A reflective framework to foster emotionally intelligent leadership in nursing
VerifiedAdded on 2022/10/14
|10
|8666
|56
AI Summary
This article proposes a reflective framework based on emotional intelligence in nurse leadership literature. It aims to support the development of nurse leadership in a practical context by integrating emotional intelligence into a reflective framework. The article explores the meaning of emotional intelligence in nursing and contextualizes the findings into a reflective framework. The proposed framework may supplement learning about emotional intelligence skills and aid the integration of emotional intelligence in a clinical environment.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
A reflective framework to foster emotionally intelligent leadership
in nursing
BIRGIT HECKEMANN M S c , R N 1, JOS M.G.A SCHOLS P h D , M D 2 and RUUD J.G. HALFENS P h D , F E A N S
3
1PhD Student, CAPHRI – School for Public Health and Primary Care,2Professor of Old Age Medicine, Faculty of
Health, Medicine and Life Sciences, Department of Family Medicine and Department of Health Services Resear
CAPHRI- School for Public Health and Primary Care and3Associate Professor, Faculty of Health, Medicine and
Life Sciences, Department of Health Care and Nursing Science, CAPHRI – School for Public Health and Primary
Care, Maastricht University, Maastricht, The Netherlands
Correspondence
Birgit Heckemann
CAPHRI
University of Maastricht
PO Box 616 MD
6200 Maastricht
the Netherlands
E-mail: b.heckemann
@maastrichtuniversity.nl
HECKEMANN B., SCHOLS J.M.G.A. & HALFENS R.J.G. (2015) Journal of Nursing
Management 23, 744–753.
A reflective framework to foster emotionally intelligent leadership in
nursing
Aim To propose a reflective framework based on the perspective of emotional
intelligence (EI) in nurse leadership literature.
Background Emotional intelligence is a self-development construct aimed at
enhancing the management of feelings and interpersonal relationships, which has
become increasingly popular in nurse leadership. Reflection is an established
means to foster learning. Integrating those aspects of emotional intelligence
pertinent to nurse leadership into a reflective framework might support the
development of nurse leadership in a practical context.
Method A sample of 22 articles, retrieved via electronic databases (Ovid/Medline,
BNI, psycArticles, Zetoc and CINAHL) and published between January 1996 and
April 2009, was analysed in a qualitative descriptive content analysis.
Result Three dimensions that characterise emotional intelligence leadership in th
context of nursing – the nurse leader as a ‘socio-cultural architect’, as a
‘responsive carer’ and as a ‘strategic visionary’ – emerged from the analysis. To
enable practical application, these dimensions were contextualised into a reflectiv
framework.
Conclusion Emotional intelligence skills are regarded as essential for establishing
empowering work environments in nursing. A reflective framework might aid the
translation of emotional intelligence into a real-world context.
Implications for nursing practice The proposed framework may supplement
learning about emotional intelligence skills and aid the integration of emotional
intelligence in a clinical environment.
Keywords:emotional intelligence, reflective framework, reflective practice, resonant
leadership
Accepted for publication: 11 November 2013
Background
Emotional intelligence (EI), a self-development concept
that promises to enhance the managementof feelings
and interpersonalrelationships,has been proposed to
augmentnurse leadershipskills (Cummingset al.
2005, Lucas et al. 2008, Feather2009).Yet little is
known about the attributes that define EI in a nursing
leadership contextand how bestto advance these in
individuals.Reflection haspreviously been suggested
744
DOI: 10.1111/jonm.12204
ª 2014 John Wiley & Sons Ltd
Journal of Nursing Management, 2015, 23, 744–753
in nursing
BIRGIT HECKEMANN M S c , R N 1, JOS M.G.A SCHOLS P h D , M D 2 and RUUD J.G. HALFENS P h D , F E A N S
3
1PhD Student, CAPHRI – School for Public Health and Primary Care,2Professor of Old Age Medicine, Faculty of
Health, Medicine and Life Sciences, Department of Family Medicine and Department of Health Services Resear
CAPHRI- School for Public Health and Primary Care and3Associate Professor, Faculty of Health, Medicine and
Life Sciences, Department of Health Care and Nursing Science, CAPHRI – School for Public Health and Primary
Care, Maastricht University, Maastricht, The Netherlands
Correspondence
Birgit Heckemann
CAPHRI
University of Maastricht
PO Box 616 MD
6200 Maastricht
the Netherlands
E-mail: b.heckemann
@maastrichtuniversity.nl
HECKEMANN B., SCHOLS J.M.G.A. & HALFENS R.J.G. (2015) Journal of Nursing
Management 23, 744–753.
A reflective framework to foster emotionally intelligent leadership in
nursing
Aim To propose a reflective framework based on the perspective of emotional
intelligence (EI) in nurse leadership literature.
Background Emotional intelligence is a self-development construct aimed at
enhancing the management of feelings and interpersonal relationships, which has
become increasingly popular in nurse leadership. Reflection is an established
means to foster learning. Integrating those aspects of emotional intelligence
pertinent to nurse leadership into a reflective framework might support the
development of nurse leadership in a practical context.
Method A sample of 22 articles, retrieved via electronic databases (Ovid/Medline,
BNI, psycArticles, Zetoc and CINAHL) and published between January 1996 and
April 2009, was analysed in a qualitative descriptive content analysis.
Result Three dimensions that characterise emotional intelligence leadership in th
context of nursing – the nurse leader as a ‘socio-cultural architect’, as a
‘responsive carer’ and as a ‘strategic visionary’ – emerged from the analysis. To
enable practical application, these dimensions were contextualised into a reflectiv
framework.
Conclusion Emotional intelligence skills are regarded as essential for establishing
empowering work environments in nursing. A reflective framework might aid the
translation of emotional intelligence into a real-world context.
Implications for nursing practice The proposed framework may supplement
learning about emotional intelligence skills and aid the integration of emotional
intelligence in a clinical environment.
Keywords:emotional intelligence, reflective framework, reflective practice, resonant
leadership
Accepted for publication: 11 November 2013
Background
Emotional intelligence (EI), a self-development concept
that promises to enhance the managementof feelings
and interpersonalrelationships,has been proposed to
augmentnurse leadershipskills (Cummingset al.
2005, Lucas et al. 2008, Feather2009).Yet little is
known about the attributes that define EI in a nursing
leadership contextand how bestto advance these in
individuals.Reflection haspreviously been suggested
744
DOI: 10.1111/jonm.12204
ª 2014 John Wiley & Sons Ltd
Journal of Nursing Management, 2015, 23, 744–753
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
as a means to foster emotionally competent nurse lead-
ership (Horton-Deutsch & Sherwood 2008),however,
tools that facilitate EI-focused reflection are lacking.
This study aims to close this gap by proposing a reflec-
tive framework that integrates the attributes pertaining
to EI in nursing leadership.
Emotional intelligence
Emotionalintelligence isa conceptthat has evolved
continually since it was first introduced into academia
by research psychologistsSalovey and Mayerin the
early 1990s. They defined EI as:
‘the ability to perceive emotions,to access and
generateemotionsso as to assist thought,to
understand emotionsand emotionalknowledge
and to reflectively regulateemotionsso as to
promote emotional and intellectual growth’.
(Mayer & Salovey 1997 p. 5)
In 1996, EI was widely popularised outside
academiccirclesby Daniel Goleman with his book
Emotional Intelligence:Why It Can Matter More
Than IQ (Goleman 1996,Bulmer-Smith et al.2009).
EI has since become a popular developmenttool and
has also found its way into health care (Freshman &
Rubino 2002).
Two major EI models,the ‘ability model’and the
‘mixed models’,have been proposed.These differin
scope,application and assessmentmethods(Schulte
et al. 2004).
Within the ability model, also called the ‘four-
branch model’,EI is described as a set of four distinct
skills and the extentto which these abilities are inte-
grated into an individual’s personality.The four abili-
ties are:‘(1) to perceive emotion,(2) to use emotion
to facilitate thought,(3) to understand emotions,and
(4) to manage emotion’(Mayer et al. 2004 p. 199).
According to this model, EI abilitiesrangefrom a
basic level (recognition of emotions) to a more sophis-
ticated level(managementof emotions)(Mayer &
Salovey 1997).
Within the ‘mixed models’,the conceptof EI is
broadened.In addition to the ability to manage emo-
tions, mixed models include a number ofpersonality
characteristics or traits such as empathy,persistence,
socialskills and motivation among others,which do
not feature in Mayer and Salovey’s definition (Schulte
et al. 2004).The mostpopular modelamongstthese
is arguably the Goleman modelof EI, which incorpo-
rates traits such as socialawareness and relationship
management (Goleman 1996).
In the past,the conceptof EI has been subjectto
substantialcriticism, mainly on the grounds that
claims of EI’s beneficialimpact on work performance
and career progression were exaggerated and insuffi-
ciently substantiated (Bulmer-Smith et al. 2009).
However, current evidence suggests that EI is in fact
positively associated with job performance and well-
being (O’Boyle Jr et al.2011).The proposed value of
EI is also increasingly being corroborated by neurosci-
entific evidence.The results of a recent study point to
a link between the self-rating of EI and the ability to
recogniseand processsocial information (Kreifelts
et al. 2010).
Emotional intelligence and nurse leadership
Emotionalintelligence with its emphasis on empower-
ment through the management of emotion appears to
be a complementary toolto support the current inter-
nationaldrive towards fostering strong nurse leader-
ship in health care (ICN 2010). Skills such as
self-awareness,the capacity to establish purpose and
direction, and motivatingand inspiring teams are
regarded asessentialassetsfor achieving substantial
improvements in clinical practice (Warriner 2009) and
as a prerequisite for the creation of empowering work
environments (Davies et al.2011).Yet little is known
aboutwhich particular attributes define EIleadership
in a nursing context (Akerjordet & Severinsson 2010).
In recent years,EI has been linked to a particular
leadership style,resonant leadership.The hallmark of
resonantleadersis the ability to work in tune with
their staffand colleagues.Resonantleaders use their
EI skills to managetheir own emotionsas well as
those ofthe people who work alongside them.They
create positive work environmentsand are aware of
organisationalneeds.They understand and success-
fully manage factors contributing to positive organisa-
tional outcomes.They are,in short, effective leaders
(Boyatzis & McKee 2005).
Resonantleadership hasalso reverberated in the
nursing literature. Current research concludes that res-
onant leadership in nursing notonly contributesto
ameliorating patientsafety and outcomes,but also
facilitates the creation of healthy work environments.
These enhance job satisfaction and the well-being of
nursesand thus contribute to recruitmentand staff
retention (Cummings et al.2010,Squires et al.2010).
There is to date a shortage ofcapable leaders within
nursing,not leastbecause leading in nursing is chal-
lenging (Hendricks et al.2010,Enterkin et al.2013).
Nurse leaders are expectedto build and sustain
ª 2014 John Wiley & Sons Ltd
Journal of Nursing Management, 2015, 23, 744–753 745
Leading with emotionalintelligence
ership (Horton-Deutsch & Sherwood 2008),however,
tools that facilitate EI-focused reflection are lacking.
This study aims to close this gap by proposing a reflec-
tive framework that integrates the attributes pertaining
to EI in nursing leadership.
Emotional intelligence
Emotionalintelligence isa conceptthat has evolved
continually since it was first introduced into academia
by research psychologistsSalovey and Mayerin the
early 1990s. They defined EI as:
‘the ability to perceive emotions,to access and
generateemotionsso as to assist thought,to
understand emotionsand emotionalknowledge
and to reflectively regulateemotionsso as to
promote emotional and intellectual growth’.
(Mayer & Salovey 1997 p. 5)
In 1996, EI was widely popularised outside
academiccirclesby Daniel Goleman with his book
Emotional Intelligence:Why It Can Matter More
Than IQ (Goleman 1996,Bulmer-Smith et al.2009).
EI has since become a popular developmenttool and
has also found its way into health care (Freshman &
Rubino 2002).
Two major EI models,the ‘ability model’and the
‘mixed models’,have been proposed.These differin
scope,application and assessmentmethods(Schulte
et al. 2004).
Within the ability model, also called the ‘four-
branch model’,EI is described as a set of four distinct
skills and the extentto which these abilities are inte-
grated into an individual’s personality.The four abili-
ties are:‘(1) to perceive emotion,(2) to use emotion
to facilitate thought,(3) to understand emotions,and
(4) to manage emotion’(Mayer et al. 2004 p. 199).
