Impact of IYCF Education on Infant Mortality in Aboriginal Population in Australia
VerifiedAdded on 2023/06/12
|11
|3318
|233
AI Summary
This study aims to evaluate the effect of Infant and young child feeding (IYCF) education program on reducing mortality rate in infants and children in Aboriginal community in Australia. The study will implement a randomised controlled trial and collect data on exclusive breastfeeding rate, duration of breastfeeding, health status of child and mortality rate of child. The study will also assess the cost-effectiveness of the program.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Health Promotion
1
1
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Title: Infant and young child feeding (IYCF) education and its impact on infant
mortality in Aboriginal population in Australia.
Abstract.
Infant and young child feeding (IYCF) will provide the necessary information through
education required to address breastfeeding problems such as retarded growth and mortality
in Aboriginal women in Australia.
Through this program awareness will be increased on the knowledge, attitude as well as
understanding about breastfeeding among Aboriginal women. It can also be helpful in finding
impact of mother’s education on breastfeeding. Potential problems related to breastfeeding
can be identified through this programme. It can be helpful in improving health and well-
being of entire society.
Background, brief literature and rationale:
Inadequate breast feeding is the most significant reason for approximately 60 % of infant and
child mortality globally. It has been established that two-thirds of the undernutrition children
feature is present in the first year of their life. Children’s growth, development and survival
can be effectively improved by Exclusive breastfeeding (EBF) in the first six months of their
life. It has been estimated that EBF can reduce children’s mortality by 20 %. EBF has been
proved as the effective preventive strategy for child mortality (Arimond et al., 2008). World
Health Organization (WHO) gave importance to address this issue because inadequate
breastfeeding can negatively influence socioeconomic development and it can augment
poverty. WHO recommended to initiate breastfeeding within first four hours after birth. In
Aboriginal people mortality rate of child is higher and it is at 25 per 1000 live births. In these
Aboriginal people, this mortality rate is still higher in children who received breastfeeding
after 24 hours after birth (McLachlan et al., 2017).
From the studies, it has been demonstrated that only 65 – 75 5 of the women breastfed new-
born in first four hours after their birth (Khan et al., 2014). Educational level of women plays
important role in initiation of breastfeeding, exclusive breastfeeding practice (EBF) and
duration of breastfeeding (Daelmans et al., 2009). However, there is less evidence for
establishing relationship between educational status of Aboriginal women and breastfeeding.
This issue is less addressed because educational status of Aboriginal women is less as
compared to other women.
2
mortality in Aboriginal population in Australia.
Abstract.
Infant and young child feeding (IYCF) will provide the necessary information through
education required to address breastfeeding problems such as retarded growth and mortality
in Aboriginal women in Australia.
Through this program awareness will be increased on the knowledge, attitude as well as
understanding about breastfeeding among Aboriginal women. It can also be helpful in finding
impact of mother’s education on breastfeeding. Potential problems related to breastfeeding
can be identified through this programme. It can be helpful in improving health and well-
being of entire society.
Background, brief literature and rationale:
Inadequate breast feeding is the most significant reason for approximately 60 % of infant and
child mortality globally. It has been established that two-thirds of the undernutrition children
feature is present in the first year of their life. Children’s growth, development and survival
can be effectively improved by Exclusive breastfeeding (EBF) in the first six months of their
life. It has been estimated that EBF can reduce children’s mortality by 20 %. EBF has been
proved as the effective preventive strategy for child mortality (Arimond et al., 2008). World
Health Organization (WHO) gave importance to address this issue because inadequate
breastfeeding can negatively influence socioeconomic development and it can augment
poverty. WHO recommended to initiate breastfeeding within first four hours after birth. In
Aboriginal people mortality rate of child is higher and it is at 25 per 1000 live births. In these
Aboriginal people, this mortality rate is still higher in children who received breastfeeding
after 24 hours after birth (McLachlan et al., 2017).
From the studies, it has been demonstrated that only 65 – 75 5 of the women breastfed new-
born in first four hours after their birth (Khan et al., 2014). Educational level of women plays
important role in initiation of breastfeeding, exclusive breastfeeding practice (EBF) and
duration of breastfeeding (Daelmans et al., 2009). However, there is less evidence for
establishing relationship between educational status of Aboriginal women and breastfeeding.
This issue is less addressed because educational status of Aboriginal women is less as
compared to other women.
2
Surely, improvement in the educational status of the women in Aboriginal community can be
helpful in improving breastfeeding status and reduction in the mortality rate of infants.
Multiple health and social determinants can influence health and quality of life in Aboriginal
children. It is necessary to explore influence of educational status of Aboriginal women on
breastfeeding and mortality rate of infants and children (Barnes and Rowe, 2013).
Goal :
Aim of this study is to evaluate effect of Infant and young child feeding (IYCF) education
programme on reducing mortality rate in infant and children in Aboriginal community.
Objectives :
Can IYCF education programme in Aboriginal mothers lessen child mortality ?
Is IYCF programme in Aboriginal mothers is cost effective?
What is effectiveness and efficiency of IYCF programme through retired healthcare
professionals?.
Study design:
In this health promotion programme, randomised controlled trial will be implemented. In
randomised controlled trial, subjects get randomised in different groups (Cook et al., 2015).
One group would be intervention group; study group and another group would be without
intervention; control group. Aboriginal women selected in this would be from the low
socioeconomic class. Educational status of these women is low in comparison to the women
in the high socioeconomic class.
