Difference in Non-Clinical Anxiety Levels between Young and Older Adults and in Respect to Depression, Cognitive Functions and Demographic Parameters
VerifiedAdded on 2023/06/12
|34
|10472
|446
AI Summary
This study aims at examining the difference in subclinical anxiety levels between young and older adults in relation to depression. The study sample was composed of young and old audits both male and female that had no clinical evidence of cognitive impairment. The participants were taken through various tests on among them those that tested on personality, retrospective memory questionnaires. More anxiety mostly causes more depression and worse cognition impairment as a result.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

CHAPTER TWO 1
Difference in Non-Clinical Anxiety Levels between Young and Older Adults and in
Respect to Depression, Cognitive Functions and Demographic Parameters
Abstracts
This study aims at examining the difference in subclinical anxiety levels between young and
older adults in relation to depression. The study sample was composed of young and old
audits both male and female that had no clinical evidence of cognitive impairment. The
participants were taken through various tests on among them those that tested on personality,
retrospective memory questionnaires. More anxiety mostly causes more depression and
worse cognition impairment as a result. The results illustrated high scores in subjective
memory complaints association with subclinical levels of depression and anxiety as well as
more negative interpersonal interactions. A deeper understanding of the variables that are
associated with subjective memory complaints may serve as a guide on how to identity
cognitive changes as early as possible and thus establishing the institutions for interventions.
Difference in Non-Clinical Anxiety Levels between Young and Older Adults and in
Respect to Depression, Cognitive Functions and Demographic Parameters
Abstracts
This study aims at examining the difference in subclinical anxiety levels between young and
older adults in relation to depression. The study sample was composed of young and old
audits both male and female that had no clinical evidence of cognitive impairment. The
participants were taken through various tests on among them those that tested on personality,
retrospective memory questionnaires. More anxiety mostly causes more depression and
worse cognition impairment as a result. The results illustrated high scores in subjective
memory complaints association with subclinical levels of depression and anxiety as well as
more negative interpersonal interactions. A deeper understanding of the variables that are
associated with subjective memory complaints may serve as a guide on how to identity
cognitive changes as early as possible and thus establishing the institutions for interventions.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
CHAPTER TWO 2
Introduction
This study aim, subjective memory function, objective cognitive function and demographic
factors, that are, age, gender, years of education, handedness, eyesight which are not
extensively iterated in previous studies. The focus of the study in this chapter will be on
subclinical anxiety levels between young and older adults in relation to depression. With the
the primary objective of this PhD research being an evaluation of the existing association
between the speed of information processing and non-clinical anxiety levels, among older
and younger adults, in relation to a plethora of brain functions, this chapter is designed to
give an understanding of the all the factors before looking at the main aim and see if there is
any correlation between it and those factor that haven’t investigated deeply before.
In as much anxiety has been examined in the various demographic groups, the young against
the old, this has only been done on clinical labels and in other cases as part of depression.
This has left not so much of extensive and explorative work on the subject. On the same note,
studies on anxiety of ageing with regard to the ageing have only been exploited on a clinical
scale. All these are illustration of limited depth of research and analysis of the task. This
study focuses on subclinical anxiety level between the young and the old in relation to
depression.
Numerous research and studies on the effect of depression and anxiety on cognition have
mainly been with relation to anxiety in a wider and general perception even though there is
one study that has given targeted the adults. Still, focus has been on studies targeting
individuals suffering from mild cognitive impairment and dementia while others have
explored formal anxiety disorders. There can be more effects of non-clinical anxiety on the
elements of information processing that what has been recognized and discussed earlier.
Studies on anxiety and age for been for a long time more inclined to clinical level among the
young and older adults. Other studied have delved into an exploration of the effects of
Introduction
This study aim, subjective memory function, objective cognitive function and demographic
factors, that are, age, gender, years of education, handedness, eyesight which are not
extensively iterated in previous studies. The focus of the study in this chapter will be on
subclinical anxiety levels between young and older adults in relation to depression. With the
the primary objective of this PhD research being an evaluation of the existing association
between the speed of information processing and non-clinical anxiety levels, among older
and younger adults, in relation to a plethora of brain functions, this chapter is designed to
give an understanding of the all the factors before looking at the main aim and see if there is
any correlation between it and those factor that haven’t investigated deeply before.
In as much anxiety has been examined in the various demographic groups, the young against
the old, this has only been done on clinical labels and in other cases as part of depression.
This has left not so much of extensive and explorative work on the subject. On the same note,
studies on anxiety of ageing with regard to the ageing have only been exploited on a clinical
scale. All these are illustration of limited depth of research and analysis of the task. This
study focuses on subclinical anxiety level between the young and the old in relation to
depression.
Numerous research and studies on the effect of depression and anxiety on cognition have
mainly been with relation to anxiety in a wider and general perception even though there is
one study that has given targeted the adults. Still, focus has been on studies targeting
individuals suffering from mild cognitive impairment and dementia while others have
explored formal anxiety disorders. There can be more effects of non-clinical anxiety on the
elements of information processing that what has been recognized and discussed earlier.
Studies on anxiety and age for been for a long time more inclined to clinical level among the
young and older adults. Other studied have delved into an exploration of the effects of
CHAPTER TWO 3
depressive symptoms on cognition among the aged and perceived anxiety as part or one of
the symptoms of depression. There have not been separate studies of subclinical anxiety from
depression despite the fact that anxiety and depression have always been linked with negative
implications on the functions of cognition (Balash et al., 2013). It is against this background
that the study examines the difference in subclinical anxiety level between young and older
adults and their links to depression, demographic parameters and its effects on cognition.
This study will also allow us to understand the differences between young and old in terms of
anxiety very well, in relation to many factors before looking deeply on attention and
information processing speed.
Depression and anxiety disorders are linked with abnormal cognitive control in the form of an
attentional bias towards negative information and reduced inhibitory control (Cisler &
Koster, 2010). Even though there is a high rate for comorbidity of the anxiety disorders and
depression, above 75%, they have various underlying neural correlates. The high comorbidity
implies commonality in etiology (Peckham, McHugh & Otto, 2010). The dorsal anterior
cingulate cortex is involved in inhibitory cognitive control. It detects conflict between
competing neural representations in the perceptuo-motor system and gives a signal to the
dorsa-lateral prefrontal cortex to help in adjusting the system to a regulated level.
Depression and clinical anxiety disorders are severe diseases that affect lives of people, both
mentally and physically (Association, 1998). Some symptoms appear in milder forms even
among individuals considered as psychologically healthy (Park et al., 2010). At the clinical
levels, anxiety and depression severely affect cognitive control (Eysneck & Derakshan,
2007). There is considerable decrease in activity within anterior cortical control structures
which is responsible for most cognitive functions including attention allocation, decision
making and impulse control. There exists evidence of an inverse relationship between
depression and resting-state activity of the anterior cingulate cortex (ACC) (Robinson M. D.,
depressive symptoms on cognition among the aged and perceived anxiety as part or one of
the symptoms of depression. There have not been separate studies of subclinical anxiety from
depression despite the fact that anxiety and depression have always been linked with negative
implications on the functions of cognition (Balash et al., 2013). It is against this background
that the study examines the difference in subclinical anxiety level between young and older
adults and their links to depression, demographic parameters and its effects on cognition.
This study will also allow us to understand the differences between young and old in terms of
anxiety very well, in relation to many factors before looking deeply on attention and
information processing speed.
Depression and anxiety disorders are linked with abnormal cognitive control in the form of an
attentional bias towards negative information and reduced inhibitory control (Cisler &
Koster, 2010). Even though there is a high rate for comorbidity of the anxiety disorders and
depression, above 75%, they have various underlying neural correlates. The high comorbidity
implies commonality in etiology (Peckham, McHugh & Otto, 2010). The dorsal anterior
cingulate cortex is involved in inhibitory cognitive control. It detects conflict between
competing neural representations in the perceptuo-motor system and gives a signal to the
dorsa-lateral prefrontal cortex to help in adjusting the system to a regulated level.
Depression and clinical anxiety disorders are severe diseases that affect lives of people, both
mentally and physically (Association, 1998). Some symptoms appear in milder forms even
among individuals considered as psychologically healthy (Park et al., 2010). At the clinical
levels, anxiety and depression severely affect cognitive control (Eysneck & Derakshan,
2007). There is considerable decrease in activity within anterior cortical control structures
which is responsible for most cognitive functions including attention allocation, decision
making and impulse control. There exists evidence of an inverse relationship between
depression and resting-state activity of the anterior cingulate cortex (ACC) (Robinson M. D.,
CHAPTER TWO 4
2007). A highly depressed individual has a hyperactive performance in the ACC, and at
certain levels of anxiety and depression, it goes into a resting state, bringing a halt to
important cognitive functions like attention allocation (Aaron T beck, Norman Epstein, &
Robert a Steer, 1988).
Just like in clinical anxiety and depression, increased levels of subclinical anxiety and
depression symptoms occur together pointing to the likelihood of the same cause (Pizzagalli
et al., 2006). Taking this approach ends up in major theoretical challenges. This is why most
researchers treat the two as one, since they both point to the same etiologies. Studies done by
various authors (Sadock, 2009) and Anxiety and Depression Association of America
(ADAA) show that anxiety and depression could have the same or different causes or
etiologies (Association, 1998), thus, it is acceptable to test the two separately and compare
results thereafter. By testing the two variables separately and thereafter making a comparison,
the differences and the similarities in the results are compared and explorations and possible
explanations into the reasons for the differences and similarities made. Nonetheless, very
few studies have focused on determining the difference in anxiety level especially subclinical
levels between young and older adults in relation to cognitive functions especially in term of
processing information. Thus, pressing need to understand the differences between anxiety
and depression first, and see how the low levels of anxiety could lead/ or cause depression.
As there is a big overlap that exists between depression and anxiety as most studies normally
treat them as one disorder and a whole clinical illness. Coming up with a more conclusive
distinction could help in developing proper interventions aimed at increasing awareness of
Anxiety levels have been known to lower the cognitive performance of people across all the
age groups (Endler, Johnson, & Flett, 2001). Anxiety loads the brain and cognition requires
brain alertness. When it is active simultaneously, it interferes with C1 neurons and diverts
2007). A highly depressed individual has a hyperactive performance in the ACC, and at
certain levels of anxiety and depression, it goes into a resting state, bringing a halt to
important cognitive functions like attention allocation (Aaron T beck, Norman Epstein, &
Robert a Steer, 1988).
Just like in clinical anxiety and depression, increased levels of subclinical anxiety and
depression symptoms occur together pointing to the likelihood of the same cause (Pizzagalli
et al., 2006). Taking this approach ends up in major theoretical challenges. This is why most
researchers treat the two as one, since they both point to the same etiologies. Studies done by
various authors (Sadock, 2009) and Anxiety and Depression Association of America
(ADAA) show that anxiety and depression could have the same or different causes or
etiologies (Association, 1998), thus, it is acceptable to test the two separately and compare
results thereafter. By testing the two variables separately and thereafter making a comparison,
the differences and the similarities in the results are compared and explorations and possible
explanations into the reasons for the differences and similarities made. Nonetheless, very
few studies have focused on determining the difference in anxiety level especially subclinical
levels between young and older adults in relation to cognitive functions especially in term of
processing information. Thus, pressing need to understand the differences between anxiety
and depression first, and see how the low levels of anxiety could lead/ or cause depression.
As there is a big overlap that exists between depression and anxiety as most studies normally
treat them as one disorder and a whole clinical illness. Coming up with a more conclusive
distinction could help in developing proper interventions aimed at increasing awareness of
Anxiety levels have been known to lower the cognitive performance of people across all the
age groups (Endler, Johnson, & Flett, 2001). Anxiety loads the brain and cognition requires
brain alertness. When it is active simultaneously, it interferes with C1 neurons and diverts
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
CHAPTER TWO 5
attention making the brain less receptive and less effective in information integration (Shah
A, Jhawar, & Goel A, 2011). There is evidence of significant decline in cognitive abilities
among older adults considered to have anxiety disorders which result in cognitive impairment
(Price and Mohlman, 2007). Apart from clinical experiments (Williams JMG & MacLeod,
1998), subclinical anxiety levels have not been seriously researched on in relation to
depression and cognitive function (affects both subjective and objective cognitive and
memory processing ability) in a population-based sample across all age groups.
Goldberg et al., (2003) compared the effect of anxiety on cognitive function of older and
younger people and found that the cognitive ability of the older group is lowered in relation
to thought process, perception and general problem solving, more than that of the younger
group. However, Unterrainer et al., (2018) differ with this observation based on the evidence
from their study, that low anxiety levels and cognitive function of people are not related
regardless of age. The associations they observed in clinical groups differed with ones in
population-based samples. Higher ratings of anxiety were associated with lower planning
performance independent of age. The evidence from the two studies, Mattay et al., (2003) and
Unterrainer et al., (2018) do not adequately explain the effects of subclinical anxiety levels on
cognitive function of individuals. This study explored this difference to help in better
understanding of how different levels of anxiety impair cognition and also help improve
measures in place to evaluate individuals with cognitive problems caused by non-clinical
anxiety and depression. Young and old people have significant differences in how the anxiety
levels affect their cognitive abilities. Old people are less susceptible to different anxiety
levels than young people as will be seen in results section, which is in concurrence with
previous studies. This is mostly because old people are more settled and do not worry about
life and all its troubles. They are more interested in living in peace and integrity. Subjective
attention making the brain less receptive and less effective in information integration (Shah
A, Jhawar, & Goel A, 2011). There is evidence of significant decline in cognitive abilities
among older adults considered to have anxiety disorders which result in cognitive impairment
(Price and Mohlman, 2007). Apart from clinical experiments (Williams JMG & MacLeod,
1998), subclinical anxiety levels have not been seriously researched on in relation to
depression and cognitive function (affects both subjective and objective cognitive and
memory processing ability) in a population-based sample across all age groups.