According to this model, EI abilitiesrangefrom a
basic level (recognition of emotions) to a more sophis-
ticated level(managementof emotions)(Mayer &
Salovey 1997).
Within the ‘mixed models’,the conceptof EI is
broadened.In addition to the ability to manage emo-
tions, mixed models include a number ofpersonality
characteristics or traits such as empathy,persistence,
socialskills and motivation among others,which do
not feature in Mayer and Salovey’s definition (Schulte
et al. 2004).The mostpopular modelamongstthese
is arguably the Goleman modelof EI, which incorpo-
rates traits such as socialawareness and relationship
management (Goleman 1996).
In the past,the conceptof EI has been subjectto
substantialcriticism, mainly on the grounds that
claims of EI’s beneficialimpact on work performance
and career progression were exaggerated and insuffi-
ciently substantiated (Bulmer-Smith et al. 2009).
However, current evidence suggests that EI is in fact
positively associated with job performance and well-
being (O’Boyle Jr et al.2011).The proposed value of
EI is also increasingly being corroborated by neurosci-
entific evidence.The results of a recent study point to
a link between the self-rating of EI and the ability to
recogniseand processsocial information (Kreifelts
et al. 2010).
Emotional intelligence and nurse leadership
Emotionalintelligence with its emphasis on empower-
ment through the management of emotion appears to
be a complementary toolto support the current inter-
nationaldrive towards fostering strong nurse leader-
ship in health care (ICN 2010). Skills such as
self-awareness,the capacity to establish purpose and
direction, and motivatingand inspiring teams are
regarded asessentialassetsfor achieving substantial
improvements in clinical practice (Warriner 2009) and
as a prerequisite for the creation of empowering work
environments (Davies et al.2011).Yet little is known
aboutwhich particular attributes define EIleadership
in a nursing context (Akerjordet & Severinsson 2010).
In recent years,EI has been linked to a particular
leadership style,resonant leadership.The hallmark of
resonantleadersis the ability to work in tune with
their staffand colleagues.Resonantleaders use their
EI skills to managetheir own emotionsas well as
those ofthe people who work alongside them.They
create positive work environmentsand are aware of
organisationalneeds.They understand and success-
fully manage factors contributing to positive organisa-
tional outcomes.They are,in short, effective leaders
(Boyatzis & McKee 2005).
Resonantleadership hasalso reverberated in the
nursing literature. Current research concludes that res-
onant leadership in nursing notonly contributesto
ameliorating patientsafety and outcomes,but also
facilitates the creation of healthy work environments.
These enhance job satisfaction and the well-being of
nursesand thus contribute to recruitmentand staff
retention (Cummings et al.2010,Squires et al.2010).
There is to date a shortage ofcapable leaders within
nursing,not leastbecause leading in nursing is chal-
lenging (Hendricks et al.2010,Enterkin et al.2013).
Nurse leaders are expectedto build and sustain
ª 2014 John Wiley & Sons Ltd
Journal of Nursing Management, 2015, 23, 744–753 745
Leading with emotionalintelligence
productiveteams. However, due to organisational
changesin health care, nurse leaders’roles have
becomeincreasinglymanagerialand removed from
front-line nursing.This may create a climate ofdis-
trust between nursing staff and nurse leaders (Udod &
Care 2013). Leading with emotionalintelligenceis
regarded as a means to bridge this gap.
Reflection, emotional intelligence and nurse
leadership
Reflection hasbeen proposed to fosteremotionally
competent or resonant leadership (Horton-Deutsch &
Sherwood 2008). While its use as a means to promote
learning or empowerment is controversial(Fook et al.
2006), reflection has become an integral component of
nurse training and advanced professionaldevelopment
(Mantzoukas & Jasper 2004).
Depending on the experience and need of the practi-
tioner,reflection may vary in depth (Rolfe et al.2001
p. 24). Goodman (1984,cited by Jasper2003 p. 7)
identified three levelsof reflection.Reflection atthe
first levelis mainly descriptive.Second levelreflection
connectsprinciplesand practice,i.e. the practitioner
assesses the implications and consequences ofactions
and beliefs,as well as the underlying rationalefor
practice.At the third and deepestlevelof reflection,
the practitioner is able to explore a complex situation
in depth by drawing on varioustheoretical,ethical,
political,personal,and professionalperspectives (Jas-
per 2003). Horton-Deutsch and Sherwood (2008) con-
cisely describe the particular value of profound,third
level reflection:
‘Reflection is like the academicprocess of
describing,analysing,synthesising and evaluat-
ing with the addition ofself-awareness.Reflec-
tion includes the emotions and feelings thatare
an integral part of practice but are often
ignored’.
(Horton-Deutsch & Sherwood 2008 p. 949).
Third-level reflection can therefore help nurse
leaders to systematically examine experiences and situ-
ations from various angles to increase selfawareness
and to promote learning from experience(Horton-
Deutsch & Sherwood 2008). A framework that
enablesthird-levelreflection hasbeen described by
Rolfe et al. (2001 p. 34–36).Their framework takes
the practitionerthrough a three-step cyclicalprocess
of analysis:from a descriptivestageover a theory
building stage to an action oriented stage (Rolfe et al.
2001 p. 34–36).
The study
Aim
The aim of this study was twofold.First, to explore
the meaning ofEI as pertaining to nurse leadership,
and second,to enable the practicalapplication of the
findings by contextualisingthem into a reflective
framework.
Design
To explore the meaning of EI in nursing,a qualitative
descriptivestudy of literaturepertaining to EI and
nurse leadership was conducted. The analysis followed
Krippendorff’s (2004 p.86) modelof content analysis
and was conducted from an epistemologicalstance of
moderate constructivism (Hoijer 2008).
Sample
Publications were selected according to the following
criteria.
Inclusion criteria:Articles,originalresearch papers,
editorials or literature review studies,written in Eng-
lish, published between January 1996 and April2009
and exploring explicitly and exclusively ‘EI’ in relation
to nurse leadership were included into the study.
Exclusion criteria:Articles addressing similarcon-
structs such as ‘social-emotional competence’, ‘psycho-
socialfunctioning’or ‘emotionallanguage skills’etc.
were excluded,because one ofthe aims ofthis study
was to define the construct called ‘EI’.
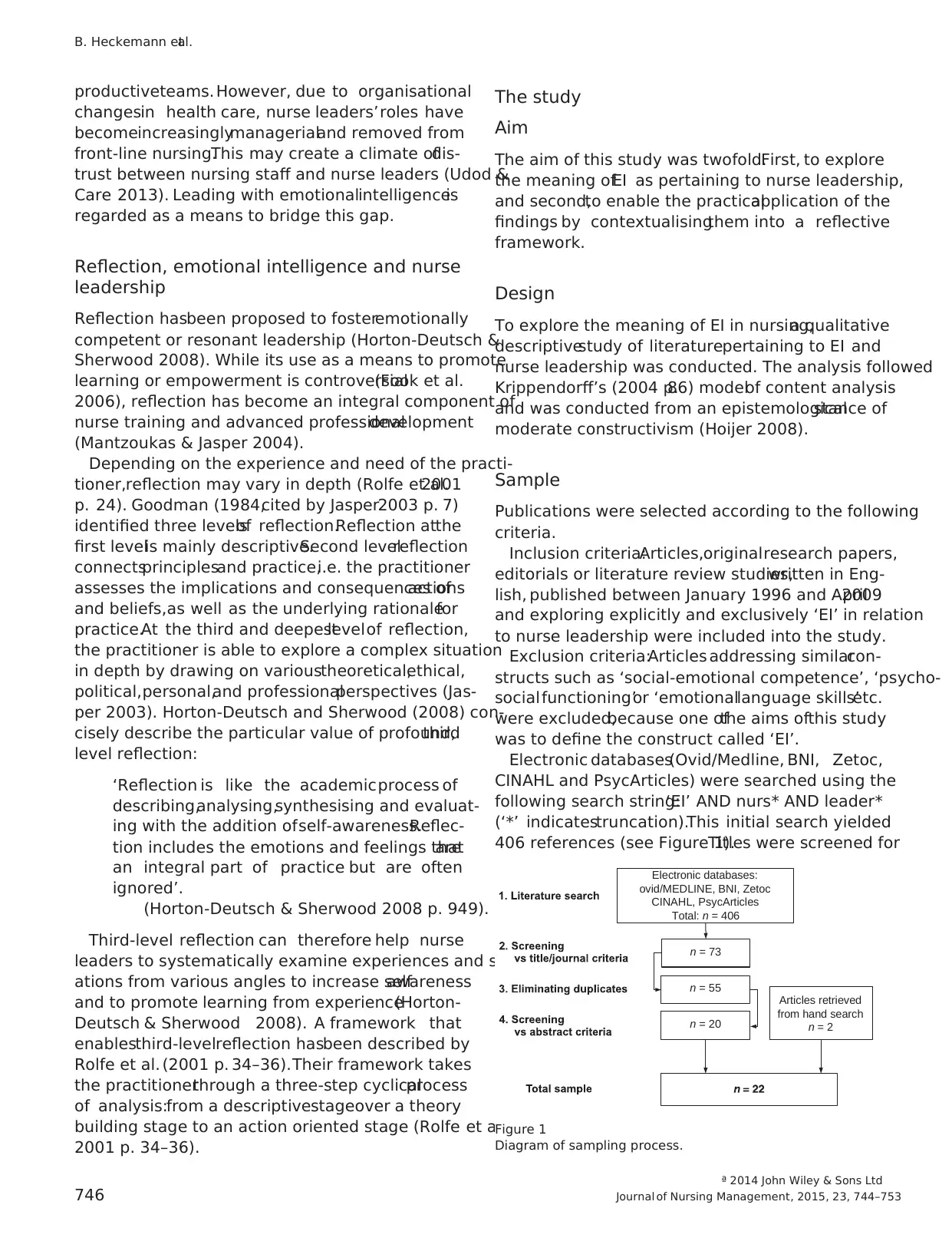
Electronic databases(Ovid/Medline, BNI, Zetoc,
CINAHL and PsycArticles) were searched using the
following search string:‘EI’ AND nurs* AND leader*
(‘*’ indicatestruncation).This initial search yielded
406 references (see Figure 1).Titles were screened for
Electronic databases:
ovid/MEDLINE, BNI, Zetoc
CINAHL, PsycArticles
Total: n = 406
Articles retrieved
from hand search
n = 2
n = 73
n = 55
n = 20
Figure 1
Diagram of sampling process.
ª 2014 John Wiley & Sons Ltd
746 Journal of Nursing Management, 2015, 23, 744–753
B. Heckemann etal.
changesin health care, nurse leaders’roles have
becomeincreasinglymanagerialand removed from
front-line nursing.This may create a climate ofdis-
trust between nursing staff and nurse leaders (Udod &
Care 2013). Leading with emotionalintelligenceis
regarded as a means to bridge this gap.
Reflection, emotional intelligence and nurse
leadership
Reflection hasbeen proposed to fosteremotionally
competent or resonant leadership (Horton-Deutsch &
Sherwood 2008). While its use as a means to promote
learning or empowerment is controversial(Fook et al.
2006), reflection has become an integral component of
nurse training and advanced professionaldevelopment
(Mantzoukas & Jasper 2004).
Depending on the experience and need of the practi-
tioner,reflection may vary in depth (Rolfe et al.2001
p. 24). Goodman (1984,cited by Jasper2003 p. 7)
identified three levelsof reflection.Reflection atthe
first levelis mainly descriptive.Second levelreflection
connectsprinciplesand practice,i.e. the practitioner
assesses the implications and consequences ofactions
and beliefs,as well as the underlying rationalefor
practice.At the third and deepestlevelof reflection,
the practitioner is able to explore a complex situation
in depth by drawing on varioustheoretical,ethical,
political,personal,and professionalperspectives (Jas-
per 2003). Horton-Deutsch and Sherwood (2008) con-
cisely describe the particular value of profound,third
level reflection:
‘Reflection is like the academicprocess of
describing,analysing,synthesising and evaluat-
ing with the addition ofself-awareness.Reflec-
tion includes the emotions and feelings thatare
an integral part of practice but are often
ignored’.
(Horton-Deutsch & Sherwood 2008 p. 949).
