Lifespan Nutrition: Sodium Intake
VerifiedAdded on 2022/11/13
|10
|2422
|319
AI Summary
This article discusses the impact of high sodium intake on children and adolescents' health. It provides information on the recommended nutrient reference values and dietary data collection methods. The article also includes a video presentation transcript and critical evaluation of three peer-reviewed studies.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: LIFESPAN NUTRITION: SODIUM INTAKE
LIFESPAN NUTRITION: SODIUM INTAKE
Name of the Student:
Name of the University:
Author note:
LIFESPAN NUTRITION: SODIUM INTAKE
Name of the Student:
Name of the University:
Author note:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1LIFESPAN NUTRITION: SODIUM INTAKE
Sodium Methodology
Recruitment and Interview
Families in Australia were reached out and contacted before eight days of the five phase
interview session. For children who are in the age group of 2 years or above, one adult was
selected and interviewed. Children and adolescents within the age group of 6 to 18 years were
personally interviewed with consent from their parents [1].
Measurement of Dietary Data
The dietary data was collected with the Automated Multiple-Pass Method (AMPM). The
first included participant interviews based on a 300 item food list to recall the beverages and
foods consumed within the last 24 hours. The second phase comprised of prompting the
participants to recall any foods which they had forgotten from a list of 6 food groups. The third
phase comprised of identifying the time of each meal consumption. The fourth phase comprised
of participants recalling from a 10, 000 food item list. The final probing phase consisted of
participants to finally recall any food which they had forgotten to report [2].
Effectiveness of Methodology
The AMPM is also used in the United States in nation-wide surveys such as the National
Health and Nutrition Examination Survey (NHANES) as well as in the 2003 to 2004 ‘What We
Eat in America’ survey [3]. The AMPM method is also in the United Kingdom as a part of the
measurement toolkit of Dietary, Anthropometry and Physical Activity (DAPA) data of the
National Health Service (NHS) [4].
Sodium Methodology
Recruitment and Interview
Families in Australia were reached out and contacted before eight days of the five phase
interview session. For children who are in the age group of 2 years or above, one adult was
selected and interviewed. Children and adolescents within the age group of 6 to 18 years were
personally interviewed with consent from their parents [1].
Measurement of Dietary Data
The dietary data was collected with the Automated Multiple-Pass Method (AMPM). The
first included participant interviews based on a 300 item food list to recall the beverages and
foods consumed within the last 24 hours. The second phase comprised of prompting the
participants to recall any foods which they had forgotten from a list of 6 food groups. The third
phase comprised of identifying the time of each meal consumption. The fourth phase comprised
of participants recalling from a 10, 000 food item list. The final probing phase consisted of
participants to finally recall any food which they had forgotten to report [2].
Effectiveness of Methodology
The AMPM is also used in the United States in nation-wide surveys such as the National
Health and Nutrition Examination Survey (NHANES) as well as in the 2003 to 2004 ‘What We
Eat in America’ survey [3]. The AMPM method is also in the United Kingdom as a part of the
measurement toolkit of Dietary, Anthropometry and Physical Activity (DAPA) data of the
National Health Service (NHS) [4].
2LIFESPAN NUTRITION: SODIUM INTAKE
Strengths and Limitations
Its strengths lies in its comprehensiveness and multiple probing methods. With five steps
and detailed databases, participants can correctly identify and recall the foods and beverages they
have consumed [5]. A key limitation, is survey bias. Participants may forget what they actually
consumed or feel the need to present themselves as ‘healthy’ resulting in incorrect responses or
‘under-reporting’. There is also no method for parents to validate the foods consumed by their
children outside home. The interview himself or herself may also be biased towards certain
families resulting in incorrect reporting [6].
