Obesity: Causes, Treatments and Impacts
VerifiedAdded on 2020/03/16
|13
|3144
|36
AI Summary
This assignment delves into the complex issue of obesity, examining its underlying causes, ranging from genetic predispositions to lifestyle factors like diet and physical activity. It highlights the detrimental effects of obesity on chronic diseases such as hypertension and diabetes. The assignment also explores various treatment strategies, including pharmacotherapy, behavioral interventions, and surgical options.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
AssignmentCover Sheet
The information on this coversheet will be included in Turnitin’s plagiarism analysis, however
your
lectures are aware of this and will disregard it
Student Details
Student Number
Family Name GivenName
UnitDetails
UnitCode UnitTitle
Nameof Lecturer DueDate
Topicof Assignment GrouporTutorial(if applicable)
Course Campus
Icertifythattheattachedassignment ismyownworkandthatanymaterialdrawnfromothersourceshasbeen
acknowledged.Thisworkhasnotpreviouslybeensubmittedforassessmentinanyotherunitorcourse.
Copyrightin assignmentsremainsmyproperty.IgrantpermissiontotheUniversitytomakecopiesof assignments
forassessment, reviewand/orrecordkeepingpurposes.InotethattheUniversityreservestherighttocheckmy
assignmentforplagiarism.Shouldthereproductionofallorpart of an assignmentberequiredbytheUniversityfor
ManualSubmission
Ifhandinginanassignmentinapaperorotherphysicalform,signheretoindicatethatyouhavereadthisform,filleditin
completelyandthat youcertifyasabove.
Signature Date OfficeUseOnly
ElectronicSubmission
OR,ifsubmittingthispaperelectronicallyasperinstructionsfortheunit,placean‘X’intheboxbelow
toindicatethat youhavereadthisformandfilleditincompletelyandthat youcertifyasabove.Please
includethispagewithyoursubmission.AnyresponsestothissubmissionwillbesenttoyourECU
emailaddress.
Agreement: Selectcheckbox: Date
Forproceduresandpenaltieson lateassignmentspleasereferto theUniversityAd m issi on,En ro lm entandAcademicPr og re ss
This information will be included in Turnitin’s plagiarism analysis, however your lecturers will disregard it.
The information on this coversheet will be included in Turnitin’s plagiarism analysis, however
your
lectures are aware of this and will disregard it
Student Details
Student Number
Family Name GivenName
UnitDetails
UnitCode UnitTitle
Nameof Lecturer DueDate
Topicof Assignment GrouporTutorial(if applicable)
Course Campus
Icertifythattheattachedassignment ismyownworkandthatanymaterialdrawnfromothersourceshasbeen
acknowledged.Thisworkhasnotpreviouslybeensubmittedforassessmentinanyotherunitorcourse.
Copyrightin assignmentsremainsmyproperty.IgrantpermissiontotheUniversitytomakecopiesof assignments
forassessment, reviewand/orrecordkeepingpurposes.InotethattheUniversityreservestherighttocheckmy
assignmentforplagiarism.Shouldthereproductionofallorpart of an assignmentberequiredbytheUniversityfor
ManualSubmission
Ifhandinginanassignmentinapaperorotherphysicalform,signheretoindicatethatyouhavereadthisform,filleditin
completelyandthat youcertifyasabove.
Signature Date OfficeUseOnly
ElectronicSubmission
OR,ifsubmittingthispaperelectronicallyasperinstructionsfortheunit,placean‘X’intheboxbelow
toindicatethat youhavereadthisformandfilleditincompletelyandthat youcertifyasabove.Please
includethispagewithyoursubmission.AnyresponsestothissubmissionwillbesenttoyourECU
emailaddress.
