Mental Health Case: Patient Examination and Therapeutic Care Plan
VerifiedAdded on 2023/06/13
|14
|2876
|284
Case Study
AI Summary
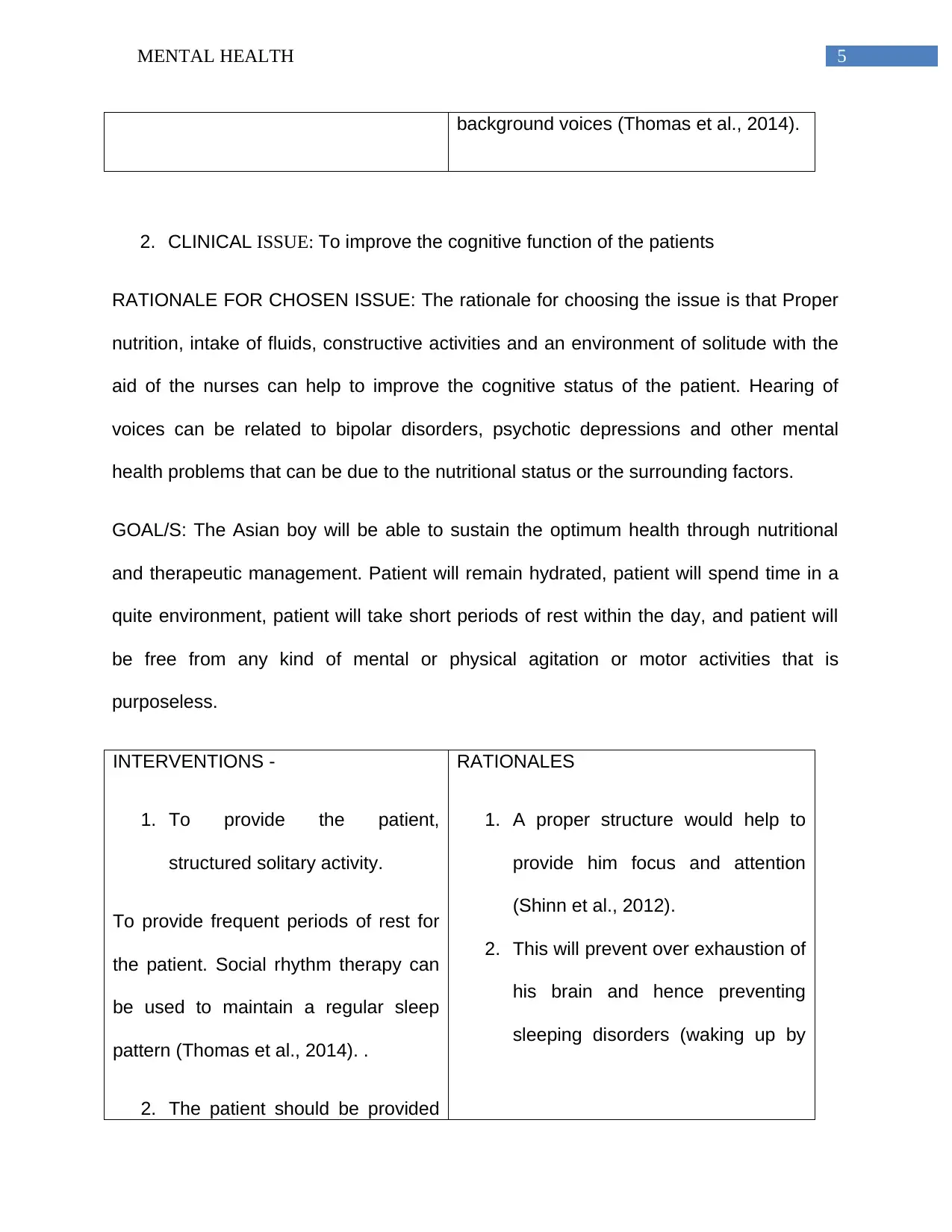
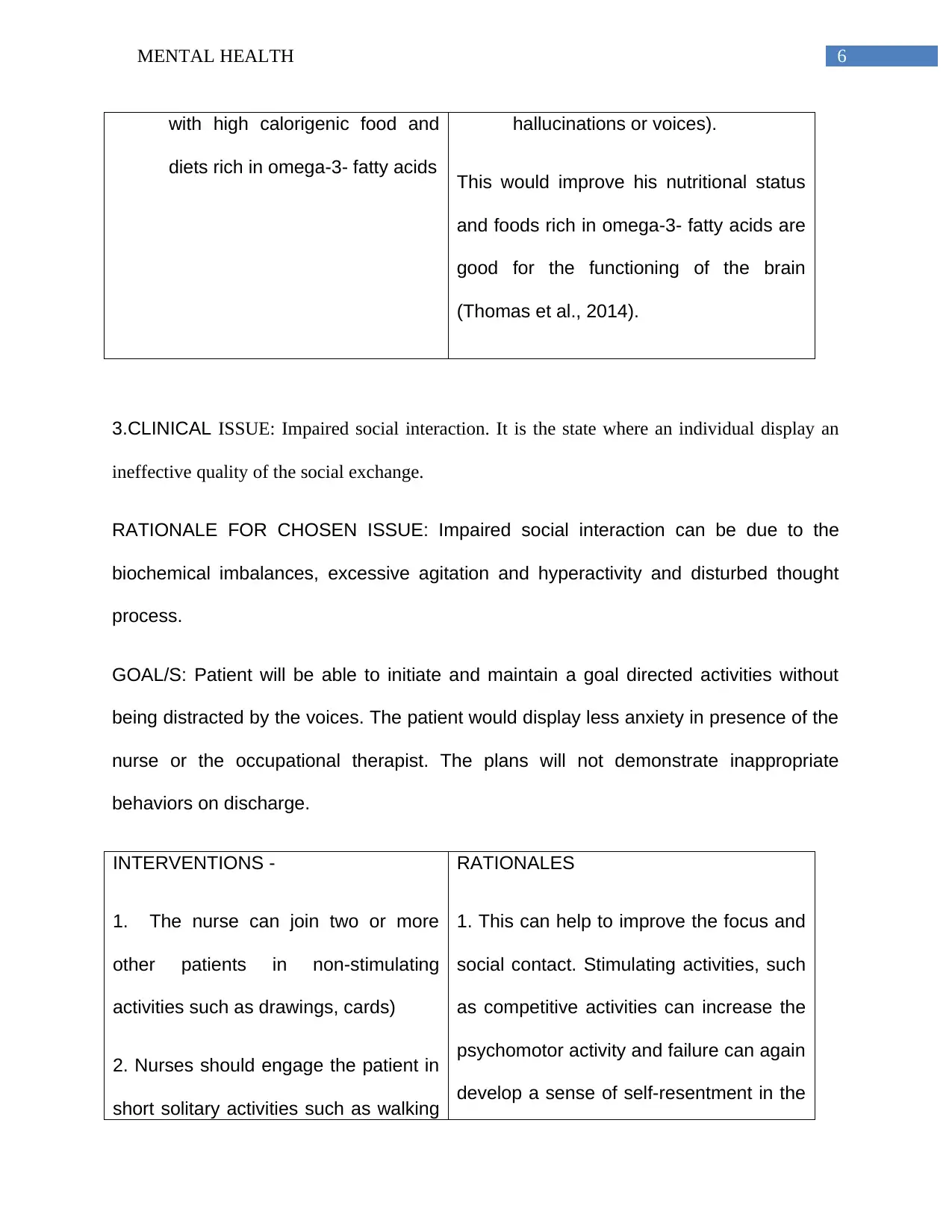