Sodium Intake and Nutrient Reference Values
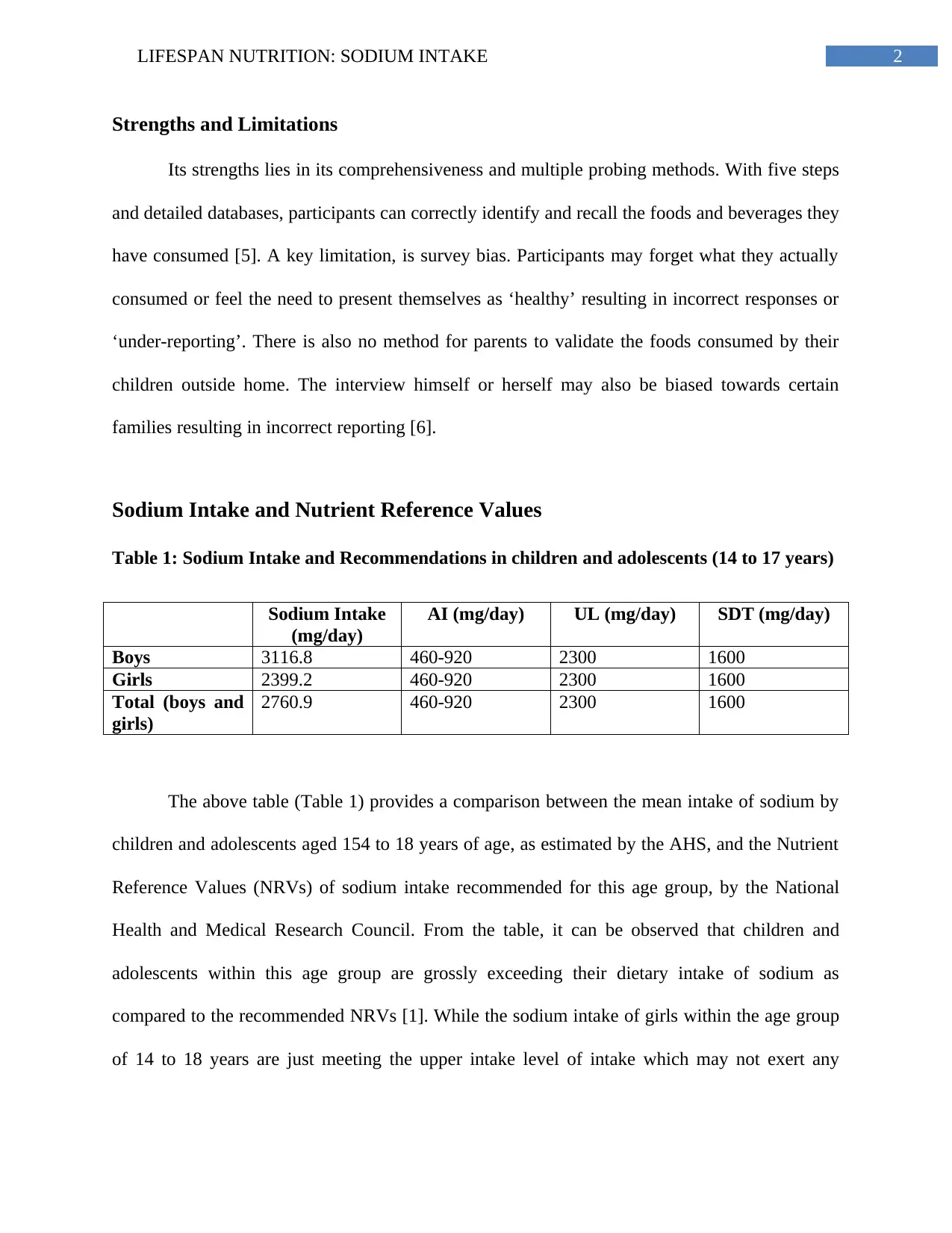
Table 1: Sodium Intake and Recommendations in children and adolescents (14 to 17 years)
Sodium Intake
(mg/day)
AI (mg/day) UL (mg/day) SDT (mg/day)
Boys 3116.8 460-920 2300 1600
Girls 2399.2 460-920 2300 1600
Total (boys and
girls)
2760.9 460-920 2300 1600
The above table (Table 1) provides a comparison between the mean intake of sodium by
children and adolescents aged 154 to 18 years of age, as estimated by the AHS, and the Nutrient
Reference Values (NRVs) of sodium intake recommended for this age group, by the National
Health and Medical Research Council. From the table, it can be observed that children and
adolescents within this age group are grossly exceeding their dietary intake of sodium as
compared to the recommended NRVs [1]. While the sodium intake of girls within the age group
of 14 to 18 years are just meeting the upper intake level of intake which may not exert any
Strengths and Limitations
Its strengths lies in its comprehensiveness and multiple probing methods. With five steps
and detailed databases, participants can correctly identify and recall the foods and beverages they
have consumed [5]. A key limitation, is survey bias. Participants may forget what they actually
consumed or feel the need to present themselves as ‘healthy’ resulting in incorrect responses or
‘under-reporting’. There is also no method for parents to validate the foods consumed by their
children outside home. The interview himself or herself may also be biased towards certain
families resulting in incorrect reporting [6].