Agreement: Selectcheckbox: Date
Forproceduresandpenaltieson lateassignmentspleasereferto theUniversityAd m issi on,En ro lm entandAcademicPr og re ss
This information will be included in Turnitin’s plagiarism analysis, however your lecturers will disregard it.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Assignment Title: CLINICAL UPDATE: OBESITY
Unit Code and Title: NSP1104 Communication in Health Care
Lecturer/Tutor: Bob Jones
Student Name: Jane Smith
Student Number: 12345678
Date of Submission: 10 April 2016
Word Count:
Unit Code and Title: NSP1104 Communication in Health Care
Lecturer/Tutor: Bob Jones
Student Name: Jane Smith
Student Number: 12345678
Date of Submission: 10 April 2016
Word Count:
3
Table of Contents
Introduction..............................................................................................................5
Discussion................................................................................................................5
Aetiology and the pathophysiology.....................................................................5
Obesity associated risk factors.............................................................................7
Impact of Obesity on some chronic diseases.......................................................8
Clinical manifestations of obesity........................................................................9
Diagnostic process.............................................................................................10
Treatment...........................................................................................................11
Conclusion.............................................................................................................12
References..............................................................................................................13
Table of Contents
Introduction..............................................................................................................5
Discussion................................................................................................................5
Aetiology and the pathophysiology.....................................................................5
Obesity associated risk factors.............................................................................7
Impact of Obesity on some chronic diseases.......................................................8
Clinical manifestations of obesity........................................................................9
Diagnostic process.............................................................................................10
Treatment...........................................................................................................11
Conclusion.............................................................................................................12
References..............................................................................................................13
4
CLINICAL UPDATE: OBESITY
Introduction
Obesity is defined as the deposition of excess adipose tissue in the body.
Obesity is a serious chronic problem that is faced by half of the population of the world.
Obesity can have a negative impact on different systems of the body contributing to serious
illnesses like heart diseases, diabetes and bone and joint diseases. The excess adipose tissue
increases the level of the fatty acids and inflammation in the body, which can give rise to the
chronic conditions like diabetes.
Half of the Australian population had become the victim of obesity and it has become one of
the leading causes of mortality, disability, morbidity, health care costs to strain the health
care system of Australia and United States (Cushing, Beazley & Law, 2017).
This report aims to discuss about the aetiology and the pathophysiology, risk factors,
clinical manifestations, diagnostic procedures and probable treatments associated with
obesity. The report provides a vivid idea about the role of life style and genetics in the
pathogenesis of this disease.
Discussion
Aetiology and the pathophysiology
Obesity has become a major problem all over the world. It has been reported that
majority of the Australians are overweight and 20% suffer from obesity. Studies say that in
2014-2015, about 63.4 % of Australian adults are found to be overweight. 7% of the total
health trouble in Australia was because of overweight and obesity (Bagchi, & Preuss, (Eds.)
2012). 84% of the burden due to obesity and overweight was found between ages 45–84.. It
CLINICAL UPDATE: OBESITY
Introduction
Obesity is defined as the deposition of excess adipose tissue in the body.
Obesity is a serious chronic problem that is faced by half of the population of the world.
Obesity can have a negative impact on different systems of the body contributing to serious
illnesses like heart diseases, diabetes and bone and joint diseases. The excess adipose tissue
increases the level of the fatty acids and inflammation in the body, which can give rise to the
chronic conditions like diabetes.
Half of the Australian population had become the victim of obesity and it has become one of
the leading causes of mortality, disability, morbidity, health care costs to strain the health
care system of Australia and United States (Cushing, Beazley & Law, 2017).
This report aims to discuss about the aetiology and the pathophysiology, risk factors,
clinical manifestations, diagnostic procedures and probable treatments associated with
obesity. The report provides a vivid idea about the role of life style and genetics in the
pathogenesis of this disease.
Discussion
Aetiology and the pathophysiology
Obesity has become a major problem all over the world. It has been reported that
majority of the Australians are overweight and 20% suffer from obesity. Studies say that in
2014-2015, about 63.4 % of Australian adults are found to be overweight. 7% of the total
health trouble in Australia was because of overweight and obesity (Bagchi, & Preuss, (Eds.)