Goldberg et al., (2003) compared the effect of anxiety on cognitive function of older and
younger people and found that the cognitive ability of the older group is lowered in relation
to thought process, perception and general problem solving, more than that of the younger
group. However, Unterrainer et al., (2018) differ with this observation based on the evidence
from their study, that low anxiety levels and cognitive function of people are not related
regardless of age. The associations they observed in clinical groups differed with ones in
population-based samples. Higher ratings of anxiety were associated with lower planning
performance independent of age. The evidence from the two studies, Mattay et al., (2003) and
Unterrainer et al., (2018) do not adequately explain the effects of subclinical anxiety levels on
cognitive function of individuals. This study explored this difference to help in better
understanding of how different levels of anxiety impair cognition and also help improve
measures in place to evaluate individuals with cognitive problems caused by non-clinical
anxiety and depression. Young and old people have significant differences in how the anxiety
levels affect their cognitive abilities. Old people are less susceptible to different anxiety
levels than young people as will be seen in results section, which is in concurrence with
previous studies. This is mostly because old people are more settled and do not worry about
life and all its troubles. They are more interested in living in peace and integrity. Subjective
CHAPTER TWO 6
and objective cognitive functions are key elements in this study since they determine how
anxiety levels influence cognitive functions of both old and young groups.
METHODS
This section briefly describes the methods used to conduct the investigation, including
participants, measuring instruments, and other details of how the research was conducted.
Ethical Considerations
This study was conducted with the guidance and approval of the Research Ethics Committee
at the University Department of Psychology, which mandates informed consent of all
participants, along with their rights to withdraw from the study at any time. The informed
consent form was signed by all participants. All data collected in this study was blinded to
participant identity and stored under password protection on the researcher’s computer. All
the data is confidential and only accessible to responsible authorities. All data collected was
used for empirical research, and not for any medical purpose.
Participants
Two groups of participants were recruited, older and younger adults. The young group
comprised of students (n=52; age 18-25 years, 21 males: 31 females) recruited from the
Psychology Department at the University. The older group of participants (n=52; age 50-80
years, 31 females: 21 males) were recruited from the community. The average age of the
young individuals was 19.92 (SD=1.57) whereas that of older adults was 66.47 (SD=4.52). In
the younger group, those who participated received 6 credits; older adult participants received
transportation expense assistance only. The young adults were recruited through the
Psychology Subject Pool System. While the older adults were identified and approached via
emails and telephone; advertisement in local newspapers, posters and flyers made the local
population aware of the study. The selection used inclusion criteria that involved individuals
who were not suffering from any clinical anxiety disorder and illustrated regular medical
and objective cognitive functions are key elements in this study since they determine how
anxiety levels influence cognitive functions of both old and young groups.
METHODS
This section briefly describes the methods used to conduct the investigation, including
participants, measuring instruments, and other details of how the research was conducted.
Ethical Considerations
This study was conducted with the guidance and approval of the Research Ethics Committee
at the University Department of Psychology, which mandates informed consent of all
participants, along with their rights to withdraw from the study at any time. The informed
consent form was signed by all participants. All data collected in this study was blinded to
participant identity and stored under password protection on the researcher’s computer. All
the data is confidential and only accessible to responsible authorities. All data collected was
used for empirical research, and not for any medical purpose.
Participants
Two groups of participants were recruited, older and younger adults. The young group
comprised of students (n=52; age 18-25 years, 21 males: 31 females) recruited from the
Psychology Department at the University. The older group of participants (n=52; age 50-80
years, 31 females: 21 males) were recruited from the community. The average age of the
young individuals was 19.92 (SD=1.57) whereas that of older adults was 66.47 (SD=4.52). In
the younger group, those who participated received 6 credits; older adult participants received
transportation expense assistance only. The young adults were recruited through the
Psychology Subject Pool System. While the older adults were identified and approached via
emails and telephone; advertisement in local newspapers, posters and flyers made the local
population aware of the study. The selection used inclusion criteria that involved individuals
who were not suffering from any clinical anxiety disorder and illustrated regular medical
CHAPTER TWO 7
visits indicating good health and no history of neurological and cognitive visual impairments;
the participants who exhibited severe depression and previous history of poor health were
excluded. Other exclusions included poor self-reported general health; past history of head
injury or neurological, medical, or psychological problems; reported cognitive impairment;
vision not normal or corrected to normal; and self-reported medications that impact cognitive
functioning. Two males were excluded from the younger group and one male excluded from
the older group due to severe depression scores in Beck Depression Inventory (BDI). The
participants were briefed about the objectives of the study and its importance to the field of
psychology. After completing the study, debriefing forms were given to them. All the
participants had normal general cognition score (26 or above) that was measured through
Montreal Cognitive Assessment (MoCA). This approach detects objective cognitive
functioning and mild cognitive impairment and assesses such cognitive domains as attention,
concentration, executive functions, memory, language, visuospatial skills, abstraction,
calculation, and orientation (Julayonont et al., 2013). The instrument consists of a variety of
verbal and pencil-and-paper tasks such as drawing a clock, copying a diagram of a cube, and
doing delayed verbal recall of a list of words. Scoring ranges from 0 to 30, with higher scores
indicating less cognitive impairment (Julayanont & Nasreddine, 2017).
Table 1: Demographic Factors of Participants
Mean (SD)
Older
adults
Young
group
Old Males Old Females
Young
Males
Young
Females
Years of
education
14.53
(4.320)
14.722
(.698)
14.70
(5.141)
14.42
(3.804)
14.57
(2.226)
14.82
(3.007)
visits indicating good health and no history of neurological and cognitive visual impairments;
the participants who exhibited severe depression and previous history of poor health were
excluded. Other exclusions included poor self-reported general health; past history of head
injury or neurological, medical, or psychological problems; reported cognitive impairment;
vision not normal or corrected to normal; and self-reported medications that impact cognitive
functioning. Two males were excluded from the younger group and one male excluded from
the older group due to severe depression scores in Beck Depression Inventory (BDI). The
participants were briefed about the objectives of the study and its importance to the field of
psychology. After completing the study, debriefing forms were given to them. All the
participants had normal general cognition score (26 or above) that was measured through
Montreal Cognitive Assessment (MoCA). This approach detects objective cognitive
functioning and mild cognitive impairment and assesses such cognitive domains as attention,
concentration, executive functions, memory, language, visuospatial skills, abstraction,
calculation, and orientation (Julayonont et al., 2013). The instrument consists of a variety of
verbal and pencil-and-paper tasks such as drawing a clock, copying a diagram of a cube, and
doing delayed verbal recall of a list of words. Scoring ranges from 0 to 30, with higher scores
indicating less cognitive impairment (Julayanont & Nasreddine, 2017).
Table 1: Demographic Factors of Participants
Mean (SD)
Older
adults
Young
group
Old Males Old Females
Young
Males
Young
Females
Years of
education
14.53
(4.320)
14.722
(.698)
14.70
(5.141)
14.42
(3.804)
14.57
(2.226)
14.82
(3.007)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CHAPTER TWO 8
Data Collection
The demographic data collected included age, gender and years of education. Some of the
instruments used included consent form, information sheet and debriefing form, questionnaire
as well as demographics form, all found in Appendix A.
Instruments
Participants completed the Beck Anxiety Inventory (BAI) (Steer & Beck A. T, 1997), the
State Trait Anxiety Inventory (STAI) in full (Spielberger, 2010), including both the State and
Trait subsections (STAI-S and STAI-T), the Beck Depression Inventory (BDI) (Beck, Aarno
T, & Robert A, 1996), the Montreal Cognitive Assessment (MoCA) version 7.1 (Ziad S
Nasreddine & Phillips, 2005), and the Prospective-Retrospective Memory Questionnaire
(PRMQ) (Slavin-Mulford & Hilsenroth, 2012). Each of these instruments is described below:
Beck Anxiety Inventory (BAI)
The Beck Anxiety Inventory (BAI) was used to determine participant anxiety levels (Liang,
Wang and Zhu, 2016). This test is a 21-item self-assessment using a four-point Likert scale
(0: “not at all” to 3: “severely”) that focuses on somatic symptoms of anxiety as a way of
distinguishing between anxiety and depression (Julian, 2011). Scoring for the BAI is
computed by adding the scores of the 21 items, and thus ranges from 0 to 63, with higher
scores indicating greater anxiety levels. A score between from 0–21 indicates no to mild
anxiety; a score between 22 and 35 indicates moderate anxiety; and a score between 36 and
63 indicates potentially severe anxiety (Beck, 1988. Reliability of the BAI has been shown
with high internal consistency as measured by Cronbach’s alpha (0.90 to 0.94).
State and Trait Anxiety Inventory (STAI)
The STAI measures the intensity of feelings of anxiety, differentiating between current-state
anxiety in the present and trait anxiety that is a general tendency to perceive situations as
threatening or anxiety-producing (McDowell, 2006). The full STAI has two separate 20-item
Data Collection
The demographic data collected included age, gender and years of education. Some of the
instruments used included consent form, information sheet and debriefing form, questionnaire
as well as demographics form, all found in Appendix A.
Instruments
Participants completed the Beck Anxiety Inventory (BAI) (Steer & Beck A. T, 1997), the
State Trait Anxiety Inventory (STAI) in full (Spielberger, 2010), including both the State and
Trait subsections (STAI-S and STAI-T), the Beck Depression Inventory (BDI) (Beck, Aarno
T, & Robert A, 1996), the Montreal Cognitive Assessment (MoCA) version 7.1 (Ziad S
Nasreddine & Phillips, 2005), and the Prospective-Retrospective Memory Questionnaire
(PRMQ) (Slavin-Mulford & Hilsenroth, 2012). Each of these instruments is described below:
Beck Anxiety Inventory (BAI)
The Beck Anxiety Inventory (BAI) was used to determine participant anxiety levels (Liang,
Wang and Zhu, 2016). This test is a 21-item self-assessment using a four-point Likert scale
(0: “not at all” to 3: “severely”) that focuses on somatic symptoms of anxiety as a way of
distinguishing between anxiety and depression (Julian, 2011). Scoring for the BAI is
computed by adding the scores of the 21 items, and thus ranges from 0 to 63, with higher
scores indicating greater anxiety levels. A score between from 0–21 indicates no to mild
anxiety; a score between 22 and 35 indicates moderate anxiety; and a score between 36 and
63 indicates potentially severe anxiety (Beck, 1988. Reliability of the BAI has been shown
with high internal consistency as measured by Cronbach’s alpha (0.90 to 0.94).
State and Trait Anxiety Inventory (STAI)
The STAI measures the intensity of feelings of anxiety, differentiating between current-state
anxiety in the present and trait anxiety that is a general tendency to perceive situations as
threatening or anxiety-producing (McDowell, 2006). The full STAI has two separate 20-item
CHAPTER TWO 9
scales, the STAI-S Anxiety scale that evaluates current state of anxiety, and the STAI-T
Anxiety scale that evaluates general, long-lasting feelings of anxiety (Dennis, Coghlan and
Vigod, 2013). Reliability of STAI is demonstrated in various publications (McDowell, 2006).
The STAI and the BAI are sometimes suggested to measure different factors of anxiety
(McDowell, 2006). In studies of young adults, the validity comparison between the BAI and
the sister measure BDI, the STAI correlated more closely with BDI than with BAI, implying
that the STAI is actually a closer measure of depression than anxiety (McDowell, 2006). This
measure identifies the current state of trait anxiety. State anxiety stays for a designated time
and often is resolved (Allan et al., 2014). In comparison, trait anxiety lingers for a long time.
The measure can effectively track trait or state anxiety through differentiation. Therefore, if
any individual develops trait anxiety, it could be easily detected using this parameter.
Beck Depression Inventory (BDI)
The BDI is a 21-element self-reporting scale using a four-choice Likert scale (ranked from 0
to 3). The possible scores range from 0 to 63, higher scores indicating greater or more severe
depression (de Oliveira and et.al., 2014). The questions in the BDI focus on cognitive
distortions common in those with depressive symptoms, such as “I blame myself for
everything bad that happens” (Farinde, 2013). It is designed for people who are at least 13
years old, with scores greater than 21 indicating clinical depression, and scores above 30
indicating severe depression. The BDI is designed to be simple to use and quick to
administer, taking less than 10 minutes (Farinde, 2013). The BDI has been demonstrated to
be valid and reliable in adolescent and elderly populations (adolescents: Kauth & Zettle,
1990; elderly: Penk & Robinowitz, 1987; Scogin et al., 1988; Wetherall & Gatz, 2005).
Internal consistency of the BDI has been demonstrated alphas approximating 0.91, and
reliability in test-retest results over a one-week period of 0.93.
scales, the STAI-S Anxiety scale that evaluates current state of anxiety, and the STAI-T
Anxiety scale that evaluates general, long-lasting feelings of anxiety (Dennis, Coghlan and
Vigod, 2013). Reliability of STAI is demonstrated in various publications (McDowell, 2006).
The STAI and the BAI are sometimes suggested to measure different factors of anxiety
(McDowell, 2006). In studies of young adults, the validity comparison between the BAI and
the sister measure BDI, the STAI correlated more closely with BDI than with BAI, implying
that the STAI is actually a closer measure of depression than anxiety (McDowell, 2006). This
measure identifies the current state of trait anxiety. State anxiety stays for a designated time
and often is resolved (Allan et al., 2014). In comparison, trait anxiety lingers for a long time.
The measure can effectively track trait or state anxiety through differentiation. Therefore, if
any individual develops trait anxiety, it could be easily detected using this parameter.
Beck Depression Inventory (BDI)
The BDI is a 21-element self-reporting scale using a four-choice Likert scale (ranked from 0
to 3). The possible scores range from 0 to 63, higher scores indicating greater or more severe
depression (de Oliveira and et.al., 2014). The questions in the BDI focus on cognitive
distortions common in those with depressive symptoms, such as “I blame myself for
everything bad that happens” (Farinde, 2013). It is designed for people who are at least 13
years old, with scores greater than 21 indicating clinical depression, and scores above 30
indicating severe depression. The BDI is designed to be simple to use and quick to
administer, taking less than 10 minutes (Farinde, 2013). The BDI has been demonstrated to
be valid and reliable in adolescent and elderly populations (adolescents: Kauth & Zettle,
1990; elderly: Penk & Robinowitz, 1987; Scogin et al., 1988; Wetherall & Gatz, 2005).
Internal consistency of the BDI has been demonstrated alphas approximating 0.91, and
reliability in test-retest results over a one-week period of 0.93.
