Evolution of Total Knee Replacement Methods
VerifiedAdded on 2022/11/26
|20
|4301
|293
AI Summary
This paper evaluates the procedure for total knee replacement methods in detail. It discusses the history, design, and considerations of total knee replacement, including cementless vs. cemented, symmetrical vs. asymmetrical, and mobile vs. fixed-bearing designs.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
MASTER PROJECT
By Name
Course
Instructor
Institution
Location
Date
By Name
Course
Instructor
Institution
Location
Date
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
ABSTRACT
Total knee replacement methods have undergone numerous evolutions for the last four decades
to offer an ssurance or improvement of the life of a patient as well as excellent formation of
joint. The need for total knee replacement would raise the increase in the length of life as well as
for the increase in the weight of the patient. Still, numerous patients aged more than 65 of late
take active part in sports and assumes better results as compared to a few years ago at last has to
be taken into consideration in enhance Asiatic demand. This paper evaluates the procedure for
total knee replacement methods in details
Total knee replacement methods have undergone numerous evolutions for the last four decades
to offer an ssurance or improvement of the life of a patient as well as excellent formation of
joint. The need for total knee replacement would raise the increase in the length of life as well as
for the increase in the weight of the patient. Still, numerous patients aged more than 65 of late
take active part in sports and assumes better results as compared to a few years ago at last has to
be taken into consideration in enhance Asiatic demand. This paper evaluates the procedure for
total knee replacement methods in details
INTRODUCTION
The human knee has a major role to play when it comes to human locomotion. The structure as
well as time behavior of the knee during various types of motion illustrate full adaptation of the
human knee to the required purpose. The knee largest has been established to be the largest joint
in the body and one that is most heavily loaded. The knee incorporates the largest bone in the
human skeleton called the femur and tibia. Another important part of the knees is the patella
mostly when it comes to extended position of joint. The lateral as well as the medial meniscus
makes up the articular surface of tibia bone. Procedures for total knee replacement changed in
the last four decades to assure enhancement in the implants of life as well as an ideal
functionality for patient along a reduction in cost (Bali et al., 2016).
The need for total knee replacement would raise the increase in the length of life as well as for
the increase in the weight of the patient. Still, numerous patients aged more than 65 of late take
active part in sports and assumes better results as compared to a few years ago at last has to be
taken into consideration in enhance Asiatic demand. Evolution of design in total knee
replacement has to meet such new necessities, the anatomic congruence, reduced wear,
articollarity as well as enhanced resistance to weight as well as to reduction of cost and stress.
LITERATURE REVIEW
Total knee replacement history
The initial models of total knee replacement, generated to copy the knee traces back to the XIX
century. The initial trial to come up with an artificial knee was done in 1860 by Vernueli who
made use of articular capsule in the recreation of a joint. Upon the initial attempt, there were
numerous other experiments carried out using various materials.
The human knee has a major role to play when it comes to human locomotion. The structure as
well as time behavior of the knee during various types of motion illustrate full adaptation of the
human knee to the required purpose. The knee largest has been established to be the largest joint
in the body and one that is most heavily loaded. The knee incorporates the largest bone in the
human skeleton called the femur and tibia. Another important part of the knees is the patella
mostly when it comes to extended position of joint. The lateral as well as the medial meniscus
makes up the articular surface of tibia bone. Procedures for total knee replacement changed in
the last four decades to assure enhancement in the implants of life as well as an ideal
functionality for patient along a reduction in cost (Bali et al., 2016).
The need for total knee replacement would raise the increase in the length of life as well as for
the increase in the weight of the patient. Still, numerous patients aged more than 65 of late take
active part in sports and assumes better results as compared to a few years ago at last has to be
taken into consideration in enhance Asiatic demand. Evolution of design in total knee
replacement has to meet such new necessities, the anatomic congruence, reduced wear,
articollarity as well as enhanced resistance to weight as well as to reduction of cost and stress.
LITERATURE REVIEW
Total knee replacement history
The initial models of total knee replacement, generated to copy the knee traces back to the XIX
century. The initial trial to come up with an artificial knee was done in 1860 by Vernueli who
made use of articular capsule in the recreation of a joint. Upon the initial attempt, there were
numerous other experiments carried out using various materials.
The initial trials for creation of total knee replacement took place in the early forties, partial
prosthesis that was done on the femoral part of joint. The first models that received a marked
success and a great diffusion were central or other posterior axis. Among the hinge models that
were received thereafter were the Lagrange with central rotating axis as well as the Gueper
(1971) that generated entirely posterior rotating axis (Bali et al., 2016).
There are numerous total knee replacements that are available in the market with each one of
them having its own rationale of design. Various designs of implant are geared toward improving
patient satisfaction through offering close to normal kinematics. The motion of medial
compartment in total knee replacement is often simplified into a ball and socket nevertheless, the
lateral converged femoral condyle in a knee implant surface guided has been designed for the
control of joint motion. The design of the condyle should be done to generate a constant or even
variable distance of bearing between the lateral and medial condyles (Bonnin et al., 2016).
In attaining a close to normal kinematics in total knee replacement, Walker demonstrates that a
knee implant that has media stability as well as lateral mobility features should be designed. For
instance, the SAIPHTM knee that has been designed in such a way that it has a medial pivot
knee kinetic sequence as well as an asymmetric posterior translation of lateral femoral condyle to
imitate motion of natural knee
The stability of SAIPH knee was studied by Shimmin et al. using video-fluoroscopy during four
various activities of bearing weight. They made a conclusion that medially conforming total knee
indicates a medial pivot motion having a tibial internal rotation. Nevertheless, Warth et al.
demonstrated that a medial pivot pattern may not to a significant extent control clinical success
upon total knee replacement based on intraoperative kinematics as well as measurement of
prosthesis that was done on the femoral part of joint. The first models that received a marked
success and a great diffusion were central or other posterior axis. Among the hinge models that
were received thereafter were the Lagrange with central rotating axis as well as the Gueper
(1971) that generated entirely posterior rotating axis (Bali et al., 2016).
There are numerous total knee replacements that are available in the market with each one of
them having its own rationale of design. Various designs of implant are geared toward improving
patient satisfaction through offering close to normal kinematics. The motion of medial
compartment in total knee replacement is often simplified into a ball and socket nevertheless, the
lateral converged femoral condyle in a knee implant surface guided has been designed for the
control of joint motion. The design of the condyle should be done to generate a constant or even
variable distance of bearing between the lateral and medial condyles (Bonnin et al., 2016).
In attaining a close to normal kinematics in total knee replacement, Walker demonstrates that a
knee implant that has media stability as well as lateral mobility features should be designed. For
instance, the SAIPHTM knee that has been designed in such a way that it has a medial pivot
knee kinetic sequence as well as an asymmetric posterior translation of lateral femoral condyle to
imitate motion of natural knee
The stability of SAIPH knee was studied by Shimmin et al. using video-fluoroscopy during four
various activities of bearing weight. They made a conclusion that medially conforming total knee
indicates a medial pivot motion having a tibial internal rotation. Nevertheless, Warth et al.
demonstrated that a medial pivot pattern may not to a significant extent control clinical success
upon total knee replacement based on intraoperative kinematics as well as measurement of
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
modern outcome. They hinted that more and further research is needed in the determination if a
specific kinematic pattern encourages optical clinical outcomes (Bozkurt et al., 2017).
Kim et al made a comparison between high flexion total knee replacement implants alongside
other implants and made a conclusion that there was not any observable improvement in terms
of the range of motion, radiolucent lines incidences as well as clinical outcomes regardless of the
theoretical range of motion benefits of high flexion prosthesis.
The kinetics of knee joint with total knee replacement was studied by Li et al in which they made
a conclusion that the clinical findings after total knee replacement would be under the influence
of such factors as quadriceps contraction, posterior tibiofemoral articular contact stability as well
as preoperative motion range.
