Mechanism of Action of Liraglutide Drug: A Detailed Analysis
VerifiedAdded on 2020/04/07
|10
|2495
|209
Report
AI Summary
This report provides a comprehensive analysis of Liraglutide, a GLP-1 receptor agonist used in the treatment of diabetes and for weight management. It details the drug's mechanism of action, including its effects on gastric emptying, appetite suppression, and activation of brain cells. The report also examines how Liraglutide upregulates intracellular cAMP and suppresses glucagon hormone secretion. Furthermore, it presents findings from Phase III clinical trials, highlighting the drug's efficacy and safety, including dosage recommendations and common side effects. The report concludes by emphasizing the benefits of Liraglutide in improving obesity-related parameters and cardiovascular health, while also acknowledging the need for further research to fully elucidate its mechanism of action. The document also references several studies and clinical trials that support the findings.
MECHANISM OF ACTION OF LIRAGLUTIDE DRUG 1
Name
Institution
Tutor
Course
Date of submission
MECHANISM OF ACTION OF LIRAGLUTIDE DRUG
Introduction
Metabolic diseases have become a major concern worldwide. Many people both young and
adults are suffering from diabetes and obesity. Weight management has, therefore, become
crucial in obese people and diabetic patients. Liraglutide is a receptor agonist and an analog of
(GLP-1 (7-37), glucagon-like peptide-1. It is also a naturally occurring human peptide, and an
analog for Arg34-GLP-1 which is replaced by Glu spaced palmitic acid on the -amino group
(Nuffer and Trujillo, p. 929) of lysine at position 26. It’s a fatty acylated GLP-1 analog which is
long-acting with a half-life of about 11-15 hours. It is administered subcutaneously in the
treatment of diabetes mellitus as a supplemental agent as well as in weight control management
of overweight and diabetic patients. It has been known to help people shed excess weight
especially those who have Body Mass Index (BMI) of ≥ 27 (overweight) and ≥ 30 (obese).
Name
Institution
Tutor
Course
Date of submission
MECHANISM OF ACTION OF LIRAGLUTIDE DRUG
Introduction
Metabolic diseases have become a major concern worldwide. Many people both young and
adults are suffering from diabetes and obesity. Weight management has, therefore, become
crucial in obese people and diabetic patients. Liraglutide is a receptor agonist and an analog of
(GLP-1 (7-37), glucagon-like peptide-1. It is also a naturally occurring human peptide, and an
analog for Arg34-GLP-1 which is replaced by Glu spaced palmitic acid on the -amino group
