Nur720: Literature Review on Dementia Palliative Care Challenges
VerifiedAdded on 2022/08/30
|30
|6463
|26
Literature Review
AI Summary
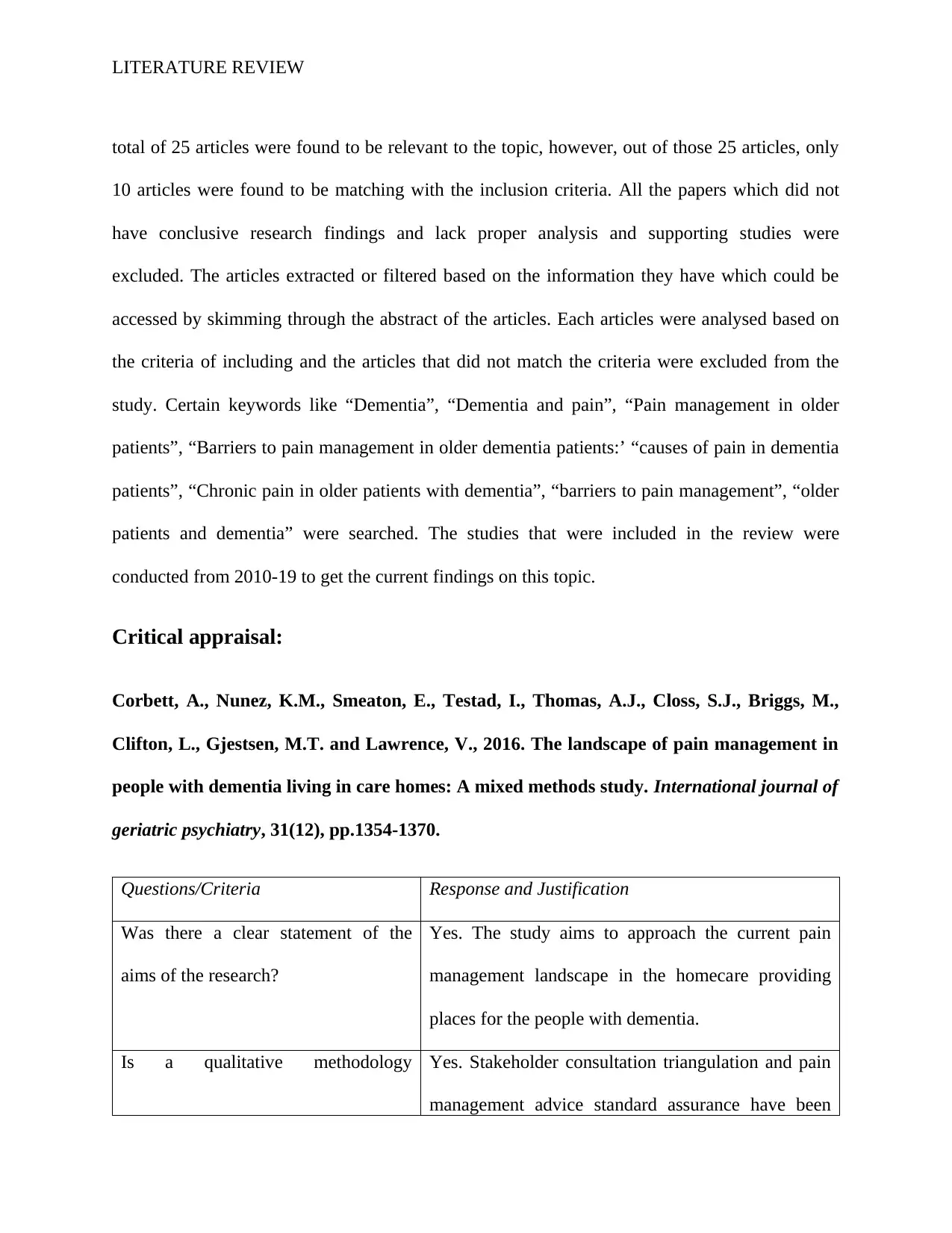
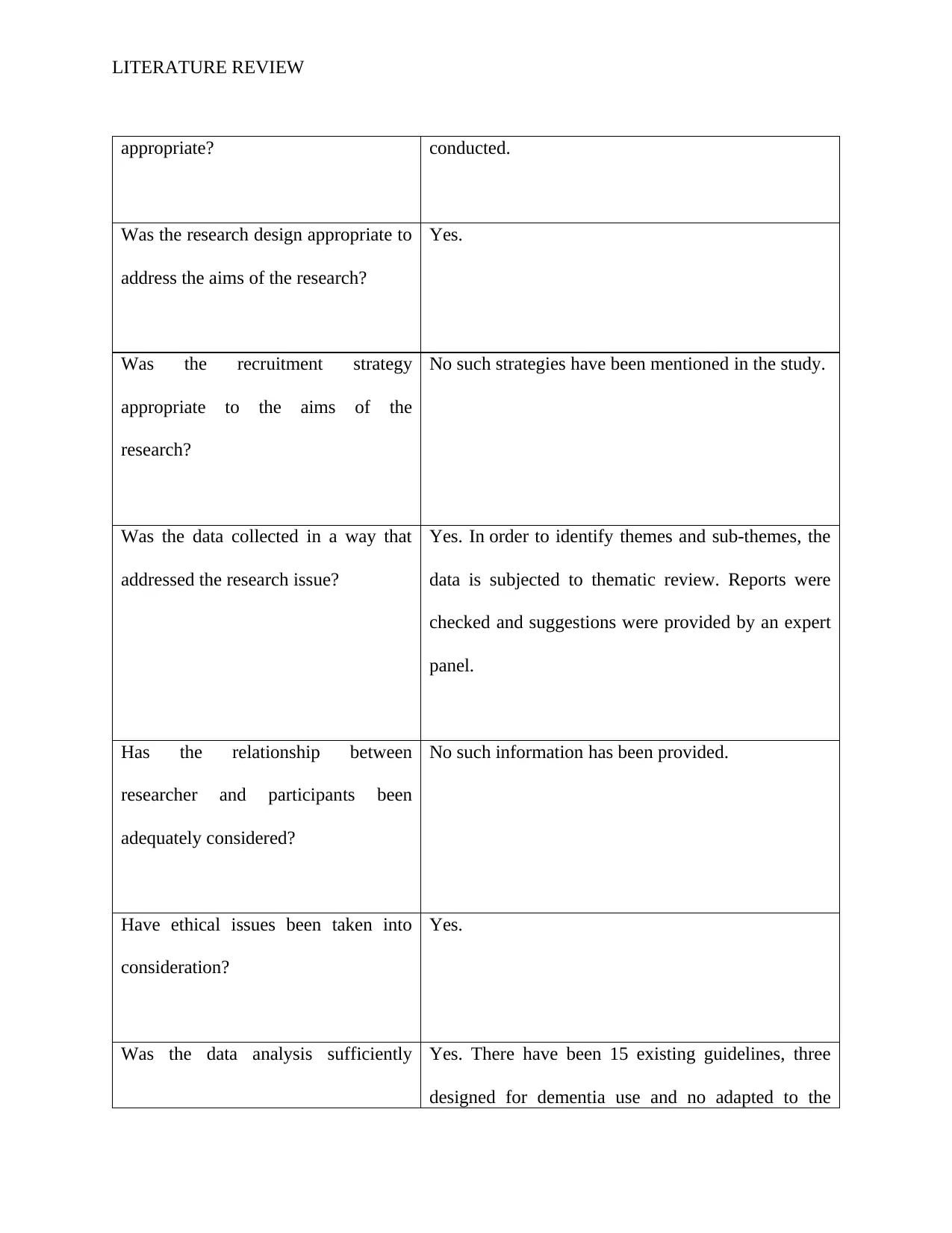