Time frame:
Work to be accomplished
Quarter 1
Months
Quarter 2
Months
Quarter 3
Months
1 2 3 4 1 2 3 4 1 2 3 4
Ethics clearance X
Project set-up X
3
helpful in improving breastfeeding status and reduction in the mortality rate of infants.
Multiple health and social determinants can influence health and quality of life in Aboriginal
children. It is necessary to explore influence of educational status of Aboriginal women on
breastfeeding and mortality rate of infants and children (Barnes and Rowe, 2013).
Goal :
Aim of this study is to evaluate effect of Infant and young child feeding (IYCF) education
programme on reducing mortality rate in infant and children in Aboriginal community.
Objectives :
Can IYCF education programme in Aboriginal mothers lessen child mortality ?
Is IYCF programme in Aboriginal mothers is cost effective?
What is effectiveness and efficiency of IYCF programme through retired healthcare
professionals?.
Study design:
In this health promotion programme, randomised controlled trial will be implemented. In
randomised controlled trial, subjects get randomised in different groups (Cook et al., 2015).
One group would be intervention group; study group and another group would be without
intervention; control group. Aboriginal women selected in this would be from the low
socioeconomic class. Educational status of these women is low in comparison to the women
in the high socioeconomic class.
Time frame:
Work to be accomplished
Quarter 1
Months
Quarter 2
Months
Quarter 3
Months
1 2 3 4 1 2 3 4 1 2 3 4
Ethics clearance X
Project set-up X
3
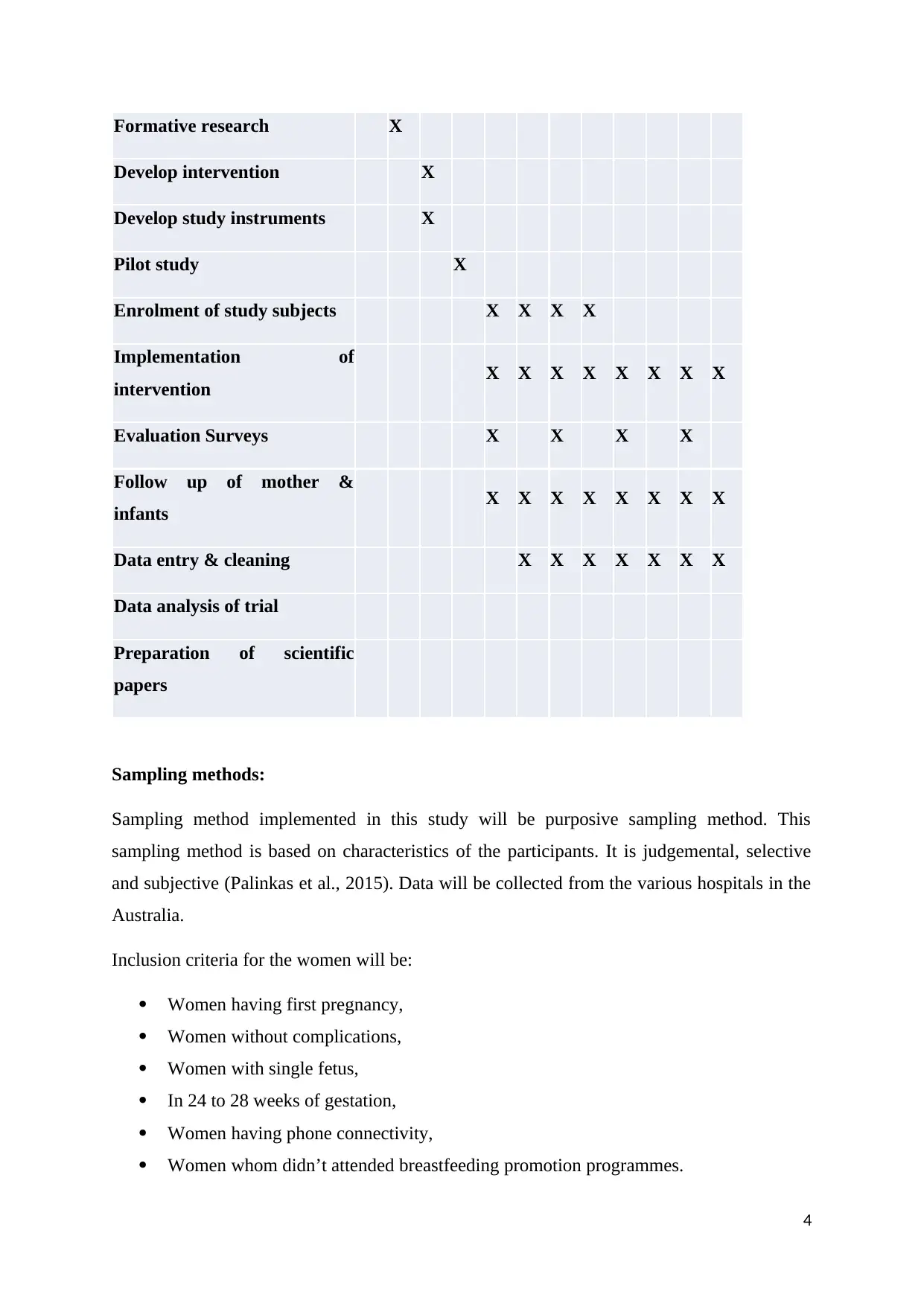
Formative research X
Develop intervention X
Develop study instruments X
Pilot study X
Enrolment of study subjects X X X X
Implementation of
intervention X X X X X X X X
Evaluation Surveys X X X X
Follow up of mother &
infants X X X X X X X X
Data entry & cleaning X X X X X X X
Data analysis of trial
Preparation of scientific
papers
Sampling methods:
Sampling method implemented in this study will be purposive sampling method. This
sampling method is based on characteristics of the participants. It is judgemental, selective
and subjective (Palinkas et al., 2015). Data will be collected from the various hospitals in the
Australia.
