Assessment of Ipilimumab for Advanced Melanoma: A Report for Australia
VerifiedAdded on 2022/11/13
|15
|3910
|1
Report
AI Summary
This report critically appraises the clinical and economic evidence surrounding the use of Ipilimumab in the treatment of advanced melanoma. It examines the drug's mechanism of action, focusing on its role as an immune checkpoint inhibitor targeting CTLA-4 to enhance antitumor T-cell responses. The report analyzes clinical trial data comparing Ipilimumab monotherapy, bi-therapy with gp100, and gp100 alone, highlighting improved survival rates with Ipilimumab. An economic evaluation using a Markov model assesses cost-effectiveness, considering factors like disease progression, quality of life, and healthcare resource utilization. The analysis concludes that Ipilimumab demonstrates significant cost-effectiveness, with recommendations for government policies and potential subsidization to address the financial burden of treatment, particularly within the Australian healthcare context. The report also includes appraisal checklists to assess the quality of the evidence presented and to inform decisions on whether this technology should be funded in Australia.

Running Head: IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
Name of the Student:
Name of the University:
Author Note:
IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
Name of the Student:
Name of the University:
Author Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
Abstract:
Cancer has been a disease of major concern today. Skin cancers are one of the most prevalent
cancers throughout the world. Various treatment strategies have been devised to treat
melanoma. This project aims to examine the applicability and the cost-effectiveness of using
Ipilimumab. This drug is administered to improve the survivability of the patients suffering
from advanced melanoma. Cost-effectiveness becomes a matter of concern when a particular
strategy or technique is higher in cost. Ipilimumab is defined to be a monoclonal antibody
that activates the immune system by targeting CTLA-4. CTLA-4 is a protein receptor that
downregulates the immune system. Melanoma is a type of cancer associated with the skin.
Melanocytes (melanin-producing cells), become mutated and become cancerous. There are
many comparators which are highly effective in treating this disease and in this particular
study, the selected comparator is gp100. GP 100 stands for glycoprotein 100. Glycoproteins
are combinations of carbohydrate and protein. The protein content is present in the form of
long polypeptides with attached glycoprotein side chains. These glycoproteins are used in
preparing immune vaccines for the treatment of melanoma in patients. Immune vaccines are
certain vaccines which boost or down-regulates the immune system of the human body. The
study was done to check the strengths of Ipilimumab (a drug used to treat melanoma) in
various methods by using Ipilimumab individually (monotherapy), Ipilimumab+gp100 (bi-
therapy) and simply with gp100. It was found that the survivability rate in case of using
Ipilimumab is comparatively higher than others. Melanoma proceeds through five stages. The
severity of the disease ascends through the stages. Ipilimumab is administered only at the late
stages of melanoma. The Grade 3 and Grade 4 patients were treated with Ipilimumab, and it
was found that the average survivability rate for the Ipilimumab is 10.1 months higher than
gp100. The dose of the Ipilimumab recommended by the physicians is 3mg/kg. This dose has
been standardized and then decide by the doctors as a standard dose. Markov model is a
Abstract:
Cancer has been a disease of major concern today. Skin cancers are one of the most prevalent
cancers throughout the world. Various treatment strategies have been devised to treat
melanoma. This project aims to examine the applicability and the cost-effectiveness of using
Ipilimumab. This drug is administered to improve the survivability of the patients suffering
from advanced melanoma. Cost-effectiveness becomes a matter of concern when a particular
strategy or technique is higher in cost. Ipilimumab is defined to be a monoclonal antibody
that activates the immune system by targeting CTLA-4. CTLA-4 is a protein receptor that
downregulates the immune system. Melanoma is a type of cancer associated with the skin.
