Diabetes Mellitus Management Project: Improving Health Outcomes in UK
VerifiedAdded on 2023/01/16
|27
|9129
|74
Project
AI Summary
This project focuses on the management of diabetes mellitus, a chronic disease affecting a significant portion of the UK population. It delves into the background of the disease, its causes (including Type 1 and Type 2 diabetes), and the importance of timely diagnosis. The project reviews existing literature on treatment strategies, including lifestyle changes, insulin therapies, and oral hypoglycemic medications, while also emphasizing the crucial role of patient education and self-care. It outlines a project plan with a budget, Gantt chart, and risk assessment, aiming to improve health outcomes, reduce mortality and morbidity, and lower the economic burden associated with diabetes. Furthermore, the project explores leadership approaches and change management strategies within healthcare settings to enhance diabetes management practices and promote effective care for vulnerable groups. The project concludes with recommendations for improving diabetes management and a reflection on the project's outcomes.
Diabetes mellitus
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
TABLE OF CONTENT
INTRODUCTION...........................................................................................................................1
Aim..............................................................................................................................................2
Objective......................................................................................................................................2
Justification..................................................................................................................................2
Statement of intention..................................................................................................................3
Background..................................................................................................................................3
LITERATURE REVIEW................................................................................................................4
Diabetes mellitus.........................................................................................................................4
Treatment and management strategies.........................................................................................5
Long term complications and their management.........................................................................7
PROJECT PLAN.............................................................................................................................8
Budget..........................................................................................................................................8
Project plan..................................................................................................................................9
Gantt chart...................................................................................................................................9
Project risk.................................................................................................................................10
Opportunities.............................................................................................................................11
DISCUSSION................................................................................................................................11
Leadership approach..................................................................................................................11
Change management and diabetes mellitus...............................................................................13
Force field analysis....................................................................................................................15
PROJECT OUTCOME AND SUCCESS EVALUATION...........................................................15
REFLECTION...............................................................................................................................17
RECOMMENDATION.................................................................................................................18
CONCLUSION..............................................................................................................................18
REFERENCES..............................................................................................................................20
APPENDIX 1.................................................................................................................................22
APPENDIX 2.................................................................................................................................23
APPENDIX 3.................................................................................................................................24
INTRODUCTION...........................................................................................................................1
Aim..............................................................................................................................................2
Objective......................................................................................................................................2
Justification..................................................................................................................................2
Statement of intention..................................................................................................................3
Background..................................................................................................................................3
LITERATURE REVIEW................................................................................................................4
Diabetes mellitus.........................................................................................................................4
Treatment and management strategies.........................................................................................5
Long term complications and their management.........................................................................7
PROJECT PLAN.............................................................................................................................8
Budget..........................................................................................................................................8
Project plan..................................................................................................................................9
Gantt chart...................................................................................................................................9
Project risk.................................................................................................................................10
Opportunities.............................................................................................................................11
DISCUSSION................................................................................................................................11
Leadership approach..................................................................................................................11
Change management and diabetes mellitus...............................................................................13
Force field analysis....................................................................................................................15
PROJECT OUTCOME AND SUCCESS EVALUATION...........................................................15
REFLECTION...............................................................................................................................17
RECOMMENDATION.................................................................................................................18
CONCLUSION..............................................................................................................................18
REFERENCES..............................................................................................................................20
APPENDIX 1.................................................................................................................................22
APPENDIX 2.................................................................................................................................23
APPENDIX 3.................................................................................................................................24

⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
INTRODUCTION
Diabetes mellitus is defined as the chronic disease in which body is not able to produce
glucose normally which is key energy source for the cells (McKnight and Gibb, 2017). The
hormone controlling glucose level in the blood (insulin) is either not produced in sufficient
quantity or body show abnormal response towards insulin. As a result of this glucose level in the
blood is increased along with several other health complications. The uncontrolled and
unmanaged symptoms can even lead to death. The chronic disease does not have any permanent
cure and requires controlling and regular monitoring of sugar level in the blood throughout the
life (Sharma, Nazareth and Petersen, 2016). The disease is also inherited to children through
pregnant women and thus it also become vital to manage the symptoms so that new born
individuals can be prevented from this life threatening chronic disease. It has been analysed that
type 1 diabetes can be caused because of the genes or the weak immune system. Type 2 diabetes
can be caused because of the overweight, obesity or physical inactivity. It usually begins with
insulin resistance.
The primary goal of the diabetes mellitus management is to prevent or eliminate the
symptoms or to even slow their progression. The health care services are characterised by the
essential attributes such as high quality care, effective and safe practices. An effective and clear
leadership is required for driving and encouraging changes at various levels of health care system
to achieve necessary goals and to assure patient safety. Within health care services the leadership
is related to both clinical workforce and management and involves multiple challenges. Diabetes
management does not require only clinical intervention for the patients but also demands for the
suitable leadership strategies to foster the changes in health care settings and communities so that
disease can be prevented and managed.