2012). 84% of the burden due to obesity and overweight was found between ages 45–84.. It
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
5
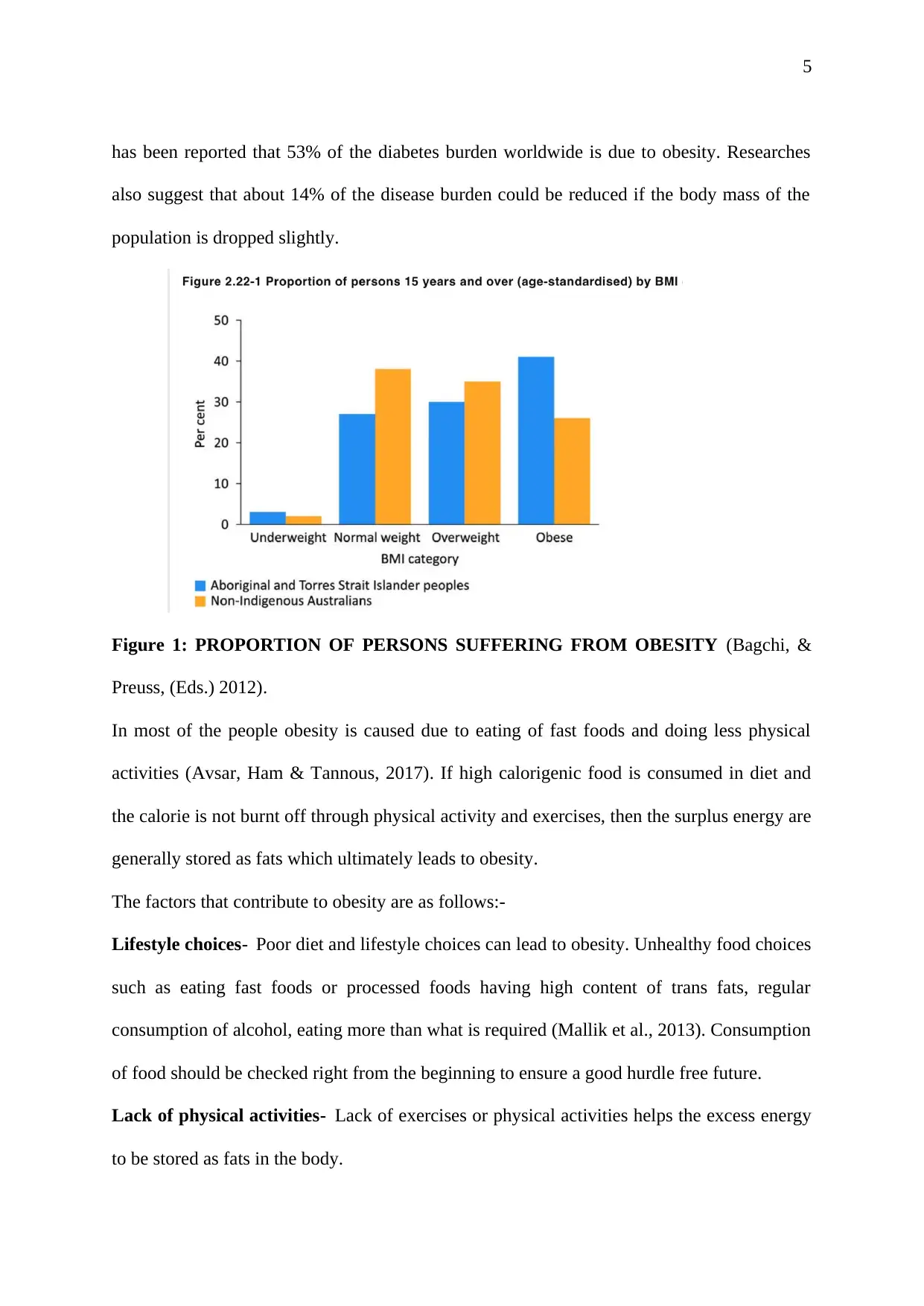
has been reported that 53% of the diabetes burden worldwide is due to obesity. Researches
also suggest that about 14% of the disease burden could be reduced if the body mass of the
population is dropped slightly.
