Effectiveness of Long-Term Antibiotics for UTIs: A Systematic Review
VerifiedAdded on 2023/05/29
|9
|3284
|279
Report
AI Summary
This report provides a systematic review of the evidence surrounding the use of long-term antibiotic therapy for urinary tract infections (UTIs). It addresses the increasing antibiotic resistance and the need for evidence-based decisions regarding long-term antibiotic use, particularly in older adults. The research question focuses on whether long-term antibiotics are more beneficial in managing UTIs, considering factors like symptom reduction, impact on frailty and multimorbidity, and patient satisfaction. The methodology involves a scoping search of databases like MEDLINE, CINAHL, and PubMed, followed by article selection based on inclusion and exclusion criteria. The GRADE method is used for data analysis, and the findings are presented in a narrative format with thematic analysis. The report acknowledges potential limitations, such as small sample sizes, and aims to disseminate findings for implementation in evidence-based practice. The ultimate goal is to inform clinicians and patients about the effectiveness of long-term antibiotic therapy for UTIs.
Practice context:
Antibiotic therapy for preventing urinary tract infections
Urinary tract infections occur due to the action of microbes, specifically bacteria and few
fungi and are one of the most common infections that affects humans. This infection primarily
affects the lower portions of the urinary tract and is also referred to as bladder infection or cystitis
(Foxman 2013). The most common cause for UTI is Escherichia coli, and certain risk factors such as,
obesity, diabetes, female anatomy, family history, and sexual intercourse. According to Foxman
(2014) some of the common symptoms of UTI include burning sensation with urination, bloody
urine, cloudy urine, pelvic pain, increased urgency, and rectal pain. Most uncomplicated cases of
UTIs are provided treatment with short course of antibiotics namely,
trimethoprim/sulfamethoxazole or nitrofurantoin (Flores-Mireles et al. 2015). Resistance to the
antibiotics that are commonly administered for treating this condition is increasing at an alarming
rate.
Under circumstances when the patient suffers from complicated UTI incidence, intravenous
or longer course of antibiotic administration is often required. Administration of
phenazopyridine often helps with the management of symptoms (Rowe and Juthani-Mehta 2014).
Older women and men are commonly prescribed antibiotics for preventing recurrent urinary tract
infections. Use of antibiotics have been recognised as the principle driver of antibiotic resistance.
Thus, use of long term antibiotics must be backed with adequate evidence, where the potential
benefits outweigh the risks (Edlin et al. 2013).
Project title:
Evaluation of available evidence for determining the effectiveness of long term antibiotic
therapy for the treatment of urinary tract infections (UTIs): a systematic review.
Evidence based practice/research question:
“Are long-term antibiotics more beneficial, to effectively manage urinary tract infections and
inform the clinicians and patients during decision making?”
Focused question model employed:
The PICO framework was used for formulating this question, in relation to evidence based
practice. This framework facilitated the framing and development of the clinical research question
and effectively assisted in adopting certain literature search strategies (Hastings and Fisher 2014).
The acronym for the research question are given below:
P- Patients with urinary tract infection
I- Long term antibiotic therapy
C- None
O- Enhanced health outcomes and reduced symptoms
1
6NU995 Project proposal template july 2016
Antibiotic therapy for preventing urinary tract infections
Urinary tract infections occur due to the action of microbes, specifically bacteria and few
fungi and are one of the most common infections that affects humans. This infection primarily
affects the lower portions of the urinary tract and is also referred to as bladder infection or cystitis
(Foxman 2013). The most common cause for UTI is Escherichia coli, and certain risk factors such as,
obesity, diabetes, female anatomy, family history, and sexual intercourse. According to Foxman
(2014) some of the common symptoms of UTI include burning sensation with urination, bloody
urine, cloudy urine, pelvic pain, increased urgency, and rectal pain. Most uncomplicated cases of
UTIs are provided treatment with short course of antibiotics namely,
trimethoprim/sulfamethoxazole or nitrofurantoin (Flores-Mireles et al. 2015). Resistance to the
antibiotics that are commonly administered for treating this condition is increasing at an alarming
rate.
Under circumstances when the patient suffers from complicated UTI incidence, intravenous
or longer course of antibiotic administration is often required. Administration of
phenazopyridine often helps with the management of symptoms (Rowe and Juthani-Mehta 2014).
Older women and men are commonly prescribed antibiotics for preventing recurrent urinary tract
infections. Use of antibiotics have been recognised as the principle driver of antibiotic resistance.
Thus, use of long term antibiotics must be backed with adequate evidence, where the potential
benefits outweigh the risks (Edlin et al. 2013).
Project title:
Evaluation of available evidence for determining the effectiveness of long term antibiotic
therapy for the treatment of urinary tract infections (UTIs): a systematic review.
Evidence based practice/research question:
“Are long-term antibiotics more beneficial, to effectively manage urinary tract infections and
inform the clinicians and patients during decision making?”
Focused question model employed:
The PICO framework was used for formulating this question, in relation to evidence based
practice. This framework facilitated the framing and development of the clinical research question
and effectively assisted in adopting certain literature search strategies (Hastings and Fisher 2014).
The acronym for the research question are given below:
P- Patients with urinary tract infection
I- Long term antibiotic therapy
C- None
O- Enhanced health outcomes and reduced symptoms
1
6NU995 Project proposal template july 2016
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Aims & objectives:
Research aim- To explore available evidence regarding the administration of long term
antibiotic therapy, in people who have been clinically diagnosed with UTI.
Research objectives-
To explore the impact of long term antibiotic therapy on symptoms of UTI
To determine the effect of long term antibiotic therapy on frailty and multimorbidity
To explore the effect of long term antibiotic therapy on patient satisfaction and user
experience
Make recommendations for changes in UTI treatment
Rationale for the project:
Urinary tract infections and subsequently recurrent UTIs, are over diagnosed in the elderly.
Thus, antibiotic prophylaxis might essentially be approved for indications that characterise bladder
dysfunction or restricted vaginal signs, in place of exact UTI, and therefore might not be able to exert
the intended benefits. Infirmity, multimorbidity, and poly-pharmacy are quite prevalent in elder
individuals and are influential factors for probable damages, such as, those associated to drug
interactions (Martín-Gutiérrez et al. 2015). In addition, older adults who have been prescribed with
trimethoprim-containing antibiotics and renin–angiotensin system inhibitors have been found to
stay at an increased likelihood of the onset of hyperkalaemia, associated hospitalisation rates, and
sudden death (Fralick et al. 2014).
