Contemporary Debates: Health Inequalities and UK Government Policies
VerifiedAdded on 2023/01/05
|11
|2387
|31
Report
AI Summary
This report analyzes health inequalities in the UK, focusing on disparities in life expectancy and government policies. It begins with an introduction to contemporary debates in moral theory and then dives into health inequities, highlighting disparities in life expectancy between the most and least deprived regions. The report presents statistical data and graphs illustrating these inequalities, including differences in mortality rates and healthy life expectancy. It explores contributing factors such as smoking and obesity and examines government policies aimed at addressing these issues, including Sure Start, child poverty initiatives, Health Action Zones (HAZs), tax credits, Public Service Agreements (PSAs), and joined-up government approaches. The report evaluates the effectiveness of these policies and discusses the government's goals and strategies for reducing health disparities, concluding with an overview of cross-cutting reviews and the importance of shaping mainstream policies.
LC462 CONTEMPORARY
DEBATES
DEBATES
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
INTRODUCTION...........................................................................................................................2
MAIN BODY..................................................................................................................................2
CONCLUSION................................................................................................................................9
REFERENCES..............................................................................................................................10
1
MAIN BODY..................................................................................................................................2
CONCLUSION................................................................................................................................9
REFERENCES..............................................................................................................................10
1
INTRODUCTION
Contemporary Debates in Moral Theory is a set of recent essays discussing key problems in
current ethics and moral thought (Baker and et.al., 2018). The size is formed by eight key
questions, for each question triggering a pair of contrasting essays, summarising the most
significant and powerful reasons for each argument. In this assessment, student discusses Health
Inequalities which is a major worry in the UK and discusses the government approach to
addressing these inequalities. Health inequity is a disparity in the health status or availability of
health care services among different demographic class due to the social situations under which
person is born, develop, live , work and age. Health inequity is disproportionate and could have
been reduces by the correct mix of government initiatives.
MAIN BODY
Health inequalities among people or cultures are preventable and inadequate disparities in
health status. From 2014 to 2016, the extent of disparities or differences in life expectancy
amongst most and least deprived regions of England was 9.3 years for men and 7.3 years for
women. Higher mortality rates in the much more vulnerable regions of heart disease, lung cancer
and chronic respiratory disease compensate for almost a third of the overall life expectancy
difference for both sexes. Cigarettes and obesity are the primary possible causes for such
diseases. Though this incidence of tobacco in England has decreased, citizens in the much more
disadvantaged areas are still much more likely to drink or smoke than citizens in the lowest
wealth quintile.
There is also no indication that differences in life expectancy has declined in recent years.
In-equality in mortality rate for females has risen from 2001 to 2003 and for males, whereas
disparity has gone up and down over time, it stays the same in 2001 to 2003. The difference in
healthier life expectancy rate between most and least deprived parts of Europe was about 19
years for males and females among 2014 and 2016 (Government.UK, 2020). People who live in
its most vulnerable areas invest almost a third of the population in bad health, compared to just
around a sixth for all those living in low income areas. In-equality in life expectancy really hasn't
improved with either sex from 2011 to 2013.
These health inequalities occur as early with large inequalities in child health (Dutta, 2018).
In 2014 to 2016, kids in its most disadvantaged areas was twice as likely to have kids with
premature birth as children throughout the less deprived areas, and this disparity has not shifted
2
Contemporary Debates in Moral Theory is a set of recent essays discussing key problems in
current ethics and moral thought (Baker and et.al., 2018). The size is formed by eight key
questions, for each question triggering a pair of contrasting essays, summarising the most
significant and powerful reasons for each argument. In this assessment, student discusses Health
Inequalities which is a major worry in the UK and discusses the government approach to
addressing these inequalities. Health inequity is a disparity in the health status or availability of
health care services among different demographic class due to the social situations under which
person is born, develop, live , work and age. Health inequity is disproportionate and could have
been reduces by the correct mix of government initiatives.
MAIN BODY
Health inequalities among people or cultures are preventable and inadequate disparities in
health status. From 2014 to 2016, the extent of disparities or differences in life expectancy
amongst most and least deprived regions of England was 9.3 years for men and 7.3 years for
women. Higher mortality rates in the much more vulnerable regions of heart disease, lung cancer
and chronic respiratory disease compensate for almost a third of the overall life expectancy
difference for both sexes. Cigarettes and obesity are the primary possible causes for such
diseases. Though this incidence of tobacco in England has decreased, citizens in the much more
disadvantaged areas are still much more likely to drink or smoke than citizens in the lowest
wealth quintile.
There is also no indication that differences in life expectancy has declined in recent years.
In-equality in mortality rate for females has risen from 2001 to 2003 and for males, whereas
disparity has gone up and down over time, it stays the same in 2001 to 2003. The difference in
healthier life expectancy rate between most and least deprived parts of Europe was about 19
years for males and females among 2014 and 2016 (Government.UK, 2020). People who live in
its most vulnerable areas invest almost a third of the population in bad health, compared to just
around a sixth for all those living in low income areas. In-equality in life expectancy really hasn't
improved with either sex from 2011 to 2013.