Melanocytes (melanin-producing cells), become mutated and become cancerous. There are
many comparators which are highly effective in treating this disease and in this particular
study, the selected comparator is gp100. GP 100 stands for glycoprotein 100. Glycoproteins
are combinations of carbohydrate and protein. The protein content is present in the form of
long polypeptides with attached glycoprotein side chains. These glycoproteins are used in
preparing immune vaccines for the treatment of melanoma in patients. Immune vaccines are
certain vaccines which boost or down-regulates the immune system of the human body. The
study was done to check the strengths of Ipilimumab (a drug used to treat melanoma) in
various methods by using Ipilimumab individually (monotherapy), Ipilimumab+gp100 (bi-
therapy) and simply with gp100. It was found that the survivability rate in case of using
Ipilimumab is comparatively higher than others. Melanoma proceeds through five stages. The
severity of the disease ascends through the stages. Ipilimumab is administered only at the late
stages of melanoma. The Grade 3 and Grade 4 patients were treated with Ipilimumab, and it
was found that the average survivability rate for the Ipilimumab is 10.1 months higher than
gp100. The dose of the Ipilimumab recommended by the physicians is 3mg/kg. This dose has
been standardized and then decide by the doctors as a standard dose. Markov model is a
2IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
model used to frame randomly changing processes. In this paper, the economic evaluation
has been done by introducing the Markov model, where three factors are associated with the
clinical outcomes, quality of life and resources related to healthcare. Markov model is used
here since the economy is a factor which changes always. Some parameters control the
economic models, but in this case, the payers’ interest plays a significant role. Indeed the use
of Ipilimumab is 95% cost-effective as compared to others. The policy practice and the
Australian government subsidization is under consideration based on the results. The schemes
are designed after analyzing the data and the survivability rate after the drug administration in
over two years. The investment and the sponsorship are certainly needed from the
government side to counter the treatment cost. Thus after analyzing the budget structure and
the cost-effectiveness, it is recommended to the government to implement the policies that
are conducive to encounter the heavy burden of the treatment.
model used to frame randomly changing processes. In this paper, the economic evaluation
has been done by introducing the Markov model, where three factors are associated with the
clinical outcomes, quality of life and resources related to healthcare. Markov model is used
here since the economy is a factor which changes always. Some parameters control the
economic models, but in this case, the payers’ interest plays a significant role. Indeed the use
of Ipilimumab is 95% cost-effective as compared to others. The policy practice and the
Australian government subsidization is under consideration based on the results. The schemes
are designed after analyzing the data and the survivability rate after the drug administration in
over two years. The investment and the sponsorship are certainly needed from the
government side to counter the treatment cost. Thus after analyzing the budget structure and
the cost-effectiveness, it is recommended to the government to implement the policies that
are conducive to encounter the heavy burden of the treatment.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
Appraisal Checklists:
Appraisal checklist 1:
Question Yes No Referenced from
Did the article describe
an important clinical
problem addressed via
a clearly formulated
question?
Menzies, A.M., Johnson, D.B.,
Ramanujam, S., Atkinson, V.G., Wong,
A.N.M., Park, J.J., McQuade, J.L.,
Shoushtari, A.N., Tsai, K.K., Eroglu, Z.
and Klein, O., 2016. Anti-PD-1 therapy in
patients with advanced melanoma and
preexisting autoimmune disorders or
major toxicity with Ipilimumab. Annals of
Oncology, 28(2), pp.368-376.
Wolchok, J.D., Hodi, F.S., Weber, J.S.,
Allison, J.P., Urba, W.J., Robert, C.,
O'Day, S.J., Hoos, A., Humphrey, R.,
Berman, D.M. and Lonberg, N., 2013.
Development of Ipilimumab: a novel
immunotherapeutic approach for the
treatment of advanced melanoma. Annals
of the New York Academy of
Sciences, 1291(1), p.1.
Yang, J.C., Hughes, M., Kammula, U.,
Royal, R., Sherry, R.M., Topalian, S.L.,
Suri, K.B., Levy, C., Allen, T.,
Mavroukakis, S. and Lowy, I., 2017.
Ipilimumab (anti-CTLA4 antibody) causes
regression of metastatic renal cell cancer
associated with enteritis and
hypophysitis. Journal of immunotherapy
(Hagerstown, Md.: 1997), 30(8), p.825.
Was a qualitative
approach appropriate?
Was the sampling
strategy clearly defined
and justified? In
particular
Appraisal Checklists:
Appraisal checklist 1:
Question Yes No Referenced from
Did the article describe
an important clinical
problem addressed via
a clearly formulated
question?
Menzies, A.M., Johnson, D.B.,
Ramanujam, S., Atkinson, V.G., Wong,
A.N.M., Park, J.J., McQuade, J.L.,
Shoushtari, A.N., Tsai, K.K., Eroglu, Z.
and Klein, O., 2016. Anti-PD-1 therapy in
patients with advanced melanoma and
preexisting autoimmune disorders or
major toxicity with Ipilimumab. Annals of
Oncology, 28(2), pp.368-376.
