Interprofessional Teamwork and Collaboration Between Community Health Workers and Healthcare Teams: An Integrative Review
VerifiedAdded on 2023/06/10
|9
|8129
|140
AI Summary
This integrative review examines interprofessional teamwork and collaboration with CHWs in research demonstrating positive health outcomes as a result of CHW intervention. The study aims to identify assumptions of effective interprofessional teamwork between CHWs and health care teams. The review methodology used two major systematic reviews of the literature. The study concludes that further research is needed to describe the nature of interprofessional teamwork and collaboration in relation to patient health outcomes.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Interprofessional Teamwork and
Collaboration Between Community Health
Workers and Healthcare Teams:
An Integrative Review
Catherine M. Franklin1, Jean M. Bernhardt2, Ruth Palan Lopez2,
Ellen R. Long-Middleton3, and Sheila Davis4
Abstract
Objectives:Community Health Workers (CHWs) serve as a means ofimproving outcomes for underserved populations.
However, their relationship within health care teams is not well studied. The purpose of this integrative review wa
published research reports that demonstrated positive health outcomes as a result ofCHW intervention to identify inter-
professionalteamwork and collaboration between CHWs and health care teams.
Methods: A total of 47 studies spanning 33 years were reviewed using an integrative literature review methodolo
to support the following assumptions of effective interprofessional teamwork between CHWs and health care tea
understanding ofroles,norms,values,and goals ofthe team;(2) egalitarianism;(3) cooperation;(4) interdependence;and(5)
synergy.
Results: Of the 47 studies,12 reported atleastone assumption ofeffective interprofessionalteamwork.Four studies
demonstrated all5 assumptions of interprofessionalteamwork.
Conclusions:Four studies identified in this integrative review serve as exemplars for effective interprofessionalteamwork
between CHWs and health care teams.Further study is needed to describe the nature ofinterprofessionalteamwork and
collaboration in relation to patient health outcomes.
Keywords
community health,access to care,community health worker,interprofessionalteamwork,collaboration
Background
Community health workers (CHWs) can improve outcomes for
underserved people.1,2Evidence exists that CHW interventions
in underserved populations improve health care management,
disease prevention,and health promotion.Community health
workers improve managementof chronic illnesses such as
asthma, diabetes, maternal–child health issues, increase health
promotion activities such as vaccinations and cancer screening,
and demonstrate netcostsavings.1-3 Based on this evidence,
interestin new CHW models has grown.Delivery systems
strive to improve health care access, improve cultural congru-
ence,and address quality and cost among the growing immi-
grant population and otherunderserved,isolated,and
vulnerable people.The CHW modelpresents an opportunity
to achieve these goals.4-6
Presently, there is a national call for greater use of CHWs
improve the nation’s health.In 2011,the Center for Disease
Controland Prevention (CDC) and the Division forHeart
1 Department of Family Medicine,East Boston Neighborhood Health Center,
East Boston,MA, USA
2 Schoolof Nursing,MGH Institute of Health Professions,Boston,MA, USA
3 College of Nursing and Health Sciences,University of Vermont,Burlington,
VT, USA
4 Partners in Health,Boston,MA, USA
Corresponding Author:
Catherine M. Franklin,Departmentof Family Medicine,East Boston
Neighborhood Health Center,20 Maverick Square,East Boston,MA 02128,
USA.
Email:franklic@ebnhc.org
Health Services Research and
ManagerialEpidemiology
1-9
ª The Author(s) 2015
Reprints and permission:
sagepub.com/journalsPermissions.nav
DOI: 10.1177/2333392815573312
hme.sagepub.com
Creative Commons CC-BY-NC:This article is distributed under the terms ofthe Creative Commons Attribution-NonCommercial3.0 License
(http://www.creativecommons.org/licenses/by-nc/3.0/) which permits non-commercialuse,reproduction and distribution ofthe work without further
permission provided the originalwork is attributed as specified on the SAGE and Open Access page (http://www.uk.sagepub.com/aboutus/openaccess
Collaboration Between Community Health
Workers and Healthcare Teams:
An Integrative Review
Catherine M. Franklin1, Jean M. Bernhardt2, Ruth Palan Lopez2,
Ellen R. Long-Middleton3, and Sheila Davis4
Abstract
Objectives:Community Health Workers (CHWs) serve as a means ofimproving outcomes for underserved populations.
However, their relationship within health care teams is not well studied. The purpose of this integrative review wa
published research reports that demonstrated positive health outcomes as a result ofCHW intervention to identify inter-
professionalteamwork and collaboration between CHWs and health care teams.
Methods: A total of 47 studies spanning 33 years were reviewed using an integrative literature review methodolo
to support the following assumptions of effective interprofessional teamwork between CHWs and health care tea
understanding ofroles,norms,values,and goals ofthe team;(2) egalitarianism;(3) cooperation;(4) interdependence;and(5)
synergy.
Results: Of the 47 studies,12 reported atleastone assumption ofeffective interprofessionalteamwork.Four studies
demonstrated all5 assumptions of interprofessionalteamwork.
Conclusions:Four studies identified in this integrative review serve as exemplars for effective interprofessionalteamwork
between CHWs and health care teams.Further study is needed to describe the nature ofinterprofessionalteamwork and
collaboration in relation to patient health outcomes.
Keywords
community health,access to care,community health worker,interprofessionalteamwork,collaboration
Background
Community health workers (CHWs) can improve outcomes for
underserved people.1,2Evidence exists that CHW interventions
in underserved populations improve health care management,
disease prevention,and health promotion.Community health
workers improve managementof chronic illnesses such as
asthma, diabetes, maternal–child health issues, increase health
promotion activities such as vaccinations and cancer screening,
and demonstrate netcostsavings.1-3 Based on this evidence,
interestin new CHW models has grown.Delivery systems
strive to improve health care access, improve cultural congru-
ence,and address quality and cost among the growing immi-
grant population and otherunderserved,isolated,and
vulnerable people.The CHW modelpresents an opportunity
to achieve these goals.4-6
Presently, there is a national call for greater use of CHWs
improve the nation’s health.In 2011,the Center for Disease
Controland Prevention (CDC) and the Division forHeart
1 Department of Family Medicine,East Boston Neighborhood Health Center,
East Boston,MA, USA
2 Schoolof Nursing,MGH Institute of Health Professions,Boston,MA, USA
3 College of Nursing and Health Sciences,University of Vermont,Burlington,
VT, USA
4 Partners in Health,Boston,MA, USA
Corresponding Author:
Catherine M. Franklin,Departmentof Family Medicine,East Boston
Neighborhood Health Center,20 Maverick Square,East Boston,MA 02128,
USA.
Email:franklic@ebnhc.org
Health Services Research and
ManagerialEpidemiology
1-9
ª The Author(s) 2015
Reprints and permission:
sagepub.com/journalsPermissions.nav
DOI: 10.1177/2333392815573312
hme.sagepub.com
Creative Commons CC-BY-NC:This article is distributed under the terms ofthe Creative Commons Attribution-NonCommercial3.0 License
(http://www.creativecommons.org/licenses/by-nc/3.0/) which permits non-commercialuse,reproduction and distribution ofthe work without further
permission provided the originalwork is attributed as specified on the SAGE and Open Access page (http://www.uk.sagepub.com/aboutus/openaccess
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Disease and Stroke Prevention published Addressing Chronic
Disease through CHWs: A Policy and Systems-Level
Approach7 which recommended thatstates integrate CHWs
in high-risk communities to prevent chronic disease. Likewise,
the Institute of Medicine (IOM)8 recommended CHWs as part
of their strategic plan to prevent, control, and reduce the impact
of hypertension.In addition,the PatientProtection and
Affordable Care Actmore commonly referred to as the
Affordable Care Act (ACA)9 identified the need to encourage
CHW engagement in health promotion and improving health
outcomes for the medically underserved. Moreover, the CDC10
has called for stronger supportfor CHW programs to help
eliminate health disparities for the prevention and management
of diabetes.
At the same time, several national and international organi-
zations began calling for interprofessional teamwork and team
training as partof the redesign of the health care system.In
2001,the IOM issued ‘‘Crossing the Quality Chasm . . .,’’11
initiated this early call. Nearly a decade later, the World Health
Organization12 identified the urgent,globalneed to integrate
interprofessional education and collaborative practice into ser-
vice, education,and health policy globally in orderto
strengthen primary care health systems.Finally,in 2011,an
expert panel of the Interprofessional Education Collaborative
introduced core competencies for interprofessional collabora-
tive practice.13Moreover, many national health care organiza-
tions14-18
have endorsed the establishment of community-based
interprofessionalteams as partof patientcentered medical
homes (PCMH), a model for primary care redesign.
Despite the strong evidence to support the use of CHWs and
the nationally recognized need for collaborative practice in
care provision,the nature and degree of teamwork and colla-
boration with CHWs within health care teams is not well under-
stood.Therefore,the purpose ofthis integrative literature
review was to examine interprofessional teamwork and colla-
boration with CHWs in research demonstrating positive health
outcomes as a result of CHW intervention
Interprofessionality and Teamwork
Research suggests that interprofessional teamwork and colla-
boration improve patientoutcomes and access to health
care.12,19-30
In addition,those health care workers who serve
as part of a team are more effective and have higher job satis-
faction than those who do not.28,31,32
The concept of ‘‘interprofessionality,’’ coined by D’Amour
and Oandasan33 as a response to fragmented health care prac-
tices,is defined as ‘‘the developmentof a cohesive practice
between professionals from different disciplines. It is the pro-
cess by which professionals reflecton and develop ways of
practicing that provides an integrated and cohesive answer to
the needs of the client/family/population.’’33(p9)Interprofes-
sionality is distinguished from multidisciplinary,which refers
to a process whereby multiple disciplines work on the same
projectin an independentand parallelfashion,33 reflecting a
lower degree of collaboration on the spectrum.
The conceptof ‘‘collaboration,’’identified as criticalto
ensure quality health care,33 is important to understand within
the context of interprofessional teams. Collaboration is desc
as conveying ‘‘the idea of sharing and implies collective acti
oriented toward a common goal, in a spirit of harmony and t
particularly in the contextof health professionals.’’57(p116)
Interprofessionalcollaboration is a ‘‘negotiated agreement
between professionals which values the expertise and contri
tions thatvarious healthcare professionals bring to patient
care’’34(p2)
and is most effective when there is good communi-
cation and a value for diverse opinions among team membe35
In a review of the literature on collaborative practice, D’Amo
et al33 identified the following fourconcepts related to
collaboration: sharing, partnership, interdependency, and po
A team is defined as ‘‘a group of people working together
achieve common purpose forwhich they hold themselves
mutually accountable.’’36(p3) The establishmentof teams
assumes that teams can outperform individuals when the ta
is complex, members have a stake in the outcome, and whe
efficient use of resources is necessary. Key elements of team
work include members having a shared work product, interd
pendenttasks,shared responsibility forproducing results,
commitmentto a common approach,and collective manage-
ment of relationships across organizational boundaries.36
Successful teamwork is necessary for collaboration to occ
Teamwork creates the environment to support the work that
the potentialto resultin collaboration.Collaboration is most
closely related to the synergy created by those on the team.