Sodium Intake and Nutrient Reference Values
Table 1: Sodium Intake and Recommendations in children and adolescents (14 to 17 years)
Sodium Intake
(mg/day)
AI (mg/day) UL (mg/day) SDT (mg/day)
Boys 3116.8 460-920 2300 1600
Girls 2399.2 460-920 2300 1600
Total (boys and
girls)
2760.9 460-920 2300 1600
The above table (Table 1) provides a comparison between the mean intake of sodium by
children and adolescents aged 154 to 18 years of age, as estimated by the AHS, and the Nutrient
Reference Values (NRVs) of sodium intake recommended for this age group, by the National
Health and Medical Research Council. From the table, it can be observed that children and
adolescents within this age group are grossly exceeding their dietary intake of sodium as
compared to the recommended NRVs [1]. While the sodium intake of girls within the age group
of 14 to 18 years are just meeting the upper intake level of intake which may not exert any
3LIFESPAN NUTRITION: SODIUM INTAKE
adverse health effect, males and both females and females overall are exceeding their intake of
sodium across all levels, that is, AI, UI and SDT [7].
Such high intake of sodium in excess than the recommendations, can result in adverse
health implications. Excessive intake of sodium results in a condition of high blood pressure or
hypertension, which if left untreated, can increase the risk of acquiring cardiovascular risks in the
future, such as heart failure and stroke. Excessive sodium consumption also increases the future
susceptibility of calcium deficiency, osteoporosis and renal disorders [8].
Summary of Evidence
The first study which was selected, was the cross sectional research by [9], which aimed
to explore the association between intake of sodium and incidence of obesity among children and
adolescents of Korea. The subjects of the study comprised of the participants (10 – 18 years, n =
1467) from the Korean National Health and Nutrition Examination Survey (2010-2-11). Data on
sodium intake was collected using 24 hour recalls and ratio of sodium and creatinine in the urine.
Obesity was investigated using three anthropometric measurements, namely, total body fat
percentage (TBFP), waist circumference (WC) and body mass index (BMI). It was found that
participants with high sodium intake and urinary excretion had higher rates of BMI (Odds Ratio:
3.13, 95 % CI 1.8), of WC (OR 2.15, 95 % CI 1.27) and of TBFP (OR: 1.92, 95 % CI 1.29,
2.86).
The second study was also a cross sectional study by [10] which explored the association
between dietary intake of sodium and vascular health outcomes across children with type 1
diabetes mellitus (T1DM). The study participants comprised of 90 male children with an average
age of 13.6 years and with T1DM. Their sodium intake was estimated using the Australian Child
adverse health effect, males and both females and females overall are exceeding their intake of
sodium across all levels, that is, AI, UI and SDT [7].
Such high intake of sodium in excess than the recommendations, can result in adverse
health implications. Excessive intake of sodium results in a condition of high blood pressure or
hypertension, which if left untreated, can increase the risk of acquiring cardiovascular risks in the
future, such as heart failure and stroke. Excessive sodium consumption also increases the future
susceptibility of calcium deficiency, osteoporosis and renal disorders [8].
Summary of Evidence
The first study which was selected, was the cross sectional research by [9], which aimed
to explore the association between intake of sodium and incidence of obesity among children and
adolescents of Korea. The subjects of the study comprised of the participants (10 – 18 years, n =
1467) from the Korean National Health and Nutrition Examination Survey (2010-2-11). Data on
sodium intake was collected using 24 hour recalls and ratio of sodium and creatinine in the urine.
Obesity was investigated using three anthropometric measurements, namely, total body fat
percentage (TBFP), waist circumference (WC) and body mass index (BMI). It was found that
participants with high sodium intake and urinary excretion had higher rates of BMI (Odds Ratio:
3.13, 95 % CI 1.8), of WC (OR 2.15, 95 % CI 1.27) and of TBFP (OR: 1.92, 95 % CI 1.29,
2.86).