CHAPTER TWO 10
Montreal Cognitive Assessment (MoCA)
The MoCA is designed to detect objective cognitive functioning and mild cognitive
impairment and assesses such cognitive domains as attention, concentration, executive
functions, memory, language, visuospatial skills, abstraction, calculation, and orientation
(Julayonont et al., 2013). The instrument consists of a variety of verbal and pencil-and-paper
tasks such as drawing a clock, copying a diagram of a cube, and doing delayed verbal recall
of a list of words. Scoring ranges from 0 to 30, with higher scores indicating less cognitive
impairment (Julayanont and Nasreddine, 2017). The MoCA is commonly used as a screening
tool to detect cognitive impairment from Alzheimer’s disease. This assessment has been used
in order to understand the objective measure in case of cognitive function (Smith, Gildeh, &
Holmes, 2007). It was necessary to examine the cognitive abilities of the participants and
relate the findings to the level of anxiety that they faced at any particular point to assess the
effect of their anxiety, as this was the focal point of the research. By testing the cognitive
abilities of the participants of the experiment, it would be possible to have an idea on the
skills they have towars, recalling, learning or even solving problems. This will illustrate and
help in the identification if the participant could be having any cognitive challenges and thus
subjective memory complaints.
Prospective-Retrospective Memory Questionnaire (PRMQ)
PRMQ is a self-reported instrument that measures prospective and retrospective memory
slips in ordinary living activities (Crawford, Crawford , G, EA, & S, 2003). The instrument
includes 16 items, each with five Likert-scale responses ranging from “very often” (scored as
a 5) to “never” (scored as a 1) in response to questions such as “Do you forget something that
you were told a few minutes before?” Half of the questions refer to retrospective memory
errors and half to prospective memory errors. Scores thus range from 16 to 80. The reliability
of the PRMQ has been estimated at 0.89 overall and 0.84 for prospective scale and 0.80 for
Montreal Cognitive Assessment (MoCA)
The MoCA is designed to detect objective cognitive functioning and mild cognitive
impairment and assesses such cognitive domains as attention, concentration, executive
functions, memory, language, visuospatial skills, abstraction, calculation, and orientation
(Julayonont et al., 2013). The instrument consists of a variety of verbal and pencil-and-paper
tasks such as drawing a clock, copying a diagram of a cube, and doing delayed verbal recall
of a list of words. Scoring ranges from 0 to 30, with higher scores indicating less cognitive
impairment (Julayanont and Nasreddine, 2017). The MoCA is commonly used as a screening
tool to detect cognitive impairment from Alzheimer’s disease. This assessment has been used
in order to understand the objective measure in case of cognitive function (Smith, Gildeh, &
Holmes, 2007). It was necessary to examine the cognitive abilities of the participants and
relate the findings to the level of anxiety that they faced at any particular point to assess the
effect of their anxiety, as this was the focal point of the research. By testing the cognitive
abilities of the participants of the experiment, it would be possible to have an idea on the
skills they have towars, recalling, learning or even solving problems. This will illustrate and
help in the identification if the participant could be having any cognitive challenges and thus
subjective memory complaints.
Prospective-Retrospective Memory Questionnaire (PRMQ)
PRMQ is a self-reported instrument that measures prospective and retrospective memory
slips in ordinary living activities (Crawford, Crawford , G, EA, & S, 2003). The instrument
includes 16 items, each with five Likert-scale responses ranging from “very often” (scored as
a 5) to “never” (scored as a 1) in response to questions such as “Do you forget something that
you were told a few minutes before?” Half of the questions refer to retrospective memory
errors and half to prospective memory errors. Scores thus range from 16 to 80. The reliability
of the PRMQ has been estimated at 0.89 overall and 0.84 for prospective scale and 0.80 for
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
CHAPTER TWO 11
the retrospective scale (Crawford et al., 2003). It does not show any significant statistical
variance for gender or age hence suitable for both sexes (Crawford et al., 2003). For non-
clinical populations, PRMQ has shown mean total scores of 38.88 (SD=9.15), mean
prospective scores on 8 items of 20.18 (SD=4.91) and mean retrospective scores on 8 items
of 18.69 (SD=4.98) (Crawford et al., 2003).
Prospective memory is the ability of an individual to remember planned actions while
retrospective memory is memory regarding the past. Both prospective and retrospective
approaches are general and approximated measurement of memory as they don’t involve any
numerical data which would have been more accurate and good or poor memory is based on
the judgment of the interested party performing memory tests on subjects. Prospective
memory focuses on when to engage in an action as opposed to giving attention to
informational content and is general measure of the ability of an individual to remember to
engage in a planned action, or planned intention at a future point in time and thus a measure
of general engagement. . The researcher can analyze whether the individual has the ability to
remember planned action or events.
RESULTS
Normality Tests
The data collected was analyzed using non-parametric techniques. Since the variables were
not evenly distributed, non-parametric methods were the most appropriate tests for the data
(Altman & Bland, 2009) since the number of observations in the study is below 2000,
Shapiro-Wilk test was used to show normality of various variables based on age and gender.
The population sample was very small since just a few people agreed to take part in the
experiment to completion thereby prompting the use of non-parametric techniques. In this
study, it was assumed that most of the population data had a normal distribution statistical
nature which further facilitated the use of non-parametric techniques. Both groups lack a
the retrospective scale (Crawford et al., 2003). It does not show any significant statistical
variance for gender or age hence suitable for both sexes (Crawford et al., 2003). For non-
clinical populations, PRMQ has shown mean total scores of 38.88 (SD=9.15), mean
prospective scores on 8 items of 20.18 (SD=4.91) and mean retrospective scores on 8 items
of 18.69 (SD=4.98) (Crawford et al., 2003).
Prospective memory is the ability of an individual to remember planned actions while
retrospective memory is memory regarding the past. Both prospective and retrospective
approaches are general and approximated measurement of memory as they don’t involve any
numerical data which would have been more accurate and good or poor memory is based on
the judgment of the interested party performing memory tests on subjects. Prospective
memory focuses on when to engage in an action as opposed to giving attention to
informational content and is general measure of the ability of an individual to remember to
engage in a planned action, or planned intention at a future point in time and thus a measure
of general engagement. . The researcher can analyze whether the individual has the ability to
remember planned action or events.
RESULTS
Normality Tests
The data collected was analyzed using non-parametric techniques. Since the variables were
not evenly distributed, non-parametric methods were the most appropriate tests for the data
(Altman & Bland, 2009) since the number of observations in the study is below 2000,
Shapiro-Wilk test was used to show normality of various variables based on age and gender.
The population sample was very small since just a few people agreed to take part in the
experiment to completion thereby prompting the use of non-parametric techniques. In this
study, it was assumed that most of the population data had a normal distribution statistical
nature which further facilitated the use of non-parametric techniques. Both groups lack a
CHAPTER TWO 12
normal distribution in BAI, p<0.05. The observations in the young group lack a normal
distribution in state anxiety, p<0.05, whereas the observations for the older adults are
normally distributed in state anxiety, p>0.05. In trait anxiety, the young group has a normal
distribution, p>0.05, while the older adults lack a normal distribution. The observations for
both young and older adults lack a normal distribution in BDI, p<0.05; this is similar for
MoCA. Lastly, the observations for both groups depict a normal distribution in PRMQ,
p>0.05.SPSS non-parametric analysis was also conducted due to the varied nature of the data
in which some were normally distributed and others not. As some of the data were normally
distributed and some of them not, SPSS non-parametric analysis was also conducted.
Age Comparison: Anxiety levels
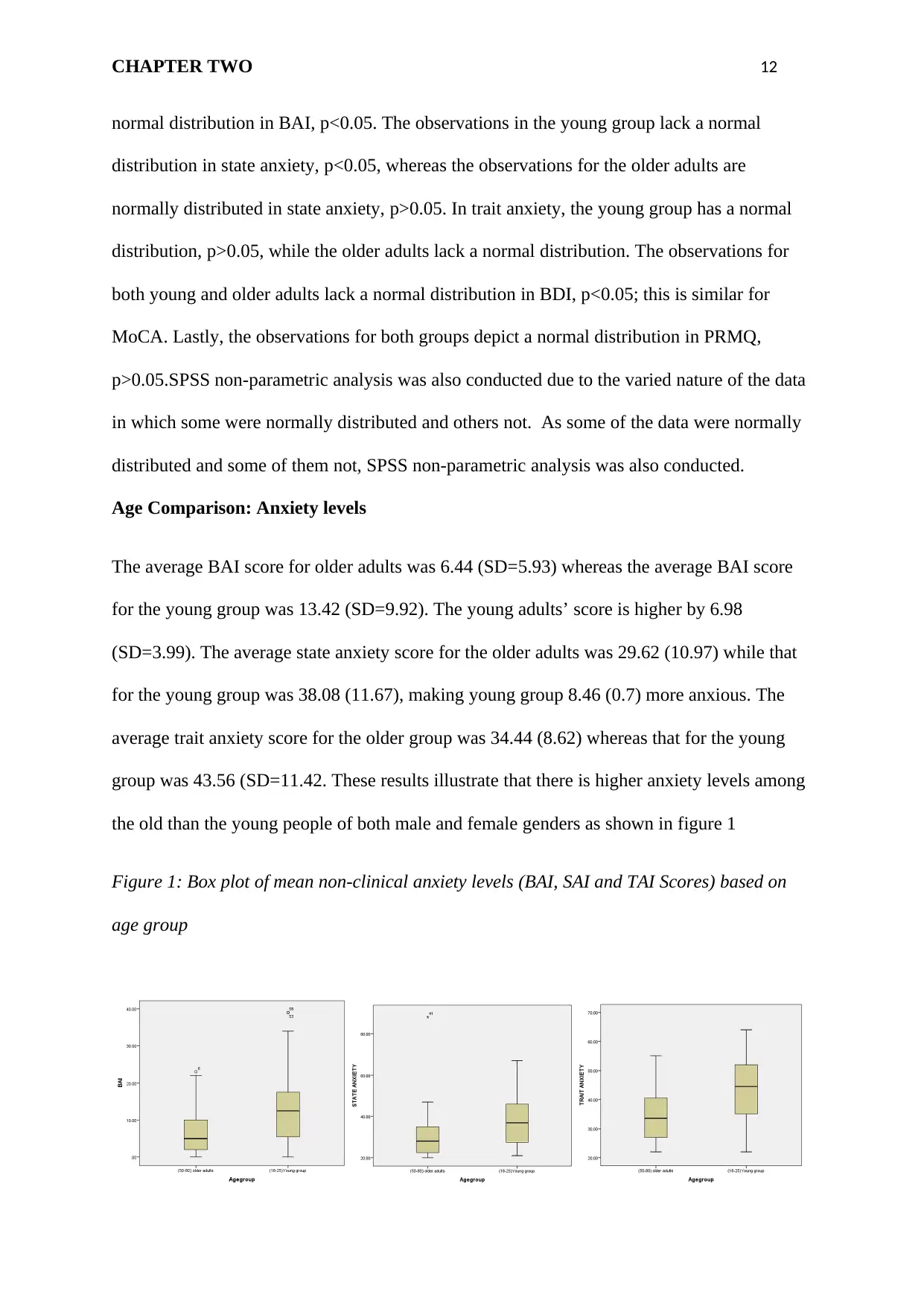
The average BAI score for older adults was 6.44 (SD=5.93) whereas the average BAI score
for the young group was 13.42 (SD=9.92). The young adults’ score is higher by 6.98
(SD=3.99). The average state anxiety score for the older adults was 29.62 (10.97) while that
for the young group was 38.08 (11.67), making young group 8.46 (0.7) more anxious. The
average trait anxiety score for the older group was 34.44 (8.62) whereas that for the young
group was 43.56 (SD=11.42. These results illustrate that there is higher anxiety levels among
the old than the young people of both male and female genders as shown in figure 1
Figure 1: Box plot of mean non-clinical anxiety levels (BAI, SAI and TAI Scores) based on
age group
normal distribution in BAI, p<0.05. The observations in the young group lack a normal
distribution in state anxiety, p<0.05, whereas the observations for the older adults are
normally distributed in state anxiety, p>0.05. In trait anxiety, the young group has a normal
distribution, p>0.05, while the older adults lack a normal distribution. The observations for
both young and older adults lack a normal distribution in BDI, p<0.05; this is similar for
MoCA. Lastly, the observations for both groups depict a normal distribution in PRMQ,
p>0.05.SPSS non-parametric analysis was also conducted due to the varied nature of the data
in which some were normally distributed and others not. As some of the data were normally
distributed and some of them not, SPSS non-parametric analysis was also conducted.
Age Comparison: Anxiety levels
The average BAI score for older adults was 6.44 (SD=5.93) whereas the average BAI score
for the young group was 13.42 (SD=9.92). The young adults’ score is higher by 6.98
(SD=3.99). The average state anxiety score for the older adults was 29.62 (10.97) while that
for the young group was 38.08 (11.67), making young group 8.46 (0.7) more anxious. The
average trait anxiety score for the older group was 34.44 (8.62) whereas that for the young
group was 43.56 (SD=11.42. These results illustrate that there is higher anxiety levels among
the old than the young people of both male and female genders as shown in figure 1
Figure 1: Box plot of mean non-clinical anxiety levels (BAI, SAI and TAI Scores) based on
age group
CHAPTER TWO 13
Mann-Whitney U test was used to determine the difference in anxiety scores between the
young and the older groups. The null hypothesis that was tested states that there is no
significant difference in the anxiety scores between the young and the older adults. There was
a significant difference in the BAI, SAI and TAI scores between the young and older adults
(U=742.00, p=0.00;n2 =0.31), (U=708.50, p=0.00;n2 =0.34) and (U=732.50, p=0.00;n2 =0.32
) respectively. This shows that the young adults were more anxious than older adults
Gender Comparison: Anxiety levels
Older Adults
Average BAI score in older males was 7.30 (SD=7.53) whereas the average score for older
females was 5.90 (SD=4.71). The average SAI score for older males was 29.00 (SD=7.44)
whereas that for older females was 30.00 (SD=12.79). The average TAI score for older males
was 34.90 (SD=9.00) whereas that for older females was 34.16 (SD=8.51) Older males were
higher in both BAI and state of anxiety scores, by 1.4(SD=2.82) and 0.74(SD=0.49)
respectively demonstrating that older males are more prone to anxiety than their counterpart
older females. .
In older adults, Mann-Whitney analysis revealed no significant difference between old males
and old females in BAI, SAI and TAI scores, (U=314.50, p=0.92; n2 =0.00), (U=304.50,
p=0.77;n2 =0.00) and (U=301.50, p=0.73;n2 =0.00) respectively.
