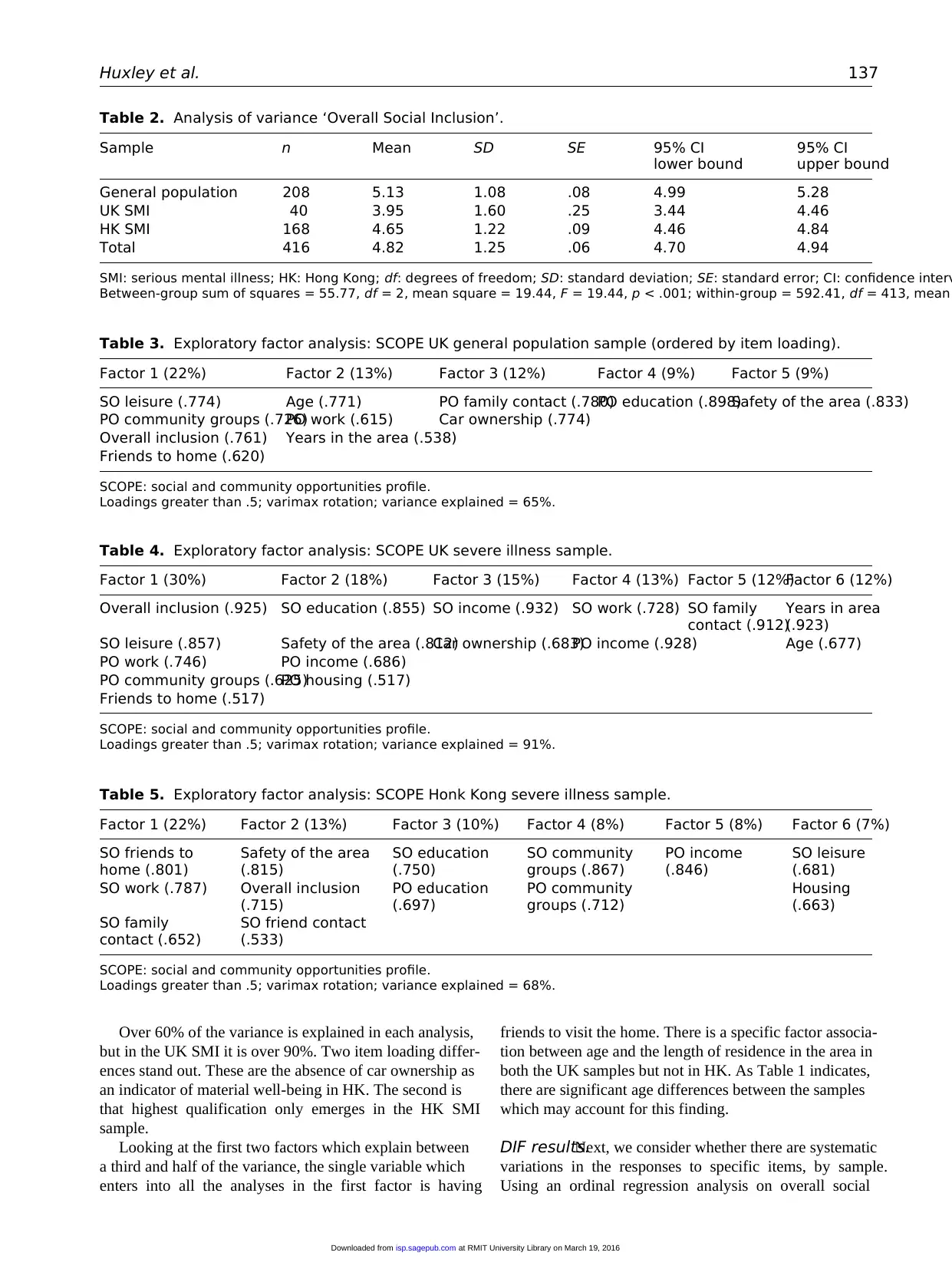
Over 60% of the variance is explained in each analysis,
but in the UK SMI it is over 90%. Two item loading differ-
ences stand out. These are the absence of car ownership as
an indicator of material well-being in HK. The second is
that highest qualification only emerges in the HK SMI
sample.
Looking at the first two factors which explain between
a third and half of the variance, the single variable which
enters into all the analyses in the first factor is having
friends to visit the home. There is a specific factor associa-
tion between age and the length of residence in the area in
both the UK samples but not in HK. As Table 1 indicates,
there are significant age differences between the samples
which may account for this finding.
DIF results.Next, we consider whether there are systematic
variations in the responses to specific items, by sample.
Using an ordinal regression analysis on overall social
Table 2. Analysis of variance ‘Overall Social Inclusion’.
Sample n Mean SD SE 95% CI
lower bound
95% CI
upper bound
General population 208 5.13 1.08 .08 4.99 5.28
UK SMI 40 3.95 1.60 .25 3.44 4.46
HK SMI 168 4.65 1.22 .09 4.46 4.84
Total 416 4.82 1.25 .06 4.70 4.94
SMI: serious mental illness; HK: Hong Kong; df: degrees of freedom; SD: standard deviation; SE: standard error; CI: confidence interv
Between-group sum of squares = 55.77, df = 2, mean square = 19.44, F = 19.44, p < .001; within-group = 592.41, df = 413, mean
Table 3. Exploratory factor analysis: SCOPE UK general population sample (ordered by item loading).
Factor 1 (22%) Factor 2 (13%) Factor 3 (12%) Factor 4 (9%) Factor 5 (9%)
SO leisure (.774) Age (.771) PO family contact (.780)PO education (.898)Safety of the area (.833)
PO community groups (.726)PO work (.615) Car ownership (.774)
Overall inclusion (.761) Years in the area (.538)
Friends to home (.620)
SCOPE: social and community opportunities profile.
