Clinical Reasoning Cycle for Heart Failure Patient
VerifiedAdded on 2022/11/18
|10
|1597
|140
Presentation
AI Summary
The presentation is based on a case study regarding Mr. Tomasi Joni, a 56 year old male of Fijian background. The presentation will include a clinical reasoning cycle that will identify the health risks of the patient from the case study. This presentation will also cover SMART goals for the patient and both pharmacological and non-pharmacological interventions for reducing health risks.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Introduction
■ The presentation is based on a case study regarding Mr. Tomasi Joni, a
56 year old male of Fijian background.
■ The presentation will include a clinical reasoning cycle that will
identify the health risks of the patient from the case study.
■ This presentation will also cover SMART goals for the patient and both
pharmacological and non-pharmacological interventions for reducing
health risks.
Name of the Student
Name of the University
■ The presentation is based on a case study regarding Mr. Tomasi Joni, a
56 year old male of Fijian background.
■ The presentation will include a clinical reasoning cycle that will
identify the health risks of the patient from the case study.
■ This presentation will also cover SMART goals for the patient and both
pharmacological and non-pharmacological interventions for reducing
health risks.
Name of the Student
Name of the University
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Consider the pt, collect cues and
information
■ Mr. Joni has been identified to suffer from the complication of heart failure
■ It is anticipated that an estimated 300,000 Australians suffer from chronic heart
failure(AIHW, 2019)
■ Roughly 30,000 new cases of heart failure are diagnosed every year (AIHW, 2019)
■ The patient’s previous history of hypertension (142/96mmHg) and acute myocardial
infarction (AMI) increases his risks of suffering from the complication since flow of
blood to the cardiac muscle gets abruptly cut off, thereby leading to tissue damage
■ His obs also indicate that he demonstrates signs of hypertension, dyspnea,
hypercholesteromia, obesity, and hypothermia