Regarding implant to wear, the impact of tibial insert confiruty as well as material on total knee
replacement wear was studied by Abdelgaied et al. where they made a conclusion that the
anticipated lifetime of total knee replacement may be enhanced through less conforming total
knee replacement implants (Ebramzadeh, 2018). Nevertheless, as a result of non-congruent an at
time unstable total knee replacement form, wear remains a constant challenge. It was reported by
Massin that wear may be reduced through enhancing techniques including a choice on the size of
implant, adapted balancing as well as alignment of component.
The results of 126 individually made implants that were customized were compared against 122
standards off shelf implant patients undergoing total knee replacement by Culler et al. They
established that patients treated using customized individually manufactured implants
demonstrated significantly reduced rates of transfusion as well as fewer adverse rates of events
with an increase in the costs. The rates of manipulation and clinical outcomes were evaluated by
specific kinematic pattern encourages optical clinical outcomes (Bozkurt et al., 2017).
Kim et al made a comparison between high flexion total knee replacement implants alongside
other implants and made a conclusion that there was not any observable improvement in terms
of the range of motion, radiolucent lines incidences as well as clinical outcomes regardless of the
theoretical range of motion benefits of high flexion prosthesis.
The kinetics of knee joint with total knee replacement was studied by Li et al in which they made
a conclusion that the clinical findings after total knee replacement would be under the influence
of such factors as quadriceps contraction, posterior tibiofemoral articular contact stability as well
as preoperative motion range.
Regarding implant to wear, the impact of tibial insert confiruty as well as material on total knee
replacement wear was studied by Abdelgaied et al. where they made a conclusion that the
anticipated lifetime of total knee replacement may be enhanced through less conforming total
knee replacement implants (Ebramzadeh, 2018). Nevertheless, as a result of non-congruent an at
time unstable total knee replacement form, wear remains a constant challenge. It was reported by
Massin that wear may be reduced through enhancing techniques including a choice on the size of
implant, adapted balancing as well as alignment of component.
The results of 126 individually made implants that were customized were compared against 122
standards off shelf implant patients undergoing total knee replacement by Culler et al. They
established that patients treated using customized individually manufactured implants
demonstrated significantly reduced rates of transfusion as well as fewer adverse rates of events
with an increase in the costs. The rates of manipulation and clinical outcomes were evaluated by
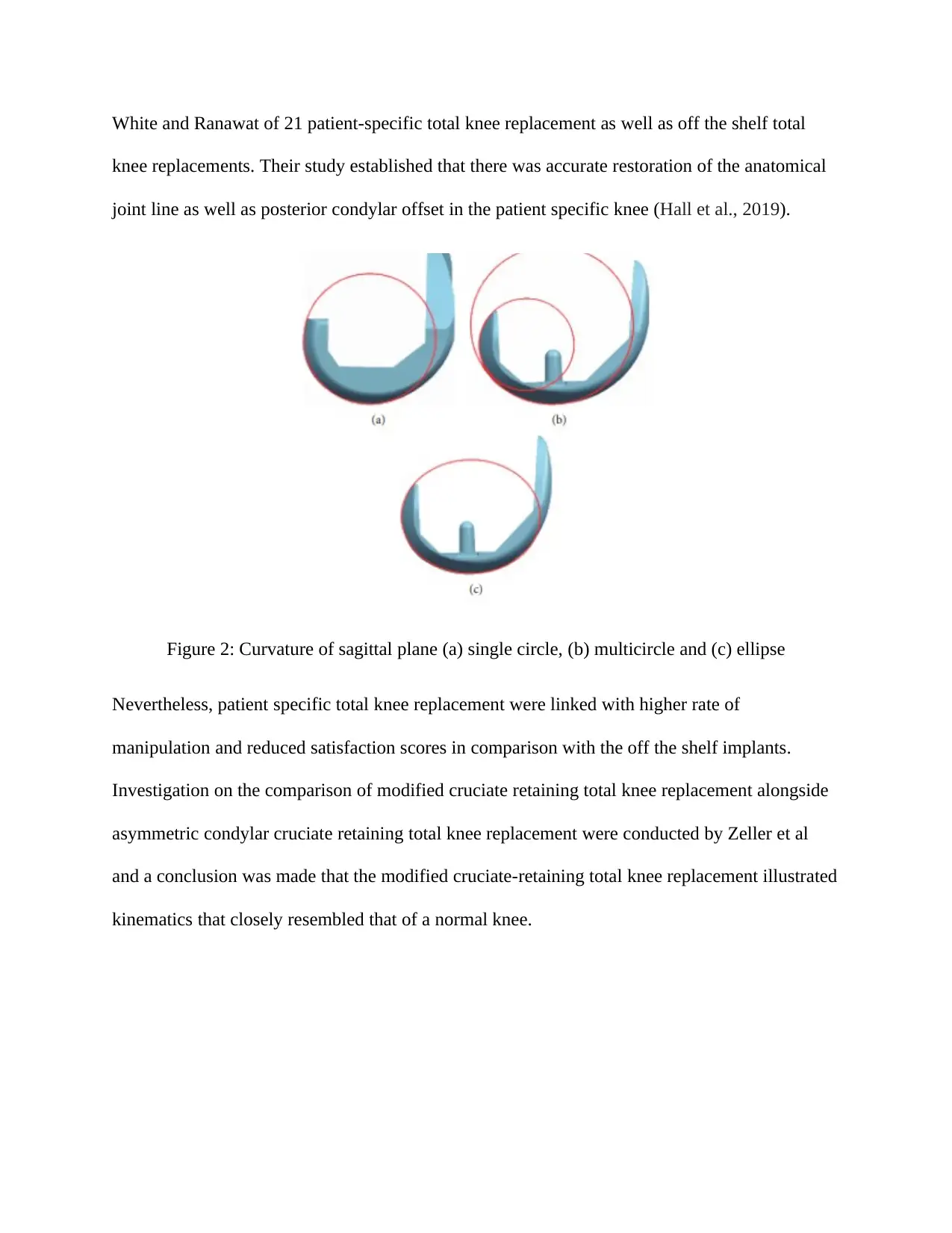
White and Ranawat of 21 patient-specific total knee replacement as well as off the shelf total
knee replacements. Their study established that there was accurate restoration of the anatomical
joint line as well as posterior condylar offset in the patient specific knee (Hall et al., 2019).
Figure 2: Curvature of sagittal plane (a) single circle, (b) multicircle and (c) ellipse
Nevertheless, patient specific total knee replacement were linked with higher rate of
manipulation and reduced satisfaction scores in comparison with the off the shelf implants.
Investigation on the comparison of modified cruciate retaining total knee replacement alongside
asymmetric condylar cruciate retaining total knee replacement were conducted by Zeller et al
and a conclusion was made that the modified cruciate-retaining total knee replacement illustrated
kinematics that closely resembled that of a normal knee.
knee replacements. Their study established that there was accurate restoration of the anatomical
joint line as well as posterior condylar offset in the patient specific knee (Hall et al., 2019).
Figure 2: Curvature of sagittal plane (a) single circle, (b) multicircle and (c) ellipse
Nevertheless, patient specific total knee replacement were linked with higher rate of
manipulation and reduced satisfaction scores in comparison with the off the shelf implants.
Investigation on the comparison of modified cruciate retaining total knee replacement alongside
asymmetric condylar cruciate retaining total knee replacement were conducted by Zeller et al
and a conclusion was made that the modified cruciate-retaining total knee replacement illustrated
kinematics that closely resembled that of a normal knee.

Figure 3: Femoral condyles (a) symmetrical and (b) asymmetrical
Figure 4: Oval curves from femoral bone model (a) sagittal view and (b) isometric view
Numerous researches demonstrated women had relatively narrower distal femoral condyle with
in comparison with men. It was shown by Wise et al. the distal as well as proximal tibial knee
shapes are varied with a difference in sex and a recommendation for further study on gaining an
understanding of the effect of shape modes was made on development of osteoarthritis
(Hamilton et al., 2015). 3D anatomic models were used by Li et al that demonstrate the shape as
well as peak positions of anterior condyle groove have differences in gender and they hinted the
trochlear shape as well as height of medial anterior should be designed in such a way that they
are specific to gender.
