University Report: Multidisciplinary Approach to Childhood Obesity
VerifiedAdded on 2023/01/23
|9
|1115
|88
Report
AI Summary
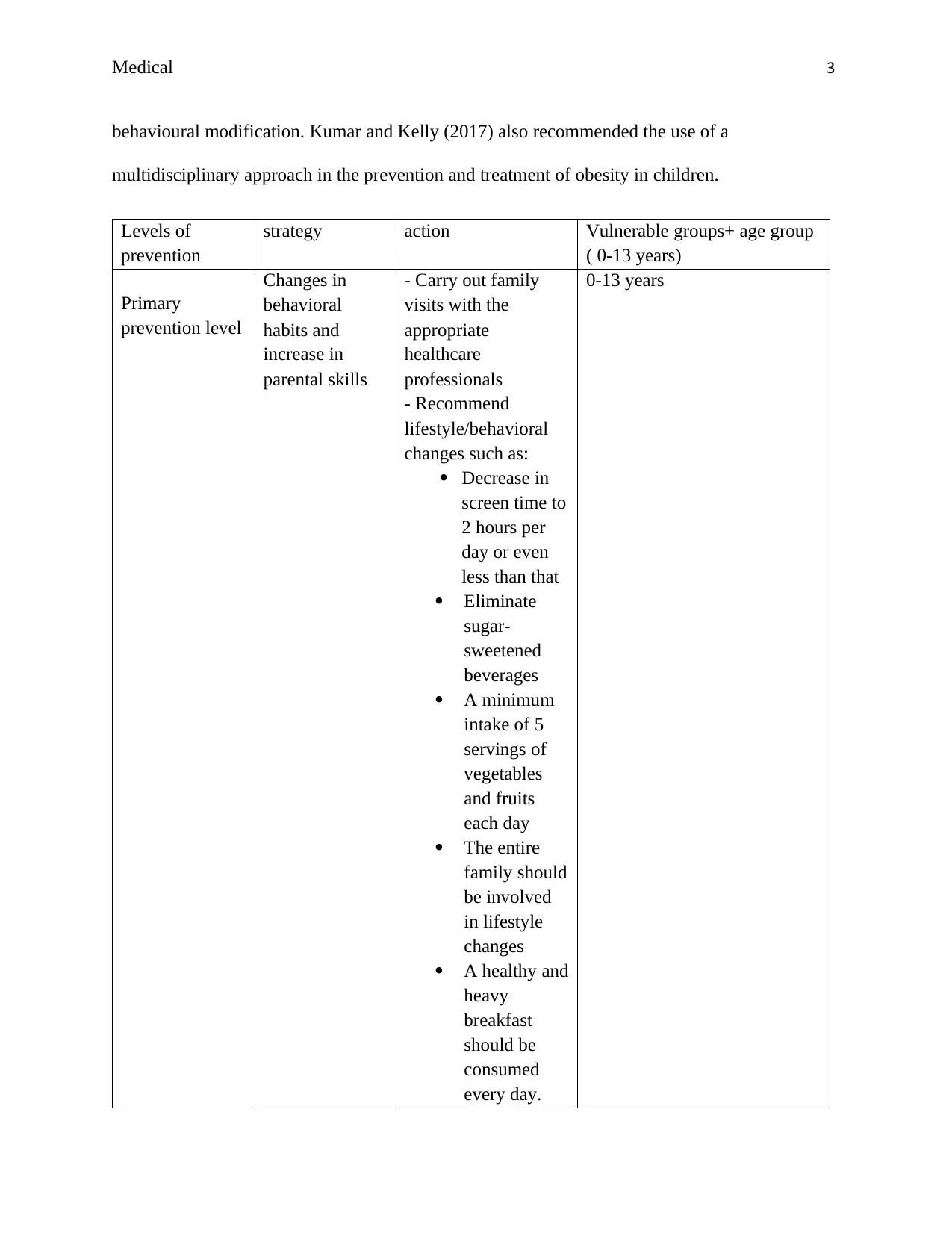
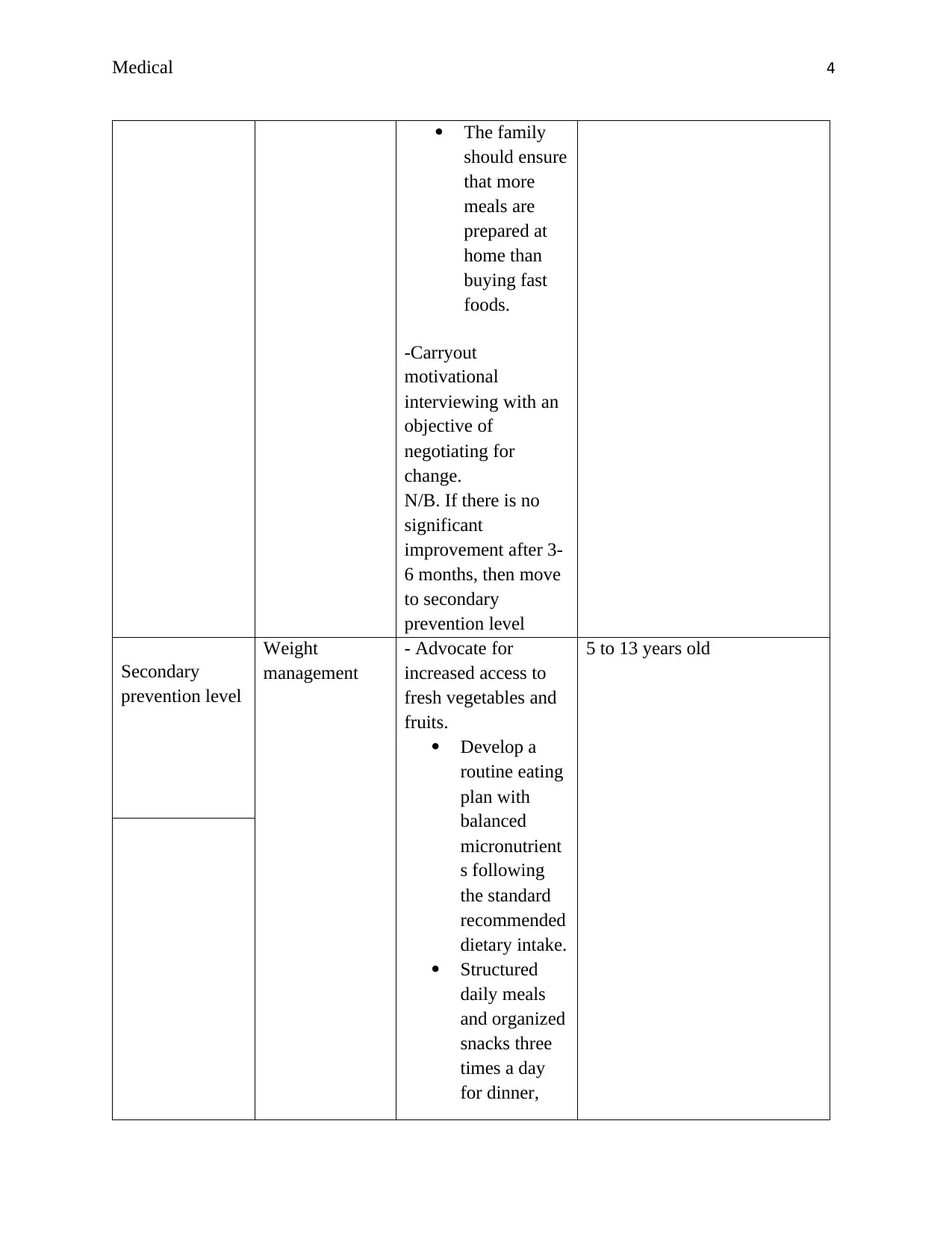
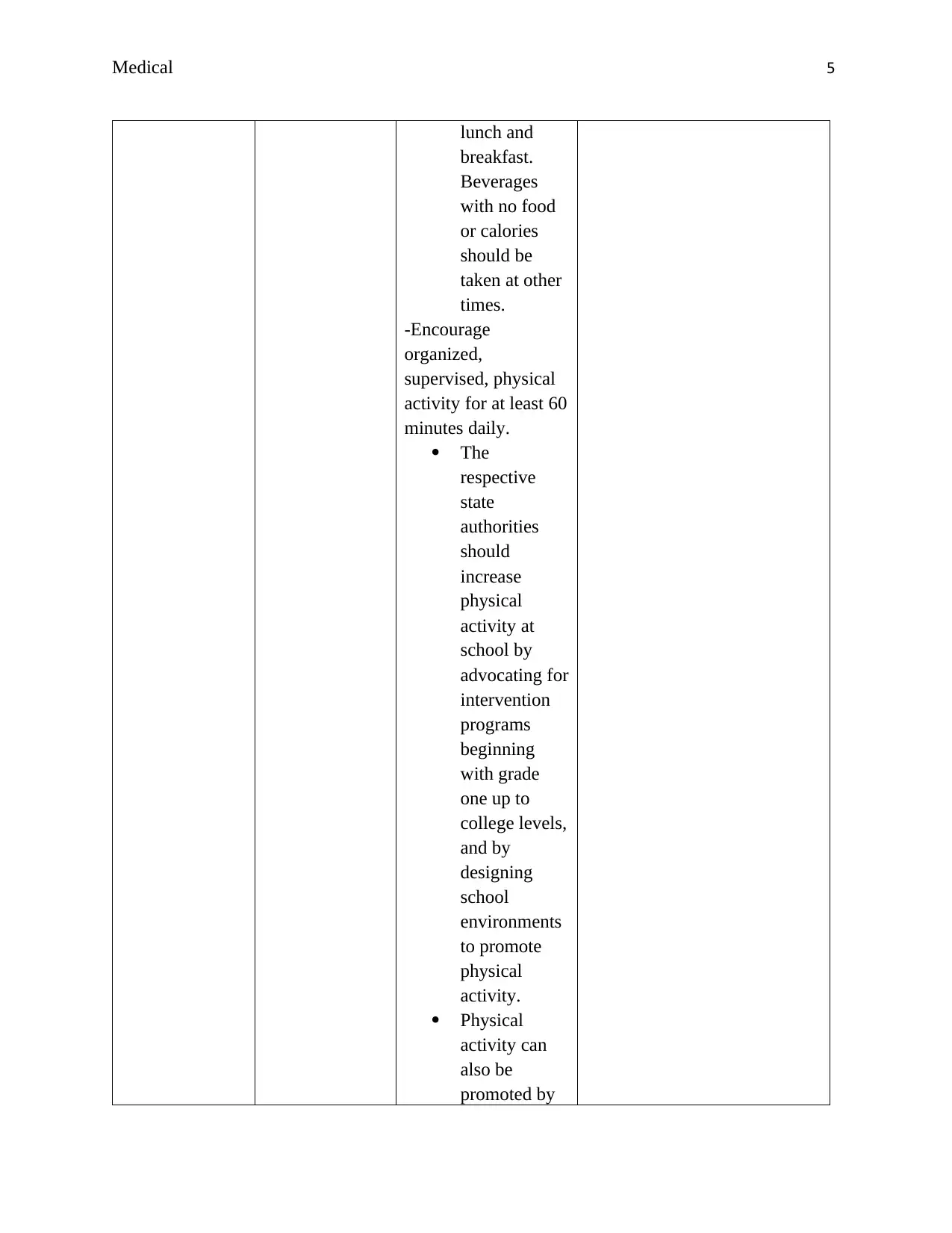