Loadings greater than .5; varimax rotation; variance explained = 65%.
Table 4. Exploratory factor analysis: SCOPE UK severe illness sample.
Factor 1 (30%) Factor 2 (18%) Factor 3 (15%) Factor 4 (13%) Factor 5 (12%)Factor 6 (12%)
Overall inclusion (.925) SO education (.855) SO income (.932) SO work (.728) SO family
contact (.912)
Years in area
(.923)
SO leisure (.857) Safety of the area (.812)Car ownership (.683)PO income (.928) Age (.677)
PO work (.746) PO income (.686)
PO community groups (.625)PO housing (.517)
Friends to home (.517)
SCOPE: social and community opportunities profile.
Loadings greater than .5; varimax rotation; variance explained = 91%.
Table 5. Exploratory factor analysis: SCOPE Honk Kong severe illness sample.
Factor 1 (22%) Factor 2 (13%) Factor 3 (10%) Factor 4 (8%) Factor 5 (8%) Factor 6 (7%)
SO friends to
home (.801)
Safety of the area
(.815)
SO education
(.750)
SO community
groups (.867)
PO income
(.846)
SO leisure
(.681)
SO work (.787) Overall inclusion
(.715)
PO education
(.697)
PO community
groups (.712)
Housing
(.663)
SO family
contact (.652)
SO friend contact
(.533)
SCOPE: social and community opportunities profile.
Loadings greater than .5; varimax rotation; variance explained = 68%.
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
Over 60% of the variance is explained in each analysis,
but in the UK SMI it is over 90%. Two item loading differ-
ences stand out. These are the absence of car ownership as
an indicator of material well-being in HK. The second is
that highest qualification only emerges in the HK SMI
sample.
Looking at the first two factors which explain between
a third and half of the variance, the single variable which
enters into all the analyses in the first factor is having
friends to visit the home. There is a specific factor associa-
tion between age and the length of residence in the area in
both the UK samples but not in HK. As Table 1 indicates,
there are significant age differences between the samples
which may account for this finding.
DIF results.Next, we consider whether there are systematic
variations in the responses to specific items, by sample.
Using an ordinal regression analysis on overall social
Table 2. Analysis of variance ‘Overall Social Inclusion’.
Sample n Mean SD SE 95% CI
lower bound
95% CI
upper bound
General population 208 5.13 1.08 .08 4.99 5.28
UK SMI 40 3.95 1.60 .25 3.44 4.46
HK SMI 168 4.65 1.22 .09 4.46 4.84
Total 416 4.82 1.25 .06 4.70 4.94
SMI: serious mental illness; HK: Hong Kong; df: degrees of freedom; SD: standard deviation; SE: standard error; CI: confidence interv
Between-group sum of squares = 55.77, df = 2, mean square = 19.44, F = 19.44, p < .001; within-group = 592.41, df = 413, mean
Table 3. Exploratory factor analysis: SCOPE UK general population sample (ordered by item loading).
Factor 1 (22%) Factor 2 (13%) Factor 3 (12%) Factor 4 (9%) Factor 5 (9%)
SO leisure (.774) Age (.771) PO family contact (.780)PO education (.898)Safety of the area (.833)
PO community groups (.726)PO work (.615) Car ownership (.774)
Overall inclusion (.761) Years in the area (.538)
Friends to home (.620)
SCOPE: social and community opportunities profile.
Loadings greater than .5; varimax rotation; variance explained = 65%.
Table 4. Exploratory factor analysis: SCOPE UK severe illness sample.
Factor 1 (30%) Factor 2 (18%) Factor 3 (15%) Factor 4 (13%) Factor 5 (12%)Factor 6 (12%)
Overall inclusion (.925) SO education (.855) SO income (.932) SO work (.728) SO family
contact (.912)
Years in area
(.923)
SO leisure (.857) Safety of the area (.812)Car ownership (.683)PO income (.928) Age (.677)
PO work (.746) PO income (.686)
PO community groups (.625)PO housing (.517)
Friends to home (.517)
SCOPE: social and community opportunities profile.
Loadings greater than .5; varimax rotation; variance explained = 91%.
Table 5. Exploratory factor analysis: SCOPE Honk Kong severe illness sample.
Factor 1 (22%) Factor 2 (13%) Factor 3 (10%) Factor 4 (8%) Factor 5 (8%) Factor 6 (7%)
SO friends to
home (.801)
Safety of the area
(.815)
SO education
(.750)
SO community
groups (.867)
PO income
(.846)
SO leisure
(.681)
SO work (.787) Overall inclusion
(.715)
PO education
(.697)
PO community
groups (.712)
Housing
(.663)
SO family
contact (.652)
SO friend contact
(.533)
SCOPE: social and community opportunities profile.
Loadings greater than .5; varimax rotation; variance explained = 68%.