Total knee atroplasty: cementless or cementite
Figure 4: Oval curves from femoral bone model (a) sagittal view and (b) isometric view
Numerous researches demonstrated women had relatively narrower distal femoral condyle with
in comparison with men. It was shown by Wise et al. the distal as well as proximal tibial knee
shapes are varied with a difference in sex and a recommendation for further study on gaining an
understanding of the effect of shape modes was made on development of osteoarthritis
(Hamilton et al., 2015). 3D anatomic models were used by Li et al that demonstrate the shape as
well as peak positions of anterior condyle groove have differences in gender and they hinted the
trochlear shape as well as height of medial anterior should be designed in such a way that they
are specific to gender.
Total knee atroplasty: cementless or cementite
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Porous coated design developed was dependent on using polyethylene pegs to evade cement. In
some research, this was an alternative to enhance implant life. The idea was first developed by
Kenna, Hungerford as Krachow. Numerous researches have been carried out to investigate the
best of the designs between the two models. One of such analyzed results done on 143 patients in
which some of the patients had a How Media Porous Coated prosthesis implant while the others
had a cemented design. The findings showed a better knee articularity for the case of the
cemented design; a significant pain incidence as well as the need of making use of crutches for a
greater lapse of time in porous coated design. The major factor in the case as well as other
researches was regarding of re-intervention specially since the tibial component loosening. In
time, enhancement of cemented atroplasty lowered the use of porous coated prosthetic design
(Hamilton et al., 2017).
Total knee atroplasty: asymmetrical or symmetrical
There is yet another subdivision in fixed-bearing prosthesis: symmetrical total knee atroplasty as
well as asymmetrical total knee atroplasty. Symmetrical total knee atroplasty were invented to
lower challenges such as patellar bad-sliding on trochlear groove or even post-operative pain as
well as to enhance articulatory of patients. Kinemax plus is an example which is a symmetrical
prosthesis, asymmetrical prosthesis and evolution of Kinematic. Numerous researches have made
comparisons between the two designs. Symmetrical total knee atroplasty has a design having a
trochlear groove parallel to knee flexion-extension axis as well as deeper to enhance patellar-
prosthesis congruence.
some research, this was an alternative to enhance implant life. The idea was first developed by
Kenna, Hungerford as Krachow. Numerous researches have been carried out to investigate the
best of the designs between the two models. One of such analyzed results done on 143 patients in
which some of the patients had a How Media Porous Coated prosthesis implant while the others
had a cemented design. The findings showed a better knee articularity for the case of the
cemented design; a significant pain incidence as well as the need of making use of crutches for a
greater lapse of time in porous coated design. The major factor in the case as well as other
researches was regarding of re-intervention specially since the tibial component loosening. In
time, enhancement of cemented atroplasty lowered the use of porous coated prosthetic design
(Hamilton et al., 2017).
Total knee atroplasty: asymmetrical or symmetrical
There is yet another subdivision in fixed-bearing prosthesis: symmetrical total knee atroplasty as
well as asymmetrical total knee atroplasty. Symmetrical total knee atroplasty were invented to
lower challenges such as patellar bad-sliding on trochlear groove or even post-operative pain as
well as to enhance articulatory of patients. Kinemax plus is an example which is a symmetrical
prosthesis, asymmetrical prosthesis and evolution of Kinematic. Numerous researches have made
comparisons between the two designs. Symmetrical total knee atroplasty has a design having a
trochlear groove parallel to knee flexion-extension axis as well as deeper to enhance patellar-
prosthesis congruence.
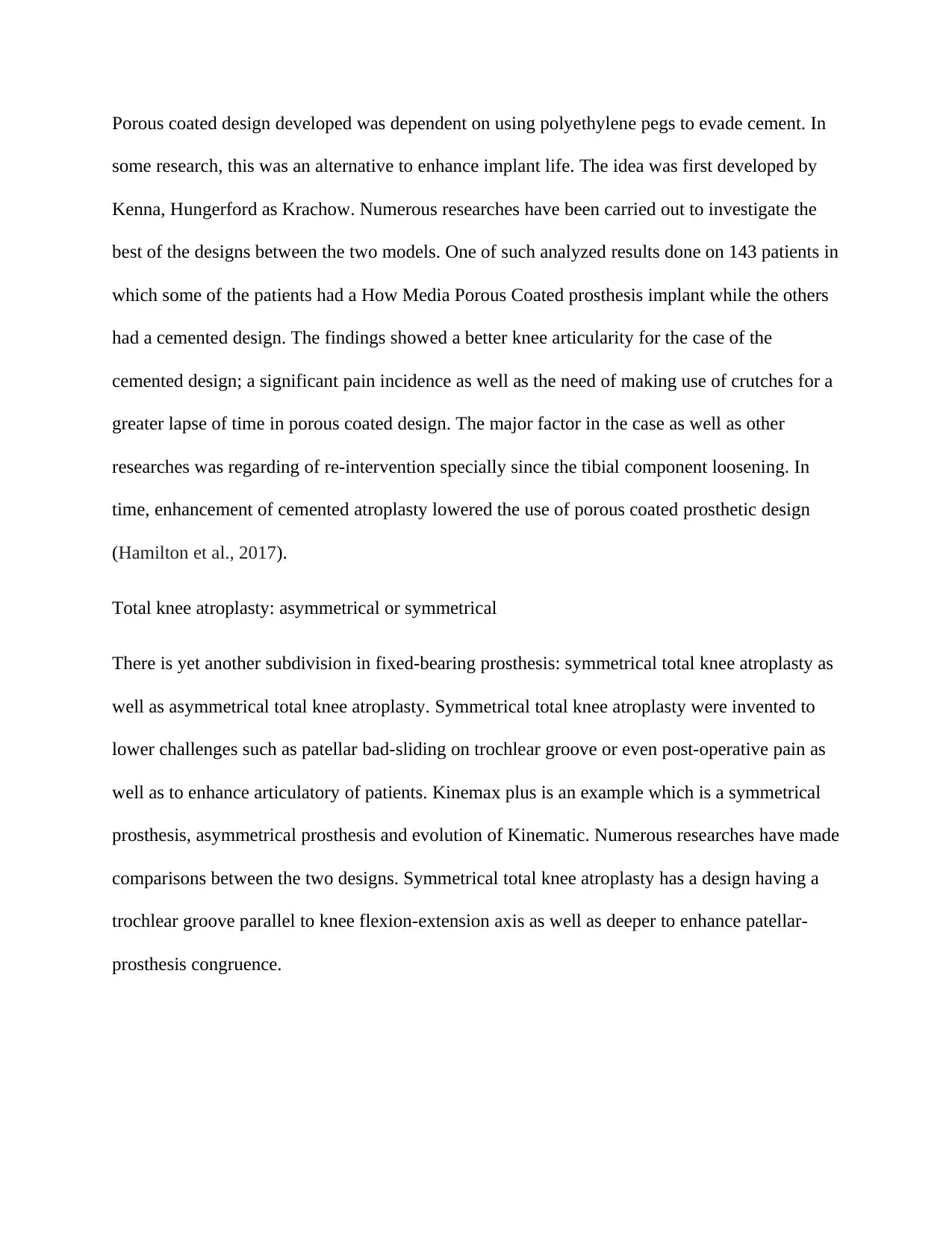
Figure 5: Newman Symmetrical against asymmetrical total knee replacement
Total knee atroplasty: mobile or fixed-bearing
Mobile bearing designs were introduced in the 1970s with the aim of enhancing the area of
contact between tibia and femur as well as lower the load and wearing out of polyethylene. Other
objectives included reduction in the strengths of dislocation in the interface of the bone and
prosthesis as well as allow better freedom of movement. An evolution of the past hinge designs
were presented by the Bousquet-Trillat’s prosthesis that showed rotating movements that could
be accommodative of tibial torsional stresses. Herbert’s prosthesis (1972) that displayed rotating
movements that was a bit different with regard to conception from the conventional hinge
models (Ishikawa et al., 2015).