(Nuffer and Trujillo, p. 929) of lysine at position 26. It’s a fatty acylated GLP-1 analog which is
long-acting with a half-life of about 11-15 hours. It is administered subcutaneously in the
treatment of diabetes mellitus as a supplemental agent as well as in weight control management
of overweight and diabetic patients. It has been known to help people shed excess weight
especially those who have Body Mass Index (BMI) of ≥ 27 (overweight) and ≥ 30 (obese).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
MECHANISM OF ACTION OF LIRAGLUTIDE DRUG 2
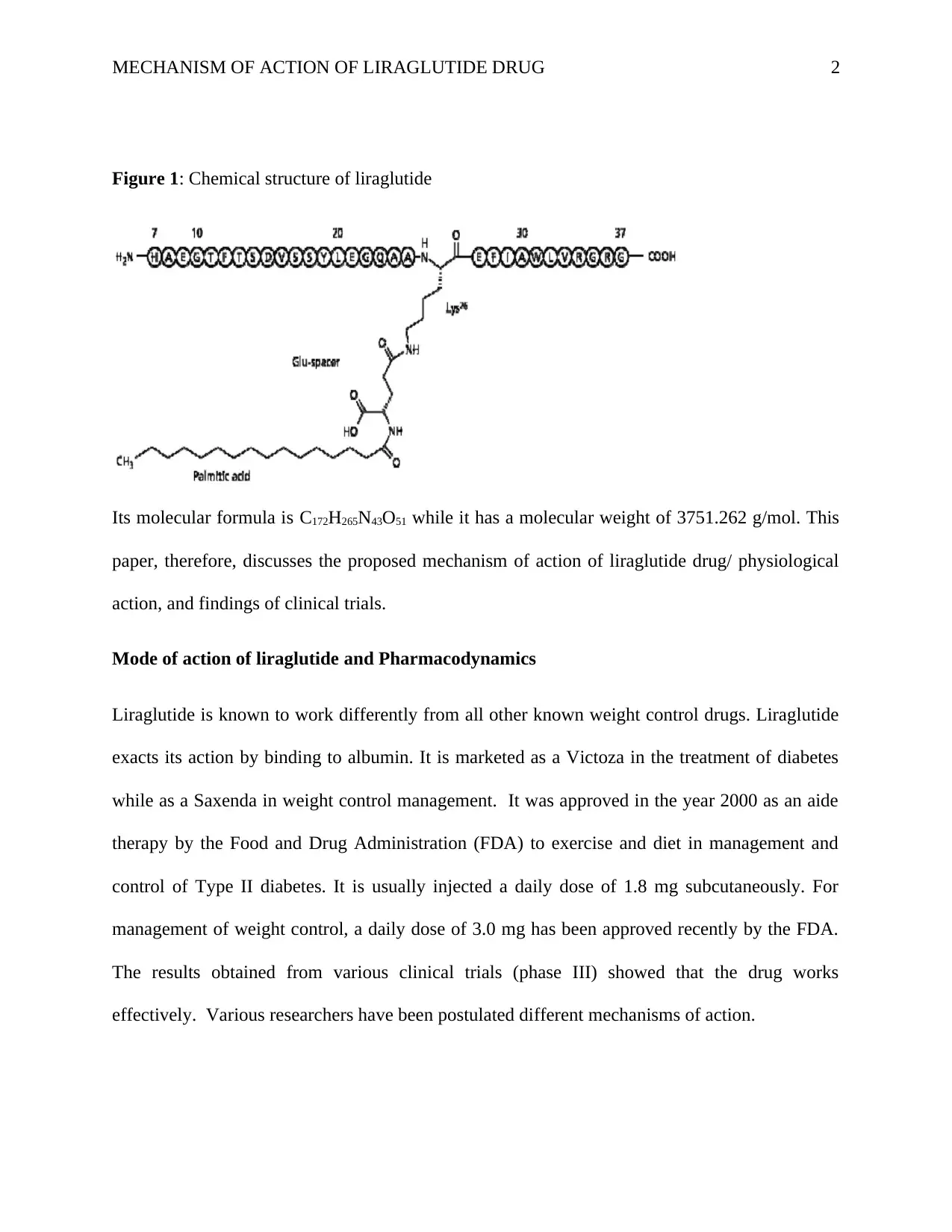
Figure 1: Chemical structure of liraglutide
Its molecular formula is C172H265N43O51 while it has a molecular weight of 3751.262 g/mol. This
paper, therefore, discusses the proposed mechanism of action of liraglutide drug/ physiological
action, and findings of clinical trials.
Mode of action of liraglutide and Pharmacodynamics
Liraglutide is known to work differently from all other known weight control drugs. Liraglutide
exacts its action by binding to albumin. It is marketed as a Victoza in the treatment of diabetes
while as a Saxenda in weight control management. It was approved in the year 2000 as an aide
therapy by the Food and Drug Administration (FDA) to exercise and diet in management and
control of Type II diabetes. It is usually injected a daily dose of 1.8 mg subcutaneously. For
management of weight control, a daily dose of 3.0 mg has been approved recently by the FDA.
The results obtained from various clinical trials (phase III) showed that the drug works
effectively. Various researchers have been postulated different mechanisms of action.
Figure 1: Chemical structure of liraglutide
Its molecular formula is C172H265N43O51 while it has a molecular weight of 3751.262 g/mol. This
paper, therefore, discusses the proposed mechanism of action of liraglutide drug/ physiological
action, and findings of clinical trials.
Mode of action of liraglutide and Pharmacodynamics
Liraglutide is known to work differently from all other known weight control drugs. Liraglutide
exacts its action by binding to albumin. It is marketed as a Victoza in the treatment of diabetes
while as a Saxenda in weight control management. It was approved in the year 2000 as an aide
therapy by the Food and Drug Administration (FDA) to exercise and diet in management and
control of Type II diabetes. It is usually injected a daily dose of 1.8 mg subcutaneously. For
management of weight control, a daily dose of 3.0 mg has been approved recently by the FDA.