Wolchok, J.D., Hodi, F.S., Weber, J.S.,
Allison, J.P., Urba, W.J., Robert, C.,
O'Day, S.J., Hoos, A., Humphrey, R.,
Berman, D.M. and Lonberg, N., 2013.
Development of Ipilimumab: a novel
immunotherapeutic approach for the
treatment of advanced melanoma. Annals
of the New York Academy of
Sciences, 1291(1), p.1.
Yang, J.C., Hughes, M., Kammula, U.,
Royal, R., Sherry, R.M., Topalian, S.L.,
Suri, K.B., Levy, C., Allen, T.,
Mavroukakis, S. and Lowy, I., 2017.
Ipilimumab (anti-CTLA4 antibody) causes
regression of metastatic renal cell cancer
associated with enteritis and
hypophysitis. Journal of immunotherapy
(Hagerstown, Md.: 1997), 30(8), p.825.
Was a qualitative
approach appropriate?
Was the sampling
strategy clearly defined
and justified? In
particular
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
Was there a Clear
discussion of the
technology given?
Curl, P., Vujic, I., van't Veer, L.J., Ortiz-
Urda, S. and Kahn, J.G., 2014. Cost-
effectiveness of treatment strategies for
BRAF-mutated metastatic
melanoma. PLoS One, 9(9), p.e107255.
Del Vecchio, M., Di Guardo, L., Ascierto,
P.A., Grimaldi, A.M., Sileni, V.C.,
Pigozzo, J., Ferraresi, V., Nuzzo, C.,
Rinaldi, G., Testori, A. and Ferrucci, P.F.,
2014. Efficacy and safety of Ipilimumab 3
mg/kg in patients with pretreated,
metastatic, mucosal melanoma. European
Journal of Cancer, 50(1), pp.121-127.
Del Vecchio, M., Di Guardo, L., Ascierto,
P.A., Grimaldi, A.M., Sileni, V.C.,
Pigozzo, J., Ferraresi, V., Nuzzo, C.,
Rinaldi, G., Testori, A. and Ferrucci, P.F.,
2014. Efficacy and safety of Ipilimumab 3
mg/kg in patients with pretreated,
metastatic, mucosal melanoma. European
Journal of Cancer, 50(1), pp.121-127.
Drysdale, E., Peng, Y., Nguyen, P., Baetz,
T. and Hanna, T.P., 2019. A population-
based study of the treatment effect of first-
line Ipilimumab for metastatic or
unresectable melanoma. Melanoma
research.
Elliott, T.M., Whiteman, D.C., Olsen,
C.M. and Gordon, L.G., 2017. Estimated
healthcare costs of melanoma in Australia
over 3 years post-diagnosis. Applied
health economics and health policy, 15(6),
pp.805-816.
Geynisman, D.M., Chien, C.R.,
Smieliauskas, F., Shen, C. and Shih,
Y.C.T., 2014. Economic evaluation of
therapeutic cancer vaccines and
immunotherapy: A systematic
review. Human vaccines &
immunotherapeutics, 10(11), pp.3415-
3424.
Was there a Clear
discussion of the
technology given?
Curl, P., Vujic, I., van't Veer, L.J., Ortiz-
Urda, S. and Kahn, J.G., 2014. Cost-
effectiveness of treatment strategies for
BRAF-mutated metastatic
melanoma. PLoS One, 9(9), p.e107255.
Del Vecchio, M., Di Guardo, L., Ascierto,
P.A., Grimaldi, A.M., Sileni, V.C.,
Pigozzo, J., Ferraresi, V., Nuzzo, C.,
Rinaldi, G., Testori, A. and Ferrucci, P.F.,
2014. Efficacy and safety of Ipilimumab 3
mg/kg in patients with pretreated,
metastatic, mucosal melanoma. European
Journal of Cancer, 50(1), pp.121-127.
Del Vecchio, M., Di Guardo, L., Ascierto,
P.A., Grimaldi, A.M., Sileni, V.C.,
Pigozzo, J., Ferraresi, V., Nuzzo, C.,
Rinaldi, G., Testori, A. and Ferrucci, P.F.,
2014. Efficacy and safety of Ipilimumab 3
mg/kg in patients with pretreated,
metastatic, mucosal melanoma. European
Journal of Cancer, 50(1), pp.121-127.
Drysdale, E., Peng, Y., Nguyen, P., Baetz,
T. and Hanna, T.P., 2019. A population-
based study of the treatment effect of first-
line Ipilimumab for metastatic or
unresectable melanoma. Melanoma
research.