■ He is under medication for angina and hypertension (metoprolol), gout and kidney
stones (allopurinol), and pain management (aspirin)
information
■ Mr. Joni has been identified to suffer from the complication of heart failure
■ It is anticipated that an estimated 300,000 Australians suffer from chronic heart
failure(AIHW, 2019)
■ Roughly 30,000 new cases of heart failure are diagnosed every year (AIHW, 2019)
■ The patient’s previous history of hypertension (142/96mmHg) and acute myocardial
infarction (AMI) increases his risks of suffering from the complication since flow of
blood to the cardiac muscle gets abruptly cut off, thereby leading to tissue damage
■ His obs also indicate that he demonstrates signs of hypertension, dyspnea,
hypercholesteromia, obesity, and hypothermia
■ He is under medication for angina and hypertension (metoprolol), gout and kidney
stones (allopurinol), and pain management (aspirin)
Process information and identify
issue
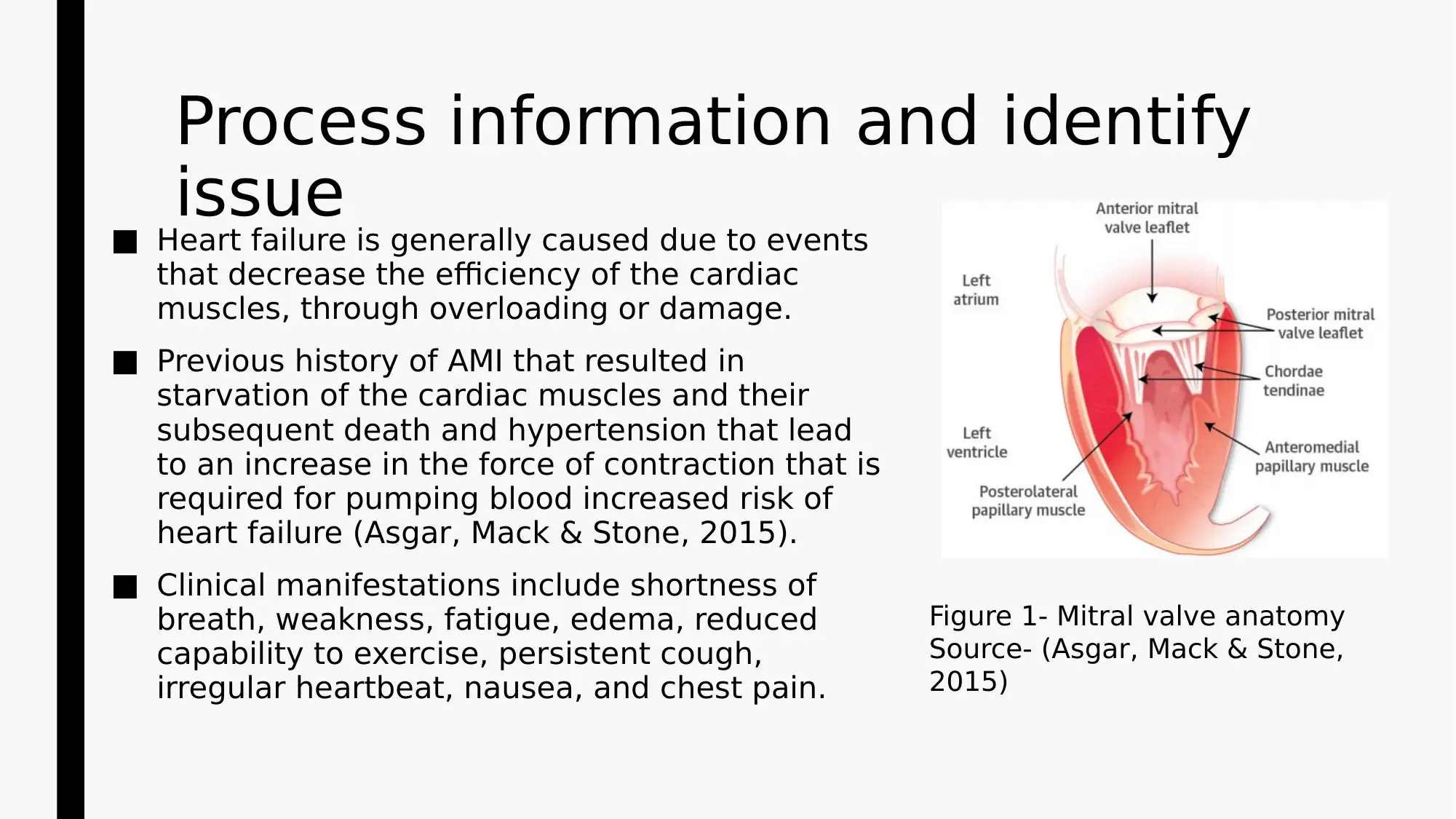
■ Heart failure is generally caused due to events
that decrease the efficiency of the cardiac
muscles, through overloading or damage.
■ Previous history of AMI that resulted in
starvation of the cardiac muscles and their
subsequent death and hypertension that lead
to an increase in the force of contraction that is
required for pumping blood increased risk of
heart failure (Asgar, Mack & Stone, 2015).
■ Clinical manifestations include shortness of
breath, weakness, fatigue, edema, reduced
capability to exercise, persistent cough,
irregular heartbeat, nausea, and chest pain.
Figure 1- Mitral valve anatomy
Source- (Asgar, Mack & Stone,
2015)
issue
■ Heart failure is generally caused due to events
that decrease the efficiency of the cardiac
muscles, through overloading or damage.
■ Previous history of AMI that resulted in
starvation of the cardiac muscles and their
subsequent death and hypertension that lead
to an increase in the force of contraction that is
required for pumping blood increased risk of
heart failure (Asgar, Mack & Stone, 2015).
■ Clinical manifestations include shortness of
breath, weakness, fatigue, edema, reduced
capability to exercise, persistent cough,
irregular heartbeat, nausea, and chest pain.