Young Adults
The average BAI score for the young males was 9.90 (SD=10.81) while that for young
females was 15.80 (SD=8.65). The mean state anxiety score for young males was 36.00
Mann-Whitney U test was used to determine the difference in anxiety scores between the
young and the older groups. The null hypothesis that was tested states that there is no
significant difference in the anxiety scores between the young and the older adults. There was
a significant difference in the BAI, SAI and TAI scores between the young and older adults
(U=742.00, p=0.00;n2 =0.31), (U=708.50, p=0.00;n2 =0.34) and (U=732.50, p=0.00;n2 =0.32
) respectively. This shows that the young adults were more anxious than older adults
Gender Comparison: Anxiety levels
Older Adults
Average BAI score in older males was 7.30 (SD=7.53) whereas the average score for older
females was 5.90 (SD=4.71). The average SAI score for older males was 29.00 (SD=7.44)
whereas that for older females was 30.00 (SD=12.79). The average TAI score for older males
was 34.90 (SD=9.00) whereas that for older females was 34.16 (SD=8.51) Older males were
higher in both BAI and state of anxiety scores, by 1.4(SD=2.82) and 0.74(SD=0.49)
respectively demonstrating that older males are more prone to anxiety than their counterpart
older females. .
In older adults, Mann-Whitney analysis revealed no significant difference between old males
and old females in BAI, SAI and TAI scores, (U=314.50, p=0.92; n2 =0.00), (U=304.50,
p=0.77;n2 =0.00) and (U=301.50, p=0.73;n2 =0.00) respectively.
Young Adults
The average BAI score for the young males was 9.90 (SD=10.81) while that for young
females was 15.80 (SD=8.65). The mean state anxiety score for young males was 36.00
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CHAPTER TWO 14
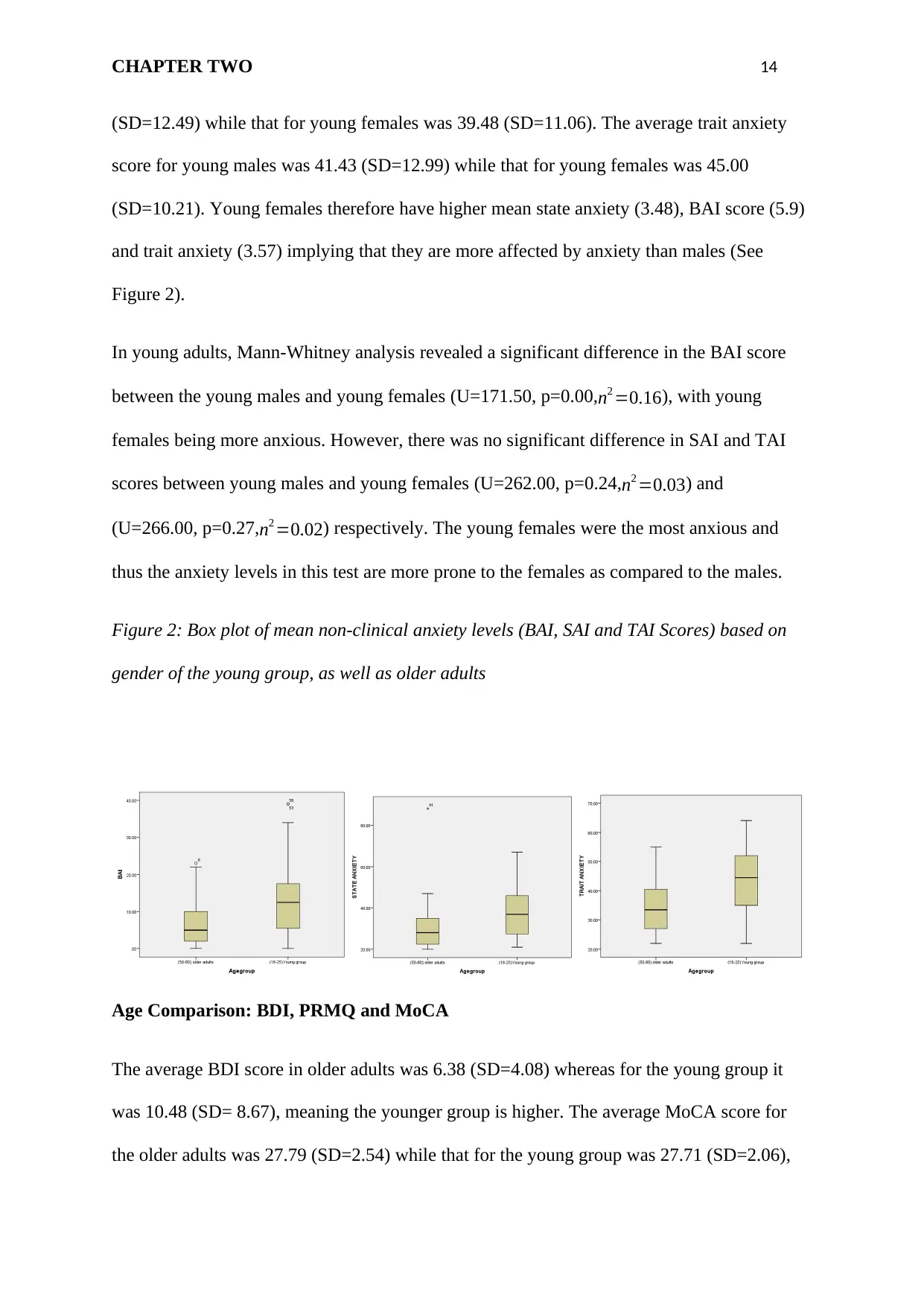
(SD=12.49) while that for young females was 39.48 (SD=11.06). The average trait anxiety
score for young males was 41.43 (SD=12.99) while that for young females was 45.00
(SD=10.21). Young females therefore have higher mean state anxiety (3.48), BAI score (5.9)
and trait anxiety (3.57) implying that they are more affected by anxiety than males (See
Figure 2).
In young adults, Mann-Whitney analysis revealed a significant difference in the BAI score
between the young males and young females (U=171.50, p=0.00, n2 =0.16), with young
females being more anxious. However, there was no significant difference in SAI and TAI
scores between young males and young females (U=262.00, p=0.24,n2 =0.03) and
(U=266.00, p=0.27,n2 =0.02) respectively. The young females were the most anxious and
thus the anxiety levels in this test are more prone to the females as compared to the males.
Figure 2: Box plot of mean non-clinical anxiety levels (BAI, SAI and TAI Scores) based on
gender of the young group, as well as older adults
Age Comparison: BDI, PRMQ and MoCA
The average BDI score in older adults was 6.38 (SD=4.08) whereas for the young group it
was 10.48 (SD= 8.67), meaning the younger group is higher. The average MoCA score for
the older adults was 27.79 (SD=2.54) while that for the young group was 27.71 (SD=2.06),
(SD=12.49) while that for young females was 39.48 (SD=11.06). The average trait anxiety
score for young males was 41.43 (SD=12.99) while that for young females was 45.00
(SD=10.21). Young females therefore have higher mean state anxiety (3.48), BAI score (5.9)
and trait anxiety (3.57) implying that they are more affected by anxiety than males (See
Figure 2).
In young adults, Mann-Whitney analysis revealed a significant difference in the BAI score
between the young males and young females (U=171.50, p=0.00, n2 =0.16), with young
females being more anxious. However, there was no significant difference in SAI and TAI
scores between young males and young females (U=262.00, p=0.24,n2 =0.03) and
(U=266.00, p=0.27,n2 =0.02) respectively. The young females were the most anxious and
thus the anxiety levels in this test are more prone to the females as compared to the males.
Figure 2: Box plot of mean non-clinical anxiety levels (BAI, SAI and TAI Scores) based on
gender of the young group, as well as older adults
Age Comparison: BDI, PRMQ and MoCA
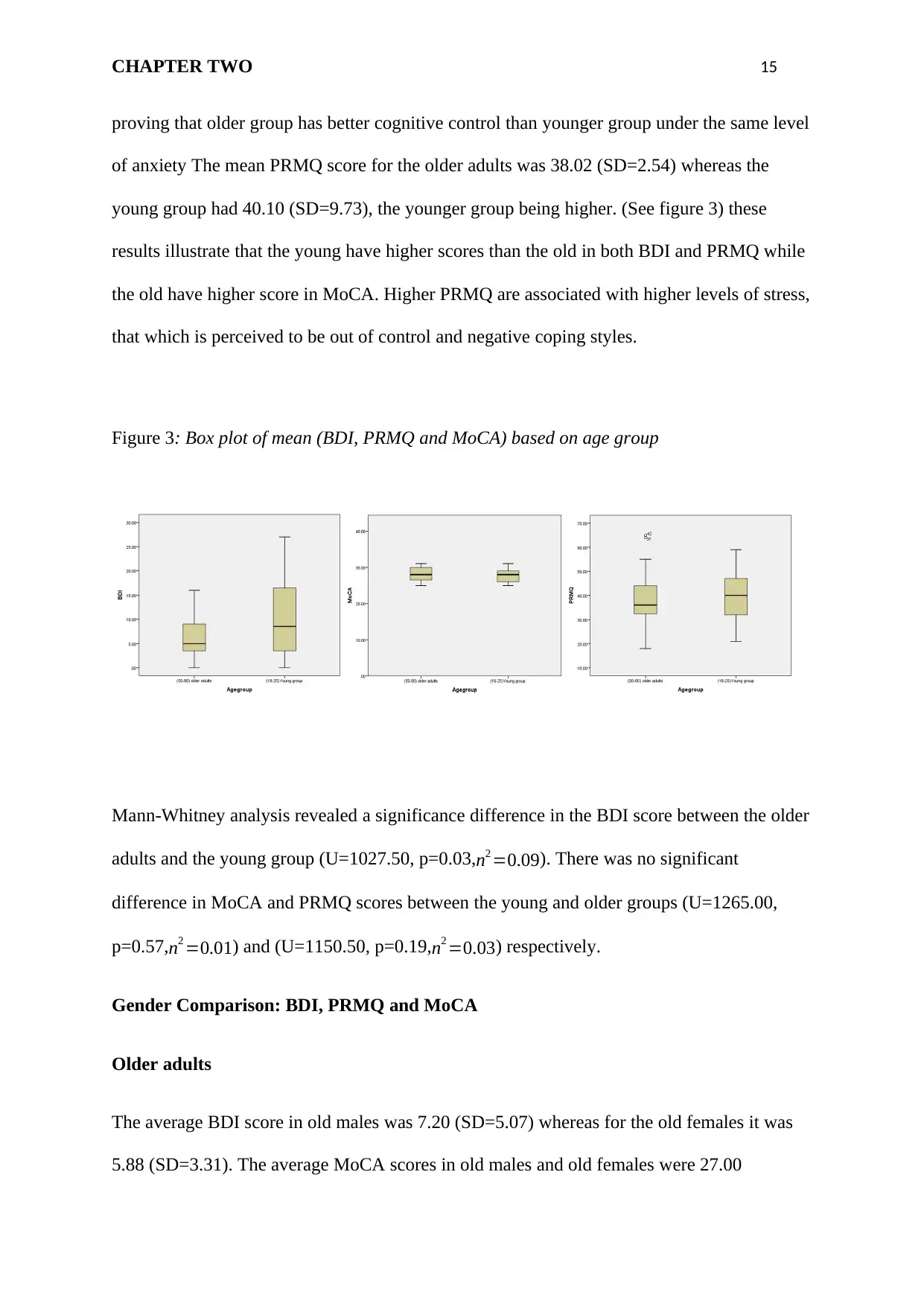
The average BDI score in older adults was 6.38 (SD=4.08) whereas for the young group it
was 10.48 (SD= 8.67), meaning the younger group is higher. The average MoCA score for
the older adults was 27.79 (SD=2.54) while that for the young group was 27.71 (SD=2.06),
CHAPTER TWO 15
proving that older group has better cognitive control than younger group under the same level
of anxiety The mean PRMQ score for the older adults was 38.02 (SD=2.54) whereas the
young group had 40.10 (SD=9.73), the younger group being higher. (See figure 3) these
results illustrate that the young have higher scores than the old in both BDI and PRMQ while
the old have higher score in MoCA. Higher PRMQ are associated with higher levels of stress,
that which is perceived to be out of control and negative coping styles.
Figure 3: Box plot of mean (BDI, PRMQ and MoCA) based on age group
Mann-Whitney analysis revealed a significance difference in the BDI score between the older
adults and the young group (U=1027.50, p=0.03,n2 =0.09). There was no significant
difference in MoCA and PRMQ scores between the young and older groups (U=1265.00,
p=0.57,n2 =0.01) and (U=1150.50, p=0.19,n2 =0.03) respectively.
Gender Comparison: BDI, PRMQ and MoCA
Older adults
The average BDI score in old males was 7.20 (SD=5.07) whereas for the old females it was
5.88 (SD=3.31). The average MoCA scores in old males and old females were 27.00
proving that older group has better cognitive control than younger group under the same level
of anxiety The mean PRMQ score for the older adults was 38.02 (SD=2.54) whereas the
young group had 40.10 (SD=9.73), the younger group being higher. (See figure 3) these
results illustrate that the young have higher scores than the old in both BDI and PRMQ while
the old have higher score in MoCA. Higher PRMQ are associated with higher levels of stress,
that which is perceived to be out of control and negative coping styles.
Figure 3: Box plot of mean (BDI, PRMQ and MoCA) based on age group
Mann-Whitney analysis revealed a significance difference in the BDI score between the older
adults and the young group (U=1027.50, p=0.03,n2 =0.09). There was no significant
difference in MoCA and PRMQ scores between the young and older groups (U=1265.00,
p=0.57,n2 =0.01) and (U=1150.50, p=0.19,n2 =0.03) respectively.