Inclusion criteria for the women will be:
Women having first pregnancy,
Women without complications,
Women with single fetus,
In 24 to 28 weeks of gestation,
Women having phone connectivity,
Women whom didn’t attended breastfeeding promotion programmes.
4
Develop intervention X
Develop study instruments X
Pilot study X
Enrolment of study subjects X X X X
Implementation of
intervention X X X X X X X X
Evaluation Surveys X X X X
Follow up of mother &
infants X X X X X X X X
Data entry & cleaning X X X X X X X
Data analysis of trial
Preparation of scientific
papers
Sampling methods:
Sampling method implemented in this study will be purposive sampling method. This
sampling method is based on characteristics of the participants. It is judgemental, selective
and subjective (Palinkas et al., 2015). Data will be collected from the various hospitals in the
Australia.
Inclusion criteria for the women will be:
Women having first pregnancy,
Women without complications,
Women with single fetus,
In 24 to 28 weeks of gestation,
Women having phone connectivity,
Women whom didn’t attended breastfeeding promotion programmes.
4
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Exclusion criteria:
Women from the areas which cannot be reached.
Target population :
600 women will be included in this study. 300 will be from the study group and 300 will be
from control group. Recruitment will start from third trimester and it will continue upto 6
months of child age.
Ethical consideration:
Declaration of Helsinki will be considered for carrying out this study. Prior to initiation of the
study, ethical approval for the conduct of the study will be taken from Human Research
Ethics Committee (HREC). Study proposal will be presented to the ethics committee of the
Primary health centre and their suggestions will be considered. Written informed consent will
be taken from women and their family members prior to enrolment in the study. These
consent forms will be documented. Participated women will be allowed to withdraw from the
study at any point of time prior to initiation and during conduct of the study. Confidentiality
will be maintained for the participated women.
Methodology:
Maternal and child health (MCH) programme will be implemented for the women in control
group. MCH programme along with IYCF programme will be implemented for women in the
intervention group. Both MCH and IYCF programme will be implemented at the community
centres. IYCF education and training programme will be implemented for the duration of two
weeks. Retried health care professionals will be recruited for providing training and
education because they are more experienced in these training and educational programmes.
Training and educational programme by these retired health care professionals will be
provided both in practical and theoretical form. Importance of breastfeeding on child health,
importance of breastfeeding on mother’s health and different techniques of breastfeeding will
be incorporated in the theoretical aspects of training and education. Different techniques of
breastfeeding will be demonstrated by senior and retired nurses and elder members of the
5
Women from the areas which cannot be reached.
Target population :
600 women will be included in this study. 300 will be from the study group and 300 will be
from control group. Recruitment will start from third trimester and it will continue upto 6
months of child age.
Ethical consideration:
Declaration of Helsinki will be considered for carrying out this study. Prior to initiation of the
study, ethical approval for the conduct of the study will be taken from Human Research
Ethics Committee (HREC). Study proposal will be presented to the ethics committee of the
Primary health centre and their suggestions will be considered. Written informed consent will
be taken from women and their family members prior to enrolment in the study. These
consent forms will be documented. Participated women will be allowed to withdraw from the
study at any point of time prior to initiation and during conduct of the study. Confidentiality
will be maintained for the participated women.
Methodology:
Maternal and child health (MCH) programme will be implemented for the women in control
group. MCH programme along with IYCF programme will be implemented for women in the
intervention group. Both MCH and IYCF programme will be implemented at the community
centres. IYCF education and training programme will be implemented for the duration of two
weeks. Retried health care professionals will be recruited for providing training and
education because they are more experienced in these training and educational programmes.
Training and educational programme by these retired health care professionals will be
provided both in practical and theoretical form. Importance of breastfeeding on child health,
importance of breastfeeding on mother’s health and different techniques of breastfeeding will
be incorporated in the theoretical aspects of training and education. Different techniques of
breastfeeding will be demonstrated by senior and retired nurses and elder members of the
5
family. This practical training might be more beneficial for first-time mothers because these
others might not be aware of correct technique of breastfeeding. After 1 week of
implementation of the programme, evaluation will be carried out for assessing benefit of the
implemented programme. Women with below level of skills need to be provided with
training for the second time. Second time training is important for these women because these
women are with less educational status and low socioeconomic class. Both children and
mothers of both control and intervention group will be assessed for the duration of 12 months
(Hmon et al., 2016).
6
others might not be aware of correct technique of breastfeeding. After 1 week of
implementation of the programme, evaluation will be carried out for assessing benefit of the
implemented programme. Women with below level of skills need to be provided with
training for the second time. Second time training is important for these women because these
women are with less educational status and low socioeconomic class. Both children and
mothers of both control and intervention group will be assessed for the duration of 12 months
(Hmon et al., 2016).