Collaboration requires two constant and key elements, name
(1) construction of collective action thataddresses the com-
plexity of client needs and (2) the construction of a team life
that integrates the perspectives of each professional where
member experiences respect and trust.33
Modelfor Integrative Review
Rice37 links teamwork and collaboration by identifying
teamwork as ‘‘a mechanism for putting collaboration into
effect.’’37(p62)
Rice identified five assumptions of teamwork that
served as the conceptual framework for this integrative revie
These assumptions are (1) a shared understanding of roles,
values, and goals of the team; (2) team functions in an egali
manner; (3) team functions in a cooperative manner; (4) tea
functions in an interdependent manner; and (5) combined eff
of the team and shared decision making are of greater bene
patients than the effects of the individual disciplines alone.
The assumptions for effective teamwork that will result in
successful collaboration described by Rice37 were operationa-
lized for this review as follows:
1. Shared understanding.Shared understanding of roles,
norms,values,and goals ofthe team:Evidence of
clearly defined goals for projectinterventions,team
member roles,or congruence of values or mission of
team members.For this review,the word ‘‘shared
understanding’’ will be used to refer to this assumption
2 Health Services Research and ManagerialEpidemiology
Disease through CHWs: A Policy and Systems-Level
Approach7 which recommended thatstates integrate CHWs
in high-risk communities to prevent chronic disease. Likewise,
the Institute of Medicine (IOM)8 recommended CHWs as part
of their strategic plan to prevent, control, and reduce the impact
of hypertension.In addition,the PatientProtection and
Affordable Care Actmore commonly referred to as the
Affordable Care Act (ACA)9 identified the need to encourage
CHW engagement in health promotion and improving health
outcomes for the medically underserved. Moreover, the CDC10
has called for stronger supportfor CHW programs to help
eliminate health disparities for the prevention and management
of diabetes.
At the same time, several national and international organi-
zations began calling for interprofessional teamwork and team
training as partof the redesign of the health care system.In
2001,the IOM issued ‘‘Crossing the Quality Chasm . . .,’’11
initiated this early call. Nearly a decade later, the World Health
Organization12 identified the urgent,globalneed to integrate
interprofessional education and collaborative practice into ser-
vice, education,and health policy globally in orderto
strengthen primary care health systems.Finally,in 2011,an
expert panel of the Interprofessional Education Collaborative
introduced core competencies for interprofessional collabora-
tive practice.13Moreover, many national health care organiza-
tions14-18
have endorsed the establishment of community-based
interprofessionalteams as partof patientcentered medical
homes (PCMH), a model for primary care redesign.
Despite the strong evidence to support the use of CHWs and
the nationally recognized need for collaborative practice in
care provision,the nature and degree of teamwork and colla-
boration with CHWs within health care teams is not well under-
stood.Therefore,the purpose ofthis integrative literature
review was to examine interprofessional teamwork and colla-
boration with CHWs in research demonstrating positive health
outcomes as a result of CHW intervention
Interprofessionality and Teamwork
Research suggests that interprofessional teamwork and colla-
boration improve patientoutcomes and access to health
care.12,19-30
In addition,those health care workers who serve
as part of a team are more effective and have higher job satis-
faction than those who do not.28,31,32
The concept of ‘‘interprofessionality,’’ coined by D’Amour
and Oandasan33 as a response to fragmented health care prac-
tices,is defined as ‘‘the developmentof a cohesive practice
between professionals from different disciplines. It is the pro-
cess by which professionals reflecton and develop ways of
practicing that provides an integrated and cohesive answer to
the needs of the client/family/population.’’33(p9)Interprofes-
sionality is distinguished from multidisciplinary,which refers
to a process whereby multiple disciplines work on the same
projectin an independentand parallelfashion,33 reflecting a
lower degree of collaboration on the spectrum.
The conceptof ‘‘collaboration,’’identified as criticalto
ensure quality health care,33 is important to understand within
the context of interprofessional teams. Collaboration is desc
as conveying ‘‘the idea of sharing and implies collective acti
oriented toward a common goal, in a spirit of harmony and t
particularly in the contextof health professionals.’’57(p116)
Interprofessionalcollaboration is a ‘‘negotiated agreement
between professionals which values the expertise and contri
tions thatvarious healthcare professionals bring to patient
care’’34(p2)
and is most effective when there is good communi-
cation and a value for diverse opinions among team membe35
In a review of the literature on collaborative practice, D’Amo
et al33 identified the following fourconcepts related to
collaboration: sharing, partnership, interdependency, and po
A team is defined as ‘‘a group of people working together
achieve common purpose forwhich they hold themselves
mutually accountable.’’36(p3) The establishmentof teams
assumes that teams can outperform individuals when the ta
is complex, members have a stake in the outcome, and whe
efficient use of resources is necessary. Key elements of team
work include members having a shared work product, interd
pendenttasks,shared responsibility forproducing results,
commitmentto a common approach,and collective manage-
ment of relationships across organizational boundaries.36
Successful teamwork is necessary for collaboration to occ
Teamwork creates the environment to support the work that
the potentialto resultin collaboration.Collaboration is most
closely related to the synergy created by those on the team.
Collaboration requires two constant and key elements, name
(1) construction of collective action thataddresses the com-
plexity of client needs and (2) the construction of a team life
that integrates the perspectives of each professional where
member experiences respect and trust.33
Modelfor Integrative Review
Rice37 links teamwork and collaboration by identifying
teamwork as ‘‘a mechanism for putting collaboration into
effect.’’37(p62)
Rice identified five assumptions of teamwork that
served as the conceptual framework for this integrative revie
These assumptions are (1) a shared understanding of roles,
values, and goals of the team; (2) team functions in an egali
manner; (3) team functions in a cooperative manner; (4) tea
functions in an interdependent manner; and (5) combined eff
of the team and shared decision making are of greater bene
patients than the effects of the individual disciplines alone.
The assumptions for effective teamwork that will result in
successful collaboration described by Rice37 were operationa-
lized for this review as follows:
1. Shared understanding.Shared understanding of roles,
norms,values,and goals ofthe team:Evidence of
clearly defined goals for projectinterventions,team
member roles,or congruence of values or mission of
team members.For this review,the word ‘‘shared
understanding’’ will be used to refer to this assumption
2 Health Services Research and ManagerialEpidemiology
2. Egalitarianism.Team functioning in an egalitarian
manner: Patients and families are part of the health care
team as evidenced by respect for their input into pre-
ferences, decision making, or goal setting.
3. Cooperation.Team functioning in a cooperative man-
ner:A working together thatrecognizes and respects
involvement and contributions of all members38as evi-
denced by team meetings or joint training.
4. Interdependence.Team functioning in an interdepen-
dentmanner:Absence ofindependence orlack of
autonomy39as evidenced by team discussions and con-
sultation between role groups.
5. Synergy. The combined efforts of the team and the shared
decision making result in a greater benefit to the patient
than the effects of the individual disciplines alone. For this
review, the word ‘‘synergy,’’ defined as a way of working
that creates an outcome that is better than the outcome any
one participant could create alone,39will be used to refer
to this assumption as evidenced when outcomes of
interventions are attributed to the collective team effort.
Aim
The aim of this integrative review was to examine interprofes-
sionalteamwork and collaboration with CHWs in research
demonstrating positive health outcomes as a resultof CHW
intervention.Key questions thatguided the review process
were (1) did the CHW function as a member of the healthcare
team? and (2) were assumptions of teamwork between CHWs
and health care teams present as defined by Rice?37
Methods
An integrative review methodology40was used to identify evi-
dence ofRice’s five assumptions ofeffective teamwork
between CHWs and providers from two majorsystematic
reviews of the literature.1,2A review of the literature was con-
ducted to identify peer-reviewed research reporting health out-
comes of CHW interventions. These studies were published in
English from 1996 to 2013 using the following electronic data-
bases: MEDLINE, PsychINFO, Cochrane Reviews, CINAHL,
and the World Wide Web. Key search terms included primary
care, health outcomes, community health worker(s) and syno-
nyms for CHW including lay health worker, outreach worker,
health advocate, and promotora de salud. Using these terms, we
found two comprehensive systematic reviews ofresearch
assessing the effect of CHW interventions.
The firstsystematic review,conducted by the Agency for
Healthcare Research and Quality,(AHRQ), 1 identified
research conducted between 1980 through November 2008 that
examined cost,outcomes,and characteristics of CHW inter-
ventions.Its review included allstudies conducted in the
United States and published in English. It excluded studies that
had fewer than 40 participants, were not original research, and
did notreporton topics relative to the key questions of the
study.It rated the quality of the studies as good, fair,or poor
based on the AHRQ Comparative Effectiveness Guide.41 In
total, these authors identified 53 original research studies.
The second systematic review reported by The New Eng-
land Comparative Effectiveness Public Advisory Council2 con-
ducted an update to the AHRQ study1 systematic review from
January 2008 through April2013 focusing on the impactof
CHW interventions on health outcomes using the same rigor
ous search criteria and quality ratings based on the AHRQ
Comparative Effectiveness Guide.41 This search yielded 18
studies. From these, a new database of 47 studies of good a
fair quality spanning the time frame of 1980 through 2013 w
created.The new database was comprised of 29 of the 53
AHRQ studies that focused solely on CHW interventions with
the newly added 18 studies thatmetcriteria in their update.
Excluded from theirreview were studies thatfocused on
improved patient knowledge or satisfaction. These 47 studie
representing the best evidence in the literature reporting po
tive health outcomes as a result of CHW interventions over a
period of33 years,form the database forthis integrative
review.
Data Abstraction
The following data were abstracted from each of the 47 rese
reports: study aim, presence of a team that included the CH
and assumptions of teamwork (shared understanding,egalitar-
ianism, cooperation, and interdependence, and synergy). Stu
that reported the same intervention in more than one public
were examined separately and counted as one study.
Data Reduction
Each study was examined to identify whether or not the CHW
a member of the health care team. A study was coded as ha
evidence of team if the CHW was reported to be a member o
multidisciplinary or interprofessional team or work with at le
one member from any other health profession. Thirty-five stu
did not report the inclusion of a CHW working as a member o
health care team and thus these studies were excluded.The
remaining 12 studies, which created the database for the re
were examined for evidence of effective teamwork-shared
understanding,team functioning in an egalitarian,cooperative,
and interdependentmanner,and synergy.The previously
described assumptions for effective teamwork were used as
coding schema, namely, (1) shared understanding, (2) egalit
ism, (3) cooperation, (4) interdependence, and (5) synergy.