Figure 1- Mitral valve anatomy
Source- (Asgar, Mack & Stone,
2015)
Identify issue (patho) – continued
■ The patient who is at a risk of heart failure, demonstrates a decreased
force of contraction in his heart
■ This can be accredited to overloading of the heart ventricles
■ In healthy heart, an increase in filling of ventricle causes amplification
of the contraction force, and increases cardiac output (Ter Maaten et
al., 2015)
■ In heart failure, the ventricle remains loaded with blood to an extent
that reduces efficacy of cardiac muscle contraction
■ This occurs due to decreased capability to form cross-link between
myosin and actin filaments in over-stretched muscles
■ The patient who is at a risk of heart failure, demonstrates a decreased
force of contraction in his heart
■ This can be accredited to overloading of the heart ventricles
■ In healthy heart, an increase in filling of ventricle causes amplification
of the contraction force, and increases cardiac output (Ter Maaten et
al., 2015)
■ In heart failure, the ventricle remains loaded with blood to an extent
that reduces efficacy of cardiac muscle contraction
■ This occurs due to decreased capability to form cross-link between
myosin and actin filaments in over-stretched muscles
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
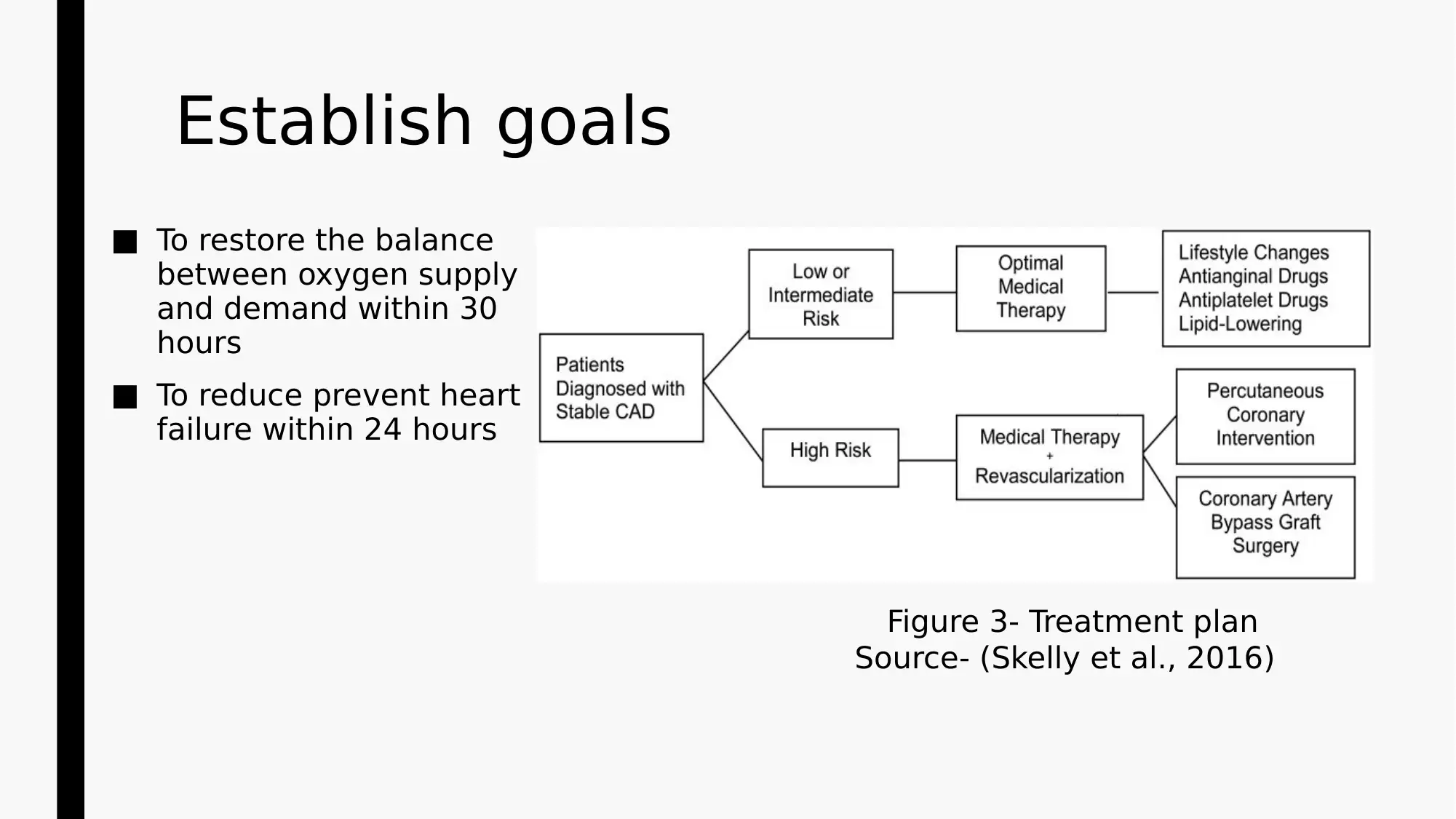
Establish goals
■ To restore the balance
between oxygen supply
and demand within 30
hours
■ To reduce prevent heart
failure within 24 hours
Figure 3- Treatment plan
Source- (Skelly et al., 2016)
■ To restore the balance
between oxygen supply
and demand within 30
hours
■ To reduce prevent heart
failure within 24 hours
Figure 3- Treatment plan
Source- (Skelly et al., 2016)
Take action
■ Pharmacological interventions- Administration of nitroglycerine and
angiotensin converting enzyme inhibitors (ACE inhibitors).