The second study was also a cross sectional study by [10] which explored the association
between dietary intake of sodium and vascular health outcomes across children with type 1
diabetes mellitus (T1DM). The study participants comprised of 90 male children with an average
age of 13.6 years and with T1DM. Their sodium intake was estimated using the Australian Child
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4LIFESPAN NUTRITION: SODIUM INTAKE
and Adolescent Eating Survey while glyceryl trinitrate mediated dilatation (GTN) and flow‐
mediated dilatation were used to evaluate the functioning of smooth and vascular endothelial
muscles. Levels of blood pressure were also estimated. A direct association was found between
high sodium intake and dysfunction of vascular smooth muscles (r = −0.31, p = .003). A positive
association was also observed between systolic blood pressure and consumption of sodium
(regression coefficient 2.4; 95% CI 0.5, 4.3; p = .01).
The third study by [11] explored the relationship between metabolic syndrome outcomes
and consumption of a Dietary Approaches to Stop Hypertension (DASH) diet across children
and adolescents. A food frequency questionnaire was used to collect dietary intake information
across 425 children and adolescents in the age group of 6 to 18 years. Metabolic syndrome
(MetS) was estimated based on the presence of waist circumference greater than the 90th
percentile of national reference curves, blood pressure greater than 90th percentile age, height
and sex and abnormal lipid profile (HDL cholesterol greater than 40 mg/dl, triglycerides greater
than 110mg/dl and fasting blood glucose greater than 100 mg/dl. The score of DASH diet intake
was based on 8 of its recommended dietary principles. The DASH diet score in the lowest
quartile (0.36, range 0.14=0.96) were associated with highest OR of MetS development(CI
95%). Increased engagement to DASH diet consumption was associated with lower levels of
blood sugar, blood pressure and blood cholesterol. (p < 0.05 for all).
Critical Evaluation
Three of the selected peer reviewed studies provided essential information on the
association between sodium intake and health outcome, such as the positive association between
high sodium intake and obesity, high sodium intake and metabolic syndrome and high sodium
and Adolescent Eating Survey while glyceryl trinitrate mediated dilatation (GTN) and flow‐
mediated dilatation were used to evaluate the functioning of smooth and vascular endothelial
muscles. Levels of blood pressure were also estimated. A direct association was found between
high sodium intake and dysfunction of vascular smooth muscles (r = −0.31, p = .003). A positive
association was also observed between systolic blood pressure and consumption of sodium
(regression coefficient 2.4; 95% CI 0.5, 4.3; p = .01).
The third study by [11] explored the relationship between metabolic syndrome outcomes
and consumption of a Dietary Approaches to Stop Hypertension (DASH) diet across children
and adolescents. A food frequency questionnaire was used to collect dietary intake information
across 425 children and adolescents in the age group of 6 to 18 years. Metabolic syndrome
(MetS) was estimated based on the presence of waist circumference greater than the 90th
percentile of national reference curves, blood pressure greater than 90th percentile age, height
and sex and abnormal lipid profile (HDL cholesterol greater than 40 mg/dl, triglycerides greater
than 110mg/dl and fasting blood glucose greater than 100 mg/dl. The score of DASH diet intake
was based on 8 of its recommended dietary principles. The DASH diet score in the lowest
quartile (0.36, range 0.14=0.96) were associated with highest OR of MetS development(CI
95%). Increased engagement to DASH diet consumption was associated with lower levels of
blood sugar, blood pressure and blood cholesterol. (p < 0.05 for all).
Critical Evaluation
Three of the selected peer reviewed studies provided essential information on the
association between sodium intake and health outcome, such as the positive association between
high sodium intake and obesity, high sodium intake and metabolic syndrome and high sodium
5LIFESPAN NUTRITION: SODIUM INTAKE
intake and vascular muscle dysfunction [9],[10],[11]. Despite three of the studies providing
information on sodium intake impact on children and adolescent health, cross sectional study
was the common research design used by all. Since cross sectional studies measure data at a
specific time point, its results may not be as valid as long term data collection periods,
characteristic of cohort studies or randomized controlled trials [12]. Further, dietary recalls and
food frequency questionnaires were the common dietary data collection method used by all,
which again is a limitation in terms of data validity due to high possibility of participant and
interviewer bias as well as forgetfulness [13]. The lack of randomization (one of the strongest
methods for conducting valid evidence based research), blinding and allocation concealment
moreover further increases the possibility of bias, statistical insignificance and statistical error in
the results obtained from all studies [14].