The results obtained from various clinical trials (phase III) showed that the drug works
effectively. Various researchers have been postulated different mechanisms of action.
MECHANISM OF ACTION OF LIRAGLUTIDE DRUG 3
Delay in gastric emptying
Usually, once food enters the stomach, it is digested and emptied within a given period.
However, liraglutide delays the frequency at which food is emptied from the stomach. The
mechanism through which it exacts its action is also known as a peripheral mode of action. It
thereby sends a signal of satiety in the intestines making one feel full. Gastrointestinal tract L-
cells produce GLP-1, a polypeptide incretin hormone in response to the introduction of food
nutrients into the lumen. Through delayed gastric emptying of food and appetite suppression,
liraglutide plays a significant role in weight lowering and maintenance (Jelsing, p. 535). Appetite
suppression ensures the patients reduce the amount of calorie intake. Hunger is known to impact
calorie intake directly. The higher the craving, the greater amount of calorie intake and hence
high chances of becoming overweight and consequently obese.
Activation of brain cells
Liraglutide works like the glucagon-like-peptide (GLP-1) hormone which regulates appetite and
cravings in the body. It usually acts on the cells of the brain hence activating them. Some studies
have shown arcuate nucleus as the region that mediates GLP-1 receptor used as an agonist by
liraglutide (Secher et al., p. 4473). The mechanism is as also known as the central mode of
action. In turn, the brain regulates the appetite making one feel less hungry. When a person eats
less, the probability of losing weight is high. Animal studies show that GLP-1R, which is a
pharmacological target for the drug, is present in brain regions responsible for food intake
regulation. Therefore, the drug activates the neurons as well as causing gene expression changes.
Delay in gastric emptying
Usually, once food enters the stomach, it is digested and emptied within a given period.
However, liraglutide delays the frequency at which food is emptied from the stomach. The
mechanism through which it exacts its action is also known as a peripheral mode of action. It
thereby sends a signal of satiety in the intestines making one feel full. Gastrointestinal tract L-
cells produce GLP-1, a polypeptide incretin hormone in response to the introduction of food
nutrients into the lumen. Through delayed gastric emptying of food and appetite suppression,
liraglutide plays a significant role in weight lowering and maintenance (Jelsing, p. 535). Appetite
suppression ensures the patients reduce the amount of calorie intake. Hunger is known to impact
calorie intake directly. The higher the craving, the greater amount of calorie intake and hence
high chances of becoming overweight and consequently obese.
Activation of brain cells
Liraglutide works like the glucagon-like-peptide (GLP-1) hormone which regulates appetite and
cravings in the body. It usually acts on the cells of the brain hence activating them. Some studies
have shown arcuate nucleus as the region that mediates GLP-1 receptor used as an agonist by
liraglutide (Secher et al., p. 4473). The mechanism is as also known as the central mode of
action. In turn, the brain regulates the appetite making one feel less hungry. When a person eats
less, the probability of losing weight is high. Animal studies show that GLP-1R, which is a
pharmacological target for the drug, is present in brain regions responsible for food intake
regulation. Therefore, the drug activates the neurons as well as causing gene expression changes.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
MECHANISM OF ACTION OF LIRAGLUTIDE DRUG 4
This results in lower hunger signals and increases the feeling of satiety. However, studies have
not yet established the specific region in the brain responsible for the drug’s action.
Upregulation of intracellular cAMP
Liraglutide upregulates the intracellular cyclic 3’, 5’-adenosine monophosphate (cAMP) which
results in the release of insulin hormone. Once liraglutide enters the body system and reaches the
pancreatic beta cells, they activate the GLP-1 receptor. When insulin hormone is released, it
lowers blood sugar concentration in the blood (Vilsbøll et al., p. 154). The insulin secretion
eventually subsides when the glucose levels in the blood decrease and approach a state of
euglycemia. There is great evidence indicating that obesity is a significant contributor to diabetes
mellitus. Most patients with Type II diabetes are obese and therefore, managing their weight
through this drug together with exercise and diet, is essential for therapy management.