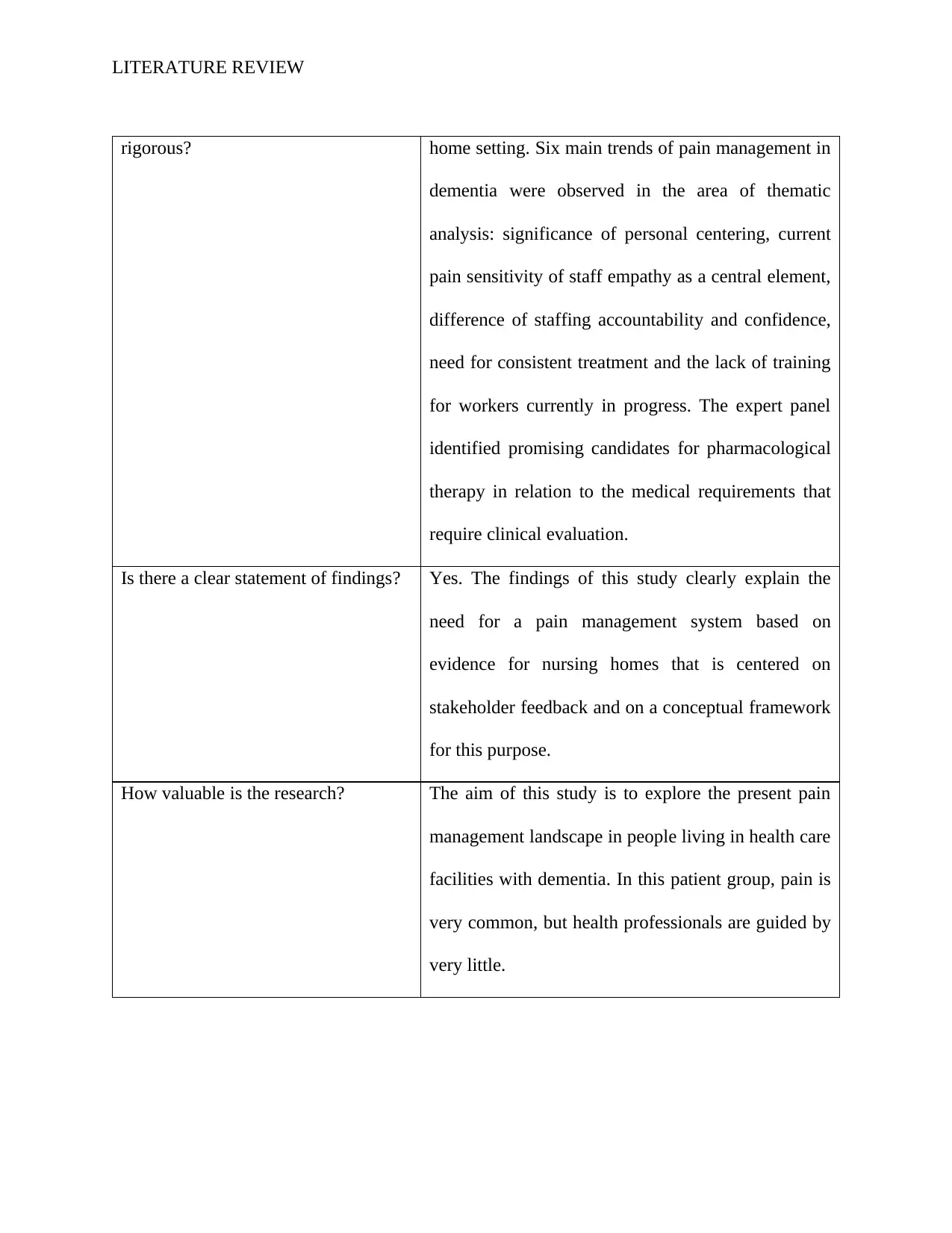
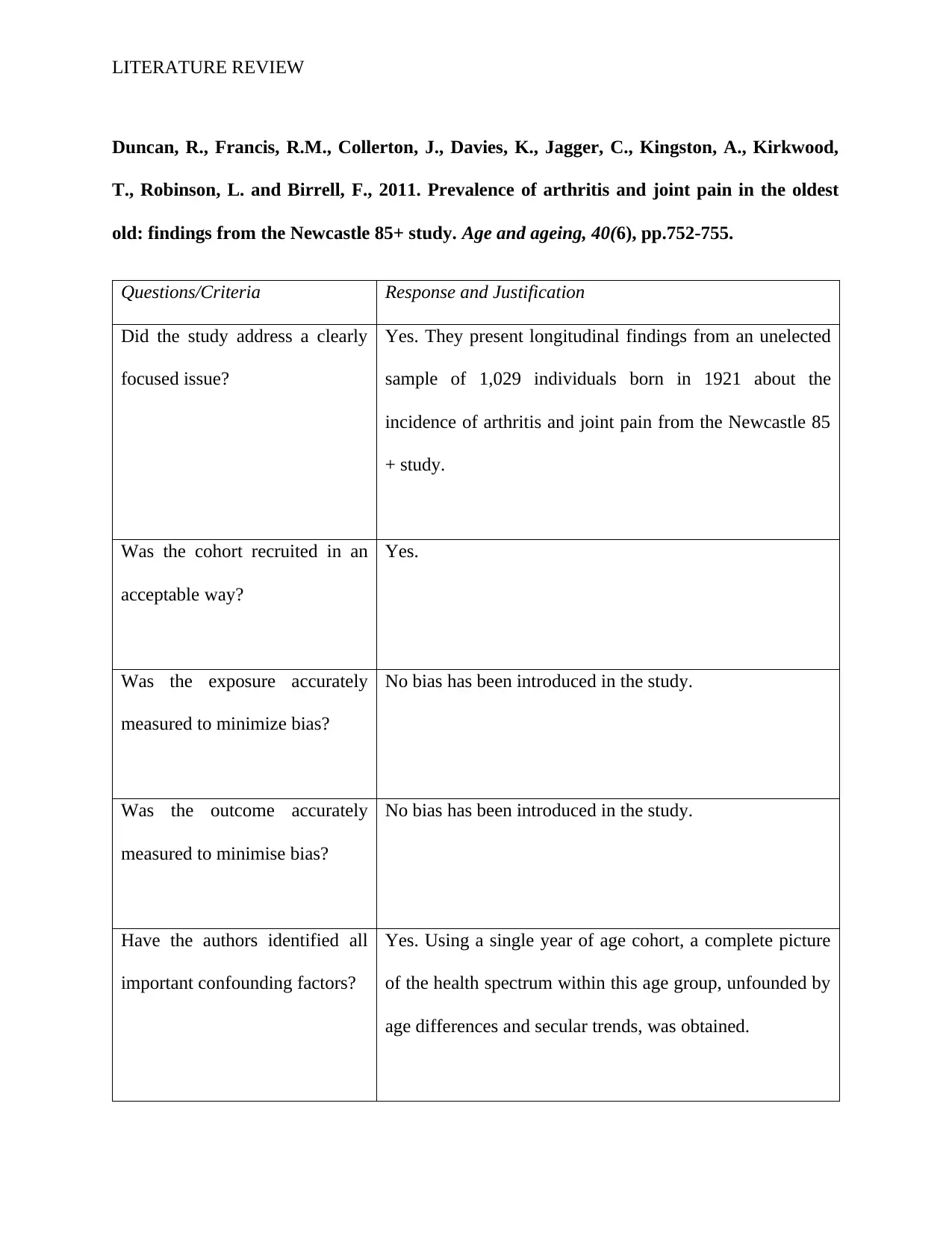
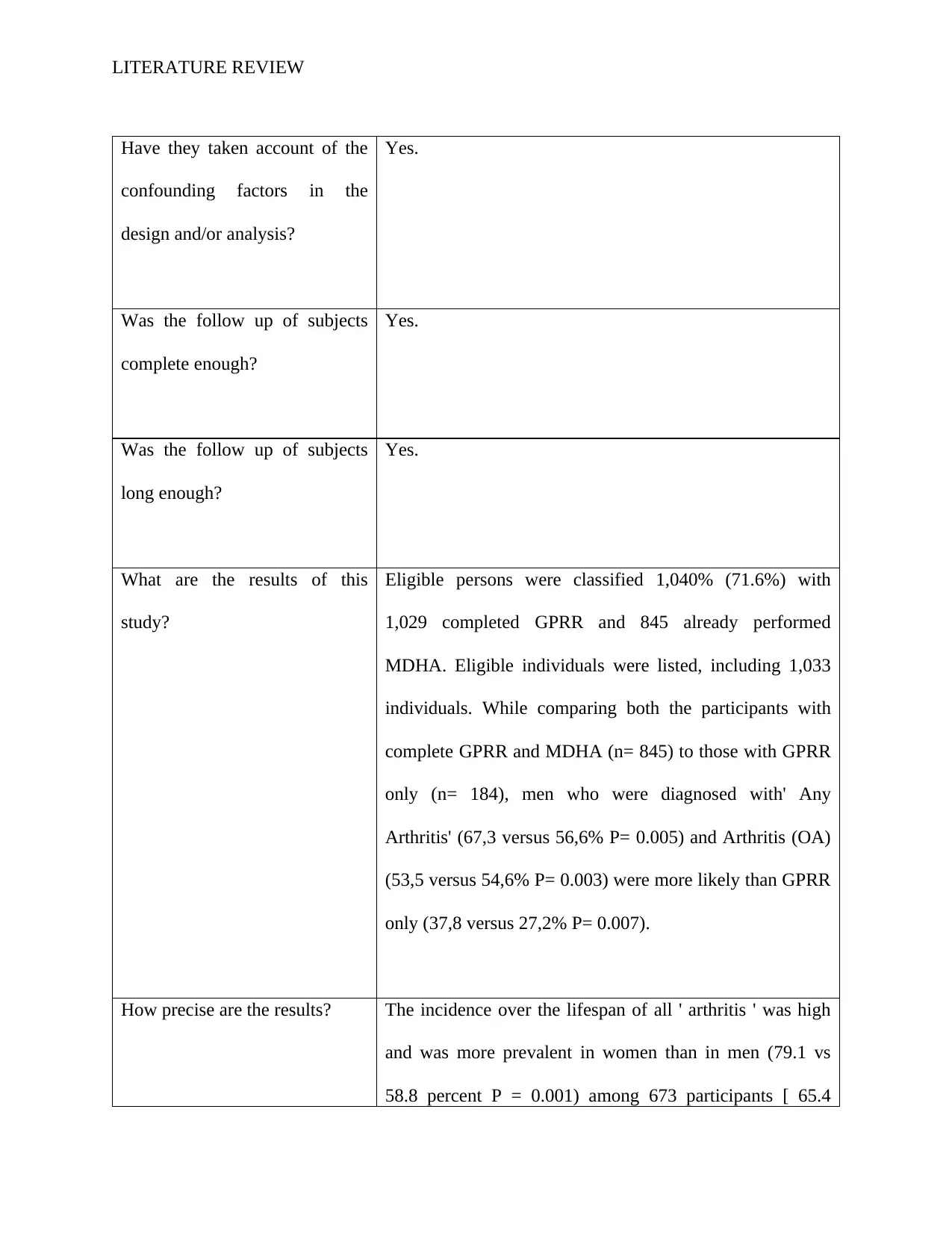
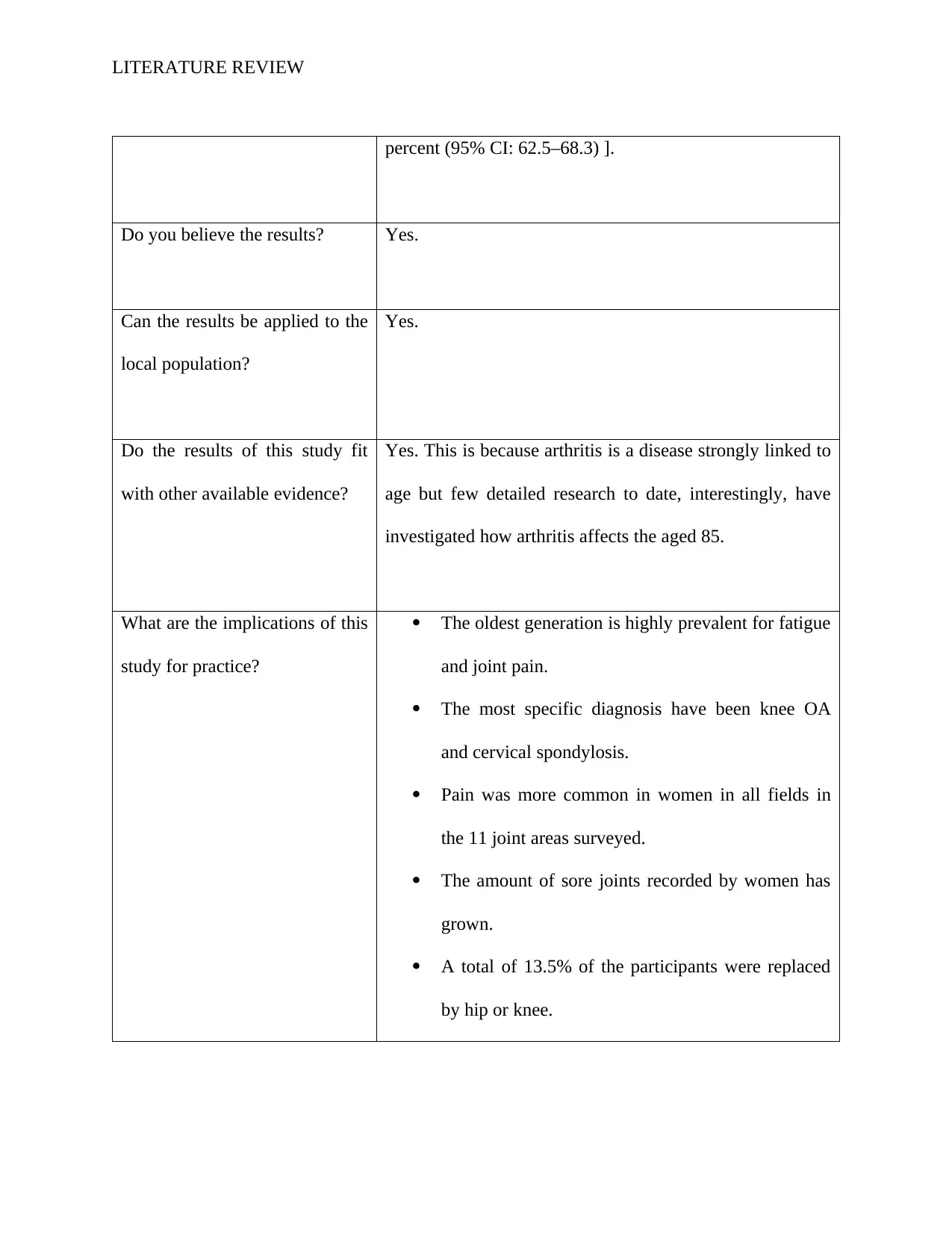
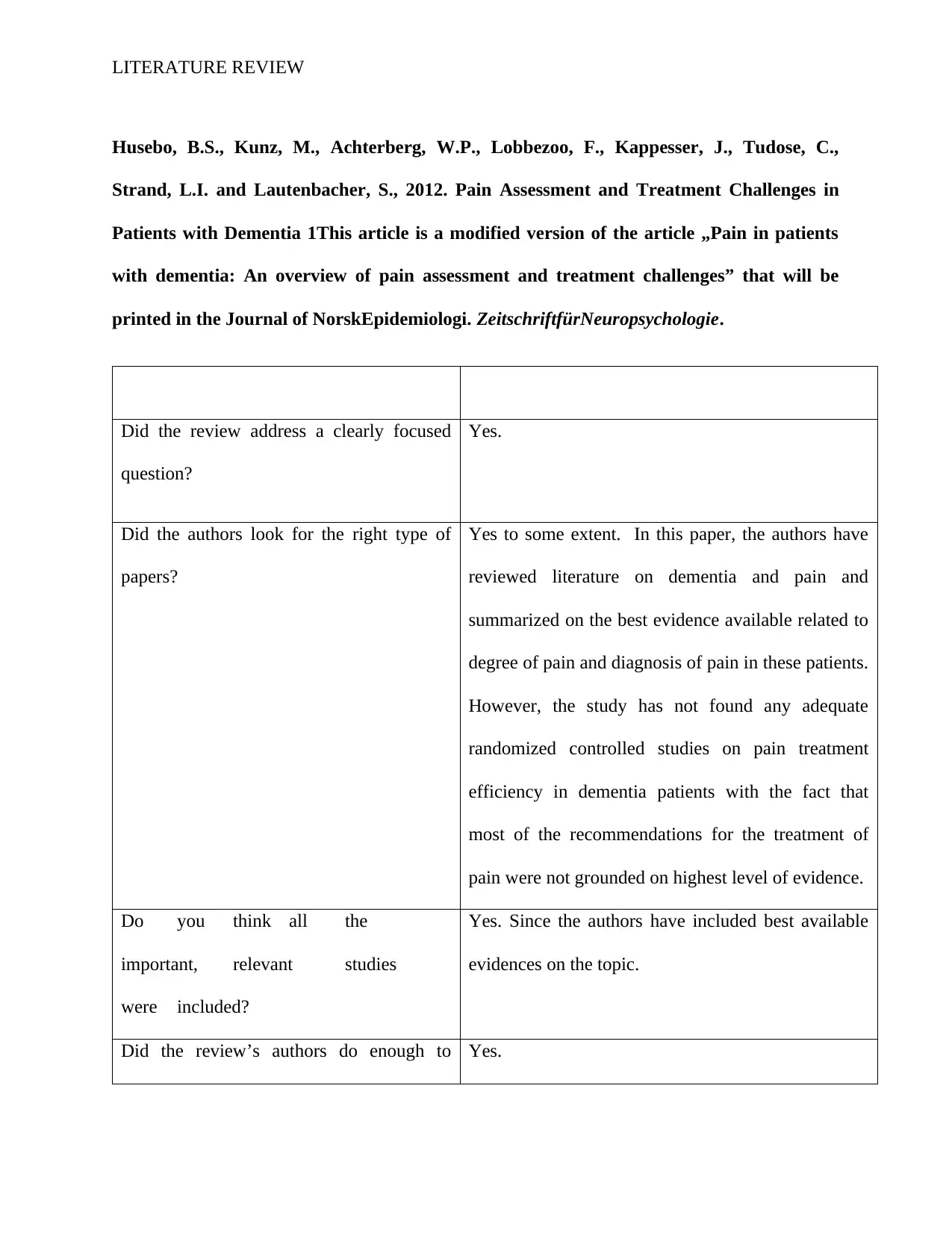