These health inequalities occur as early with large inequalities in child health (Dutta, 2018).
In 2014 to 2016, kids in its most disadvantaged areas was twice as likely to have kids with
premature birth as children throughout the less deprived areas, and this disparity has not shifted
2
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
since 2010 to 2012. Recent statistics indicate that children in even the most impoverished areas
are much more than 3 significantly more likely to occur dental decay than children throughout
the least deprived backgrounds, while in-equality has decreased in absolute terms from the fiscal
year 2014 to 2015.
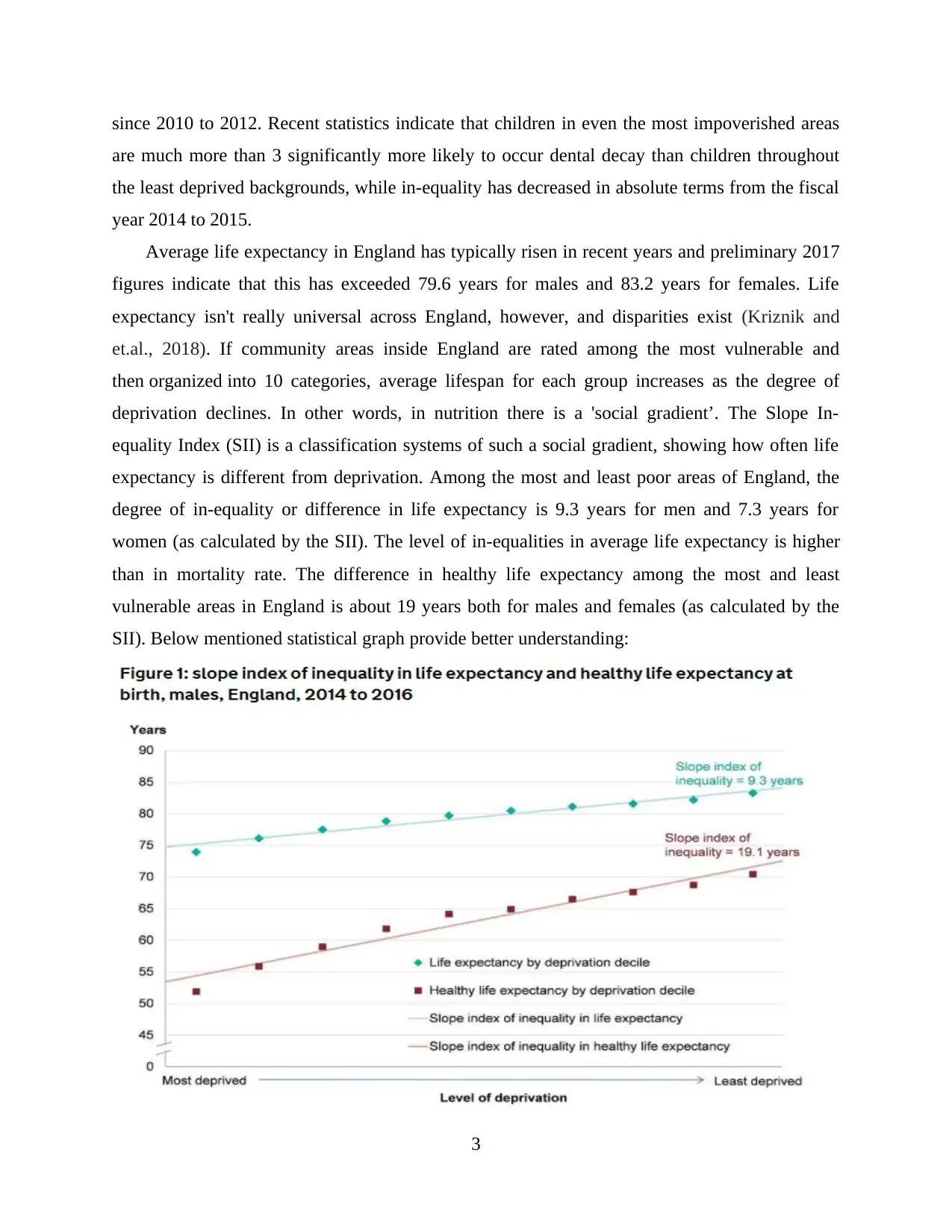
Average life expectancy in England has typically risen in recent years and preliminary 2017
figures indicate that this has exceeded 79.6 years for males and 83.2 years for females. Life
expectancy isn't really universal across England, however, and disparities exist (Kriznik and
et.al., 2018). If community areas inside England are rated among the most vulnerable and
then organized into 10 categories, average lifespan for each group increases as the degree of
deprivation declines. In other words, in nutrition there is a 'social gradient’. The Slope In-
equality Index (SII) is a classification systems of such a social gradient, showing how often life
expectancy is different from deprivation. Among the most and least poor areas of England, the
degree of in-equality or difference in life expectancy is 9.3 years for men and 7.3 years for
women (as calculated by the SII). The level of in-equalities in average life expectancy is higher
than in mortality rate. The difference in healthy life expectancy among the most and least
vulnerable areas in England is about 19 years both for males and females (as calculated by the
SII). Below mentioned statistical graph provide better understanding:
3
are much more than 3 significantly more likely to occur dental decay than children throughout
the least deprived backgrounds, while in-equality has decreased in absolute terms from the fiscal
year 2014 to 2015.