Due to the fact that hinge models are not respective to normal knee kinematics, they established
indication only in circumstances of extreme knee capsule ligament laxity. Among the first people
to general total knee prosthesis included Gunston in 1965 as per the principle of sliding. The
Total knee atroplasty: mobile or fixed-bearing
Mobile bearing designs were introduced in the 1970s with the aim of enhancing the area of
contact between tibia and femur as well as lower the load and wearing out of polyethylene. Other
objectives included reduction in the strengths of dislocation in the interface of the bone and
prosthesis as well as allow better freedom of movement. An evolution of the past hinge designs
were presented by the Bousquet-Trillat’s prosthesis that showed rotating movements that could
be accommodative of tibial torsional stresses. Herbert’s prosthesis (1972) that displayed rotating
movements that was a bit different with regard to conception from the conventional hinge
models (Ishikawa et al., 2015).
Due to the fact that hinge models are not respective to normal knee kinematics, they established
indication only in circumstances of extreme knee capsule ligament laxity. Among the first people
to general total knee prosthesis included Gunston in 1965 as per the principle of sliding. The
prosthesis enabled a reduced bone resection as well as the lack of constraints allowed the
absorption of the mechanical stresses by apparatus of joint capsule ligaments.
However, with such design the releasing of forces occurred in constrained region of tibial
ephyfisis at risk of implant sinking thus the tendency of construction of unblock bicondylar
sliding prosthesis.
Insall’s Total condylar prosthesis was as well created in 1973 using the Insall and Gunston’s
models most likely having been taken into consideration as the initial modern prosthesis. The
design of Insall’s offered PCL sacrifice as well as stability on the sagittal plane which was
warned by the articular conformation. The total condylar prosthesis design was inclusive of a
chrome cobalt femoral part with symmetrical femoral anterior flanges for the case of patella
articulation.
The femoral condyles that are symmetrical bore reducing sagittal radius of curvature posteriorly
and were each convex in coral plane (Martin et al., 2017). The articular surface which is double
dished of tibial polyethylene part was ideally congruent with femoral part in extension as well as
congruent with regard to coronal plane when it comes to flexion. The anterior as well as
posterior lips of tibial part having a metaphyseal stem were used in the resistance of the
translation as well as location of the parts to avoid tilting of prosthesis when undergoing a
symmetrical loading.
The tibial part was initially entirely polyethylene even though metal backing was later
incorporated to enable more transfer of uniform stress to the underlying cancellous metaphyseal
bone as well as avoid deformation of polyethylene. An all polyethylene patella part having a
dome shape was included in resurfacing on the patella having a central fixation lug. Among the
absorption of the mechanical stresses by apparatus of joint capsule ligaments.
However, with such design the releasing of forces occurred in constrained region of tibial
ephyfisis at risk of implant sinking thus the tendency of construction of unblock bicondylar
sliding prosthesis.
Insall’s Total condylar prosthesis was as well created in 1973 using the Insall and Gunston’s
models most likely having been taken into consideration as the initial modern prosthesis. The
design of Insall’s offered PCL sacrifice as well as stability on the sagittal plane which was
warned by the articular conformation. The total condylar prosthesis design was inclusive of a
chrome cobalt femoral part with symmetrical femoral anterior flanges for the case of patella
articulation.
The femoral condyles that are symmetrical bore reducing sagittal radius of curvature posteriorly
and were each convex in coral plane (Martin et al., 2017). The articular surface which is double
dished of tibial polyethylene part was ideally congruent with femoral part in extension as well as
congruent with regard to coronal plane when it comes to flexion. The anterior as well as
posterior lips of tibial part having a metaphyseal stem were used in the resistance of the
translation as well as location of the parts to avoid tilting of prosthesis when undergoing a
symmetrical loading.
The tibial part was initially entirely polyethylene even though metal backing was later
incorporated to enable more transfer of uniform stress to the underlying cancellous metaphyseal
bone as well as avoid deformation of polyethylene. An all polyethylene patella part having a
dome shape was included in resurfacing on the patella having a central fixation lug. Among the
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
initial criticisms of total knee condylar prosthesis revolved around the tendency of subluxation
posteriority when under flexion in case the flexion gap was not in a perfect balance with regard
to the extension gap as well as a smaller flexion range in comparison with prosthesis designs
which enabled femoral rollback to take place (Miller et al., 2018).
By not being able to roll back, there was impinging of the posterior femoral metaphysis against
tibial articular surface in total condylar knee at about 95 flexion degree. Correction of such
problems saw the development of the Insall-Burstein posterior cruciate stabilized design through
the addition of a mechanism of central cam to articular surface geometry of total condylar
prosthesis. A central post was engaged by the cam on femoral component on tibial articular
surface at about 70 degree of flexion and resulted in the contact point of femoral tibial
articulation being posteriorly displaced thereby having an effect on femoral rollback and
enabling even more flexion.
There was development of cruciate-sacrificing total condylar prosthesis at the same time as the
development of duo patellar prosthesis with sagittal plane contour of femoral part that was
shaped anatomically (Pfitzner et al., 2018). The prosthesis was inclusive of retention of posterior
cruciate ligament. Initially, the lateral as well as medial tibial plateau parts were different even
though this was later revised to a single piece tibial component having a cut-out for retention of
PCL. Most of such design features are maintained in the current designs.
Total knee atroplasty: substitution designs or preservation designs
A great number of total knee replacements these days tend to be fixed bearing i.e. less mobile
bearing, dividing in the middle PLC preservation designs and PLC substitution designs.
Numerous papers were conducted to investigate which of the designs was better to assure
posteriority when under flexion in case the flexion gap was not in a perfect balance with regard
to the extension gap as well as a smaller flexion range in comparison with prosthesis designs
which enabled femoral rollback to take place (Miller et al., 2018).
By not being able to roll back, there was impinging of the posterior femoral metaphysis against
tibial articular surface in total condylar knee at about 95 flexion degree. Correction of such
problems saw the development of the Insall-Burstein posterior cruciate stabilized design through
the addition of a mechanism of central cam to articular surface geometry of total condylar
prosthesis. A central post was engaged by the cam on femoral component on tibial articular
surface at about 70 degree of flexion and resulted in the contact point of femoral tibial
articulation being posteriorly displaced thereby having an effect on femoral rollback and
enabling even more flexion.
There was development of cruciate-sacrificing total condylar prosthesis at the same time as the
development of duo patellar prosthesis with sagittal plane contour of femoral part that was
shaped anatomically (Pfitzner et al., 2018). The prosthesis was inclusive of retention of posterior
cruciate ligament. Initially, the lateral as well as medial tibial plateau parts were different even
though this was later revised to a single piece tibial component having a cut-out for retention of
PCL. Most of such design features are maintained in the current designs.
Total knee atroplasty: substitution designs or preservation designs
A great number of total knee replacements these days tend to be fixed bearing i.e. less mobile
bearing, dividing in the middle PLC preservation designs and PLC substitution designs.
Numerous papers were conducted to investigate which of the designs was better to assure
enhanced results. It was not as easy noting significant variations in the two designs since the
reliability as well as guarantee were similar for the two during the years. Some of the authors
were in preference of CR designs with most of the papers indicating that PCL retaining, assures
strength of extensor apparatus, admits conservation of propriocentvity, and allows easier revision
of the surgery as well as consenting of bone stock preservation with reduced risk of fracture.
Other researchers did not prefer either of the two designs as they generated similar features and
characteristics even as others were in preference with the substitution design (Webb et al., 2017).