The bacteria that are responsible for UTI are found to enter the urinary bladder through the
urethra. However, these infections also occur due to lymph and blood. There is mounting evidence
for the fact that females are placed at a greater risk for developing UTI due to their anatomy
(Foxman 2013). Antibiotic resistance refers to the capability of microbes to resist the impacts of
certain medication that has the potential to successfully kill the microbe. Resistant microbes are
often difficult to treat, and thus require high dosage of antimicrobial and/or alternative medications
(Niranjan and Malini 2014). These approaches are often more expensive and have toxic impacts on
the body of the UTI patients. The resistance to antibiotics often arise due to three different
mechanisms namely, genetic mechanisms, natural resistance, or acquiring it from others (Bryce et al.
2016). Thus, microbes that are resistant to several antimicrobials are referred to as multidrug
resistant (MDR).
Overview of methods:
A scoping search strategy of several academic databases that are associated with life science
and medicine including MEDLINE, CINAHL, and PubMed was conducted. These electronic search
engines and databases were fed with key phrases and search terms that were relevant to the
phenomenon being investigated (Aveyard 2014). The search was conducted in order to extract
relevant evidences from already existing scholarly literature, in order to draw significant conclusions
to the research question. The search terms comprised of medical subject headings and keywords
that contained information on urinary tract infection and long term antibiotic use.
2
6NU995 Project proposal template july 2016
Research aim- To explore available evidence regarding the administration of long term
antibiotic therapy, in people who have been clinically diagnosed with UTI.
Research objectives-
To explore the impact of long term antibiotic therapy on symptoms of UTI
To determine the effect of long term antibiotic therapy on frailty and multimorbidity
To explore the effect of long term antibiotic therapy on patient satisfaction and user
experience
Make recommendations for changes in UTI treatment
Rationale for the project:
Urinary tract infections and subsequently recurrent UTIs, are over diagnosed in the elderly.
Thus, antibiotic prophylaxis might essentially be approved for indications that characterise bladder
dysfunction or restricted vaginal signs, in place of exact UTI, and therefore might not be able to exert
the intended benefits. Infirmity, multimorbidity, and poly-pharmacy are quite prevalent in elder
individuals and are influential factors for probable damages, such as, those associated to drug
interactions (Martín-Gutiérrez et al. 2015). In addition, older adults who have been prescribed with
trimethoprim-containing antibiotics and renin–angiotensin system inhibitors have been found to
stay at an increased likelihood of the onset of hyperkalaemia, associated hospitalisation rates, and
sudden death (Fralick et al. 2014).
The bacteria that are responsible for UTI are found to enter the urinary bladder through the
urethra. However, these infections also occur due to lymph and blood. There is mounting evidence
for the fact that females are placed at a greater risk for developing UTI due to their anatomy
(Foxman 2013). Antibiotic resistance refers to the capability of microbes to resist the impacts of
certain medication that has the potential to successfully kill the microbe. Resistant microbes are
often difficult to treat, and thus require high dosage of antimicrobial and/or alternative medications
(Niranjan and Malini 2014). These approaches are often more expensive and have toxic impacts on
the body of the UTI patients. The resistance to antibiotics often arise due to three different
mechanisms namely, genetic mechanisms, natural resistance, or acquiring it from others (Bryce et al.
2016). Thus, microbes that are resistant to several antimicrobials are referred to as multidrug
resistant (MDR).
Overview of methods:
A scoping search strategy of several academic databases that are associated with life science
and medicine including MEDLINE, CINAHL, and PubMed was conducted. These electronic search
engines and databases were fed with key phrases and search terms that were relevant to the
phenomenon being investigated (Aveyard 2014). The search was conducted in order to extract
relevant evidences from already existing scholarly literature, in order to draw significant conclusions
to the research question. The search terms comprised of medical subject headings and keywords