Figure 1: PROPORTION OF PERSONS SUFFERING FROM OBESITY (Bagchi, &
Preuss, (Eds.) 2012).
In most of the people obesity is caused due to eating of fast foods and doing less physical
activities (Avsar, Ham & Tannous, 2017). If high calorigenic food is consumed in diet and
the calorie is not burnt off through physical activity and exercises, then the surplus energy are
generally stored as fats which ultimately leads to obesity.
The factors that contribute to obesity are as follows:-
Lifestyle choices- Poor diet and lifestyle choices can lead to obesity. Unhealthy food choices
such as eating fast foods or processed foods having high content of trans fats, regular
consumption of alcohol, eating more than what is required (Mallik et al., 2013). Consumption
of food should be checked right from the beginning to ensure a good hurdle free future.
Lack of physical activities- Lack of exercises or physical activities helps the excess energy
to be stored as fats in the body.
has been reported that 53% of the diabetes burden worldwide is due to obesity. Researches
also suggest that about 14% of the disease burden could be reduced if the body mass of the
population is dropped slightly.
Figure 1: PROPORTION OF PERSONS SUFFERING FROM OBESITY (Bagchi, &
Preuss, (Eds.) 2012).
In most of the people obesity is caused due to eating of fast foods and doing less physical
activities (Avsar, Ham & Tannous, 2017). If high calorigenic food is consumed in diet and
the calorie is not burnt off through physical activity and exercises, then the surplus energy are
generally stored as fats which ultimately leads to obesity.
The factors that contribute to obesity are as follows:-
Lifestyle choices- Poor diet and lifestyle choices can lead to obesity. Unhealthy food choices
such as eating fast foods or processed foods having high content of trans fats, regular
consumption of alcohol, eating more than what is required (Mallik et al., 2013). Consumption
of food should be checked right from the beginning to ensure a good hurdle free future.
Lack of physical activities- Lack of exercises or physical activities helps the excess energy
to be stored as fats in the body.
6
Genetics- genes can be responsible for being overweight and obesity. It has been
reported that the risk of Obesity is eight times higher in a person with an obese family history
as compared to a person having no family history of obesity (Bolton et al., 2017). Inheriting
of obesity may depend on the phenotype, it appears to be higher for the phenotypes linked to
weight or body fat excess (5-40%) and adipose tissue distribution (40-55%) and as the
Adiposity and weight gain increases with age and is influenced by heredity.
Evidences show that obesity of monogenic types may be caused by gene mutations; however,
yet now, only 78 cases worldwide supports the fact that obesity relates to genetic mutations in
seven distinct genes (Bolton et al., 2017). Sequence variations in a pool of 56 different genes
have been reported to be associated with obesity phenotypes, although only ten of those
genes gave positive results in five studies.
Obesity associated risk factors
Some of the obesity associated risk factors are: low LDL cholesterol, high HDL
cholesterol, high glucose and high blood pressure (Hardy, Czech & Corvera, 2012). Obese
people are also susceptible to high risks of cardiovascular diseases (Hall et al., 2014). Obesity
is one of the contributing factors of the type 2 diabetes, osteoarthritis, and some cancers
(colon, breast, endometrial, kidney gall bladder and liver).
Other variable risk factors that are associated with obesity are stroke, sleep apnea, mental
illness due to inferiority complex (Hall et al., 2014).
Problems related to obesity and overweight has risen drastically within a decade. Some
chronic clinical conditions that are influences by the body mass index are cancers, diabetes,
chronic kidney diseases, gall bladder diseases, asthma and dementia (Hardy, O. T., Czech &
Corvera, 2012). It has also been reported that obese females have larger risks of developing
PCOS (Polycystic ovary syndrome) (Hall et al., 2014).