Elliott, T.M., Whiteman, D.C., Olsen,
C.M. and Gordon, L.G., 2017. Estimated
healthcare costs of melanoma in Australia
over 3 years post-diagnosis. Applied
health economics and health policy, 15(6),
pp.805-816.
Geynisman, D.M., Chien, C.R.,
Smieliauskas, F., Shen, C. and Shih,
Y.C.T., 2014. Economic evaluation of
therapeutic cancer vaccines and
immunotherapy: A systematic
review. Human vaccines &
immunotherapeutics, 10(11), pp.3415-
3424.
5IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
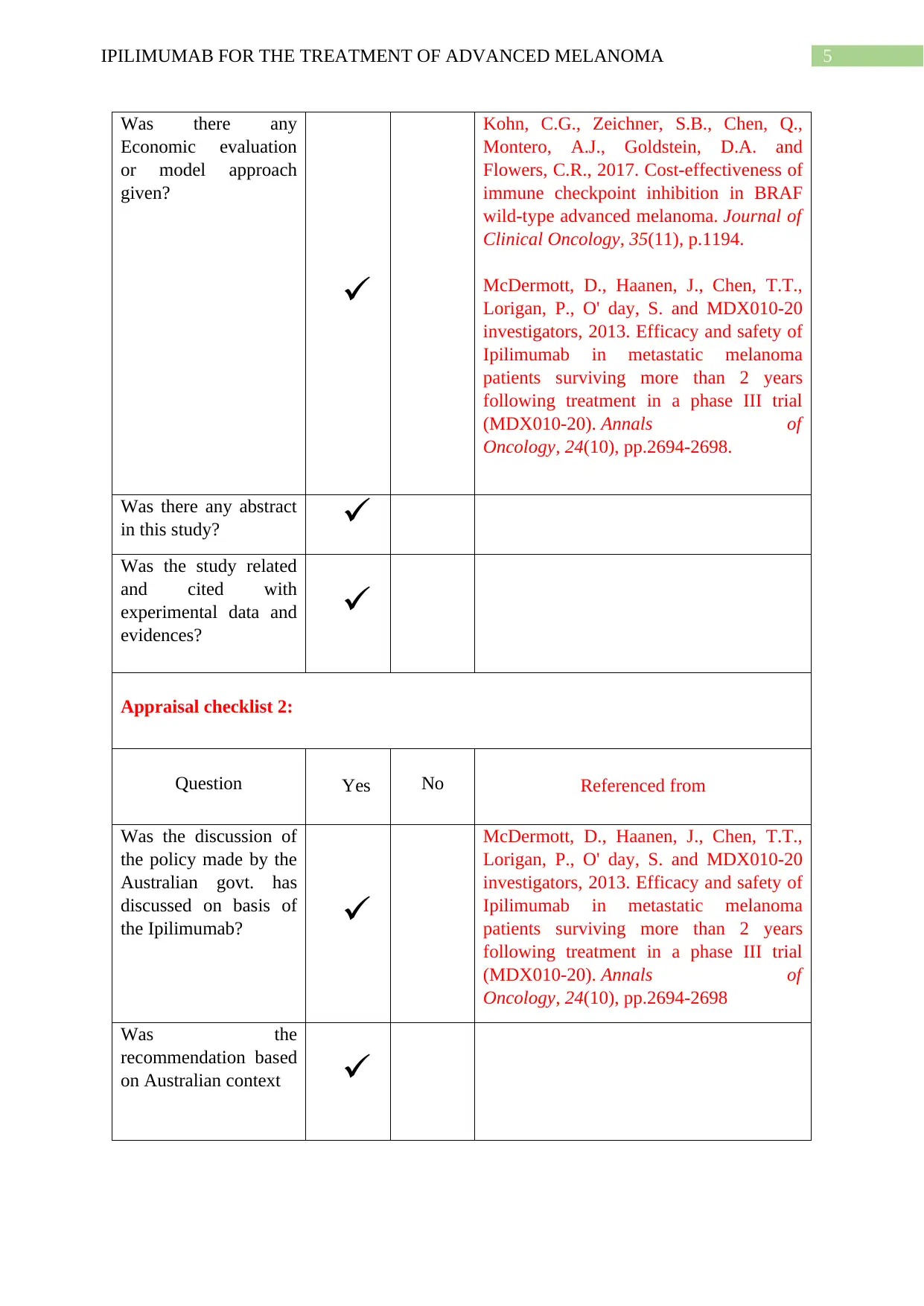
Was there any
Economic evaluation
or model approach
given?