Results
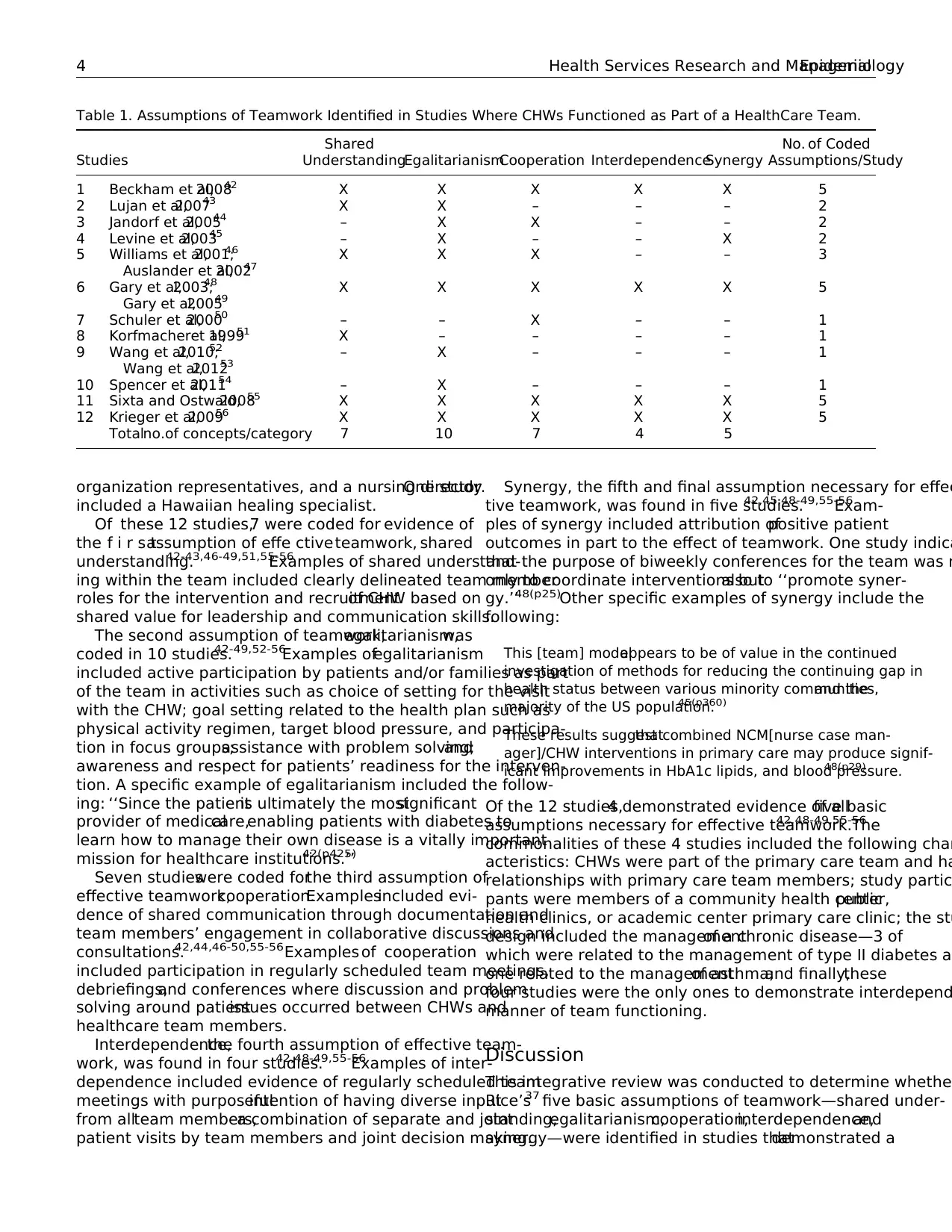
Analysis of the 47 best evidence studies revealed 12 studies
reported the CHW functioning as part of a health care team.42-56
See Table 1 for data display. The composition of the teams w
most often CHWs with nurses, physicians, and dietitians. Les
frequently, teams consisted of CHWs with social workers, pro
ect coordinators, research assistants, psychologists, commu
Franklin et al 3
manner: Patients and families are part of the health care
team as evidenced by respect for their input into pre-
ferences, decision making, or goal setting.
3. Cooperation.Team functioning in a cooperative man-
ner:A working together thatrecognizes and respects
involvement and contributions of all members38as evi-
denced by team meetings or joint training.
4. Interdependence.Team functioning in an interdepen-
dentmanner:Absence ofindependence orlack of
autonomy39as evidenced by team discussions and con-
sultation between role groups.
5. Synergy. The combined efforts of the team and the shared
decision making result in a greater benefit to the patient
than the effects of the individual disciplines alone. For this
review, the word ‘‘synergy,’’ defined as a way of working
that creates an outcome that is better than the outcome any
one participant could create alone,39will be used to refer
to this assumption as evidenced when outcomes of
interventions are attributed to the collective team effort.
Aim
The aim of this integrative review was to examine interprofes-
sionalteamwork and collaboration with CHWs in research
demonstrating positive health outcomes as a resultof CHW
intervention.Key questions thatguided the review process
were (1) did the CHW function as a member of the healthcare
team? and (2) were assumptions of teamwork between CHWs
and health care teams present as defined by Rice?37
Methods
An integrative review methodology40was used to identify evi-
dence ofRice’s five assumptions ofeffective teamwork
between CHWs and providers from two majorsystematic
reviews of the literature.1,2A review of the literature was con-
ducted to identify peer-reviewed research reporting health out-
comes of CHW interventions. These studies were published in
English from 1996 to 2013 using the following electronic data-
bases: MEDLINE, PsychINFO, Cochrane Reviews, CINAHL,
and the World Wide Web. Key search terms included primary
care, health outcomes, community health worker(s) and syno-
nyms for CHW including lay health worker, outreach worker,
health advocate, and promotora de salud. Using these terms, we
found two comprehensive systematic reviews ofresearch
assessing the effect of CHW interventions.
The firstsystematic review,conducted by the Agency for
Healthcare Research and Quality,(AHRQ), 1 identified
research conducted between 1980 through November 2008 that
examined cost,outcomes,and characteristics of CHW inter-
ventions.Its review included allstudies conducted in the
United States and published in English. It excluded studies that
had fewer than 40 participants, were not original research, and
did notreporton topics relative to the key questions of the
study.It rated the quality of the studies as good, fair,or poor
based on the AHRQ Comparative Effectiveness Guide.41 In
total, these authors identified 53 original research studies.
The second systematic review reported by The New Eng-
land Comparative Effectiveness Public Advisory Council2 con-
ducted an update to the AHRQ study1 systematic review from
January 2008 through April2013 focusing on the impactof
CHW interventions on health outcomes using the same rigor
ous search criteria and quality ratings based on the AHRQ
Comparative Effectiveness Guide.41 This search yielded 18
studies. From these, a new database of 47 studies of good a
fair quality spanning the time frame of 1980 through 2013 w
created.The new database was comprised of 29 of the 53
AHRQ studies that focused solely on CHW interventions with
the newly added 18 studies thatmetcriteria in their update.
Excluded from theirreview were studies thatfocused on
improved patient knowledge or satisfaction. These 47 studie
representing the best evidence in the literature reporting po
tive health outcomes as a result of CHW interventions over a
period of33 years,form the database forthis integrative
review.
Data Abstraction
The following data were abstracted from each of the 47 rese
reports: study aim, presence of a team that included the CH
and assumptions of teamwork (shared understanding,egalitar-
ianism, cooperation, and interdependence, and synergy). Stu
that reported the same intervention in more than one public
were examined separately and counted as one study.
Data Reduction
Each study was examined to identify whether or not the CHW
a member of the health care team. A study was coded as ha
evidence of team if the CHW was reported to be a member o
multidisciplinary or interprofessional team or work with at le
one member from any other health profession. Thirty-five stu
did not report the inclusion of a CHW working as a member o
health care team and thus these studies were excluded.The
remaining 12 studies, which created the database for the re
were examined for evidence of effective teamwork-shared
understanding,team functioning in an egalitarian,cooperative,
and interdependentmanner,and synergy.The previously
described assumptions for effective teamwork were used as
coding schema, namely, (1) shared understanding, (2) egalit
ism, (3) cooperation, (4) interdependence, and (5) synergy.
Results
Analysis of the 47 best evidence studies revealed 12 studies
reported the CHW functioning as part of a health care team.42-56
See Table 1 for data display. The composition of the teams w
most often CHWs with nurses, physicians, and dietitians. Les
frequently, teams consisted of CHWs with social workers, pro
ect coordinators, research assistants, psychologists, commu
Franklin et al 3
organization representatives, and a nursing director.One study
included a Hawaiian healing specialist.
Of these 12 studies,7 were coded for evidence of
the f i r s tassumption of effe ctiveteamwork, shared
understanding.42-43,46-49,51,55-56
Examples of shared understand-
ing within the team included clearly delineated team member
roles for the intervention and recruitmentof CHW based on
shared value for leadership and communication skills.
The second assumption of teamwork,egalitarianism,was
coded in 10 studies.42-49,52-56
Examples ofegalitarianism
included active participation by patients and/or families as part
of the team in activities such as choice of setting for the visit
with the CHW; goal setting related to the health plan such as
physical activity regimen, target blood pressure, and participa-
tion in focus groups;assistance with problem solving;and
awareness and respect for patients’ readiness for the interven-
tion. A specific example of egalitarianism included the follow-
ing: ‘‘Since the patientis ultimately the mostsignificant
provider of medicalcare,enabling patients with diabetes to
learn how to manage their own disease is a vitally important
mission for healthcare institutions.’’42(p425)
Seven studieswere coded forthe third assumption of
effective teamwork,cooperation.Examplesincluded evi-
dence of shared communication through documentation and
team members’ engagement in collaborative discussions and
consultations.42,44,46-50,55-56Examples of cooperation
included participation in regularly scheduled team meetings,
debriefings,and conferences where discussion and problem
solving around patientissues occurred between CHWs and
healthcare team members.
Interdependence,the fourth assumption of effective team-
work, was found in four studies.42,48-49,55-56
Examples of inter-
dependence included evidence of regularly scheduled team
meetings with purposefulintention of having diverse input
from allteam members,a combination of separate and joint
patient visits by team members and joint decision making.
Synergy, the fifth and final assumption necessary for effec
tive teamwork, was found in five studies.42,45,48-49,55-56
Exam-
ples of synergy included attribution ofpositive patient
outcomes in part to the effect of teamwork. One study indica
that the purpose of biweekly conferences for the team was n
only to coordinate interventions butalso to ‘‘promote syner-
gy.’’48(p25)Other specific examples of synergy include the
following:
This [team] modelappears to be of value in the continued
investigation of methods for reducing the continuing gap in
health status between various minority communities,and the
majority of the US population.45(p360)
These results suggestthatcombined NCM[nurse case man-
ager]/CHW interventions in primary care may produce signif-
icant improvements in HbA1c lipids, and blood pressure.48(p29)
Of the 12 studies,4 demonstrated evidence of allfive basic
assumptions necessary for effective teamwork.42,48-49,55-56
The
commonalities of these 4 studies included the following char
acteristics: CHWs were part of the primary care team and ha
relationships with primary care team members; study partic
pants were members of a community health center,public
health clinics, or academic center primary care clinic; the stu
design included the managementof a chronic disease—3 of
which were related to the management of type II diabetes an
one related to the managementof asthma;and finally,these
four studies were the only ones to demonstrate interdepend
manner of team functioning.
Discussion
This integrative review was conducted to determine whether
Rice’s37 five basic assumptions of teamwork—shared under-
standing,egalitarianism,cooperation,interdependence,and
synergy—were identified in studies thatdemonstrated a
Table 1. Assumptions of Teamwork Identified in Studies Where CHWs Functioned as Part of a HealthCare Team.
