Health Promotion Evidence Critique Report: Indigenous Australians
VerifiedAdded on 2022/08/21
|3
|1736
|13
Report
AI Summary
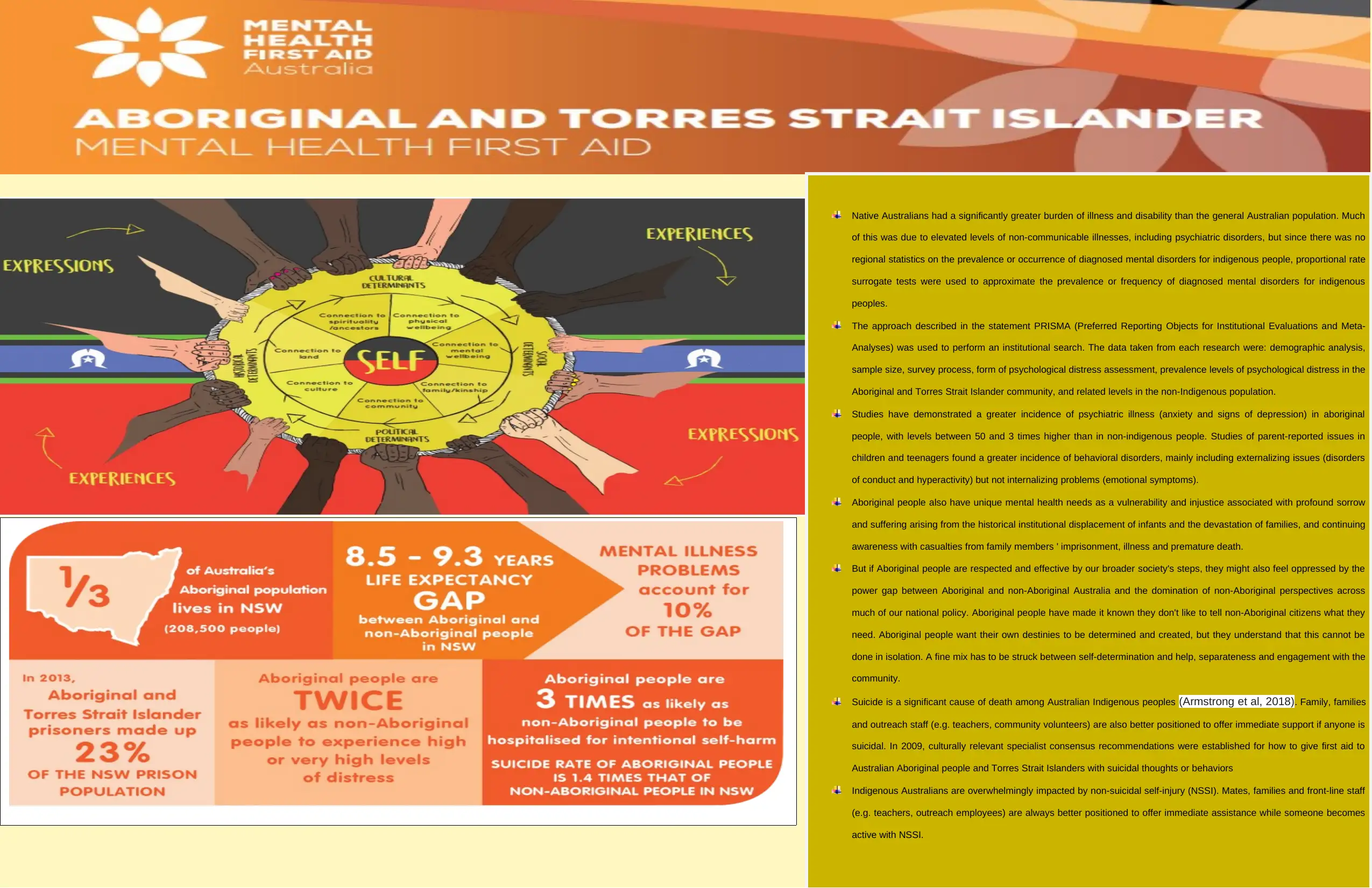
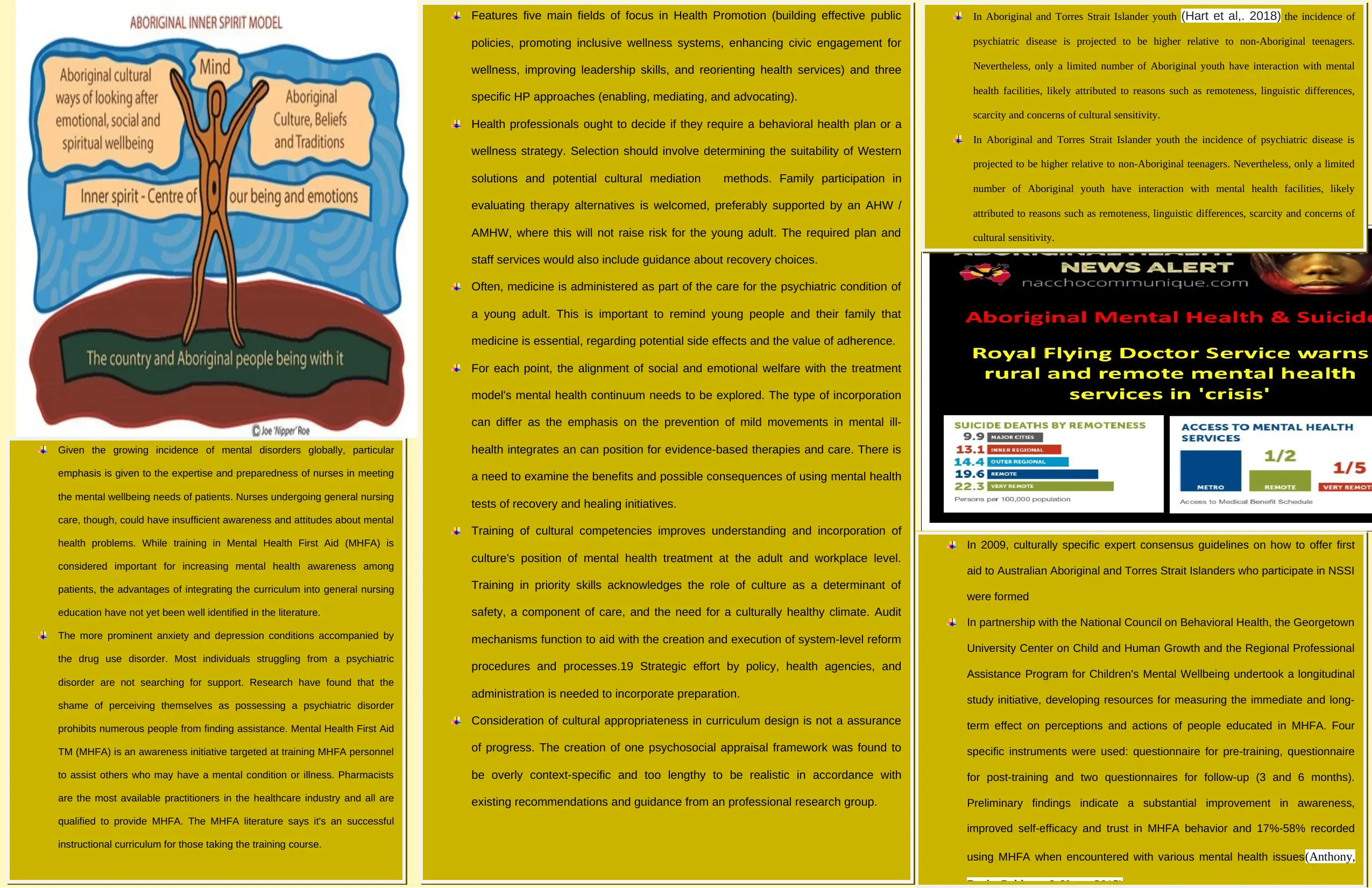
This report critically analyzes health promotion strategies, specifically focusing on the health challenges faced by Indigenous Australians. It examines the elevated burden of illness, including psychiatric disorders, and the unique mental health needs of this population. The report explores the use of proportional rate surrogate tests due to the lack of regional statistics, referencing the PRISMA approach for institutional search. It highlights the increased incidence of psychiatric illnesses and behavioral disorders in Indigenous communities. Furthermore, the report delves into the relevance of health promotion messages, the application of the Ottawa Charter's strategies (enable, mediate, advocate), and how this knowledge can be utilized in future nursing practice. The report also addresses the impact of suicide and non-suicidal self-injury, the importance of Mental Health First Aid, and the integration of cultural competencies in mental health treatment. It emphasizes the need for culturally appropriate curriculum design, audit mechanisms, and strategic effort by policy and health agencies to incorporate preparation. The report references various studies and guidelines, including those for supporting Indigenous Australians experiencing suicidal thoughts and behaviors, and non-suicidal self-injury.
1 out of 3
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
© 2024 | Zucol Services PVT LTD | All rights reserved.