6
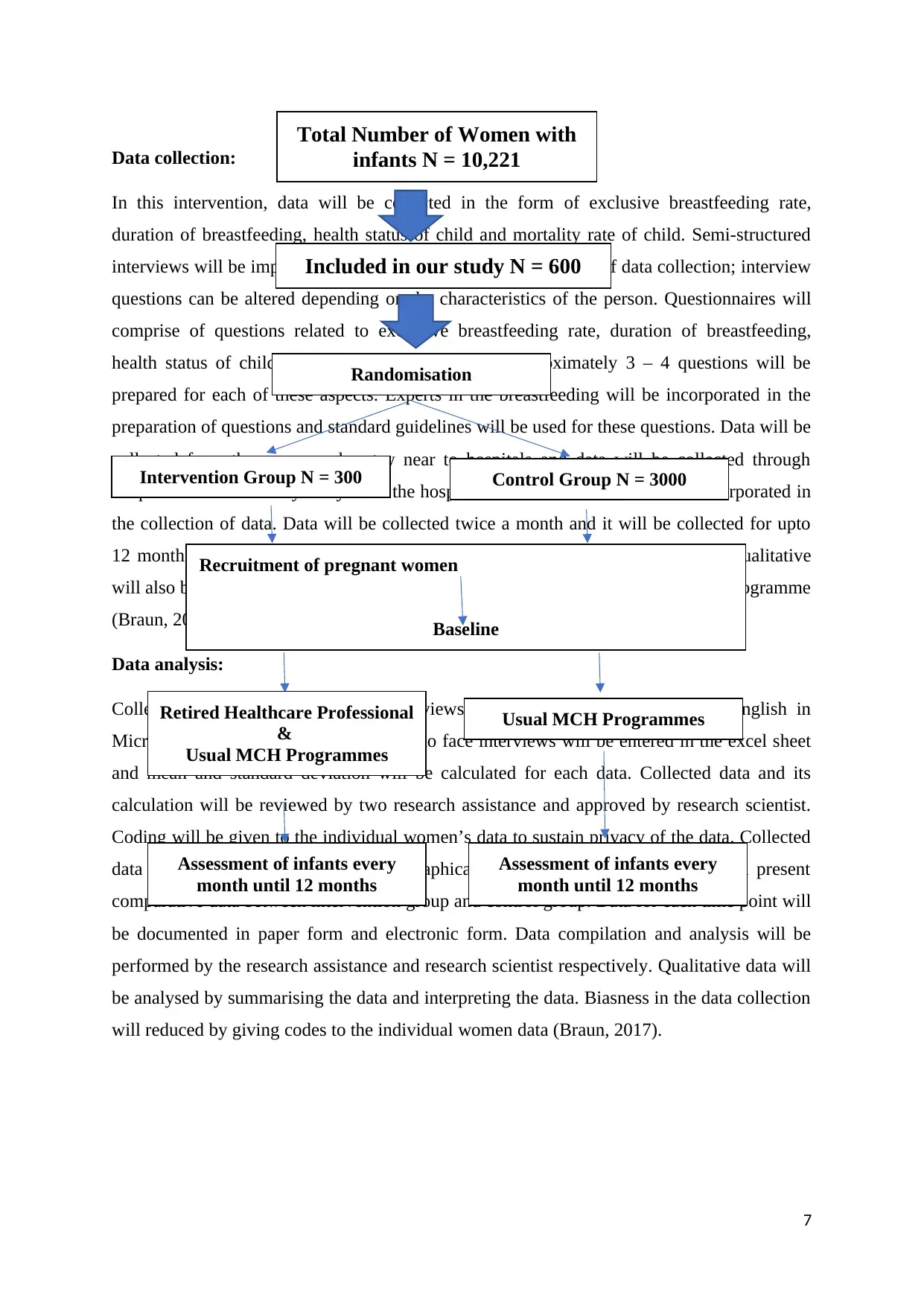
Data collection:
In this intervention, data will be collected in the form of exclusive breastfeeding rate,
duration of breastfeeding, health status of child and mortality rate of child. Semi-structured
interviews will be implemented in this study because in this type of data collection; interview
questions can be altered depending on the characteristics of the person. Questionnaires will
comprise of questions related to exclusive breastfeeding rate, duration of breastfeeding,
health status of child and mortality rate of child. Approximately 3 – 4 questions will be
prepared for each of these aspects. Experts in the breastfeeding will be incorporated in the
preparation of questions and standard guidelines will be used for these questions. Data will be
collected from the women who stay near to hospitals and data will be collected through
telephone those who stay away from the hospitals. 10 research nurses will be incorporated in
the collection of data. Data will be collected twice a month and it will be collected for upto
12 months of child age. This type is considered as quantitative data. Moreover, qualitative
will also be collected in the form of cost effectiveness of breastfeeding promotion programme
(Braun, 2017).
Data analysis:
Collected data through telephonic interviews will be transcribed verbatim in English in
Microsoft Excel. Data Collected by face-to face interviews will be entered in the excel sheet
and mean and standard deviation will be calculated for each data. Collected data and its
calculation will be reviewed by two research assistance and approved by research scientist.
Coding will be given to the individual women’s data to sustain privacy of the data. Collected
data will be presented in tabular and graphical form. These graphs and table will present
comparative data between intervention group and control group. Data for each time point will
be documented in paper form and electronic form. Data compilation and analysis will be
performed by the research assistance and research scientist respectively. Qualitative data will
be analysed by summarising the data and interpreting the data. Biasness in the data collection
will reduced by giving codes to the individual women data (Braun, 2017).