Studies
Shared
UnderstandingEgalitarianismCooperation InterdependenceSynergy
No. of Coded
Assumptions/Study
1 Beckham et al,200842 X X X X X 5
2 Lujan et al,200743 X X – – – 2
3 Jandorf et al,200544 – X X – – 2
4 Levine et al,200345 – X – – X 2
5 Williams et al,2001;46
Auslander et al,200247
X X X – – 3
6 Gary et al,2003;48
Gary et al,200549
X X X X X 5
7 Schuler et al,200050 – – X – – 1
8 Korfmacheret al,199951 X – – – – 1
9 Wang et al,2010;52
Wang et al,201253
– X – – – 1
10 Spencer et al,201154 – X – – – 1
11 Sixta and Ostwald,200855 X X X X X 5
12 Krieger et al,200956 X X X X X 5
Totalno.of concepts/category 7 10 7 4 5
4 Health Services Research and ManagerialEpidemiology
included a Hawaiian healing specialist.
Of these 12 studies,7 were coded for evidence of
the f i r s tassumption of effe ctiveteamwork, shared
understanding.42-43,46-49,51,55-56
Examples of shared understand-
ing within the team included clearly delineated team member
roles for the intervention and recruitmentof CHW based on
shared value for leadership and communication skills.
The second assumption of teamwork,egalitarianism,was
coded in 10 studies.42-49,52-56
Examples ofegalitarianism
included active participation by patients and/or families as part
of the team in activities such as choice of setting for the visit
with the CHW; goal setting related to the health plan such as
physical activity regimen, target blood pressure, and participa-
tion in focus groups;assistance with problem solving;and
awareness and respect for patients’ readiness for the interven-
tion. A specific example of egalitarianism included the follow-
ing: ‘‘Since the patientis ultimately the mostsignificant
provider of medicalcare,enabling patients with diabetes to
learn how to manage their own disease is a vitally important
mission for healthcare institutions.’’42(p425)
Seven studieswere coded forthe third assumption of
effective teamwork,cooperation.Examplesincluded evi-
dence of shared communication through documentation and
team members’ engagement in collaborative discussions and
consultations.42,44,46-50,55-56Examples of cooperation
included participation in regularly scheduled team meetings,
debriefings,and conferences where discussion and problem
solving around patientissues occurred between CHWs and
healthcare team members.
Interdependence,the fourth assumption of effective team-
work, was found in four studies.42,48-49,55-56
Examples of inter-
dependence included evidence of regularly scheduled team
meetings with purposefulintention of having diverse input
from allteam members,a combination of separate and joint
patient visits by team members and joint decision making.
Synergy, the fifth and final assumption necessary for effec
tive teamwork, was found in five studies.42,45,48-49,55-56
Exam-
ples of synergy included attribution ofpositive patient
outcomes in part to the effect of teamwork. One study indica
that the purpose of biweekly conferences for the team was n
only to coordinate interventions butalso to ‘‘promote syner-
gy.’’48(p25)Other specific examples of synergy include the
following:
This [team] modelappears to be of value in the continued
investigation of methods for reducing the continuing gap in
health status between various minority communities,and the
majority of the US population.45(p360)
These results suggestthatcombined NCM[nurse case man-
ager]/CHW interventions in primary care may produce signif-
icant improvements in HbA1c lipids, and blood pressure.48(p29)
Of the 12 studies,4 demonstrated evidence of allfive basic
assumptions necessary for effective teamwork.42,48-49,55-56
The
commonalities of these 4 studies included the following char
acteristics: CHWs were part of the primary care team and ha
relationships with primary care team members; study partic
pants were members of a community health center,public
health clinics, or academic center primary care clinic; the stu
design included the managementof a chronic disease—3 of
which were related to the management of type II diabetes an
one related to the managementof asthma;and finally,these
four studies were the only ones to demonstrate interdepend
manner of team functioning.
Discussion
This integrative review was conducted to determine whether
Rice’s37 five basic assumptions of teamwork—shared under-
standing,egalitarianism,cooperation,interdependence,and
synergy—were identified in studies thatdemonstrated a
Table 1. Assumptions of Teamwork Identified in Studies Where CHWs Functioned as Part of a HealthCare Team.
Studies
Shared
UnderstandingEgalitarianismCooperation InterdependenceSynergy
No. of Coded
Assumptions/Study
1 Beckham et al,200842 X X X X X 5
2 Lujan et al,200743 X X – – – 2
3 Jandorf et al,200544 – X X – – 2
4 Levine et al,200345 – X – – X 2
5 Williams et al,2001;46
Auslander et al,200247
X X X – – 3
6 Gary et al,2003;48
Gary et al,200549
X X X X X 5
7 Schuler et al,200050 – – X – – 1
8 Korfmacheret al,199951 X – – – – 1
9 Wang et al,2010;52
Wang et al,201253
– X – – – 1
10 Spencer et al,201154 – X – – – 1
11 Sixta and Ostwald,200855 X X X X X 5
12 Krieger et al,200956 X X X X X 5
Totalno.of concepts/category 7 10 7 4 5
4 Health Services Research and ManagerialEpidemiology
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
positive effect on patient outcomes when CHWs functionedas
partof healthcare teams.Two systematic reviews of CHW
interventions with positive health outcomes thatspanned 33
years (1980-2013) were used as the basis for this integrative
review. Findings reveal that in 12 of the 47 studies that com-
prised the database, CHWs functioned as part of a health care
team.Of these 12 studies,all reported atleastone aspectof
interprofessionalteamwork.This finding supports the IOM11
and World Health Organization12 call for the integration of
interprofessional teamwork as part of health care education and
practice redesign to build stronger health care systems. Assum-
ing that effective teamwork facilitates collaboration, organiza-
tions that create interprofessional teams will be positioned to
better attain positive patient health outcomes.
In over half of the 12 studies in the database in this inte-
grative review, there was evidence of a shared understanding of
roles,norms,values,or goals among team members42-43,46-
49,51,55-56
and cooperative manner of functioning.42,44,46-50,55-56
These findings supportthe idea thatmutualunderstanding,
respect for individual roles and a sharing of goals and values,
and cooperation are important for effective teamwork between
CHWs and health care team members.These findings support
the importance ofpartnership and the need forregular
communication among team members.
In the majority of the studies,42-49,52-56
health care teams
functioned incorporating egalitarianism. Engaging patients and
families as active participants in the healthcare team is consis-
tent with the 2001 IOM11 report and is a fundamental concept
underpinning the Patient Centered Medical Home.14This team
characteristic represents a paradigm shift from a traditionally
paternalistic system where health care providers make deci-
sions independent of the patient’s input to one that is inclusive
and empowering for both patients and families.
A third of the 12 studies42,48-49,55-56
demonstrated evidence of
interdependence suggesting thatthese teams functioned as a
whole referring to and consulting with one another regardless
of position and designated leadership role. These findings exem-
plify interprofessional work,distinguishing it from the parallel
process of multidisciplinary work.57 Interdependence between
health care team members supports a shift away from traditional
barriers which include medical dominance, issues of professional
turf, the sense of exclusive authority that may be developed in
professional training, and lack of awareness of other team mem-
bers’ skills and roles.37These same 4 studies42, 48-49, 55-56
demon-
strated evidence of all of the assumptions of effective teamwork
and may serve as exemplars for effective teamwork between
CHWs and healthcare team members.
Less than half of the studies42,45,48-49,55-56
demonstrated evi-
dence thatteamwork led to a synergistic effectfor patients.
This is the desired and ultimate goal of interprofessional col-
laboration. The team recognizes and strives to work together to
ensure that the outcome is better than any one individual mem-
ber could achieve alone. These findings support the investment
in the developmentof interprofessionalteams thatinclude
CHWs for primary care practices as called for by the ACA9
and IOM58 and undergirds the PCMH model.14
Implications
This integrative review demonstrates a beginning understan
ing of whateffective teamwork and successfulcollaboration
looks like when a CHW is integrated into interprofessional
health care teams where the associated positive health out-
comes are credited to CHW interventions. Each of the assum
tions exhibited alone represents a key aspectin laying a
foundation for interprofessional teamwork. These elements o
teamwork need to be present and supported in order to fost
successful collaboration.
Four studies in this integrative review exhibited all of the
five assumptions for effective teamwork according to Rice.37
The characteristics described in these studies suggest that t
best opportunity for successful teamwork and collaboration
when CHWs are integrated into a primary care health team,
reflect the population they serve, are trained in cultural sens
tivity, and participate in the management of chronic illnesse
Additionalcharacteristics cited in these four studies suggest
that effective teamwork and collaboration exist when patien
are members of a community health, public health, or acade
primary care clinic.
These findings have implications for allmembers of the
healthcare team as redesign of the workforce in practices is
implemented.Members mustidentify and engage with their
team.Incorporating these assumptions willnot necessarily
come naturally to healthcare teams as many health professi
als are educated to practice in parallel fashion to other disci
plines. Accepting CHWs as equitable membersof the
healthcare team may be a challenge for teams that are accu
tomed to the medical provider assuming the role as the lead
and directing unlicensed staff.All team members willneed
training in how individuals can function at maximal capacity
within a team. Experiential team-based pilots with continuou
evaluation and identification for improvement should also be
considered. Support from senior leadership in terms of missi
and values,stated expectations,and financialand human
resources will also be necessary.
The addition ofunlicensed health care workers such as
CHWs onto interprofessionalteams improves access and
patient outcomes with respect to chronic illnesses and reduc
health disparities. The CHWs bring knowledge of culture and
communities, relationships with members of the communitie
and experience in health screening, prevention, and health p
motion.Community health centers and public health clinics,
predominantly located in low income and medically under-
served neighborhoods, are committed to hiring from their lo
communities.59,60
Patient care can no longer be delivered within the silos of
individual health professions.Workforce redesign is essential
to accommodate the growing number of individuals entering
the health care system. With the emphasis on the developm
of primary care teams within the PCMH movement,14primary
care practices will become the hub of access to care. Theref
it is criticalfor health care policy makers,researchers,and
clinicians to examine the feasibility and value of integrating
Franklin et al 5
partof healthcare teams.Two systematic reviews of CHW
interventions with positive health outcomes thatspanned 33
years (1980-2013) were used as the basis for this integrative
review. Findings reveal that in 12 of the 47 studies that com-
prised the database, CHWs functioned as part of a health care
team.Of these 12 studies,all reported atleastone aspectof
interprofessionalteamwork.This finding supports the IOM11
and World Health Organization12 call for the integration of
interprofessional teamwork as part of health care education and
practice redesign to build stronger health care systems. Assum-
ing that effective teamwork facilitates collaboration, organiza-
tions that create interprofessional teams will be positioned to
better attain positive patient health outcomes.
In over half of the 12 studies in the database in this inte-
grative review, there was evidence of a shared understanding of
roles,norms,values,or goals among team members42-43,46-
49,51,55-56
and cooperative manner of functioning.42,44,46-50,55-56
These findings supportthe idea thatmutualunderstanding,
respect for individual roles and a sharing of goals and values,
and cooperation are important for effective teamwork between
CHWs and health care team members.These findings support
the importance ofpartnership and the need forregular
communication among team members.