The leadership changes can assist health professionals to effectively manage their
patients as well as vulnerable groups who needs critical attention and care. At present obesity
induced diabetes among children is major concern for the health communities because improper
life style is giving children a life long chronic diseases at very young age (Mutuota, Hill and
Claydon, 2017). Thus best recommendations about the management of diabetes includes
awareness programs along with the self care and life style changes. For the management of
diabetes there is need of close monitoring of routine activities, eating habits and disease
symptoms. Thus the key purpose of this project is management and early recognition of the
1
Diabetes mellitus is defined as the chronic disease in which body is not able to produce
glucose normally which is key energy source for the cells (McKnight and Gibb, 2017). The
hormone controlling glucose level in the blood (insulin) is either not produced in sufficient
quantity or body show abnormal response towards insulin. As a result of this glucose level in the
blood is increased along with several other health complications. The uncontrolled and
unmanaged symptoms can even lead to death. The chronic disease does not have any permanent
cure and requires controlling and regular monitoring of sugar level in the blood throughout the
life (Sharma, Nazareth and Petersen, 2016). The disease is also inherited to children through
pregnant women and thus it also become vital to manage the symptoms so that new born
individuals can be prevented from this life threatening chronic disease. It has been analysed that
type 1 diabetes can be caused because of the genes or the weak immune system. Type 2 diabetes
can be caused because of the overweight, obesity or physical inactivity. It usually begins with
insulin resistance.
The primary goal of the diabetes mellitus management is to prevent or eliminate the
symptoms or to even slow their progression. The health care services are characterised by the
essential attributes such as high quality care, effective and safe practices. An effective and clear
leadership is required for driving and encouraging changes at various levels of health care system
to achieve necessary goals and to assure patient safety. Within health care services the leadership
is related to both clinical workforce and management and involves multiple challenges. Diabetes
management does not require only clinical intervention for the patients but also demands for the
suitable leadership strategies to foster the changes in health care settings and communities so that
disease can be prevented and managed.
The leadership changes can assist health professionals to effectively manage their
patients as well as vulnerable groups who needs critical attention and care. At present obesity
induced diabetes among children is major concern for the health communities because improper
life style is giving children a life long chronic diseases at very young age (Mutuota, Hill and
Claydon, 2017). Thus best recommendations about the management of diabetes includes
awareness programs along with the self care and life style changes. For the management of
diabetes there is need of close monitoring of routine activities, eating habits and disease
symptoms. Thus the key purpose of this project is management and early recognition of the
1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
disease so that cost and severity of the diabetes mellitus can be controlled (Simmons, Wenzel
and Zgibor, 2016).
The major goal of the diabetes treatment and management process is to control the blood
sugar level so that progression or symptoms worsening can be prevented. Type 1 diabetes can be
managed through exercise, dietary changes as well as insulin while type 2 diabetes is
manageable by weight reduction, dietary changes, insulin and non-insulin medications. The
management strategies of diabetes depends upon variety of factors such as health status and
medical history of the patient, impact of medication on patient, accessibility and effectiveness of
health care system and management cost for each patient (Preshaw and Bissett, 2019). The goal
of diabetes management is to maintain the normal value of blood glucose level, triglyceride and
cholesterol. The management practices in correct direction can also assist in restricting the
possible emergence of diabetes related health problems.
Aim
To manage the symptoms and complications related to diabetes mellitus for reducing the
economic cost, mortality and morbidity. The project also aims at improving the quality of life by
providing relieve to symptoms and promoting regular monitoring of diabetes progression so that
health complications can be prevented by delivering timely intervention.
Objective
To enhance the health outcomes and productivity of life of patients of diabetes.
To manage the symptoms and development of diabetes mellitus in patients and
vulnerable groups.
To lower the economic burden, mortality and morbidity of diabetes.
Justification
The number of type 2 diabetes mellitus patients has been rising significantly. At present
nearly 4 million people in UK are living with diabetes (Diabetes Prevalence, 2019). It includes
both diagnosed and undiagnosed individuals. The factors such as symptoms management, life
style, eating habits and access to health care services plays crucial role in managing both chronic
and acute complications related to diabetes. Thus it is essential to manage diabetes mellitus so
that number of deaths and vulnerable people can be controlled. The obesity is one of the key
reason for increasing prevalence of diabetes mellitus.
2
and Zgibor, 2016).
The major goal of the diabetes treatment and management process is to control the blood
sugar level so that progression or symptoms worsening can be prevented. Type 1 diabetes can be
managed through exercise, dietary changes as well as insulin while type 2 diabetes is
manageable by weight reduction, dietary changes, insulin and non-insulin medications. The
management strategies of diabetes depends upon variety of factors such as health status and
medical history of the patient, impact of medication on patient, accessibility and effectiveness of
health care system and management cost for each patient (Preshaw and Bissett, 2019). The goal
of diabetes management is to maintain the normal value of blood glucose level, triglyceride and
cholesterol. The management practices in correct direction can also assist in restricting the
possible emergence of diabetes related health problems.
Aim
To manage the symptoms and complications related to diabetes mellitus for reducing the
economic cost, mortality and morbidity. The project also aims at improving the quality of life by
providing relieve to symptoms and promoting regular monitoring of diabetes progression so that
health complications can be prevented by delivering timely intervention.