Average life expectancy in England has typically risen in recent years and preliminary 2017
figures indicate that this has exceeded 79.6 years for males and 83.2 years for females. Life
expectancy isn't really universal across England, however, and disparities exist (Kriznik and
et.al., 2018). If community areas inside England are rated among the most vulnerable and
then organized into 10 categories, average lifespan for each group increases as the degree of
deprivation declines. In other words, in nutrition there is a 'social gradient’. The Slope In-
equality Index (SII) is a classification systems of such a social gradient, showing how often life
expectancy is different from deprivation. Among the most and least poor areas of England, the
degree of in-equality or difference in life expectancy is 9.3 years for men and 7.3 years for
women (as calculated by the SII). The level of in-equalities in average life expectancy is higher
than in mortality rate. The difference in healthy life expectancy among the most and least
vulnerable areas in England is about 19 years both for males and females (as calculated by the
SII). Below mentioned statistical graph provide better understanding:
3
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
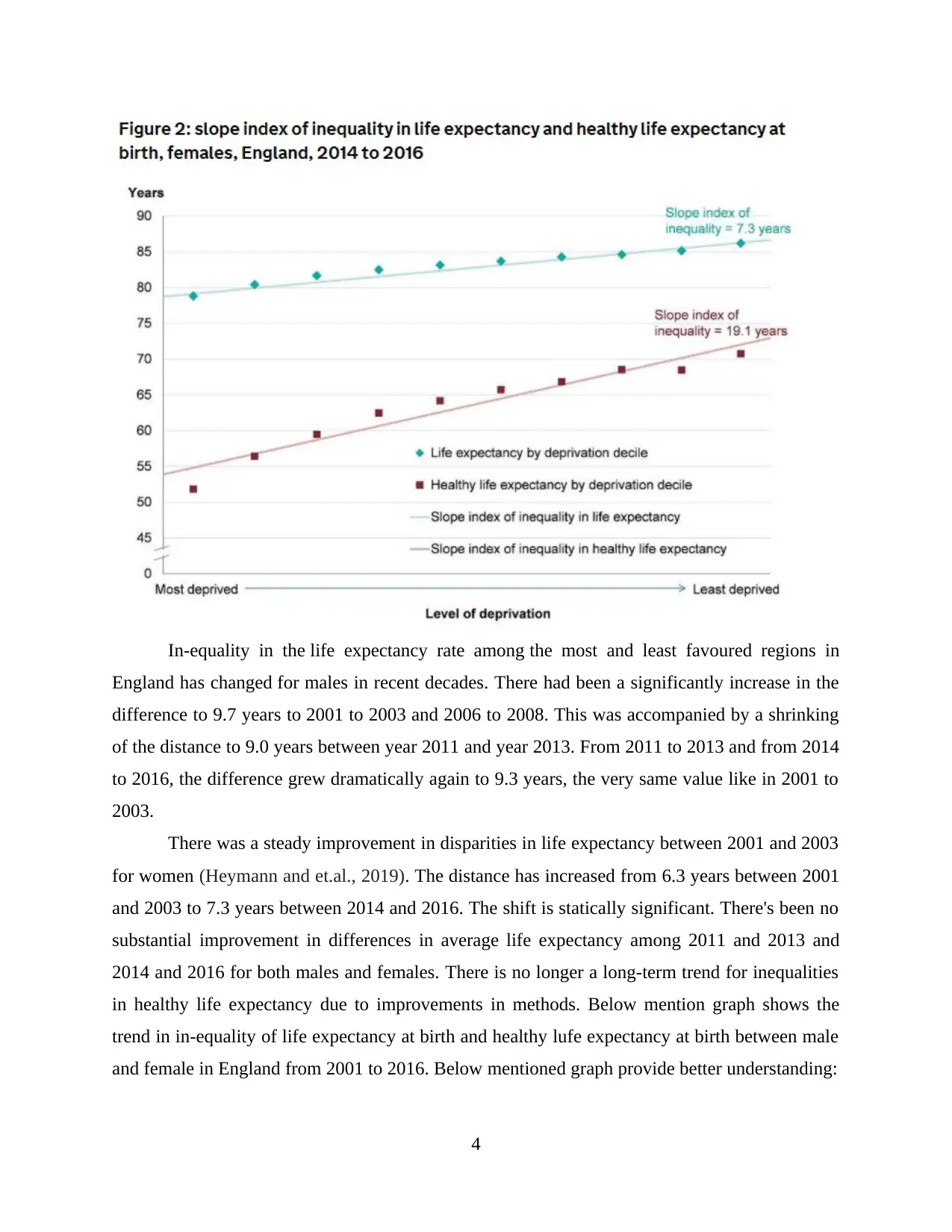
In-equality in the life expectancy rate among the most and least favoured regions in
England has changed for males in recent decades. There had been a significantly increase in the
difference to 9.7 years to 2001 to 2003 and 2006 to 2008. This was accompanied by a shrinking
of the distance to 9.0 years between year 2011 and year 2013. From 2011 to 2013 and from 2014
to 2016, the difference grew dramatically again to 9.3 years, the very same value like in 2001 to
2003.