■ Nitroglycerine exets both peripheral hemodynamic and direct
coronary impacts that will help in vasodilation of the coronary arteries
and systemic veins (Maruhashi et al., 2016)
■ ACE inhibitors will help in controlling elevated blood pressure and also
prevent heart failure by dilating blood vessels (Romero, Orias & Weir,
2015)
■ Pharmacological interventions- Administration of nitroglycerine and
angiotensin converting enzyme inhibitors (ACE inhibitors).
■ Nitroglycerine exets both peripheral hemodynamic and direct
coronary impacts that will help in vasodilation of the coronary arteries
and systemic veins (Maruhashi et al., 2016)
■ ACE inhibitors will help in controlling elevated blood pressure and also
prevent heart failure by dilating blood vessels (Romero, Orias & Weir,
2015)
Take action - continued
■ Non-pharmacological interventions- Recommending dietary modifications
and performing aerobic exercise
■ Daily consumption of Mediterranean diet that includes whole grains,
fruits, vegetables, and healthy fat will reduce risks for adverse cardiac
events, in comparison to low-fat diet (Rosato et al., 2019)
■ Aerobic exercise will enhance cardiovascular fitness and increase
capability of using oxygen (Drenowatz et al., 2015)
■ Non-pharmacological interventions- Recommending dietary modifications
and performing aerobic exercise
■ Daily consumption of Mediterranean diet that includes whole grains,
fruits, vegetables, and healthy fat will reduce risks for adverse cardiac
events, in comparison to low-fat diet (Rosato et al., 2019)
■ Aerobic exercise will enhance cardiovascular fitness and increase
capability of using oxygen (Drenowatz et al., 2015)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Take action – continued
■ Provide convenience and play the role of an active listener to
understand his apprehensions and health related concerns
■ Helping him lean what heart failure is, its pervasiveness, and the
common signs and symptoms
■ Providing clear information about the medical condition
■ Development of actionable plans that can be followed post discharge
from the hospital
■ Encouraging smoking cessation and adherence to proper dietary
modification
■ Provide convenience and play the role of an active listener to
understand his apprehensions and health related concerns
■ Helping him lean what heart failure is, its pervasiveness, and the
common signs and symptoms
■ Providing clear information about the medical condition
■ Development of actionable plans that can be followed post discharge
from the hospital
■ Encouraging smoking cessation and adherence to proper dietary
modification
Conclusion
■ The primary health risk identified from the case study was heart
failure
■ The two goals were to maintain equilibrium between oxygen demand
and supply and reduce heart failure incident
■ Reduction in blood pressure, and no reports of heart failure or CAD
would help in evaluating success of the interventions
■ The clinical reasoning cycle helped in increasing my awareness on
CAD, AMI, and the associated risks for cardiac dysfunctioning.
■ It also increase understanding on the mechanism of action of different
pharmacological management techniques.
■ The primary health risk identified from the case study was heart
failure
■ The two goals were to maintain equilibrium between oxygen demand
and supply and reduce heart failure incident
■ Reduction in blood pressure, and no reports of heart failure or CAD
would help in evaluating success of the interventions
■ The clinical reasoning cycle helped in increasing my awareness on
CAD, AMI, and the associated risks for cardiac dysfunctioning.
■ It also increase understanding on the mechanism of action of different
pharmacological management techniques.