Gender Comparison: BDI, PRMQ and MoCA
Older adults
The average BDI score in old males was 7.20 (SD=5.07) whereas for the old females it was
5.88 (SD=3.31). The average MoCA scores in old males and old females were 27.00
CHAPTER TWO 16
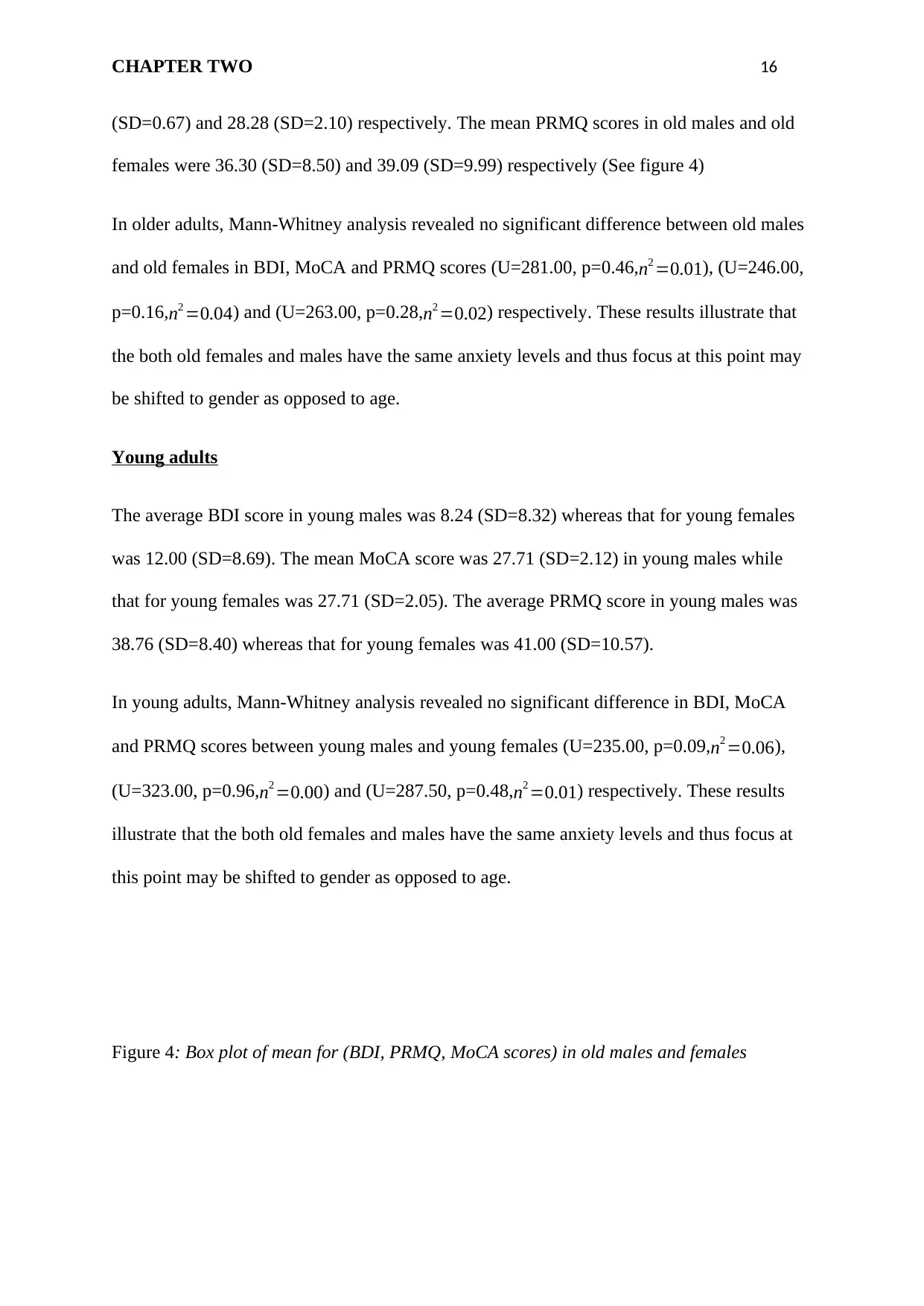
(SD=0.67) and 28.28 (SD=2.10) respectively. The mean PRMQ scores in old males and old
females were 36.30 (SD=8.50) and 39.09 (SD=9.99) respectively (See figure 4)
In older adults, Mann-Whitney analysis revealed no significant difference between old males
and old females in BDI, MoCA and PRMQ scores (U=281.00, p=0.46,n2 =0.01), (U=246.00,
p=0.16,n2 =0.04) and (U=263.00, p=0.28, n2 =0.02) respectively. These results illustrate that
the both old females and males have the same anxiety levels and thus focus at this point may
be shifted to gender as opposed to age.
Young adults
The average BDI score in young males was 8.24 (SD=8.32) whereas that for young females
was 12.00 (SD=8.69). The mean MoCA score was 27.71 (SD=2.12) in young males while
that for young females was 27.71 (SD=2.05). The average PRMQ score in young males was
38.76 (SD=8.40) whereas that for young females was 41.00 (SD=10.57).
In young adults, Mann-Whitney analysis revealed no significant difference in BDI, MoCA
and PRMQ scores between young males and young females (U=235.00, p=0.09,n2 =0.06),
(U=323.00, p=0.96,n2 =0.00) and (U=287.50, p=0.48, n2 =0.01) respectively. These results
illustrate that the both old females and males have the same anxiety levels and thus focus at
this point may be shifted to gender as opposed to age.
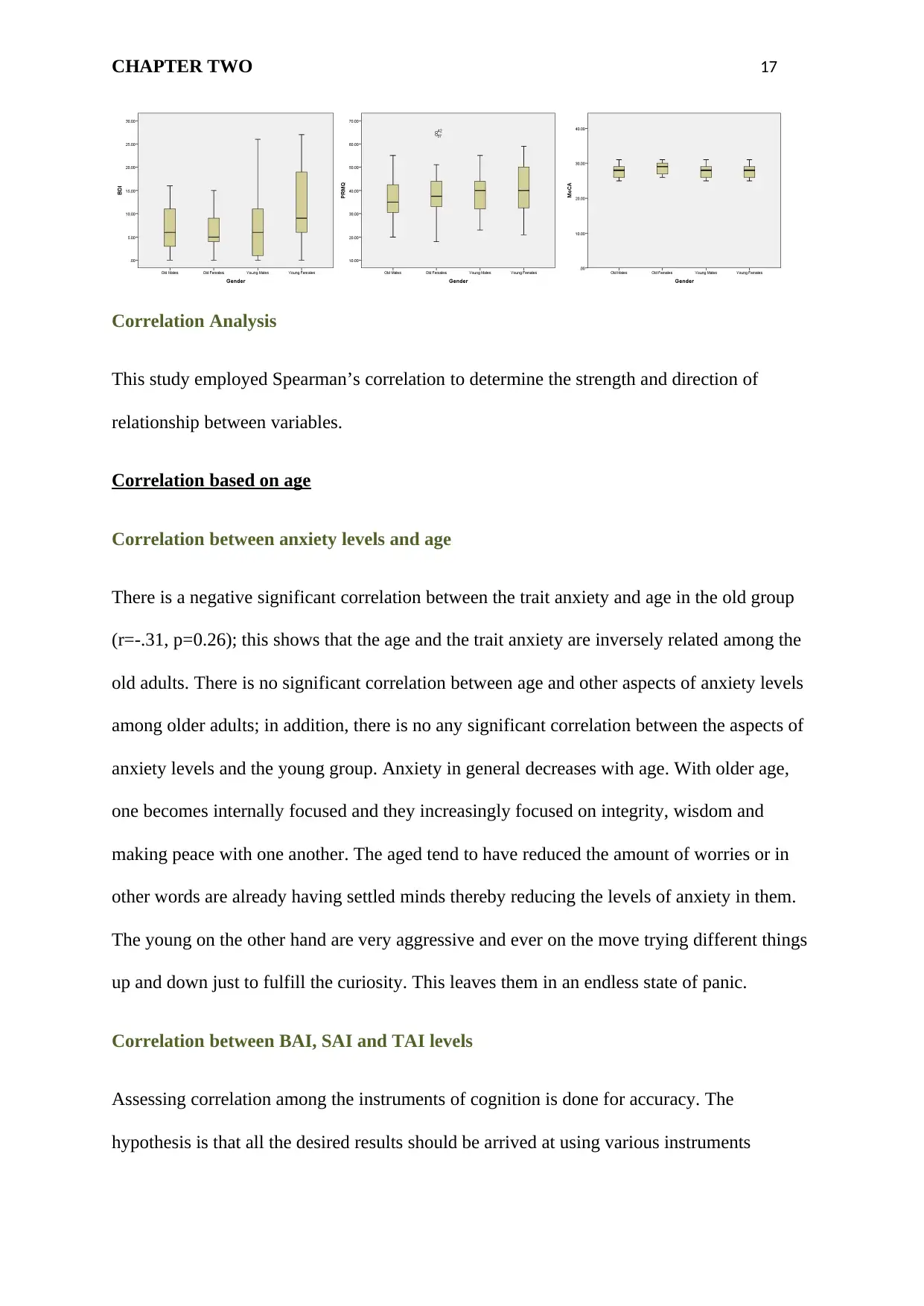
Figure 4: Box plot of mean for (BDI, PRMQ, MoCA scores) in old males and females
(SD=0.67) and 28.28 (SD=2.10) respectively. The mean PRMQ scores in old males and old
females were 36.30 (SD=8.50) and 39.09 (SD=9.99) respectively (See figure 4)
In older adults, Mann-Whitney analysis revealed no significant difference between old males
and old females in BDI, MoCA and PRMQ scores (U=281.00, p=0.46,n2 =0.01), (U=246.00,
p=0.16,n2 =0.04) and (U=263.00, p=0.28, n2 =0.02) respectively. These results illustrate that
the both old females and males have the same anxiety levels and thus focus at this point may
be shifted to gender as opposed to age.
Young adults
The average BDI score in young males was 8.24 (SD=8.32) whereas that for young females
was 12.00 (SD=8.69). The mean MoCA score was 27.71 (SD=2.12) in young males while
that for young females was 27.71 (SD=2.05). The average PRMQ score in young males was
38.76 (SD=8.40) whereas that for young females was 41.00 (SD=10.57).
In young adults, Mann-Whitney analysis revealed no significant difference in BDI, MoCA
and PRMQ scores between young males and young females (U=235.00, p=0.09,n2 =0.06),
(U=323.00, p=0.96,n2 =0.00) and (U=287.50, p=0.48, n2 =0.01) respectively. These results
illustrate that the both old females and males have the same anxiety levels and thus focus at
this point may be shifted to gender as opposed to age.
Figure 4: Box plot of mean for (BDI, PRMQ, MoCA scores) in old males and females
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
CHAPTER TWO 17
Correlation Analysis
This study employed Spearman’s correlation to determine the strength and direction of
relationship between variables.
Correlation based on age
Correlation between anxiety levels and age
There is a negative significant correlation between the trait anxiety and age in the old group
(r=-.31, p=0.26); this shows that the age and the trait anxiety are inversely related among the
old adults. There is no significant correlation between age and other aspects of anxiety levels
among older adults; in addition, there is no any significant correlation between the aspects of
anxiety levels and the young group. Anxiety in general decreases with age. With older age,
one becomes internally focused and they increasingly focused on integrity, wisdom and
making peace with one another. The aged tend to have reduced the amount of worries or in
other words are already having settled minds thereby reducing the levels of anxiety in them.
The young on the other hand are very aggressive and ever on the move trying different things
up and down just to fulfill the curiosity. This leaves them in an endless state of panic.
Correlation between BAI, SAI and TAI levels
Assessing correlation among the instruments of cognition is done for accuracy. The
hypothesis is that all the desired results should be arrived at using various instruments
Correlation Analysis
This study employed Spearman’s correlation to determine the strength and direction of
relationship between variables.
Correlation based on age
Correlation between anxiety levels and age
There is a negative significant correlation between the trait anxiety and age in the old group
(r=-.31, p=0.26); this shows that the age and the trait anxiety are inversely related among the
old adults. There is no significant correlation between age and other aspects of anxiety levels
among older adults; in addition, there is no any significant correlation between the aspects of
anxiety levels and the young group. Anxiety in general decreases with age. With older age,
one becomes internally focused and they increasingly focused on integrity, wisdom and
making peace with one another. The aged tend to have reduced the amount of worries or in
other words are already having settled minds thereby reducing the levels of anxiety in them.
The young on the other hand are very aggressive and ever on the move trying different things
up and down just to fulfill the curiosity. This leaves them in an endless state of panic.
Correlation between BAI, SAI and TAI levels
Assessing correlation among the instruments of cognition is done for accuracy. The
hypothesis is that all the desired results should be arrived at using various instruments
CHAPTER TWO 18
without much deviation from each other. There is a positive significant correlation between
TAI anxiety and BAI in the older group, (r=.33, p=0.02). There is also a positive significant
correlation between SAI and TAI in the older group, (r=.72, p=.000). In addition, there is a
positive significant correlation between BAI and STAI in the younger group, (r=.62, p=.000)
and (r=.67 p=.000), as well as there is a positive significant correlation between SAI and TAI
in the younger group, (r=.78, p=.000). The correlation between the two instruments can be
used in establishing the accuracy and reliability of the findings from the experiment.
Correlation between anxiety levels and years of education
There are no significant correlations between the years of education and aspects of anxiety
levels in both young and older adults (p > .05).
Correlation between anxiety levels and handedness
There are no significant correlations between the handedness and the aspects of anxiety levels
in both young and older adults (p > .05).
Correlation between anxiety levels and eyesight/vision
There are no significant correlations between the vision and aspects of anxiety levels in both
young and older adults (p > .05).
Correlation between anxiety levels and depression
There is significant positive correlation between depression and state anxiety in older adults
(r=.36, p=0.01); this is a positive relationship. Moreover, depression and trait anxiety have a
positive significant relationship in older adults (r=.40, p=0.00). There is a significant positive
relationship between state anxiety and depression in the young group (r=.74, p=0.00); also,
there is a positive significant correlation between the trait anxiety and depression in the
without much deviation from each other. There is a positive significant correlation between
TAI anxiety and BAI in the older group, (r=.33, p=0.02). There is also a positive significant
correlation between SAI and TAI in the older group, (r=.72, p=.000). In addition, there is a
positive significant correlation between BAI and STAI in the younger group, (r=.62, p=.000)
and (r=.67 p=.000), as well as there is a positive significant correlation between SAI and TAI
in the younger group, (r=.78, p=.000). The correlation between the two instruments can be
used in establishing the accuracy and reliability of the findings from the experiment.
Correlation between anxiety levels and years of education
There are no significant correlations between the years of education and aspects of anxiety
levels in both young and older adults (p > .05).
Correlation between anxiety levels and handedness
There are no significant correlations between the handedness and the aspects of anxiety levels
in both young and older adults (p > .05).
Correlation between anxiety levels and eyesight/vision
There are no significant correlations between the vision and aspects of anxiety levels in both
young and older adults (p > .05).
Correlation between anxiety levels and depression
There is significant positive correlation between depression and state anxiety in older adults
(r=.36, p=0.01); this is a positive relationship. Moreover, depression and trait anxiety have a
positive significant relationship in older adults (r=.40, p=0.00). There is a significant positive
relationship between state anxiety and depression in the young group (r=.74, p=0.00); also,
there is a positive significant correlation between the trait anxiety and depression in the
CHAPTER TWO 19
young group (r=.78, p=0.00). This could be taken to illustrate that anxiety has an impact
depression in all the genders and across every age group even though at greater magnitude I
older adults. Depression is thus a health challenge that affects every individual and hence
mitigating measures should be set in place to ensure awareness is creating which may help in
checking on the levels of its impacts.