There was a steady improvement in disparities in life expectancy between 2001 and 2003
for women (Heymann and et.al., 2019). The distance has increased from 6.3 years between 2001
and 2003 to 7.3 years between 2014 and 2016. The shift is statically significant. There's been no
substantial improvement in differences in average life expectancy among 2011 and 2013 and
2014 and 2016 for both males and females. There is no longer a long-term trend for inequalities
in healthy life expectancy due to improvements in methods. Below mention graph shows the
trend in in-equality of life expectancy at birth and healthy lufe expectancy at birth between male
and female in England from 2001 to 2016. Below mentioned graph provide better understanding:
4
England has changed for males in recent decades. There had been a significantly increase in the
difference to 9.7 years to 2001 to 2003 and 2006 to 2008. This was accompanied by a shrinking
of the distance to 9.0 years between year 2011 and year 2013. From 2011 to 2013 and from 2014
to 2016, the difference grew dramatically again to 9.3 years, the very same value like in 2001 to
2003.
There was a steady improvement in disparities in life expectancy between 2001 and 2003
for women (Heymann and et.al., 2019). The distance has increased from 6.3 years between 2001
and 2003 to 7.3 years between 2014 and 2016. The shift is statically significant. There's been no
substantial improvement in differences in average life expectancy among 2011 and 2013 and
2014 and 2016 for both males and females. There is no longer a long-term trend for inequalities
in healthy life expectancy due to improvements in methods. Below mention graph shows the
trend in in-equality of life expectancy at birth and healthy lufe expectancy at birth between male
and female in England from 2001 to 2016. Below mentioned graph provide better understanding:
4
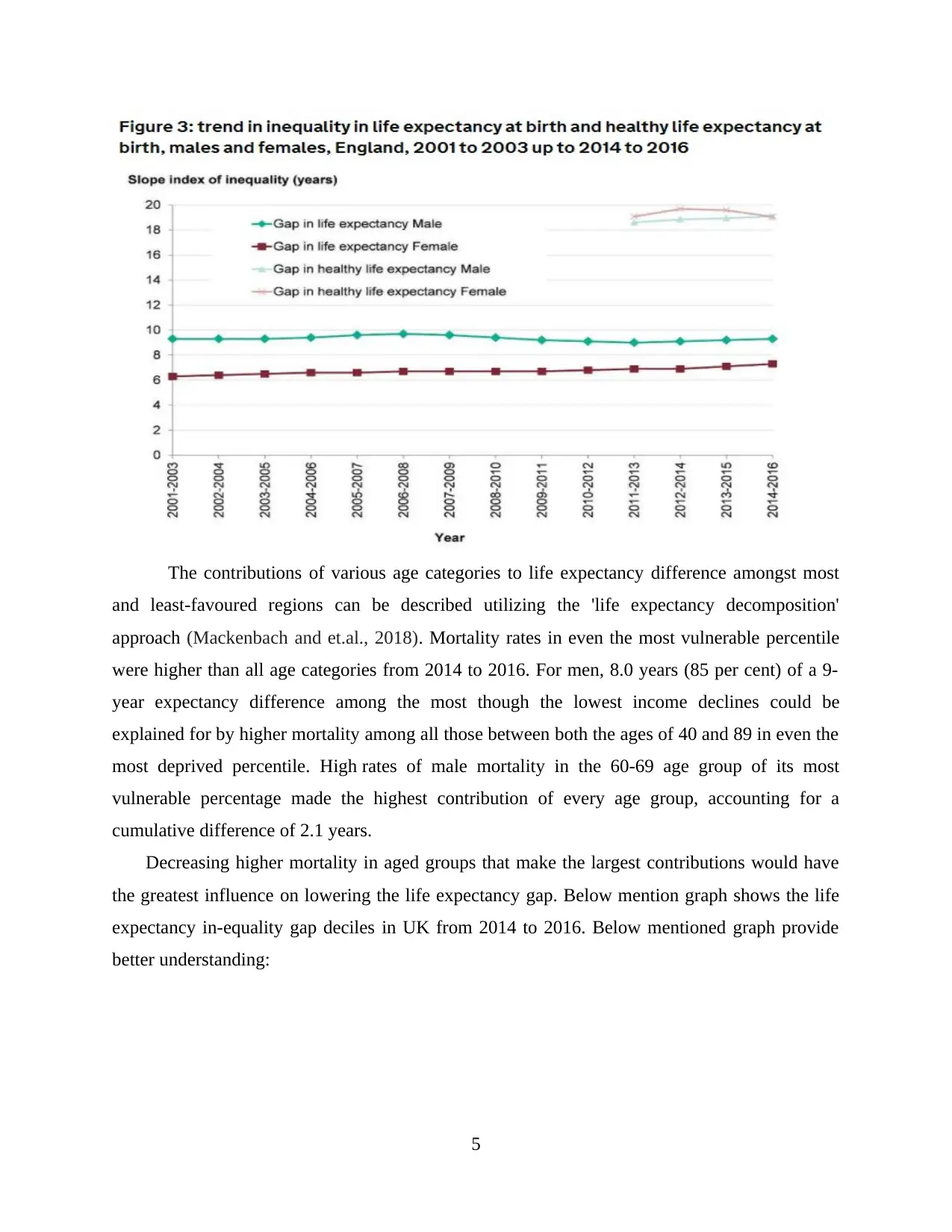
The contributions of various age categories to life expectancy difference amongst most
and least-favoured regions can be described utilizing the 'life expectancy decomposition'
approach (Mackenbach and et.al., 2018). Mortality rates in even the most vulnerable percentile
were higher than all age categories from 2014 to 2016. For men, 8.0 years (85 per cent) of a 9-
year expectancy difference among the most though the lowest income declines could be
explained for by higher mortality among all those between both the ages of 40 and 89 in even the
most deprived percentile. High rates of male mortality in the 60-69 age group of its most
vulnerable percentage made the highest contribution of every age group, accounting for a
cumulative difference of 2.1 years.