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
138 International Journal of Social Psychiatry 62(2)
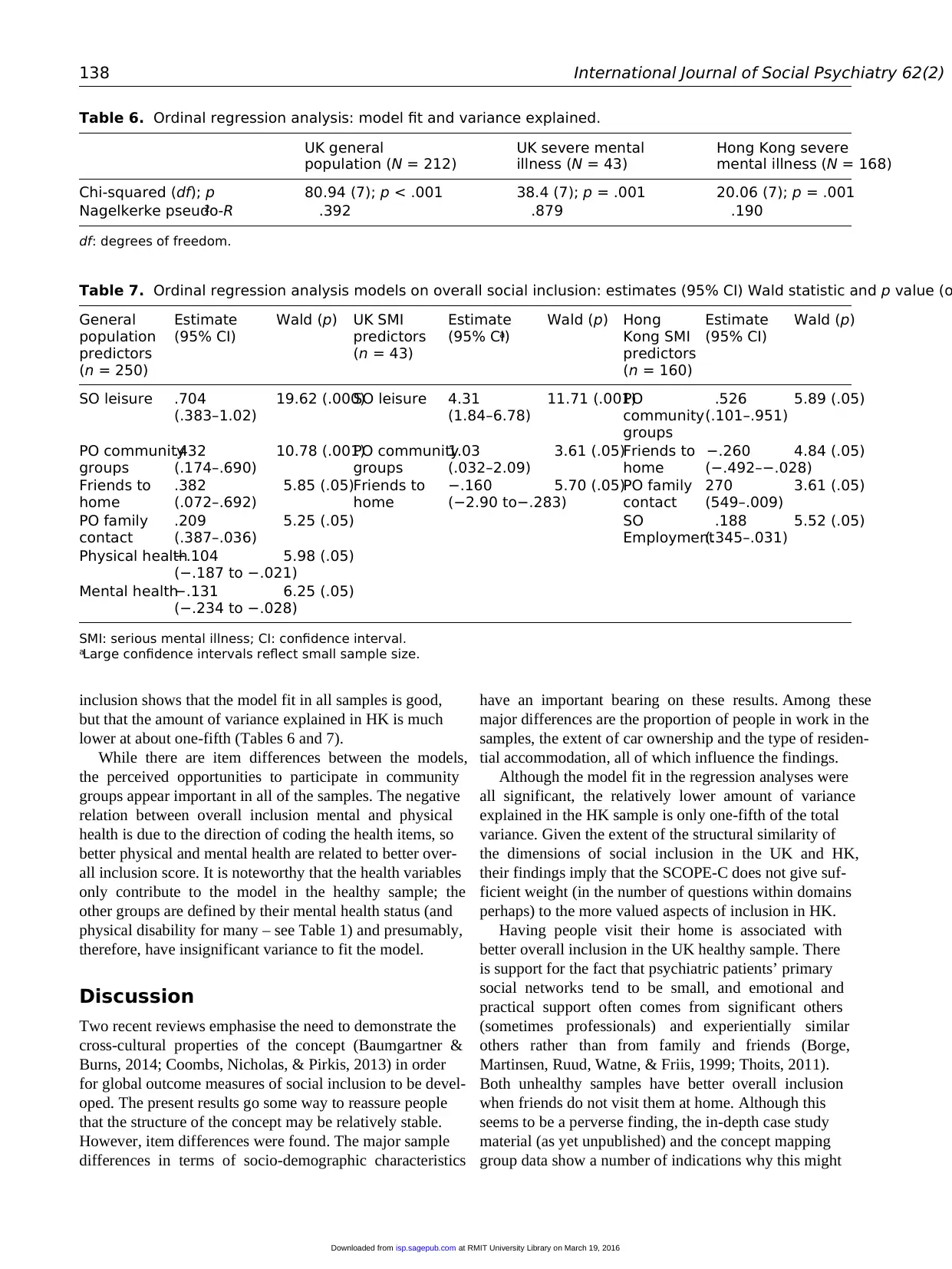
inclusion shows that the model fit in all samples is good,
but that the amount of variance explained in HK is much
lower at about one-fifth (Tables 6 and 7).
While there are item differences between the models,
the perceived opportunities to participate in community
groups appear important in all of the samples. The negative
relation between overall inclusion mental and physical
health is due to the direction of coding the health items, so
better physical and mental health are related to better over-
all inclusion score. It is noteworthy that the health variables
only contribute to the model in the healthy sample; the
other groups are defined by their mental health status (and
physical disability for many – see Table 1) and presumably,
therefore, have insignificant variance to fit the model.
Discussion
Two recent reviews emphasise the need to demonstrate the
cross-cultural properties of the concept (Baumgartner &
Burns, 2014; Coombs, Nicholas, & Pirkis, 2013) in order
for global outcome measures of social inclusion to be devel-
oped. The present results go some way to reassure people
that the structure of the concept may be relatively stable.
However, item differences were found. The major sample
differences in terms of socio-demographic characteristics
have an important bearing on these results. Among these
major differences are the proportion of people in work in the
samples, the extent of car ownership and the type of residen-
tial accommodation, all of which influence the findings.
Although the model fit in the regression analyses were
all significant, the relatively lower amount of variance
explained in the HK sample is only one-fifth of the total
variance. Given the extent of the structural similarity of
the dimensions of social inclusion in the UK and HK,
their findings imply that the SCOPE-C does not give suf-
ficient weight (in the number of questions within domains
perhaps) to the more valued aspects of inclusion in HK.
Having people visit their home is associated with
better overall inclusion in the UK healthy sample. There
is support for the fact that psychiatric patients’ primary
social networks tend to be small, and emotional and
practical support often comes from significant others
(sometimes professionals) and experientially similar
others rather than from family and friends (Borge,
Martinsen, Ruud, Watne, & Friis, 1999; Thoits, 2011).
Both unhealthy samples have better overall inclusion
when friends do not visit them at home. Although this
seems to be a perverse finding, the in-depth case study
material (as yet unpublished) and the concept mapping
group data show a number of indications why this might
Table 6. Ordinal regression analysis: model fit and variance explained.
UK general
population (N = 212)
UK severe mental
illness (N = 43)
Hong Kong severe
mental illness (N = 168)
Chi-squared (df); p 80.94 (7); p < .001 38.4 (7); p = .001 20.06 (7); p = .001
Nagelkerke pseudo-R2 .392 .879 .190
df: degrees of freedom.