The correlation between anxiety levels and objective cognitive Function (MoCA)
There is no significant correlation between the levels of anxiety and objective cognitive
function (MoCA) in both the older adults and the young group (p > .05).
The correlation between anxiety levels and subjective memory complaint (PRMQ)
There is a significant positive correlation between the state anxiety and subjective memory
complaint in older adults (r=.32, p=0.00). In addition, the trait anxiety and subjective memory
complaint in older adults have a positive significant correlation (r=.50, p=.00). There is a
significant positive correlation between the subjective memory complaint and trait anxiety in
the younger group (r=.34, p=.01). These positive correlations indicate that the variables have
a uniform relationship; increase in one variable might result in a significant increase in the
other variable. This means that there is an increase in subjective memory complaints as one
increase in the age. Subjective memory complaints may reflect quite early in the health of an
individual with subtle variations in cognition and the accompanying personality traits in older
adults.
Correlations by Gender
The correlation between anxiety levels and gender
There is a significant negative correlation between trait anxiety and age in old males, (r=-.50,
p=0.03); an inverse relationship indicates that an increase in age reduces the trait anxiety,
while no significant correlation between age and aspects of anxiety level is made in old
females, young males and young females. This means that older males are least affected by
young group (r=.78, p=0.00). This could be taken to illustrate that anxiety has an impact
depression in all the genders and across every age group even though at greater magnitude I
older adults. Depression is thus a health challenge that affects every individual and hence
mitigating measures should be set in place to ensure awareness is creating which may help in
checking on the levels of its impacts.
The correlation between anxiety levels and objective cognitive Function (MoCA)
There is no significant correlation between the levels of anxiety and objective cognitive
function (MoCA) in both the older adults and the young group (p > .05).
The correlation between anxiety levels and subjective memory complaint (PRMQ)
There is a significant positive correlation between the state anxiety and subjective memory
complaint in older adults (r=.32, p=0.00). In addition, the trait anxiety and subjective memory
complaint in older adults have a positive significant correlation (r=.50, p=.00). There is a
significant positive correlation between the subjective memory complaint and trait anxiety in
the younger group (r=.34, p=.01). These positive correlations indicate that the variables have
a uniform relationship; increase in one variable might result in a significant increase in the
other variable. This means that there is an increase in subjective memory complaints as one
increase in the age. Subjective memory complaints may reflect quite early in the health of an
individual with subtle variations in cognition and the accompanying personality traits in older
adults.
Correlations by Gender
The correlation between anxiety levels and gender
There is a significant negative correlation between trait anxiety and age in old males, (r=-.50,
p=0.03); an inverse relationship indicates that an increase in age reduces the trait anxiety,
while no significant correlation between age and aspects of anxiety level is made in old
females, young males and young females. This means that older males are least affected by
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CHAPTER TWO 20
anxiety whereas as the relationship between anxiety and gender in the old and young females
and young males is insignificant. This can be taken to be the female gender is not affected by
anxiety at any age while the males feel the negative impacts of anxiety when they age.
Correlation between BAI, STAI and TAI levels
There is a positive significant correlation between BAI and STAI in old males group, (r=.45,
p=0.046) and (r=.59, p=0.006), because they are close measures of anxiety levels. There is
also a positive significant correlation between STAI and TAI in old males, (r=.65, p=.002). In
addition, there is a positive significant correlation between STAI and TAI in old females,
(r=.79, p=.000). Also, there is a positive significant correlation between BAI, STAI in the
young males, (r=.56, p=.008) and (r=.70 p=.000), as well as a positive significant correlation
between state anxiety and trait anxiety in the same group, (r=.86, p=.000). There is a positive
significant correlation between BAI, STAI and TAI in the young females, (r=.56, p=.001)
and (r=.60, p=.000), as well as a positive significant correlation between state anxiety and
trait anxiety in the same group, (r=.69, p=.000).
The correlation between anxiety levels and years of education
There is no significant correlation between years of education and aspects of anxiety in old
males, old females, young males and young females (p> .05).
The correlation between anxiety levels and handedness
There is no significant correlation between handedness and aspects of anxiety in old males
and females, and young males and females (p > .05).
The correlation between anxiety levels and vision
There is no significant correlation between vision and the aspects of anxiety in old males, old
females, young males and young females (p > .05).
anxiety whereas as the relationship between anxiety and gender in the old and young females
and young males is insignificant. This can be taken to be the female gender is not affected by
anxiety at any age while the males feel the negative impacts of anxiety when they age.
Correlation between BAI, STAI and TAI levels
There is a positive significant correlation between BAI and STAI in old males group, (r=.45,
p=0.046) and (r=.59, p=0.006), because they are close measures of anxiety levels. There is
also a positive significant correlation between STAI and TAI in old males, (r=.65, p=.002). In
addition, there is a positive significant correlation between STAI and TAI in old females,
(r=.79, p=.000). Also, there is a positive significant correlation between BAI, STAI in the
young males, (r=.56, p=.008) and (r=.70 p=.000), as well as a positive significant correlation
between state anxiety and trait anxiety in the same group, (r=.86, p=.000). There is a positive
significant correlation between BAI, STAI and TAI in the young females, (r=.56, p=.001)
and (r=.60, p=.000), as well as a positive significant correlation between state anxiety and
trait anxiety in the same group, (r=.69, p=.000).
The correlation between anxiety levels and years of education
There is no significant correlation between years of education and aspects of anxiety in old
males, old females, young males and young females (p> .05).
The correlation between anxiety levels and handedness
There is no significant correlation between handedness and aspects of anxiety in old males
and females, and young males and females (p > .05).
The correlation between anxiety levels and vision
There is no significant correlation between vision and the aspects of anxiety in old males, old
females, young males and young females (p > .05).
CHAPTER TWO 21
The correlation between anxiety levels and depression
There is a positive significant correlation between the trait anxiety and depression in old
males (r=.51, p=.02); increase in depression increases with the trait anxiety. There is a
positive significant correlation between state anxiety and depression in young males and
young females (r=.64, p=.00) and (r=.80, p=.00) respectively. Both young males and females
depict a positive significant correlation between depression and the trait anxiety (r=.82,
p=.00) and (r=.72, p=.00). This could be taken to illustrate that anxiety has an impact
depression in all the genders and across every age group. Depression is thus a health
challenge that affects every individual and hence mitigating measures should be set in place
to ensure awareness is creating which may help in checking on the levels of its impacts.
The correlation between anxiety levels and objective cognitive Function (MoCA)
There is no significant correlation between objective cognitive function and aspects of
anxiety in old males, old females, young males and young females (p > .05).
The correlation between anxiety levels and subjective memory complaint (PRMQ)
There is a positive significant correlation between trait anxiety and subjective memory
complaint in old males, (r=.60, p=0.01). State anxiety and subjective memory complaint have
a positive significant correlation in old females (r=.36, p=0.045), including significant
positive correlation between trait anxiety and subjective memory complaint, (r=.47, p=0.01).
The young females have a positive significant correlation between subjective memory
complaint and state anxiety and trait anxiety, (r=.37, p=.04) and (r=.46, p=.01) respectively.
Positive correlation between subjective memory complaint and anxiety levels depict that
increase in anxiety levels affects the subjective memory complaint negatively. This was
illustrated by the higher complaints received from the group of people with subjective
memory complaints as they reacted to as they illustrated a sort of frightened feeling as if there
was something awful that was yet to happen to them. This was an interesting finding that
The correlation between anxiety levels and depression
There is a positive significant correlation between the trait anxiety and depression in old
males (r=.51, p=.02); increase in depression increases with the trait anxiety. There is a
positive significant correlation between state anxiety and depression in young males and
young females (r=.64, p=.00) and (r=.80, p=.00) respectively. Both young males and females
depict a positive significant correlation between depression and the trait anxiety (r=.82,
p=.00) and (r=.72, p=.00). This could be taken to illustrate that anxiety has an impact
depression in all the genders and across every age group. Depression is thus a health
challenge that affects every individual and hence mitigating measures should be set in place
to ensure awareness is creating which may help in checking on the levels of its impacts.
The correlation between anxiety levels and objective cognitive Function (MoCA)
There is no significant correlation between objective cognitive function and aspects of
anxiety in old males, old females, young males and young females (p > .05).
The correlation between anxiety levels and subjective memory complaint (PRMQ)
There is a positive significant correlation between trait anxiety and subjective memory
complaint in old males, (r=.60, p=0.01). State anxiety and subjective memory complaint have
a positive significant correlation in old females (r=.36, p=0.045), including significant
positive correlation between trait anxiety and subjective memory complaint, (r=.47, p=0.01).
The young females have a positive significant correlation between subjective memory
complaint and state anxiety and trait anxiety, (r=.37, p=.04) and (r=.46, p=.01) respectively.
Positive correlation between subjective memory complaint and anxiety levels depict that
increase in anxiety levels affects the subjective memory complaint negatively. This was
illustrated by the higher complaints received from the group of people with subjective
memory complaints as they reacted to as they illustrated a sort of frightened feeling as if there
was something awful that was yet to happen to them. This was an interesting finding that
CHAPTER TWO 22
could give insights in the cardinal feature of anxiety. These results conclude that there is a
relationship between subjective memory complaint and anxiety.
DISCUSSION
As can be observed from the above results, there is a positive correlation between trait
anxiety and subjective memory complaint in old males, no significant correlation between
objective cognitive function and aspects of anxiety in all age groups and gender, no
significant correlation between vision and the aspects of anxiety in old males in all the groups
and gender, a positive significant correlation between the trait anxiety and depression in old
males, no significant correlation between handedness and aspects of anxiety in all groups and
gender among other findings from the experiment.
Subclinical anxiety levels between young and older adults, and its effects on their cognition is
therefore of significance. The study expounds on this subject and finds that different levels of
anxiety cause different levels of depression which affect cognition differently. More anxiety
mostly causes more depression and worse cognition impairment as a result (Beaudreau &
O'hara, 2008) . Age determines how much effect anxiety will have on cognition, with older
people less susceptible.
Considering age and gender difference between the young and old groups, anxiety in old
males was found to be significant, reducing with increase in age. As one age, he/she becomes
internally focused and increasingly sensitive on matters integrity, wisdom and peace,
explaining the decrease in anxiety with age. This conforms to previous studies made
(Gottfries CG, 1998), (Jorm AF, 2005). Jorm in his study says that when examining anxiety
and depression with age, the most common trend was for an initial rise with age, then a drop.
There is a significant positive correlation between depression and anxiety, both state and trait
anxiety. A higher level of state or trait anxiety was found to be directly proportional to levels
could give insights in the cardinal feature of anxiety. These results conclude that there is a
relationship between subjective memory complaint and anxiety.
DISCUSSION
As can be observed from the above results, there is a positive correlation between trait
anxiety and subjective memory complaint in old males, no significant correlation between
objective cognitive function and aspects of anxiety in all age groups and gender, no
significant correlation between vision and the aspects of anxiety in old males in all the groups
and gender, a positive significant correlation between the trait anxiety and depression in old
males, no significant correlation between handedness and aspects of anxiety in all groups and
gender among other findings from the experiment.
Subclinical anxiety levels between young and older adults, and its effects on their cognition is
therefore of significance. The study expounds on this subject and finds that different levels of
anxiety cause different levels of depression which affect cognition differently. More anxiety
mostly causes more depression and worse cognition impairment as a result (Beaudreau &
O'hara, 2008) . Age determines how much effect anxiety will have on cognition, with older
people less susceptible.
Considering age and gender difference between the young and old groups, anxiety in old
males was found to be significant, reducing with increase in age. As one age, he/she becomes
internally focused and increasingly sensitive on matters integrity, wisdom and peace,
explaining the decrease in anxiety with age. This conforms to previous studies made
(Gottfries CG, 1998), (Jorm AF, 2005). Jorm in his study says that when examining anxiety
and depression with age, the most common trend was for an initial rise with age, then a drop.
There is a significant positive correlation between depression and anxiety, both state and trait
anxiety. A higher level of state or trait anxiety was found to be directly proportional to levels
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
CHAPTER TWO 23
of depression, to clinical levels. (Klerman, 1977) Klerman in his handbook of studies on
depression says that non-psychotic depression forms, commonly called neurotic depression,
occur in patients who exhibited symptoms of anxiety neurosis. (Lader, 1983)(Citation) Lader
also confirms that both conditions are accompanied by a number of physical and
psychological changes that are identical.
Non-clinical anxiety levels, state and trait anxiety, in young and old groups were found to
cause significant subjective memory complaint (DiMatteo, Lepper, & Croghan, 2000). The
variables have a uniform relationship, direct proportionality, an increase in one leading to
more subjective memory complaint. (Reid & MacLullich , 2006)Louise M Reid’s study
shows that subjective memory complaints and cognitive impairment in older people were
very consistently related to personality traits e.g., anxiety neurosis and depression.
According to MoCA, subclinical anxiety has no significant correlation between objective
cognitive functions in young and old groups (Zelinski EM & Cr., 1990). It could make one
more active and attentive to the particular event causing the anxiety. Further increase in
subclinical anxiety however, affects cognitive functions adversely, causing panic and related
attacks, and eventually depression (Bassuk SS, Berkman LF, & Wypij D, 1998). (Balash,
2012) Yacov Balash however, disagrees stating that there is significant cognitive
performance decline in elders with associated subclinical anxiety and subjective memory
complaints. He focuses on the elderly only, and does not look at the whole population, which
makes the little significance of declining cognitive ability of the elderly quite negligible.
Demographic factors i.e., years of education, handedness and vision were found to have very
little effect on causing anxiety though they play an important role in brain and cognitive
functioning. Other studies (Goldenberg) confirm this fact and stress that demographic factors
of depression, to clinical levels. (Klerman, 1977) Klerman in his handbook of studies on
depression says that non-psychotic depression forms, commonly called neurotic depression,
occur in patients who exhibited symptoms of anxiety neurosis. (Lader, 1983)(Citation) Lader
also confirms that both conditions are accompanied by a number of physical and
psychological changes that are identical.