that contained information on urinary tract infection and long term antibiotic use.
2
6NU995 Project proposal template july 2016
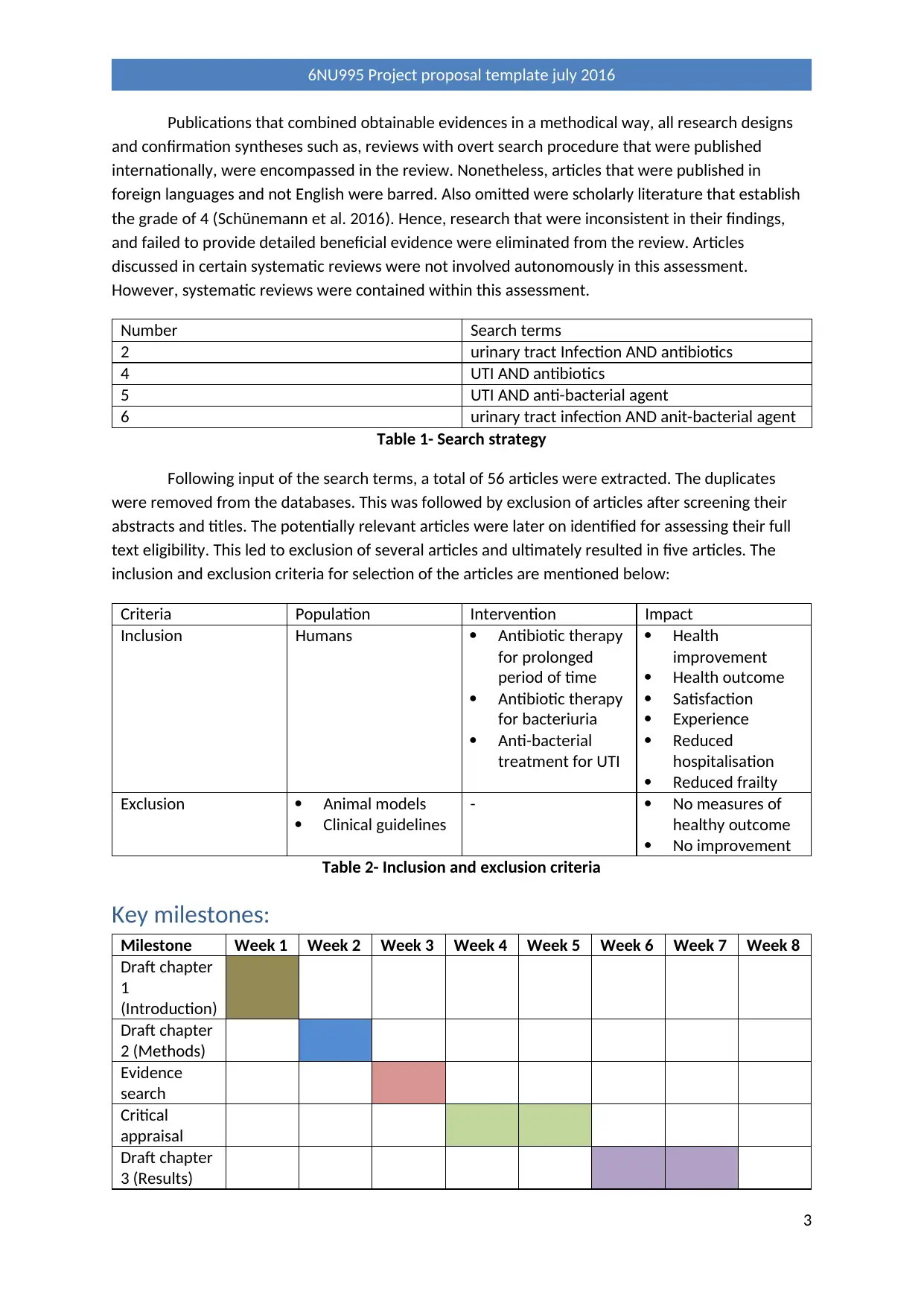
Publications that combined obtainable evidences in a methodical way, all research designs
and confirmation syntheses such as, reviews with overt search procedure that were published
internationally, were encompassed in the review. Nonetheless, articles that were published in
foreign languages and not English were barred. Also omitted were scholarly literature that establish
the grade of 4 (Schünemann et al. 2016). Hence, research that were inconsistent in their findings,
and failed to provide detailed beneficial evidence were eliminated from the review. Articles
discussed in certain systematic reviews were not involved autonomously in this assessment.
However, systematic reviews were contained within this assessment.
Number Search terms
2 urinary tract Infection AND antibiotics
4 UTI AND antibiotics
5 UTI AND anti-bacterial agent
6 urinary tract infection AND anit-bacterial agent
Table 1- Search strategy
Following input of the search terms, a total of 56 articles were extracted. The duplicates
were removed from the databases. This was followed by exclusion of articles after screening their
abstracts and titles. The potentially relevant articles were later on identified for assessing their full
text eligibility. This led to exclusion of several articles and ultimately resulted in five articles. The
inclusion and exclusion criteria for selection of the articles are mentioned below:
Criteria Population Intervention Impact
Inclusion Humans Antibiotic therapy
for prolonged
period of time
Antibiotic therapy
for bacteriuria
Anti-bacterial
treatment for UTI
Health
improvement
Health outcome
Satisfaction
Experience
Reduced
hospitalisation
Reduced frailty
Exclusion Animal models
Clinical guidelines
- No measures of
healthy outcome
No improvement
Table 2- Inclusion and exclusion criteria
Key milestones:
Milestone Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7 Week 8
Draft chapter
1
(Introduction)
Draft chapter
2 (Methods)
Evidence
search
Critical
appraisal
Draft chapter
3 (Results)
3
6NU995 Project proposal template july 2016
and confirmation syntheses such as, reviews with overt search procedure that were published
internationally, were encompassed in the review. Nonetheless, articles that were published in
foreign languages and not English were barred. Also omitted were scholarly literature that establish
the grade of 4 (Schünemann et al. 2016). Hence, research that were inconsistent in their findings,
and failed to provide detailed beneficial evidence were eliminated from the review. Articles
discussed in certain systematic reviews were not involved autonomously in this assessment.
However, systematic reviews were contained within this assessment.
Number Search terms
2 urinary tract Infection AND antibiotics
4 UTI AND antibiotics
5 UTI AND anti-bacterial agent
6 urinary tract infection AND anit-bacterial agent
Table 1- Search strategy
Following input of the search terms, a total of 56 articles were extracted. The duplicates
were removed from the databases. This was followed by exclusion of articles after screening their
abstracts and titles. The potentially relevant articles were later on identified for assessing their full
text eligibility. This led to exclusion of several articles and ultimately resulted in five articles. The
inclusion and exclusion criteria for selection of the articles are mentioned below:
Criteria Population Intervention Impact
Inclusion Humans Antibiotic therapy
for prolonged
period of time
Antibiotic therapy
for bacteriuria
Anti-bacterial
treatment for UTI
Health
improvement
Health outcome
Satisfaction
Experience
Reduced
hospitalisation
Reduced frailty
Exclusion Animal models
Clinical guidelines
- No measures of
healthy outcome
No improvement
Table 2- Inclusion and exclusion criteria
Key milestones:
Milestone Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7 Week 8
Draft chapter
1
(Introduction)
Draft chapter
2 (Methods)
Evidence
search
Critical
appraisal
Draft chapter
3 (Results)
3
6NU995 Project proposal template july 2016
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Draft chapter
4 (Discussion)
Table 3- Key milestones
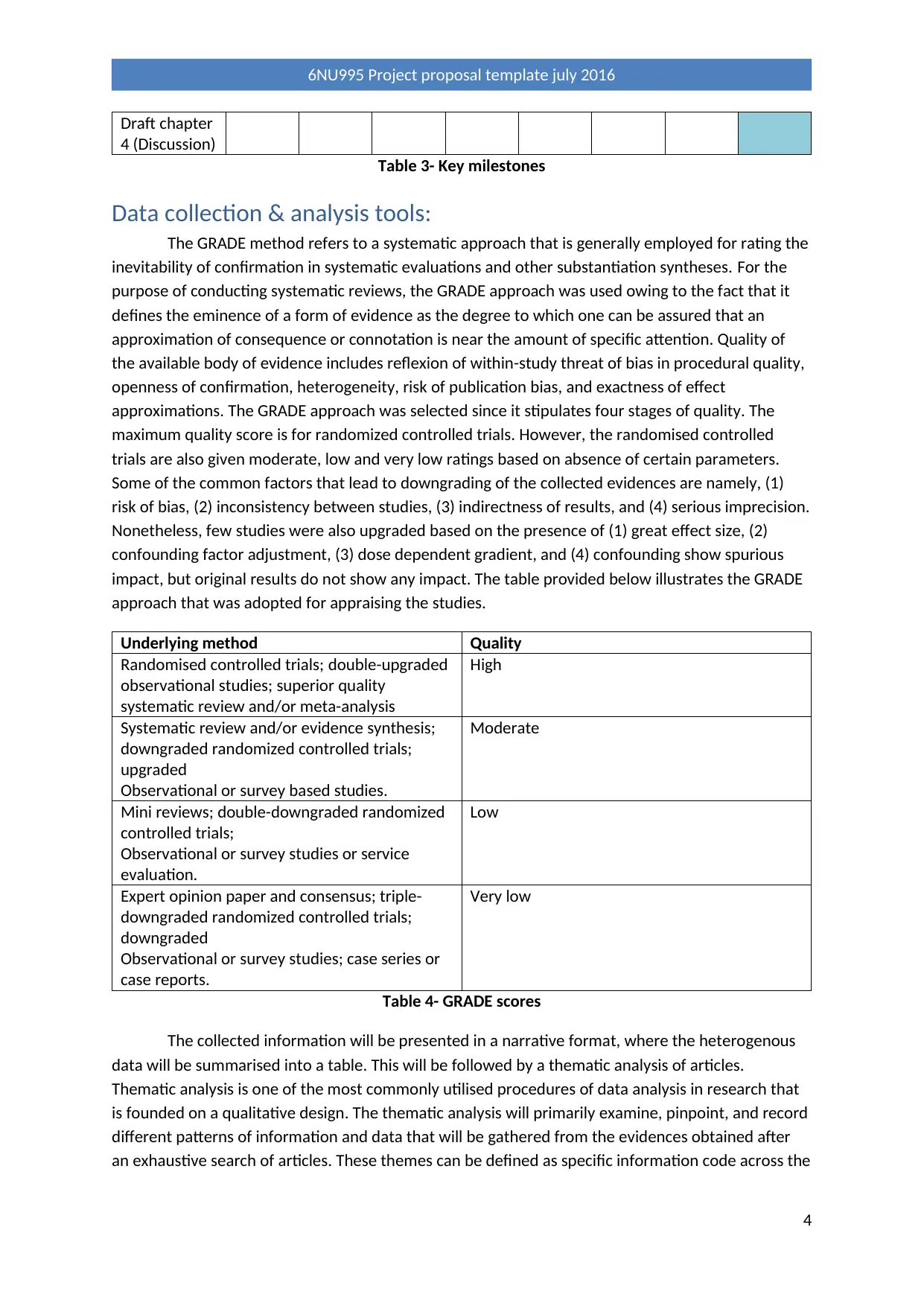
Data collection & analysis tools:
The GRADE method refers to a systematic approach that is generally employed for rating the
inevitability of confirmation in systematic evaluations and other substantiation syntheses. For the