Table 7. Ordinal regression analysis models on overall social inclusion: estimates (95% CI) Wald statistic and p value (o
General
population
predictors
(n = 250)
Estimate
(95% CI)
Wald (p) UK SMI
predictors
(n = 43)
Estimate
(95% CI)a
Wald (p) Hong
Kong SMI
predictors
(n = 160)
Estimate
(95% CI)
Wald (p)
SO leisure .704
(.383–1.02)
19.62 (.000)SO leisure 4.31
(1.84–6.78)
11.71 (.001)PO
community
groups
.526
(.101–.951)
5.89 (.05)
PO community
groups
.432
(.174–.690)
10.78 (.001)PO community
groups
1.03
(.032–2.09)
3.61 (.05)Friends to
home
−.260
(−.492–−.028)
4.84 (.05)
Friends to
home
.382
(.072–.692)
5.85 (.05)Friends to
home
−.160
(−2.90 to−.283)
5.70 (.05)PO family
contact
270
(549–.009)
3.61 (.05)
PO family
contact
.209
(.387–.036)
5.25 (.05) SO
Employment
.188
(.345–.031)
5.52 (.05)
Physical health−.104
(−.187 to −.021)
5.98 (.05)
Mental health−.131
(−.234 to −.028)
6.25 (.05)
SMI: serious mental illness; CI: confidence interval.
aLarge confidence intervals reflect small sample size.
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
inclusion shows that the model fit in all samples is good,
but that the amount of variance explained in HK is much
lower at about one-fifth (Tables 6 and 7).
While there are item differences between the models,
the perceived opportunities to participate in community
groups appear important in all of the samples. The negative
relation between overall inclusion mental and physical
health is due to the direction of coding the health items, so
better physical and mental health are related to better over-
all inclusion score. It is noteworthy that the health variables
only contribute to the model in the healthy sample; the
other groups are defined by their mental health status (and
physical disability for many – see Table 1) and presumably,
therefore, have insignificant variance to fit the model.
Discussion
Two recent reviews emphasise the need to demonstrate the
cross-cultural properties of the concept (Baumgartner &
Burns, 2014; Coombs, Nicholas, & Pirkis, 2013) in order
for global outcome measures of social inclusion to be devel-
oped. The present results go some way to reassure people
that the structure of the concept may be relatively stable.
However, item differences were found. The major sample
differences in terms of socio-demographic characteristics
have an important bearing on these results. Among these
major differences are the proportion of people in work in the
samples, the extent of car ownership and the type of residen-
tial accommodation, all of which influence the findings.
Although the model fit in the regression analyses were
all significant, the relatively lower amount of variance
explained in the HK sample is only one-fifth of the total
variance. Given the extent of the structural similarity of
the dimensions of social inclusion in the UK and HK,
their findings imply that the SCOPE-C does not give suf-
ficient weight (in the number of questions within domains
perhaps) to the more valued aspects of inclusion in HK.
Having people visit their home is associated with
better overall inclusion in the UK healthy sample. There
is support for the fact that psychiatric patients’ primary
social networks tend to be small, and emotional and
practical support often comes from significant others
(sometimes professionals) and experientially similar
others rather than from family and friends (Borge,
Martinsen, Ruud, Watne, & Friis, 1999; Thoits, 2011).
Both unhealthy samples have better overall inclusion
when friends do not visit them at home. Although this
seems to be a perverse finding, the in-depth case study
material (as yet unpublished) and the concept mapping
group data show a number of indications why this might
Table 6. Ordinal regression analysis: model fit and variance explained.
UK general
population (N = 212)
UK severe mental
illness (N = 43)
Hong Kong severe
mental illness (N = 168)
Chi-squared (df); p 80.94 (7); p < .001 38.4 (7); p = .001 20.06 (7); p = .001
Nagelkerke pseudo-R2 .392 .879 .190
df: degrees of freedom.
Table 7. Ordinal regression analysis models on overall social inclusion: estimates (95% CI) Wald statistic and p value (o
General
population
predictors
(n = 250)
Estimate
(95% CI)
Wald (p) UK SMI
predictors
(n = 43)
Estimate
(95% CI)a
Wald (p) Hong
Kong SMI
predictors
(n = 160)
Estimate
(95% CI)
Wald (p)
SO leisure .704
(.383–1.02)
19.62 (.000)SO leisure 4.31
(1.84–6.78)
11.71 (.001)PO
community
groups
.526
(.101–.951)
5.89 (.05)
PO community
groups
.432
(.174–.690)
10.78 (.001)PO community
groups
1.03
(.032–2.09)
3.61 (.05)Friends to
home
−.260
(−.492–−.028)
4.84 (.05)
Friends to
home
.382
(.072–.692)
5.85 (.05)Friends to
home
−.160
(−2.90 to−.283)
5.70 (.05)PO family
contact
270
(549–.009)
3.61 (.05)
PO family
contact
.209
(.387–.036)
5.25 (.05) SO
Employment
.188
(.345–.031)
5.52 (.05)
Physical health−.104
(−.187 to −.021)
5.98 (.05)
Mental health−.131
(−.234 to −.028)
6.25 (.05)
SMI: serious mental illness; CI: confidence interval.
aLarge confidence intervals reflect small sample size.
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from

Huxley et al. 139
be the case. First, patients in group home settings in HK
and United Kingdom are encouraged to go out to social-
ise, rather than stay at home all day. In HK, and to a
lesser extent in the United Kingdom, homes are often
small and not especially welcoming. In addition, some
of the housing locations are themselves a factor in that
they are often in deprived neighbourhoods and tower
blocks which the patient feel is stigmatising, and they
would rather socialise away from home at work or in
community groups.