Kohn, C.G., Zeichner, S.B., Chen, Q.,
Montero, A.J., Goldstein, D.A. and
Flowers, C.R., 2017. Cost-effectiveness of
immune checkpoint inhibition in BRAF
wild-type advanced melanoma. Journal of
Clinical Oncology, 35(11), p.1194.
McDermott, D., Haanen, J., Chen, T.T.,
Lorigan, P., O' day, S. and MDX010-20
investigators, 2013. Efficacy and safety of
Ipilimumab in metastatic melanoma
patients surviving more than 2 years
following treatment in a phase III trial
(MDX010-20). Annals of
Oncology, 24(10), pp.2694-2698.
Was there any abstract
in this study?
Was the study related
and cited with
experimental data and
evidences?
Appraisal checklist 2:
Question Yes No Referenced from
Was the discussion of
the policy made by the
Australian govt. has
discussed on basis of
the Ipilimumab?
McDermott, D., Haanen, J., Chen, T.T.,
Lorigan, P., O' day, S. and MDX010-20
investigators, 2013. Efficacy and safety of
Ipilimumab in metastatic melanoma
patients surviving more than 2 years
following treatment in a phase III trial
(MDX010-20). Annals of
Oncology, 24(10), pp.2694-2698
Was the
recommendation based
on Australian context
Was there any
Economic evaluation
or model approach
given?
Kohn, C.G., Zeichner, S.B., Chen, Q.,
Montero, A.J., Goldstein, D.A. and
Flowers, C.R., 2017. Cost-effectiveness of
immune checkpoint inhibition in BRAF
wild-type advanced melanoma. Journal of
Clinical Oncology, 35(11), p.1194.
McDermott, D., Haanen, J., Chen, T.T.,
Lorigan, P., O' day, S. and MDX010-20
investigators, 2013. Efficacy and safety of
Ipilimumab in metastatic melanoma
patients surviving more than 2 years
following treatment in a phase III trial
(MDX010-20). Annals of
Oncology, 24(10), pp.2694-2698.
Was there any abstract
in this study?
Was the study related
and cited with
experimental data and
evidences?
Appraisal checklist 2:
Question Yes No Referenced from
Was the discussion of
the policy made by the
Australian govt. has
discussed on basis of
the Ipilimumab?
McDermott, D., Haanen, J., Chen, T.T.,
Lorigan, P., O' day, S. and MDX010-20
investigators, 2013. Efficacy and safety of
Ipilimumab in metastatic melanoma
patients surviving more than 2 years
following treatment in a phase III trial
(MDX010-20). Annals of
Oncology, 24(10), pp.2694-2698
Was the
recommendation based
on Australian context
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
To what extent are the
findings of the study
transferable to make
healthcare schemes?
Was the conclusion
justified to the thesis
statement?
To what extent are the
findings of the study
transferable to make
healthcare schemes?
Was the conclusion
justified to the thesis
statement?
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
Introduction:
Ipilimumab, an effective drug to that, is used in case of immunotherapy to counter
carcinogenic cells. In this study, the application of this drug is confined within the field of
melanoma treatment (Drysdale et al. 2019). The drug attacks the T-cells of the body and acts
as a blocker to tumour cells (Yang et al. 2017). This immunotherapy is indeed expensive.
Thus the aim of this project is to critically examine and justify the cost-effectiveness and the
survivability rate of the immunotherapy by using Ipilimumab.
Discussion:
The discussion is based on the use of Ipilimumab in advanced melanoma, its
survivability rate by applying on patients and the cost-effectiveness of using this drug.
Background and Description of Ipilimumab:
Ipilimumab is an effective drug to treat skin cancer (melanoma). According to
Intlekofer and Thompson (2013) Ipilimumab aims CTLA-4 (Cytotoxic T lymphocyte) protein
and block this molecule to terminate the proliferation of melanoma cells in the human body.
Ipilimumab is a monoclonal antibody and an immune checkpoint inhibitor. The medicinal
name of Ipilimumab is MDX-010, and commercial name is Yervoy. Melanoma treatment is
harder at later stages. According to the report of WHO (World Health Organization), in the
year 2008 among 200,000 patients suffering from acute advanced melanoma 46,000 died. In
the year of 2011 in the US, 8790 people died among 70,230 (Barzey et al. 2013). The cases
of melanoma are also increasing in Australia, the European Union, and South Africa also.