7
Total Number of Women with
infants N = 10,221
Included in our study N = 600
Randomisation
Intervention Group N = 300 Control Group N = 3000
Recruitment of pregnant women
Baseline
Retired Healthcare Professional
&
Usual MCH Programmes
Usual MCH Programmes
Assessment of infants every
month until 12 months
Assessment of infants every
month until 12 months
In this intervention, data will be collected in the form of exclusive breastfeeding rate,
duration of breastfeeding, health status of child and mortality rate of child. Semi-structured
interviews will be implemented in this study because in this type of data collection; interview
questions can be altered depending on the characteristics of the person. Questionnaires will
comprise of questions related to exclusive breastfeeding rate, duration of breastfeeding,
health status of child and mortality rate of child. Approximately 3 – 4 questions will be
prepared for each of these aspects. Experts in the breastfeeding will be incorporated in the
preparation of questions and standard guidelines will be used for these questions. Data will be
collected from the women who stay near to hospitals and data will be collected through
telephone those who stay away from the hospitals. 10 research nurses will be incorporated in
the collection of data. Data will be collected twice a month and it will be collected for upto
12 months of child age. This type is considered as quantitative data. Moreover, qualitative
will also be collected in the form of cost effectiveness of breastfeeding promotion programme
(Braun, 2017).
Data analysis:
Collected data through telephonic interviews will be transcribed verbatim in English in
Microsoft Excel. Data Collected by face-to face interviews will be entered in the excel sheet
and mean and standard deviation will be calculated for each data. Collected data and its
calculation will be reviewed by two research assistance and approved by research scientist.
Coding will be given to the individual women’s data to sustain privacy of the data. Collected
data will be presented in tabular and graphical form. These graphs and table will present
comparative data between intervention group and control group. Data for each time point will
be documented in paper form and electronic form. Data compilation and analysis will be
performed by the research assistance and research scientist respectively. Qualitative data will
be analysed by summarising the data and interpreting the data. Biasness in the data collection
will reduced by giving codes to the individual women data (Braun, 2017).
7
Total Number of Women with
infants N = 10,221
Included in our study N = 600
Randomisation
Intervention Group N = 300 Control Group N = 3000
Recruitment of pregnant women
Baseline
Retired Healthcare Professional
&
Usual MCH Programmes
Usual MCH Programmes
Assessment of infants every
month until 12 months
Assessment of infants every
month until 12 months
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Statistical analysis:
Power calculation will be performed on 300 participants each from the intervention and
control group. Mean difference values between the intervention group and control group will
be determined.
Power calculation will be performed on 300 participants each from intervention group and
control group. Difference in the mean vales between intervention group and control group
will be calculated. SPSS statistical software package version 18.0 (SPSS Inc., Chicago, IL,
USA) will be used for the statistical analysis. ‘t’ test and one-way repeated measures
ANOVA will be used for intergroup comparisons based on its suitability. Tukey test will be
used for post hoc comparisons and Pearson’s coefficients will be implemented for identifying
correlation among different variables (Petrie and Sabin, 2016).
Anticipated outcome and significance:
We anticipated that frequency of breastfeeding will become double in intervention group in
comparison to the control group. This planned intervention will offer valid evidence for role
of women’s education in lessening children and neonates mortality in Aboriginal community.
Outcome of this intervention will be beneficial in promoting child growth in Aboriginal
community. This intervention will be beneficial in finding impact of mother’s education on
breastfeeding in first four hours of child birth. We are anticipating, mothers with education
and training will increase frequency of breastfeeding in first four hours of child birth in
comparison to the mothers without education. Duration of EBF can be effectively improved
by providing education and training to the mothers. This intervention will also be helpful in
promoting Baby Friendly Hospital Initiative in primary health centre. Outcome of this study
will be compared with other studies conducted by Government and non-government
organisations. Confidence of mothers in breastfeeding can be effectively improved by
providing education and training to the mothers. It is evident that mothers undergone
caesarean deliveries with reduced frequency and duration of breastfeeding in comparison to
the normal delivery. Hence, impact of mother’s education on frequency and duration of
breastfeeding will be determined in this intervention. Guidelines for improving frequency and
duration of breastfeeding can be prepared by using outcome of this intervention. Potential
problems specific to Aboriginal people during breastfeeding can be identified through this
study. Identifying these problems can be helpful in planning effective intervention for
8
Power calculation will be performed on 300 participants each from the intervention and
control group. Mean difference values between the intervention group and control group will
be determined.
Power calculation will be performed on 300 participants each from intervention group and
control group. Difference in the mean vales between intervention group and control group
will be calculated. SPSS statistical software package version 18.0 (SPSS Inc., Chicago, IL,
USA) will be used for the statistical analysis. ‘t’ test and one-way repeated measures
ANOVA will be used for intergroup comparisons based on its suitability. Tukey test will be
used for post hoc comparisons and Pearson’s coefficients will be implemented for identifying
correlation among different variables (Petrie and Sabin, 2016).
Anticipated outcome and significance:
We anticipated that frequency of breastfeeding will become double in intervention group in
comparison to the control group. This planned intervention will offer valid evidence for role
of women’s education in lessening children and neonates mortality in Aboriginal community.