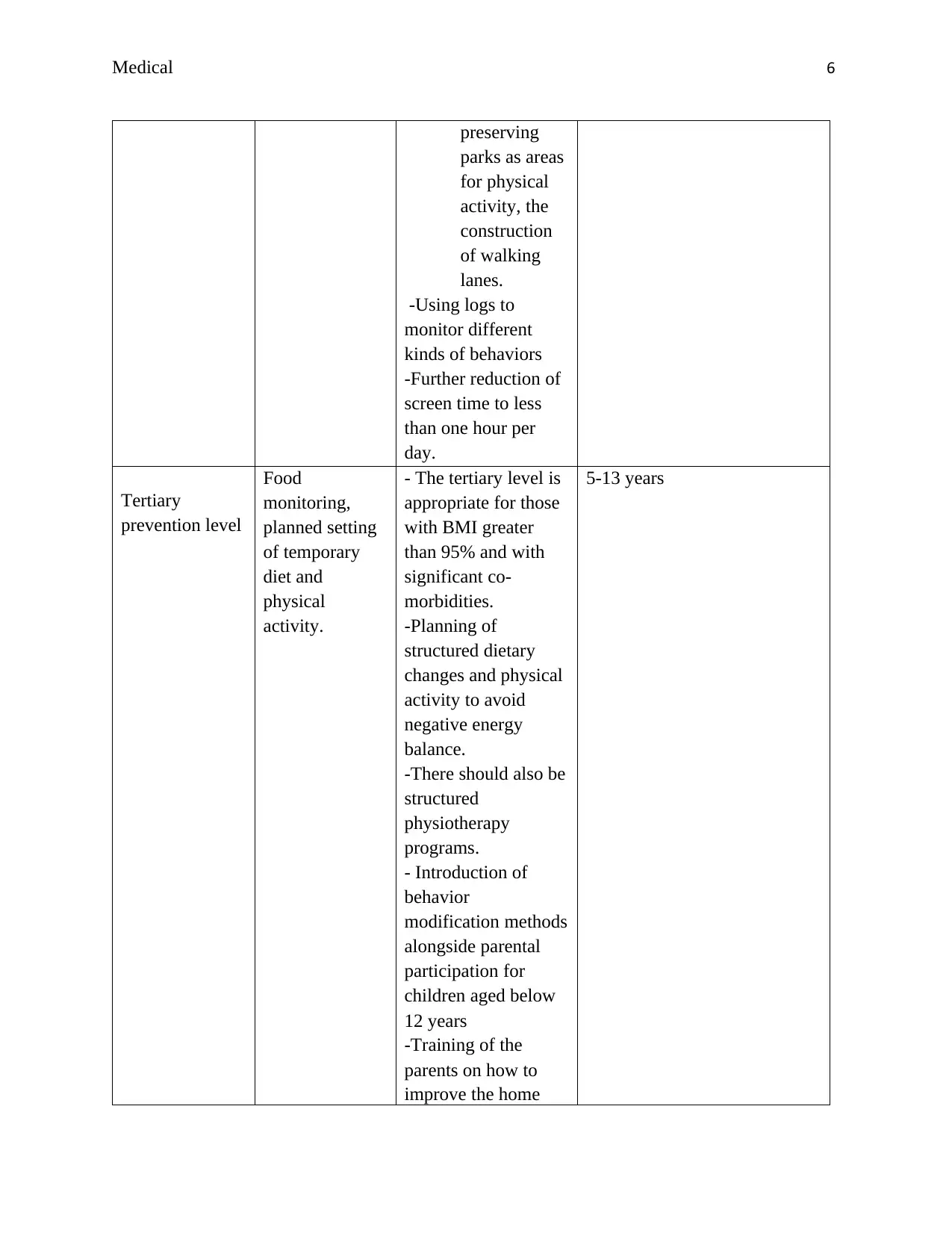
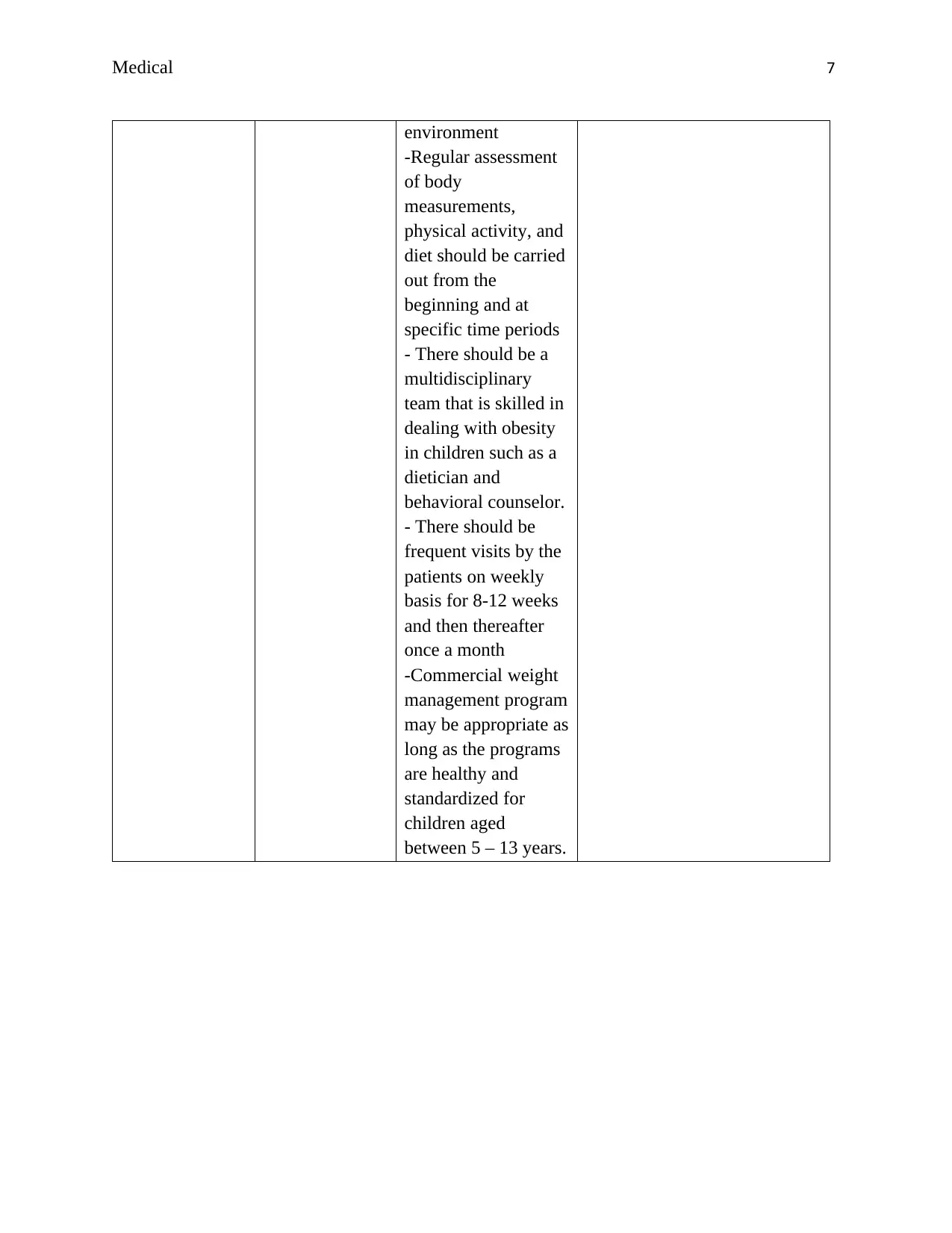
This report, prepared for a Community Health and Disease Prevention course, examines the global issue of childhood obesity, citing statistics from the World Health Organization and the Australian Institute of Health and Welfare. It explores the health risks associated with childhood obesity, such as cardiovascular diseases, and emphasizes the need for effective intervention strategies. The report proposes a multidisciplinary approach, detailing primary, secondary, and tertiary prevention levels. These levels involve behavioral changes, weight management techniques, structured dietary changes, and physical activity promotion. The report references studies supporting this approach and outlines specific actions for each prevention level, targeting vulnerable age groups and involving family participation. The report also includes a comprehensive list of references that support the research and recommendations presented.

1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.