In the majority of the studies,42-49,52-56
health care teams
functioned incorporating egalitarianism. Engaging patients and
families as active participants in the healthcare team is consis-
tent with the 2001 IOM11 report and is a fundamental concept
underpinning the Patient Centered Medical Home.14This team
characteristic represents a paradigm shift from a traditionally
paternalistic system where health care providers make deci-
sions independent of the patient’s input to one that is inclusive
and empowering for both patients and families.
A third of the 12 studies42,48-49,55-56
demonstrated evidence of
interdependence suggesting thatthese teams functioned as a
whole referring to and consulting with one another regardless
of position and designated leadership role. These findings exem-
plify interprofessional work,distinguishing it from the parallel
process of multidisciplinary work.57 Interdependence between
health care team members supports a shift away from traditional
barriers which include medical dominance, issues of professional
turf, the sense of exclusive authority that may be developed in
professional training, and lack of awareness of other team mem-
bers’ skills and roles.37These same 4 studies42, 48-49, 55-56
demon-
strated evidence of all of the assumptions of effective teamwork
and may serve as exemplars for effective teamwork between
CHWs and healthcare team members.
Less than half of the studies42,45,48-49,55-56
demonstrated evi-
dence thatteamwork led to a synergistic effectfor patients.
This is the desired and ultimate goal of interprofessional col-
laboration. The team recognizes and strives to work together to
ensure that the outcome is better than any one individual mem-
ber could achieve alone. These findings support the investment
in the developmentof interprofessionalteams thatinclude
CHWs for primary care practices as called for by the ACA9
and IOM58 and undergirds the PCMH model.14
Implications
This integrative review demonstrates a beginning understan
ing of whateffective teamwork and successfulcollaboration
looks like when a CHW is integrated into interprofessional
health care teams where the associated positive health out-
comes are credited to CHW interventions. Each of the assum
tions exhibited alone represents a key aspectin laying a
foundation for interprofessional teamwork. These elements o
teamwork need to be present and supported in order to fost
successful collaboration.
Four studies in this integrative review exhibited all of the
five assumptions for effective teamwork according to Rice.37
The characteristics described in these studies suggest that t
best opportunity for successful teamwork and collaboration
when CHWs are integrated into a primary care health team,
reflect the population they serve, are trained in cultural sens
tivity, and participate in the management of chronic illnesse
Additionalcharacteristics cited in these four studies suggest
that effective teamwork and collaboration exist when patien
are members of a community health, public health, or acade
primary care clinic.
These findings have implications for allmembers of the
healthcare team as redesign of the workforce in practices is
implemented.Members mustidentify and engage with their
team.Incorporating these assumptions willnot necessarily
come naturally to healthcare teams as many health professi
als are educated to practice in parallel fashion to other disci
plines. Accepting CHWs as equitable membersof the
healthcare team may be a challenge for teams that are accu
tomed to the medical provider assuming the role as the lead
and directing unlicensed staff.All team members willneed
training in how individuals can function at maximal capacity
within a team. Experiential team-based pilots with continuou
evaluation and identification for improvement should also be
considered. Support from senior leadership in terms of missi
and values,stated expectations,and financialand human
resources will also be necessary.
The addition ofunlicensed health care workers such as
CHWs onto interprofessionalteams improves access and
patient outcomes with respect to chronic illnesses and reduc
health disparities. The CHWs bring knowledge of culture and
communities, relationships with members of the communitie
and experience in health screening, prevention, and health p
motion.Community health centers and public health clinics,
predominantly located in low income and medically under-
served neighborhoods, are committed to hiring from their lo
communities.59,60
Patient care can no longer be delivered within the silos of
individual health professions.Workforce redesign is essential
to accommodate the growing number of individuals entering
the health care system. With the emphasis on the developm
of primary care teams within the PCMH movement,14primary
care practices will become the hub of access to care. Theref
it is criticalfor health care policy makers,researchers,and
clinicians to examine the feasibility and value of integrating
Franklin et al 5
CHWs into primary care while stillpreserving their role as
advocates in community-related activities and initiatives.
Several recently published reports address the integration of
CHWs into PCMH health care teams and highlight the need for
clearly defined team roles,education of both providers and
CHWs about their respective roles, teambuilding, clinical and
management training of CHWs, clear systems for communica-
tion, an evaluation plan, and institutional protocols to support
the integration of CHWs into healthcare teams.61-63
Additional
work is needed to examine the best methods to provide team
training, program evaluation,role clarity, and team
communication.
The integration of interprofessionalteamwork and colla-
boration with primary care workforce redesign thatincludes
CHWs sits on the brink of bridging the primary care and public
health gap as described by the IOM.58This integration presents
an opportunity to reduce cost and health disparities as well as
improve access,chronic illness management,and patient and
team satisfaction.It holds promise as a model that could pro-
mote overall health of individuals,families and communities
thereby strengthening the healthcare system overall.
Limitations
The findings of this integrative review mustbe examined in
light of its limitations. Primarily, it examined studies of health
outcomes for individuals as a result of CHW intervention that
were not designed specifically to examine the effect of team-
work and collaboration. As a result, it is possible that elements
of teamwork and collaborative relationships were present but
were not reported.In addition,it is important to note that the
35 studies that did not report teamwork between CHW and care
teams also achieved positive patientoutcomes.The factthat
neither teamwork nor collaboration within the healthcare team
was discussed does notdiminish the importance ofthese
outcomes.
Conclusion
This integrative review identified evidence of interprofes-
sional teamwork and collaboration between CHWs within the
healthcare team from research,which demonstrated positive
health outcomes as a result of CHW intervention. These find-
ings are importantas we begin to understand the role of
CHWs in interprofessionalteams.Further study of the out-
comes ofteamwork and collaboration involving CHWs is
needed to understand the potentialof this interprofessional
model.
Acknowledgements
Jessica Bell,MS Director of the Library and InstructionalDesign
MGH Institute of Health Professions, Boston, MA Provided assistance
with literature review and methods in library science.Marisa Capo-
greco, BS DoctoralStudent, Occupational Therapy MGH Institute of
Health Professions,Boston,MA Provided technicalwriting support
funded by the Schoolof Nursing, MGH Institute of Health
Professions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respec
the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research,author-
ship, and/or publication of this article.
References
1. Viswanathan M,Kraschnewski J,Nishikawa B, et al.Outcomes
of community health worker interventions.Evid Rep Technol
Assess.AssessmentNo. 181.AHRQ Publication No.09-E014.
Rockville,MD: Agency for Healthcare Research and Quality.
June 2009.
2. The New England Comparative Effectiveness Public Advisory
Council. Community health workers: a review of program evolu
tion, evidence on effectiveness and value, and status of workfo
development in New England: The Institute for Clinical and Eco
nomic Review.Web site.http://cepac.icer-review.org/wp-con-
tent/uploads/2011/04/CHW-Final-Report-07-26-MASTER1.pdf.
Published May 24, 2013. Updated, July, 2013. Accessed April 2,
2014.
3. Massachusetts Department of Public Health.Community health
workers in Massachusetts:improving health care and public
health.2009.Web site.http://www.mass.gov/eohhs/docs/dph/
com-health/com-health-workers/legislature-report.pdf.Published
December, 2009. Accessed April 6, 2014.
4. American Public Health Association.Supportfor community
health workers to increase health access and to reduce health
inequities.Policy number 20091.Web site.http://www.apha.
org/policies-and-advocacy/public-health-policy-statements/
policy-database/2014/07/09/14/19/support-for-community-
health-workers-to-increase-health-access-and-to-reduce-health
inequities.Updated 2009.Published November10, 2009.
Accessed April 2, 2014.
5. U.S. Department of Health and Human Services Health Resourc
and Services Administration Bureau of Health Profession. Com-
munity health workers evidence-based models toolbox:HRSA
office of ruralhealth policy.2011.Web site.http://www.hrsa.
gov/ruralhealth/pdf/chwtoolkit.pdf.Published August,2011.
Accessed July 10, 2014.
6. U.S. Department of Health and Human Services Bureau of Heal
Professions. Community health worker national workforce study
2007.Web site.http://bhpr.hrsa.gov/healthworkforce/reports/
chwstudy2007.pdf. Published March, 2007. Accessed March 10
2014.
7. Center for Disease Controland Prevention.Addressing chronic
disease through community health workers: a policy and system
level approach. 2011. Web site. http://www.cdc.gov/dhdsp/docs
chw_brief.pdf. Published 2011. Accessed July 7, 2014.
8. Institute of Medicine.A population-based policy and systems
change approach to preventand controlhypertension.The
NationalAcademies Press.Web site.http://www.iom.edu/
Reports/2010/A-Population-Based-Policy-and-Systems-Change-
Approach-to-Prevent-and-Control-Hypertension.aspx.Published
February 22, 2010. Accessed April 12, 2014.
6 Health Services Research and ManagerialEpidemiology
advocates in community-related activities and initiatives.
Several recently published reports address the integration of
CHWs into PCMH health care teams and highlight the need for
clearly defined team roles,education of both providers and
CHWs about their respective roles, teambuilding, clinical and
management training of CHWs, clear systems for communica-
tion, an evaluation plan, and institutional protocols to support
the integration of CHWs into healthcare teams.61-63
Additional
work is needed to examine the best methods to provide team
training, program evaluation,role clarity, and team
communication.
The integration of interprofessionalteamwork and colla-
boration with primary care workforce redesign thatincludes
CHWs sits on the brink of bridging the primary care and public
health gap as described by the IOM.58This integration presents
an opportunity to reduce cost and health disparities as well as
improve access,chronic illness management,and patient and
team satisfaction.It holds promise as a model that could pro-
mote overall health of individuals,families and communities
thereby strengthening the healthcare system overall.
Limitations
The findings of this integrative review mustbe examined in
light of its limitations. Primarily, it examined studies of health
outcomes for individuals as a result of CHW intervention that
were not designed specifically to examine the effect of team-
work and collaboration. As a result, it is possible that elements
of teamwork and collaborative relationships were present but
were not reported.In addition,it is important to note that the
35 studies that did not report teamwork between CHW and care
teams also achieved positive patientoutcomes.The factthat
neither teamwork nor collaboration within the healthcare team
was discussed does notdiminish the importance ofthese
outcomes.
Conclusion
This integrative review identified evidence of interprofes-
sional teamwork and collaboration between CHWs within the
healthcare team from research,which demonstrated positive
health outcomes as a result of CHW intervention. These find-
ings are importantas we begin to understand the role of
CHWs in interprofessionalteams.Further study of the out-
comes ofteamwork and collaboration involving CHWs is
needed to understand the potentialof this interprofessional
model.
Acknowledgements
Jessica Bell,MS Director of the Library and InstructionalDesign
MGH Institute of Health Professions, Boston, MA Provided assistance
with literature review and methods in library science.Marisa Capo-
greco, BS DoctoralStudent, Occupational Therapy MGH Institute of
Health Professions,Boston,MA Provided technicalwriting support
funded by the Schoolof Nursing, MGH Institute of Health
Professions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respec
the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research,author-
ship, and/or publication of this article.