Third-level reflection can therefore help nurse
leaders to systematically examine experiences and situ-
ations from various angles to increase selfawareness
and to promote learning from experience(Horton-
Deutsch & Sherwood 2008). A framework that
enablesthird-levelreflection hasbeen described by
Rolfe et al. (2001 p. 34–36).Their framework takes
the practitionerthrough a three-step cyclicalprocess
of analysis:from a descriptivestageover a theory
building stage to an action oriented stage (Rolfe et al.
2001 p. 34–36).
The study
Aim
The aim of this study was twofold.First, to explore
the meaning ofEI as pertaining to nurse leadership,
and second,to enable the practicalapplication of the
findings by contextualisingthem into a reflective
framework.
Design
To explore the meaning of EI in nursing,a qualitative
descriptivestudy of literaturepertaining to EI and
nurse leadership was conducted. The analysis followed
Krippendorff’s (2004 p.86) modelof content analysis
and was conducted from an epistemologicalstance of
moderate constructivism (Hoijer 2008).
Sample
Publications were selected according to the following
criteria.
Inclusion criteria:Articles,originalresearch papers,
editorials or literature review studies,written in Eng-
lish, published between January 1996 and April2009
and exploring explicitly and exclusively ‘EI’ in relation
to nurse leadership were included into the study.
Exclusion criteria:Articles addressing similarcon-
structs such as ‘social-emotional competence’, ‘psycho-
socialfunctioning’or ‘emotionallanguage skills’etc.
were excluded,because one ofthe aims ofthis study
was to define the construct called ‘EI’.
Electronic databases(Ovid/Medline, BNI, Zetoc,
CINAHL and PsycArticles) were searched using the
following search string:‘EI’ AND nurs* AND leader*
(‘*’ indicatestruncation).This initial search yielded
406 references (see Figure 1).Titles were screened for
Electronic databases:
ovid/MEDLINE, BNI, Zetoc
CINAHL, PsycArticles
Total: n = 406
Articles retrieved
from hand search
n = 2
n = 73
n = 55
n = 20
Figure 1
Diagram of sampling process.
ª 2014 John Wiley & Sons Ltd
746 Journal of Nursing Management, 2015, 23, 744–753
B. Heckemann etal.
relevance to the study and the numberof references
thus reduced to 73.After removalof duplicates,55
referencesremained.Abstractswere screened against
the inclusion criteria and 20 referencesretained.An
additionaltwo referenceswere obtained through a
search ofreferences in sample articles.All 22 articles
were studied in depth for relevance to the study.The
final sample consisted of 22 articles and met the crite-
ria of a census in that it included allthe articles that
were relevantto the area of investigation (Krippen-
dorff 2004).
Data collection and analysis
The process of content analysis has been likened to a
dance,as it is neverlinear,but recursive and rather
like a ‘journey with the data’ (Miller & Crabtree
1999b p.127–143).Yet for the purposes of clarity,it
is presented here in a linearfashion.Krippendorff’s
modelof content analysis (2004 p.83–86) guided this
research. It comprises the following components:
• Unitising: ‘Units’ are the segmentsof text to be
analysed.The base unitin this study was the sen-
tence.If a number ofsentences in a sequence per-
tained to particular ideas or thoughts logically,they
were coded as a single unit to preserve the original
meaning. Each article was analysed in its entirety.
• Sampling:The sample consisted of22 articles and
met the criteria of a census.
• Recording/coding: The sample texts were first coded
using pre-defined codecategories(templatestyle),
and,in a second round,to corroborate the findings,
in an editing style,which enabled deep engagement
with the texts (Miller & Crabtree 1999a). Data
were recorded using RQDA (R package for Qualita-
tive Data Analysis),an open-source software tool
that is easily availableover the internet(Huang
2009).
• Reducing the data:To extract major themes,data
were summarised and reduced during two rounds of
coding.
• Abductive inference:Abductive inference is the pro-
cess of bridging the gap between description of data
and the conclusionsdrawn from data.The under-
pinning idea is that the data themselvesprovide
proof for the conclusionsthat have been derived
from the same (Krippendorff2004).However,the
conclusions drawn need to be backed up or ‘war-
ranted’by a theoreticalconstructthat acts like a
hypothesisand explains the texts’ intendeduse
(Krippendorff2004). In content analysis,research
questions serve this purpose.According to Krippen-
dorff (2004 p. 31–32), research questionsbear a
similarity to hypotheses in observationalresearch in
so far as they focusthe research by delineating a
numberof possibleand, at the outset,uncertain
answers.In this study,the analyticalconstruct was
based on the following research questions:Which
common theoreticalconcepts ofEI are used in the
nursing literature? How are concepts and their defi-
nitions critiqued and justified?What is the value
ascribed to EI in generaland for leadership in nurs-
ing?
The initial analyticalconstructproved to be too
restrictive to extract relevant data to contextualise and
corroborate the findings,therefore itwas, during the
iterative process of analysis, continuouslyrevised
(Krippendorff 2004).
• Narrating:‘Narrating’concerns presentation ofthe
results in a comprehensible fashion.(Please refer to
respective section – results – of this publication.)
Results
The findingsare presented asa corroboration and
contextualisation ofmajor themes thatemerged as a
result of both coding phases.
Description of the sample characteristics
From the stated authors’aims,three different types of
publications were distinguishable:
Advocacy and opinion articles (n = 16; Kerfoot
1996, Tahan 2000, Snow 2001, Amendolair2003,
Porter-O’Grady 2003, Prosser 2003, Vitello-Cicciu
2003, Daniel 2004, Fuimano 2004, Baggett & Baggett
2005, Borbasi& Jackson 2005, Piper 2005,Stichler
2006, Triola 2007, Eason 2009, Wright 2009),
research reports (n = 2;Cummings et al.2005,Lucas
et al. 2008), and literaturereviews(n = 4; Vitello-
Cicciu 2002, Herbert & Edgar 2004, Akerjordet&
Severinsson 2008, Feather 2009).
The most frequently employed theoretical model was
the Goleman model. All of the 16 ‘advocacy and opin-
ion articles’referred to this model,which was chosen
either explicitly (10/16) or implicitly (6/16) by present-
ing a modelof EI featuring characteristics that corre-
sponded with those proposed by Goleman (1996).
Both research reportswere based on Goleman’s
assessmenttools (Cummings et al.2005, Lucas et al.
2008).Lucas et al.(2008) described and critiqued the
ª 2014 John Wiley & Sons Ltd
Journal of Nursing Management, 2015, 23, 744–753 747
Leading with emotionalintelligence
thus reduced to 73.After removalof duplicates,55
referencesremained.Abstractswere screened against
the inclusion criteria and 20 referencesretained.An
additionaltwo referenceswere obtained through a
search ofreferences in sample articles.All 22 articles
were studied in depth for relevance to the study.The
final sample consisted of 22 articles and met the crite-
ria of a census in that it included allthe articles that
were relevantto the area of investigation (Krippen-
dorff 2004).
Data collection and analysis
The process of content analysis has been likened to a
dance,as it is neverlinear,but recursive and rather
like a ‘journey with the data’ (Miller & Crabtree
1999b p.127–143).Yet for the purposes of clarity,it
is presented here in a linearfashion.Krippendorff’s
modelof content analysis (2004 p.83–86) guided this
research. It comprises the following components:
• Unitising: ‘Units’ are the segmentsof text to be
analysed.The base unitin this study was the sen-
tence.If a number ofsentences in a sequence per-
tained to particular ideas or thoughts logically,they
were coded as a single unit to preserve the original
meaning. Each article was analysed in its entirety.
• Sampling:The sample consisted of22 articles and
met the criteria of a census.
• Recording/coding: The sample texts were first coded
using pre-defined codecategories(templatestyle),
and,in a second round,to corroborate the findings,
in an editing style,which enabled deep engagement
with the texts (Miller & Crabtree 1999a). Data
were recorded using RQDA (R package for Qualita-
tive Data Analysis),an open-source software tool
that is easily availableover the internet(Huang
2009).
• Reducing the data:To extract major themes,data
were summarised and reduced during two rounds of
coding.
• Abductive inference:Abductive inference is the pro-
cess of bridging the gap between description of data
and the conclusionsdrawn from data.The under-
pinning idea is that the data themselvesprovide
proof for the conclusionsthat have been derived
from the same (Krippendorff2004).However,the
conclusions drawn need to be backed up or ‘war-
ranted’by a theoreticalconstructthat acts like a
hypothesisand explains the texts’ intendeduse
(Krippendorff2004). In content analysis,research
questions serve this purpose.According to Krippen-
dorff (2004 p. 31–32), research questionsbear a
similarity to hypotheses in observationalresearch in
so far as they focusthe research by delineating a
numberof possibleand, at the outset,uncertain
answers.In this study,the analyticalconstruct was
based on the following research questions:Which
common theoreticalconcepts ofEI are used in the
nursing literature? How are concepts and their defi-
nitions critiqued and justified?What is the value
ascribed to EI in generaland for leadership in nurs-
ing?
The initial analyticalconstructproved to be too
restrictive to extract relevant data to contextualise and
corroborate the findings,therefore itwas, during the
iterative process of analysis, continuouslyrevised
(Krippendorff 2004).
• Narrating:‘Narrating’concerns presentation ofthe
results in a comprehensible fashion.(Please refer to
respective section – results – of this publication.)
Results
The findingsare presented asa corroboration and
contextualisation ofmajor themes thatemerged as a
result of both coding phases.
Description of the sample characteristics
From the stated authors’aims,three different types of
publications were distinguishable:
Advocacy and opinion articles (n = 16; Kerfoot
1996, Tahan 2000, Snow 2001, Amendolair2003,
Porter-O’Grady 2003, Prosser 2003, Vitello-Cicciu
2003, Daniel 2004, Fuimano 2004, Baggett & Baggett
2005, Borbasi& Jackson 2005, Piper 2005,Stichler
2006, Triola 2007, Eason 2009, Wright 2009),
research reports (n = 2;Cummings et al.2005,Lucas
et al. 2008), and literaturereviews(n = 4; Vitello-
Cicciu 2002, Herbert & Edgar 2004, Akerjordet&
Severinsson 2008, Feather 2009).
The most frequently employed theoretical model was
the Goleman model. All of the 16 ‘advocacy and opin-
ion articles’referred to this model,which was chosen
either explicitly (10/16) or implicitly (6/16) by present-
ing a modelof EI featuring characteristics that corre-
sponded with those proposed by Goleman (1996).
Both research reportswere based on Goleman’s
assessmenttools (Cummings et al.2005, Lucas et al.
2008).Lucas et al.(2008) described and critiqued the
ª 2014 John Wiley & Sons Ltd
Journal of Nursing Management, 2015, 23, 744–753 747
Leading with emotionalintelligence
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
constructof EI and gave a rationale forchoosing a
particular model.
Cummingset al. (2005) explained theirmodel of
choice,the Goleman model,but did not critique the
construct or justify their approach.
The literaturereview studiesprovided overviews
withoutfavouring any ofthe EI models.Out of four
review studies,threediscussed EIcritically (Vitello-
Cicciu 2002,Herbert& Edgar 2004, Feather 2009).
One study neither discussed different models or defini-
tions,nor critically evaluated EI(Akerjordet& Seve-
rinsson 2008).
Emotional intelligence in nurse leadership
There is consensuswithin the sampletexts that EI
nurse leadersare high performers who contribute to
organisationalsuccess at various levels.On a personal
level,this effectis mediated by increased self-aware-
ness. Prosser (2003 p. 357) writes:
‘Through understanding the concept of EI, we can
better see the significance of self-awareness, social
awareness,self-management,and relationship
management to our performance as a leader’.
The EI leaders also contribute to enhanced perfor-
mance of their staff,by inspiring,motivating and cre-
ating a nurturing environmentfor thosewho work
under their lead:
‘Leaders with a high levelof EI drive emotions
positively,bring out the bestin all members of
an organisation,and connectwith others atan
emotionallevelto make work more meaningful,
as well as infusing vitality and energy into the
workplace’.
(Akerjordet & Severinsson 2008 p. 568)
In addition to motivating and inspiring,an EI nurse
leader aligns staff with organisational values:
‘Leadership involves leading and influencing peo-
ple to develop shared values, vision and expecta-
tions to enhanceorganisationalstrategicgoals
and effectiveness’. (Feather 2009 p. 379)
This congruence between organisationalvalues and
staff values creates a dedicated workforce:
‘The essentialwork of leadersis keeping the
organisation and its membersdisciplined and
focused;discerning and directing theorganisa-
tion to create a good fitbetween its efforts and
what it is becoming;and energising and encour-
aging workersthroughoutthe chaosand com-
plexity of this journey’.