Objective
To enhance the health outcomes and productivity of life of patients of diabetes.
To manage the symptoms and development of diabetes mellitus in patients and
vulnerable groups.
To lower the economic burden, mortality and morbidity of diabetes.
Justification
The number of type 2 diabetes mellitus patients has been rising significantly. At present
nearly 4 million people in UK are living with diabetes (Diabetes Prevalence, 2019). It includes
both diagnosed and undiagnosed individuals. The factors such as symptoms management, life
style, eating habits and access to health care services plays crucial role in managing both chronic
and acute complications related to diabetes. Thus it is essential to manage diabetes mellitus so
that number of deaths and vulnerable people can be controlled. The obesity is one of the key
reason for increasing prevalence of diabetes mellitus.
2
The lack of effective diabetes management practices and programs is also one of the key
force which is increasing the prevalence of the disease (Hopkins, Taylor and Lean, 2019). Thus it
is required to develop a project which aims at management practices. The project is vital for
improving the education and awareness among both communities and health professionals. It
will guide service providers so that they can adopt suitable nursing and health care interventions
to assess the care needs of individuals and how they can reduce the severity and complexity of
the disease.
In addition to the prevention of disease there is also need of improving the symptom
management of the patients so that long term risk factors and complications of the disease can be
avoided or delayed. The improved management practices adopted by health care professionals is
also helpful in managing the economic stress associated with the disease (Wisting and Snoek,
2019). The treatment such as insulin therapies, treatment cost for other risks factors or diseases
originated from the diabetes mellitus also needs financial assistance or home care support
services.
Diabetes management requires close monitoring and person centred care approach for the
patient. Thus multidisciplinary teams must work in collaboration with each other so that they can
identify and fulfil the care requirements of the patient (Morris and Bain, 2019). The leadership
plays a crucial role in the quality of services and thus it is vital to understand the different
approaches of leadership and change management for making the project successful and
improving the diabetes management practices.
Statement of intention
The purpose of this project is to increase the awareness among communities about the
management of diabetes mellitus. The health professionals must adopt suitable strategies to
support communities so that diabetes risks can be prevented and symptoms of the patients can be
managed. The project also intend to enhance the quality of life of diabetes patients by improving
the management and leadership attributes of health care professionals.
Background
Diabetes mellitus is metabolic disorder in which blood sugar level is elevates over time.
The project targets the UK population in which diabetes prevalence is increasing rapidly. It is
estimated that by 2025 there will be around 4 million people suffering from type 2 diabetes. In
UK disease is growing rapidly at high rate and is now one of the most common life threatening
3
force which is increasing the prevalence of the disease (Hopkins, Taylor and Lean, 2019). Thus it
is required to develop a project which aims at management practices. The project is vital for
improving the education and awareness among both communities and health professionals. It
will guide service providers so that they can adopt suitable nursing and health care interventions
to assess the care needs of individuals and how they can reduce the severity and complexity of
the disease.
In addition to the prevention of disease there is also need of improving the symptom
management of the patients so that long term risk factors and complications of the disease can be
avoided or delayed. The improved management practices adopted by health care professionals is
also helpful in managing the economic stress associated with the disease (Wisting and Snoek,
2019). The treatment such as insulin therapies, treatment cost for other risks factors or diseases
originated from the diabetes mellitus also needs financial assistance or home care support
services.
Diabetes management requires close monitoring and person centred care approach for the
patient. Thus multidisciplinary teams must work in collaboration with each other so that they can
identify and fulfil the care requirements of the patient (Morris and Bain, 2019). The leadership
plays a crucial role in the quality of services and thus it is vital to understand the different
approaches of leadership and change management for making the project successful and
improving the diabetes management practices.
Statement of intention
The purpose of this project is to increase the awareness among communities about the
management of diabetes mellitus. The health professionals must adopt suitable strategies to
support communities so that diabetes risks can be prevented and symptoms of the patients can be
managed. The project also intend to enhance the quality of life of diabetes patients by improving
the management and leadership attributes of health care professionals.
Background
Diabetes mellitus is metabolic disorder in which blood sugar level is elevates over time.
The project targets the UK population in which diabetes prevalence is increasing rapidly. It is
estimated that by 2025 there will be around 4 million people suffering from type 2 diabetes. In
UK disease is growing rapidly at high rate and is now one of the most common life threatening
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
disease. It is also predicted that at present UK have around 549, 000 people who have diabetes
which is yet to be diagnosed. Thus there is strong need to manage the disease so UK population
can be provided a quality life. The disease is also considered as life threatening due to its related
health complications which includes nerve damage, cardiovascular diseases such as stroke or
heart attack, retinopathy, skin diseases, Alzheimer and hearing impairment (Tay, de Bock and
Mayer-Davis, 2019).
For the study different population groups such as children suffering from obesity,
children with family history of diabetes and people diagnosed with diabetes will be taken into
account.. Thus diabetes management project aims at prevention and control of the diabetes
among vulnerable and affected groups by improving health care interventions and management
practices.