Non-clinical anxiety levels, state and trait anxiety, in young and old groups were found to
cause significant subjective memory complaint (DiMatteo, Lepper, & Croghan, 2000). The
variables have a uniform relationship, direct proportionality, an increase in one leading to
more subjective memory complaint. (Reid & MacLullich , 2006)Louise M Reid’s study
shows that subjective memory complaints and cognitive impairment in older people were
very consistently related to personality traits e.g., anxiety neurosis and depression.
According to MoCA, subclinical anxiety has no significant correlation between objective
cognitive functions in young and old groups (Zelinski EM & Cr., 1990). It could make one
more active and attentive to the particular event causing the anxiety. Further increase in
subclinical anxiety however, affects cognitive functions adversely, causing panic and related
attacks, and eventually depression (Bassuk SS, Berkman LF, & Wypij D, 1998). (Balash,
2012) Yacov Balash however, disagrees stating that there is significant cognitive
performance decline in elders with associated subclinical anxiety and subjective memory
complaints. He focuses on the elderly only, and does not look at the whole population, which
makes the little significance of declining cognitive ability of the elderly quite negligible.
Demographic factors i.e., years of education, handedness and vision were found to have very
little effect on causing anxiety though they play an important role in brain and cognitive
functioning. Other studies (Goldenberg) confirm this fact and stress that demographic factors
CHAPTER TWO 24
affect an individual’s self-esteem. In cases where one’s self-esteem is low, anxiety crops in,
but of very low subclinical value.
The findings from this research are in support of the hypothesis of this study that claimed a
correlation between anxiety levels and subjective memory complaints. This is also in
agreement with the findings from the previous research and works by preceding scholars
even though their work mainly focused on anxiety levels and subjective memory complaints
on the elderly. Still, the higher scores of PMRQ were linked to poor memory performance
and execute of function tasks. Another hypothesis is that they would be a relationship
between subjective memory complaints and negative emotional changes among them
depression and anxiety. The results illustrated high scores in subjective memory complaints
association with subclinical levels of depression and anxiety as well as more negative
interpersonal interactions. A deeper understanding of the variables that are associated with
subjective memory complaints may serve as a guide on how to identity cognitive changes as
early as possible and thus establishing the institutions for interventions. Numerous effective
strategies for cognitive training have been identified by researcher.
Generally, the older demographic group do not seek help for subjective memory complaints.
The fee that turn up for such assistance risk by turned away by the healthcare providers
owing to possibilities of negative impairment results for formal neurocognitive tests. The
measures adopted in this study may be of significance help in the identification of preclinical
MCI individuals especially when a self-report scale is used in measuring subjective memory
complaints alongside short measures of cognition, mean-in-life and mood.
A number of limitations should be taken into account when interpreting the findings of this
study. The sample of people that are used as participant are a group of well educated,
professionally skilful as well as reasonably healthy participants who have greater
affect an individual’s self-esteem. In cases where one’s self-esteem is low, anxiety crops in,
but of very low subclinical value.
The findings from this research are in support of the hypothesis of this study that claimed a
correlation between anxiety levels and subjective memory complaints. This is also in
agreement with the findings from the previous research and works by preceding scholars
even though their work mainly focused on anxiety levels and subjective memory complaints
on the elderly. Still, the higher scores of PMRQ were linked to poor memory performance
and execute of function tasks. Another hypothesis is that they would be a relationship
between subjective memory complaints and negative emotional changes among them
depression and anxiety. The results illustrated high scores in subjective memory complaints
association with subclinical levels of depression and anxiety as well as more negative
interpersonal interactions. A deeper understanding of the variables that are associated with
subjective memory complaints may serve as a guide on how to identity cognitive changes as
early as possible and thus establishing the institutions for interventions. Numerous effective
strategies for cognitive training have been identified by researcher.
Generally, the older demographic group do not seek help for subjective memory complaints.
The fee that turn up for such assistance risk by turned away by the healthcare providers
owing to possibilities of negative impairment results for formal neurocognitive tests. The
measures adopted in this study may be of significance help in the identification of preclinical
MCI individuals especially when a self-report scale is used in measuring subjective memory
complaints alongside short measures of cognition, mean-in-life and mood.
A number of limitations should be taken into account when interpreting the findings of this
study. The sample of people that are used as participant are a group of well educated,
professionally skilful as well as reasonably healthy participants who have greater
CHAPTER TWO 25
involvement with men and women. Non-restrictive eligibility and adjustments of the statics
was used in compensating the problem that resulted from generalizability. Another possible
limitation to the study is selection bias since the sample was composed of only those people
who accepted to take part in the study and had full information. Nonetheless, there was a low
level of loss that was to be followed up which was found to be nondifferential across all the
sites considered throughout the study.
Future research will be more focused on treatment of both subclinical and clinical anxiety and
depression disorders on their different levels of intensity. Current treatment of such disorders
is general, regardless of the extent of damage already caused to the patients. If heeded,
recovery of patients will be faster. More study on depression and its link to anxiety is
currently being done to gain better understanding on the disorders they are responsible for,
and how to prevent them in future.
Previous research on matters of anxiety and depression based more on the older population,
and are mostly not usually population-based. This research however, is population-based,
including both the young and old adults. This has given rise to other questions that should be
researched on for improvements in the field of psychology:
How can patients suffering from depression as a result of different subclinical
anxiety levels be assessed
There are treatment measures in place for treatment of anxiety and depressive
disorders, but are so far not specific to different levels of subclinical anxiety. The
modes in place are normal treatment, for normal cases, and isolation treatment for
extreme cases. Studies should therefore commence in filling up the intermediary
mode of treatment for varying levels of anxiety disorders.
involvement with men and women. Non-restrictive eligibility and adjustments of the statics
was used in compensating the problem that resulted from generalizability. Another possible
limitation to the study is selection bias since the sample was composed of only those people
who accepted to take part in the study and had full information. Nonetheless, there was a low
level of loss that was to be followed up which was found to be nondifferential across all the
sites considered throughout the study.
Future research will be more focused on treatment of both subclinical and clinical anxiety and
depression disorders on their different levels of intensity. Current treatment of such disorders
is general, regardless of the extent of damage already caused to the patients. If heeded,
recovery of patients will be faster. More study on depression and its link to anxiety is
currently being done to gain better understanding on the disorders they are responsible for,
and how to prevent them in future.
Previous research on matters of anxiety and depression based more on the older population,
and are mostly not usually population-based. This research however, is population-based,
including both the young and old adults. This has given rise to other questions that should be
researched on for improvements in the field of psychology:
How can patients suffering from depression as a result of different subclinical
anxiety levels be assessed
There are treatment measures in place for treatment of anxiety and depressive
disorders, but are so far not specific to different levels of subclinical anxiety. The
modes in place are normal treatment, for normal cases, and isolation treatment for
extreme cases. Studies should therefore commence in filling up the intermediary
mode of treatment for varying levels of anxiety disorders.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CHAPTER TWO 26
How can both young and old adults be assessed differently for subclinical anxiety
related disorders? Young and old people have different susceptibilities to anxiety
and are therefore affected differently. The mode of treatment administered should be
different and more effective than the current ones. Studies should be focused on the
mode of treatment to help these generations.
These questions give insights to the details of the study and how the findings from the
experiment can be made more meaningful. The aim of the study is to examine the difference
in subclinical anxiety levels between young and older adults in relation anxiety. This aim is
best achievable when all the characteristics of the study population are taken into
consideration. This will give a wide range of findings from which comparison and analysis is
to be made.
Limitations and recommendations
During the research, the number of adults with or without subjective memory complaints was
not enough. We could not therefore make conclusive comparisons between age and anxiety
on subjective memory. Most of the participants in their groups were at the same levels of
education, or had had almost the same amount of years of education in different fields. This
could be the reason why we did not find any differences in anxiety levels correlation with
education levels. We did not use any neurophysiological equipment, such as EEG or FMRI
machines; to see brain functions during testing thus all of the anatomical relations discussed
in this study are theoretical making it challenging to draw conclusive arguments can therefore
not be drawn from these results. The instruments used in data collection, including PRMQ,
BAI. STAI, TAI, do not give 100% accuracy, and are therefore subjects to more scrutiny.
More studies should be centered on assessment of anxiety disorders at its different levels of
intensity. Psychological associations should invest more in the study of anxiety, depression
How can both young and old adults be assessed differently for subclinical anxiety
related disorders? Young and old people have different susceptibilities to anxiety
and are therefore affected differently. The mode of treatment administered should be
different and more effective than the current ones. Studies should be focused on the
mode of treatment to help these generations.
These questions give insights to the details of the study and how the findings from the
experiment can be made more meaningful. The aim of the study is to examine the difference
in subclinical anxiety levels between young and older adults in relation anxiety. This aim is
best achievable when all the characteristics of the study population are taken into
consideration. This will give a wide range of findings from which comparison and analysis is
to be made.
Limitations and recommendations
During the research, the number of adults with or without subjective memory complaints was
not enough. We could not therefore make conclusive comparisons between age and anxiety
on subjective memory. Most of the participants in their groups were at the same levels of
education, or had had almost the same amount of years of education in different fields. This
could be the reason why we did not find any differences in anxiety levels correlation with
education levels. We did not use any neurophysiological equipment, such as EEG or FMRI
machines; to see brain functions during testing thus all of the anatomical relations discussed
in this study are theoretical making it challenging to draw conclusive arguments can therefore
not be drawn from these results. The instruments used in data collection, including PRMQ,
BAI. STAI, TAI, do not give 100% accuracy, and are therefore subjects to more scrutiny.
More studies should be centered on assessment of anxiety disorders at its different levels of
intensity. Psychological associations should invest more in the study of anxiety, depression
CHAPTER TWO 27
and cognition as it is an important and wide aspect of psychology and neuroscience that has
not been delved into yet.
Conclusion
There was established a correlation between subjective memory complaints and subclinical
anxiety. Such findings suggest how useful self-scale measuring subjective memory
complaints in collaboration with short measures if subclinical anxiety is. Such an approach is
one excellent approach that can be used in the identification of the vulnerability of the elders
too the changes in the cognitive performance. Still, assistance to individual suffering from
subjective memory complaints may be done through changes in the lifestyles. To achieve
such benefit, there is need to create awareness among the various demographic groups on the
significance of measuring subjective memory complaints in everyone.
Demographic factors do not cause much anxiety, but should not be ignored altogether.
Subjective memory functions and objective cognitive functions are the ones most affected by
non-clinical anxiety as seen in the study. Therefore, it is necessary to come up with pro-active
measures to deal with subclinical anxiety depending on their intensity in an individual.
Research into this aspect of subclinical anxiety and depression should be intensified.
It would be more accurate to test anxiety levels by examining brain activity using EEG and
FMRI machines in patients exhibiting symptoms of subclinical anxiety, which would confirm
the findings of this study.
From the study, it is clear that young people are more affected with clinical and non-clinical
anxiety and depression effects than the older population. This is an indication that programs
should be initiated to study the cause of their worrying levels of anxiety and create awareness
among the youth, and teach them about these conditions, so that those that are affected can
come out and get help.
and cognition as it is an important and wide aspect of psychology and neuroscience that has
not been delved into yet.
Conclusion
There was established a correlation between subjective memory complaints and subclinical
anxiety. Such findings suggest how useful self-scale measuring subjective memory
complaints in collaboration with short measures if subclinical anxiety is. Such an approach is
one excellent approach that can be used in the identification of the vulnerability of the elders
too the changes in the cognitive performance. Still, assistance to individual suffering from
subjective memory complaints may be done through changes in the lifestyles. To achieve
such benefit, there is need to create awareness among the various demographic groups on the
significance of measuring subjective memory complaints in everyone.
Demographic factors do not cause much anxiety, but should not be ignored altogether.
Subjective memory functions and objective cognitive functions are the ones most affected by
non-clinical anxiety as seen in the study. Therefore, it is necessary to come up with pro-active
measures to deal with subclinical anxiety depending on their intensity in an individual.
Research into this aspect of subclinical anxiety and depression should be intensified.
It would be more accurate to test anxiety levels by examining brain activity using EEG and
FMRI machines in patients exhibiting symptoms of subclinical anxiety, which would confirm
the findings of this study.
From the study, it is clear that young people are more affected with clinical and non-clinical
anxiety and depression effects than the older population. This is an indication that programs
should be initiated to study the cause of their worrying levels of anxiety and create awareness
among the youth, and teach them about these conditions, so that those that are affected can
come out and get help.

CHAPTER TWO 28
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
CHAPTER TWO 29
References
Aaron T Beck, Gary Brown, Robert a Steer, Judy I Eidelson, & John H Riskind. (1987).
Differentiating anxiety and depression: A test of the cognitive content-specifiity and
hypothesis. Journal of abnormal psychology, 179.
Aaron T beck, Norman Epstein, G. B., & Robert a Steer. (1988). Aninventory for measuring
clinical anxiety: psychometric properties. Journal of consulting and clinical
psychology , 893.
Administration, U. A. (2013). Older Americans Behavioral Health issue brief 6:Depression
and Anxiety: Screening and Intervention.
Altman, G. D., & Bland, M. J. (2009). Parametric vs Non-parametric methods of data
analysis. Cambridge: BMJ Publishing Group.
antoinette M Lee, sieu Keung Lam, & Daniel Yee Tak Fong. (2007). Prevalence, course, and
risk factors for antenatal anxiety and depression. Obstetrics & Gynecology, 1102-
1112.
Association, A. P. (1998). Diagnostic and statistical manual of mental disorders. Washington
DC.
Balash, Y. (2012). Subjective Memory Complaints with effective state and cognitive
peerformance in elders. Tel Aviv, Israel.
Bassett SS, & Folstein MF. (1993). Memory complaint, memory performance and psychiatric
diagnosis . A commmunity study, 145-154.
References
Aaron T Beck, Gary Brown, Robert a Steer, Judy I Eidelson, & John H Riskind. (1987).
Differentiating anxiety and depression: A test of the cognitive content-specifiity and
hypothesis. Journal of abnormal psychology, 179.
Aaron T beck, Norman Epstein, G. B., & Robert a Steer. (1988). Aninventory for measuring
clinical anxiety: psychometric properties. Journal of consulting and clinical
psychology , 893.
Administration, U. A. (2013). Older Americans Behavioral Health issue brief 6:Depression
and Anxiety: Screening and Intervention.
Altman, G. D., & Bland, M. J. (2009). Parametric vs Non-parametric methods of data
analysis. Cambridge: BMJ Publishing Group.
antoinette M Lee, sieu Keung Lam, & Daniel Yee Tak Fong. (2007). Prevalence, course, and
risk factors for antenatal anxiety and depression. Obstetrics & Gynecology, 1102-
1112.