Decreasing higher mortality in aged groups that make the largest contributions would have
the greatest influence on lowering the life expectancy gap. Below mention graph shows the life
expectancy in-equality gap deciles in UK from 2014 to 2016. Below mentioned graph provide
better understanding:
5
and least-favoured regions can be described utilizing the 'life expectancy decomposition'
approach (Mackenbach and et.al., 2018). Mortality rates in even the most vulnerable percentile
were higher than all age categories from 2014 to 2016. For men, 8.0 years (85 per cent) of a 9-
year expectancy difference among the most though the lowest income declines could be
explained for by higher mortality among all those between both the ages of 40 and 89 in even the
most deprived percentile. High rates of male mortality in the 60-69 age group of its most
vulnerable percentage made the highest contribution of every age group, accounting for a
cumulative difference of 2.1 years.
Decreasing higher mortality in aged groups that make the largest contributions would have
the greatest influence on lowering the life expectancy gap. Below mention graph shows the life
expectancy in-equality gap deciles in UK from 2014 to 2016. Below mentioned graph provide
better understanding:
5
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
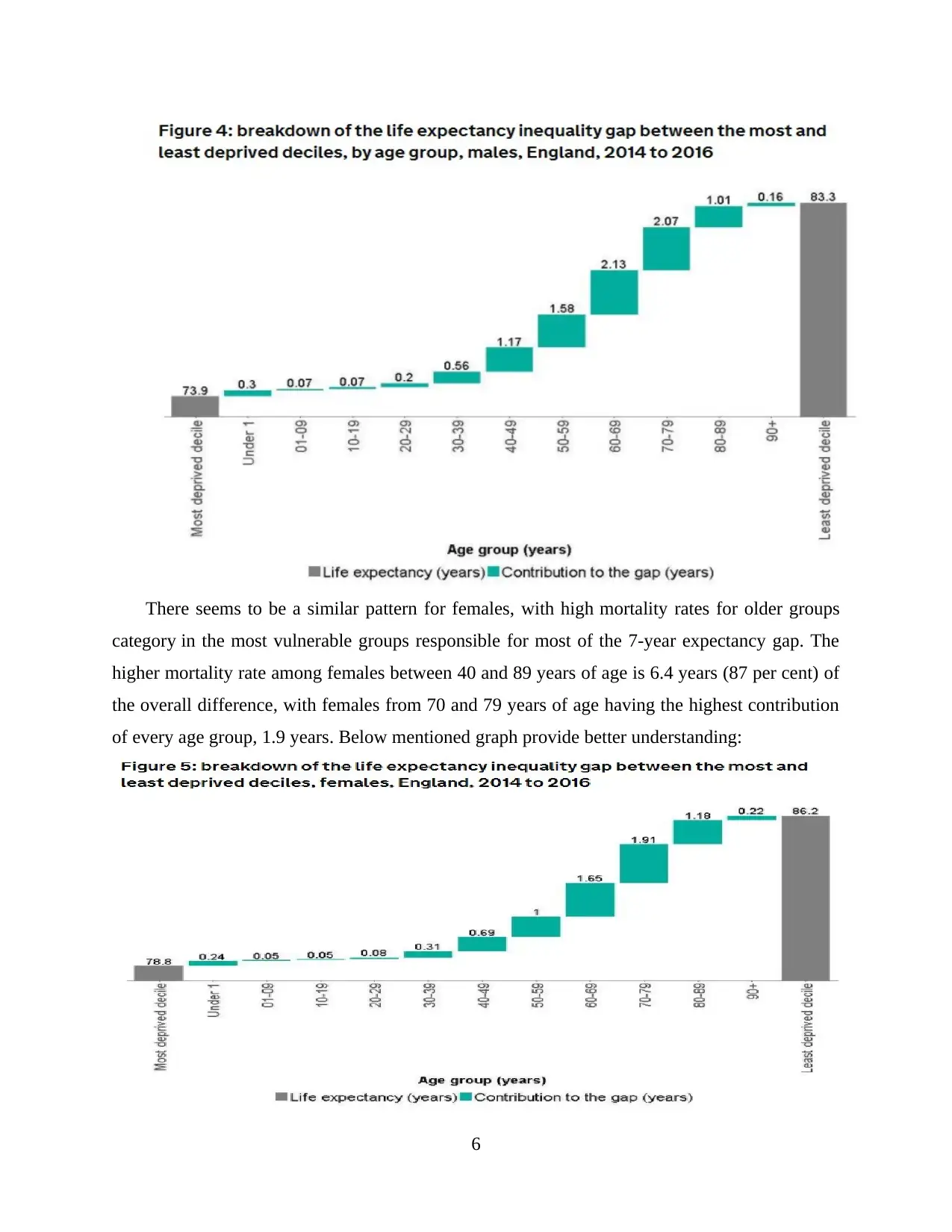
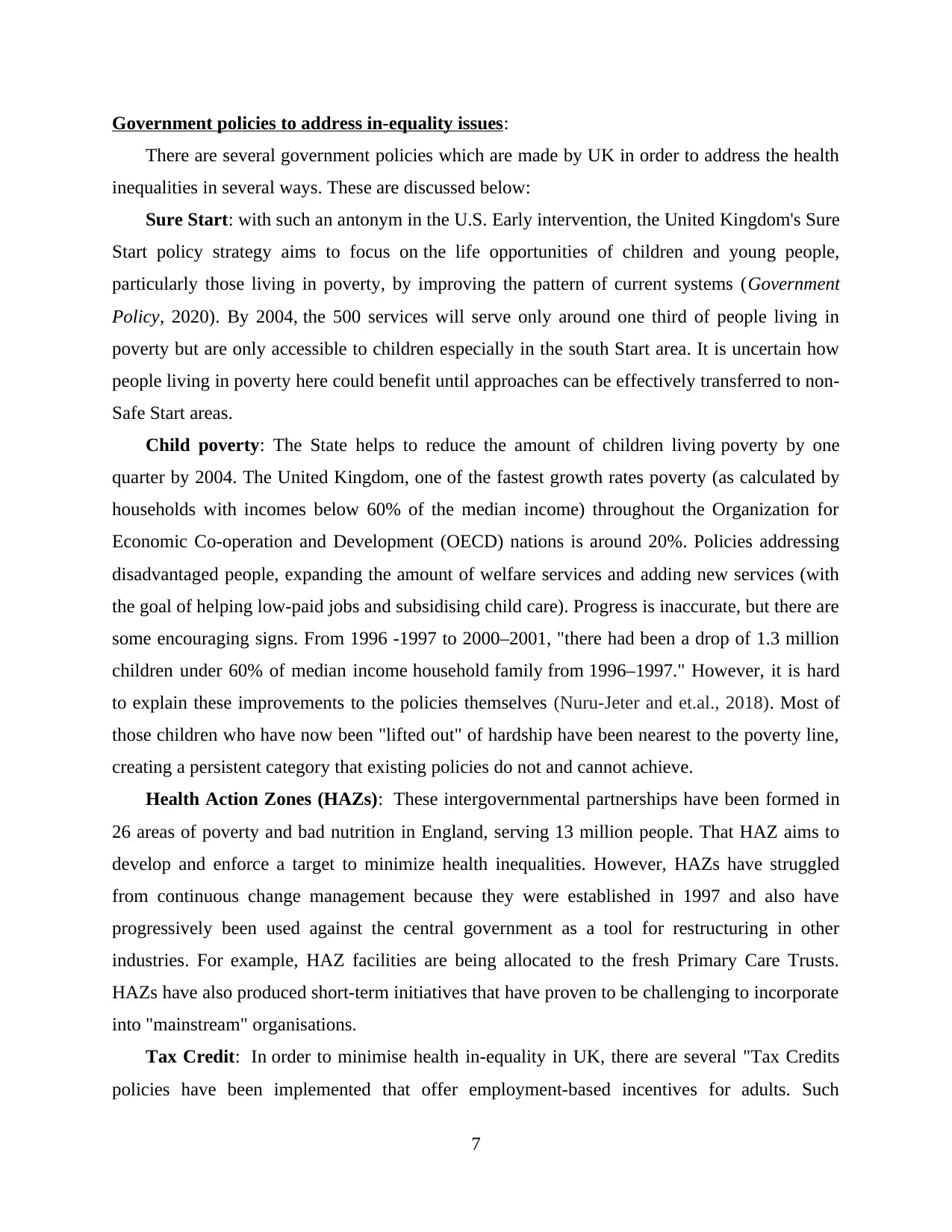
There seems to be a similar pattern for females, with high mortality rates for older groups
category in the most vulnerable groups responsible for most of the 7-year expectancy gap. The
higher mortality rate among females between 40 and 89 years of age is 6.4 years (87 per cent) of
the overall difference, with females from 70 and 79 years of age having the highest contribution
of every age group, 1.9 years. Below mentioned graph provide better understanding:
6
category in the most vulnerable groups responsible for most of the 7-year expectancy gap. The
higher mortality rate among females between 40 and 89 years of age is 6.4 years (87 per cent) of
the overall difference, with females from 70 and 79 years of age having the highest contribution
of every age group, 1.9 years. Below mentioned graph provide better understanding:
6
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Government policies to address in-equality issues:
There are several government policies which are made by UK in order to address the health
inequalities in several ways. These are discussed below:
Sure Start: with such an antonym in the U.S. Early intervention, the United Kingdom's Sure
Start policy strategy aims to focus on the life opportunities of children and young people,
particularly those living in poverty, by improving the pattern of current systems (Government
Policy, 2020). By 2004, the 500 services will serve only around one third of people living in
poverty but are only accessible to children especially in the south Start area. It is uncertain how
people living in poverty here could benefit until approaches can be effectively transferred to non-
Safe Start areas.