purpose of conducting systematic reviews, the GRADE approach was used owing to the fact that it
defines the eminence of a form of evidence as the degree to which one can be assured that an
approximation of consequence or connotation is near the amount of specific attention. Quality of
the available body of evidence includes reflexion of within-study threat of bias in procedural quality,
openness of confirmation, heterogeneity, risk of publication bias, and exactness of effect
approximations. The GRADE approach was selected since it stipulates four stages of quality. The
maximum quality score is for randomized controlled trials. However, the randomised controlled
trials are also given moderate, low and very low ratings based on absence of certain parameters.
Some of the common factors that lead to downgrading of the collected evidences are namely, (1)
risk of bias, (2) inconsistency between studies, (3) indirectness of results, and (4) serious imprecision.
Nonetheless, few studies were also upgraded based on the presence of (1) great effect size, (2)
confounding factor adjustment, (3) dose dependent gradient, and (4) confounding show spurious
impact, but original results do not show any impact. The table provided below illustrates the GRADE
approach that was adopted for appraising the studies.
Underlying method Quality
Randomised controlled trials; double-upgraded
observational studies; superior quality
systematic review and/or meta-analysis
High
Systematic review and/or evidence synthesis;
downgraded randomized controlled trials;
upgraded
Observational or survey based studies.
Moderate
Mini reviews; double-downgraded randomized
controlled trials;
Observational or survey studies or service
evaluation.
Low
Expert opinion paper and consensus; triple-
downgraded randomized controlled trials;
downgraded
Observational or survey studies; case series or
case reports.
Very low
Table 4- GRADE scores
The collected information will be presented in a narrative format, where the heterogenous
data will be summarised into a table. This will be followed by a thematic analysis of articles.
Thematic analysis is one of the most commonly utilised procedures of data analysis in research that
is founded on a qualitative design. The thematic analysis will primarily examine, pinpoint, and record
different patterns of information and data that will be gathered from the evidences obtained after
an exhaustive search of articles. These themes can be defined as specific information code across the
4
6NU995 Project proposal template july 2016
4 (Discussion)
Table 3- Key milestones
Data collection & analysis tools:
The GRADE method refers to a systematic approach that is generally employed for rating the
inevitability of confirmation in systematic evaluations and other substantiation syntheses. For the
purpose of conducting systematic reviews, the GRADE approach was used owing to the fact that it
defines the eminence of a form of evidence as the degree to which one can be assured that an
approximation of consequence or connotation is near the amount of specific attention. Quality of
the available body of evidence includes reflexion of within-study threat of bias in procedural quality,
openness of confirmation, heterogeneity, risk of publication bias, and exactness of effect
approximations. The GRADE approach was selected since it stipulates four stages of quality. The
maximum quality score is for randomized controlled trials. However, the randomised controlled
trials are also given moderate, low and very low ratings based on absence of certain parameters.
Some of the common factors that lead to downgrading of the collected evidences are namely, (1)
risk of bias, (2) inconsistency between studies, (3) indirectness of results, and (4) serious imprecision.
Nonetheless, few studies were also upgraded based on the presence of (1) great effect size, (2)
confounding factor adjustment, (3) dose dependent gradient, and (4) confounding show spurious
impact, but original results do not show any impact. The table provided below illustrates the GRADE
approach that was adopted for appraising the studies.
Underlying method Quality
Randomised controlled trials; double-upgraded
observational studies; superior quality
systematic review and/or meta-analysis
High
Systematic review and/or evidence synthesis;
downgraded randomized controlled trials;
upgraded
Observational or survey based studies.
Moderate
Mini reviews; double-downgraded randomized
controlled trials;
Observational or survey studies or service
evaluation.