There are no car owners in the HK sample, and this is a
reflection of the cost of purchasing a car in HK and of the
living arrangements in high-rise apartment blocks and close
proximity to family members, and the ease of transport
around the city and the lowest level of car ownership of any
major global conurbation (Cullinane 2002; Cullinane &
Cullinane, 2003). However, in the United Kingdom, car
ownership is more necessary and has been used previously
as a proxy indicator of material wealth and does have a
bearing on inclusion, especially in rural areas. Another
indicator of material well-being needs to be substituted for
or added to car ownership for SCOPE-C, for example, the
size of the space available per family member might be a
better indicator of material advantage in HK. Although we
amended some of the SCOPE objective questions to make
them consistent with the wording of the HK census, we
may have to add more questions or revise existing ones in
order to explain more of the variance of overall inclusion.
Conclusion
SCOPE is one of very few direct measures of social inclu-
sion (Baumgartner & Burns, 2014) and has been singled
out as one of only two measures worthy of further develop-
ment work (Coombs et al., 2013). The need for a global
cross-cultural measure that has been developed and tested
in diverse settings has been reiterated recently (Baumgartner
& Burns, 2014).
The lower amount of variance explained in the HK
sample suggests that improvements can be made to capture
more of the variance of overall inclusion. This will be the
subject of further data gathering and qualitative analysis
from detailed case studies and a feedback event for NGO
managers and workers, plus a re-consideration of the con-
cept mapping data. Evidently, an instrument developed to
measure the particular circumstances of one disability
group in one culture is more likely to explain a large
amount of the variance of local responses. When re-located
into another culture, although the structure of domains of
inclusion remains similar, the power to explain overall
inclusion ratings seems to be diminishing.
China’s future major health problem is going to be the
management of chronic diseases (of which mental health
is a major one) in community settings (World Health
Organization (WHO), 2008). A suitably modified SCOPE-C
may be used by mental health services in HK and mainland
China as they strive to promote a more inclusive society for
their citizens and particular disadvantaged groups.
Acknowledgements
This project was funded by Economic & Social Research Council
(Project no.: ES/K005227/1). We are thankful to the NGOs who
facilitate our contact with the voluntary participants who took
part in the study. These NGOs include Baptist Oi Kwan Social
Services, Caritas Hong Kong, Fu Hong Society, Stewards Social
Services, The Mental Health Association of Hong Kong, and The
Society of Rehabilitation and Crime Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect
to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support
for the research, authorship, and/or publication of this article:
This project was funded by Economic & Social Research Council
(Project no.: ES/K005227/1).
References
Baumgartner, J. N., & Burns, J. K. (2014). Measuring social
inclusion – A key outcome in global mental health.
International Journal of Epidemiology, 43, 354–364.
doi:10.1093/ije/dyt224
Berg, M., Jahnsen, R., Holm, I., & Hussain, A. (2003). Translation of
a multi-disciplinary assessment – Procedures to achieve func-
tional equivalence. Advances in Physiotherapy, 5(2), 57–66.
Blaxland, M., Fisher, K. R., & Shang, X. (2015). Transitional
and developmental challenges for Chinese social policy.
Asian Social Work and Policy Review, 9, 1–2. doi:10.1111/
aswp.12047
Borge, L., Martinsen, E. W., Ruud, T., Watne, O., & Friis, S.
(1999). Quality of life, loneliness, and social contact among
long-term psychiatric patients. Psychiatric Services, 50,
81–84. doi:10.1176/ps.50.1.81
Boushey, H., Fremstad, S., Gragg, R., & Waller, M. (2007).
Social inclusion for the USA: Advocating the use of the con-
cept in the USA. Available at: www.inclusionist.org/files/
socialinclusionusa.pdf
Bowden, A., & Fox-Rushby, J. A. (2003). A systematic and criti-
cal review of the process of translation and adaptation of
generic health-related quality of life measures in Africa,
Asia, Eastern Europe, the Middle East, South America.
Social Science & Medicine, 57, 1289–1306.
Chan, K., Chiu, M., Evans, S., Huxley, P. J., & Ng, Y. L.
(2015b). Application of SCOPE-C to measure social inclu-
sion among mental health services users in Hong Kong.
Community Mental Health Journal. Advance online publi-
cation. doi:10.1007/s10597-015-9907-z
Chan, K., Evans, S., Chiu, M., Huxley, P. J., & Ng, Y. L. (2014a).
Relationship between health, experience of discrimination,
and social inclusion among mental health service users in
Hong Kong. Social Indicators Research, 124(1), 127–139.
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
be the case. First, patients in group home settings in HK
and United Kingdom are encouraged to go out to social-
ise, rather than stay at home all day. In HK, and to a
lesser extent in the United Kingdom, homes are often
small and not especially welcoming. In addition, some
of the housing locations are themselves a factor in that
they are often in deprived neighbourhoods and tower
blocks which the patient feel is stigmatising, and they
would rather socialise away from home at work or in
community groups.
There are no car owners in the HK sample, and this is a
reflection of the cost of purchasing a car in HK and of the
living arrangements in high-rise apartment blocks and close
proximity to family members, and the ease of transport
around the city and the lowest level of car ownership of any
major global conurbation (Cullinane 2002; Cullinane &
Cullinane, 2003). However, in the United Kingdom, car
ownership is more necessary and has been used previously
as a proxy indicator of material wealth and does have a
bearing on inclusion, especially in rural areas. Another
indicator of material well-being needs to be substituted for
or added to car ownership for SCOPE-C, for example, the
size of the space available per family member might be a
better indicator of material advantage in HK. Although we
amended some of the SCOPE objective questions to make
them consistent with the wording of the HK census, we
may have to add more questions or revise existing ones in
order to explain more of the variance of overall inclusion.
Conclusion
SCOPE is one of very few direct measures of social inclu-
sion (Baumgartner & Burns, 2014) and has been singled
out as one of only two measures worthy of further develop-
ment work (Coombs et al., 2013). The need for a global
cross-cultural measure that has been developed and tested
in diverse settings has been reiterated recently (Baumgartner
& Burns, 2014).