Genetics- genes can be responsible for being overweight and obesity. It has been
reported that the risk of Obesity is eight times higher in a person with an obese family history
as compared to a person having no family history of obesity (Bolton et al., 2017). Inheriting
of obesity may depend on the phenotype, it appears to be higher for the phenotypes linked to
weight or body fat excess (5-40%) and adipose tissue distribution (40-55%) and as the
Adiposity and weight gain increases with age and is influenced by heredity.
Evidences show that obesity of monogenic types may be caused by gene mutations; however,
yet now, only 78 cases worldwide supports the fact that obesity relates to genetic mutations in
seven distinct genes (Bolton et al., 2017). Sequence variations in a pool of 56 different genes
have been reported to be associated with obesity phenotypes, although only ten of those
genes gave positive results in five studies.
Obesity associated risk factors
Some of the obesity associated risk factors are: low LDL cholesterol, high HDL
cholesterol, high glucose and high blood pressure (Hardy, Czech & Corvera, 2012). Obese
people are also susceptible to high risks of cardiovascular diseases (Hall et al., 2014). Obesity
is one of the contributing factors of the type 2 diabetes, osteoarthritis, and some cancers
(colon, breast, endometrial, kidney gall bladder and liver).
Other variable risk factors that are associated with obesity are stroke, sleep apnea, mental
illness due to inferiority complex (Hall et al., 2014).
Problems related to obesity and overweight has risen drastically within a decade. Some
chronic clinical conditions that are influences by the body mass index are cancers, diabetes,
chronic kidney diseases, gall bladder diseases, asthma and dementia (Hardy, O. T., Czech &
Corvera, 2012). It has also been reported that obese females have larger risks of developing
PCOS (Polycystic ovary syndrome) (Hall et al., 2014).