For the case of other authors, PLC retaining was not a very useful aspect of knee cinematic as
they suggested it was quite challenging to attain an ideal balance between collateral ligaments as
well as central pivot in CR designs. It was instead noticed by Insall that PS designs had a
relationship with patellar pain, dislocation, malfunction as well as sub-dislocation. Another
research indicated that PS design aided in the transmission of relatively heavier load especially
on the tibial axis which is accompanied with an increase in the wear.
Prosthesis design where both cruciate are not sacrificed is not often used due to the issue with
balance between the four various knee ligaments. The anatomic congruence of the tibial and
femoral tends to be less than CR design in comparison with the PS design allows enhanced ROM
but as well results in a sliding as well as wear stress increment and thus instability of prosthetic
components. Still, a major anatomic congruence results in less knee kinematic variability with
enhanced stability even though this is not a guarantee of enhanced function of the patient neo-
joint.
Rather, notable articular congruence of the PS design on both femoral as well as tibial
component, consenting posterior dislocation of femur during hyper-flexion movements, some
good factor even though consents as well an interior alongside posterior damage for main wear
reliability as well as guarantee were similar for the two during the years. Some of the authors
were in preference of CR designs with most of the papers indicating that PCL retaining, assures
strength of extensor apparatus, admits conservation of propriocentvity, and allows easier revision
of the surgery as well as consenting of bone stock preservation with reduced risk of fracture.
Other researchers did not prefer either of the two designs as they generated similar features and
characteristics even as others were in preference with the substitution design (Webb et al., 2017).
For the case of other authors, PLC retaining was not a very useful aspect of knee cinematic as
they suggested it was quite challenging to attain an ideal balance between collateral ligaments as
well as central pivot in CR designs. It was instead noticed by Insall that PS designs had a
relationship with patellar pain, dislocation, malfunction as well as sub-dislocation. Another
research indicated that PS design aided in the transmission of relatively heavier load especially
on the tibial axis which is accompanied with an increase in the wear.
Prosthesis design where both cruciate are not sacrificed is not often used due to the issue with
balance between the four various knee ligaments. The anatomic congruence of the tibial and
femoral tends to be less than CR design in comparison with the PS design allows enhanced ROM
but as well results in a sliding as well as wear stress increment and thus instability of prosthetic
components. Still, a major anatomic congruence results in less knee kinematic variability with
enhanced stability even though this is not a guarantee of enhanced function of the patient neo-
joint.
Rather, notable articular congruence of the PS design on both femoral as well as tibial
component, consenting posterior dislocation of femur during hyper-flexion movements, some
good factor even though consents as well an interior alongside posterior damage for main wear
which in some cases evolves to form a fracture. Still femoral resection needed to generate a
femoral housing may become a challenge for smaller knee. Finally both CR and PS there is in
addition tibial wear between tibial metal as well bearing metal which is a challenge suppose
there is inadequate prosthesis locking.
Methodology
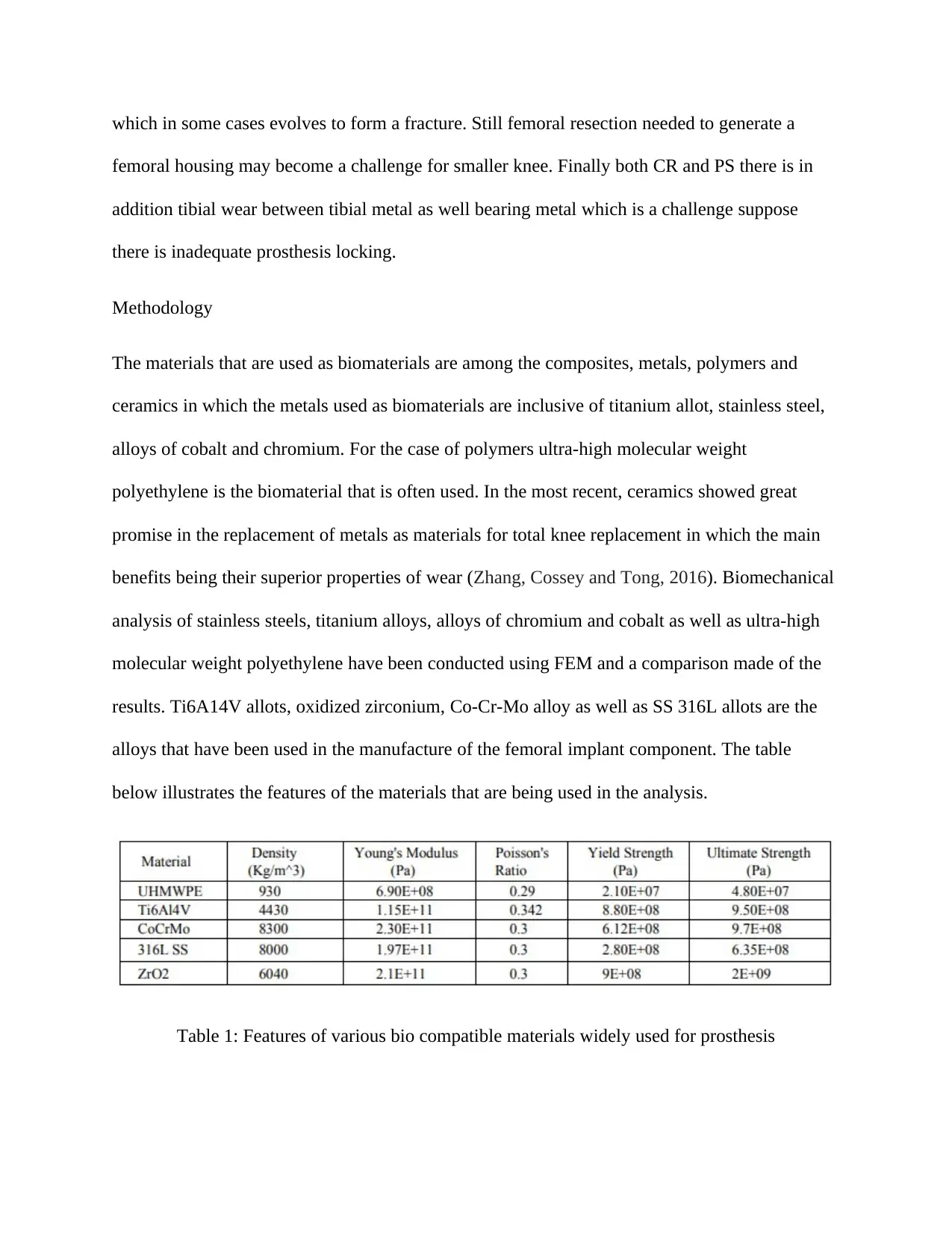
The materials that are used as biomaterials are among the composites, metals, polymers and
ceramics in which the metals used as biomaterials are inclusive of titanium allot, stainless steel,
alloys of cobalt and chromium. For the case of polymers ultra-high molecular weight
polyethylene is the biomaterial that is often used. In the most recent, ceramics showed great
promise in the replacement of metals as materials for total knee replacement in which the main
benefits being their superior properties of wear (Zhang, Cossey and Tong, 2016). Biomechanical
analysis of stainless steels, titanium alloys, alloys of chromium and cobalt as well as ultra-high
molecular weight polyethylene have been conducted using FEM and a comparison made of the
results. Ti6A14V allots, oxidized zirconium, Co-Cr-Mo alloy as well as SS 316L allots are the
alloys that have been used in the manufacture of the femoral implant component. The table
below illustrates the features of the materials that are being used in the analysis.
Table 1: Features of various bio compatible materials widely used for prosthesis
femoral housing may become a challenge for smaller knee. Finally both CR and PS there is in
addition tibial wear between tibial metal as well bearing metal which is a challenge suppose
there is inadequate prosthesis locking.