(Porter-O’Grady 2003 p. 110).
Part and parcel of this is to utilise emotions in the lead-
ership process.EI leaders arouse passion in their staff,
and they create a culture that nurtures this passion:
‘To accomplish passion,everyonemust under-
stand the mission,and their heartsand souls
must be nurtured by the values that are lived in
the culture of the organisation’.
(Piper 2005 p. 44)
According to Amendolair (2003 p. 26), this is where
the true value of EI lies:
‘The value of EI is great:if employees’emotions
are pushed toward positive thoughtsand their
enthusiasm ignited,their performancesoars.
Emotions can drive people more forcefully than
any words ever could’.
Increased staffperformancewill also affect team
performance and contribute to organisationalperfor-
mance and success.A ‘ripple effect’is attributed to EI
leadership: the EI leader, as a reflective and self-aware
person,createsa healthy and supportive work envi-
ronment for their staff.This environment allows staff
to perform to the best of their ability and to cope with
stressful working conditions.
The findings described above highlightthe EI nurse
leader’s pivotal role. Two points are particularly relevant
in this respect: First, nurse leadership is essential for cre-
ating a work environment that can sustain a workforce
fit to survive in an increasingly competitive environment.
Second,EI nurse leadership has a ‘ripple effect’on the
individual state, on the team and on the organisation.
These essentialpoints can be further conceptualised
into three central,interlinked dimensionsthat cha-
racterise EI nurse leadership:The nurse leaderis a
‘socio-cultural architect’, ‘responsive carer’ and ‘strate-
gic visionary’.
The term ‘socio-cultural architect’ relates to a leader’s
ability actively to influence and create the workplace
culture and its values.Like an architect who designs a
building,the leaderdesignsthe culture ofthe work
environment.In this process,the leader acts as a role
model, whose actions are based on personal beliefs and
values.The following quote stipulates the importance
of the leader’s role in creating the socio-cultural climate
within a team:
‘The mood,attitude and contiguous patterns of
interaction of the leader with the state and oth-
ª 2014 John Wiley & Sons Ltd
748 Journal of Nursing Management, 2015, 23, 744–753
B. Heckemann etal.
particular model.
Cummingset al. (2005) explained theirmodel of
choice,the Goleman model,but did not critique the
construct or justify their approach.
The literaturereview studiesprovided overviews
withoutfavouring any ofthe EI models.Out of four
review studies,threediscussed EIcritically (Vitello-
Cicciu 2002,Herbert& Edgar 2004, Feather 2009).
One study neither discussed different models or defini-
tions,nor critically evaluated EI(Akerjordet& Seve-
rinsson 2008).
Emotional intelligence in nurse leadership
There is consensuswithin the sampletexts that EI
nurse leadersare high performers who contribute to
organisationalsuccess at various levels.On a personal
level,this effectis mediated by increased self-aware-
ness. Prosser (2003 p. 357) writes:
‘Through understanding the concept of EI, we can
better see the significance of self-awareness, social
awareness,self-management,and relationship
management to our performance as a leader’.
The EI leaders also contribute to enhanced perfor-
mance of their staff,by inspiring,motivating and cre-
ating a nurturing environmentfor thosewho work
under their lead:
‘Leaders with a high levelof EI drive emotions
positively,bring out the bestin all members of
an organisation,and connectwith others atan
emotionallevelto make work more meaningful,
as well as infusing vitality and energy into the
workplace’.
(Akerjordet & Severinsson 2008 p. 568)
In addition to motivating and inspiring,an EI nurse
leader aligns staff with organisational values:
‘Leadership involves leading and influencing peo-
ple to develop shared values, vision and expecta-
tions to enhanceorganisationalstrategicgoals
and effectiveness’. (Feather 2009 p. 379)
This congruence between organisationalvalues and
staff values creates a dedicated workforce:
‘The essentialwork of leadersis keeping the
organisation and its membersdisciplined and
focused;discerning and directing theorganisa-
tion to create a good fitbetween its efforts and
what it is becoming;and energising and encour-
aging workersthroughoutthe chaosand com-
plexity of this journey’.
(Porter-O’Grady 2003 p. 110).
Part and parcel of this is to utilise emotions in the lead-
ership process.EI leaders arouse passion in their staff,
and they create a culture that nurtures this passion:
‘To accomplish passion,everyonemust under-
stand the mission,and their heartsand souls
must be nurtured by the values that are lived in
the culture of the organisation’.
(Piper 2005 p. 44)
According to Amendolair (2003 p. 26), this is where
the true value of EI lies:
‘The value of EI is great:if employees’emotions
are pushed toward positive thoughtsand their
enthusiasm ignited,their performancesoars.
Emotions can drive people more forcefully than
any words ever could’.
Increased staffperformancewill also affect team
performance and contribute to organisationalperfor-
mance and success.A ‘ripple effect’is attributed to EI
leadership: the EI leader, as a reflective and self-aware
person,createsa healthy and supportive work envi-
ronment for their staff.This environment allows staff
to perform to the best of their ability and to cope with
stressful working conditions.
The findings described above highlightthe EI nurse
leader’s pivotal role. Two points are particularly relevant
in this respect: First, nurse leadership is essential for cre-
ating a work environment that can sustain a workforce
fit to survive in an increasingly competitive environment.
Second,EI nurse leadership has a ‘ripple effect’on the
individual state, on the team and on the organisation.
These essentialpoints can be further conceptualised
into three central,interlinked dimensionsthat cha-
racterise EI nurse leadership:The nurse leaderis a
‘socio-cultural architect’, ‘responsive carer’ and ‘strate-
gic visionary’.
The term ‘socio-cultural architect’ relates to a leader’s
ability actively to influence and create the workplace
culture and its values.Like an architect who designs a
building,the leaderdesignsthe culture ofthe work
environment.In this process,the leader acts as a role
model, whose actions are based on personal beliefs and
values.The following quote stipulates the importance
of the leader’s role in creating the socio-cultural climate
within a team:
‘The mood,attitude and contiguous patterns of
interaction of the leader with the state and oth-
ª 2014 John Wiley & Sons Ltd
748 Journal of Nursing Management, 2015, 23, 744–753
B. Heckemann etal.
ers have a tremendous effect on the culture, con-
text and content of work. […] More impor-
tantly, the leader’s behaviours have a
tremendousimpact on the behavioursof the
team. This research furthershows that when
emotionsare tracked together,they are largely
interdependent,meaningthat everyoneshares
the impactof the emotions ofany one member
of the team.Staff also take clear emotionalcues
from leaders.The mood and resultant pattern of
behaviour of the leader creates a lasting impres-
sion reflected in the team’s behaviour’.
(Porter-O’Grady 2003 p. 108)
While this will apply to any leader,the EI leader
has specific moralvalues that contribute to creating a
healthy work environment,as Amendolair (2003)
highlights:
‘Nursing leaders must develop their EI to create
a climate that allows and encourages the staff to
becomelifelong learners,and passion in their
work so they may display compassion to their
patients and quiet the fires that are causing burn-
out and pushing nurses out of the profession’.
(Amendolair 2003 p. 27)
The term ‘responsive carer’relates to the nurse lea-
der’s ability to perceive,identify and act according to
information relating to herown emotionalstateas
well as that of her staff.
A nurse leaderneedsto be responsive to herown
needs, in order to be able to care for others:
‘Caring for themselves as nurse leaders is one of
the most important things they can do to provide
good care for others’.
(Akerjordet & Severinsson 2008 p. 569)
Caring for others requires empathy and giving the sup-
port that staff need to retain a state of emotional balance.
‘[Emotionally intelligentleaders]can easily step
into another’s shoes and see the world from their
perspective’. (Kerfoot 1996 p. 60)
This caring attitude is grounded in a genuine appre-
ciation of staff, because
‘[Nurses] in leadership positions have the vitally
importantresponsibility ofrecognising the pre-
cious resource they have in their nursing staff’.
(Feather 2009 p. 380)
In caring for their staff, the leadertakespersonal
responsibility for those who work with her:
‘[a]s a nurse leader,[…] to best manageand
coordinate patient care, your leadership
approach mustoffer sensitivity and responsive-
ness to nurses’increased physicaland emotional
labor’. (Vitello-Cicciu 2003 p. 30)
As ‘strategicvisionaries’,nurse leadershave the
foresightto anticipate changes ofdirection in health
care planning and to develop coping strategiesthat
enable organisationsto survive within the current
challengingclimate. Porter-O’Grady(2003 p. 109)
explains:
‘Leaders are fundamentally interested in the direc-
tion of an organisation rather than simply its func-
tions and activities.Leaders attemptto view all
activity in the context of the major themes,ebbs
and flows,and trajectories of human endeavour.
In short, leaders see their role from the balcony
rather than from the street. Leaders operate with
a sense of vision. They can see all of the activities
of work in the contextof how action coalesces
and synthesises around the processes and direction
of the organisational journey’.
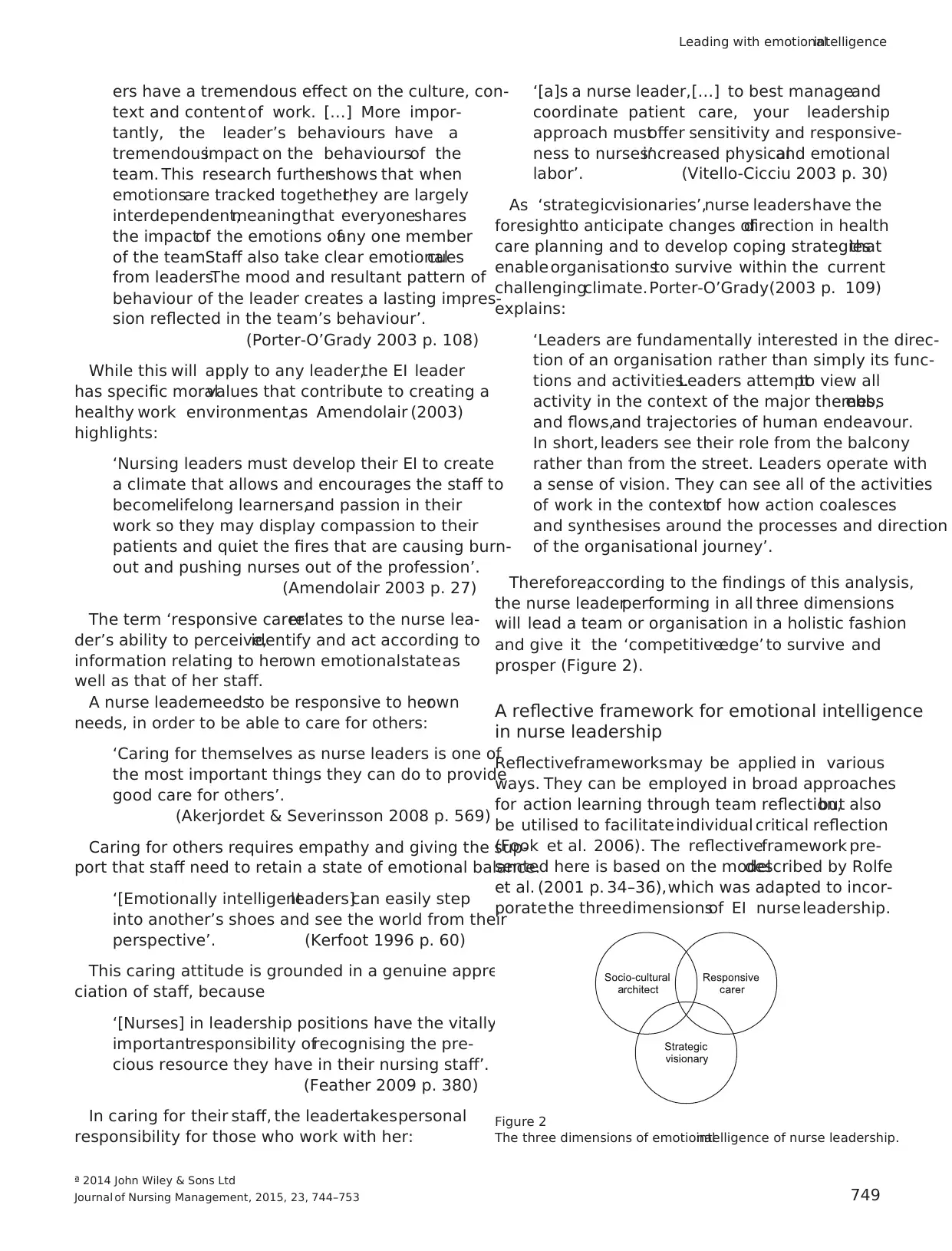
Therefore,according to the findings of this analysis,
the nurse leaderperforming in all three dimensions
will lead a team or organisation in a holistic fashion
and give it the ‘competitiveedge’ to survive and
prosper (Figure 2).
