Schizophrenia: Mental Status Examination and Nursing Care Plan
VerifiedAdded on 2023/06/14
|6
|1991
|423
Case Study
AI Summary
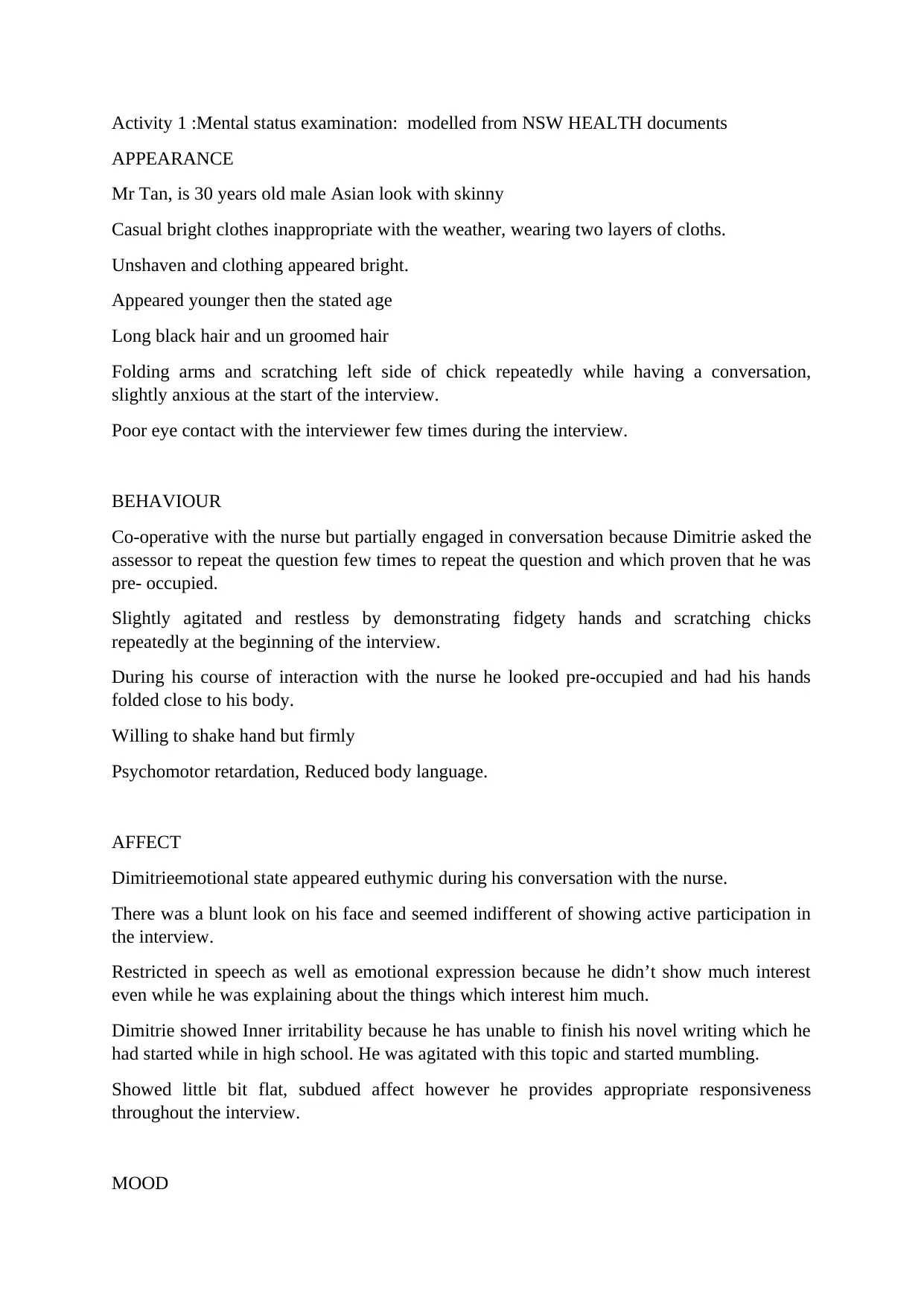
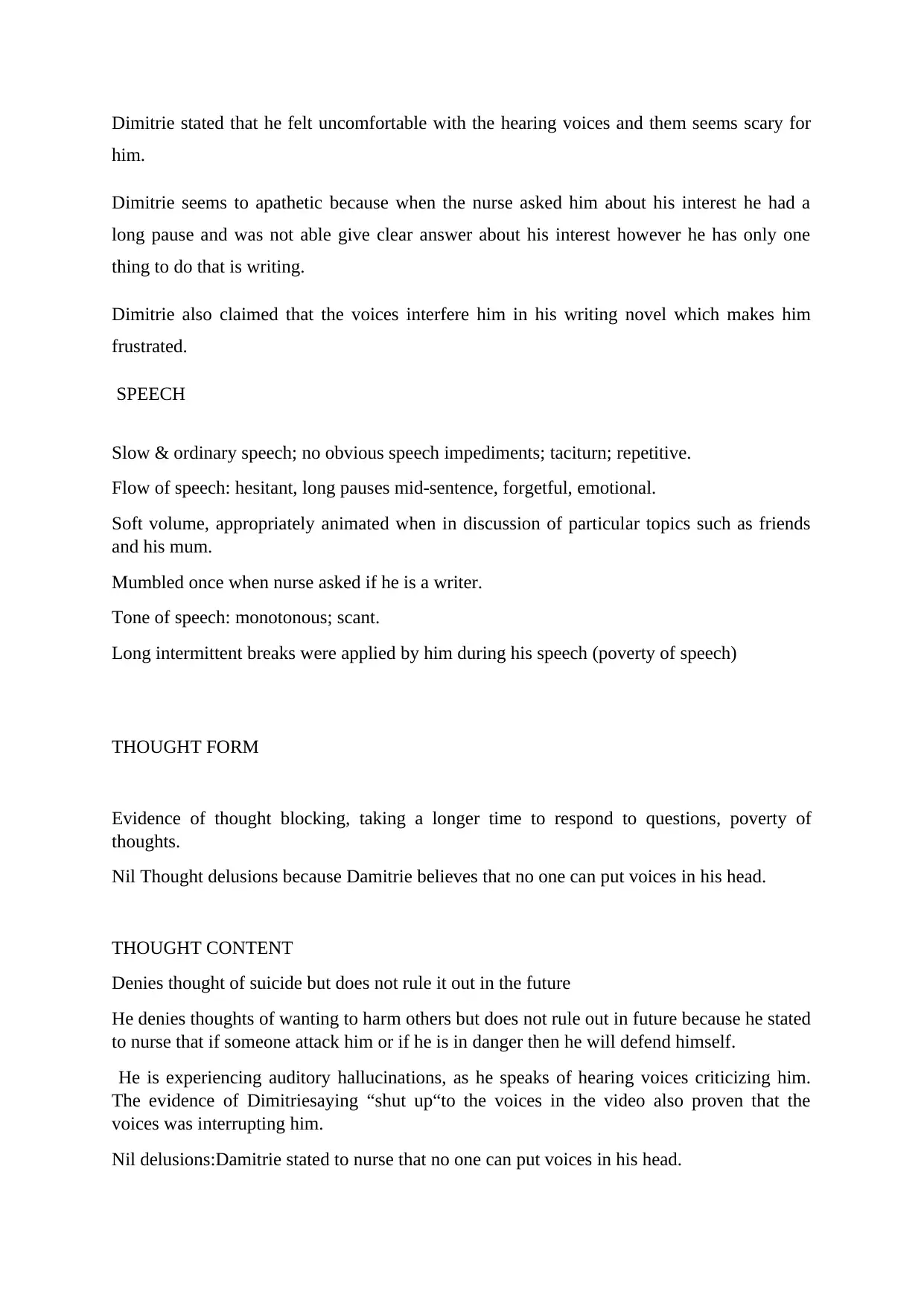
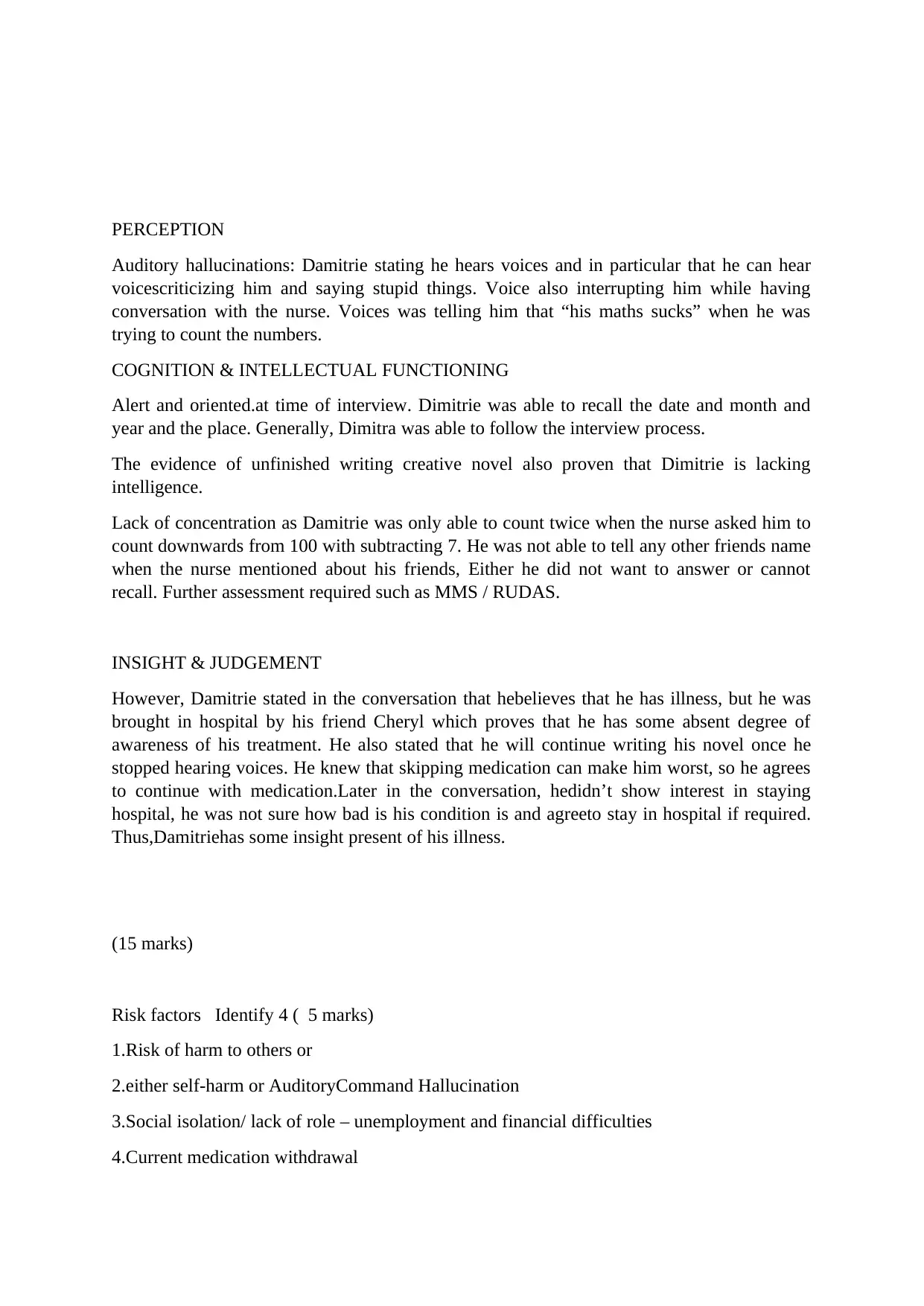
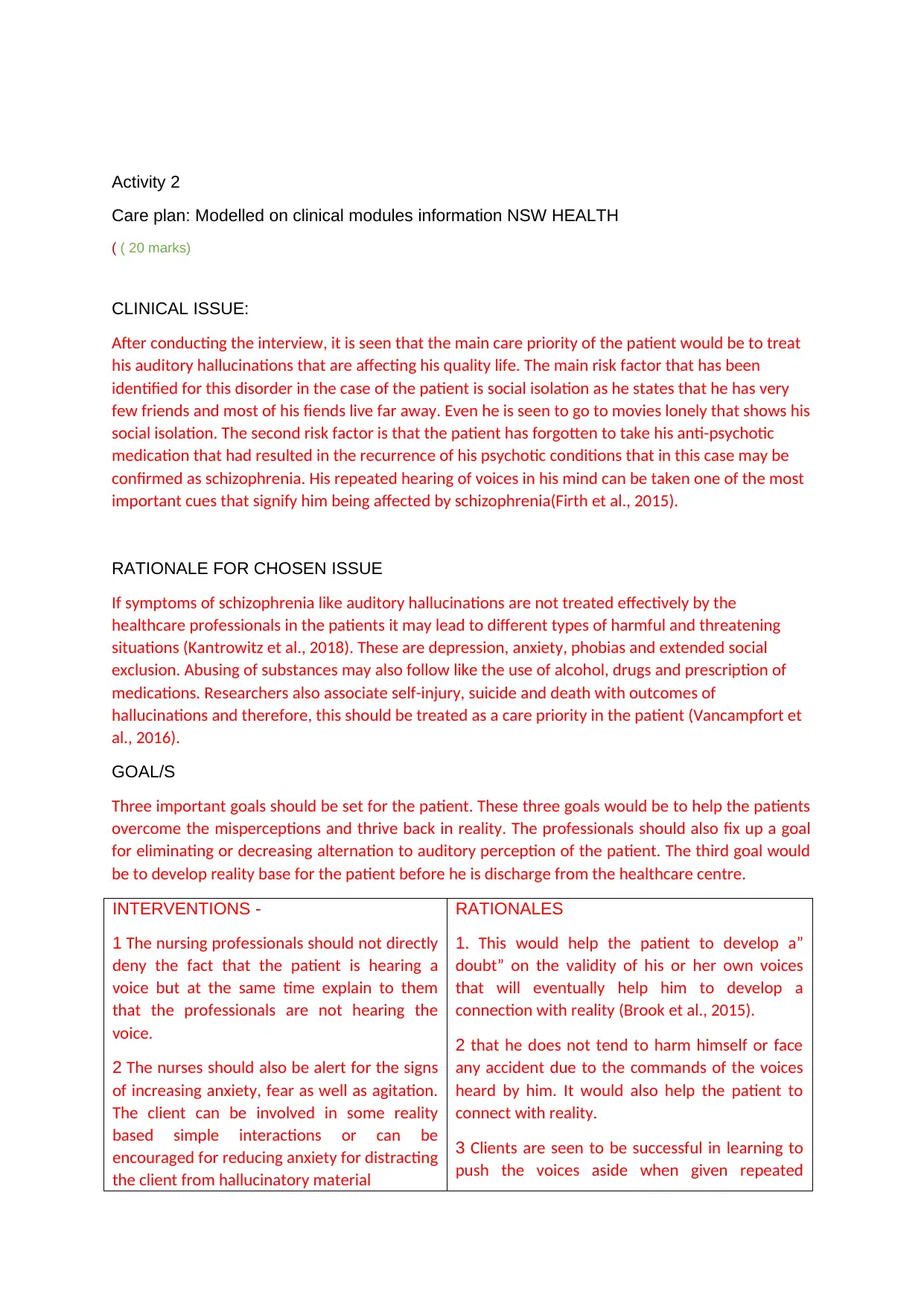
This assignment presents a case study of a 30-year-old male, Mr. Tan, exhibiting symptoms indicative of schizophrenia, focusing on a mental status examination and the development of a comprehensive care plan. The mental status examination covers appearance, behavior, affect, mood, speech, thought form and content, perception (auditory hallucinations), cognition and intellectual functioning, and insight and judgment. Key risk factors identified include potential harm to self or others, auditory command hallucinations, social isolation, and medication withdrawal. The care plan prioritizes addressing auditory hallucinations and social isolation, with goals focused on reality orientation and reducing perceptual disturbances. Nursing interventions emphasize building trust, validating the patient's experience without reinforcing hallucinations, and managing anxiety. The evaluation will focus on medication effectiveness, adherence to treatment, and the patient's overall mental status. The reflection highlights positive aspects of the nurse's approach, such as body language and pacing, alongside areas for improvement, like using open-ended questions and ensuring confidentiality. Desklib provides access to similar solved assignments and study resources for students.
1 out of 6
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.