Low
Expert opinion paper and consensus; triple-
downgraded randomized controlled trials;
downgraded
Observational or survey studies; case series or
case reports.
Very low
Table 4- GRADE scores
The collected information will be presented in a narrative format, where the heterogenous
data will be summarised into a table. This will be followed by a thematic analysis of articles.
Thematic analysis is one of the most commonly utilised procedures of data analysis in research that
is founded on a qualitative design. The thematic analysis will primarily examine, pinpoint, and record
different patterns of information and data that will be gathered from the evidences obtained after
an exhaustive search of articles. These themes can be defined as specific information code across the
4
6NU995 Project proposal template july 2016
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
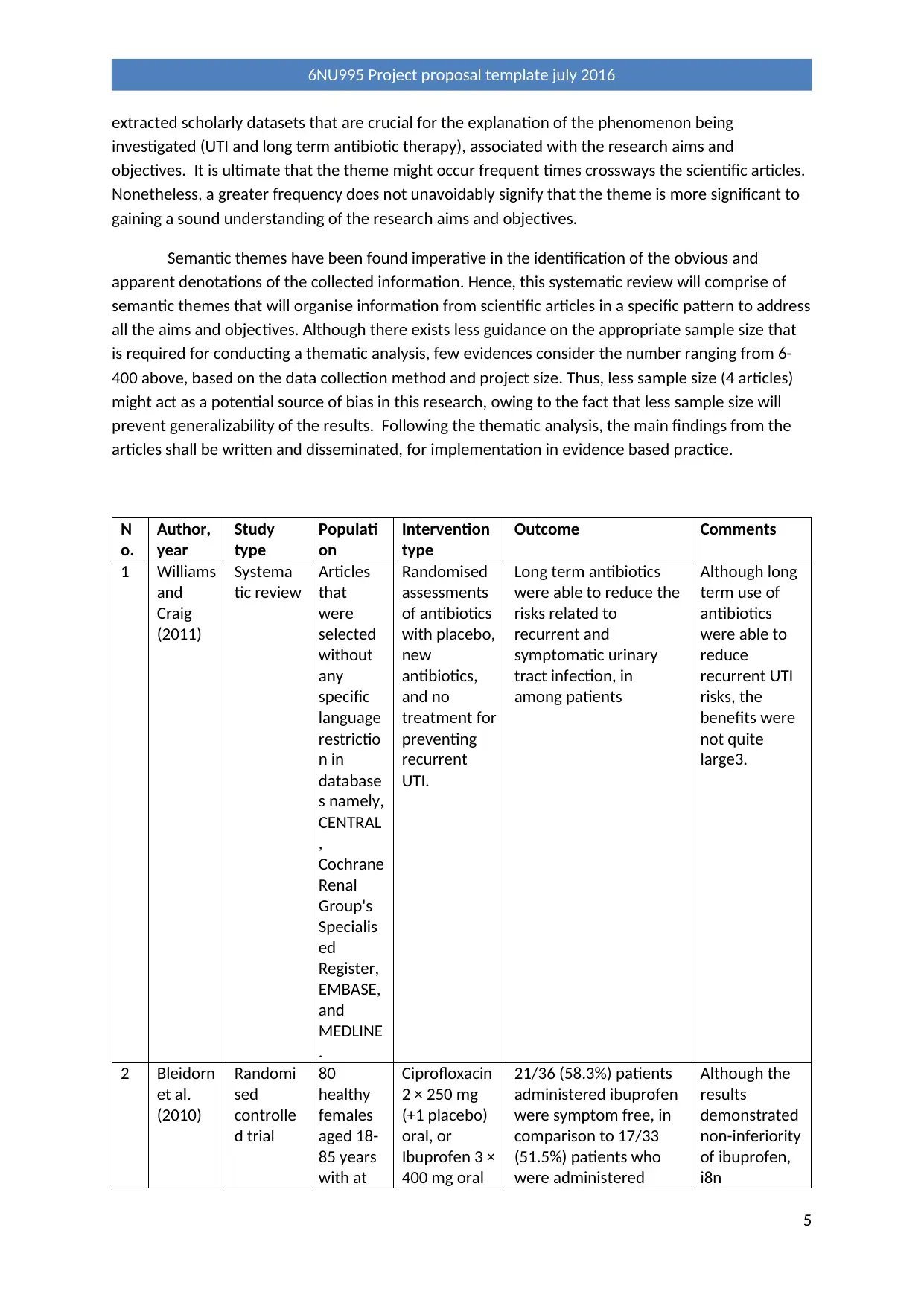
extracted scholarly datasets that are crucial for the explanation of the phenomenon being
investigated (UTI and long term antibiotic therapy), associated with the research aims and
objectives. It is ultimate that the theme might occur frequent times crossways the scientific articles.
Nonetheless, a greater frequency does not unavoidably signify that the theme is more significant to
gaining a sound understanding of the research aims and objectives.
Semantic themes have been found imperative in the identification of the obvious and
apparent denotations of the collected information. Hence, this systematic review will comprise of
semantic themes that will organise information from scientific articles in a specific pattern to address
all the aims and objectives. Although there exists less guidance on the appropriate sample size that
is required for conducting a thematic analysis, few evidences consider the number ranging from 6-
400 above, based on the data collection method and project size. Thus, less sample size (4 articles)
might act as a potential source of bias in this research, owing to the fact that less sample size will
prevent generalizability of the results. Following the thematic analysis, the main findings from the
articles shall be written and disseminated, for implementation in evidence based practice.
N
o.
Author,
year
Study
type
Populati
on
Intervention
type
Outcome Comments
1 Williams
and
Craig
(2011)
Systema
tic review
Articles
that
were
selected
without
any
specific
language
restrictio
n in
database
s namely,
CENTRAL
,
Cochrane
Renal
Group's
Specialis
ed
Register,
EMBASE,
and
MEDLINE
.
Randomised
assessments
of antibiotics
with placebo,
new
antibiotics,
and no
treatment for
preventing
recurrent
UTI.
Long term antibiotics
were able to reduce the
risks related to
recurrent and
symptomatic urinary
tract infection, in
among patients
Although long
term use of
antibiotics
were able to
reduce
recurrent UTI
risks, the
benefits were
not quite
large3.
2 Bleidorn
et al.