Suppression of glucagon hormone secretion
Liraglutide suppresses glucagon production in a glucose-dependent manner. However, it does
not affect the usual means by which glucagon responds to hypoglycemia. The combined effect of
lowering glucagon secretion and increasing insulin secretion reduces both the post-prandial and
fasting blood glucose levels. The effect, however, is more pronounced in pre-diabetic patients as
compared to persons with normal blood sugar (Drucker and Nauck, p. 1699). Obese and
overweight people are known to have high blood sugar as compared to individuals with normal
BMI. That’s why there exists a strong connection between obesity and Type II diabetes. Diabetic
patients are advised to watch their weight, diet, and exercise regularly.
Phase III clinical trials
This results in lower hunger signals and increases the feeling of satiety. However, studies have
not yet established the specific region in the brain responsible for the drug’s action.
Upregulation of intracellular cAMP
Liraglutide upregulates the intracellular cyclic 3’, 5’-adenosine monophosphate (cAMP) which
results in the release of insulin hormone. Once liraglutide enters the body system and reaches the
pancreatic beta cells, they activate the GLP-1 receptor. When insulin hormone is released, it
lowers blood sugar concentration in the blood (Vilsbøll et al., p. 154). The insulin secretion
eventually subsides when the glucose levels in the blood decrease and approach a state of
euglycemia. There is great evidence indicating that obesity is a significant contributor to diabetes
mellitus. Most patients with Type II diabetes are obese and therefore, managing their weight
through this drug together with exercise and diet, is essential for therapy management.
Suppression of glucagon hormone secretion
Liraglutide suppresses glucagon production in a glucose-dependent manner. However, it does
not affect the usual means by which glucagon responds to hypoglycemia. The combined effect of
lowering glucagon secretion and increasing insulin secretion reduces both the post-prandial and
fasting blood glucose levels. The effect, however, is more pronounced in pre-diabetic patients as
compared to persons with normal blood sugar (Drucker and Nauck, p. 1699). Obese and
overweight people are known to have high blood sugar as compared to individuals with normal
BMI. That’s why there exists a strong connection between obesity and Type II diabetes. Diabetic
patients are advised to watch their weight, diet, and exercise regularly.
Phase III clinical trials
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
MECHANISM OF ACTION OF LIRAGLUTIDE DRUG 5
Several studies using animal and human models have been carried out to establish the
mechanism of action of liraglutide as well as its efficacy and safety. The very first study for
phase III was conducted using patients with BMI of between 30 and 40 in eight European
countries. The trials used four different doses of liraglutide and a placebo. The doses were 3.0
mg, 2.8 mg, 1.8 mg, and 1.2 mg for the liraglutide. Weight loss was 7.2 kg, 6.3 kg, 5.5 kg, and
4.8 kg respectively and for the placebo, it was 2.8 kg (Mehta et al., p. 7). By looking at the
results, it’s clear that 3.0 mg worked better than other doses.
A study by Pi-Sunyer et al., (2005) involving five phase two and three trials have also shown that
the drug is superior compared to a placebo. The study carried out for 56 weeks proved the
efficiency of the drug. 49.8% of the people who took part in the study, had lost ≥5% of weight as
compared to placebo (13.5%). Even compared to orlistat, the only drug permitted by the
Australian government for long-term weight management, liraglutide, proved to be quite
effective. Most of the phase III trials involved a comparison study between overweight and obese
patients, a placebo, and a positive control using a weight management drug agent.
Findings
Where the study varied the concentration and dosage of the liraglutide drug, 3.0 mg stood out as
the most effective. Those individuals treated with 3.0 mg of the liraglutide drug had better mean
self-esteem, improved mean physical function score, and had lower rates of prediabetes. It
remains the reason why 3.0 mg is the approved dose by FDA (Colman et al., p. 1578). The drug
is recommended to be taken daily once as a single dose. Weight loss differs among the patients
due to several factors such as genetic variations. However, weight loss of about 5-10% in obese
individuals is known to reduce various complications associated with obesity. Shedding off
excess weight improves the quality of life of the patients as well as increasing their life
Several studies using animal and human models have been carried out to establish the
mechanism of action of liraglutide as well as its efficacy and safety. The very first study for
phase III was conducted using patients with BMI of between 30 and 40 in eight European
countries. The trials used four different doses of liraglutide and a placebo. The doses were 3.0
mg, 2.8 mg, 1.8 mg, and 1.2 mg for the liraglutide. Weight loss was 7.2 kg, 6.3 kg, 5.5 kg, and
4.8 kg respectively and for the placebo, it was 2.8 kg (Mehta et al., p. 7). By looking at the
results, it’s clear that 3.0 mg worked better than other doses.