References
1. Viswanathan M,Kraschnewski J,Nishikawa B, et al.Outcomes
of community health worker interventions.Evid Rep Technol
Assess.AssessmentNo. 181.AHRQ Publication No.09-E014.
Rockville,MD: Agency for Healthcare Research and Quality.
June 2009.
2. The New England Comparative Effectiveness Public Advisory
Council. Community health workers: a review of program evolu
tion, evidence on effectiveness and value, and status of workfo
development in New England: The Institute for Clinical and Eco
nomic Review.Web site.http://cepac.icer-review.org/wp-con-
tent/uploads/2011/04/CHW-Final-Report-07-26-MASTER1.pdf.
Published May 24, 2013. Updated, July, 2013. Accessed April 2,
2014.
3. Massachusetts Department of Public Health.Community health
workers in Massachusetts:improving health care and public
health.2009.Web site.http://www.mass.gov/eohhs/docs/dph/
com-health/com-health-workers/legislature-report.pdf.Published
December, 2009. Accessed April 6, 2014.
4. American Public Health Association.Supportfor community
health workers to increase health access and to reduce health
inequities.Policy number 20091.Web site.http://www.apha.
org/policies-and-advocacy/public-health-policy-statements/
policy-database/2014/07/09/14/19/support-for-community-
health-workers-to-increase-health-access-and-to-reduce-health
inequities.Updated 2009.Published November10, 2009.
Accessed April 2, 2014.
5. U.S. Department of Health and Human Services Health Resourc
and Services Administration Bureau of Health Profession. Com-
munity health workers evidence-based models toolbox:HRSA
office of ruralhealth policy.2011.Web site.http://www.hrsa.
gov/ruralhealth/pdf/chwtoolkit.pdf.Published August,2011.
Accessed July 10, 2014.
6. U.S. Department of Health and Human Services Bureau of Heal
Professions. Community health worker national workforce study
2007.Web site.http://bhpr.hrsa.gov/healthworkforce/reports/
chwstudy2007.pdf. Published March, 2007. Accessed March 10
2014.
7. Center for Disease Controland Prevention.Addressing chronic
disease through community health workers: a policy and system
level approach. 2011. Web site. http://www.cdc.gov/dhdsp/docs
chw_brief.pdf. Published 2011. Accessed July 7, 2014.
8. Institute of Medicine.A population-based policy and systems
change approach to preventand controlhypertension.The
NationalAcademies Press.Web site.http://www.iom.edu/
Reports/2010/A-Population-Based-Policy-and-Systems-Change-
Approach-to-Prevent-and-Control-Hypertension.aspx.Published
February 22, 2010. Accessed April 12, 2014.
6 Health Services Research and ManagerialEpidemiology
9. One hundred eleventh Congress of the United States of America.
Patient protection and affordable care act, 42 (USC). 2010. Pub L
No. 111-148, 124 Stat 855. Ammended May 1, 2010.
10. Centers for Disease Controland Prevention.Community health
workers/promotores de salud:criticalconnections in commu-
nities.Web site.http://www.cdc.gov/diabetes/projects/pdfs/
comm.pdf. Accessed July 7, 2014.
11. Institute of Medicine.Committee on Quality of Health Care in
America. Crossing the quality chasm: a new health system for the
21st century.National Academies Press; 2001.Web site.http://
www.nap.edu/catalog.php?record_id¼10027.Published March,
2001. Accessed April 12, 2014.
12. World Health Organization (WHO).Framework for action on
interprofessionaleducation and collaborative practice.Geneva:
World Health Organization,Departmentof Human Resources
for Health.2010.Web site.http://www.who.int/hrh/resources/
framework_action/en/.Published 2010.Accessed August16,
2014.
13. InterprofessionalEducation Collaborative ExpertPanel.Core
competencies for interprofessional collaborative practice: report
of an expertpanel.Washington,DC: InterprofessionalEduca-
tion Collaborative.2011.Web site.http://www.aacn.nche.edu/
education-resources/ipecreport.pdf.Accessed on August16,
2014.
14. Agency for Healthcare Research and Quality.Patientcentered
medical home: resource center.Web site.http://pcmh.ahrq.gov/.
Updated 2014. Accessed August 16, 2014.
15. American Academy of Family Physicians,American Academy
of Pediatrics, American College of Physicians, American Osteo-
pathic Association. Joint principles of the patient-centered med-
ical home. Del Medical J. 2008;80(1):21-22.
16. NationalPartnership for Women and Families.Patient-centered
medicalhome.Web site.http://www.nationalpartnership.org/
issues/health/patient-centered-medical-home.html.Published
2014.Updated 2015. Accessed August 16, 2014.
17. Institute of Medicine.Committee on the RobertWood Johnson
Foundation Initiative on the Future of Nursing.The future of
nursing:leading change,advancing health.NationalAcademies
Press;2010.Web site.http://www.iom.edu/Reports/2010/The-
Future-of-Nursing-Leading-Change-Advancing-Health.aspx.
Published 2011. Accessed April 12, 2014.
18. Blue Cross Blue Shield.Blue Cross and Blue Shield patient-
centered medical home programs are improving the practice and
delivery of primary care in communities nationwide.Available
June 4,2012.Web site.http://www.bcbs.com/healthcare-news/
bcbsa/blue-cross-and-blue-shield-4.html.Published June 4,
2012. Accessed August 16, 2014.
19. Archer J, Bower P, Gilbody S, et al. Collaborative care for depres-
sion and anxiety problems.Cochrane Database Syst Rev.2012;
10:1-277.
20. Bower P, Campbell S, Bojke C, Sibbald B. Team structure, team
climate and the quality of care in primary care: an observational
study. Qual Saf Health Care. 2003;12(4):273-279.
21. Davenport DL,Henderson WG,Mosca CL, Khuri SF,Mentzer
RM Jr. Risk-adjusted morbidity in teaching hospitals correlates with
reported levels of communication and collaboration on surgical
teams but not with scale measures of teamwork climate, safety
mate, or working conditions. J Am Coll Surg. 2007;205(6):778-7
22. Schmid AA,Kapoor JR,Miech EJ, et al. A multidisciplinary
stroke clinic for outpatient care of veterans with cerebrovascula
disease.J Multidiscip Healthc.2011;4:111-118.doi:10.2147/
JMDH.S17154.
23. Richardson LP,Ludman E,Lindenbaum J,et al. Collaboartive
care for adolescents with depression in primary care:a rando-
mized clinical trial. JAMA. 2014;312(8):809-816.
24. Thota AB, Sipe TA, Byard GJ, et al. Collaborative care to
improve the management of depressive disorders: a communit
guide systematic review and meta-analysis.Am J Prev Med.
2012;42(5):525-538.
25. Pape GA, Hunt JS, Butler KL, et al. Team-based care approach t
cholesterolmanagementin diabetes mellitus:two-year cluster
randomized controlled trial.Arch Intern Med.2011;171(16):
1480-1486.
26. Howard-Thompson A, Farland MZ, Byrd DC, et al. Pharmacist-
physician collaboration for diabetes care:cardiovascular out-
comes. Ann Pharmacother. 2013;47(11):1471-1477.
27. Sorbero ME,Farley DO,Mattke S,Lovejoy SL.Outcome mea-
sures for effective teamwork in inpatient care: final report. Ran
Corporation;2008.Web site.http://www.rand.org/content/dam/
rand/pubs/technical_reports/2008/RAND_TR462.pdf.Accessed
August 16, 2014.
28. Raab CA, Will SEB, Richards SL, O’Mara E. The effect of col-
laboration on obstetric patient safety in three academic facilitie
J Obstet Gynecol Neonatal Nurs. 2013;42(5):606-616.
29. Neily J, Mills PD, Young-Xu Y, et al. Association between imple-
mentation of a medical team training program and surgical mo
tality. JAMA. 2010;304(15):1693-1700.
30. Zatzick D, Russo J, Lord SP, et al. Collaborative care interventio
targeting violence risk behaviors, substance us, and posttraum
stress and depressive symptoms in injured adolescents: a rand
mized clinical trial. JAMA Pediatrics. 2014;168(8):532-539.
31. Abramson JS,MizrahiT. When socialworkers and physicians
collaborate:positive and negative interdisciplinary experiences.
Soc Work. 1996;41(3):270-281.
32. Baggs JG, Ryan A. Intensive care unit nurse-physician collabora
tion and nurse satisfaction. Nurs Econ. 1990;8(6):386-392.
33. D’amour D, Oandasan I. Interprofessionality as the field of inter
professionalpractice and interprofessionaleducation:an emer-
ging concept. J Interprof Care. 2005;19(S1):8-20.
34. Zwarenstein M,Goldman J,Reeves S.Interprofessionalcolla-
boration:effects of practice-based interventions on professional
practice and healthcare outcomes. Cochrane Database Syst Re
2009;3(CD000072):1-30.
35. BuscemiJ, Steglitz J,Spring B.The impactof team science
collaborations in health care: a synopsis and comment on Inter
professional collaboration: effects of practice-based interventio
on professional practice and healthcare outcomes.Transl Behav
Med. 2012;2(4):378-379.
36. Scholtes PR, Joiner BL, Streibel BJ. The Team Handbook. 3rd ed
Madison, WI: Oriel; 2003.
37. Rice AH. Interdisciplinary collaboration in health care: educatio
practice, and research. Natl Acad Pract Forum. 2000;2(1):59-73
Franklin et al 7
Patient protection and affordable care act, 42 (USC). 2010. Pub L
No. 111-148, 124 Stat 855. Ammended May 1, 2010.
10. Centers for Disease Controland Prevention.Community health
workers/promotores de salud:criticalconnections in commu-
nities.Web site.http://www.cdc.gov/diabetes/projects/pdfs/
comm.pdf. Accessed July 7, 2014.
11. Institute of Medicine.Committee on Quality of Health Care in
America. Crossing the quality chasm: a new health system for the
21st century.National Academies Press; 2001.Web site.http://
www.nap.edu/catalog.php?record_id¼10027.Published March,
2001. Accessed April 12, 2014.
12. World Health Organization (WHO).Framework for action on
interprofessionaleducation and collaborative practice.Geneva:
World Health Organization,Departmentof Human Resources
for Health.2010.Web site.http://www.who.int/hrh/resources/
framework_action/en/.Published 2010.Accessed August16,
2014.
13. InterprofessionalEducation Collaborative ExpertPanel.Core
competencies for interprofessional collaborative practice: report
of an expertpanel.Washington,DC: InterprofessionalEduca-
tion Collaborative.2011.Web site.http://www.aacn.nche.edu/
education-resources/ipecreport.pdf.Accessed on August16,
2014.
14. Agency for Healthcare Research and Quality.Patientcentered
medical home: resource center.Web site.http://pcmh.ahrq.gov/.
Updated 2014. Accessed August 16, 2014.
15. American Academy of Family Physicians,American Academy
of Pediatrics, American College of Physicians, American Osteo-
pathic Association. Joint principles of the patient-centered med-
ical home. Del Medical J. 2008;80(1):21-22.