(2010)
Randomi
sed
controlle
d trial
80
healthy
females
aged 18-
85 years
with at
Ciprofloxacin
2 × 250 mg
(+1 placebo)
oral, or
Ibuprofen 3 ×
400 mg oral
21/36 (58.3%) patients
administered ibuprofen
were symptom free, in
comparison to 17/33
(51.5%) patients who
were administered
Although the
results
demonstrated
non-inferiority
of ibuprofen,
i8n
5
6NU995 Project proposal template july 2016
investigated (UTI and long term antibiotic therapy), associated with the research aims and
objectives. It is ultimate that the theme might occur frequent times crossways the scientific articles.
Nonetheless, a greater frequency does not unavoidably signify that the theme is more significant to
gaining a sound understanding of the research aims and objectives.
Semantic themes have been found imperative in the identification of the obvious and
apparent denotations of the collected information. Hence, this systematic review will comprise of
semantic themes that will organise information from scientific articles in a specific pattern to address
all the aims and objectives. Although there exists less guidance on the appropriate sample size that
is required for conducting a thematic analysis, few evidences consider the number ranging from 6-
400 above, based on the data collection method and project size. Thus, less sample size (4 articles)
might act as a potential source of bias in this research, owing to the fact that less sample size will
prevent generalizability of the results. Following the thematic analysis, the main findings from the
articles shall be written and disseminated, for implementation in evidence based practice.
N
o.
Author,
year
Study
type
Populati
on
Intervention
type
Outcome Comments
1 Williams
and
Craig
(2011)
Systema
tic review
Articles
that
were
selected
without
any
specific
language
restrictio
n in
database
s namely,
CENTRAL
,
Cochrane
Renal
Group's
Specialis
ed
Register,
EMBASE,
and
MEDLINE
.
Randomised
assessments
of antibiotics
with placebo,
new
antibiotics,
and no
treatment for
preventing
recurrent
UTI.
Long term antibiotics
were able to reduce the
risks related to
recurrent and
symptomatic urinary
tract infection, in
among patients
Although long
term use of
antibiotics
were able to
reduce
recurrent UTI
risks, the
benefits were
not quite
large3.
2 Bleidorn
et al.
(2010)
Randomi
sed
controlle
d trial
80
healthy
females
aged 18-
85 years
with at
Ciprofloxacin
2 × 250 mg
(+1 placebo)
oral, or
Ibuprofen 3 ×
400 mg oral
21/36 (58.3%) patients
administered ibuprofen
were symptom free, in
comparison to 17/33
(51.5%) patients who
were administered
Although the
results
demonstrated
non-inferiority
of ibuprofen,
i8n
5
6NU995 Project proposal template july 2016
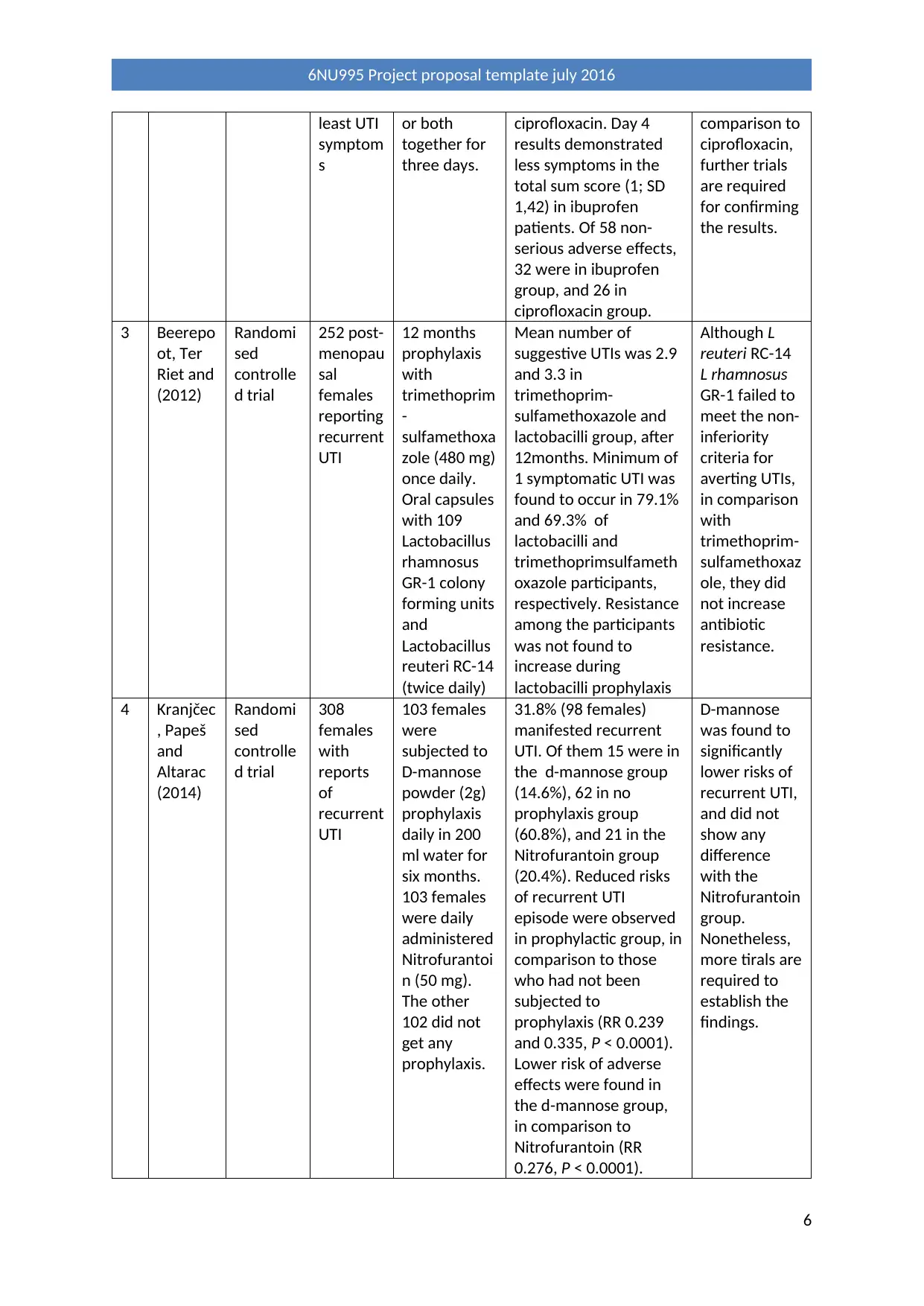
least UTI
symptom
s
or both
together for
three days.
ciprofloxacin. Day 4
results demonstrated
less symptoms in the
total sum score (1; SD
1,42) in ibuprofen
patients. Of 58 non-
serious adverse effects,
32 were in ibuprofen
group, and 26 in
ciprofloxacin group.
comparison to
ciprofloxacin,
further trials
are required
for confirming
the results.