Outcome of this intervention will be beneficial in promoting child growth in Aboriginal
community. This intervention will be beneficial in finding impact of mother’s education on
breastfeeding in first four hours of child birth. We are anticipating, mothers with education
and training will increase frequency of breastfeeding in first four hours of child birth in
comparison to the mothers without education. Duration of EBF can be effectively improved
by providing education and training to the mothers. This intervention will also be helpful in
promoting Baby Friendly Hospital Initiative in primary health centre. Outcome of this study
will be compared with other studies conducted by Government and non-government
organisations. Confidence of mothers in breastfeeding can be effectively improved by
providing education and training to the mothers. It is evident that mothers undergone
caesarean deliveries with reduced frequency and duration of breastfeeding in comparison to
the normal delivery. Hence, impact of mother’s education on frequency and duration of
breastfeeding will be determined in this intervention. Guidelines for improving frequency and
duration of breastfeeding can be prepared by using outcome of this intervention. Potential
problems specific to Aboriginal people during breastfeeding can be identified through this
study. Identifying these problems can be helpful in planning effective intervention for
8
improving breastfeeding and reducing mortality rate in Aboriginal children (Wen et., 2009;
Jiang et al., 2012).
Relation between socioeconomic factor like education and breastfeeding can be identified
through this intervention. This intervention can also be helpful in identifying potential gaps in
providing healthcare services at the primary healthcare centres. Hence, these gaps can be
effectively addressed to improve healthcare services at the primary healthcare centres.
Support from family and community members is most important factor for promotion of
breastfeeding in Aboriginal population.
Mother’s education for the improvement of breastfeeding is a long duration process; hence,
beneficial results of this intervention will be helpful for improvement of health and well-
being of the entire society. Augmentation in frequency and duration of breastfeeding can be
helpful in improving overall growth and development of children (Santo et al., 2007; Jiang et
al., 2012). It can be helpful in improving health of future generations. It can result in reducing
health expenditure of Aboriginal people. It can produce positive impact on economy of
Australia for the longer duration. Health of future generations of Aboriginal people can
improve their productivity and it can result in social and economic growth and development
of Australia. This study enrolled large number of Aboriginal women; hence these results can
be extrapolated to other population also. Results of this study produced data related to women
with low socioeconomic class; hence, this data would get more significance because
breastfeeding promotion is required more in low socioeconomic class women as compared to
the high socioeconomic class women (Senarath et al., 2010).
Budget and cost-effective analysis:
Implemented IYCF intervention programme will have fixed budget. This fixed budget
comprises of administrative cost, travel cost, material cost and staffing cost. Administrative
cost comprises of institutional Review Board fees, courier expenses, phone lines, long
distance charges, and storage expenses and photocopying. Travel cost comprises of
transportation and accommodation expenses cost which is required for visits to the different
hospitals and different houses of the women. Staffing cost comprises of salaries for retired
health care professionals, research assistance, research scientist, nurses, consultants and
statistician. Materials cost comprises of cost for paper, pens, folders, binders and labels cost.
Cost effective analysis will be carried out by comparing incurred cost and outcome observed.
9
Jiang et al., 2012).
Relation between socioeconomic factor like education and breastfeeding can be identified
through this intervention. This intervention can also be helpful in identifying potential gaps in
providing healthcare services at the primary healthcare centres. Hence, these gaps can be
effectively addressed to improve healthcare services at the primary healthcare centres.
Support from family and community members is most important factor for promotion of
breastfeeding in Aboriginal population.
Mother’s education for the improvement of breastfeeding is a long duration process; hence,
beneficial results of this intervention will be helpful for improvement of health and well-
being of the entire society. Augmentation in frequency and duration of breastfeeding can be
helpful in improving overall growth and development of children (Santo et al., 2007; Jiang et
al., 2012). It can be helpful in improving health of future generations. It can result in reducing
health expenditure of Aboriginal people. It can produce positive impact on economy of
Australia for the longer duration. Health of future generations of Aboriginal people can
improve their productivity and it can result in social and economic growth and development
of Australia. This study enrolled large number of Aboriginal women; hence these results can
be extrapolated to other population also. Results of this study produced data related to women
with low socioeconomic class; hence, this data would get more significance because
breastfeeding promotion is required more in low socioeconomic class women as compared to
the high socioeconomic class women (Senarath et al., 2010).
Budget and cost-effective analysis:
Implemented IYCF intervention programme will have fixed budget. This fixed budget
comprises of administrative cost, travel cost, material cost and staffing cost. Administrative
cost comprises of institutional Review Board fees, courier expenses, phone lines, long
distance charges, and storage expenses and photocopying. Travel cost comprises of
transportation and accommodation expenses cost which is required for visits to the different
hospitals and different houses of the women. Staffing cost comprises of salaries for retired
health care professionals, research assistance, research scientist, nurses, consultants and
statistician. Materials cost comprises of cost for paper, pens, folders, binders and labels cost.
Cost effective analysis will be carried out by comparing incurred cost and outcome observed.