7
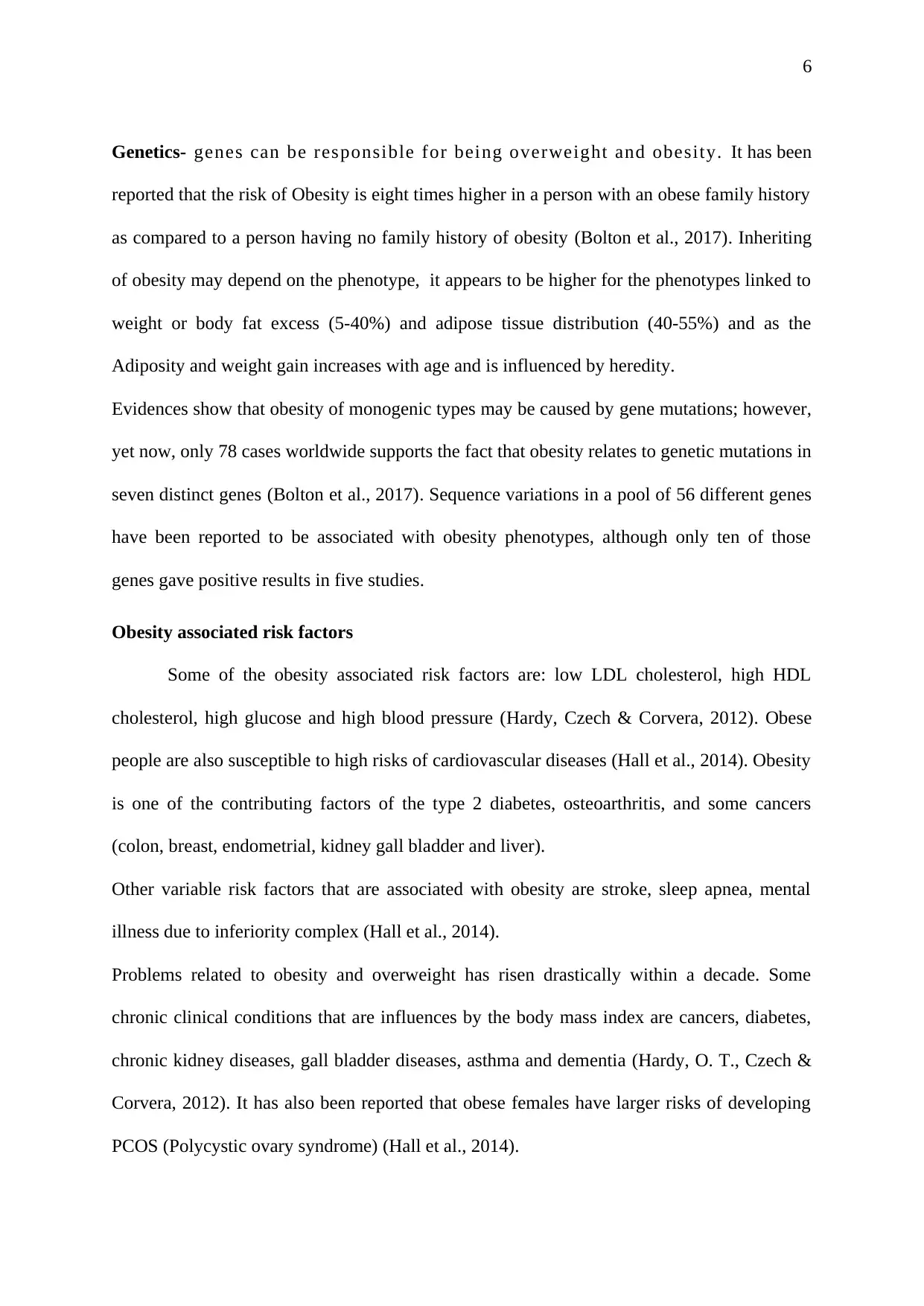
Figure 1: RISK FACTORS ASSOCIATED WITH OBESITY (Malik, Willett & Hu, 2013).
Impact of Obesity on some chronic diseases
Obesity plays a crucial role in the pathophysiology of diabetes mellitus, dyslipidemia,
hypertension, insulin resistance, artherosclerosis. Obesity is caused due to the
hypersecreation of the adipokines (Hall et al., 2014). Obesity influence the dysfunction
related to cardiac, liver, pulmonary, intestinal, endocrine and the exocrine functions. Insulin-
resistant, Inflammatory, hypertensive, and thrombotic-promoting atherogenic adipokines are
counterbalanced by anti-atherogenic and anti-inflammatory adipocyte hormones such as
adiponectin, visfatin, and acylation-stimulating protein (Illan Gomez et al., 2014).
Adiponectin is protective against liver fibrosis owing to its anti-inflammatory upshot,
whereas inflammatory cytokines like as tumor necrosis factor-α are harmful for both fatty
liver and the release of pancreatic insulin (Illan Gomez et al., 2014). Obesity enhances
immune dysfunction due to the inflammatory adipokine secretion and thus is a responsible
factor for many cancers like oesophageal, hepatocellular, and colon.
Figure 1: RISK FACTORS ASSOCIATED WITH OBESITY (Malik, Willett & Hu, 2013).
Impact of Obesity on some chronic diseases
Obesity plays a crucial role in the pathophysiology of diabetes mellitus, dyslipidemia,
hypertension, insulin resistance, artherosclerosis. Obesity is caused due to the
hypersecreation of the adipokines (Hall et al., 2014). Obesity influence the dysfunction
related to cardiac, liver, pulmonary, intestinal, endocrine and the exocrine functions. Insulin-
resistant, Inflammatory, hypertensive, and thrombotic-promoting atherogenic adipokines are
counterbalanced by anti-atherogenic and anti-inflammatory adipocyte hormones such as
adiponectin, visfatin, and acylation-stimulating protein (Illan Gomez et al., 2014).