References
Asgar, A. W., Mack, M. J., & Stone, G. W. (2015). Secondary mitral regurgitation in heart failure: pathophysiology, prognosis, and therapeutic considerations. Journal of the
American College of Cardiology, 65(12), 1231-1248. DOI: 10.1016/j.jacc.2015.02.009
Australian Institute of Health and Welfare. (2019). Heart failure. . . what of the future?
https://www.aihw.gov.au/reports/heart-stroke-vascular-diseases/heart-failure-future/contents/summary
Cahill, L. E., Sacks, F. M., Rimm, E. B., & Jensen, M. K. (2019). Cholesterol Efflux Capacity, HDL Cholesterol, and Risk of Coronary Heart Disease: a Nested Case-Control Study in
Men. Journal of lipid research, jlr- P093823. doi: 10.1194/jlr.P093823
Chen, S., Shimada, K., Crother, T. R., Yamashita, M., & Arditi, M. (2018). Role of Autophagy in Macrophages During Acute Myocardial Infraction. Arteriosclerosis, Thrombosis, and
Vascular Biology, 38(Suppl_1), A423- A423. https://doi.org/10.1161/atvb.38.suppl_1.423
Daw, J., Margolis, R., & Wright, L. (2017). Emerging adulthood, emergent health lifestyles: Sociodemographic determinants of trajectories of smoking, binge drinking, obesity, and
sedentary behavior. Journal of health and social behavior, 58(2), 181-197. https://doi.org/10.1177%2F0022146517702421
Drenowatz, C., Sui, X., Fritz, S., Lavie, C. J., Beattie, P. F., Church, T. S., & Blair, S. N. (2015). The association between resistance exercise and cardiovascular disease risk in
women. Journal of science and medicine in sport, 18(6), 632-636. https://doi.org/10.1016/j.jsams.2014.09.009
Ibanez, B., James, S., Agewall, S., Antunes, M. J., Bucciarelli-Ducci, C., Bueno, H., ... & Hindricks, G. (2017). 2017 ESC Guidelines for the management of acute myocardial infarction
in patients presenting with ST- segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the
European Society of Cardiology (ESC). European heart journal, 39(2), 119-177. https://doi.org/10.1093/eurheartj/ehx393
Maruhashi, T., Kajikawa, M., Nakashima, A., Iwamoto, Y., Iwamoto, A., Oda, N., ... & Watanabe, N. (2016). Nitroglycerine-induced vasodilation in coronary and brachial arteries in
patients with suspected coronary artery disease. International journal of cardiology, 219, 312-316. doi: 10.1097/HJH.0000000000001750
Romero, C. A., Orias, M., & Weir, M. R. (2015). Novel RAAS agonists and antagonists: clinical applications and controversies. Nature Reviews Endocrinology, 11(4), 242.
https://doi.org/10.1038/nrendo.2015.6
Rosato, V., Temple, N. J., La Vecchia, C., Castellan, G., Tavani, A., & Guercio, V. (2019). Mediterranean diet and cardiovascular disease: a systematic review and meta-analysis of
observational studies. European journal of nutrition, 58(1), 173-191. https://doi.org/10.1007/s00394-017-1582-0
Sit, J. W., Chair, S. Y., Choi, K. C., Chan, C. W., Chan, A. W., Qiu, X., & Taylor-Piliae, R. E. (2017). Abstract NS7: Strategies for Enhancing Stroke Self-management Among Older Stroke
Survivors: A Mixed Methods Inquiry. Stroke, 48(suppl_1), ANS7-ANS7. https://www.ahajournals.org/doi/abs/10.1161/str.48.suppl_1.ns7
Skelly, A. C., Hashimoto, R., Buckley, D. I., Brodt, E. D., Noelck, N., Totten, A. M., ... & McDonagh, M. (2016). Noninvasive testing for coronary artery disease.
https://www.ncbi.nlm.nih.gov/books/NBK361148/
Swier, V. J., Tang, L., Radwan, M. M., & Agrawal, D. K. (2016). The role of high cholesterol-high fructose diet on coronary arteriosclerosis. Histology and histopathology, 31(2), 167-
176. DOI: 10.14670/HH-11-652
Ter Maaten, J. M., Valente, M. A., Damman, K., Hillege, H. L., Navis, G., & Voors, A. A. (2015). Diuretic response in acute heart failure—pathophysiology, evaluation, and
therapy. Nature Reviews Cardiology, 12(3), 184. https://doi.org/10.1038/nrcardio.2014.215
Asgar, A. W., Mack, M. J., & Stone, G. W. (2015). Secondary mitral regurgitation in heart failure: pathophysiology, prognosis, and therapeutic considerations. Journal of the
American College of Cardiology, 65(12), 1231-1248. DOI: 10.1016/j.jacc.2015.02.009
Australian Institute of Health and Welfare. (2019). Heart failure. . . what of the future?