LITERATURE REVIEW
Diabetes mellitus
According to Bird and Turner, (2016) accurate and timely diagnosis of the diabetes is one
of the essential aspect for the management of diabetes. The healthcare leaders put a major
emphasis on diagnostic criteria. In addition to this productive management not only prioritise the
controlling of blood glucose level only but also give priority to diabetes associated risk factors
like obesity, smoking and hyperlipidaemia and blood pressure monitoring. Self care is one of the
most effective treatment strategy in diabetes management. Thus the first step of management
involves the diabetes education to communities and individuals. Vulnerable groups and patients
must be encouraged and supported to actively monitor and manage their health outcomes. Self
monitoring strategies enhances the safety, quality and effectiveness of treatment therapy.
In the same context Purewal and Fisher, (2018) stated that diabetes management goals
can be achieved when treatment strategies and priorities are tailored to individual needs. It
begins with the confident and careful diagnosis of diabetes. The measurement of blood glucose
level and the symptoms such as unexplained weight loss, increased urine volume and thirst or
marked glycosuria can be critical symptoms which indicates the diagnosis of the disease. The
individuals who does not have these classical symptoms but which are high risk such as those
with positive family history, obesity and elderly must also be subjected to diagnosis procedure.
The timely and accurate diagnosis is vital for the effective management of disease. As per the
view of Brooks and Chakera, (2019) along with the symptoms clinicians must also pay attention
4
which is yet to be diagnosed. Thus there is strong need to manage the disease so UK population
can be provided a quality life. The disease is also considered as life threatening due to its related
health complications which includes nerve damage, cardiovascular diseases such as stroke or
heart attack, retinopathy, skin diseases, Alzheimer and hearing impairment (Tay, de Bock and
Mayer-Davis, 2019).
For the study different population groups such as children suffering from obesity,
children with family history of diabetes and people diagnosed with diabetes will be taken into
account.. Thus diabetes management project aims at prevention and control of the diabetes
among vulnerable and affected groups by improving health care interventions and management
practices.
LITERATURE REVIEW
Diabetes mellitus
According to Bird and Turner, (2016) accurate and timely diagnosis of the diabetes is one
of the essential aspect for the management of diabetes. The healthcare leaders put a major
emphasis on diagnostic criteria. In addition to this productive management not only prioritise the
controlling of blood glucose level only but also give priority to diabetes associated risk factors
like obesity, smoking and hyperlipidaemia and blood pressure monitoring. Self care is one of the
most effective treatment strategy in diabetes management. Thus the first step of management
involves the diabetes education to communities and individuals. Vulnerable groups and patients
must be encouraged and supported to actively monitor and manage their health outcomes. Self
monitoring strategies enhances the safety, quality and effectiveness of treatment therapy.
In the same context Purewal and Fisher, (2018) stated that diabetes management goals
can be achieved when treatment strategies and priorities are tailored to individual needs. It
begins with the confident and careful diagnosis of diabetes. The measurement of blood glucose
level and the symptoms such as unexplained weight loss, increased urine volume and thirst or
marked glycosuria can be critical symptoms which indicates the diagnosis of the disease. The
individuals who does not have these classical symptoms but which are high risk such as those
with positive family history, obesity and elderly must also be subjected to diagnosis procedure.
The timely and accurate diagnosis is vital for the effective management of disease. As per the
view of Brooks and Chakera, (2019) along with the symptoms clinicians must also pay attention
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
to the full history of patients. For this purpose factors such as cardiovascular complications,
hypertension, obesity, smoking, family history, neuropathic complications must also be taken
into account.
Treatment and management strategies
Wilmot, Hammond and Gregory, (2016) suggested treatment strategies of diabetes
consist of three major components like dietary and life style changes, insulin treatment and oral
hypoglycaemic therapy. Education is an integral element of the diabetes management which
ensure that patient, health professionals and carers have adequate knowledge and skills to
promote self care and for achieving desired health outcomes. The health leaders must encourage
or motivate the vulnerable groups or patients to set therapeutic goals for controlling weight,
blood sugar or blood pressure.
Goode and Hoover, (2018) stated that initial management of diabetes must be based upon
combination of dietary therapy with physical activities (if possible). For the patients having
presence of hyperglycaemia the pharmacologic therapies such as insulin or oral hypoglycaemic
drugs must also be taken into account. It is also required that individuals and carers must have
adequate knowledge of therapy targets, nutritional requirements, extent and type of physical
activities, meal planning and life style improvements. The health professionals must also educate
individuals regarding emergency and life threatening situations such as detection and
management of complications like skin care or visionary issues, management of emergency
situations like hypoglycaemia, self monitoring and actions against the results of self analysis.
According to Barnard and Breton, (2018) for the diabetes management of all target
groups diet is foremost management aspect. The dietary treatment of the disease ensure that
weight of the individual is control and their nutritional requirements are also fulfilled. Thus it is
suggested that cholesterol consumption must be restricted or limited to only less than 300 mg on
daily basis. The nutritive sweeteners and excessive salt intake must be restricted. The dietary
control is not only advised for the diabetic population but is also suggested for the vulnerable
groups who are higher risk of developing disease.