Comparator, population and circumstances of using Ipilimumab:
The most effective and operative comparator of Ipilimumab is gp100 (glycoprotein
100, a tumour antigen, specifically used for cancer cell chemotherapy treatment). The
Introduction:
Ipilimumab, an effective drug to that, is used in case of immunotherapy to counter
carcinogenic cells. In this study, the application of this drug is confined within the field of
melanoma treatment (Drysdale et al. 2019). The drug attacks the T-cells of the body and acts
as a blocker to tumour cells (Yang et al. 2017). This immunotherapy is indeed expensive.
Thus the aim of this project is to critically examine and justify the cost-effectiveness and the
survivability rate of the immunotherapy by using Ipilimumab.
Discussion:
The discussion is based on the use of Ipilimumab in advanced melanoma, its
survivability rate by applying on patients and the cost-effectiveness of using this drug.
Background and Description of Ipilimumab:
Ipilimumab is an effective drug to treat skin cancer (melanoma). According to
Intlekofer and Thompson (2013) Ipilimumab aims CTLA-4 (Cytotoxic T lymphocyte) protein
and block this molecule to terminate the proliferation of melanoma cells in the human body.
Ipilimumab is a monoclonal antibody and an immune checkpoint inhibitor. The medicinal
name of Ipilimumab is MDX-010, and commercial name is Yervoy. Melanoma treatment is
harder at later stages. According to the report of WHO (World Health Organization), in the
year 2008 among 200,000 patients suffering from acute advanced melanoma 46,000 died. In
the year of 2011 in the US, 8790 people died among 70,230 (Barzey et al. 2013). The cases
of melanoma are also increasing in Australia, the European Union, and South Africa also.
Comparator, population and circumstances of using Ipilimumab:
The most effective and operative comparator of Ipilimumab is gp100 (glycoprotein
100, a tumour antigen, specifically used for cancer cell chemotherapy treatment). The
8IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
application of gp100 is unapproved because the experimental observation on economic
evaluation and cost-effectiveness of gp100 is under confirmation (Wolchok et al. 2013). Thus
for the analysis, a potential standard is highly needed, which is actually Ipilimumab.
Population affected by melanoma are directly related to this treatment procedure. A
very effective treatment model (time-dependent treatment model) was used among 2793
patients who were suffering from acute melanoma. In this population-based study in Ontario
during the year period of 2007-2015, only 289 patients were treated with Ipilimumab (2010-
2015) and from the remaining 175 were given dacarbazine care (Barzey et al. 2013). It was
observed that, Ipilimumab adjusted the danger ratio.. In the case of sensitivity based
population study, the utilities found from the Ipilimumab (MDX010-20) was assessed on
applying the drug on people (McDermott et al. 2013). The result was Ipilimumab is more
sensitive and effective to quality of life. The competitors of this drug are way more specific
to carcinogenic cells and not on life quality factor.
The circumstances of using Ipilimumab is a cancer therapy (immunotherapy, a
specialized part of chemotherapy). Ipilimumab which helps to shrink the cancer cells and
tumours of patients affected by advanced melanoma.
application of gp100 is unapproved because the experimental observation on economic
evaluation and cost-effectiveness of gp100 is under confirmation (Wolchok et al. 2013). Thus
for the analysis, a potential standard is highly needed, which is actually Ipilimumab.
Population affected by melanoma are directly related to this treatment procedure. A
very effective treatment model (time-dependent treatment model) was used among 2793
patients who were suffering from acute melanoma. In this population-based study in Ontario
during the year period of 2007-2015, only 289 patients were treated with Ipilimumab (2010-
2015) and from the remaining 175 were given dacarbazine care (Barzey et al. 2013). It was
observed that, Ipilimumab adjusted the danger ratio.. In the case of sensitivity based
population study, the utilities found from the Ipilimumab (MDX010-20) was assessed on
applying the drug on people (McDermott et al. 2013). The result was Ipilimumab is more
sensitive and effective to quality of life. The competitors of this drug are way more specific
to carcinogenic cells and not on life quality factor.
The circumstances of using Ipilimumab is a cancer therapy (immunotherapy, a
specialized part of chemotherapy). Ipilimumab which helps to shrink the cancer cells and
tumours of patients affected by advanced melanoma.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
Safety, Efficacy and effectiveness of Ipilimumab:
There are a few safety measures regarding the usage of Ipilimumab are as follows:
Age should be minimum of 16 years theoretically, but it would be better if the patient
is at least 18 years minimum.
