REPORT MANAGEMENT AND APPLICATION OF HEALTH DATA FOR DECISION-MAKING
VerifiedAdded on 2019/10/30
|6
|1353
|436
Report
AI Summary
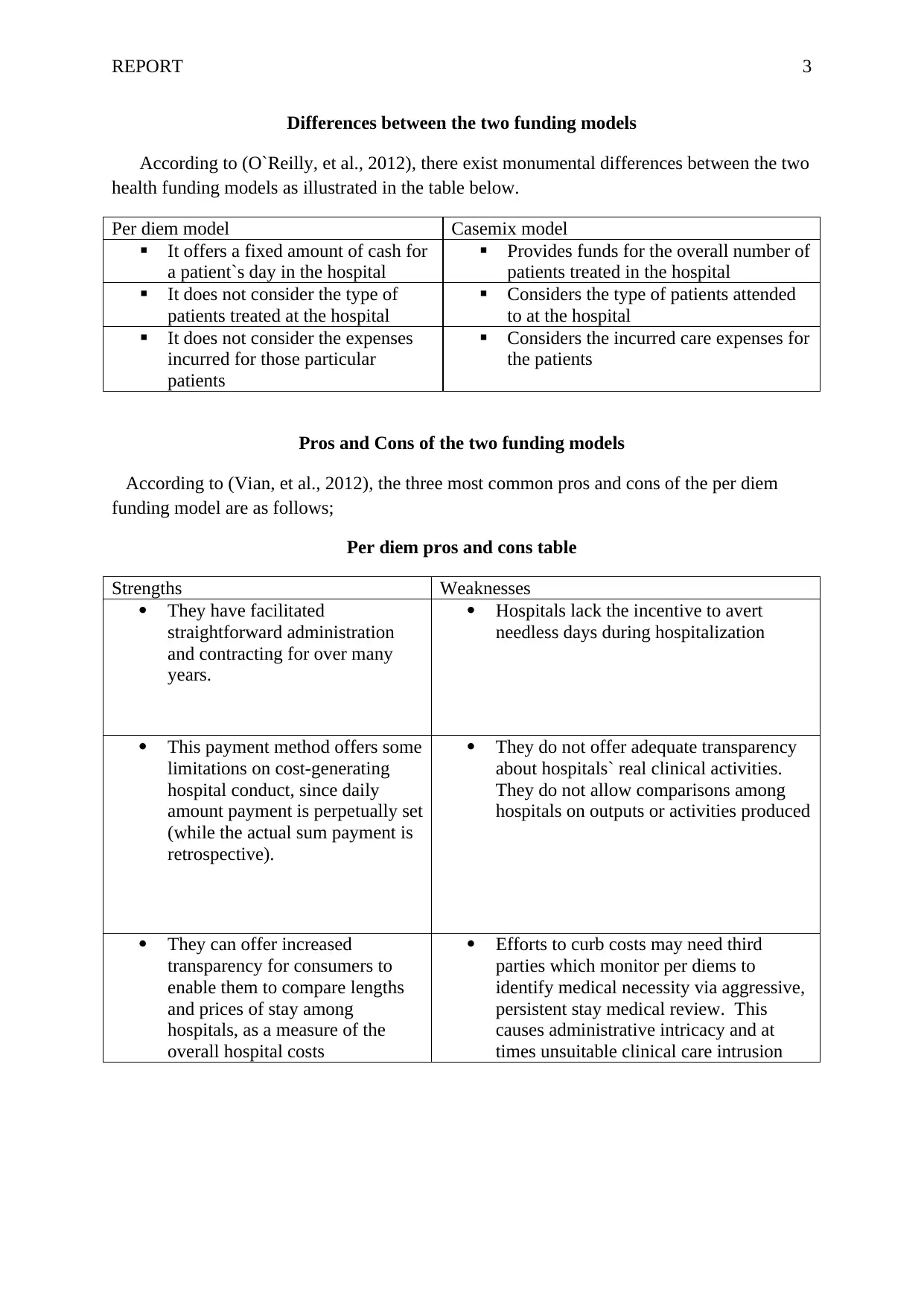
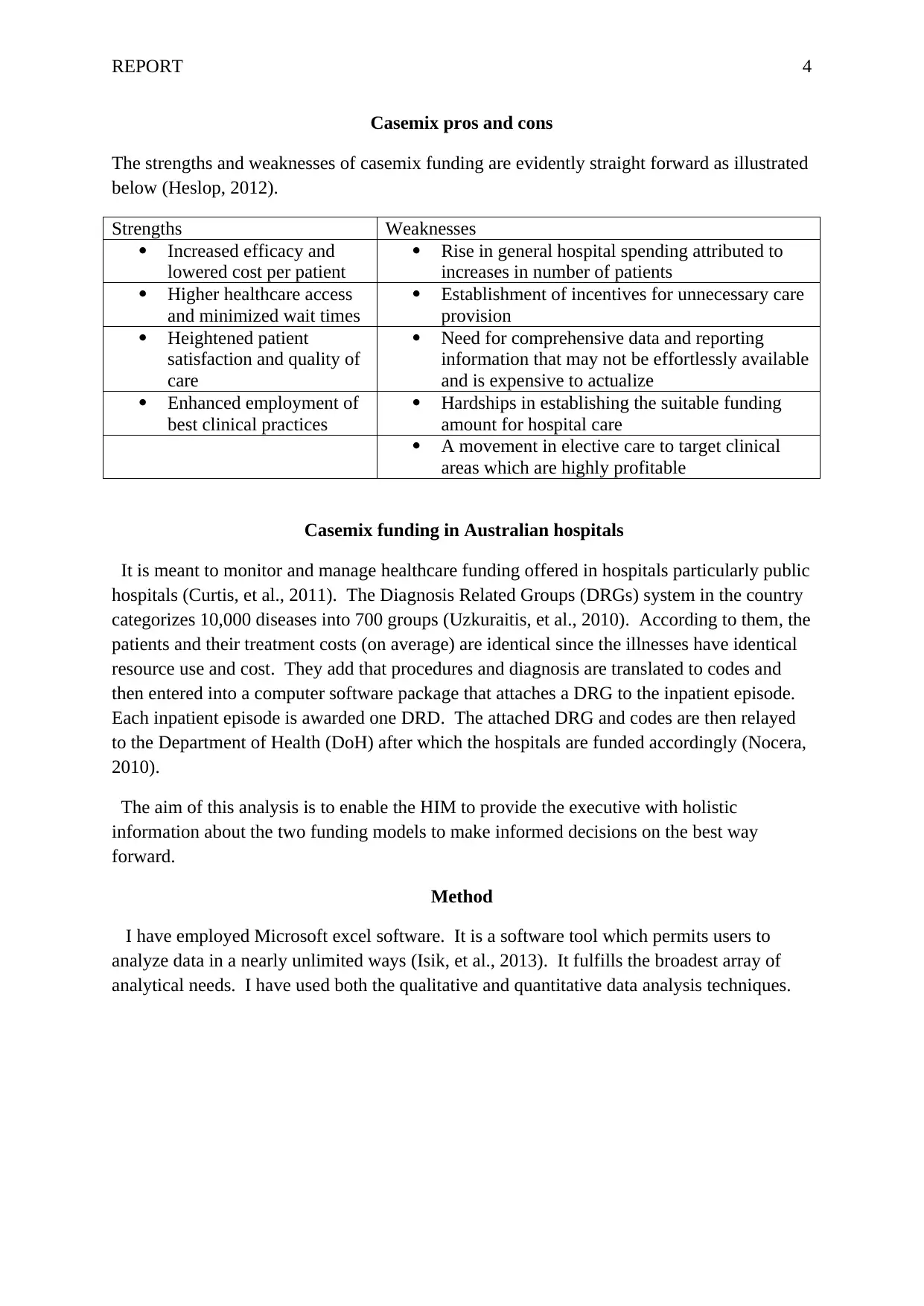
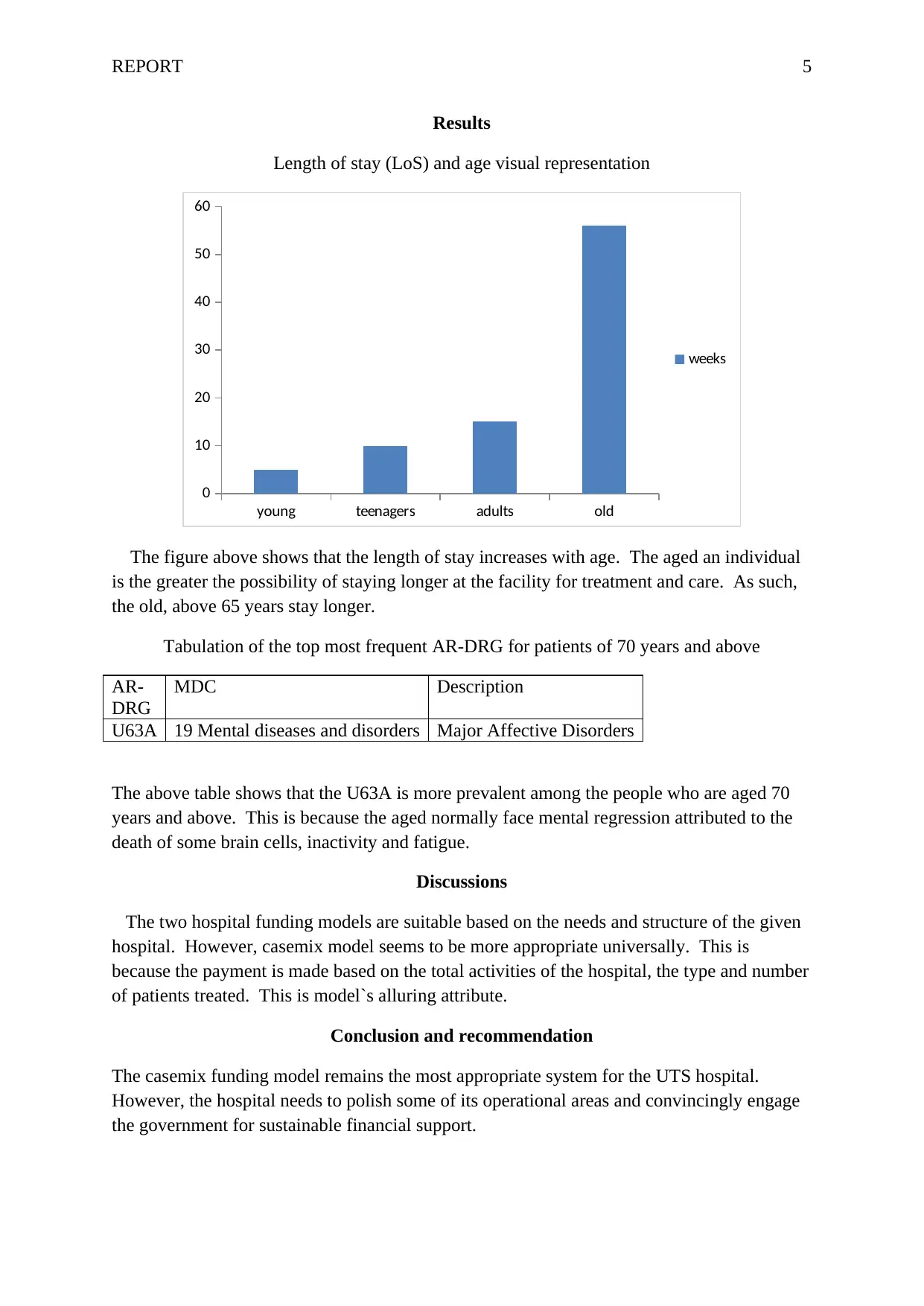
The report discusses two hospital funding models: per diem and casemix. Per diem provides a fixed cash amount for a patient's day in the hospital, regardless of expenses incurred, while casemix assigns funds based on activities performed by hospitals and types of patients treated. The report highlights the pros and cons of each model, including increased transparency and incentives for unnecessary care provision with casemix, but also higher costs and administrative complexities. The casemix model is recommended as a suitable funding system for UTS hospital due to its ability to monitor and manage healthcare funding.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

1 out of 6
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
© 2024 | Zucol Services PVT LTD | All rights reserved.