A study by Pi-Sunyer et al., (2005) involving five phase two and three trials have also shown that
the drug is superior compared to a placebo. The study carried out for 56 weeks proved the
efficiency of the drug. 49.8% of the people who took part in the study, had lost ≥5% of weight as
compared to placebo (13.5%). Even compared to orlistat, the only drug permitted by the
Australian government for long-term weight management, liraglutide, proved to be quite
effective. Most of the phase III trials involved a comparison study between overweight and obese
patients, a placebo, and a positive control using a weight management drug agent.
Findings
Where the study varied the concentration and dosage of the liraglutide drug, 3.0 mg stood out as
the most effective. Those individuals treated with 3.0 mg of the liraglutide drug had better mean
self-esteem, improved mean physical function score, and had lower rates of prediabetes. It
remains the reason why 3.0 mg is the approved dose by FDA (Colman et al., p. 1578). The drug
is recommended to be taken daily once as a single dose. Weight loss differs among the patients
due to several factors such as genetic variations. However, weight loss of about 5-10% in obese
individuals is known to reduce various complications associated with obesity. Shedding off
excess weight improves the quality of life of the patients as well as increasing their life
MECHANISM OF ACTION OF LIRAGLUTIDE DRUG 6
expectancy. Most of these clinical trials involved obese and overweight non-diabetic adults at
baseline. Apart from weight loss, individuals given the drug had better glycemic control, reduced
diastolic and systolic blood pressure as well as reduced waistline circumference as compared to
those given the placebo. If you compare two groups in which one is given the placebo while the
other liraglutide, the group given the placebo develop Type II diabetes during the treatment
period as compared to placebo group.
Precautions and side effects
After 12 weeks of liraglutide use and the patient does not lose at least 5% of the weight they
initially started with, discontinuation of the drug use is recommended immediately. The drug use
should be accompanied by exercise activity and a low-calorie diet to enhance its efficiency
(Wadden et al., p. 1443). The most often reported side effects in phase III controlled trials
include; diarrhea, nausea, constipation, and vomiting. Many people in the liraglutide group
experienced more side effects than those in the placebo group. The most common involve
gastrointestinal system, and this led to some patients withdrawing from the study. Other less
common side effects include; gallbladder-related events, pancreatitis, and neoplasms (Peterson
and Pollom, p. 39)
Benefits of using liraglutide
Liraglutide shows significant improvement in various obesity-related parameters and co-
morbidities. It has a positive effect on the cardiovascular diseases. It lowers high blood pressure,
reduces the waist circumference as well as the severity of obstructive sleep apnoea. It also has a
positive effect on glycemic patients. Liraglutide is known to cause a reversal of pre-diabetes,
delay progression of Type II diabetes and lower glycosylated hemoglobin levels (Nuffer and
expectancy. Most of these clinical trials involved obese and overweight non-diabetic adults at
baseline. Apart from weight loss, individuals given the drug had better glycemic control, reduced
diastolic and systolic blood pressure as well as reduced waistline circumference as compared to
those given the placebo. If you compare two groups in which one is given the placebo while the
other liraglutide, the group given the placebo develop Type II diabetes during the treatment
period as compared to placebo group.
Precautions and side effects
After 12 weeks of liraglutide use and the patient does not lose at least 5% of the weight they
initially started with, discontinuation of the drug use is recommended immediately. The drug use
should be accompanied by exercise activity and a low-calorie diet to enhance its efficiency
(Wadden et al., p. 1443). The most often reported side effects in phase III controlled trials
include; diarrhea, nausea, constipation, and vomiting. Many people in the liraglutide group
experienced more side effects than those in the placebo group. The most common involve
gastrointestinal system, and this led to some patients withdrawing from the study. Other less
common side effects include; gallbladder-related events, pancreatitis, and neoplasms (Peterson
and Pollom, p. 39)
Benefits of using liraglutide
Liraglutide shows significant improvement in various obesity-related parameters and co-
morbidities. It has a positive effect on the cardiovascular diseases. It lowers high blood pressure,
reduces the waist circumference as well as the severity of obstructive sleep apnoea. It also has a
positive effect on glycemic patients. Liraglutide is known to cause a reversal of pre-diabetes,
delay progression of Type II diabetes and lower glycosylated hemoglobin levels (Nuffer and
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

MECHANISM OF ACTION OF LIRAGLUTIDE DRUG 7
Trujillo, p. 929). All in all, it improves the overall quality of life of the patients by improving
their mental, physical and physiological health.