The lower amount of variance explained in the HK
sample suggests that improvements can be made to capture
more of the variance of overall inclusion. This will be the
subject of further data gathering and qualitative analysis
from detailed case studies and a feedback event for NGO
managers and workers, plus a re-consideration of the con-
cept mapping data. Evidently, an instrument developed to
measure the particular circumstances of one disability
group in one culture is more likely to explain a large
amount of the variance of local responses. When re-located
into another culture, although the structure of domains of
inclusion remains similar, the power to explain overall
inclusion ratings seems to be diminishing.
China’s future major health problem is going to be the
management of chronic diseases (of which mental health
is a major one) in community settings (World Health
Organization (WHO), 2008). A suitably modified SCOPE-C
may be used by mental health services in HK and mainland
China as they strive to promote a more inclusive society for
their citizens and particular disadvantaged groups.
Acknowledgements
This project was funded by Economic & Social Research Council
(Project no.: ES/K005227/1). We are thankful to the NGOs who
facilitate our contact with the voluntary participants who took
part in the study. These NGOs include Baptist Oi Kwan Social
Services, Caritas Hong Kong, Fu Hong Society, Stewards Social
Services, The Mental Health Association of Hong Kong, and The
Society of Rehabilitation and Crime Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect
to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support
for the research, authorship, and/or publication of this article:
This project was funded by Economic & Social Research Council
(Project no.: ES/K005227/1).
References
Baumgartner, J. N., & Burns, J. K. (2014). Measuring social
inclusion – A key outcome in global mental health.
International Journal of Epidemiology, 43, 354–364.
doi:10.1093/ije/dyt224
Berg, M., Jahnsen, R., Holm, I., & Hussain, A. (2003). Translation of
a multi-disciplinary assessment – Procedures to achieve func-
tional equivalence. Advances in Physiotherapy, 5(2), 57–66.
Blaxland, M., Fisher, K. R., & Shang, X. (2015). Transitional
and developmental challenges for Chinese social policy.
Asian Social Work and Policy Review, 9, 1–2. doi:10.1111/
aswp.12047
Borge, L., Martinsen, E. W., Ruud, T., Watne, O., & Friis, S.
(1999). Quality of life, loneliness, and social contact among
long-term psychiatric patients. Psychiatric Services, 50,
81–84. doi:10.1176/ps.50.1.81
Boushey, H., Fremstad, S., Gragg, R., & Waller, M. (2007).
Social inclusion for the USA: Advocating the use of the con-
cept in the USA. Available at: www.inclusionist.org/files/
socialinclusionusa.pdf
Bowden, A., & Fox-Rushby, J. A. (2003). A systematic and criti-
cal review of the process of translation and adaptation of
generic health-related quality of life measures in Africa,
Asia, Eastern Europe, the Middle East, South America.
Social Science & Medicine, 57, 1289–1306.
Chan, K., Chiu, M., Evans, S., Huxley, P. J., & Ng, Y. L.
(2015b). Application of SCOPE-C to measure social inclu-
sion among mental health services users in Hong Kong.
Community Mental Health Journal. Advance online publi-
cation. doi:10.1007/s10597-015-9907-z
Chan, K., Evans, S., Chiu, M., Huxley, P. J., & Ng, Y. L. (2014a).
Relationship between health, experience of discrimination,
and social inclusion among mental health service users in
Hong Kong. Social Indicators Research, 124(1), 127–139.
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
140 International Journal of Social Psychiatry 62(2)
Chan, K., Evans, S., Ng, Y. L., Chiu, M., & Huxley, P. (2014b).
A concept mapping study on social inclusion in Hong Kong.
Social Indicators Research, 119, 121–137.
Chan, K., Huxley, P. J., Chiu, M., Evans, S., & Ma, Y. (2015a).
Social inclusion and health conditions among Chinese
immigrants in Hong Kong and the United Kingdom: An
exploratory study. Social Indicators Research. Advance
online publication. doi:10.1007/s11205-015-0910-0
Cheung, Y. B., & Thumboo, J. (2006). Developing health-related
quality-of-life instruments for use in Asia: The issues.
Pharmacoeconomics, 24, 643–650.
Commission of the European Communities. (2000). Social pol-
icy agenda: Communication from the Commission to the
Council, the European Parliament, the economic and social
committee and the committee of the regions. Brussels,
Belgium: Author.
Coombs, T., Nicholas, A., & Pirkis, J. (2013). A review of social
inclusion measures. The Australian and New Zealand Journal
of Psychiatry, 47, 906–919. doi:10.1177/0004867413491161
Council for the European Union. (2003). Joint report by the
Commission and the Council on social inclusion. Brussels,
Belgium: Author.
Cullinane, S. (2002). The relationship between car ownership
and public transport provision: A case study of Hong Kong.
Transport Policy, 9, 29–39.
Cullinane, S., & Cullinane, C. (2003). Car dependence in a
public transport dominated city: Evidence from Hong
Kong. Transportation Research Part D: Transport and
Environment, 8, 129–138.
Curran, C., Burchardt, T., Knapp, M., Mcdaid, D., & Li, B.
(2007). Changes in multidisciplinary systematic reviewing:
A study on social exclusion and mental health policy. Social
Policy and Administration, 1, 289–312.
Fischer, R., & Fontaine, J. R. J. (2011). Methods for investigating
structural equivalence. In D. Matsumoto & F. J. R. Van de
Vijver (Eds.), Cross cultural research methods in psychol-
ogy (pp. 179–215). Cambridge, UK: Cambridge University
Press.
Fisher, K., & Jing, L. (2008). Chinese disability independent liv-
ing policy. Disability and Society, 23, 171–185.
Gordon, D. (2000). Breadline Europe: The measurement of pov-
erty. Bristol, UK: Policy Press.