Child poverty: The State helps to reduce the amount of children living poverty by one
quarter by 2004. The United Kingdom, one of the fastest growth rates poverty (as calculated by
households with incomes below 60% of the median income) throughout the Organization for
Economic Co-operation and Development (OECD) nations is around 20%. Policies addressing
disadvantaged people, expanding the amount of welfare services and adding new services (with
the goal of helping low-paid jobs and subsidising child care). Progress is inaccurate, but there are
some encouraging signs. From 1996 -1997 to 2000–2001, "there had been a drop of 1.3 million
children under 60% of median income household family from 1996–1997." However, it is hard
to explain these improvements to the policies themselves (Nuru-Jeter and et.al., 2018). Most of
those children who have now been "lifted out" of hardship have been nearest to the poverty line,
creating a persistent category that existing policies do not and cannot achieve.
Health Action Zones (HAZs): These intergovernmental partnerships have been formed in
26 areas of poverty and bad nutrition in England, serving 13 million people. That HAZ aims to
develop and enforce a target to minimize health inequalities. However, HAZs have struggled
from continuous change management because they were established in 1997 and also have
progressively been used against the central government as a tool for restructuring in other
industries. For example, HAZ facilities are being allocated to the fresh Primary Care Trusts.
HAZs have also produced short-term initiatives that have proven to be challenging to incorporate
into "mainstream" organisations.
Tax Credit: In order to minimise health in-equality in UK, there are several "Tax Credits
policies have been implemented that offer employment-based incentives for adults. Such
7
There are several government policies which are made by UK in order to address the health
inequalities in several ways. These are discussed below:
Sure Start: with such an antonym in the U.S. Early intervention, the United Kingdom's Sure
Start policy strategy aims to focus on the life opportunities of children and young people,
particularly those living in poverty, by improving the pattern of current systems (Government
Policy, 2020). By 2004, the 500 services will serve only around one third of people living in
poverty but are only accessible to children especially in the south Start area. It is uncertain how
people living in poverty here could benefit until approaches can be effectively transferred to non-
Safe Start areas.
Child poverty: The State helps to reduce the amount of children living poverty by one
quarter by 2004. The United Kingdom, one of the fastest growth rates poverty (as calculated by
households with incomes below 60% of the median income) throughout the Organization for
Economic Co-operation and Development (OECD) nations is around 20%. Policies addressing
disadvantaged people, expanding the amount of welfare services and adding new services (with
the goal of helping low-paid jobs and subsidising child care). Progress is inaccurate, but there are
some encouraging signs. From 1996 -1997 to 2000–2001, "there had been a drop of 1.3 million
children under 60% of median income household family from 1996–1997." However, it is hard
to explain these improvements to the policies themselves (Nuru-Jeter and et.al., 2018). Most of
those children who have now been "lifted out" of hardship have been nearest to the poverty line,
creating a persistent category that existing policies do not and cannot achieve.
Health Action Zones (HAZs): These intergovernmental partnerships have been formed in
26 areas of poverty and bad nutrition in England, serving 13 million people. That HAZ aims to
develop and enforce a target to minimize health inequalities. However, HAZs have struggled
from continuous change management because they were established in 1997 and also have
progressively been used against the central government as a tool for restructuring in other
industries. For example, HAZ facilities are being allocated to the fresh Primary Care Trusts.
HAZs have also produced short-term initiatives that have proven to be challenging to incorporate
into "mainstream" organisations.
Tax Credit: In order to minimise health in-equality in UK, there are several "Tax Credits
policies have been implemented that offer employment-based incentives for adults. Such
7
as Working Families Tax Credit [WFTC] and Children's Tax Credits, It was similar to the U.S.
Earned Income Tax Credit and Child Tax Credit. This tax credits are connected with "New Deal"
programmes for single parent families and persons with disabilities which provide benefits
like child care costs or employment subsidies to allow certain groups to work. Their effect on
jobs is anticipated to be modest. For example, the WFTC is estimated to increase the rate of
employment of single mothers by 3%.
Public Service Agreement (PSA): It is a type of "contract" among both the spending
departments and finance ministry. Many departments include PSAs which might result in
significant declines in health inequalities, and that most have still not been designed with that in
mind (Iammarino, Rodríguez-Pose and Storper, 2019). PSA research highlights the need for such
a stronger link among policy (spending), results and for better transparency. The PSAs represent
the increasing role of ministry of finance in public policy.