In similar context Hoppe, Cade and Carter, (2017) stated that for the non-diabetic
population alcohol consumptions must also be restricted or limited. In response to the critical
role of diet in diabetes management individual needs and dietary intake assessment must be done
as an essential part of the initial management process. As leader nurses must have abilities to
5
hypertension, obesity, smoking, family history, neuropathic complications must also be taken
into account.
Treatment and management strategies
Wilmot, Hammond and Gregory, (2016) suggested treatment strategies of diabetes
consist of three major components like dietary and life style changes, insulin treatment and oral
hypoglycaemic therapy. Education is an integral element of the diabetes management which
ensure that patient, health professionals and carers have adequate knowledge and skills to
promote self care and for achieving desired health outcomes. The health leaders must encourage
or motivate the vulnerable groups or patients to set therapeutic goals for controlling weight,
blood sugar or blood pressure.
Goode and Hoover, (2018) stated that initial management of diabetes must be based upon
combination of dietary therapy with physical activities (if possible). For the patients having
presence of hyperglycaemia the pharmacologic therapies such as insulin or oral hypoglycaemic
drugs must also be taken into account. It is also required that individuals and carers must have
adequate knowledge of therapy targets, nutritional requirements, extent and type of physical
activities, meal planning and life style improvements. The health professionals must also educate
individuals regarding emergency and life threatening situations such as detection and
management of complications like skin care or visionary issues, management of emergency
situations like hypoglycaemia, self monitoring and actions against the results of self analysis.
According to Barnard and Breton, (2018) for the diabetes management of all target
groups diet is foremost management aspect. The dietary treatment of the disease ensure that
weight of the individual is control and their nutritional requirements are also fulfilled. Thus it is
suggested that cholesterol consumption must be restricted or limited to only less than 300 mg on
daily basis. The nutritive sweeteners and excessive salt intake must be restricted. The dietary
control is not only advised for the diabetic population but is also suggested for the vulnerable
groups who are higher risk of developing disease.
In similar context Hoppe, Cade and Carter, (2017) stated that for the non-diabetic
population alcohol consumptions must also be restricted or limited. In response to the critical
role of diet in diabetes management individual needs and dietary intake assessment must be done
as an essential part of the initial management process. As leader nurses must have abilities to
5
lead and work in collaboration with dieticians. In cases when dieticians are not present nurses
can also work with physicians. Contrary to this Kong and Gregory, (2016) suggested that food
intake and choice of people greatly depends upon local circumstances such as food availability,
cultural and social values as well as economic factors. Health professionals must develop
leadership attributes so that they can lead the health care team and dietary counselling can
become a continuing process. The dietary consideration and meal planning becomes more crucial
element of the management plan for diabetes patients. The health professionals must focus on
even distribution of meal throughout the day, energy intake on routine basis and consistency of
food timings.
Berry, Davies and Dempster, (2019) elucidated that physical activities not only
encourages weight loss but also improve the sensitivity of insulin which lowers the level of
blood glucose. As per the capability and requirement of person dietary treatment must also align
with the exercise and physical activity programs. The people must also be informed about
hypoglycaemia risk and strategies to eliminate its complications. In support to dietary and
exercise management strategies Barnes and Harriss, (2018) believed that for quality health
outcomes oral hypoglycaemia drugs must be considered only when combination of diet and
physical exercise fails to achieve the targets of therapy. Patient must be made aware of signs and
symptoms of diabetes at an early stage. In diabetes they might face problem of frequent
urination. This can be because when blood sugar level is high, kidney tries to remove the excess
of sugar by filtering it out through urine. So patients must be given education about this situation.
This can support them in enhancing their health outcome. It has also been analysed that patient
suffering from diabetes also faces problem of increased thrust. The frequent urination that is
necessary to remove excess sugar from the blood can result in the body losing additional water
As per the view of Taylor and Barnes, (2019) a productive and efficient diabetes
management requires high level of awareness. Thus it is necessary to control rise and fall of
blood sugar level, weight and other aspects. Along with the dietary plan it is also required that
individuals must be aware of the impact a particular type of food have on sugar level. In addition
to the food type, the combination of food and quantity of different food is also crucial in
regulation of blood sugar level. When clinicians works in team with dieticians they must give
knowledge to patient regarding portion sizes and carbohydrate counting. The vulnerable groups
who are suggested to manage weight must try to plan meal which has balanced components. It is
6
can also work with physicians. Contrary to this Kong and Gregory, (2016) suggested that food
intake and choice of people greatly depends upon local circumstances such as food availability,
cultural and social values as well as economic factors. Health professionals must develop
leadership attributes so that they can lead the health care team and dietary counselling can
become a continuing process. The dietary consideration and meal planning becomes more crucial
element of the management plan for diabetes patients. The health professionals must focus on
even distribution of meal throughout the day, energy intake on routine basis and consistency of
food timings.