It can be used only for the cases which are at stage 3 or stage 4 of advanced
melanoma and surgically un-operative (unresectable).
Doses are 3 mg per kg, and this will be continued in 3 weeks for the four treatments
(Del Vecchio et al. 2014).
Assessment of the tumour cell must be done after 12 or 13 weeks for the eligibility to
use Ipilimumab.
The analysis of data ensures the Efficacy of using Ipilimumab in case of treating
advanced melanoma. The effectiveness of using Ipilimumab was supported by the random
trial on patients who are suffering from advanced melanoma. The case study was done on
patients who got monotherapy (only use of Ipilimumab), bi-therapy (Ipilimumab+ gp100)
and protein alone. The result of times for the survivability found 21 months in bi-therapy,
27.8 months for monotherapy and 17.2 months for the protein (gp100). Hence the Efficacy
and effectiveness of Ipilimumab have found (Hodi et al. 2010).
Economic Evaluation of Ipilimumab with modelling approach:
The economic evaluation was done on the basis of Markov Economic Healthcare
Model. There are three factors which determine the cost-effectiveness of the model those are
the stable disease, progression and death (Kohn et al. 2017). In this specific case, the model
parameter which determines the factors in this model is the perspective of the payer.
Parameters such as productivity loss, cost of the patient time and cost in case of transport are
not considered here.
Safety, Efficacy and effectiveness of Ipilimumab:
There are a few safety measures regarding the usage of Ipilimumab are as follows:
Age should be minimum of 16 years theoretically, but it would be better if the patient
is at least 18 years minimum.
It can be used only for the cases which are at stage 3 or stage 4 of advanced
melanoma and surgically un-operative (unresectable).
Doses are 3 mg per kg, and this will be continued in 3 weeks for the four treatments
(Del Vecchio et al. 2014).
Assessment of the tumour cell must be done after 12 or 13 weeks for the eligibility to
use Ipilimumab.
The analysis of data ensures the Efficacy of using Ipilimumab in case of treating
advanced melanoma. The effectiveness of using Ipilimumab was supported by the random
trial on patients who are suffering from advanced melanoma. The case study was done on
patients who got monotherapy (only use of Ipilimumab), bi-therapy (Ipilimumab+ gp100)
and protein alone. The result of times for the survivability found 21 months in bi-therapy,
27.8 months for monotherapy and 17.2 months for the protein (gp100). Hence the Efficacy
and effectiveness of Ipilimumab have found (Hodi et al. 2010).
Economic Evaluation of Ipilimumab with modelling approach:
The economic evaluation was done on the basis of Markov Economic Healthcare
Model. There are three factors which determine the cost-effectiveness of the model those are
the stable disease, progression and death (Kohn et al. 2017). In this specific case, the model
parameter which determines the factors in this model is the perspective of the payer.
Parameters such as productivity loss, cost of the patient time and cost in case of transport are
not considered here.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
Outcome measures in clinical evidence and its relation with economic evidence:
After an experimental trial, it was found that 20% of the patients are still alive in this
Ipilimumab trial. From the clinical outcome, it was found that an average number of patients
treated with Ipilimumab got an estimated life expectancy approx. Three years which is
generally higher than other health technology used in advanced melanoma. The life
expectancy is about 20% high in case of Ipilimumab (Curl et al. 2014). Thus, it is found from
the model-based approach of economic evaluation that Ipilimumab is 95% possibly to be
economical and effective at a willingness-to-pay of £146,000/QALY (Geynisman et al.
2014).
Justification of resource used for economic evaluation:
It has been found from the discussion that the cost factor and the perspective of the
payer is the sole factor in evaluating and justifying the economic model. Markov model has
been used to evaluate. Ipilimumab is not very cost effective.The PD-1 drug is way more cost-
effective in comparison to Ipilimumab (Menzies et al. 2016). Other factors are survivability,
clinical outcomes of using Ipilimumab.
Impact of uncertainty and assumption on results:
There is some uncertainly playing a crucial role in the survivability estimation. The
survival extrapolation of the data regarding the trial of MDX010-20 affects the result. The
data was based on some basic assumptions based on the Markov model. Studies were based
on the comparison of the survivability rate of monotherapy and bi-therapy
(ipilimumab+gp100) is precise enough (the result was 20% in comparison to other).