3 Beerepo
ot, Ter
Riet and
(2012)
Randomi
sed
controlle
d trial
252 post-
menopau
sal
females
reporting
recurrent
UTI
12 months
prophylaxis
with
trimethoprim
-
sulfamethoxa
zole (480 mg)
once daily.
Oral capsules
with 109
Lactobacillus
rhamnosus
GR-1 colony
forming units
and
Lactobacillus
reuteri RC-14
(twice daily)
Mean number of
suggestive UTIs was 2.9
and 3.3 in
trimethoprim-
sulfamethoxazole and
lactobacilli group, after
12months. Minimum of
1 symptomatic UTI was
found to occur in 79.1%
and 69.3% of
lactobacilli and
trimethoprimsulfameth
oxazole participants,
respectively. Resistance
among the participants
was not found to
increase during
lactobacilli prophylaxis
Although L
reuteri RC-14
L rhamnosus
GR-1 failed to
meet the non-
inferiority
criteria for
averting UTIs,
in comparison
with
trimethoprim-
sulfamethoxaz
ole, they did
not increase
antibiotic
resistance.
4 Kranjčec
, Papeš
and
Altarac
(2014)
Randomi
sed
controlle
d trial
308
females
with
reports
of
recurrent
UTI
103 females
were
subjected to
D-mannose
powder (2g)
prophylaxis
daily in 200
ml water for
six months.
103 females
were daily
administered
Nitrofurantoi
n (50 mg).
The other
102 did not
get any
prophylaxis.
31.8% (98 females)
manifested recurrent
UTI. Of them 15 were in
the d-mannose group
(14.6%), 62 in no
prophylaxis group
(60.8%), and 21 in the
Nitrofurantoin group
(20.4%). Reduced risks
of recurrent UTI
episode were observed
in prophylactic group, in
comparison to those
who had not been
subjected to
prophylaxis (RR 0.239
and 0.335, P < 0.0001).
Lower risk of adverse
effects were found in
the d-mannose group,
in comparison to
Nitrofurantoin (RR
0.276, P < 0.0001).
D-mannose
was found to
significantly
lower risks of
recurrent UTI,
and did not
show any
difference
with the
Nitrofurantoin
group.
Nonetheless,
more tirals are
required to
establish the
findings.
6
6NU995 Project proposal template july 2016
symptom
s
or both
together for
three days.
ciprofloxacin. Day 4
results demonstrated
less symptoms in the
total sum score (1; SD
1,42) in ibuprofen
patients. Of 58 non-
serious adverse effects,
32 were in ibuprofen
group, and 26 in
ciprofloxacin group.
comparison to
ciprofloxacin,
further trials
are required
for confirming
the results.
3 Beerepo
ot, Ter
Riet and
(2012)
Randomi
sed
controlle
d trial
252 post-
menopau
sal
females
reporting
recurrent
UTI
12 months
prophylaxis
with
trimethoprim
-
sulfamethoxa
zole (480 mg)
once daily.
Oral capsules
with 109
Lactobacillus
rhamnosus
GR-1 colony
forming units
and
Lactobacillus
reuteri RC-14
(twice daily)
Mean number of
suggestive UTIs was 2.9
and 3.3 in
trimethoprim-
sulfamethoxazole and
lactobacilli group, after
12months. Minimum of
1 symptomatic UTI was
found to occur in 79.1%
and 69.3% of
lactobacilli and
trimethoprimsulfameth
oxazole participants,
respectively. Resistance
among the participants
was not found to
increase during
lactobacilli prophylaxis
Although L
reuteri RC-14
L rhamnosus
GR-1 failed to
meet the non-
inferiority
criteria for
averting UTIs,
in comparison
with
trimethoprim-
sulfamethoxaz
ole, they did
not increase
antibiotic
resistance.
4 Kranjčec
, Papeš
and
Altarac
(2014)
Randomi
sed
controlle
d trial
308
females
with
reports
of
recurrent
UTI
103 females
were
subjected to
D-mannose
powder (2g)
prophylaxis
daily in 200
ml water for
six months.
103 females
were daily
administered
Nitrofurantoi
n (50 mg).
The other
102 did not
get any
prophylaxis.
31.8% (98 females)
manifested recurrent
UTI. Of them 15 were in
the d-mannose group
(14.6%), 62 in no
prophylaxis group
(60.8%), and 21 in the
Nitrofurantoin group
(20.4%). Reduced risks
of recurrent UTI
episode were observed
in prophylactic group, in
comparison to those
who had not been
subjected to
prophylaxis (RR 0.239
and 0.335, P < 0.0001).
Lower risk of adverse
effects were found in
the d-mannose group,
in comparison to
Nitrofurantoin (RR
0.276, P < 0.0001).
D-mannose
was found to
significantly
lower risks of
recurrent UTI,
and did not
show any
difference
with the
Nitrofurantoin
group.
Nonetheless,
more tirals are
required to
establish the
findings.
6
6NU995 Project proposal template july 2016
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

Table 5- Summary of evidences
7
6NU995 Project proposal template july 2016
7
6NU995 Project proposal template july 2016
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
References
Aveyard, H., 2014. Doing a literature review in health and social care: A practical guide. McGraw-Hill
Education (UK).
Beerepoot, M., Ter Riet, G. and Nys, S., 2012. Lactobacilli versus antibiotics to prevent urinary tract
infections. A randomized double-blind non-inferiority trial in postmenopausal women. Arch Int
Med, 172, pp.704-12.
Bleidorn, J., Gágyor, I., Kochen, M.M., Wegscheider, K. and Hummers-Pradier, E., 2010. Symptomatic
treatment (ibuprofen) or antibiotics (ciprofloxacin) for uncomplicated urinary tract infection?-results
of a randomized controlled pilot trial. BMC medicine, 8(1), p.30.
Bryce, A., Hay, A.D., Lane, I.F., Thornton, H.V., Wootton, M. and Costelloe, C., 2016. Global
prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli
and association with routine use of antibiotics in primary care: systematic review and meta-
analysis. bmj, 352, p.i939.