9
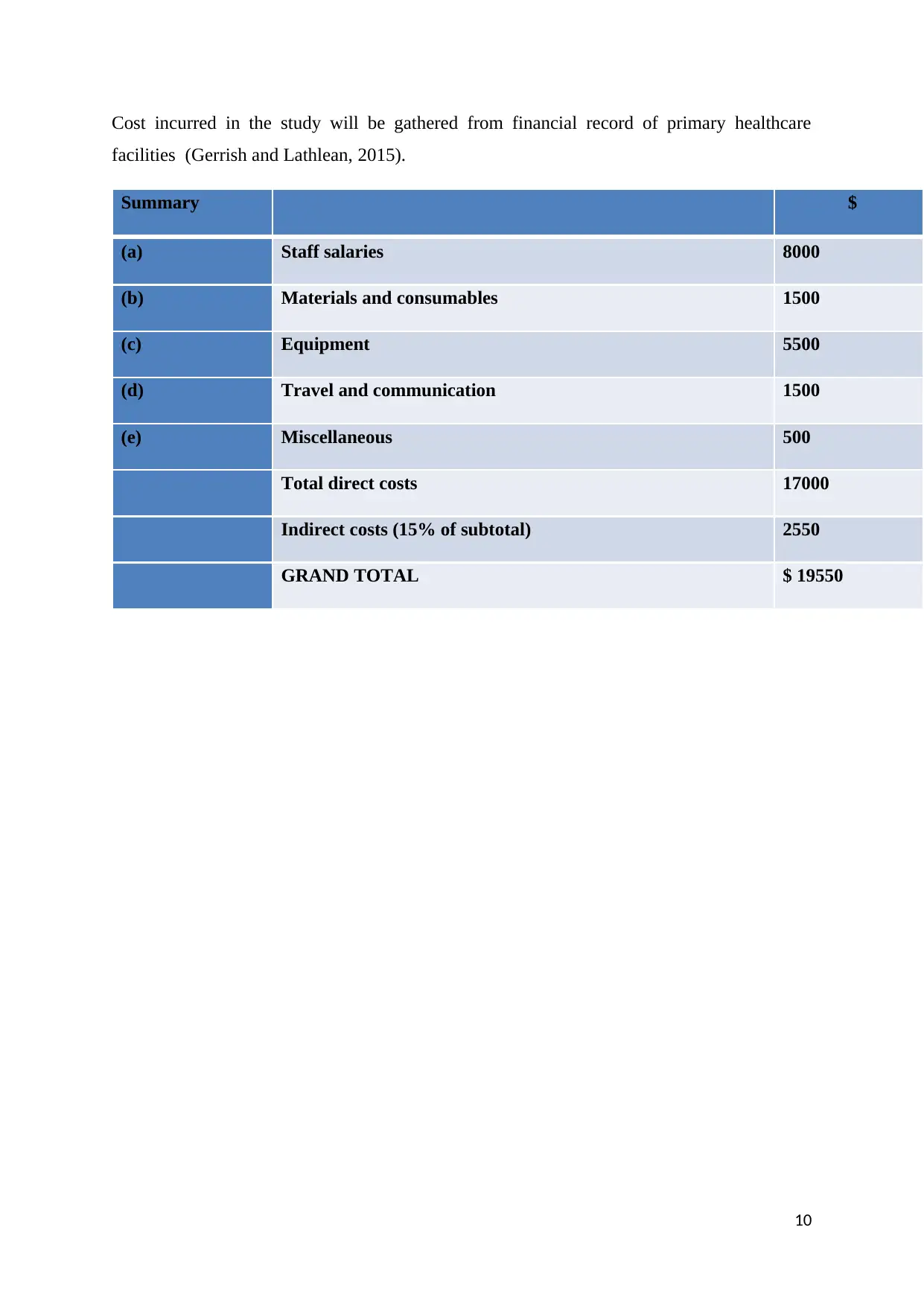
Cost incurred in the study will be gathered from financial record of primary healthcare
facilities (Gerrish and Lathlean, 2015).
Summary $
(a) Staff salaries 8000
(b) Materials and consumables 1500
(c) Equipment 5500
(d) Travel and communication 1500
(e) Miscellaneous 500
Total direct costs 17000
Indirect costs (15% of subtotal) 2550
GRAND TOTAL $ 19550
10
facilities (Gerrish and Lathlean, 2015).
Summary $
(a) Staff salaries 8000
(b) Materials and consumables 1500
(c) Equipment 5500
(d) Travel and communication 1500
(e) Miscellaneous 500
Total direct costs 17000
Indirect costs (15% of subtotal) 2550
GRAND TOTAL $ 19550
10
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
References:
Arimond, M., Daelmans, B., Dewey, K. (2008). Indicators for feeding practices in children.
Lancet, 371(9612), 541–2.
Barnes, M., and Rowe, J. (2013). Child, Youth and Family Health: Strengthening
Communities. Elsevier Health Sciences.
Braun, V. (2017). Collecting Qualitative Data: A Practical Guide to Textual, Media and
Virtual Techniques. Cambridge University Press.
Cook, J.A., Hislop, J., Altman, D.G., Fayers, P., Briggs, A.H., Ramsay, C.R., and Norrie, J.D.
(2015). Specifying the target difference in the primary outcome for a randomised
controlled trial: guidance for researchers. Trials, 16, 12. doi: 10.1186/s13063-014-
0526-8.
Daelmans, B., Dewey, K., and Arimond, M. (2009). New and updated indicators for
assessing infant and young child feeding. Food and Nutrition Bulletin, 30(2), S256.
Gerrish, K., and Lathlean, J. (2015). The Research Process in Nursing. John Wiley & Sons.
Hmone, M.P., Dibley, M.J., Li, M., and Alam, A. (2016). A formative study to inform
mHealth based randomized controlled trial intervention to promote exclusive
breastfeeding practices in Myanmar: incorporating qualitative study findings. BMC
Medical Informatics and Decision Making, 16, 60. doi: 10.1186/s12911-016-0301-8.