A reflective framework for emotional intelligence
in nurse leadership
Reflectiveframeworksmay be applied in various
ways. They can be employed in broad approaches
for action learning through team reflection,but also
be utilised to facilitateindividual critical reflection
(Fook et al. 2006). The reflectiveframework pre-
sented here is based on the modeldescribed by Rolfe
et al. (2001 p. 34–36),which was adapted to incor-
poratethe threedimensionsof EI nurseleadership.
Figure 2
The three dimensions of emotionalintelligence of nurse leadership.
ª 2014 John Wiley & Sons Ltd
Journal of Nursing Management, 2015, 23, 744–753 749
Leading with emotionalintelligence
text and content of work. […] More impor-
tantly, the leader’s behaviours have a
tremendousimpact on the behavioursof the
team. This research furthershows that when
emotionsare tracked together,they are largely
interdependent,meaningthat everyoneshares
the impactof the emotions ofany one member
of the team.Staff also take clear emotionalcues
from leaders.The mood and resultant pattern of
behaviour of the leader creates a lasting impres-
sion reflected in the team’s behaviour’.
(Porter-O’Grady 2003 p. 108)
While this will apply to any leader,the EI leader
has specific moralvalues that contribute to creating a
healthy work environment,as Amendolair (2003)
highlights:
‘Nursing leaders must develop their EI to create
a climate that allows and encourages the staff to
becomelifelong learners,and passion in their
work so they may display compassion to their
patients and quiet the fires that are causing burn-
out and pushing nurses out of the profession’.
(Amendolair 2003 p. 27)
The term ‘responsive carer’relates to the nurse lea-
der’s ability to perceive,identify and act according to
information relating to herown emotionalstateas
well as that of her staff.
A nurse leaderneedsto be responsive to herown
needs, in order to be able to care for others:
‘Caring for themselves as nurse leaders is one of
the most important things they can do to provide
good care for others’.
(Akerjordet & Severinsson 2008 p. 569)
Caring for others requires empathy and giving the sup-
port that staff need to retain a state of emotional balance.
‘[Emotionally intelligentleaders]can easily step
into another’s shoes and see the world from their
perspective’. (Kerfoot 1996 p. 60)
This caring attitude is grounded in a genuine appre-
ciation of staff, because
‘[Nurses] in leadership positions have the vitally
importantresponsibility ofrecognising the pre-
cious resource they have in their nursing staff’.
(Feather 2009 p. 380)
In caring for their staff, the leadertakespersonal
responsibility for those who work with her:
‘[a]s a nurse leader,[…] to best manageand
coordinate patient care, your leadership
approach mustoffer sensitivity and responsive-
ness to nurses’increased physicaland emotional
labor’. (Vitello-Cicciu 2003 p. 30)
As ‘strategicvisionaries’,nurse leadershave the
foresightto anticipate changes ofdirection in health
care planning and to develop coping strategiesthat
enable organisationsto survive within the current
challengingclimate. Porter-O’Grady(2003 p. 109)
explains:
‘Leaders are fundamentally interested in the direc-
tion of an organisation rather than simply its func-
tions and activities.Leaders attemptto view all
activity in the context of the major themes,ebbs
and flows,and trajectories of human endeavour.
In short, leaders see their role from the balcony
rather than from the street. Leaders operate with
a sense of vision. They can see all of the activities
of work in the contextof how action coalesces
and synthesises around the processes and direction
of the organisational journey’.
Therefore,according to the findings of this analysis,
the nurse leaderperforming in all three dimensions
will lead a team or organisation in a holistic fashion
and give it the ‘competitiveedge’ to survive and
prosper (Figure 2).
A reflective framework for emotional intelligence
in nurse leadership
Reflectiveframeworksmay be applied in various
ways. They can be employed in broad approaches
for action learning through team reflection,but also
be utilised to facilitateindividual critical reflection
(Fook et al. 2006). The reflectiveframework pre-
sented here is based on the modeldescribed by Rolfe
et al. (2001 p. 34–36),which was adapted to incor-
poratethe threedimensionsof EI nurseleadership.
Figure 2
The three dimensions of emotionalintelligence of nurse leadership.
ª 2014 John Wiley & Sons Ltd
Journal of Nursing Management, 2015, 23, 744–753 749
Leading with emotionalintelligence
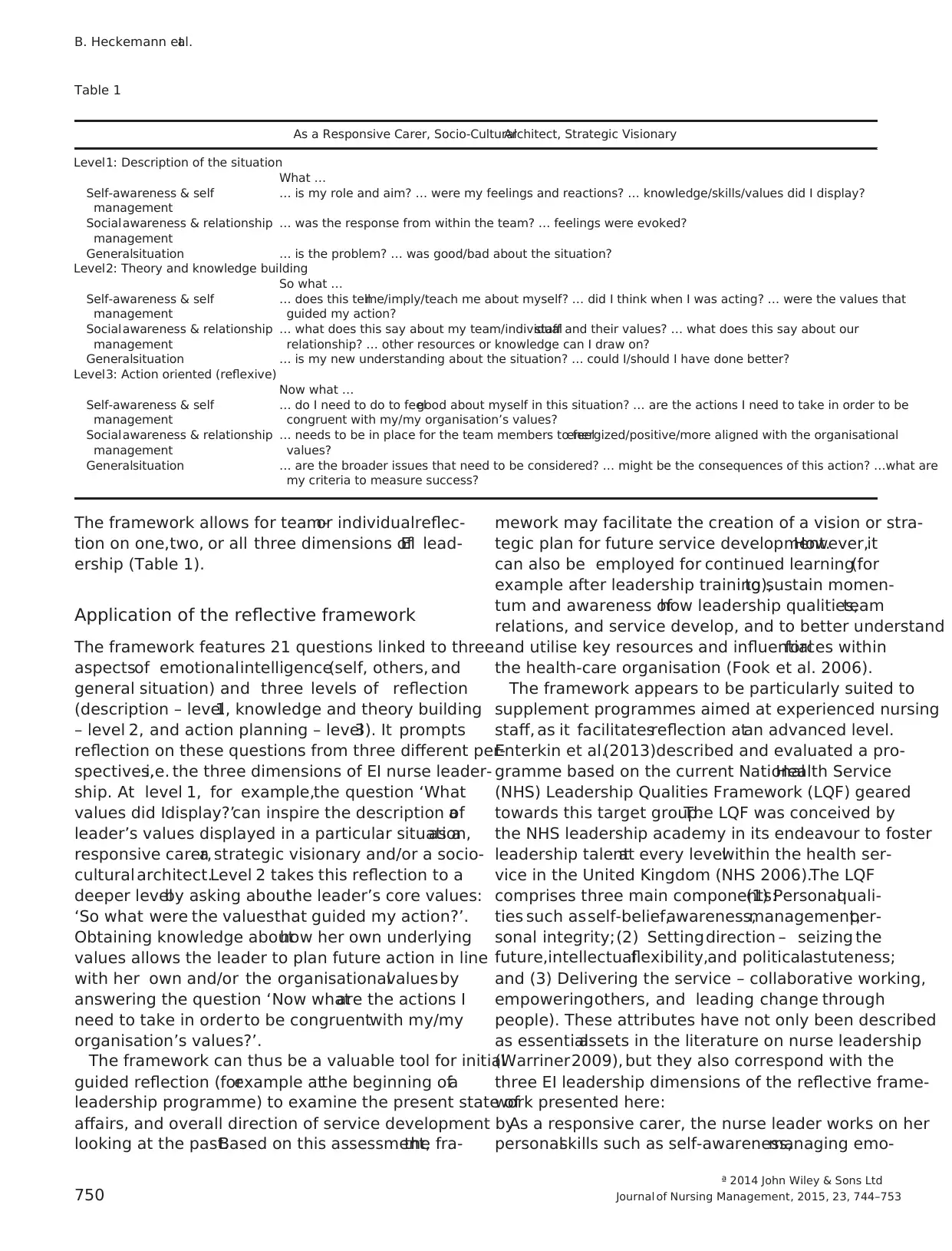
The framework allows for team-or individualreflec-
tion on one,two, or all three dimensions ofEI lead-
ership (Table 1).
Application of the reflective framework
The framework features 21 questions linked to three
aspectsof emotionalintelligence(self, others, and
general situation) and three levels of reflection
(description – level1, knowledge and theory building
– level 2, and action planning – level3). It prompts
reflection on these questions from three different per-
spectives,i.e. the three dimensions of EI nurse leader-
ship. At level 1, for example,the question ‘What
values did Idisplay?’can inspire the description ofa
leader’s values displayed in a particular situation,as a
responsive carer,a strategic visionary and/or a socio-
cultural architect.Level 2 takes this reflection to a
deeper levelby asking aboutthe leader’s core values:
‘So what were the valuesthat guided my action?’.
Obtaining knowledge abouthow her own underlying
values allows the leader to plan future action in line
with her own and/or the organisationalvaluesby
answering the question ‘Now whatare the actions I
need to take in order to be congruentwith my/my
organisation’s values?’.
The framework can thus be a valuable tool for initial
guided reflection (forexample atthe beginning ofa
leadership programme) to examine the present state of
affairs, and overall direction of service development by
looking at the past.Based on this assessment,the fra-
mework may facilitate the creation of a vision or stra-
tegic plan for future service development.However,it
can also be employed for continued learning(for
example after leadership training),to sustain momen-
tum and awareness ofhow leadership qualities,team
relations, and service develop, and to better understand
and utilise key resources and influentialforces within
the health-care organisation (Fook et al. 2006).
The framework appears to be particularly suited to
supplement programmes aimed at experienced nursing
staff, as it facilitatesreflection atan advanced level.
Enterkin et al.(2013)described and evaluated a pro-
gramme based on the current NationalHealth Service
(NHS) Leadership Qualities Framework (LQF) geared
towards this target group.The LQF was conceived by
the NHS leadership academy in its endeavour to foster
leadership talentat every levelwithin the health ser-
vice in the United Kingdom (NHS 2006).The LQF
comprises three main components:(1) Personalquali-
ties such asself-belief,awareness,management,per-
sonal integrity;(2) Settingdirection – seizing the
future,intellectualflexibility,and politicalastuteness;
and (3) Delivering the service – collaborative working,
empoweringothers, and leading change through
people). These attributes have not only been described
as essentialassets in the literature on nurse leadership
(Warriner2009), but they also correspond with the
three EI leadership dimensions of the reflective frame-
work presented here:
As a responsive carer, the nurse leader works on her
personalskills such as self-awareness,managing emo-
Table 1
As a Responsive Carer, Socio-CulturalArchitect, Strategic Visionary
Level1: Description of the situation
What …
Self-awareness & self
management
… is my role and aim? … were my feelings and reactions? … knowledge/skills/values did I display?
Socialawareness & relationship
management
… was the response from within the team? … feelings were evoked?
Generalsituation … is the problem? … was good/bad about the situation?
Level2: Theory and knowledge building
So what …
Self-awareness & self
management
… does this tellme/imply/teach me about myself? … did I think when I was acting? … were the values that
guided my action?
Socialawareness & relationship
management
… what does this say about my team/individualstaff and their values? … what does this say about our
relationship? … other resources or knowledge can I draw on?
Generalsituation … is my new understanding about the situation? … could I/should I have done better?
Level3: Action oriented (reflexive)
Now what …
Self-awareness & self
management
… do I need to do to feelgood about myself in this situation? … are the actions I need to take in order to be
congruent with my/my organisation’s values?
Socialawareness & relationship
management
… needs to be in place for the team members to feelenergized/positive/more aligned with the organisational
values?
Generalsituation … are the broader issues that need to be considered? … might be the consequences of this action? …what are
my criteria to measure success?
ª 2014 John Wiley & Sons Ltd
750 Journal of Nursing Management, 2015, 23, 744–753
B. Heckemann etal.
tion on one,two, or all three dimensions ofEI lead-
ership (Table 1).