Edlin, R.S., Shapiro, D.J., Hersh, A.L. and Copp, H.L., 2013. Antibiotic resistance patterns of outpatient
pediatric urinary tract infections. The Journal of urology, 190(1), pp.222-227.
Flores-Mireles, A.L., Walker, J.N., Caparon, M. and Hultgren, S.J., 2015. Urinary tract infections:
epidemiology, mechanisms of infection and treatment options. Nature reviews microbiology, 13(5),
p.269.
Foxman, B., 2013. Urinary tract infection. In Women and Health (Second Edition) (pp. 553-564).
Foxman, B., 2014. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk
factors, and disease burden. Infectious disease clinics of North America, 28(1), pp.1-13.
Fralick, M., Macdonald, E.M., Gomes, T., Antoniou, T., Hollands, S., Mamdani, M.M. and Juurlink,
D.N., 2014. Co-trimoxazole and sudden death in patients receiving inhibitors of renin-angiotensin
system: population based study. Bmj, 349, p.g6196.
Hastings, C. and Fisher, C.A., 2014. Searching for proof: Creating and using an actionable PICO
question. Nursing management, 45(8), pp.9-12.
Kranjčec, B., Papeš, D. and Altarac, S., 2014. D-mannose powder for prophylaxis of recurrent urinary
tract infections in women: a randomized clinical trial. World journal of urology, 32(1), pp.79-84.
Martín-Gutiérrez, G., Porras-González, A., Martín-Pérez, C., Lepe, J.A. and Aznar, J., 2015. Evaluation
and optimization of the Sysmex UF1000i system for the screening of urinary tract infection in
primary health care elderly patients. Enfermedades infecciosas y microbiologia clinica, 33(5), pp.320-
323.
Niranjan, V. and Malini, A., 2014. Antimicrobial resistance pattern in Escherichia coli causing urinary
tract infection among inpatients. The Indian journal of medical research, 139(6), p.945.
Rowe, T.A. and Juthani-Mehta, M., 2014. Diagnosis and management of urinary tract infection in
older adults. Infectious disease clinics of North America, 28(1), p.75.
8
6NU995 Project proposal template july 2016
Aveyard, H., 2014. Doing a literature review in health and social care: A practical guide. McGraw-Hill
Education (UK).
Beerepoot, M., Ter Riet, G. and Nys, S., 2012. Lactobacilli versus antibiotics to prevent urinary tract
infections. A randomized double-blind non-inferiority trial in postmenopausal women. Arch Int
Med, 172, pp.704-12.
Bleidorn, J., Gágyor, I., Kochen, M.M., Wegscheider, K. and Hummers-Pradier, E., 2010. Symptomatic
treatment (ibuprofen) or antibiotics (ciprofloxacin) for uncomplicated urinary tract infection?-results
of a randomized controlled pilot trial. BMC medicine, 8(1), p.30.
Bryce, A., Hay, A.D., Lane, I.F., Thornton, H.V., Wootton, M. and Costelloe, C., 2016. Global
prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli
and association with routine use of antibiotics in primary care: systematic review and meta-
analysis. bmj, 352, p.i939.
Edlin, R.S., Shapiro, D.J., Hersh, A.L. and Copp, H.L., 2013. Antibiotic resistance patterns of outpatient
pediatric urinary tract infections. The Journal of urology, 190(1), pp.222-227.
Flores-Mireles, A.L., Walker, J.N., Caparon, M. and Hultgren, S.J., 2015. Urinary tract infections:
epidemiology, mechanisms of infection and treatment options. Nature reviews microbiology, 13(5),
p.269.
Foxman, B., 2013. Urinary tract infection. In Women and Health (Second Edition) (pp. 553-564).
Foxman, B., 2014. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk
factors, and disease burden. Infectious disease clinics of North America, 28(1), pp.1-13.
Fralick, M., Macdonald, E.M., Gomes, T., Antoniou, T., Hollands, S., Mamdani, M.M. and Juurlink,
D.N., 2014. Co-trimoxazole and sudden death in patients receiving inhibitors of renin-angiotensin
system: population based study. Bmj, 349, p.g6196.
Hastings, C. and Fisher, C.A., 2014. Searching for proof: Creating and using an actionable PICO
question. Nursing management, 45(8), pp.9-12.
Kranjčec, B., Papeš, D. and Altarac, S., 2014. D-mannose powder for prophylaxis of recurrent urinary
tract infections in women: a randomized clinical trial. World journal of urology, 32(1), pp.79-84.
Martín-Gutiérrez, G., Porras-González, A., Martín-Pérez, C., Lepe, J.A. and Aznar, J., 2015. Evaluation
and optimization of the Sysmex UF1000i system for the screening of urinary tract infection in
primary health care elderly patients. Enfermedades infecciosas y microbiologia clinica, 33(5), pp.320-
323.
Niranjan, V. and Malini, A., 2014. Antimicrobial resistance pattern in Escherichia coli causing urinary
tract infection among inpatients. The Indian journal of medical research, 139(6), p.945.
Rowe, T.A. and Juthani-Mehta, M., 2014. Diagnosis and management of urinary tract infection in
older adults. Infectious disease clinics of North America, 28(1), p.75.
8
6NU995 Project proposal template july 2016
Schünemann, H.J., Mustafa, R., Brozek, J., Santesso, N., Alonso-Coello, P., Guyatt, G., Scholten, R.,
Langendam, M., Leeflang, M.M., Akl, E.A. and Singh, J.A., 2016. GRADE Guidelines: 16. GRADE
evidence to decision frameworks for tests in clinical practice and public health. Journal of clinical
epidemiology, 76, pp.89-98.
Williams, G. and Craig, J.C., 2011. Long term antibiotics for preventing recurrent urinary tract‐
infection in children. Cochrane database of systematic reviews, (3).
9
6NU995 Project proposal template july 2016
Langendam, M., Leeflang, M.M., Akl, E.A. and Singh, J.A., 2016. GRADE Guidelines: 16. GRADE
evidence to decision frameworks for tests in clinical practice and public health. Journal of clinical
epidemiology, 76, pp.89-98.
Williams, G. and Craig, J.C., 2011. Long term antibiotics for preventing recurrent urinary tract‐
infection in children. Cochrane database of systematic reviews, (3).
9
6NU995 Project proposal template july 2016
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.