Association, A. P. (1998). Diagnostic and statistical manual of mental disorders. Washington
DC.
Balash, Y. (2012). Subjective Memory Complaints with effective state and cognitive
peerformance in elders. Tel Aviv, Israel.
Bassett SS, & Folstein MF. (1993). Memory complaint, memory performance and psychiatric
diagnosis . A commmunity study, 145-154.
CHAPTER TWO 30
Bassuk SS, Berkman LF, & Wypij D. (1998). Depressive symptomatology and Incident
cognitive decline in an elderly community sample. Arch Gen Psychiatry, 1073-1081.
Beaudreau, S. A., & O'hara, R. (2008). Late-life anxiety and cognitive impairment: a review.
The American Journal of Geriatric Psychiatry, 790-803.
Crawford, Crawford , J., G, S., EA, M., & S, D. S. (2003). The Prospective and Retrospective
Memory Questionnaire. 261-275.
Daniel L Segal, & sara Honn Qualls. (2018). Aging and Mental Health. John Wiley & Sons.
Daniela C Goncalves, & Byrne, G. J. (2012). Interventions for generalized anxiety disorder in
older adults: systematic review and meta-analysis. Journal of Anxiety disorders 26(1),
1-11.
David A Clark, & Aaron t Beck. (2010). Cognitive theory and therapyof anxiety and
depression: Convergence with neurobiological findings. Trends in cognitive sciences,
418-424.
David Watson, Kris Weber, Jana Smith Assenheimer, & Lee anna Clark. (1995). Testing a
tripartite model: Evaluating the convergent and discriminant validity of anxiety and
depression symptom scale. Journal of abnormal psychology, 3.
DiMatteo, M. R., Lepper, S. H., & Croghan, T. W. (2000). Depression is a risk factor for
non-compliance with medical treatment: meta-analysis of the effects of anxiety and
depression on patient adherence. Archives of Internal Medicine, 2101-2107.
EJM Bierman, & HC Comijs. (2005). Effect of Anxiety versus depression on cognition in
later life. The American Journal Of Geriatric Psychiatry, 686-693.
Bassuk SS, Berkman LF, & Wypij D. (1998). Depressive symptomatology and Incident
cognitive decline in an elderly community sample. Arch Gen Psychiatry, 1073-1081.
Beaudreau, S. A., & O'hara, R. (2008). Late-life anxiety and cognitive impairment: a review.
The American Journal of Geriatric Psychiatry, 790-803.
Crawford, Crawford , J., G, S., EA, M., & S, D. S. (2003). The Prospective and Retrospective
Memory Questionnaire. 261-275.
Daniel L Segal, & sara Honn Qualls. (2018). Aging and Mental Health. John Wiley & Sons.
Daniela C Goncalves, & Byrne, G. J. (2012). Interventions for generalized anxiety disorder in
older adults: systematic review and meta-analysis. Journal of Anxiety disorders 26(1),
1-11.
David A Clark, & Aaron t Beck. (2010). Cognitive theory and therapyof anxiety and
depression: Convergence with neurobiological findings. Trends in cognitive sciences,
418-424.
David Watson, Kris Weber, Jana Smith Assenheimer, & Lee anna Clark. (1995). Testing a
tripartite model: Evaluating the convergent and discriminant validity of anxiety and
depression symptom scale. Journal of abnormal psychology, 3.
DiMatteo, M. R., Lepper, S. H., & Croghan, T. W. (2000). Depression is a risk factor for
non-compliance with medical treatment: meta-analysis of the effects of anxiety and
depression on patient adherence. Archives of Internal Medicine, 2101-2107.
EJM Bierman, & HC Comijs. (2005). Effect of Anxiety versus depression on cognition in
later life. The American Journal Of Geriatric Psychiatry, 686-693.
CHAPTER TWO 31
Endler, N. S., Johnson, J. M., & Flett, G. M. (2001). General self-efficacy and control in
relation to anxiety and cognitive performance. Current Psychology, 36-52.
Erkinjuntti T, Ostbye T, & Steenhuis R, H. V. (1997). The effect of different diagnostic
criteria on the prevalence of dementia. N Engl J Med, 1667-1674.
Eysneck, M. W., & Derakshan, N. (2007). anxiety and Cognitive Perforance: Attentional
Control Theory. Emotion, 336.
Flicker C, & Ferris SH, R. B. (1993). A longitudinal study of cognitive function in persons
with subjective memory complaints. J Am Geriatr , 1029-1032.
Gail Davies, & Sarah E Harris, C. A. (2014). A genome-wide association study implicates the
APOE locus in non-pathological cognitive ageing. Molecular Psychiatry, 1.
Goldenberg, R. B. (n.d.). The power of personality: The comparative validity of personality
traits,socio-economic status and cognitive ability for predicting important life
outcomes. Perspective on psychological science, 313-345.
Gottfries CG, e. a. (1998). Is there a difference between elderly and younger patients with
regard to the symptomatology and aetiology of depression? Intl Psychopharmacol.
Jiro takaki, Tadahiro Nishi, & Hiromi Shimoyama. (2005). Possible interactive effects of
demograohic factors and stress coping mechanisms on depression and anxiety in
maintenance hemodialysis patients. Journal of psychosomatic research , 217-223.
Jones RN, & Gallo JJ. (2001). Education bias in the mini-mental state examination. Int
Psychogeriatr, 299-310.
Jorm AF, e. a. (2005). Age group differences in psychological distress: The role of
psychosocial risk factors that vary with age. Psychol Med.
Endler, N. S., Johnson, J. M., & Flett, G. M. (2001). General self-efficacy and control in
relation to anxiety and cognitive performance. Current Psychology, 36-52.
Erkinjuntti T, Ostbye T, & Steenhuis R, H. V. (1997). The effect of different diagnostic
criteria on the prevalence of dementia. N Engl J Med, 1667-1674.
Eysneck, M. W., & Derakshan, N. (2007). anxiety and Cognitive Perforance: Attentional
Control Theory. Emotion, 336.
Flicker C, & Ferris SH, R. B. (1993). A longitudinal study of cognitive function in persons
with subjective memory complaints. J Am Geriatr , 1029-1032.
Gail Davies, & Sarah E Harris, C. A. (2014). A genome-wide association study implicates the
APOE locus in non-pathological cognitive ageing. Molecular Psychiatry, 1.
Goldenberg, R. B. (n.d.). The power of personality: The comparative validity of personality
traits,socio-economic status and cognitive ability for predicting important life
outcomes. Perspective on psychological science, 313-345.
Gottfries CG, e. a. (1998). Is there a difference between elderly and younger patients with
regard to the symptomatology and aetiology of depression? Intl Psychopharmacol.
Jiro takaki, Tadahiro Nishi, & Hiromi Shimoyama. (2005). Possible interactive effects of
demograohic factors and stress coping mechanisms on depression and anxiety in
maintenance hemodialysis patients. Journal of psychosomatic research , 217-223.
Jones RN, & Gallo JJ. (2001). Education bias in the mini-mental state examination. Int
Psychogeriatr, 299-310.
Jorm AF, e. a. (2005). Age group differences in psychological distress: The role of
psychosocial risk factors that vary with age. Psychol Med.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CHAPTER TWO 32
Julie Hugo, & mary Ganguli. (2014). Dementia and cognitive impairment: epidemiology,
diagnosis, and treatment. Clinics in geriatric medicine, 421-442.
Jungwirth S, & Fischer P. (2004). Subjective Memory Complaints and Objective memory
impairment in the Vienna-Transdanube aging. J Am Geriatr, 263-268.
KB Wolitzky-Taylor, & N Castriotta. (2010). Anxiety Disorders in older adults: a
comprehensive review. Depression and Anxiety, 190-211.
Klerman, G. (1977). Handbook of Study on Depression.
Kliegel, M., & Theodor. (2017). Can The Prospective retrospective Memory Questionnaire
Predict annual prospective memory performance. Saarland: Springer International
Publishing AG.
Lader, M. (1983). Individual Differences and Psychopathology. Elsevier Science Journals.
Lam LCW, & Tam CWC. (2005). Subjective memory complaints in Chinese subjects with
mild cognitive impairment and early Alzheimer'sdiseae. Int J Geriatr Psychiatry, 876-
882.
Lauren S Hallion, & Ruscio, A. M. (2011). A meta-analysis of the effect of cognitive bias
modification on anxiety and depression. Psychological bulletin, 940.
Longstreth, G. F. (1993). Bowel patterns and anxiety: Demographic Factors. Journal of
Clinical gastroentology, 128-132.
Rafael Marciniak, Katerina Sheardova, & Pavia Cermakova. (2014). Effect of meditation on
cognitive functions in contect of aging and neurodegenerative diseases. Frontiers in
behavioral neuroscience, 17.
Julie Hugo, & mary Ganguli. (2014). Dementia and cognitive impairment: epidemiology,
diagnosis, and treatment. Clinics in geriatric medicine, 421-442.
Jungwirth S, & Fischer P. (2004). Subjective Memory Complaints and Objective memory
impairment in the Vienna-Transdanube aging. J Am Geriatr, 263-268.
KB Wolitzky-Taylor, & N Castriotta. (2010). Anxiety Disorders in older adults: a
comprehensive review. Depression and Anxiety, 190-211.
Klerman, G. (1977). Handbook of Study on Depression.
Kliegel, M., & Theodor. (2017). Can The Prospective retrospective Memory Questionnaire
Predict annual prospective memory performance. Saarland: Springer International
Publishing AG.
Lader, M. (1983). Individual Differences and Psychopathology. Elsevier Science Journals.
Lam LCW, & Tam CWC. (2005). Subjective memory complaints in Chinese subjects with
mild cognitive impairment and early Alzheimer'sdiseae. Int J Geriatr Psychiatry, 876-
882.
Lauren S Hallion, & Ruscio, A. M. (2011). A meta-analysis of the effect of cognitive bias
modification on anxiety and depression. Psychological bulletin, 940.
Longstreth, G. F. (1993). Bowel patterns and anxiety: Demographic Factors. Journal of
Clinical gastroentology, 128-132.
Rafael Marciniak, Katerina Sheardova, & Pavia Cermakova. (2014). Effect of meditation on
cognitive functions in contect of aging and neurodegenerative diseases. Frontiers in
behavioral neuroscience, 17.
CHAPTER TWO 33
Reid, L. M., & MacLullich , A. J. (2006). Subjective Memory Complaints and Cognitive
Impairment in Older People. S. Karger AG.
Robinson M. D., M. B. (2007). Introversion, Inhibition and Displayed Anxiety. Journal of
Research in Personality, 558-578.
Roma A., R. A. (2013). Pediatric Anxiety Disorders: A Clinical Guide. Humana Press.
Sadock, B. J. (2009). Comprehensive Textbook Of Psychiatry. Philadelphia: Wolters Kluwer.
Shah A, Jhawar, S. S., & Goel A. (2011). Analysis of the anatomy of the Papez circuit and
adjoining limbic system by fibre dissection techniques. Journal of Neural Science,
289-298.
Sinn, N., Milte, C. M., Street, S. J., & Buckley, D. J. (2012). Effects of n-3 fatty acids, EPA v
DHA, on depressive symptoms,quality of life, memory and executive function in
older adults with mild cognitive impairment. British Journal of Nutrition, 1682-1693.
Smith, T., Gildeh, N., & Holmes, C. (2007). The Montreal Cognitive Assessment: Validity
and utility in a memory clinic setting. The Canadian Journal of Psychiatry, 329-332.
Stefan G Hoffman, Alice T Sawyer, & Ashley A Witt. (2010). The effect of mindfulness-
based therapy on anxiety and depression: A meta-analytic review. Journal of
consulting and clinical psychology, 169.
Williams JMG, W. F., & MacLeod. (1998). Cognitive Psychology and Emotional Disorders.
Chichester, England: Wiley.
Yaffe K, & T, B. (2005). The influence of depression on cognitive decline in community-
dwelling elderly persons. Am J Geriatr Psychiatry, 402-408.
Reid, L. M., & MacLullich , A. J. (2006). Subjective Memory Complaints and Cognitive
Impairment in Older People. S. Karger AG.
Robinson M. D., M. B. (2007). Introversion, Inhibition and Displayed Anxiety. Journal of
Research in Personality, 558-578.
Roma A., R. A. (2013). Pediatric Anxiety Disorders: A Clinical Guide. Humana Press.
Sadock, B. J. (2009). Comprehensive Textbook Of Psychiatry. Philadelphia: Wolters Kluwer.
Shah A, Jhawar, S. S., & Goel A. (2011). Analysis of the anatomy of the Papez circuit and
adjoining limbic system by fibre dissection techniques. Journal of Neural Science,
289-298.
Sinn, N., Milte, C. M., Street, S. J., & Buckley, D. J. (2012). Effects of n-3 fatty acids, EPA v
DHA, on depressive symptoms,quality of life, memory and executive function in
older adults with mild cognitive impairment. British Journal of Nutrition, 1682-1693.
Smith, T., Gildeh, N., & Holmes, C. (2007). The Montreal Cognitive Assessment: Validity
and utility in a memory clinic setting. The Canadian Journal of Psychiatry, 329-332.
Stefan G Hoffman, Alice T Sawyer, & Ashley A Witt. (2010). The effect of mindfulness-
based therapy on anxiety and depression: A meta-analytic review. Journal of
consulting and clinical psychology, 169.
Williams JMG, W. F., & MacLeod. (1998). Cognitive Psychology and Emotional Disorders.
Chichester, England: Wiley.
Yaffe K, & T, B. (2005). The influence of depression on cognitive decline in community-
dwelling elderly persons. Am J Geriatr Psychiatry, 402-408.

CHAPTER TWO 34
Yen Ying Lim, pau Maruff, David Ames, & Ralph N Martins. (2013). Effect of amyloid on
memory and non-memory decline from preclinical to clinical Alzheimer's disease.
Brain, 221-231.
Zelinski EM, & Cr., A.-B. (1990). Memory Functioning Questionnaire: Concurrent validity
with memory performance and self reported memory failures . Psychol Aging , 388-
399.
Yen Ying Lim, pau Maruff, David Ames, & Ralph N Martins. (2013). Effect of amyloid on
memory and non-memory decline from preclinical to clinical Alzheimer's disease.
Brain, 221-231.
Zelinski EM, & Cr., A.-B. (1990). Memory Functioning Questionnaire: Concurrent validity
with memory performance and self reported memory failures . Psychol Aging , 388-
399.
1 out of 34
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.