Application of the reflective framework
The framework features 21 questions linked to three
aspectsof emotionalintelligence(self, others, and
general situation) and three levels of reflection
(description – level1, knowledge and theory building
– level 2, and action planning – level3). It prompts
reflection on these questions from three different per-
spectives,i.e. the three dimensions of EI nurse leader-
ship. At level 1, for example,the question ‘What
values did Idisplay?’can inspire the description ofa
leader’s values displayed in a particular situation,as a
responsive carer,a strategic visionary and/or a socio-
cultural architect.Level 2 takes this reflection to a
deeper levelby asking aboutthe leader’s core values:
‘So what were the valuesthat guided my action?’.
Obtaining knowledge abouthow her own underlying
values allows the leader to plan future action in line
with her own and/or the organisationalvaluesby
answering the question ‘Now whatare the actions I
need to take in order to be congruentwith my/my
organisation’s values?’.
The framework can thus be a valuable tool for initial
guided reflection (forexample atthe beginning ofa
leadership programme) to examine the present state of
affairs, and overall direction of service development by
looking at the past.Based on this assessment,the fra-
mework may facilitate the creation of a vision or stra-
tegic plan for future service development.However,it
can also be employed for continued learning(for
example after leadership training),to sustain momen-
tum and awareness ofhow leadership qualities,team
relations, and service develop, and to better understand
and utilise key resources and influentialforces within
the health-care organisation (Fook et al. 2006).
The framework appears to be particularly suited to
supplement programmes aimed at experienced nursing
staff, as it facilitatesreflection atan advanced level.
Enterkin et al.(2013)described and evaluated a pro-
gramme based on the current NationalHealth Service
(NHS) Leadership Qualities Framework (LQF) geared
towards this target group.The LQF was conceived by
the NHS leadership academy in its endeavour to foster
leadership talentat every levelwithin the health ser-
vice in the United Kingdom (NHS 2006).The LQF
comprises three main components:(1) Personalquali-
ties such asself-belief,awareness,management,per-
sonal integrity;(2) Settingdirection – seizing the
future,intellectualflexibility,and politicalastuteness;
and (3) Delivering the service – collaborative working,
empoweringothers, and leading change through
people). These attributes have not only been described
as essentialassets in the literature on nurse leadership
(Warriner2009), but they also correspond with the
three EI leadership dimensions of the reflective frame-
work presented here:
As a responsive carer, the nurse leader works on her
personalskills such as self-awareness,managing emo-
Table 1
As a Responsive Carer, Socio-CulturalArchitect, Strategic Visionary
Level1: Description of the situation
What …
Self-awareness & self
management
… is my role and aim? … were my feelings and reactions? … knowledge/skills/values did I display?
Socialawareness & relationship
management
… was the response from within the team? … feelings were evoked?
Generalsituation … is the problem? … was good/bad about the situation?
Level2: Theory and knowledge building
So what …
Self-awareness & self
management
… does this tellme/imply/teach me about myself? … did I think when I was acting? … were the values that
guided my action?
Socialawareness & relationship
management
… what does this say about my team/individualstaff and their values? … what does this say about our
relationship? … other resources or knowledge can I draw on?
Generalsituation … is my new understanding about the situation? … could I/should I have done better?
Level3: Action oriented (reflexive)
Now what …
Self-awareness & self
management
… do I need to do to feelgood about myself in this situation? … are the actions I need to take in order to be
congruent with my/my organisation’s values?
Socialawareness & relationship
management
… needs to be in place for the team members to feelenergized/positive/more aligned with the organisational
values?
Generalsituation … are the broader issues that need to be considered? … might be the consequences of this action? …what are
my criteria to measure success?
ª 2014 John Wiley & Sons Ltd
750 Journal of Nursing Management, 2015, 23, 744–753
B. Heckemann etal.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

tions and acting with integrity. As a strategic visionary
and socio-culturalarchitect,the nurse leader demon-
strates,according to the resultsof this research,the
ability to work with others, manageindividuals,
teams,and resources,improve servicesand plan for
future developmentwith intellectualflexibility.Con-
sidering this overlap,the reflective framework of EI in
nursing leadership could be a valuable addition to any
leadership programme based on the NHS LQF.
However,the reflective framework incorporates the
hallmarks of EI nurse leadership and thereby addresses
the emotionalside of leadershipas well. In this
respect,it broadensthe scope ofthe LQF in that it
prompts the nurse leader not just to examine her own
emotions,but also to consider the feelingsof the
people working alongside her.The awarenessof co-
worker emotions has been highlighted as an important
factor for sustaining positiveworking relationsand
communication,as the increasingly managerialnature
of nurse leaders’roles and the ensuing estrangement
from front-line nursing may create a climate ofdis-
trust between nurse leaders and front-line staff
(Squires et al. 2010, Udod & Care 2013).
The inclusion of the emotionalside of leading
makesthe framework also suitable forreflection on
the attributes of resonant leadership(Cummings
2004),or on a recentmodelproposed by Drenkard
(2012),who conceptualised EIleadership in relation
to self, to others, and to systems.
Discussion
The results of a qualitative descriptive content analysis
related to emotionalintelligence in nursing leadership
presented in this paper offer a novel perspective of the
defining roles of an emotionallyintelligentnurse
leaderwho performsas a ‘responsive carer’,‘socio-
culturalarchitect’and ‘strategic visionary’.Moreover,
the findingshave been made available forpractical,
real-life application by contextualising them within a
reflective framework modeled after Rolfe et al.
(2001).Pending practicalapplication and evaluation,
this framework could supplementnurse training pro-
grammes that foster not just the managerial,but also
the emotional side of leadership.
However,there are a number oflimitations to this
study. The research method,content analysis,has
been criticised for lack ofrigour in its approach and
adherence to methodologicalstandards (Krippendorff
2004). Moreover, the analyseswere done by one
researcher (B.H.). In acknowledgement of these limita-
tions, an open research process was chosen, all aspects
of which were documented to enable externalscru-
tiny. To enhance both validity and reliability ofthe
results,an ‘audittrail’ comprising the raw data,cod-
ing protocols including coding notes, coding diary and
handwrittenrecords was kept (Lincoln & Guba
1985). In addition, the main researcher(B.H.) also
kept a reflectivecoding diary to log thoughts and
ideas thatdeveloped during the research process and
to monitor how her own perception changed and
developed during the work with the data (Lincoln &
Guba 1985).
A second limitation is the restriction ofthe sample
to articles published between January 1996 and April
2009. Literature relating to nurse leadership and EI
published since was not included in the content analy-
sis.However,the characteristics of EI leadership iden-
tified within the sample ofarticlesanalysed in this
study resound with the values attached to EIleader-
ship in the current nursing literature (e.g. Squires et al.
2010, Codier et al. 2011, Dellaria Doas2011). The
findingsand resulting reflective framework therefore
still appear to be applicable and relevant, and, in fact,
timely.In current literature,the question how to fos-
ter EI skills in nurse leaders appears to be of increas-
ing concern.Training is regarded as essentialin this
respect(Croskerry et al.2010, Codier et al. 2011),
with recentevidence pointing towardssome positive
effectof EI training for nurses(Codier et al. 2011).
Nevertheless,there stillremains ample scope for fur-
ther research into how EI skills may be enhanced. The
reflectiveframework proposed heremay well be a
valuable addition to courses and respective evaluation
projectsaimed at EI developmentin nurse leaders.
Because of the criticism that has been leveled at reflec-
tion as a method,the organisation ofthe three roles
of EI leadership in a reflective framework also war-
rants discussion.To this day,the benefits of reflection
have not been proven by empirical research. Neverthe-
less,reflection is extensively employed in health care
as part of a broad approach to learning aimed at fos-
tering criticalthinking (Fook et al.2006). A recent
interview studywith successfulnurse leadershigh-
lighted theimportanceof self-guided and self-moti-
vated reflection forleadersto understand theirown
sense ofpurpose and to gain insightinto their core
values and beliefs (Murphy 2012). A nurse leader who
has found reflection to be a suitable toolto aid her
personaldevelopmentand strategicplanningmight
therefore find the proposed reflective framework a use-
ful ‘aide-memoire’.
Reflection based on theprinciplesof EI has also
previouslybeen discussed in thenursing literature.
ª 2014 John Wiley & Sons Ltd
Journal of Nursing Management, 2015, 23, 744–753 751
Leading with emotionalintelligence
and socio-culturalarchitect,the nurse leader demon-
strates,according to the resultsof this research,the
ability to work with others, manageindividuals,
teams,and resources,improve servicesand plan for
future developmentwith intellectualflexibility.Con-
sidering this overlap,the reflective framework of EI in
nursing leadership could be a valuable addition to any
leadership programme based on the NHS LQF.
However,the reflective framework incorporates the
hallmarks of EI nurse leadership and thereby addresses
the emotionalside of leadershipas well. In this
respect,it broadensthe scope ofthe LQF in that it
prompts the nurse leader not just to examine her own
emotions,but also to consider the feelingsof the
people working alongside her.The awarenessof co-
worker emotions has been highlighted as an important
factor for sustaining positiveworking relationsand
communication,as the increasingly managerialnature
of nurse leaders’roles and the ensuing estrangement
from front-line nursing may create a climate ofdis-
trust between nurse leaders and front-line staff
(Squires et al. 2010, Udod & Care 2013).
The inclusion of the emotionalside of leading
makesthe framework also suitable forreflection on
the attributes of resonant leadership(Cummings
2004),or on a recentmodelproposed by Drenkard
(2012),who conceptualised EIleadership in relation
to self, to others, and to systems.
Discussion
The results of a qualitative descriptive content analysis
related to emotionalintelligence in nursing leadership
presented in this paper offer a novel perspective of the
defining roles of an emotionallyintelligentnurse
leaderwho performsas a ‘responsive carer’,‘socio-
culturalarchitect’and ‘strategic visionary’.Moreover,
the findingshave been made available forpractical,
real-life application by contextualising them within a
reflective framework modeled after Rolfe et al.
(2001).Pending practicalapplication and evaluation,
this framework could supplementnurse training pro-
grammes that foster not just the managerial,but also
the emotional side of leadership.
However,there are a number oflimitations to this
study. The research method,content analysis,has
been criticised for lack ofrigour in its approach and
adherence to methodologicalstandards (Krippendorff
2004). Moreover, the analyseswere done by one
researcher (B.H.). In acknowledgement of these limita-
tions, an open research process was chosen, all aspects
of which were documented to enable externalscru-
tiny. To enhance both validity and reliability ofthe
results,an ‘audittrail’ comprising the raw data,cod-
ing protocols including coding notes, coding diary and
handwrittenrecords was kept (Lincoln & Guba
1985). In addition, the main researcher(B.H.) also
kept a reflectivecoding diary to log thoughts and
ideas thatdeveloped during the research process and
to monitor how her own perception changed and
developed during the work with the data (Lincoln &
Guba 1985).
A second limitation is the restriction ofthe sample
to articles published between January 1996 and April
2009. Literature relating to nurse leadership and EI
published since was not included in the content analy-
sis.However,the characteristics of EI leadership iden-
tified within the sample ofarticlesanalysed in this
study resound with the values attached to EIleader-
ship in the current nursing literature (e.g. Squires et al.
2010, Codier et al. 2011, Dellaria Doas2011). The
findingsand resulting reflective framework therefore
still appear to be applicable and relevant, and, in fact,
timely.In current literature,the question how to fos-
ter EI skills in nurse leaders appears to be of increas-
ing concern.Training is regarded as essentialin this
respect(Croskerry et al.2010, Codier et al. 2011),
with recentevidence pointing towardssome positive
effectof EI training for nurses(Codier et al. 2011).
Nevertheless,there stillremains ample scope for fur-
ther research into how EI skills may be enhanced. The
reflectiveframework proposed heremay well be a
valuable addition to courses and respective evaluation
projectsaimed at EI developmentin nurse leaders.
Because of the criticism that has been leveled at reflec-
tion as a method,the organisation ofthe three roles
of EI leadership in a reflective framework also war-
rants discussion.To this day,the benefits of reflection
have not been proven by empirical research. Neverthe-
less,reflection is extensively employed in health care
as part of a broad approach to learning aimed at fos-
tering criticalthinking (Fook et al.2006). A recent
interview studywith successfulnurse leadershigh-
lighted theimportanceof self-guided and self-moti-
vated reflection forleadersto understand theirown
sense ofpurpose and to gain insightinto their core
values and beliefs (Murphy 2012). A nurse leader who
has found reflection to be a suitable toolto aid her
personaldevelopmentand strategicplanningmight
therefore find the proposed reflective framework a use-
ful ‘aide-memoire’.