Conclusion
The incidence of obesity and other chronic related diseases occurrence is increasing each day.
They lead to high rate of morbidity and mortality, and as well they contribute to serious health
consequences. Weight loss and maintenance of healthy BMI improves quality of life as well as
reduces various complications related to obesity such as cardiovascular diseases. Liraglutide has
shown high efficacy in ensuring weight loss and keeping the excess weight off for good. The
mechanism of action, however, remains elusive and there is a need for more research to elucidate
the actual mode of action of the drug.
Trujillo, p. 929). All in all, it improves the overall quality of life of the patients by improving
their mental, physical and physiological health.
Conclusion
The incidence of obesity and other chronic related diseases occurrence is increasing each day.
They lead to high rate of morbidity and mortality, and as well they contribute to serious health
consequences. Weight loss and maintenance of healthy BMI improves quality of life as well as
reduces various complications related to obesity such as cardiovascular diseases. Liraglutide has
shown high efficacy in ensuring weight loss and keeping the excess weight off for good. The
mechanism of action, however, remains elusive and there is a need for more research to elucidate
the actual mode of action of the drug.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
MECHANISM OF ACTION OF LIRAGLUTIDE DRUG 8
References
Astrup, A., Rössner, S., Van Gaal, L., Rissanen, A., Niskanen, L., Al Hakim, M., Madsen, J.,
Rasmussen, M.F., Lean, M.E. and NN8022-1807 Study Group, 2009. Effects of liraglutide in the
treatment of obesity: a randomised, double-blind, placebo-controlled study. The Lancet,
374(9701), pp.1606-1616.
Colman, E., Golden, J., Roberts, M., Egan, A., Weaver, J. and Rosebraugh, C., 2012. The FDA's
assessment of two drugs for chronic weight management. New England Journal of Medicine,
367(17), pp.1577-1579.
Drucker, D.J. and Nauck, M.A., 2006. The incretin system: glucagon-like peptide-1 receptor
agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. The Lancet, 368(9548),
pp.1696-1705.
Jelsing, J., Vrang, N., Hansen, G., Raun, K., Tang‐Christensen, M. and Bjerre Knudsen, L.,
2012. Liraglutide: short‐lived effect on gastric emptying—long lasting effects on body weight.
Diabetes, Obesity and Metabolism, 14(6), pp.531-538.
References
Astrup, A., Rössner, S., Van Gaal, L., Rissanen, A., Niskanen, L., Al Hakim, M., Madsen, J.,
Rasmussen, M.F., Lean, M.E. and NN8022-1807 Study Group, 2009. Effects of liraglutide in the
treatment of obesity: a randomised, double-blind, placebo-controlled study. The Lancet,
374(9701), pp.1606-1616.
Colman, E., Golden, J., Roberts, M., Egan, A., Weaver, J. and Rosebraugh, C., 2012. The FDA's
assessment of two drugs for chronic weight management. New England Journal of Medicine,
367(17), pp.1577-1579.
Drucker, D.J. and Nauck, M.A., 2006. The incretin system: glucagon-like peptide-1 receptor
agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. The Lancet, 368(9548),
pp.1696-1705.
Jelsing, J., Vrang, N., Hansen, G., Raun, K., Tang‐Christensen, M. and Bjerre Knudsen, L.,
2012. Liraglutide: short‐lived effect on gastric emptying—long lasting effects on body weight.
Diabetes, Obesity and Metabolism, 14(6), pp.531-538.
MECHANISM OF ACTION OF LIRAGLUTIDE DRUG 9
Mehta, A., Marso, S.P. and Neeland, I.J., 2017. Liraglutide for weight management: a critical
review of the evidence. Obesity Science & Practice, 3(1), pp.3-14.
Nuffer, W.A. and Trujillo, J.M., 2015. Liraglutide: a new option for the treatment of obesity.
Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, 35(10), pp.926-
934.
Nuffer, W.A. and Trujillo, J.M., 2015. Liraglutide: a new option for the treatment of obesity.
Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, 35(10), pp.926-
934.
Peterson, G.E. and Pollom, R.D., 2010. Liraglutide in clinical practice: dosing, safety and
efficacy. International Journal of Clinical Practice, 64(s167), pp.35-43.
Pi-Sunyer, X., Astrup, A., Fujioka, K., Greenway, F., Halpern, A., Krempf, M., Lau, D.C., le
Roux, C.W., Violante Ortiz, R., Jensen, C.B. and Wilding, J.P., 2015. A randomized, controlled
trial of 3.0 mg of liraglutide in weight management. New England Journal of Medicine, 373(1),
pp.11-22.
Secher, A., Jelsing, J., Baquero, A.F., Hecksher-Sørensen, J., Cowley, M.A., Dalbøge, L.S.,
Hansen, G., Grove, K.L., Pyke, C., Raun, K. and Schäffer, L., 2014. The arcuate nucleus
mediates GLP-1 receptor agonist liraglutide-dependent weight loss. The Journal of clinical
investigation, 124(10), p.4473.
Mehta, A., Marso, S.P. and Neeland, I.J., 2017. Liraglutide for weight management: a critical
review of the evidence. Obesity Science & Practice, 3(1), pp.3-14.
Nuffer, W.A. and Trujillo, J.M., 2015. Liraglutide: a new option for the treatment of obesity.
Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, 35(10), pp.926-
934.
Nuffer, W.A. and Trujillo, J.M., 2015. Liraglutide: a new option for the treatment of obesity.
Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, 35(10), pp.926-
934.
Peterson, G.E. and Pollom, R.D., 2010. Liraglutide in clinical practice: dosing, safety and
efficacy. International Journal of Clinical Practice, 64(s167), pp.35-43.
Pi-Sunyer, X., Astrup, A., Fujioka, K., Greenway, F., Halpern, A., Krempf, M., Lau, D.C., le
Roux, C.W., Violante Ortiz, R., Jensen, C.B. and Wilding, J.P., 2015. A randomized, controlled
trial of 3.0 mg of liraglutide in weight management. New England Journal of Medicine, 373(1),
pp.11-22.
Secher, A., Jelsing, J., Baquero, A.F., Hecksher-Sørensen, J., Cowley, M.A., Dalbøge, L.S.,
Hansen, G., Grove, K.L., Pyke, C., Raun, K. and Schäffer, L., 2014. The arcuate nucleus
mediates GLP-1 receptor agonist liraglutide-dependent weight loss. The Journal of clinical
investigation, 124(10), p.4473.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
MECHANISM OF ACTION OF LIRAGLUTIDE DRUG 10
Vilsbøll, T., Brock, B., Perrild, H., Levin, K., Lervang, H.H., Kølendorf, K., Krarup, T.,
Schmitz, O., Zdravkovic, M., Le‐Thi, T. and Madsbad, S., 2008. Liraglutide, a once‐daily human
GLP‐1 analogue, improves pancreatic B‐cell function and arginine‐stimulated insulin secretion
during hyperglycaemia in patients with Type 2 diabetes mellitus. Diabetic Medicine, 25(2),
pp.152-156.
Wadden, T.A., Hollander, P., Klein, S., Niswender, K., Woo, V., Hale, P.M. and Aronne, L.,
2013. Weight maintenance and additional weight loss with liraglutide after low-calorie-diet-
induced weight loss: the SCALE Maintenance randomized study. International journal of
obesity, 37(11), p.1443.
Vilsbøll, T., Brock, B., Perrild, H., Levin, K., Lervang, H.H., Kølendorf, K., Krarup, T.,
Schmitz, O., Zdravkovic, M., Le‐Thi, T. and Madsbad, S., 2008. Liraglutide, a once‐daily human
GLP‐1 analogue, improves pancreatic B‐cell function and arginine‐stimulated insulin secretion
during hyperglycaemia in patients with Type 2 diabetes mellitus. Diabetic Medicine, 25(2),
pp.152-156.
Wadden, T.A., Hollander, P., Klein, S., Niswender, K., Woo, V., Hale, P.M. and Aronne, L.,
2013. Weight maintenance and additional weight loss with liraglutide after low-calorie-diet-
induced weight loss: the SCALE Maintenance randomized study. International journal of
obesity, 37(11), p.1443.
1 out of 10

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.