A major strength of the study by [9] however, was the extensively large sample size,
which reduces the impact of statistical errors and enhances reliability. However, the usage of a
spot urine analysis method rather than gold standard methods of 24 hours urine analysis, is again
a key limitation in terms of reliability. A major strength of the study by [10] is the usage of flow‐
mediated dilatation and glyceryl trinitrate mediated dilatation methods which are more accurate
and comprehensive methods of analyzing endothelial functioning as compared to blood
parameters. The relatively small sample size and the prevalence of males, are major limitations
in terms of lack of applicability, generalization and internal validity. The large sample size and
the broad range of the age group of participants selected in the study by [11] is a major strength
in comparison to the other two studies in terms of reliability, applicability and reduction of
statistical error. However, it must be noted that sample comprised of ‘healthy’ subjects and
hence, data reflecting positive association between DASH diet consumption and healthy blood
intake and vascular muscle dysfunction [9],[10],[11]. Despite three of the studies providing
information on sodium intake impact on children and adolescent health, cross sectional study
was the common research design used by all. Since cross sectional studies measure data at a
specific time point, its results may not be as valid as long term data collection periods,
characteristic of cohort studies or randomized controlled trials [12]. Further, dietary recalls and
food frequency questionnaires were the common dietary data collection method used by all,
which again is a limitation in terms of data validity due to high possibility of participant and
interviewer bias as well as forgetfulness [13]. The lack of randomization (one of the strongest
methods for conducting valid evidence based research), blinding and allocation concealment
moreover further increases the possibility of bias, statistical insignificance and statistical error in
the results obtained from all studies [14].
A major strength of the study by [9] however, was the extensively large sample size,
which reduces the impact of statistical errors and enhances reliability. However, the usage of a
spot urine analysis method rather than gold standard methods of 24 hours urine analysis, is again
a key limitation in terms of reliability. A major strength of the study by [10] is the usage of flow‐
mediated dilatation and glyceryl trinitrate mediated dilatation methods which are more accurate
and comprehensive methods of analyzing endothelial functioning as compared to blood
parameters. The relatively small sample size and the prevalence of males, are major limitations
in terms of lack of applicability, generalization and internal validity. The large sample size and
the broad range of the age group of participants selected in the study by [11] is a major strength
in comparison to the other two studies in terms of reliability, applicability and reduction of
statistical error. However, it must be noted that sample comprised of ‘healthy’ subjects and
hence, data reflecting positive association between DASH diet consumption and healthy blood
6LIFESPAN NUTRITION: SODIUM INTAKE
pressure and lipid profiles may not be accurate but rather a reflection of long term consumption
of foods in the participants’ household.
Video Presentation: Transcript
In a shocking report, the findings of the Australian Health Survey (AHS) indicate that
excessively high consumption of sodium across Australian children and adolescents.
Using a 5 phase Automated Pass Method, the survey collected information on the types
of foods consumed by children and adolescents, since the last 24 hours. The data reported that
the average consumption of sodium in boys (3116.8 mg/day), girls (2399.2 mg/day) and overall
children and adolescents aged between 14 to 18 years of age (2760.9 mg/day) were much higher
than the recommended NRVs of adequate intake (460-920 mg/day), upper limit intake (2300
mg/day) and suggested dietary intake of sodium (2300 mg/day).
High sodium intake has been linked to high blood pressure and risk of heart attacks and
strokes in the future. Children and adolescents must follow a diet and exercise plan as per the
Recommended Dietary and Physical Activity Guidelines set by the Department of Health.
pressure and lipid profiles may not be accurate but rather a reflection of long term consumption
of foods in the participants’ household.
Video Presentation: Transcript
In a shocking report, the findings of the Australian Health Survey (AHS) indicate that
excessively high consumption of sodium across Australian children and adolescents.