16. NationalPartnership for Women and Families.Patient-centered
medicalhome.Web site.http://www.nationalpartnership.org/
issues/health/patient-centered-medical-home.html.Published
2014.Updated 2015. Accessed August 16, 2014.
17. Institute of Medicine.Committee on the RobertWood Johnson
Foundation Initiative on the Future of Nursing.The future of
nursing:leading change,advancing health.NationalAcademies
Press;2010.Web site.http://www.iom.edu/Reports/2010/The-
Future-of-Nursing-Leading-Change-Advancing-Health.aspx.
Published 2011. Accessed April 12, 2014.
18. Blue Cross Blue Shield.Blue Cross and Blue Shield patient-
centered medical home programs are improving the practice and
delivery of primary care in communities nationwide.Available
June 4,2012.Web site.http://www.bcbs.com/healthcare-news/
bcbsa/blue-cross-and-blue-shield-4.html.Published June 4,
2012. Accessed August 16, 2014.
19. Archer J, Bower P, Gilbody S, et al. Collaborative care for depres-
sion and anxiety problems.Cochrane Database Syst Rev.2012;
10:1-277.
20. Bower P, Campbell S, Bojke C, Sibbald B. Team structure, team
climate and the quality of care in primary care: an observational
study. Qual Saf Health Care. 2003;12(4):273-279.
21. Davenport DL,Henderson WG,Mosca CL, Khuri SF,Mentzer
RM Jr. Risk-adjusted morbidity in teaching hospitals correlates with
reported levels of communication and collaboration on surgical
teams but not with scale measures of teamwork climate, safety
mate, or working conditions. J Am Coll Surg. 2007;205(6):778-7
22. Schmid AA,Kapoor JR,Miech EJ, et al. A multidisciplinary
stroke clinic for outpatient care of veterans with cerebrovascula
disease.J Multidiscip Healthc.2011;4:111-118.doi:10.2147/
JMDH.S17154.
23. Richardson LP,Ludman E,Lindenbaum J,et al. Collaboartive
care for adolescents with depression in primary care:a rando-
mized clinical trial. JAMA. 2014;312(8):809-816.
24. Thota AB, Sipe TA, Byard GJ, et al. Collaborative care to
improve the management of depressive disorders: a communit
guide systematic review and meta-analysis.Am J Prev Med.
2012;42(5):525-538.
25. Pape GA, Hunt JS, Butler KL, et al. Team-based care approach t
cholesterolmanagementin diabetes mellitus:two-year cluster
randomized controlled trial.Arch Intern Med.2011;171(16):
1480-1486.
26. Howard-Thompson A, Farland MZ, Byrd DC, et al. Pharmacist-
physician collaboration for diabetes care:cardiovascular out-
comes. Ann Pharmacother. 2013;47(11):1471-1477.
27. Sorbero ME,Farley DO,Mattke S,Lovejoy SL.Outcome mea-
sures for effective teamwork in inpatient care: final report. Ran
Corporation;2008.Web site.http://www.rand.org/content/dam/
rand/pubs/technical_reports/2008/RAND_TR462.pdf.Accessed
August 16, 2014.
28. Raab CA, Will SEB, Richards SL, O’Mara E. The effect of col-
laboration on obstetric patient safety in three academic facilitie
J Obstet Gynecol Neonatal Nurs. 2013;42(5):606-616.
29. Neily J, Mills PD, Young-Xu Y, et al. Association between imple-
mentation of a medical team training program and surgical mo
tality. JAMA. 2010;304(15):1693-1700.
30. Zatzick D, Russo J, Lord SP, et al. Collaborative care interventio
targeting violence risk behaviors, substance us, and posttraum
stress and depressive symptoms in injured adolescents: a rand
mized clinical trial. JAMA Pediatrics. 2014;168(8):532-539.
31. Abramson JS,MizrahiT. When socialworkers and physicians
collaborate:positive and negative interdisciplinary experiences.
Soc Work. 1996;41(3):270-281.
32. Baggs JG, Ryan A. Intensive care unit nurse-physician collabora
tion and nurse satisfaction. Nurs Econ. 1990;8(6):386-392.
33. D’amour D, Oandasan I. Interprofessionality as the field of inter
professionalpractice and interprofessionaleducation:an emer-
ging concept. J Interprof Care. 2005;19(S1):8-20.
34. Zwarenstein M,Goldman J,Reeves S.Interprofessionalcolla-
boration:effects of practice-based interventions on professional
practice and healthcare outcomes. Cochrane Database Syst Re
2009;3(CD000072):1-30.
35. BuscemiJ, Steglitz J,Spring B.The impactof team science
collaborations in health care: a synopsis and comment on Inter
professional collaboration: effects of practice-based interventio
on professional practice and healthcare outcomes.Transl Behav
Med. 2012;2(4):378-379.
36. Scholtes PR, Joiner BL, Streibel BJ. The Team Handbook. 3rd ed
Madison, WI: Oriel; 2003.
37. Rice AH. Interdisciplinary collaboration in health care: educatio
practice, and research. Natl Acad Pract Forum. 2000;2(1):59-73
Franklin et al 7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
38. Barr O.Interdisciplinary teamwork:consideration of the chal-
lenges. Br J Nurs. 1997;6(17):1005-1010.
39. Gage M. From independence to interdependence: creating syner-
gistic healthcare teams. J Nurs Adm. 1998;28(4):17-26.
40. Whittemore R, Knafl K. The integrative review: updated metho-
dology. J Adv Nurs. 2005;52(5):546-553.
41. Agency forHealthcare Research and Quality.Methods guide
for effectiveness and comparative effectiveness reviews.Web
site. http://effectivehealthcare.ahrq.gov/ehc/products/60/318/
CER-Methods-Guide-140109.pdf.Published October,2007.
Updated January,2014.Accessed July 7,2014.
42. Beckham S, Bradley S, Washburn A, Taumua T. Diabetes man-
agement:utilizing community health workers in a Hawaiian/
Samoan population.J Health Care Poor Underserved.2008;
19(2):416-427.
43. Lujan J,Ostwald SK,Ortiz M.Promotora diabetes intervention
for Mexican Americans. Diabetes Educ. 2007;33(4):660-670.
44. Jandorf L, Gutierrez Y, Lopez J, Christie J, Itzkowitz SH. Use of a
patientnavigator to increase colorectalcancer screening in an
urban neighborhood health clinic.J Urban Health.2005;82(2):
216-224.
45. Levine DM,Bone LR,Hill MN, et al. The effectiveness of a
community/academic health center partnership in decreasing the
level of blood pressure in an urban African-American population.
Ethn Dis. 2003;13(3):354–361.
46. Williams JH,Belle GA,Houston C,Haire-Joshu D,Auslander
WF. Process evaluation methods of a peer-delivered health pro-
motion program for African American women.Health Promot
Pract. 2001;2(2):135-142.
47. AuslanderW, Haire-Joshu D,Houston C,Rhee CW.A con-
trolled evaluation of staging dietary patterns to reduce the risk
of diabetes in african-american women.Diabetes Care.2002;
25(5):809-814.
48. Gary TL, Bone LR, Hill MN, et al. Randomized controlled trial of
the effects of nurse case manager and community health worker
interventions on risk factors for diabetes-related complications in
urban african americans. Prev Med. 2003;37(1):23-32.
49. Gary TL,Hill-Briggs F,Batts-Turner M,BrancatiFL. Transla-
tional research principles of an effectiveness trial for diabetes care
in an urban african american population.Diabetes Educ.2005;
31(6):880-889.
50. Schuler ME, Nair P, Black MM, Kettinger L. Mother-infant inter-
action: effects of a home intervention and ongoing maternal drug
use. J Clin Child Psychol. 2000;29(3):424-431.
51. Korfmacher J, O’Brien R, Hiatt S, Olds D. Differences in program
imp nurses and paraprofessionals providing home visits during
pregnancy and infancy: a randomized trial. Am J Public Health.
1999;89(12):1847-1851.
52. Wang EA, Hong CS, Samuels L, Shavit S, Sanders R, Kushel M.
Transitions clinic:creating a community-based model of health
care for recently released California prisoners. Public Health Rep.
2010;125(2):171-177.
53. Wang EA, Hong CS, Shavit S, Sanders R, Kessell E, Kushel MB.
Engaging individuals recently released from prison into primary
care:a randomized trial.Am J Public Health.2012;102(9):
e22-e29.
54. Spencer MS,Rosland AM,Kieffer EC,et al.Effectiveness of a
community health worker intervention among African American
and Latino adults with type 2 diabetes: a randomized controlled
trial. Am J Public Health. 2011;101(12):2253-2260.
55. Sixta CS,Ostwald S.Texas-Mexico border intervention by pro-
motores for patients with type 2 diabetes.Diabetes Educ.2008;
34(2):299-309.
56. Krieger J, Takaro TK, Song L, Beaudet N, Edwards K. A rando-
mized controlled trial of asthma self-management support com
paring clinic-based nurses and in-home community health
workers: the Seattle–King county healthy homes II project. Arch
Pediatr Adolesc Med. 2009;163(2):141-149.
57. D’Amour D, Ferrada-Videla M, San Martin Rodriguez L, Beau-
lieu M. The conceptual basis for interprofessional collaboration:
core concepts and theoretical frameworks. J Interprof Care. 200
19(S1):116-131.
58. Institute of Medicine.Primary care and public health: exploring
integration to improve population health. The National Academ
Press.2012.Web site.http://www.iom.edu/Reports/2012/Pri-
mary-Care-and-Public-Health.aspx.Published 2012.Accessed
June 16, 2014.
59. Bond MA, Haynes MC, Toof RA, Holmberg MD, Quinteros JR.
Healthdiversity: practices that support diverse staffing in comm
nity health centers.University of Massachusetts,Lowell: Center
for Women and Work. 2011. Web site. http://www.uml.edu/docs
Healthy%20Diversity%20Report_tcm18-49658.pdf.Accessed
August 16, 2014.
60. Whelan EM.The importance ofcommunity health centers:
engines of economic activity and job creation. Center for Amer
ican Progress.Web site.https://www.americanprogress.org/
issues/healthcare/report/2010/08/09/8195/the-importance-of-
community-health-centers/.Published August 9, 2010.
Accessed June 16, 2014.
61. Islam N,NadkatniSK, Zahn D,Skillman M,Kwon SC,Trinh-
Shevrin C. Integrating community health workers within Patient
Protection and Affordable Care Actimplementation.J Public
Health ManagementPractice.2015;21(1):42-50.doi:10.1097/
PHH.0000000000000084.
62. Matiz LA, Pereyz PJ, Jacotin PG, Cruz C, Ramirez-Diaz E, Nieto
AR. The impactof integrating community health workers into
patient-centered medical home. J Prim Care Community Health
2014;5(4):271-274. doi:10.1177/2150131914540694.
63. Wennerstrom A,Bui T, Harden-Barrios J,Price-Haywood EG.
Integrating community health workers into a patient-centered
medical home to support disease self management among Viet
namese American: lessons learned.Health Promot Pract.2015;
6(1):72-83. doi:10.1177/1524839914547760.