Health Disparity goals: The Acheson Study did not propose goals for the elimination of
health disparities. In its plan for a public health policy, the government did not endorse "at this
point to set global objectives. Since the cause is complicated and several factors interact." Two
national goals were set in 2001 and these are discussed below:
"Beginning with child under one year, to decline the mortality gap among manual groups
and the community for everyone by at least 10% by 2010."
"Begin with health departments to minimize the difference among the fifth of the places
with the lower life expectancy and the population even more by at least 10% by 2010."
Joined-up government (JUG): In this policy, complex challenges are often multi-faceted,
and so government policies involve policymakers to work side by side through
department’s problems faced by other nations which have pursued solutions comparable to the
United Kingdom (Williams and Fullagar, 2019). While a "system-wide" approach to health in-
equality is helpful, JUG may often be inadequate. For example, policy development may include
several departments, but accountability for execution may reside with one department.
Conversely, financial redistribution policies could be less vulnerable to the problem of divided
government.
Cross-cutting Review: The Finance Ministry has developed cross-cutting assessments to
advise government expenditure in areas beyond the jurisdictions of spending divisions. Health
inequalities underwent a cross-cutting study in 2001. A group of public servants on all agencies
8
Earned Income Tax Credit and Child Tax Credit. This tax credits are connected with "New Deal"
programmes for single parent families and persons with disabilities which provide benefits
like child care costs or employment subsidies to allow certain groups to work. Their effect on
jobs is anticipated to be modest. For example, the WFTC is estimated to increase the rate of
employment of single mothers by 3%.
Public Service Agreement (PSA): It is a type of "contract" among both the spending
departments and finance ministry. Many departments include PSAs which might result in
significant declines in health inequalities, and that most have still not been designed with that in
mind (Iammarino, Rodríguez-Pose and Storper, 2019). PSA research highlights the need for such
a stronger link among policy (spending), results and for better transparency. The PSAs represent
the increasing role of ministry of finance in public policy.
Health Disparity goals: The Acheson Study did not propose goals for the elimination of
health disparities. In its plan for a public health policy, the government did not endorse "at this
point to set global objectives. Since the cause is complicated and several factors interact." Two
national goals were set in 2001 and these are discussed below:
"Beginning with child under one year, to decline the mortality gap among manual groups
and the community for everyone by at least 10% by 2010."
"Begin with health departments to minimize the difference among the fifth of the places
with the lower life expectancy and the population even more by at least 10% by 2010."
Joined-up government (JUG): In this policy, complex challenges are often multi-faceted,
and so government policies involve policymakers to work side by side through
department’s problems faced by other nations which have pursued solutions comparable to the
United Kingdom (Williams and Fullagar, 2019). While a "system-wide" approach to health in-
equality is helpful, JUG may often be inadequate. For example, policy development may include
several departments, but accountability for execution may reside with one department.
Conversely, financial redistribution policies could be less vulnerable to the problem of divided
government.
Cross-cutting Review: The Finance Ministry has developed cross-cutting assessments to
advise government expenditure in areas beyond the jurisdictions of spending divisions. Health
inequalities underwent a cross-cutting study in 2001. A group of public servants on all agencies
8
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

has examined research findings and government information sources. They recognized a need for
a long term government plan to resolve health in-equality and the value of shaping mainstream
policies in all aspects of government. They promoted a greater emphasis on marginalised
communities, better preventive health services, better diet and physical activity programmes, and
enhanced housing conditions. Released at the end of 2002, it would be too early to determine the
effects of the study.
CONCLUSION
From the above discussion it has been concluded that government policies has made
considerable strides, but has also faced considerable drawbacks. Having the subject on the policy
platform is a big move forward in itself. In addition, advancement has been achieved in policy-
making frameworks and mechanisms and in understanding the possible effect of all initiatives on
health regarding inequalities. Drawbacks are evident in scarce evidence of successful action,
minimal evidence of improvement in middle markers and results, weak efforts to continue JUG,
and inadequate incorporation of "health inequalities" policy within conventional structures.
These aspects in which improvement has been produced and the problems discussed offer
guidance for other countries in these policy efforts.
9
a long term government plan to resolve health in-equality and the value of shaping mainstream
policies in all aspects of government. They promoted a greater emphasis on marginalised
communities, better preventive health services, better diet and physical activity programmes, and
enhanced housing conditions. Released at the end of 2002, it would be too early to determine the
effects of the study.
CONCLUSION
From the above discussion it has been concluded that government policies has made
considerable strides, but has also faced considerable drawbacks. Having the subject on the policy
platform is a big move forward in itself. In addition, advancement has been achieved in policy-
making frameworks and mechanisms and in understanding the possible effect of all initiatives on
health regarding inequalities. Drawbacks are evident in scarce evidence of successful action,
minimal evidence of improvement in middle markers and results, weak efforts to continue JUG,
and inadequate incorporation of "health inequalities" policy within conventional structures.
These aspects in which improvement has been produced and the problems discussed offer
guidance for other countries in these policy efforts.
9
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
REFERENCES
Books & Journals
10
Books & Journals
10
1 out of 11
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.