Using a 5 phase Automated Pass Method, the survey collected information on the types
of foods consumed by children and adolescents, since the last 24 hours. The data reported that
the average consumption of sodium in boys (3116.8 mg/day), girls (2399.2 mg/day) and overall
children and adolescents aged between 14 to 18 years of age (2760.9 mg/day) were much higher
than the recommended NRVs of adequate intake (460-920 mg/day), upper limit intake (2300
mg/day) and suggested dietary intake of sodium (2300 mg/day).
High sodium intake has been linked to high blood pressure and risk of heart attacks and
strokes in the future. Children and adolescents must follow a diet and exercise plan as per the
Recommended Dietary and Physical Activity Guidelines set by the Department of Health.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7LIFESPAN NUTRITION: SODIUM INTAKE
References
1. Australian Bureau of Statistics. Australian Health Survey: Nutrition First Results – Food
and Nutrients, 2011-12 [Internet]. Ausstats.abs.gov.au. 2019 [cited 31 July 2019].
Available from:
https://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/4683FD7315DFDFDBCA257D
080014F9E0/$File/australian%20health%20survey%20nutrition%20first%20results%20-
%20food%20and%20nutrients,%202011-12.pdf.
2. Australian Bureau of Statistics. 4363.0.55.001 - Australian Health Survey: Users' Guide,
2011-13 [Internet]. Abs.gov.au. 2019 [cited 31 July 2019]. Available from:
https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/4363.0.55.001Chapter65022011-13.
3. United States Department of Agriculture. AMPM - USDA Automated Multiple-Pass
Method : USDA ARS [Internet]. Ars.usda.gov. 2019 [cited 31 July 2019]. Available
from: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-
nutrition-research-center/food-surveys-research-group/docs/ampm-usda-automated-
multiple-pass-method/.
4. National Health Service. DAPA Measurement Toolkit [Internet]. Dapa-toolkit.mrc.ac.uk.
2019 [cited 31 July 2019]. Available from: https://dapa-toolkit.mrc.ac.uk/diet/subjective-
methods/24-hour-dietary-recall.
5. Hewawitharana SC, Thompson FE, Loria CM, Strauss W, Nagaraja J, Ritchie L, Webb
KL. Comparison of the NHANES dietary screener questionnaire to the Automated Self-
Administered 24-Hour Recall for Children in the Healthy Communities Study. Nutrition
journal. 2018 Dec;17(1):111.
References
1. Australian Bureau of Statistics. Australian Health Survey: Nutrition First Results – Food
and Nutrients, 2011-12 [Internet]. Ausstats.abs.gov.au. 2019 [cited 31 July 2019].
Available from:
https://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/4683FD7315DFDFDBCA257D
080014F9E0/$File/australian%20health%20survey%20nutrition%20first%20results%20-
%20food%20and%20nutrients,%202011-12.pdf.
2. Australian Bureau of Statistics. 4363.0.55.001 - Australian Health Survey: Users' Guide,
2011-13 [Internet]. Abs.gov.au. 2019 [cited 31 July 2019]. Available from:
https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/4363.0.55.001Chapter65022011-13.
3. United States Department of Agriculture. AMPM - USDA Automated Multiple-Pass
Method : USDA ARS [Internet]. Ars.usda.gov. 2019 [cited 31 July 2019]. Available
from: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-
nutrition-research-center/food-surveys-research-group/docs/ampm-usda-automated-
multiple-pass-method/.
4. National Health Service. DAPA Measurement Toolkit [Internet]. Dapa-toolkit.mrc.ac.uk.
2019 [cited 31 July 2019]. Available from: https://dapa-toolkit.mrc.ac.uk/diet/subjective-
methods/24-hour-dietary-recall.
5. Hewawitharana SC, Thompson FE, Loria CM, Strauss W, Nagaraja J, Ritchie L, Webb
KL. Comparison of the NHANES dietary screener questionnaire to the Automated Self-
Administered 24-Hour Recall for Children in the Healthy Communities Study. Nutrition
journal. 2018 Dec;17(1):111.
8LIFESPAN NUTRITION: SODIUM INTAKE
6. Thompson FE, Subar AF. Dietary assessment methodology. InNutrition in the Prevention
and Treatment of Disease 2017 Jan 1 (pp. 5-48). Academic Press.