Berry, Davies and Dempster, (2019) elucidated that physical activities not only
encourages weight loss but also improve the sensitivity of insulin which lowers the level of
blood glucose. As per the capability and requirement of person dietary treatment must also align
with the exercise and physical activity programs. The people must also be informed about
hypoglycaemia risk and strategies to eliminate its complications. In support to dietary and
exercise management strategies Barnes and Harriss, (2018) believed that for quality health
outcomes oral hypoglycaemia drugs must be considered only when combination of diet and
physical exercise fails to achieve the targets of therapy. Patient must be made aware of signs and
symptoms of diabetes at an early stage. In diabetes they might face problem of frequent
urination. This can be because when blood sugar level is high, kidney tries to remove the excess
of sugar by filtering it out through urine. So patients must be given education about this situation.
This can support them in enhancing their health outcome. It has also been analysed that patient
suffering from diabetes also faces problem of increased thrust. The frequent urination that is
necessary to remove excess sugar from the blood can result in the body losing additional water
As per the view of Taylor and Barnes, (2019) a productive and efficient diabetes
management requires high level of awareness. Thus it is necessary to control rise and fall of
blood sugar level, weight and other aspects. Along with the dietary plan it is also required that
individuals must be aware of the impact a particular type of food have on sugar level. In addition
to the food type, the combination of food and quantity of different food is also crucial in
regulation of blood sugar level. When clinicians works in team with dieticians they must give
knowledge to patient regarding portion sizes and carbohydrate counting. The vulnerable groups
who are suggested to manage weight must try to plan meal which has balanced components. It is
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
the responsibility of the health professionals to ensure that t here is coordination between insulin
or other diabetes medication and the diet taken so that sugar levels remains within normal range.
Goode and Hoover, (2018) believed that though physical activities are suggested by
health professionals but these3 must be commenced with due care. Along with intensive work
outs the light activities such as gardening, walking or being on feet for extended periods can also
help to improve the sugar level. Thus the health professionals must not only focus on diet plan
and medications but also provide a well formulated exercise plan to their patients. The number of
sets for exercise, type of work out and exercise schedule must also be prepared in consultation
with the health professionals.
In the same context Wisting and Snoek, (2019) stated that insulin and other medications
are designed for reducing the blood sugar level when other management interventions are not
sufficient. However the efficiency of medication plan also depends upon their quantity or dosage
and timing. Diabetic patients must have precaution while taking other medications with insulin
dosage. There must be a balance between meal plan and medication dosage. Along with the self
control and monitoring from the patient, health service providers are also responsible for
ensuring the safety and management of diabetes symptoms.
Diabetes management program bring significant changes to life style. Thus individuals
are also required to make their life stress free. According to Preshaw and Bissett, (2019)
practices such as smoking or drinking alcohols can worsen the symptoms of diabetes and can
also encourage the complications of diabetes likes nephropathy. These changes can make
individuals depressed and anxious. Hence for better care it is recommended that along with the
physical symptoms diabetes management must also include psychological aspects such as
depression so that individuals can cooperate and work together with health communities to
manage the progression and symptoms of their diabetic condition. Effective diabetes
management and prevention programs require support from individual, carers, health
professionals and multidisciplinary team which can provide an integrated care to the diabetes
vulnerable groups or patients.
Long term complications and their management
As per Barnard and Breton, (2018) the diabetes mellitus and its life threatening
complications includes a wide range of issues. The key long term complications are related to
eye or visionary issues, cardiovascular diseases as well as kidney issues. The diabetic retinopathy
7
or other diabetes medication and the diet taken so that sugar levels remains within normal range.
Goode and Hoover, (2018) believed that though physical activities are suggested by
health professionals but these3 must be commenced with due care. Along with intensive work
outs the light activities such as gardening, walking or being on feet for extended periods can also
help to improve the sugar level. Thus the health professionals must not only focus on diet plan
and medications but also provide a well formulated exercise plan to their patients. The number of
sets for exercise, type of work out and exercise schedule must also be prepared in consultation
with the health professionals.
In the same context Wisting and Snoek, (2019) stated that insulin and other medications
are designed for reducing the blood sugar level when other management interventions are not
sufficient. However the efficiency of medication plan also depends upon their quantity or dosage
and timing. Diabetic patients must have precaution while taking other medications with insulin
dosage. There must be a balance between meal plan and medication dosage. Along with the self
control and monitoring from the patient, health service providers are also responsible for
ensuring the safety and management of diabetes symptoms.
Diabetes management program bring significant changes to life style. Thus individuals
are also required to make their life stress free. According to Preshaw and Bissett, (2019)
practices such as smoking or drinking alcohols can worsen the symptoms of diabetes and can
also encourage the complications of diabetes likes nephropathy. These changes can make
individuals depressed and anxious. Hence for better care it is recommended that along with the
physical symptoms diabetes management must also include psychological aspects such as
depression so that individuals can cooperate and work together with health communities to
manage the progression and symptoms of their diabetic condition. Effective diabetes
management and prevention programs require support from individual, carers, health
professionals and multidisciplinary team which can provide an integrated care to the diabetes
vulnerable groups or patients.