Adiponectin is protective against liver fibrosis owing to its anti-inflammatory upshot,
whereas inflammatory cytokines like as tumor necrosis factor-α are harmful for both fatty
liver and the release of pancreatic insulin (Illan Gomez et al., 2014). Obesity enhances
immune dysfunction due to the inflammatory adipokine secretion and thus is a responsible
factor for many cancers like oesophageal, hepatocellular, and colon.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
Clinical manifestations of obesity
Obesity is one of the major health concerns of Australia and affects all age groups
equally. The rates have increased dramatically over the past decade and Australia presently is
being rated as one of the fattest developed nations. Therefore, attributed to the large and wide
clinical manifestations of obesity intervention protocols need to be designed. As per the
recorded data, between 2004-2005 almost 41% males and 25 % females were considered as
obese and the numbers have been increasing ever since. However, as commented by Avsar et
al. (2017), there are a large number of clinical manifestations of obesity which can affect the
long term health of the individual. Though, the causes of obesity vary, however very often a
genetic pre-disposition have been found. Additionally, some tendencies have been noted
particularly in the youth today that is largely and by far depending upon fast foods to get their
nutrition.
Some of the clinical manifestations of obesity are expressed in day to day health
problems such as increased sweating, breathlessness, fatigue, joint pains. Additionally,
excess weight could also be related with the presence of other symptoms such as diabetes and
hormonal disorders. As commented by Comans et al.(2013), obesity also increases the risk
of some of the life threatening conditions many fold times such as cardiac arrhythmia,
ischemic heart and conditions such as polycystic ovarian syndrome. As per reports and
evidences almost 42 % of the diabetes cases had been linked to obesity. Moreover, the obese
could be divided into three distinct classes such as obese 1, obese 2 and obese 3. The
differentiation of the classes has been done for analysing the risk of co-morbid conditions
such as coronary heart disease and fatal conditions as stroke. The BMI index have been
divided in between from 30-40, where a BMI index 35 -40 indicates severe obesity.
Clinical manifestations of obesity
Obesity is one of the major health concerns of Australia and affects all age groups
equally. The rates have increased dramatically over the past decade and Australia presently is
being rated as one of the fattest developed nations. Therefore, attributed to the large and wide
clinical manifestations of obesity intervention protocols need to be designed. As per the
recorded data, between 2004-2005 almost 41% males and 25 % females were considered as
obese and the numbers have been increasing ever since. However, as commented by Avsar et
al. (2017), there are a large number of clinical manifestations of obesity which can affect the
long term health of the individual. Though, the causes of obesity vary, however very often a
genetic pre-disposition have been found. Additionally, some tendencies have been noted
particularly in the youth today that is largely and by far depending upon fast foods to get their
nutrition.
Some of the clinical manifestations of obesity are expressed in day to day health
problems such as increased sweating, breathlessness, fatigue, joint pains. Additionally,
excess weight could also be related with the presence of other symptoms such as diabetes and
hormonal disorders. As commented by Comans et al.(2013), obesity also increases the risk
of some of the life threatening conditions many fold times such as cardiac arrhythmia,
ischemic heart and conditions such as polycystic ovarian syndrome. As per reports and
evidences almost 42 % of the diabetes cases had been linked to obesity. Moreover, the obese
could be divided into three distinct classes such as obese 1, obese 2 and obese 3. The
differentiation of the classes has been done for analysing the risk of co-morbid conditions
such as coronary heart disease and fatal conditions as stroke. The BMI index have been
divided in between from 30-40, where a BMI index 35 -40 indicates severe obesity.
9
Diagnostic process
The diagnosis of obesity consists of a number of methods which could be employed
for the detection of moderate to severe obesity within an individual. Some of the measures
taken by the doctors include recording the patient history for the presence of other co-morbid
conditions. As commented by Cushing et al. (2017), the presence of family history of obesity
could be related to overweight conditions in an individual. Apart from that the doctor may
also make a record of the dietary or the lifestyle patterns of the patient. Additionally,
conducting a normal physical check up such as heart rate, blood pressure, rate of breathing
can help the physician in understanding the general health condition of the patient. As
asserted by Bolton et al.(2017), checking the BMI on an annual basis can also help in
comprehending the risk factors associated with the health of the patient. Moreover,
conducting some of the test such as cholesterol, liver function, fasting glucose and thyroid
can provide the general physician with a concise picture regarding the patient health.