Cost-effectiveness of using Ipilimumab:
In 2010 the checkpoint inhibitor was used for immunotherapy was the Ipilimumab
which was very effective by performance but not by cost. Several economic models were
Outcome measures in clinical evidence and its relation with economic evidence:
After an experimental trial, it was found that 20% of the patients are still alive in this
Ipilimumab trial. From the clinical outcome, it was found that an average number of patients
treated with Ipilimumab got an estimated life expectancy approx. Three years which is
generally higher than other health technology used in advanced melanoma. The life
expectancy is about 20% high in case of Ipilimumab (Curl et al. 2014). Thus, it is found from
the model-based approach of economic evaluation that Ipilimumab is 95% possibly to be
economical and effective at a willingness-to-pay of £146,000/QALY (Geynisman et al.
2014).
Justification of resource used for economic evaluation:
It has been found from the discussion that the cost factor and the perspective of the
payer is the sole factor in evaluating and justifying the economic model. Markov model has
been used to evaluate. Ipilimumab is not very cost effective.The PD-1 drug is way more cost-
effective in comparison to Ipilimumab (Menzies et al. 2016). Other factors are survivability,
clinical outcomes of using Ipilimumab.
Impact of uncertainty and assumption on results:
There is some uncertainly playing a crucial role in the survivability estimation. The
survival extrapolation of the data regarding the trial of MDX010-20 affects the result. The
data was based on some basic assumptions based on the Markov model. Studies were based
on the comparison of the survivability rate of monotherapy and bi-therapy
(ipilimumab+gp100) is precise enough (the result was 20% in comparison to other).
Cost-effectiveness of using Ipilimumab:
In 2010 the checkpoint inhibitor was used for immunotherapy was the Ipilimumab
which was very effective by performance but not by cost. Several economic models were
11IPILIMUMAB FOR THE TREATMENT OF ADVANCED MELANOMA
involved in the analysis of the cost-effectiveness of Ipilimumab; the best one of them is the
Markov model. According to that model, the QALY (quality-adjusted life year) is
considerably high for the Ipilimumab+gp100 or Ipilimumab + Nivolumab. Injection per cost
is $ 30,000; thus, four doses need $ 120,000, which is certainly a threat to the payer (Curl et
al. 2014).
Applicability and Recommendation of Ipilimumab in the Australian context:
The applicability of Ipilimumab in case of treating the melanoma is certainly a case of
consideration. The Australian government subsidization in case of treatment with Ipilimumab
is based on the condition of sponsorship of the “managed entry scheme” to examine the
outcome of 2-year survivability rate of the patients (Elliott et al. 2017). Thus a positive
outcome (that is survivability and quality of life) from the results is needed to prepare a
health policy to counter the advance melanoma from the government side.
Conclusion:
Ipilimumab use in treatment of the advanced melanoma is highly effective, and it is
also justified by the clinical outcomes that have found experimentally. In cost effective
evaluation of using Ipilimumab, it was found that the treatment is expensive. Dealing with
financial problems recommendeds that the government should make such subsidized schemes
so that people affected by melanoma can avail the facility easily.
involved in the analysis of the cost-effectiveness of Ipilimumab; the best one of them is the
Markov model. According to that model, the QALY (quality-adjusted life year) is
considerably high for the Ipilimumab+gp100 or Ipilimumab + Nivolumab. Injection per cost
is $ 30,000; thus, four doses need $ 120,000, which is certainly a threat to the payer (Curl et
al. 2014).
Applicability and Recommendation of Ipilimumab in the Australian context:
The applicability of Ipilimumab in case of treating the melanoma is certainly a case of
consideration. The Australian government subsidization in case of treatment with Ipilimumab
is based on the condition of sponsorship of the “managed entry scheme” to examine the
outcome of 2-year survivability rate of the patients (Elliott et al. 2017). Thus a positive
outcome (that is survivability and quality of life) from the results is needed to prepare a
health policy to counter the advance melanoma from the government side.
Conclusion:
Ipilimumab use in treatment of the advanced melanoma is highly effective, and it is
also justified by the clinical outcomes that have found experimentally. In cost effective
evaluation of using Ipilimumab, it was found that the treatment is expensive. Dealing with
financial problems recommendeds that the government should make such subsidized schemes
so that people affected by melanoma can avail the facility easily.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 15
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.