https://www.aihw.gov.au/reports/heart-stroke-vascular-diseases/heart-failure-future/contents/summary
Cahill, L. E., Sacks, F. M., Rimm, E. B., & Jensen, M. K. (2019). Cholesterol Efflux Capacity, HDL Cholesterol, and Risk of Coronary Heart Disease: a Nested Case-Control Study in
Men. Journal of lipid research, jlr- P093823. doi: 10.1194/jlr.P093823
Chen, S., Shimada, K., Crother, T. R., Yamashita, M., & Arditi, M. (2018). Role of Autophagy in Macrophages During Acute Myocardial Infraction. Arteriosclerosis, Thrombosis, and
Vascular Biology, 38(Suppl_1), A423- A423. https://doi.org/10.1161/atvb.38.suppl_1.423
Daw, J., Margolis, R., & Wright, L. (2017). Emerging adulthood, emergent health lifestyles: Sociodemographic determinants of trajectories of smoking, binge drinking, obesity, and
sedentary behavior. Journal of health and social behavior, 58(2), 181-197. https://doi.org/10.1177%2F0022146517702421
Drenowatz, C., Sui, X., Fritz, S., Lavie, C. J., Beattie, P. F., Church, T. S., & Blair, S. N. (2015). The association between resistance exercise and cardiovascular disease risk in
women. Journal of science and medicine in sport, 18(6), 632-636. https://doi.org/10.1016/j.jsams.2014.09.009
Ibanez, B., James, S., Agewall, S., Antunes, M. J., Bucciarelli-Ducci, C., Bueno, H., ... & Hindricks, G. (2017). 2017 ESC Guidelines for the management of acute myocardial infarction
in patients presenting with ST- segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the
European Society of Cardiology (ESC). European heart journal, 39(2), 119-177. https://doi.org/10.1093/eurheartj/ehx393
Maruhashi, T., Kajikawa, M., Nakashima, A., Iwamoto, Y., Iwamoto, A., Oda, N., ... & Watanabe, N. (2016). Nitroglycerine-induced vasodilation in coronary and brachial arteries in
patients with suspected coronary artery disease. International journal of cardiology, 219, 312-316. doi: 10.1097/HJH.0000000000001750
Romero, C. A., Orias, M., & Weir, M. R. (2015). Novel RAAS agonists and antagonists: clinical applications and controversies. Nature Reviews Endocrinology, 11(4), 242.
https://doi.org/10.1038/nrendo.2015.6
Rosato, V., Temple, N. J., La Vecchia, C., Castellan, G., Tavani, A., & Guercio, V. (2019). Mediterranean diet and cardiovascular disease: a systematic review and meta-analysis of
observational studies. European journal of nutrition, 58(1), 173-191. https://doi.org/10.1007/s00394-017-1582-0
Sit, J. W., Chair, S. Y., Choi, K. C., Chan, C. W., Chan, A. W., Qiu, X., & Taylor-Piliae, R. E. (2017). Abstract NS7: Strategies for Enhancing Stroke Self-management Among Older Stroke
Survivors: A Mixed Methods Inquiry. Stroke, 48(suppl_1), ANS7-ANS7. https://www.ahajournals.org/doi/abs/10.1161/str.48.suppl_1.ns7
Skelly, A. C., Hashimoto, R., Buckley, D. I., Brodt, E. D., Noelck, N., Totten, A. M., ... & McDonagh, M. (2016). Noninvasive testing for coronary artery disease.
https://www.ncbi.nlm.nih.gov/books/NBK361148/
Swier, V. J., Tang, L., Radwan, M. M., & Agrawal, D. K. (2016). The role of high cholesterol-high fructose diet on coronary arteriosclerosis. Histology and histopathology, 31(2), 167-
176. DOI: 10.14670/HH-11-652
Ter Maaten, J. M., Valente, M. A., Damman, K., Hillege, H. L., Navis, G., & Voors, A. A. (2015). Diuretic response in acute heart failure—pathophysiology, evaluation, and
therapy. Nature Reviews Cardiology, 12(3), 184. https://doi.org/10.1038/nrcardio.2014.215
1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.