Reflection based on theprinciplesof EI has also
previouslybeen discussed in thenursing literature.
ª 2014 John Wiley & Sons Ltd
Journal of Nursing Management, 2015, 23, 744–753 751
Leading with emotionalintelligence
The strategiesproposed by Horton-Deutschand
Sherwood (2008)addressall areasthat are relevant
to developing nurse leadership.In this respect,their
modelis similar to the one proposed here.However,
the framework presentedin this work offers a
guided approach to reflectionin that it prompts
nursesto consider the various dimensionsof their
own leadership role,combined with the possibility
longitudinally to assessthe developmentof the ser-
vice, work relationshipsand self-awarenessby look-
ing at the past,presentand future.These potential
benefitswarrant the framework’sapplicationin a
practicalcontext.
Conclusion
The study presentedhere compriseda qualitative
descriptive content analysis of the literature related to
EI in nursing leadership.It contributesto current
knowledgein that it offers a novel perspectiveon
leadership by proposing three essential roles of a nurse
leader and by contextualising these within a reflective
framework.
The reflectiveframework may guide reflection
through the critical analysisand evaluation of the
work environment and organisational culture past and
present.It contributes to currentnursing practice by
facilitating nurse leaders to explore, analyse and foster
their EI leadership skills to assist with strategic work-
force planning.
However,this study also highlightsthe scopefor
further research into the three dimensions of EI leader-
ship.To date,this modelholds mere theoreticalvalue
as it emerged from an analysisof nursing literature,
but its validity would be strengthened if critiqued and
discussed in a wideracademic and nursing commu-
nity. Similarly,the reflective framework requires test-
ing in a real-life context, as it is at presenta
theoreticalconstructrequiring evaluation to ascertain
its value for the nursing profession.
Acknowledgements
We are very gratefulto Dr Peter Harper (RN, PhD)
(retired),former senior lecturer at Thames Valley
University,now University ofWest London, London,
UK who supervised this project.
Source of funding
This study wasconducted withoutany institutional,
third party private or corporate financial support.
Ethical approval
This research projectwas based on nursing related
articles publicly available and intended for dissemina-
tion; there was no direct involvementof human
participants.
References
AkerjordetK. & Severinsson E.(2008)Emotionally intelligent
nurse leadership: a literature review study. Journal of Nursing
Management 16 (5), 565–577.
Akerjordet K. & Severinsson E. (2010) The state of the science of
emotional intelligence related to nursing leadership: an integra-
tive review. Journal of Nursing Management 18 (4), 363–382.
AmendolairD. (2003) Emotional intelligence– essential for
developing nurse leaders. Nurse Leader 1 (6), 25–27.
BaggettM.M. & BaggettF.B. (2005)Move from management
to high-level leadership. Nursing Management 36 (7), 12.
Borbasi S. & Jackson D. (2005) Nursing leadership: power, pol-
itics and gender:the role of emotionalintelligence.Collegian
(Royal College of Nursing, Australia) 12 (1), 5–6.
Boyatzis R.& McKee A. (2005) Resonant Leadership.Harvard
Business School Press, Boston, MA.
Bulmer-SmithK., Profetto-McGrath J. & Cummings G.G.
(2009)Emotionalintelligence and nursing:an integrative lit-
erature review.InternationalJournal of Nursing Studies46
(12), 1624–1636.
Codier E.,Kamikawa C.& Kooker B.M. (2011) The impact of
emotionalintelligence development on nurse managers.Nurs-
ing Administration Quarterly 35 (3), 270–276.
Croskerry P., Abbass A. & Wu A.W. (2010) Emotional influences
in patient safety. Journal of Patient Safety 6 (4), 199–205.
Cummings G.(2004)Investing relationalenergy:the hallmark
of resonantleadership.Nursing Leadership (Toronto,Ont.)
17 (4), 76–87.
Cummings G., Hayduk L. & Estabrooks C. (2005) Mitigating the
impact of hospitalrestructuring on nurses:the responsibility of
emotionally intelligent leadership. Nursing Research 54 (1), 2–12.
Cummings G.G.,MacGregor T., Davey M. et al. (2010) Lead-
ership styles and outcome patterns for the nursing workforce
and work environment:a systematicreview. International
Journal of Nursing Studies 47 (3), 363–385.
Daniel A. (2004) EQ and empowering leadership.Singapore
Nursing Journal 31 (2), 20–25.
Davies A.,Wong C.A. & Laschinger H.(2011) Nurses’partici-
pation in personal knowledge transfer: the role of
leader–memberexchange(LMX) and structural empower-
ment. Journal of Nursing Management 19 (5), 632–643.
Dellaria Doas M. (2011) Is emotional competence a viable com-
ponentin today’s work environment? Journalfor Nurses in
Staff Development 27 (5), 206–209.
Drenkard K.(2012) The transformative power of personaland
organizationalleadership.Nursing Administration Quarterly
36 (2), 147–154.
Eason T. (2009) Emotional intelligence and nursing leadership: a
successful combination. Creative Nursing 15 (4), 184–185.
Enterkin J., Robb E. & McLaren S. (2013)Clinical leadership
for high-quality care:developing future ward leaders.Journal
of Nursing Management 21(2), 206–216.
ª 2014 John Wiley & Sons Ltd
752 Journal of Nursing Management, 2015, 23, 744–753
B. Heckemann etal.
Sherwood (2008)addressall areasthat are relevant
to developing nurse leadership.In this respect,their
modelis similar to the one proposed here.However,
the framework presentedin this work offers a
guided approach to reflectionin that it prompts
nursesto consider the various dimensionsof their
own leadership role,combined with the possibility
longitudinally to assessthe developmentof the ser-
vice, work relationshipsand self-awarenessby look-
ing at the past,presentand future.These potential
benefitswarrant the framework’sapplicationin a
practicalcontext.
Conclusion
The study presentedhere compriseda qualitative
descriptive content analysis of the literature related to
EI in nursing leadership.It contributesto current
knowledgein that it offers a novel perspectiveon
leadership by proposing three essential roles of a nurse
leader and by contextualising these within a reflective
framework.
The reflectiveframework may guide reflection
through the critical analysisand evaluation of the
work environment and organisational culture past and
present.It contributes to currentnursing practice by
facilitating nurse leaders to explore, analyse and foster
their EI leadership skills to assist with strategic work-
force planning.
However,this study also highlightsthe scopefor
further research into the three dimensions of EI leader-
ship.To date,this modelholds mere theoreticalvalue
as it emerged from an analysisof nursing literature,
but its validity would be strengthened if critiqued and
discussed in a wideracademic and nursing commu-
nity. Similarly,the reflective framework requires test-
ing in a real-life context, as it is at presenta
theoreticalconstructrequiring evaluation to ascertain
its value for the nursing profession.
Acknowledgements
We are very gratefulto Dr Peter Harper (RN, PhD)
(retired),former senior lecturer at Thames Valley
University,now University ofWest London, London,
UK who supervised this project.
Source of funding
This study wasconducted withoutany institutional,
third party private or corporate financial support.
Ethical approval
This research projectwas based on nursing related
articles publicly available and intended for dissemina-
tion; there was no direct involvementof human
participants.
References
AkerjordetK. & Severinsson E.(2008)Emotionally intelligent
nurse leadership: a literature review study. Journal of Nursing
Management 16 (5), 565–577.
Akerjordet K. & Severinsson E. (2010) The state of the science of
emotional intelligence related to nursing leadership: an integra-
tive review. Journal of Nursing Management 18 (4), 363–382.
AmendolairD. (2003) Emotional intelligence– essential for
developing nurse leaders. Nurse Leader 1 (6), 25–27.
BaggettM.M. & BaggettF.B. (2005)Move from management
to high-level leadership. Nursing Management 36 (7), 12.
Borbasi S. & Jackson D. (2005) Nursing leadership: power, pol-
itics and gender:the role of emotionalintelligence.Collegian
(Royal College of Nursing, Australia) 12 (1), 5–6.
Boyatzis R.& McKee A. (2005) Resonant Leadership.Harvard
Business School Press, Boston, MA.
Bulmer-SmithK., Profetto-McGrath J. & Cummings G.G.
(2009)Emotionalintelligence and nursing:an integrative lit-
erature review.InternationalJournal of Nursing Studies46
(12), 1624–1636.
Codier E.,Kamikawa C.& Kooker B.M. (2011) The impact of
emotionalintelligence development on nurse managers.Nurs-
ing Administration Quarterly 35 (3), 270–276.
Croskerry P., Abbass A. & Wu A.W. (2010) Emotional influences
in patient safety. Journal of Patient Safety 6 (4), 199–205.
Cummings G.(2004)Investing relationalenergy:the hallmark
of resonantleadership.Nursing Leadership (Toronto,Ont.)
17 (4), 76–87.
Cummings G., Hayduk L. & Estabrooks C. (2005) Mitigating the
impact of hospitalrestructuring on nurses:the responsibility of
emotionally intelligent leadership. Nursing Research 54 (1), 2–12.
Cummings G.G.,MacGregor T., Davey M. et al. (2010) Lead-
ership styles and outcome patterns for the nursing workforce
and work environment:a systematicreview. International
Journal of Nursing Studies 47 (3), 363–385.
Daniel A. (2004) EQ and empowering leadership.Singapore
Nursing Journal 31 (2), 20–25.
Davies A.,Wong C.A. & Laschinger H.(2011) Nurses’partici-
pation in personal knowledge transfer: the role of
leader–memberexchange(LMX) and structural empower-
ment. Journal of Nursing Management 19 (5), 632–643.
Dellaria Doas M. (2011) Is emotional competence a viable com-
ponentin today’s work environment? Journalfor Nurses in
Staff Development 27 (5), 206–209.
Drenkard K.(2012) The transformative power of personaland
organizationalleadership.Nursing Administration Quarterly
36 (2), 147–154.
Eason T. (2009) Emotional intelligence and nursing leadership: a
successful combination. Creative Nursing 15 (4), 184–185.
Enterkin J., Robb E. & McLaren S. (2013)Clinical leadership
for high-quality care:developing future ward leaders.Journal
of Nursing Management 21(2), 206–216.
ª 2014 John Wiley & Sons Ltd
752 Journal of Nursing Management, 2015, 23, 744–753
B. Heckemann etal.
Feather R.(2009)Emotionalintelligence in relation to nursing
leadership:doesit matter? Journalof Nursing Management
17 (3), 376–382.
Fook J., White S. & Gardner F. (2006) Critical reflection:a
review of contemporaryliteratureand understandings.In
Critical Reflection in Health and SocialCare (S. White, J.
Fook & F. Gardnereds),pp. 3–20. Open University Press,
Maidenhead, UK.
Freshman B. & Rubino L. (2002) Emotional intelligence:a core
competency for health care administrators.The Health Care
Manager 20 (4), 1–9.
Fuimano J. (2004)Raise your emotionalintelligence.Nursing
Management 35 (7), 10–12.
Goleman D.(1996) EmotionalIntelligence:Why It Can Matter
More Than IQ, new edn. Bloomsbury Publishing Plc, London.
Hendricks J.M., Cope V.C. & Harris M. (2010)A leadership
program in an undergraduate nursing course in Western Aus-
tralia: building leaders in our midst.Nurse Education Today
30 (3), 252–257.
Herbert R.& Edgar L. (2004) Emotionalintelligence:a primal
dimension of nursing leadership? Nursing Leadership 17 (4),
56–63.
Hoijer B. (2008) Ontological assumptions and generalizations in
qualitative (audience) research.European Journalof Commu-
nication 23 (3), 275–294.
Horton-Deutsch S. & Sherwood G. (2008) Reflection: an educa-
tional strategy to develop emotionally-competentnurse lead-
ers. Journal of Nursing Management 16 (8), 946–954.
Huang R. (2009)RQDA: R-based qualitative data analysis.R
package version 0.1-7. Available at: http://rqda.r-forge.r-
project.org/, accessed 29 May 2009.
InternationalCouncil of Nurses (ICN) (2010) Leadership for
Change:Background.[Online]. Available at:http://www.icn.
ch/pillarsprograms/background/, accessed 12 May 2011.