7. National Health and Medical Research Council. NUTRIENT REFERENCE VALUES
FOR AUSTRALIA AND NEW ZEALAND [Internet]. Nhmrc.gov.au. 2019 [cited 31
July 2019]. Available from: https://www.nhmrc.gov.au/sites/default/files/images/nutrient-
refererence-dietary-intakes.pdf.
8. Yang Q, Zhang Z, Kuklina EV, Fang J, Ayala C, Hong Y, Loustalot F, Dai S, Gunn JP,
Tian N, Cogswell ME. Sodium intake and blood pressure among US children and
adolescents. Pediatrics. 2012 Oct 1;130(4):611-9.
9. Lee SK, Kim MK. Relationship of sodium intake with obesity among Korean children
and adolescents: Korea National Health and Nutrition Examination Survey. British
Journal of Nutrition. 2016 Mar;115(5):834-41.
10. Anderson J, Couper JJ, Toome S, Mpundu‐Kaambwa C, Giles LC, Gent R, Coppin B,
Peña AS. Dietary sodium intake relates to vascular health in children with type 1
diabetes. Pediatric diabetes. 2018 Feb;19(1):138-42.
11. Asghari G, Yuzbashian E, Mirmiran P, Hooshmand F, Najafi R, Azizi F. Dietary
approaches to stop hypertension (DASH) dietary pattern is associated with reduced
incidence of metabolic syndrome in children and adolescents. The Journal of pediatrics.
2016 Jul 1;174:178-84.
12. Watson R. Quantitative research. Nursing Standard (2014+). 2015 Apr 1;29(31):44.
13. Knüppel S, Norman K, Boeing H. Is a Single 24-hour Dietary Recall per Person
Sufficient to Estimate the Population Distribution of Usual Dietary Intake?. The Journal
of nutrition. 2019 Jun 7.
6. Thompson FE, Subar AF. Dietary assessment methodology. InNutrition in the Prevention
and Treatment of Disease 2017 Jan 1 (pp. 5-48). Academic Press.
7. National Health and Medical Research Council. NUTRIENT REFERENCE VALUES
FOR AUSTRALIA AND NEW ZEALAND [Internet]. Nhmrc.gov.au. 2019 [cited 31
July 2019]. Available from: https://www.nhmrc.gov.au/sites/default/files/images/nutrient-
refererence-dietary-intakes.pdf.
8. Yang Q, Zhang Z, Kuklina EV, Fang J, Ayala C, Hong Y, Loustalot F, Dai S, Gunn JP,
Tian N, Cogswell ME. Sodium intake and blood pressure among US children and
adolescents. Pediatrics. 2012 Oct 1;130(4):611-9.
9. Lee SK, Kim MK. Relationship of sodium intake with obesity among Korean children
and adolescents: Korea National Health and Nutrition Examination Survey. British
Journal of Nutrition. 2016 Mar;115(5):834-41.
10. Anderson J, Couper JJ, Toome S, Mpundu‐Kaambwa C, Giles LC, Gent R, Coppin B,
Peña AS. Dietary sodium intake relates to vascular health in children with type 1
diabetes. Pediatric diabetes. 2018 Feb;19(1):138-42.
11. Asghari G, Yuzbashian E, Mirmiran P, Hooshmand F, Najafi R, Azizi F. Dietary
approaches to stop hypertension (DASH) dietary pattern is associated with reduced
incidence of metabolic syndrome in children and adolescents. The Journal of pediatrics.
2016 Jul 1;174:178-84.
12. Watson R. Quantitative research. Nursing Standard (2014+). 2015 Apr 1;29(31):44.
13. Knüppel S, Norman K, Boeing H. Is a Single 24-hour Dietary Recall per Person
Sufficient to Estimate the Population Distribution of Usual Dietary Intake?. The Journal
of nutrition. 2019 Jun 7.

9LIFESPAN NUTRITION: SODIUM INTAKE
14. Rosenberger WF, Lachin JM. Randomization in clinical trials: theory and practice. John
Wiley & Sons; 2015 Nov 23.
14. Rosenberger WF, Lachin JM. Randomization in clinical trials: theory and practice. John
Wiley & Sons; 2015 Nov 23.
1 out of 10
Related Documents



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.