Long term complications and their management
As per Barnard and Breton, (2018) the diabetes mellitus and its life threatening
complications includes a wide range of issues. The key long term complications are related to
eye or visionary issues, cardiovascular diseases as well as kidney issues. The diabetic retinopathy
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
which is major cause of visual disability is encountered in less than 10 years of insulin dependent
diabetes mellitus. The effective diabetes control can lower the probability of occurrence of
retinopathy. The use of laser photocoagulation on timely diagnosis of retinopathy can be used to
prevent severe visionary loss. The health professionals must refer regular assessment of diabetic
patients so that retinopathy can be detected in the initial stages only. For this purpose retinal
changes, cataract and glaucoma must be detected and treated at the earliest. The treatment must
also emphasis on controlling blood pressure and glycaemia.
According to Sharma, Nazareth and Petersen, (2016) the prime cause of deaths associated
with diabetes is due to diabetic nephropathy. It is significant reason of morbidity and high health
care costs which can also lead to end stage renal issues demanding renal transplantation or
dialysis. The progression of nephropathy can be slowed or prevented by strict glycaemic control,
timely detection of infections, avoidance of nephrotoxic drugs and effective treatment plan for
hypertension. Thus in addition to the dietary and medication control health professionals must
also be refereed for assessment of protein levels and microalbuminuna in urine annually. The
service providers and family members must not neglect the symptoms such as foot infections or
early lesions.
Bird and Turner, (2016) elucidated that after nephropathy, the cardiovascular diseases
(CVD) such as strokes, coronary heart diseases are also responsible for deaths among diabetic
population. The screening of early signs for the CVD must be performed. The management plan
must include activities which promote physical exercises, weight management interventions,
correction of CVD risk factors and cessation of smoking and alcohol. The hypertension can also
enhance the vulnerability and the severity of the diabetes risk factors.
PROJECT PLAN
Budget
The major expenses of the project will be in data collection and implementation of
management strategies such as promotional events for increasing awareness about diabetes and
to provide necessary support services to the patients. The total cost estimated for the project is
£2000. This total project cost also includes cost for internet, secondary data sources like books,
journals and printing costs.
8
diabetes mellitus. The effective diabetes control can lower the probability of occurrence of
retinopathy. The use of laser photocoagulation on timely diagnosis of retinopathy can be used to
prevent severe visionary loss. The health professionals must refer regular assessment of diabetic
patients so that retinopathy can be detected in the initial stages only. For this purpose retinal
changes, cataract and glaucoma must be detected and treated at the earliest. The treatment must
also emphasis on controlling blood pressure and glycaemia.
According to Sharma, Nazareth and Petersen, (2016) the prime cause of deaths associated
with diabetes is due to diabetic nephropathy. It is significant reason of morbidity and high health
care costs which can also lead to end stage renal issues demanding renal transplantation or
dialysis. The progression of nephropathy can be slowed or prevented by strict glycaemic control,
timely detection of infections, avoidance of nephrotoxic drugs and effective treatment plan for
hypertension. Thus in addition to the dietary and medication control health professionals must
also be refereed for assessment of protein levels and microalbuminuna in urine annually. The
service providers and family members must not neglect the symptoms such as foot infections or
early lesions.
Bird and Turner, (2016) elucidated that after nephropathy, the cardiovascular diseases
(CVD) such as strokes, coronary heart diseases are also responsible for deaths among diabetic
population. The screening of early signs for the CVD must be performed. The management plan
must include activities which promote physical exercises, weight management interventions,
correction of CVD risk factors and cessation of smoking and alcohol. The hypertension can also
enhance the vulnerability and the severity of the diabetes risk factors.
PROJECT PLAN
Budget
The major expenses of the project will be in data collection and implementation of
management strategies such as promotional events for increasing awareness about diabetes and
to provide necessary support services to the patients. The total cost estimated for the project is
£2000. This total project cost also includes cost for internet, secondary data sources like books,
journals and printing costs.
8
Project plan
To evaluate the learnings from the diabetes management project, plan-do-study-act
(PDSA) model is used. Various stages of this model are as follows:
Plan: In this phase of project management strategies, purpose and objectives are planned. The
outcomes will be measured in terms of number of patients, sugar level and other health
parameters of the patients, cost reduction and reduced hospital admissions.
Do: In this stage project activities are implemented and activities are executed to manage the
disease and health outcomes of the patients. An effective interaction is also made with the
patients so that their issues can be resolved and needs can be fulfilled.
Study: In this stage outcomes are monitored and evaluated so that actual outcomes of the project
are compared with planned target. The evaluation is also helpful to evaluate the various
challenges which can affect the future stages or outcomes of the project.
Act: In the last phase of the project conclusions are made if integration of leadership and
management approaches have succeeded in diabetes controlling or not. The stage also guides
health professionals to analyse if patients needs are taken into account or not for the better health
care service delivery.