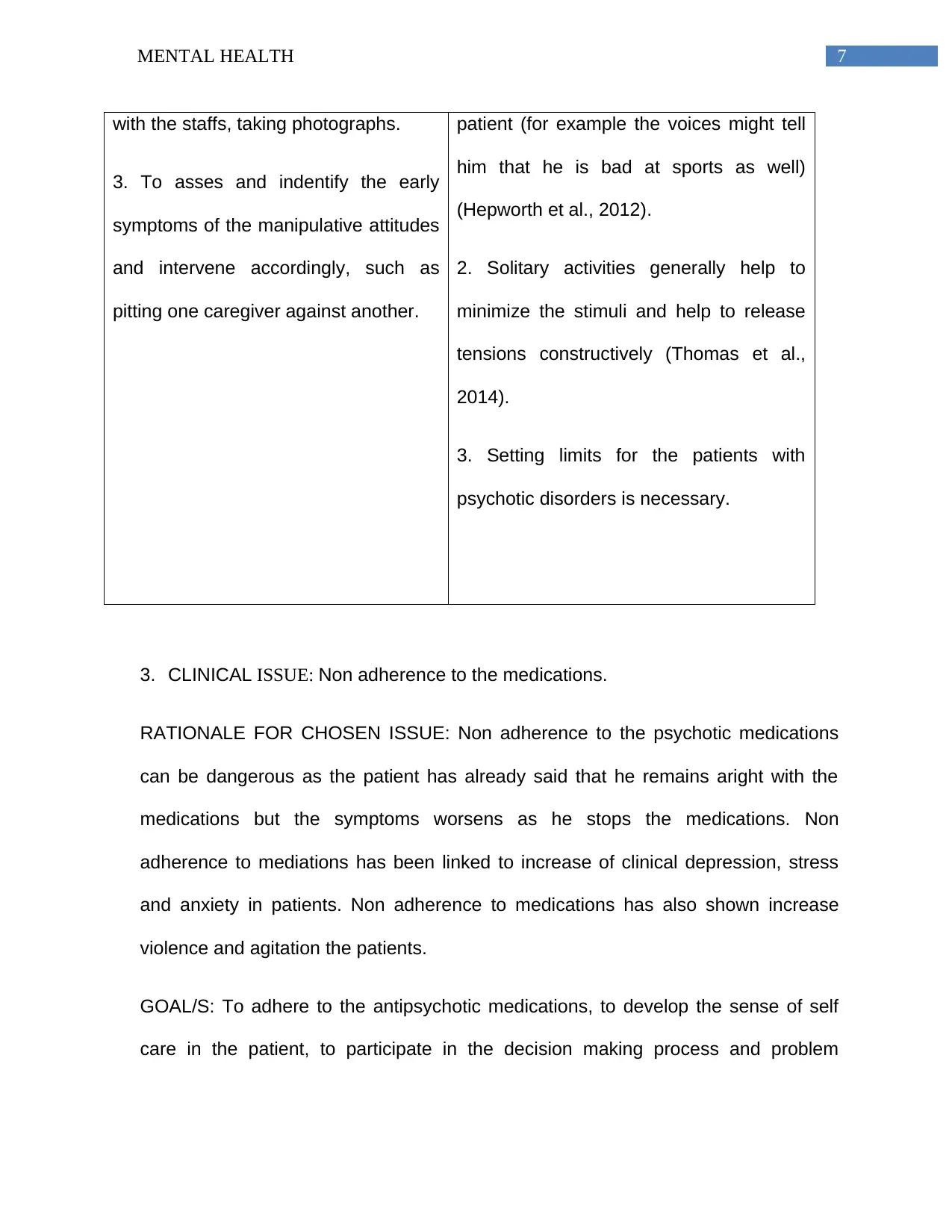
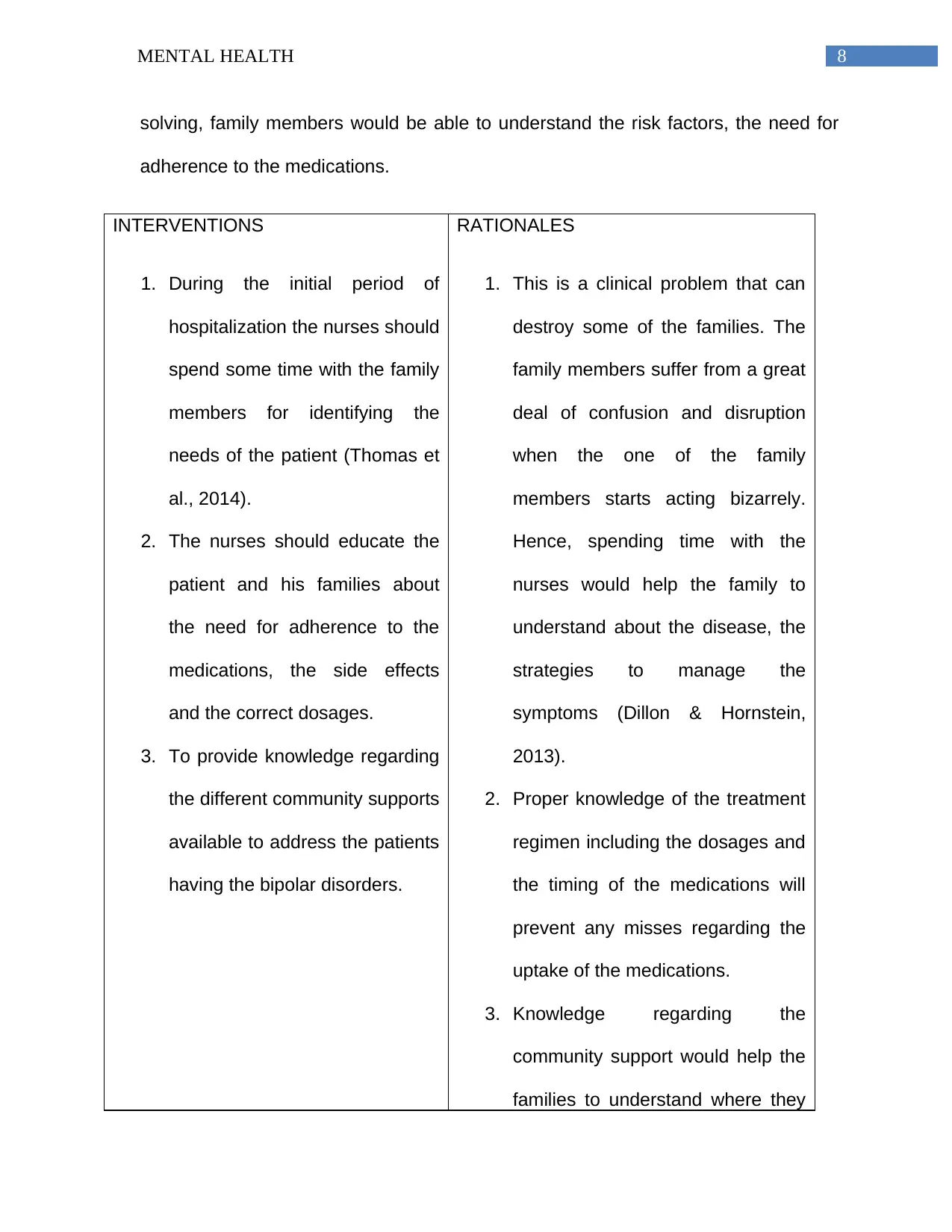
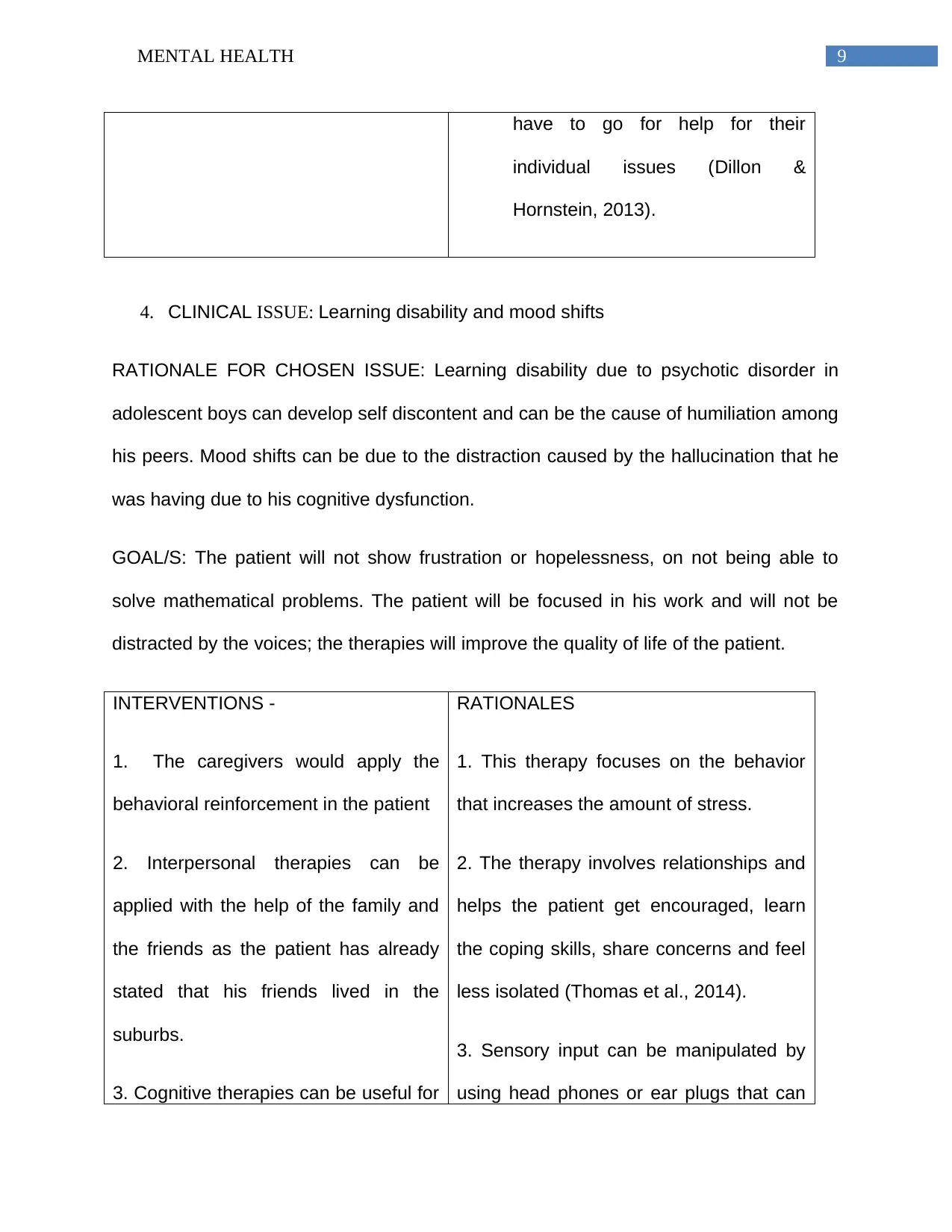
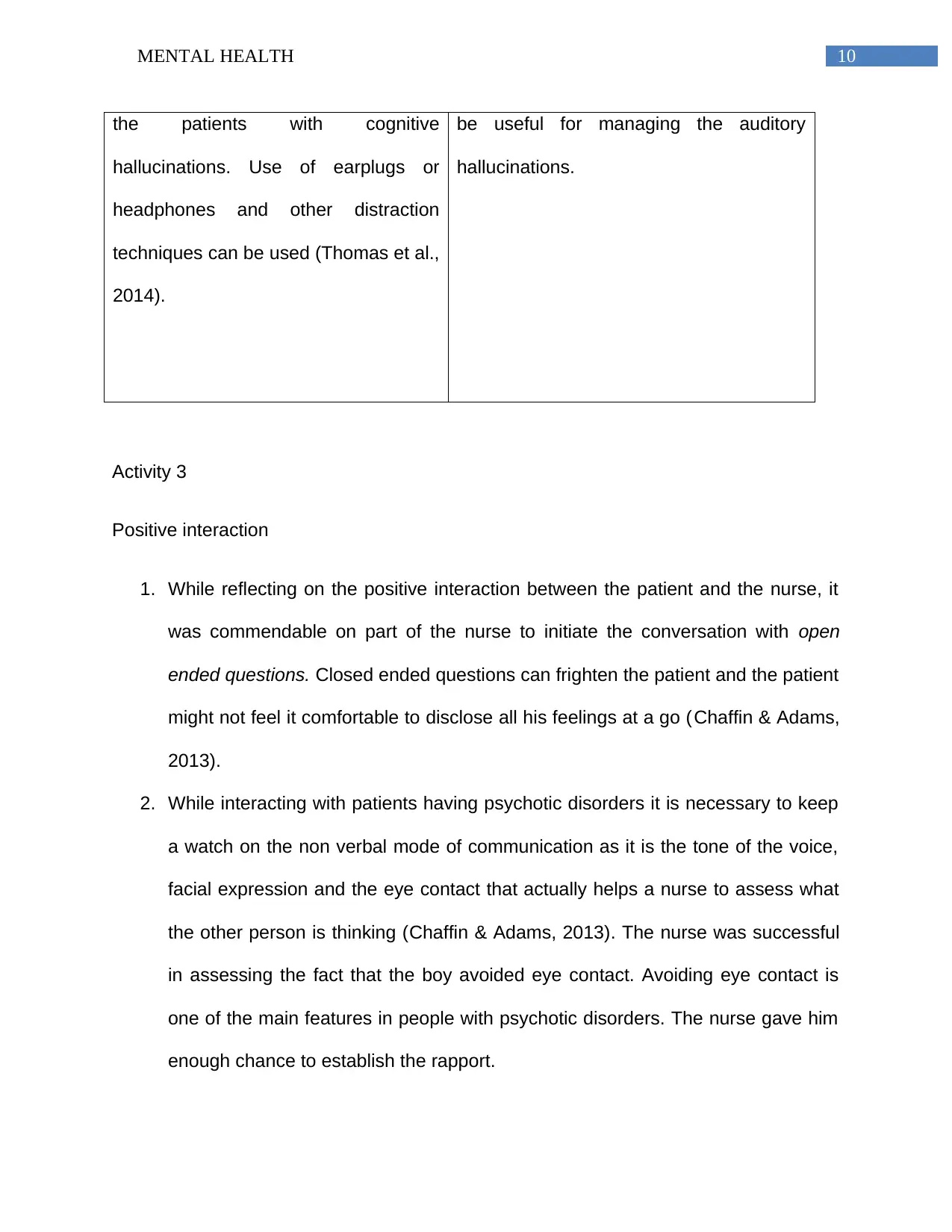
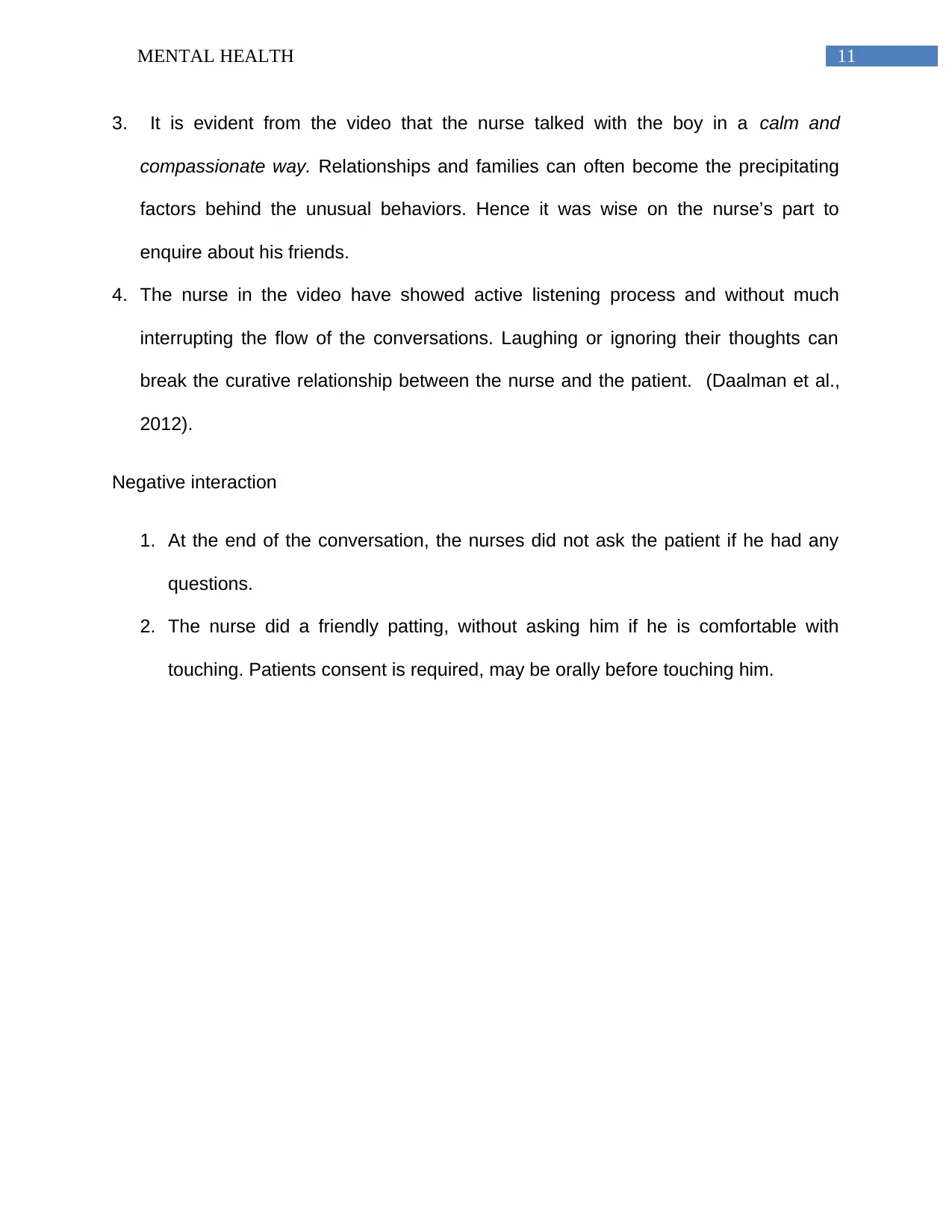
This case study presents a mental health assessment of a young Asian male experiencing auditory hallucinations and related challenges. The mental status examination covers appearance, behavior, affect, mood, speech, thought form and content, perception, cognition, and insight. Key risk factors identified include cognitive, affective, and psychomotor factors, potential sleeping disorders, and frustration related to learning disabilities. The comprehensive care plan addresses clinical issues such as hearing voices, impaired cognitive function, impaired social interaction, non-adherence to medications, and learning disabilities. Interventions include monitoring behavior, improving nutrition, social rhythm therapy, structured solitary activities, and cognitive therapies. The study also reflects on positive nurse-patient interactions and the importance of open-ended questions and non-verbal communication. The goal is to improve the patient's quality of life through therapeutic management and family support. Desklib provides a platform for students to access such solved assignments and past papers for academic assistance.

1 out of 14
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.