Jasper M. (2003) Beginning Reflective Practice:Foundations in
Nursing and Health Care, new edn. Nelson Thornes, Chelten-
ham, UK.
Kerfoot K. (1996)The emotionalside of leadership:the nurse
manager’s challenge. Nursing Economics 14 (1), 59–61.
Kreifelts B.,Ethofer T., Huberle E., Grodd W. & Wildgruber
D. (2010) Association of trait emotional intelligence and indi-
vidual fMRI-activation patternsduring the perceptionof
socialsignals from voice and face.Human Brain Mapping 31
(7), 979–991.
Krippendorff K. (2004) Content Analysis: An Introduction to its
Methodology,2nd edn. Sage Publications Inc, Thousand
Oaks, CA.
Lincoln Y. & Guba E.G. (1985)Naturalistic Inquiry,1st edn.
Sage Publications Inc, Newbury Park, CA.
Lucas V.,Laschinger H.K.& Wong C.A. (2008) The impact of
emotionalintelligent leadership on staff nurse empowerment:
the moderating effect ofspan of control.Journal of Nursing
Management 16 (8), 964–973.
MantzoukasS. & Jasper M.A. (2004)Reflective practice and
daily ward reality:a covertpower game.Journal of Clinical
Nursing 13 (8), 925–933.
Mayer J.D. & Salovey P. (1997) What is emotional intelligence?
In Emotional Developmentand Emotional Intelligence:
Implications for Educators (P.Salovey & D.Sluyter eds),pp.
3–31. Basic Books, New York, NY.
Mayer J.D., Salovey P. & Caruso D.R. (2004) Emotional intelli-
gence. Theory, findings and implications. Psychological
Inquiry 15 (3), 197–215.
Miller W.L. & Crabtree B.F. (1999a) Clinical research. In Doing
Qualitative Research,2nd edn (B.F.Crabtree & W.L. Miller
eds), pp. 3–32. Sage Publications Inc, Thousand Oaks, CA.
Miller W.L. & Crabtree B.F. (1999b)The dance ofinterpreta-
tion. In Doing Qualitative Research,2nd edn (B.F.Crabtree
& W.L. Miller eds), pp. 127–143. Sage, Thousand Oaks, CA.
Murphy L.G. (2012) Authentic leadership:becoming and
remaining an authentic nurse leader.The Journal of Nursing
Administration 42 (11), 507–512.
NHS Institute for Innovation and Improvement(2006).NHS
Leadership QualitiesFramework.Available at: http://www.
nipec.hscni.net/wardsister/docs/LQF.pdf, accessed 6 June 2013.
O’Boyle E.H. Jr, Humphrey R.H., Pollack J.M., Hawyer T.H.
& Story P.A. (2011)The relation between emotionalintelli-
gence and job performance: a meta-analysis. Journal of Orga-
nizational Behavior 32 (5), 788–818.
Piper L.E. (2005)Passion in today’shealth care leaders.The
Health Care Manager 24 (1), 44–47.
Porter-O’Grady T. (2003) A different age for leadership. Part 1:
new context,new content.JONA: The Journal of Nursing
Administration 33 (2), 105–110.
Prosser S. (2003) Emotional intelligence:an illuminating
approach. Professional Nurse 18 (6), 357.
Rolfe G., Freshwater D.& Jasper M. (2001) CriticalReflection
for Nursing and the Helping Professions: A User’s Guide. Pal-
grave Macmillan, Basingstoke.
Schulte M., Ree M. & Carretta T. (2004) Emotionalintelli-
gence:not much more than g and personality.Personality
and Individual Differences 37 (5), 1059–1068.
Snow J.L. (2001) Looking beyond nursing for clues to effective
leadership.JONA: The Journalof Nursing Administration 31
(9), 440–443.
Squires M., Tourangeau A., Spence Laschinger H.K. & Doran D.
(2010)The link between leadership and safety outcomesin
hospitals. Journal of Nursing Management 18 (8), 914–925.
Stichler J.F.(2006) Emotionalintelligence.A critical leadership
quality for the nurse executive.AWHONN Lifelines/Associa-
tion of Women’s Health,Obstetric and NeonatalNurses 10
(5), 422–425.
Tahan H. (2000) Emotionally intelligent case managers make a
difference. Lippincott’s Case Management: Managing the Pro-
cess of Patient Care 5 (4), 162–167.
Triola N. (2007) Authentic leadership beginswith emotional
intelligence. AACN Advanced Critical Care 18 (3), 244–247.
Udod S.A. & Care W.D. (2013) ‘Walking a tight rope’: an investi-
gation of nurse managers’work stressors and coping experi-
ences. Journal of Research in Nursing 18 (1), 67–79.
Vitello-Cicciu J.M. (2002) Exploring emotional intelligence.
Implicationsfor nursing leaders.The Journal of Nursing
Administration 32 (4), 203–210.
Vitello-Cicciu J.M. (2003)Innovative leadership through emo-
tional intelligence. Nursing Management 34 (10), 28–32.
Warriner S. (2009) Midwifery and nursing leadership in the
ever-changing NHS.British Journal of Midwifery 17 (12),
764–771.
Wright S. (2009) The realskills. Nursing Standard 24 (15–17),
24–25.
ª 2014 John Wiley & Sons Ltd
Journal of Nursing Management, 2015, 23, 744–753 753
Leading with emotionalintelligence
leadership:doesit matter? Journalof Nursing Management
17 (3), 376–382.
Fook J., White S. & Gardner F. (2006) Critical reflection:a
review of contemporaryliteratureand understandings.In
Critical Reflection in Health and SocialCare (S. White, J.
Fook & F. Gardnereds),pp. 3–20. Open University Press,
Maidenhead, UK.
Freshman B. & Rubino L. (2002) Emotional intelligence:a core
competency for health care administrators.The Health Care
Manager 20 (4), 1–9.
Fuimano J. (2004)Raise your emotionalintelligence.Nursing
Management 35 (7), 10–12.
Goleman D.(1996) EmotionalIntelligence:Why It Can Matter
More Than IQ, new edn. Bloomsbury Publishing Plc, London.
Hendricks J.M., Cope V.C. & Harris M. (2010)A leadership
program in an undergraduate nursing course in Western Aus-
tralia: building leaders in our midst.Nurse Education Today
30 (3), 252–257.
Herbert R.& Edgar L. (2004) Emotionalintelligence:a primal
dimension of nursing leadership? Nursing Leadership 17 (4),
56–63.
Hoijer B. (2008) Ontological assumptions and generalizations in
qualitative (audience) research.European Journalof Commu-
nication 23 (3), 275–294.
Horton-Deutsch S. & Sherwood G. (2008) Reflection: an educa-
tional strategy to develop emotionally-competentnurse lead-
ers. Journal of Nursing Management 16 (8), 946–954.
Huang R. (2009)RQDA: R-based qualitative data analysis.R
package version 0.1-7. Available at: http://rqda.r-forge.r-
project.org/, accessed 29 May 2009.
InternationalCouncil of Nurses (ICN) (2010) Leadership for
Change:Background.[Online]. Available at:http://www.icn.
ch/pillarsprograms/background/, accessed 12 May 2011.
Jasper M. (2003) Beginning Reflective Practice:Foundations in
Nursing and Health Care, new edn. Nelson Thornes, Chelten-
ham, UK.
Kerfoot K. (1996)The emotionalside of leadership:the nurse
manager’s challenge. Nursing Economics 14 (1), 59–61.
Kreifelts B.,Ethofer T., Huberle E., Grodd W. & Wildgruber
D. (2010) Association of trait emotional intelligence and indi-
vidual fMRI-activation patternsduring the perceptionof
socialsignals from voice and face.Human Brain Mapping 31
(7), 979–991.
Krippendorff K. (2004) Content Analysis: An Introduction to its
Methodology,2nd edn. Sage Publications Inc, Thousand
Oaks, CA.
Lincoln Y. & Guba E.G. (1985)Naturalistic Inquiry,1st edn.
Sage Publications Inc, Newbury Park, CA.
Lucas V.,Laschinger H.K.& Wong C.A. (2008) The impact of
emotionalintelligent leadership on staff nurse empowerment:
the moderating effect ofspan of control.Journal of Nursing
Management 16 (8), 964–973.
MantzoukasS. & Jasper M.A. (2004)Reflective practice and
daily ward reality:a covertpower game.Journal of Clinical
Nursing 13 (8), 925–933.
Mayer J.D. & Salovey P. (1997) What is emotional intelligence?
In Emotional Developmentand Emotional Intelligence:
Implications for Educators (P.Salovey & D.Sluyter eds),pp.
3–31. Basic Books, New York, NY.
Mayer J.D., Salovey P. & Caruso D.R. (2004) Emotional intelli-
gence. Theory, findings and implications. Psychological
Inquiry 15 (3), 197–215.
Miller W.L. & Crabtree B.F. (1999a) Clinical research. In Doing
Qualitative Research,2nd edn (B.F.Crabtree & W.L. Miller
eds), pp. 3–32. Sage Publications Inc, Thousand Oaks, CA.
Miller W.L. & Crabtree B.F. (1999b)The dance ofinterpreta-
tion. In Doing Qualitative Research,2nd edn (B.F.Crabtree
& W.L. Miller eds), pp. 127–143. Sage, Thousand Oaks, CA.
Murphy L.G. (2012) Authentic leadership:becoming and
remaining an authentic nurse leader.The Journal of Nursing
Administration 42 (11), 507–512.
NHS Institute for Innovation and Improvement(2006).NHS
Leadership QualitiesFramework.Available at: http://www.
nipec.hscni.net/wardsister/docs/LQF.pdf, accessed 6 June 2013.
O’Boyle E.H. Jr, Humphrey R.H., Pollack J.M., Hawyer T.H.
& Story P.A. (2011)The relation between emotionalintelli-
gence and job performance: a meta-analysis. Journal of Orga-
nizational Behavior 32 (5), 788–818.
Piper L.E. (2005)Passion in today’shealth care leaders.The
Health Care Manager 24 (1), 44–47.
Porter-O’Grady T. (2003) A different age for leadership. Part 1:
new context,new content.JONA: The Journal of Nursing
Administration 33 (2), 105–110.
Prosser S. (2003) Emotional intelligence:an illuminating
approach. Professional Nurse 18 (6), 357.
Rolfe G., Freshwater D.& Jasper M. (2001) CriticalReflection
for Nursing and the Helping Professions: A User’s Guide. Pal-
grave Macmillan, Basingstoke.
Schulte M., Ree M. & Carretta T. (2004) Emotionalintelli-
gence:not much more than g and personality.Personality
and Individual Differences 37 (5), 1059–1068.
Snow J.L. (2001) Looking beyond nursing for clues to effective
leadership.JONA: The Journalof Nursing Administration 31
(9), 440–443.
Squires M., Tourangeau A., Spence Laschinger H.K. & Doran D.
(2010)The link between leadership and safety outcomesin
hospitals. Journal of Nursing Management 18 (8), 914–925.
Stichler J.F.(2006) Emotionalintelligence.A critical leadership
quality for the nurse executive.AWHONN Lifelines/Associa-
tion of Women’s Health,Obstetric and NeonatalNurses 10
(5), 422–425.
Tahan H. (2000) Emotionally intelligent case managers make a
difference. Lippincott’s Case Management: Managing the Pro-
cess of Patient Care 5 (4), 162–167.
Triola N. (2007) Authentic leadership beginswith emotional
intelligence. AACN Advanced Critical Care 18 (3), 244–247.
Udod S.A. & Care W.D. (2013) ‘Walking a tight rope’: an investi-
gation of nurse managers’work stressors and coping experi-
ences. Journal of Research in Nursing 18 (1), 67–79.
Vitello-Cicciu J.M. (2002) Exploring emotional intelligence.
Implicationsfor nursing leaders.The Journal of Nursing
Administration 32 (4), 203–210.
Vitello-Cicciu J.M. (2003)Innovative leadership through emo-
tional intelligence. Nursing Management 34 (10), 28–32.
Warriner S. (2009) Midwifery and nursing leadership in the
ever-changing NHS.British Journal of Midwifery 17 (12),
764–771.
Wright S. (2009) The realskills. Nursing Standard 24 (15–17),
24–25.
ª 2014 John Wiley & Sons Ltd
Journal of Nursing Management, 2015, 23, 744–753 753
Leading with emotionalintelligence
1 out of 10
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.