Herdman, M., Fox-Rushby, J., & Badia, X. (1998). A model of
equivalence in the cultural adaptation of HRQoL instruments:
The universalist approach. Quality of Life Research, 7, 323–335.
Huxley, P., Evans, S., Madge, S., Webber, M., Burchardt,
T., McDaid, D., & Knapp, M. (2012). Development of a
social inclusion index to capture subjective and objective
life domains (Phase II): Psychometric development study.
Health Technology Assessment, 16, iii–vii, ix–xii, 1–241.
doi:10.3310/hta16010
Johnson, T. P., Shavitt, S., & Holbrook, A. L. (2011). Survey
response styles across cultures. In D. Matsumoto & F. J.
R. Van de Vijver (Eds.), Cross cultural research methods
in psychology (pp. 130–178). Cambridge, UK: Cambridge
University Press.
Lee, J. W., & Jung, D. Y. (2006). Measurement issues across
different cultures. Journal of Korean Academy of Nursing,
36, 1295–1300.
Leff, J., & Warner, R. (2006). Social inclusion of people with
mental illness. Cambridge, UK: Cambridge University Press.
Luhrmann, T. M. (2014, December 15). Wheat people vs. rice
people – Association for Psychological Science. International
New York Times. Retrieved from http://www.psychologicals-
cience.org/index.php/news/wheat-people-vs-rice-people.html
Mahler, C., Jank, S., Reuschenbach, B., & Szecsenyi, J. (2009).
‘Let’s quickly translate this questionnaire’ – Guidelines for
translation and implementation of English-language assess-
ment instruments. Pflegewissenschaft, 13(1), 5–12.
Matsumoto, D., & Van de Vijver, F. J. R. (Eds.). (2011). Cross-
cultural research methods in psychology. New York, NY:
Cambridge University Press.
Mental Health Europe. (2008). From exclusion to inclusion:
The way forward to promoting social inclusion of people
with mental health problems in Europe. Brussels, Belgium:
Mental Health Europe.
Repper, J., & Perkins, R. (2003). Social inclusion and recov-
ery: A model for mental health practice. London, England:
Baillière Tindall.
Steele, G., & Lynch, S. M. (2013). The pursuit of happiness in
China: Individualism, collectivism, and subjective well-
being during China’s economic and social transformation.
Social Indicators Research, 114, 441–451.
Streiner, D. L., & Norman, G. R. (2008). Health measurement
scales: A practical guide to their development and use (4th
ed.). Oxford, UK: Oxford University Press.
Thoits, P. A. (2011). Mechanisms linking social ties and support
to physical and mental health. Journal of Health and Social
Behavior, 52, 145–161. doi:10.1177/0022146510395592
Townsend, P. (1979). Poverty in the United Kingdom.
Harmondsworth, UK: Penguin.
Tran, T. V. (2009). Developing cross cultural measurement.
Oxford, UK: Oxford University Press.
Ungvari, G., & Chiu, H. F. K. (2004). The state of psychiatry
in Hong Kong: A bird’s eye view. International Journal of
Social Psychiatry, 50, 5–9.
Van de Vijver, F. J. R., & Leung, K. (2011). Equivalence and
bias: A review of concepts, models and data analytic pro-
cedures. In D. Matsumoto & F. J. R. Van de Vijver (Eds.),
Cross cultural research methods in psychology (pp. 33–34).
Cambridge, UK: Cambridge University Press.
Van Widenfelt, B. M., Treffers, P. D., De Beurs, E., Siebelink,
B. M., & Koudijs, E. (2005). Translation and cross-cultural
adaptation of assessment instruments used in psychologi-
cal research with children and families. Clinical Child and
Family Psychology Review, 8, 135–147.
Wang, S., Marquez, P., & Langenbrunner, J. (2011). Toward a
healthy and harmonious life in China: Stemming the rising
tide of non-communicable diseases. Human Development
Unit, The World Bank, Washington.
Willgerodt, M. A., Kataoka-Yahiro, M., Kim, E., & Ceria, C.
(2005). Issues of instrument translation in research on Asian
immigrant populations. Journal of Professional Nursing,
21, 231–239.
World Health Organization. (2008). mhGAP: Mental health gap
action programme: Scaling up care for mental, neurologi-
cal, and substance use disorders. Retrieved from http://
www.who.int/mental_health/mhgap_final_english.pdf
Wright, N., & Stickley, T. (2013). Concepts of social inclu-
sion, exclusion and mental health: A review of the interna-
tional literature. Journal of Psychiatric and Mental Health
Nursing, 20(1), 71–81.
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
Chan, K., Evans, S., Ng, Y. L., Chiu, M., & Huxley, P. (2014b).
A concept mapping study on social inclusion in Hong Kong.
Social Indicators Research, 119, 121–137.
Chan, K., Huxley, P. J., Chiu, M., Evans, S., & Ma, Y. (2015a).
Social inclusion and health conditions among Chinese
immigrants in Hong Kong and the United Kingdom: An
exploratory study. Social Indicators Research. Advance
online publication. doi:10.1007/s11205-015-0910-0
Cheung, Y. B., & Thumboo, J. (2006). Developing health-related
quality-of-life instruments for use in Asia: The issues.
Pharmacoeconomics, 24, 643–650.
Commission of the European Communities. (2000). Social pol-
icy agenda: Communication from the Commission to the
Council, the European Parliament, the economic and social
committee and the committee of the regions. Brussels,
Belgium: Author.
Coombs, T., Nicholas, A., & Pirkis, J. (2013). A review of social
inclusion measures. The Australian and New Zealand Journal
of Psychiatry, 47, 906–919. doi:10.1177/0004867413491161
Council for the European Union. (2003). Joint report by the
Commission and the Council on social inclusion. Brussels,
Belgium: Author.