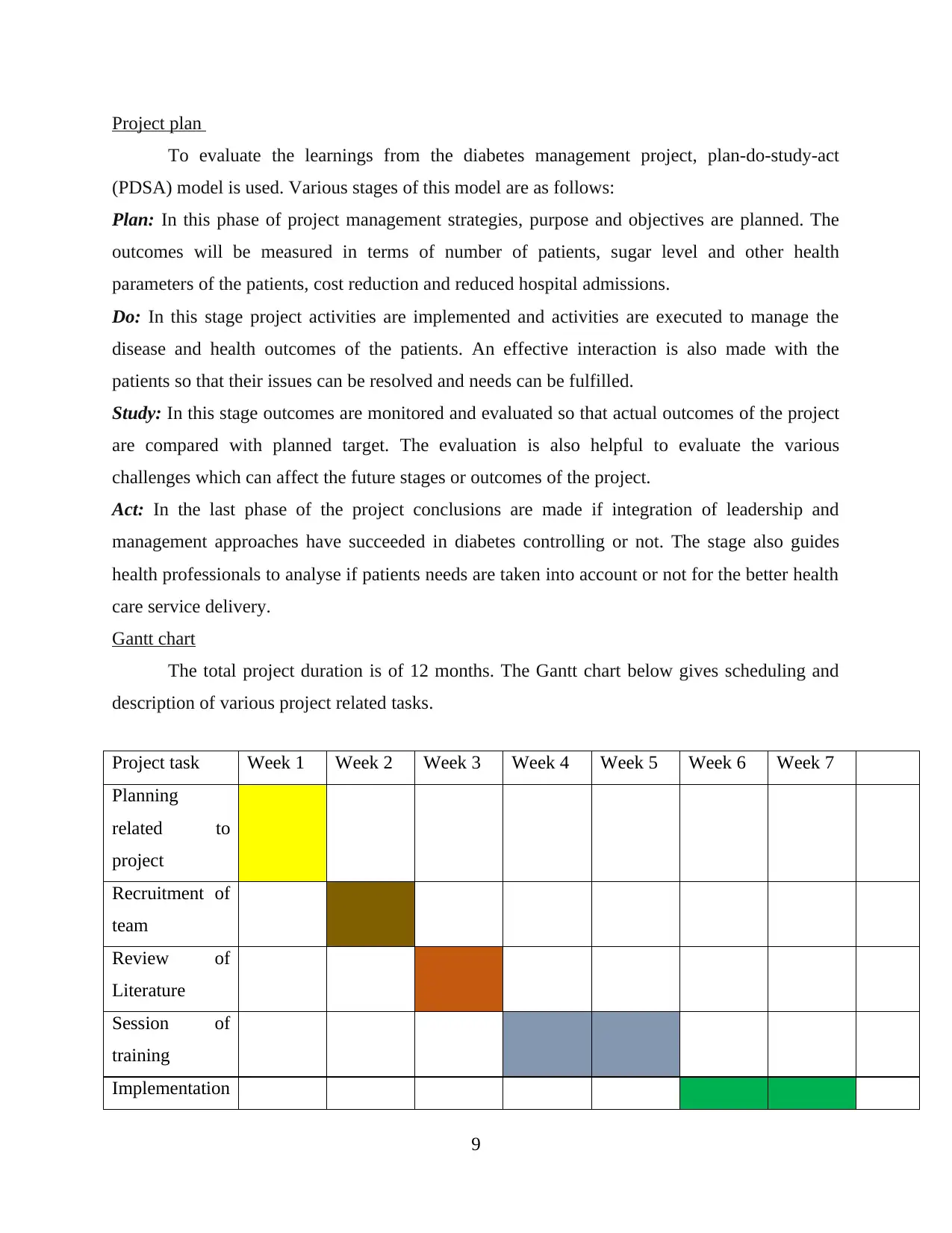
Gantt chart
The total project duration is of 12 months. The Gantt chart below gives scheduling and
description of various project related tasks.
Project task Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7
Planning
related to
project
Recruitment of
team
Review of
Literature
Session of
training
Implementation
9
To evaluate the learnings from the diabetes management project, plan-do-study-act
(PDSA) model is used. Various stages of this model are as follows:
Plan: In this phase of project management strategies, purpose and objectives are planned. The
outcomes will be measured in terms of number of patients, sugar level and other health
parameters of the patients, cost reduction and reduced hospital admissions.
Do: In this stage project activities are implemented and activities are executed to manage the
disease and health outcomes of the patients. An effective interaction is also made with the
patients so that their issues can be resolved and needs can be fulfilled.
Study: In this stage outcomes are monitored and evaluated so that actual outcomes of the project
are compared with planned target. The evaluation is also helpful to evaluate the various
challenges which can affect the future stages or outcomes of the project.
Act: In the last phase of the project conclusions are made if integration of leadership and
management approaches have succeeded in diabetes controlling or not. The stage also guides
health professionals to analyse if patients needs are taken into account or not for the better health
care service delivery.
Gantt chart
The total project duration is of 12 months. The Gantt chart below gives scheduling and
description of various project related tasks.
Project task Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7
Planning
related to
project
Recruitment of
team
Review of
Literature
Session of
training
Implementation
9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 27
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.