Methodology
The materials that are used as biomaterials are among the composites, metals, polymers and
ceramics in which the metals used as biomaterials are inclusive of titanium allot, stainless steel,
alloys of cobalt and chromium. For the case of polymers ultra-high molecular weight
polyethylene is the biomaterial that is often used. In the most recent, ceramics showed great
promise in the replacement of metals as materials for total knee replacement in which the main
benefits being their superior properties of wear (Zhang, Cossey and Tong, 2016). Biomechanical
analysis of stainless steels, titanium alloys, alloys of chromium and cobalt as well as ultra-high
molecular weight polyethylene have been conducted using FEM and a comparison made of the
results. Ti6A14V allots, oxidized zirconium, Co-Cr-Mo alloy as well as SS 316L allots are the
alloys that have been used in the manufacture of the femoral implant component. The table
below illustrates the features of the materials that are being used in the analysis.
Table 1: Features of various bio compatible materials widely used for prosthesis
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Procedure
CAD Modeling
The performance of prosthesis is to a great extent influenced by its geometry hence the need of
settling for the standard procedure in modeling the prosthesis. The various mechanical designs
are modelled using the pro/engineer as well as for conducting associated manufacturing as well
as design applications. PRO-E 5.0 was used in the development of the geometrical models.
Figure 6: 2D femur mode
Figure 7: 2D tibia module
CAD Modeling
The performance of prosthesis is to a great extent influenced by its geometry hence the need of
settling for the standard procedure in modeling the prosthesis. The various mechanical designs
are modelled using the pro/engineer as well as for conducting associated manufacturing as well
as design applications. PRO-E 5.0 was used in the development of the geometrical models.
Figure 6: 2D femur mode
Figure 7: 2D tibia module
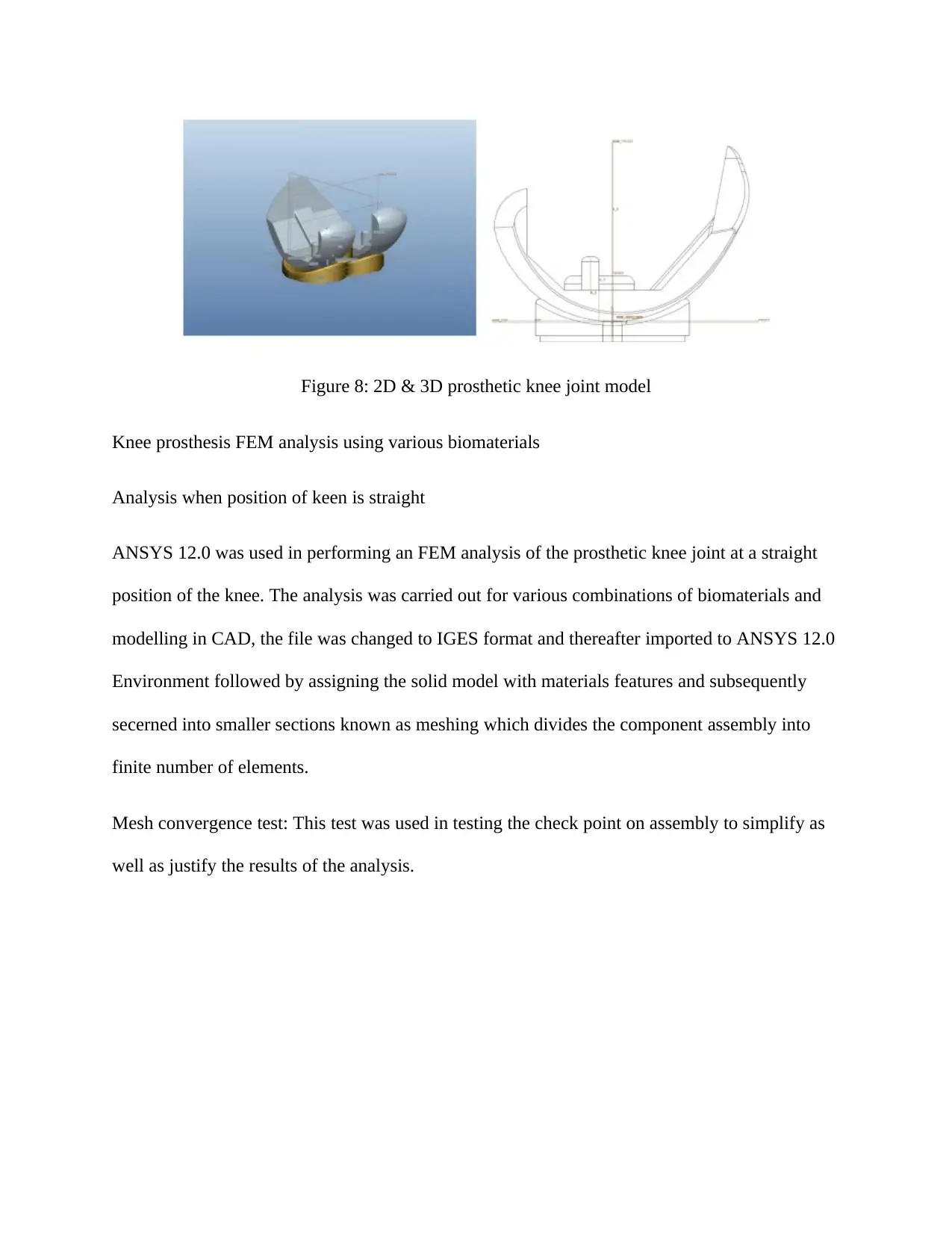
Figure 8: 2D & 3D prosthetic knee joint model
Knee prosthesis FEM analysis using various biomaterials
Analysis when position of keen is straight
ANSYS 12.0 was used in performing an FEM analysis of the prosthetic knee joint at a straight
position of the knee. The analysis was carried out for various combinations of biomaterials and
modelling in CAD, the file was changed to IGES format and thereafter imported to ANSYS 12.0
Environment followed by assigning the solid model with materials features and subsequently
secerned into smaller sections known as meshing which divides the component assembly into
finite number of elements.
Mesh convergence test: This test was used in testing the check point on assembly to simplify as
well as justify the results of the analysis.
Knee prosthesis FEM analysis using various biomaterials
Analysis when position of keen is straight
ANSYS 12.0 was used in performing an FEM analysis of the prosthetic knee joint at a straight
position of the knee. The analysis was carried out for various combinations of biomaterials and
modelling in CAD, the file was changed to IGES format and thereafter imported to ANSYS 12.0
Environment followed by assigning the solid model with materials features and subsequently
secerned into smaller sections known as meshing which divides the component assembly into
finite number of elements.
Mesh convergence test: This test was used in testing the check point on assembly to simplify as
well as justify the results of the analysis.