Jiang, H., Li, M., Yang, D., Wen, L.M., Hunter, C., He, G., and Qian, X. (2012). Awareness,
intention, and needs regarding breastfeeding: findings from first-time mothers in
Shanghai, China. Breastfeeding Medicine, 7(6), 526–34.
Khan, J., Vesel, L., Bahl, R., and Martines, J.C. (2014). Timing of breastfeeding initiation
and exclusivity of breastfeeding during the first month of life: effects on neonatal
mortality and morbidity-a systematic review and meta-analysis. Maternal and Child
Health Journal, 19, 468–79.
McLachlan, H.L., Shafiei, T., and Forster, D.A. (2017). Breastfeeding initiation for
Aboriginal and Torres Strait Islander women in Victoria: analysis of routinely
collected population-based data. Women Birth, 30(5), 361-366.
Palinkas, L. A., Sarah, M. H., Carla, A. G., Jennifer, P. W., Naihua, D., and Kimberly, H. P.
(2015). Purposeful sampling for qualitative data collection and analysis in mixed
method implementation research. Administration and Policy in Mental Health and
Mental Health, 42(5), 533–544.
Petrie, A., and Sabin, C. (2009). Medical Statistics at a Glance. John Wiley & Sons.
Santo, L.C.E., De Oliveira, L.D., and Giugliani, E.R.J. (2007). Factors Associated with Low
Incidence of Exclusive Breastfeeding forthe First 6 Months. Birth, 34(3), 212–9.
Senarath, U., Dibley, M.J., and Agho, K.E. (2010). Factors associated with nonexclusive
breastfeeding in five East and Southeast Asian countries: a multilevel analysis.
Journal of Human Lactation, 26(3), 248–57.
Wen, L.M., Baur, L.A., Rissel, C., Alperstein, G., and Simpson, J.M. (2009). Intention to
breastfeed and awareness of health recommendations: findings from firsttime mothers
in southwest Sydney, Australia. International Breastfeeding Journal, 4(1), 9–9.
11
Arimond, M., Daelmans, B., Dewey, K. (2008). Indicators for feeding practices in children.
Lancet, 371(9612), 541–2.
Barnes, M., and Rowe, J. (2013). Child, Youth and Family Health: Strengthening
Communities. Elsevier Health Sciences.
Braun, V. (2017). Collecting Qualitative Data: A Practical Guide to Textual, Media and
Virtual Techniques. Cambridge University Press.
Cook, J.A., Hislop, J., Altman, D.G., Fayers, P., Briggs, A.H., Ramsay, C.R., and Norrie, J.D.
(2015). Specifying the target difference in the primary outcome for a randomised
controlled trial: guidance for researchers. Trials, 16, 12. doi: 10.1186/s13063-014-
0526-8.
Daelmans, B., Dewey, K., and Arimond, M. (2009). New and updated indicators for
assessing infant and young child feeding. Food and Nutrition Bulletin, 30(2), S256.
Gerrish, K., and Lathlean, J. (2015). The Research Process in Nursing. John Wiley & Sons.
Hmone, M.P., Dibley, M.J., Li, M., and Alam, A. (2016). A formative study to inform
mHealth based randomized controlled trial intervention to promote exclusive
breastfeeding practices in Myanmar: incorporating qualitative study findings. BMC
Medical Informatics and Decision Making, 16, 60. doi: 10.1186/s12911-016-0301-8.
Jiang, H., Li, M., Yang, D., Wen, L.M., Hunter, C., He, G., and Qian, X. (2012). Awareness,
intention, and needs regarding breastfeeding: findings from first-time mothers in
Shanghai, China. Breastfeeding Medicine, 7(6), 526–34.
Khan, J., Vesel, L., Bahl, R., and Martines, J.C. (2014). Timing of breastfeeding initiation
and exclusivity of breastfeeding during the first month of life: effects on neonatal
mortality and morbidity-a systematic review and meta-analysis. Maternal and Child
Health Journal, 19, 468–79.
McLachlan, H.L., Shafiei, T., and Forster, D.A. (2017). Breastfeeding initiation for
Aboriginal and Torres Strait Islander women in Victoria: analysis of routinely
collected population-based data. Women Birth, 30(5), 361-366.
Palinkas, L. A., Sarah, M. H., Carla, A. G., Jennifer, P. W., Naihua, D., and Kimberly, H. P.
(2015). Purposeful sampling for qualitative data collection and analysis in mixed
method implementation research. Administration and Policy in Mental Health and
Mental Health, 42(5), 533–544.
Petrie, A., and Sabin, C. (2009). Medical Statistics at a Glance. John Wiley & Sons.
Santo, L.C.E., De Oliveira, L.D., and Giugliani, E.R.J. (2007). Factors Associated with Low
Incidence of Exclusive Breastfeeding forthe First 6 Months. Birth, 34(3), 212–9.
Senarath, U., Dibley, M.J., and Agho, K.E. (2010). Factors associated with nonexclusive
breastfeeding in five East and Southeast Asian countries: a multilevel analysis.
Journal of Human Lactation, 26(3), 248–57.
Wen, L.M., Baur, L.A., Rissel, C., Alperstein, G., and Simpson, J.M. (2009). Intention to
breastfeed and awareness of health recommendations: findings from firsttime mothers
in southwest Sydney, Australia. International Breastfeeding Journal, 4(1), 9–9.
11
1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.