Author Biographies
Catherine M.Franklin DNP,FNP-C received a doctor of Nursing
Practice from the MGH Institute of Health Professions where she al
served as ClinicalAssistantProfessor and AssistantDean for the
Accelerated Baccalaureate Nursing Program.She received a BS in
Nursing at Fitchburg State College, Fitchburg, MA, a MS in Nursing
Administration and Community Health from Salem State College,
8 Health Services Research and ManagerialEpidemiology
lenges. Br J Nurs. 1997;6(17):1005-1010.
39. Gage M. From independence to interdependence: creating syner-
gistic healthcare teams. J Nurs Adm. 1998;28(4):17-26.
40. Whittemore R, Knafl K. The integrative review: updated metho-
dology. J Adv Nurs. 2005;52(5):546-553.
41. Agency forHealthcare Research and Quality.Methods guide
for effectiveness and comparative effectiveness reviews.Web
site. http://effectivehealthcare.ahrq.gov/ehc/products/60/318/
CER-Methods-Guide-140109.pdf.Published October,2007.
Updated January,2014.Accessed July 7,2014.
42. Beckham S, Bradley S, Washburn A, Taumua T. Diabetes man-
agement:utilizing community health workers in a Hawaiian/
Samoan population.J Health Care Poor Underserved.2008;
19(2):416-427.
43. Lujan J,Ostwald SK,Ortiz M.Promotora diabetes intervention
for Mexican Americans. Diabetes Educ. 2007;33(4):660-670.
44. Jandorf L, Gutierrez Y, Lopez J, Christie J, Itzkowitz SH. Use of a
patientnavigator to increase colorectalcancer screening in an
urban neighborhood health clinic.J Urban Health.2005;82(2):
216-224.
45. Levine DM,Bone LR,Hill MN, et al. The effectiveness of a
community/academic health center partnership in decreasing the
level of blood pressure in an urban African-American population.
Ethn Dis. 2003;13(3):354–361.
46. Williams JH,Belle GA,Houston C,Haire-Joshu D,Auslander
WF. Process evaluation methods of a peer-delivered health pro-
motion program for African American women.Health Promot
Pract. 2001;2(2):135-142.
47. AuslanderW, Haire-Joshu D,Houston C,Rhee CW.A con-
trolled evaluation of staging dietary patterns to reduce the risk
of diabetes in african-american women.Diabetes Care.2002;
25(5):809-814.
48. Gary TL, Bone LR, Hill MN, et al. Randomized controlled trial of
the effects of nurse case manager and community health worker
interventions on risk factors for diabetes-related complications in
urban african americans. Prev Med. 2003;37(1):23-32.
49. Gary TL,Hill-Briggs F,Batts-Turner M,BrancatiFL. Transla-
tional research principles of an effectiveness trial for diabetes care
in an urban african american population.Diabetes Educ.2005;
31(6):880-889.
50. Schuler ME, Nair P, Black MM, Kettinger L. Mother-infant inter-
action: effects of a home intervention and ongoing maternal drug
use. J Clin Child Psychol. 2000;29(3):424-431.
51. Korfmacher J, O’Brien R, Hiatt S, Olds D. Differences in program
imp nurses and paraprofessionals providing home visits during
pregnancy and infancy: a randomized trial. Am J Public Health.
1999;89(12):1847-1851.
52. Wang EA, Hong CS, Samuels L, Shavit S, Sanders R, Kushel M.
Transitions clinic:creating a community-based model of health
care for recently released California prisoners. Public Health Rep.
2010;125(2):171-177.
53. Wang EA, Hong CS, Shavit S, Sanders R, Kessell E, Kushel MB.
Engaging individuals recently released from prison into primary
care:a randomized trial.Am J Public Health.2012;102(9):
e22-e29.
54. Spencer MS,Rosland AM,Kieffer EC,et al.Effectiveness of a
community health worker intervention among African American
and Latino adults with type 2 diabetes: a randomized controlled
trial. Am J Public Health. 2011;101(12):2253-2260.
55. Sixta CS,Ostwald S.Texas-Mexico border intervention by pro-
motores for patients with type 2 diabetes.Diabetes Educ.2008;
34(2):299-309.
56. Krieger J, Takaro TK, Song L, Beaudet N, Edwards K. A rando-
mized controlled trial of asthma self-management support com
paring clinic-based nurses and in-home community health
workers: the Seattle–King county healthy homes II project. Arch
Pediatr Adolesc Med. 2009;163(2):141-149.
57. D’Amour D, Ferrada-Videla M, San Martin Rodriguez L, Beau-
lieu M. The conceptual basis for interprofessional collaboration:
core concepts and theoretical frameworks. J Interprof Care. 200
19(S1):116-131.
58. Institute of Medicine.Primary care and public health: exploring
integration to improve population health. The National Academ
Press.2012.Web site.http://www.iom.edu/Reports/2012/Pri-
mary-Care-and-Public-Health.aspx.Published 2012.Accessed
June 16, 2014.
59. Bond MA, Haynes MC, Toof RA, Holmberg MD, Quinteros JR.
Healthdiversity: practices that support diverse staffing in comm
nity health centers.University of Massachusetts,Lowell: Center
for Women and Work. 2011. Web site. http://www.uml.edu/docs
Healthy%20Diversity%20Report_tcm18-49658.pdf.Accessed
August 16, 2014.
60. Whelan EM.The importance ofcommunity health centers:
engines of economic activity and job creation. Center for Amer
ican Progress.Web site.https://www.americanprogress.org/
issues/healthcare/report/2010/08/09/8195/the-importance-of-
community-health-centers/.Published August 9, 2010.
Accessed June 16, 2014.
61. Islam N,NadkatniSK, Zahn D,Skillman M,Kwon SC,Trinh-
Shevrin C. Integrating community health workers within Patient
Protection and Affordable Care Actimplementation.J Public
Health ManagementPractice.2015;21(1):42-50.doi:10.1097/
PHH.0000000000000084.
62. Matiz LA, Pereyz PJ, Jacotin PG, Cruz C, Ramirez-Diaz E, Nieto
AR. The impactof integrating community health workers into
patient-centered medical home. J Prim Care Community Health
2014;5(4):271-274. doi:10.1177/2150131914540694.
63. Wennerstrom A,Bui T, Harden-Barrios J,Price-Haywood EG.
Integrating community health workers into a patient-centered
medical home to support disease self management among Viet
namese American: lessons learned.Health Promot Pract.2015;
6(1):72-83. doi:10.1177/1524839914547760.
Author Biographies
Catherine M.Franklin DNP,FNP-C received a doctor of Nursing
Practice from the MGH Institute of Health Professions where she al
served as ClinicalAssistantProfessor and AssistantDean for the
Accelerated Baccalaureate Nursing Program.She received a BS in
Nursing at Fitchburg State College, Fitchburg, MA, a MS in Nursing
Administration and Community Health from Salem State College,
8 Health Services Research and ManagerialEpidemiology
Salem, MA, and a CAGS in Primary Care at Simmons College, Bos-
ton, MA.Dr. Franklin is currently the Administrative Director for the
Department of Family Medicine at East Boston Neighborhood Health
Center in East Boston, MA where she also maintains a clinical primary
care practice.
Jean M. Bernhardt,PhD, NEA-BC, FNP-BC, CNP received her
doctorate in Nursing and Health Policy from the University of
Massachusetts, Boston, MA.She attended the University of Virgi-
nia and Fitchburg State College.Dr. Bernhardtis an Associate
Professor in the School of Nursing at the MGH Institute of Health
Professions and currently the Administrative Director and a Family
Nurse Practitionerat MGH Charlestown Healthcare Centerin
Boston, MA.
Ruth Palan Lopez, PhD, GNP-BC received a BS in Nursing at Boston
College in Chestnut Hill, MA, USA. She subsequently received a MS
in Gerontological Nursing at Boston University, and a PhD at Boston
College. Dr. Lopez was a Hartford Foundation, Claire M. Fagin Post-
Doctoral Fellow at the University of Pennsylvania. She is currently an
associate professor of Nursing at the MGH Institute of Health Profe
sions,in Boston,MA where she is also the Coordinator of the Doc-
torate in Nursing Practice Program.
Ellen R. Long-Middleton, PhD, RN, FNP-BC earned a BS in Nursing
from the University of Vermont, MS in Nursing from the University
Washington, and PhD from Boston College. Dr. Long-Middleton was
a Post-Doctoral Fellow in the HIV/AIDS Prevention and Care Fellow-
ship atthe University of California San Francisco.She currently
serves as an Associate Professor in the College of Nursing and Hea
Sciences atthe University ofVermontand is a Family Nurse
Practitioner.
Sheila Davis,DNP, ANP-BC, FAAN received a BS in Nursing at
Northeastern University,Boston,MA, a MS in Nursing and Doctor
of Nursing Practice from the MGH Institute of Health Professions
where she also served as Clinical Assistant Professor. Currently, Dr
Davis is the Chief Nursing Officer at Partners In Health and is leadi
the non-governmental organization’s Ebola response efforts in We
Africa.
Franklin et al 9
ton, MA.Dr. Franklin is currently the Administrative Director for the
Department of Family Medicine at East Boston Neighborhood Health
Center in East Boston, MA where she also maintains a clinical primary
care practice.
Jean M. Bernhardt,PhD, NEA-BC, FNP-BC, CNP received her
doctorate in Nursing and Health Policy from the University of
Massachusetts, Boston, MA.She attended the University of Virgi-
nia and Fitchburg State College.Dr. Bernhardtis an Associate
Professor in the School of Nursing at the MGH Institute of Health
Professions and currently the Administrative Director and a Family
Nurse Practitionerat MGH Charlestown Healthcare Centerin
Boston, MA.
Ruth Palan Lopez, PhD, GNP-BC received a BS in Nursing at Boston
College in Chestnut Hill, MA, USA. She subsequently received a MS
in Gerontological Nursing at Boston University, and a PhD at Boston
College. Dr. Lopez was a Hartford Foundation, Claire M. Fagin Post-
Doctoral Fellow at the University of Pennsylvania. She is currently an
associate professor of Nursing at the MGH Institute of Health Profe
sions,in Boston,MA where she is also the Coordinator of the Doc-
torate in Nursing Practice Program.
Ellen R. Long-Middleton, PhD, RN, FNP-BC earned a BS in Nursing
from the University of Vermont, MS in Nursing from the University
Washington, and PhD from Boston College. Dr. Long-Middleton was
a Post-Doctoral Fellow in the HIV/AIDS Prevention and Care Fellow-
ship atthe University of California San Francisco.She currently
serves as an Associate Professor in the College of Nursing and Hea
Sciences atthe University ofVermontand is a Family Nurse
Practitioner.
Sheila Davis,DNP, ANP-BC, FAAN received a BS in Nursing at
Northeastern University,Boston,MA, a MS in Nursing and Doctor
of Nursing Practice from the MGH Institute of Health Professions
where she also served as Clinical Assistant Professor. Currently, Dr
Davis is the Chief Nursing Officer at Partners In Health and is leadi
the non-governmental organization’s Ebola response efforts in We
Africa.
Franklin et al 9
1 out of 9
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.