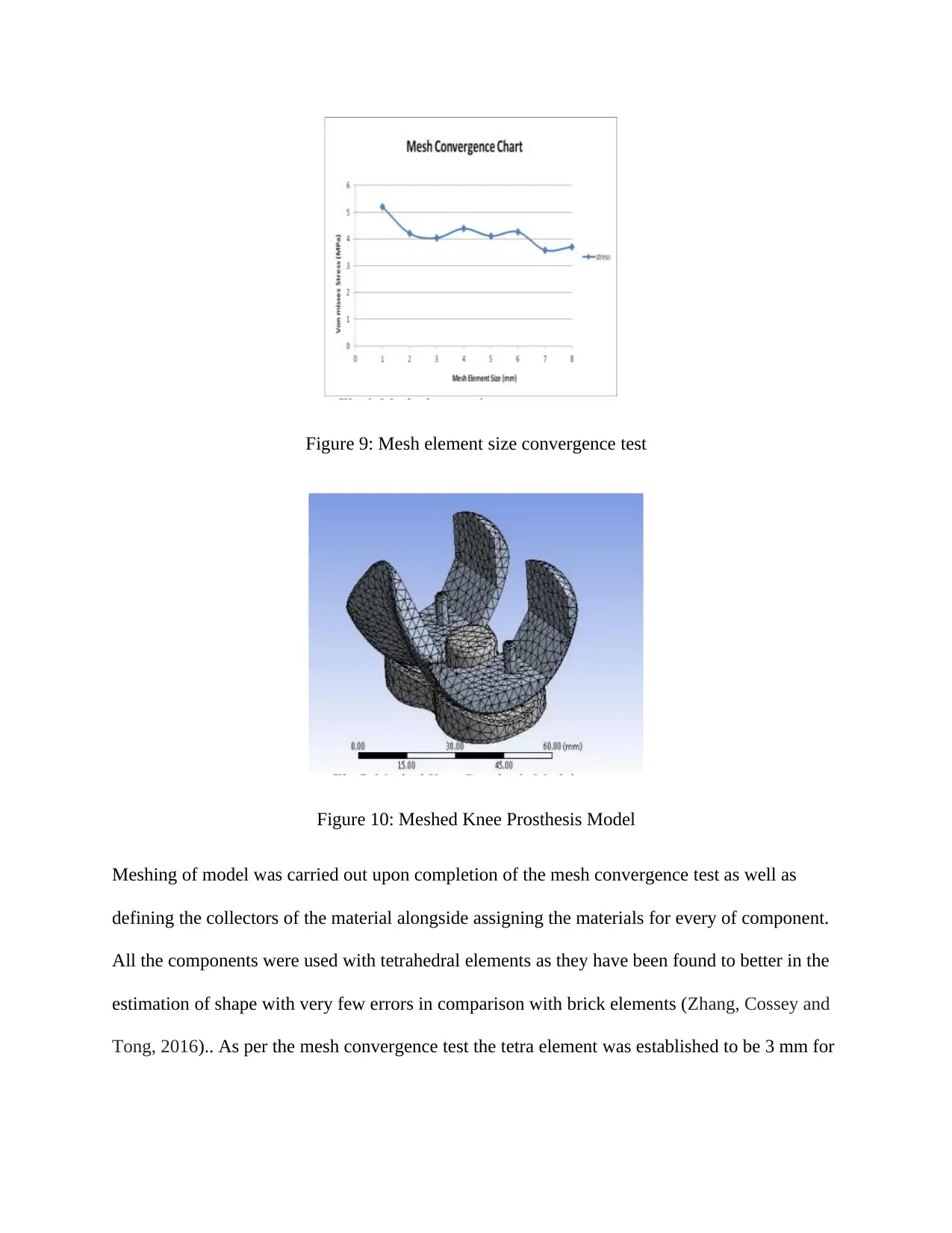
Figure 9: Mesh element size convergence test
Figure 10: Meshed Knee Prosthesis Model
Meshing of model was carried out upon completion of the mesh convergence test as well as
defining the collectors of the material alongside assigning the materials for every of component.
All the components were used with tetrahedral elements as they have been found to better in the
estimation of shape with very few errors in comparison with brick elements (Zhang, Cossey and
Tong, 2016).. As per the mesh convergence test the tetra element was established to be 3 mm for
Figure 10: Meshed Knee Prosthesis Model
Meshing of model was carried out upon completion of the mesh convergence test as well as
defining the collectors of the material alongside assigning the materials for every of component.
All the components were used with tetrahedral elements as they have been found to better in the
estimation of shape with very few errors in comparison with brick elements (Zhang, Cossey and
Tong, 2016).. As per the mesh convergence test the tetra element was established to be 3 mm for
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
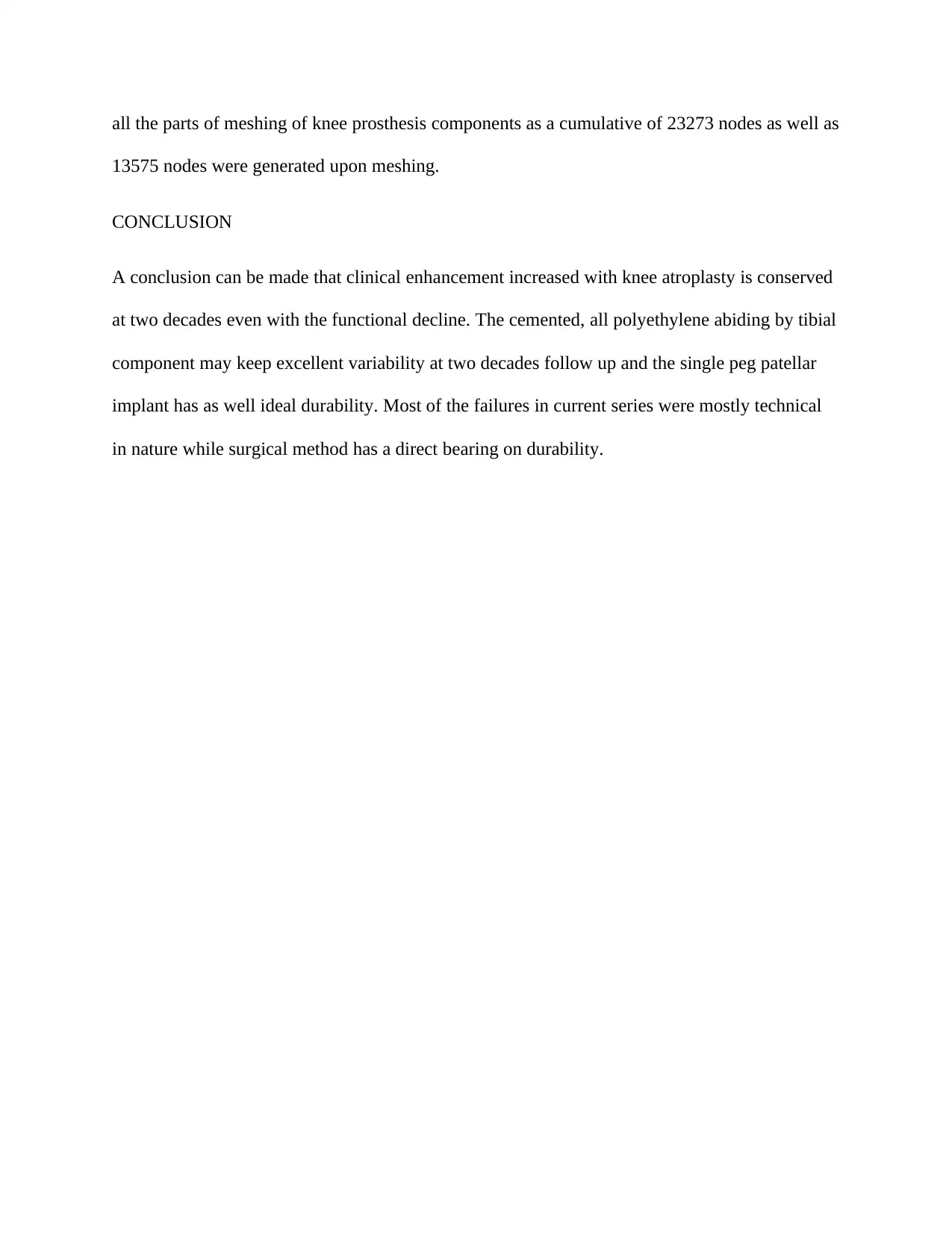
all the parts of meshing of knee prosthesis components as a cumulative of 23273 nodes as well as
13575 nodes were generated upon meshing.
CONCLUSION
A conclusion can be made that clinical enhancement increased with knee atroplasty is conserved
at two decades even with the functional decline. The cemented, all polyethylene abiding by tibial
component may keep excellent variability at two decades follow up and the single peg patellar
implant has as well ideal durability. Most of the failures in current series were mostly technical
in nature while surgical method has a direct bearing on durability.
13575 nodes were generated upon meshing.
CONCLUSION
A conclusion can be made that clinical enhancement increased with knee atroplasty is conserved
at two decades even with the functional decline. The cemented, all polyethylene abiding by tibial
component may keep excellent variability at two decades follow up and the single peg patellar
implant has as well ideal durability. Most of the failures in current series were mostly technical
in nature while surgical method has a direct bearing on durability.