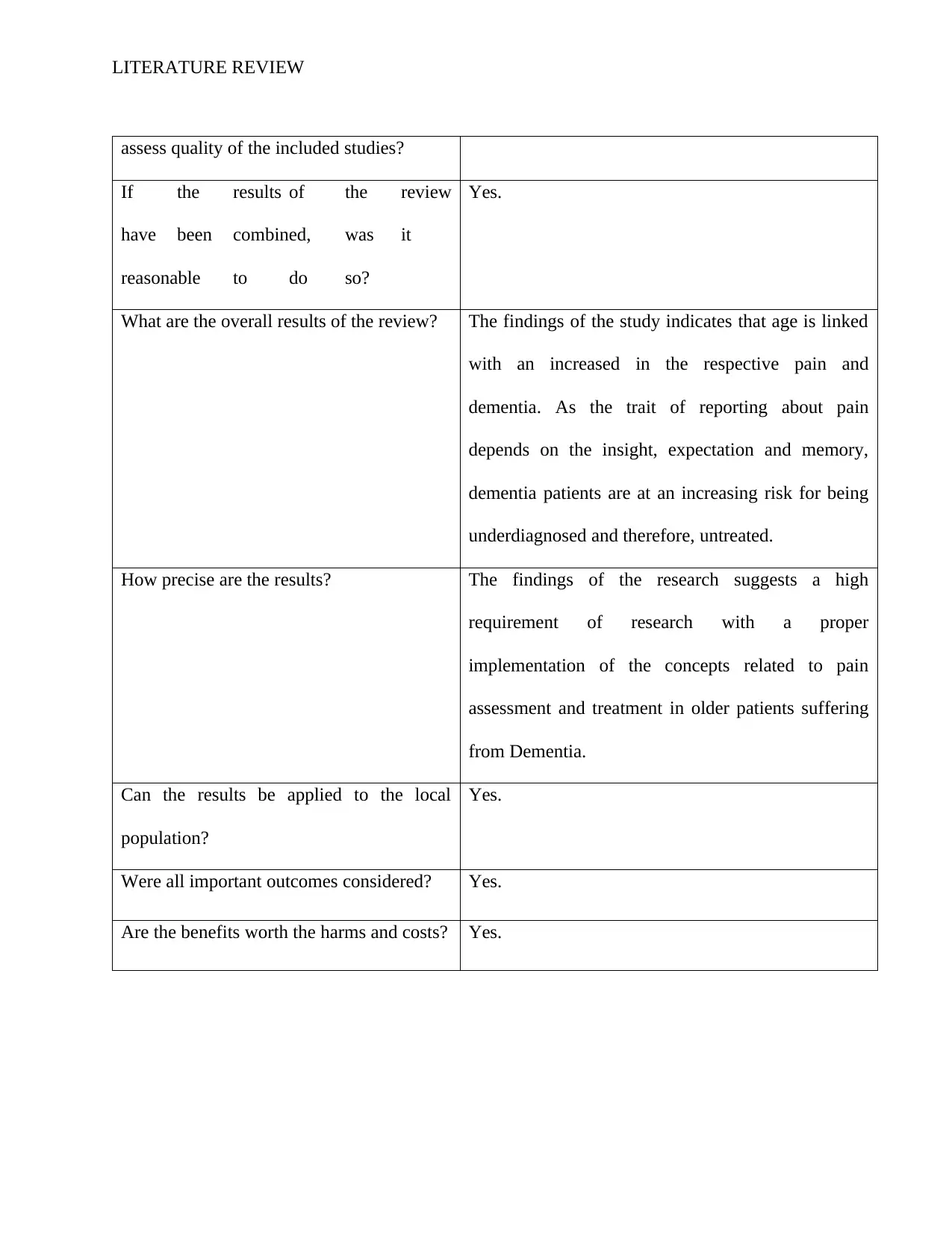
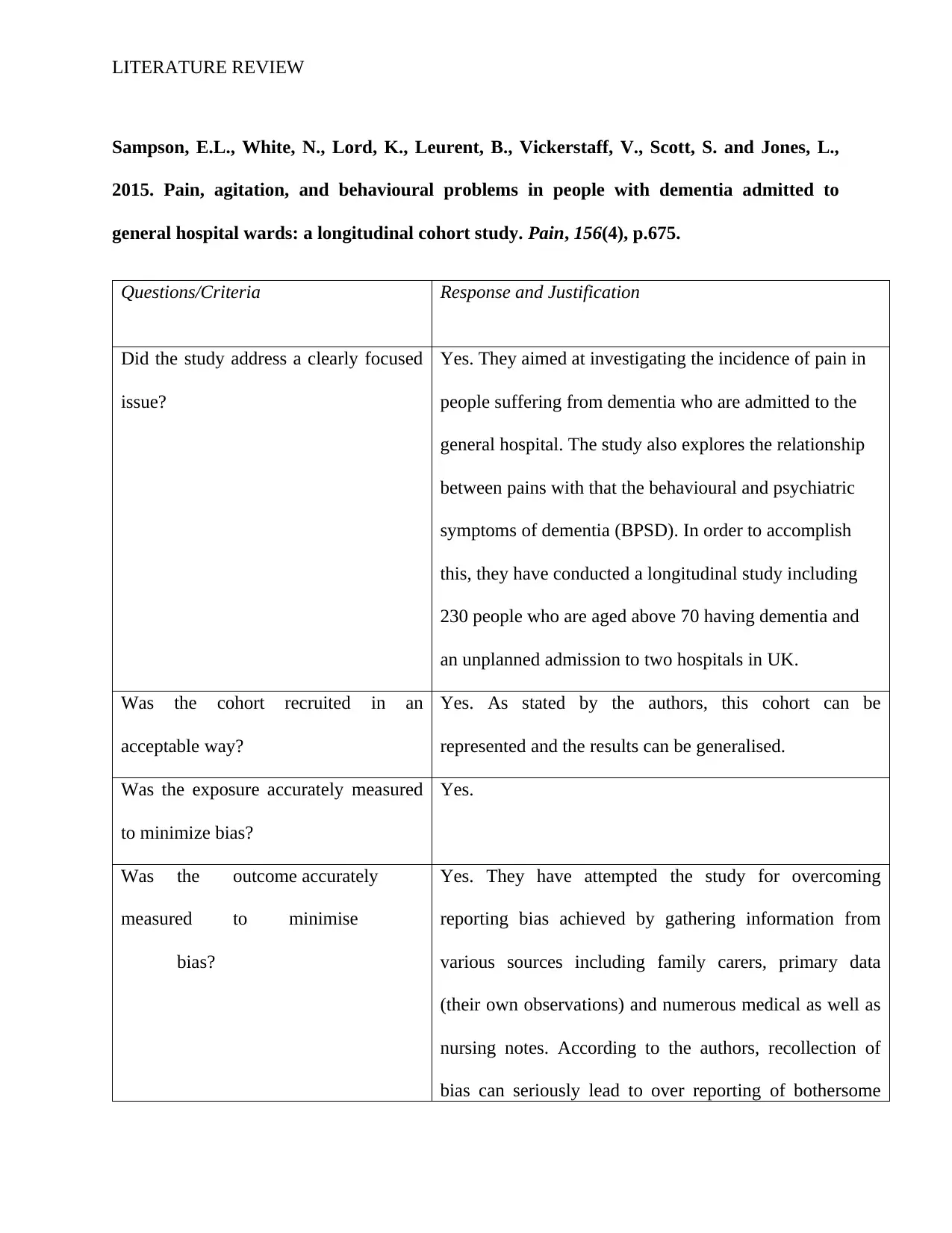
This literature review examines the challenges in providing palliative care to individuals with dementia, particularly within residential care settings. The review highlights that patients with dementia often experience inadequate pain control and end-of-life care due to communication difficulties, under-recognition of pain, and challenges in prognosis. The review explores the barriers to effective pain management, including cognitive impairment and the inability to self-report pain. The author conducted a search of online databases such as CINAHL, Pub Med and Google Scholar and analyzed multiple research papers, including those from Corbett et al. (2016), Duncan et al. (2011), Husebo et al. (2012), and Sampson et al. (2015), to identify key issues and potential solutions. The review emphasizes the need for comprehensive and palliative care approaches and offers recommendations to improve patient outcomes. The study also focuses on the importance of effective communication, staff training, and the implementation of evidence-based pain management strategies to enhance the quality of life for dementia patients during their final stages of life.



1 out of 30
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.