Cullinane, S. (2002). The relationship between car ownership
and public transport provision: A case study of Hong Kong.
Transport Policy, 9, 29–39.
Cullinane, S., & Cullinane, C. (2003). Car dependence in a
public transport dominated city: Evidence from Hong
Kong. Transportation Research Part D: Transport and
Environment, 8, 129–138.
Curran, C., Burchardt, T., Knapp, M., Mcdaid, D., & Li, B.
(2007). Changes in multidisciplinary systematic reviewing:
A study on social exclusion and mental health policy. Social
Policy and Administration, 1, 289–312.
Fischer, R., & Fontaine, J. R. J. (2011). Methods for investigating
structural equivalence. In D. Matsumoto & F. J. R. Van de
Vijver (Eds.), Cross cultural research methods in psychol-
ogy (pp. 179–215). Cambridge, UK: Cambridge University
Press.
Fisher, K., & Jing, L. (2008). Chinese disability independent liv-
ing policy. Disability and Society, 23, 171–185.
Gordon, D. (2000). Breadline Europe: The measurement of pov-
erty. Bristol, UK: Policy Press.
Herdman, M., Fox-Rushby, J., & Badia, X. (1998). A model of
equivalence in the cultural adaptation of HRQoL instruments:
The universalist approach. Quality of Life Research, 7, 323–335.
Huxley, P., Evans, S., Madge, S., Webber, M., Burchardt,
T., McDaid, D., & Knapp, M. (2012). Development of a
social inclusion index to capture subjective and objective
life domains (Phase II): Psychometric development study.
Health Technology Assessment, 16, iii–vii, ix–xii, 1–241.
doi:10.3310/hta16010
Johnson, T. P., Shavitt, S., & Holbrook, A. L. (2011). Survey
response styles across cultures. In D. Matsumoto & F. J.
R. Van de Vijver (Eds.), Cross cultural research methods
in psychology (pp. 130–178). Cambridge, UK: Cambridge
University Press.
Lee, J. W., & Jung, D. Y. (2006). Measurement issues across
different cultures. Journal of Korean Academy of Nursing,
36, 1295–1300.
Leff, J., & Warner, R. (2006). Social inclusion of people with
mental illness. Cambridge, UK: Cambridge University Press.
Luhrmann, T. M. (2014, December 15). Wheat people vs. rice
people – Association for Psychological Science. International
New York Times. Retrieved from http://www.psychologicals-
cience.org/index.php/news/wheat-people-vs-rice-people.html
Mahler, C., Jank, S., Reuschenbach, B., & Szecsenyi, J. (2009).
‘Let’s quickly translate this questionnaire’ – Guidelines for
translation and implementation of English-language assess-
ment instruments. Pflegewissenschaft, 13(1), 5–12.
Matsumoto, D., & Van de Vijver, F. J. R. (Eds.). (2011). Cross-
cultural research methods in psychology. New York, NY:
Cambridge University Press.
Mental Health Europe. (2008). From exclusion to inclusion:
The way forward to promoting social inclusion of people
with mental health problems in Europe. Brussels, Belgium:
Mental Health Europe.
Repper, J., & Perkins, R. (2003). Social inclusion and recov-
ery: A model for mental health practice. London, England:
Baillière Tindall.
Steele, G., & Lynch, S. M. (2013). The pursuit of happiness in
China: Individualism, collectivism, and subjective well-
being during China’s economic and social transformation.
Social Indicators Research, 114, 441–451.
Streiner, D. L., & Norman, G. R. (2008). Health measurement
scales: A practical guide to their development and use (4th
ed.). Oxford, UK: Oxford University Press.
Thoits, P. A. (2011). Mechanisms linking social ties and support
to physical and mental health. Journal of Health and Social
Behavior, 52, 145–161. doi:10.1177/0022146510395592
Townsend, P. (1979). Poverty in the United Kingdom.
Harmondsworth, UK: Penguin.
Tran, T. V. (2009). Developing cross cultural measurement.
Oxford, UK: Oxford University Press.
Ungvari, G., & Chiu, H. F. K. (2004). The state of psychiatry
in Hong Kong: A bird’s eye view. International Journal of
Social Psychiatry, 50, 5–9.
Van de Vijver, F. J. R., & Leung, K. (2011). Equivalence and
bias: A review of concepts, models and data analytic pro-
cedures. In D. Matsumoto & F. J. R. Van de Vijver (Eds.),
Cross cultural research methods in psychology (pp. 33–34).
Cambridge, UK: Cambridge University Press.
Van Widenfelt, B. M., Treffers, P. D., De Beurs, E., Siebelink,
B. M., & Koudijs, E. (2005). Translation and cross-cultural
adaptation of assessment instruments used in psychologi-
cal research with children and families. Clinical Child and
Family Psychology Review, 8, 135–147.
Wang, S., Marquez, P., & Langenbrunner, J. (2011). Toward a
healthy and harmonious life in China: Stemming the rising
tide of non-communicable diseases. Human Development
Unit, The World Bank, Washington.
Willgerodt, M. A., Kataoka-Yahiro, M., Kim, E., & Ceria, C.
(2005). Issues of instrument translation in research on Asian
immigrant populations. Journal of Professional Nursing,
21, 231–239.
World Health Organization. (2008). mhGAP: Mental health gap
action programme: Scaling up care for mental, neurologi-
cal, and substance use disorders. Retrieved from http://
www.who.int/mental_health/mhgap_final_english.pdf
Wright, N., & Stickley, T. (2013). Concepts of social inclu-
sion, exclusion and mental health: A review of the interna-
tional literature. Journal of Psychiatric and Mental Health
Nursing, 20(1), 71–81.
at RMIT University Library on March 19, 2016isp.sagepub.comDownloaded from
1 out of 8
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.