References
Ansari, F., Lee, T., Malito, L., Martin, A., Gunther, S.B., Harmsen, S., Norris, T.R., Ries, M.,
Van Citters, D. and Pruitt, L., 2016. Analysis of severely fractured glenoid components: clinical
consequences of biomechanics, design, and materials selection on implant performance. Journal
of shoulder and elbow surgery, 25(7), pp.1041-1050
Bali, K., Naudie, D.D., Howard, J.L., McCalden, R.W., MacDonald, S.J. and Teeter, M.G., 2016.
Comparison of tibial insert polyethylene damage in rotating hinge and highly constrained total
knee arthroplasty: a retrieval analysis. The Journal of arthroplasty, 31(1), pp.290-294
Bonnin, M.P., Saffarini, M., Bossard, N., Dantony, E. and Victor, J., 2016. Morphometric
analysis of the distal femur in total knee arthroplasty and native knees. The bone & joint
journal, 98(1), pp.49-57
Bozkurt, M., Tahta, M., Gursoy, S. and Akkaya, M., 2017. Total and intercondylar notch bone
resection in posterior stabilized knee arthroplasty: analysis of five manufacturer designs. Knee
Surgery, Sports Traumatology, Arthroscopy, 25(6), pp.1731-1735
Ebramzadeh, E., 2018. CORR Insights®: Current Total Knee Designs: Does Baseplate
Roughness or Locking Mechanism Design Affect Polyethylene Backside Wear?. Clinical
orthopaedics and related research, 476(3), p.615
Hall, R.K., Ewing, J.A., Beal, M.D., Manning, D.W. and Siston, R.A., 2019. Medially‐stabilized
total knee arthroplasty does not alter knee laxity and balance in cadaveric knees. Journal of
Orthopaedic Research®, 37(2), pp.335-349
Ansari, F., Lee, T., Malito, L., Martin, A., Gunther, S.B., Harmsen, S., Norris, T.R., Ries, M.,
Van Citters, D. and Pruitt, L., 2016. Analysis of severely fractured glenoid components: clinical
consequences of biomechanics, design, and materials selection on implant performance. Journal
of shoulder and elbow surgery, 25(7), pp.1041-1050
Bali, K., Naudie, D.D., Howard, J.L., McCalden, R.W., MacDonald, S.J. and Teeter, M.G., 2016.
Comparison of tibial insert polyethylene damage in rotating hinge and highly constrained total
knee arthroplasty: a retrieval analysis. The Journal of arthroplasty, 31(1), pp.290-294
Bonnin, M.P., Saffarini, M., Bossard, N., Dantony, E. and Victor, J., 2016. Morphometric
analysis of the distal femur in total knee arthroplasty and native knees. The bone & joint
journal, 98(1), pp.49-57
Bozkurt, M., Tahta, M., Gursoy, S. and Akkaya, M., 2017. Total and intercondylar notch bone
resection in posterior stabilized knee arthroplasty: analysis of five manufacturer designs. Knee
Surgery, Sports Traumatology, Arthroscopy, 25(6), pp.1731-1735
Ebramzadeh, E., 2018. CORR Insights®: Current Total Knee Designs: Does Baseplate
Roughness or Locking Mechanism Design Affect Polyethylene Backside Wear?. Clinical
orthopaedics and related research, 476(3), p.615
Hall, R.K., Ewing, J.A., Beal, M.D., Manning, D.W. and Siston, R.A., 2019. Medially‐stabilized
total knee arthroplasty does not alter knee laxity and balance in cadaveric knees. Journal of
Orthopaedic Research®, 37(2), pp.335-349
Hamilton, D.F., Burnett, R., Patton, J.T., Howie, C.R., Moran, M., Simpson, A.H.R.W. and
Gaston, P., 2015. Implant design influences patient outcome after total knee arthroplasty: a
prospective double-blind randomised controlled trial. The bone & joint journal, 97(1), pp.64-70
Hamilton, W.G., Ammeen, D.J., Parks, N.L., Goyal, N., Engh, G.A. and Engh Jr, C.A., 2017.
Patellar cut and composite thickness: the influence on postoperative motion and complications in
total knee arthroplasty. The Journal of arthroplasty, 32(6), pp.1803-1807
Ishikawa, M., Kuriyama, S., Ito, H., Furu, M., Nakamura, S. and Matsuda, S., 2015. Kinematic
alignment produces near-normal knee motion but increases contact stress after total knee
arthroplasty: a case study on a single implant design. The Knee, 22(3), pp.206-212
Martin, J.R., Jennings, J.M., Watters, T.S., Levy, D.L., McNabb, D.C. and Dennis, D.A., 2017.
Femoral implant design modification decreases the incidence of patellar crepitus in total knee
arthroplasty. The Journal of arthroplasty, 32(4), pp.1310-1313
Miller, A.J., Stimac, J.D., Smith, L.S., Feher, A.W., Yakkanti, M.R. and Malkani, A.L., 2018.
Results of cemented vs cementless primary total knee arthroplasty using the same implant
design. The Journal of arthroplasty, 33(4), pp.1089-1093
Pfitzner, T., Moewis, P., Stein, P., Boeth, H., Trepczynski, A., von Roth, P. and Duda, G.N.,
2018. Modifications of femoral component design in multi-radius total knee arthroplasty lead to
higher lateral posterior femoro-tibial translation. Knee Surgery, Sports Traumatology,
Arthroscopy, 26(6), pp.1645-1655
Webb, J.E., Yang, H.Y., Collins, J.E., Losina, E., Thornhill, T.S. and Katz, J.N., 2017. The
evolution of implant design decreases the incidence of lateral release in primary total knee
arthroplasty. The Journal of arthroplasty, 32(5), pp.1505-1509
Gaston, P., 2015. Implant design influences patient outcome after total knee arthroplasty: a
prospective double-blind randomised controlled trial. The bone & joint journal, 97(1), pp.64-70
Hamilton, W.G., Ammeen, D.J., Parks, N.L., Goyal, N., Engh, G.A. and Engh Jr, C.A., 2017.
Patellar cut and composite thickness: the influence on postoperative motion and complications in
total knee arthroplasty. The Journal of arthroplasty, 32(6), pp.1803-1807
Ishikawa, M., Kuriyama, S., Ito, H., Furu, M., Nakamura, S. and Matsuda, S., 2015. Kinematic
alignment produces near-normal knee motion but increases contact stress after total knee
arthroplasty: a case study on a single implant design. The Knee, 22(3), pp.206-212
Martin, J.R., Jennings, J.M., Watters, T.S., Levy, D.L., McNabb, D.C. and Dennis, D.A., 2017.
Femoral implant design modification decreases the incidence of patellar crepitus in total knee
arthroplasty. The Journal of arthroplasty, 32(4), pp.1310-1313
Miller, A.J., Stimac, J.D., Smith, L.S., Feher, A.W., Yakkanti, M.R. and Malkani, A.L., 2018.
Results of cemented vs cementless primary total knee arthroplasty using the same implant
design. The Journal of arthroplasty, 33(4), pp.1089-1093
Pfitzner, T., Moewis, P., Stein, P., Boeth, H., Trepczynski, A., von Roth, P. and Duda, G.N.,
2018. Modifications of femoral component design in multi-radius total knee arthroplasty lead to
higher lateral posterior femoro-tibial translation. Knee Surgery, Sports Traumatology,
Arthroscopy, 26(6), pp.1645-1655
Webb, J.E., Yang, H.Y., Collins, J.E., Losina, E., Thornhill, T.S. and Katz, J.N., 2017. The
evolution of implant design decreases the incidence of lateral release in primary total knee
arthroplasty. The Journal of arthroplasty, 32(5), pp.1505-1509
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Zhang, Q.H., Cossey, A. and Tong, J., 2016. Stress shielding in periprosthetic bone following a
total knee replacement: effects of implant material, design and alignment. Medical engineering
& physics, 38(12), pp.1481-1488
total knee replacement: effects of implant material, design and alignment. Medical engineering
& physics, 38(12), pp.1481-1488
1 out of 20
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.