Treatment
The objective of obesity treatment is to maintain a healthy weight. This can be
accomplished by combining both pharmacological and non pharmacological ways-
Dietary changes- Calorie reduction and opting healthier eating habits are crucial for
overcoming obesity. Processed and fast foods containing high levels of trans fats should be
avoided. High carbohydrate or sugar containing food should be avoided (Zhang et al., 2014).
Foods having low energy density such as fresh fruits, vegetables and whole –grain
carbohydrates should be consumed. Low fat dairy products can be consumed (Bagchi &
Preuss, (Eds.) 2012).
Exercise and activity- Moderate to intense exercises helps in burning out the extra calories
(Zhang et al., 2014).
Diagnostic process
The diagnosis of obesity consists of a number of methods which could be employed
for the detection of moderate to severe obesity within an individual. Some of the measures
taken by the doctors include recording the patient history for the presence of other co-morbid
conditions. As commented by Cushing et al. (2017), the presence of family history of obesity
could be related to overweight conditions in an individual. Apart from that the doctor may
also make a record of the dietary or the lifestyle patterns of the patient. Additionally,
conducting a normal physical check up such as heart rate, blood pressure, rate of breathing
can help the physician in understanding the general health condition of the patient. As
asserted by Bolton et al.(2017), checking the BMI on an annual basis can also help in
comprehending the risk factors associated with the health of the patient. Moreover,
conducting some of the test such as cholesterol, liver function, fasting glucose and thyroid
can provide the general physician with a concise picture regarding the patient health.
Treatment
The objective of obesity treatment is to maintain a healthy weight. This can be
accomplished by combining both pharmacological and non pharmacological ways-
Dietary changes- Calorie reduction and opting healthier eating habits are crucial for
overcoming obesity. Processed and fast foods containing high levels of trans fats should be
avoided. High carbohydrate or sugar containing food should be avoided (Zhang et al., 2014).
Foods having low energy density such as fresh fruits, vegetables and whole –grain
carbohydrates should be consumed. Low fat dairy products can be consumed (Bagchi &
Preuss, (Eds.) 2012).
Exercise and activity- Moderate to intense exercises helps in burning out the extra calories
(Zhang et al., 2014).
10
Behavior changes- Cessation of drugs and alcohol consumption, coping up with stresses
without the help of any addictives (Zhang et al., 2014). Several weight loss programs and
support groups are there for achieving the weight loss goals.
Weight-loss medication- some of the commonly administered weight loss medications are
lorcaserin (Belviq), orlistat (Xenical), topiramate (Qsymia), phentermine, naltrexone
(Contrave) and buproprion , and liraglutide (Saxenda) (Carter et al., 2012, Kushner, 2014).
Weight-loss surgery- Sometimes Weight-loss surgery or bariatric surgery is done. Weigt los
surgery can be done if one is having extreme obesity (40BMI or higher) (Buchwald & Oien,
2013). Some of the weight loss surgeries are Gastric bypass surgery, Laproscopic adjustable
gastric banding, Biliopancreatic diversion with a duodenal switch and gastric sleeve.
Other treatments- Blockage of the vagal nerve can be another treatment of obesity. It
involves implantation of a device under the skin of the abdomen that sends intermittent
electrical pulses to the vagus nerve of the abdomen, which tells the brain whether the
stomach is empty or full (Bagchi & Preuss, (Eds.) 2012).
Prevention of weight regain after obesity treatment- Healthy diet and regular physical
activity and keeping a track of the physical activity can prevent regaining of weight.
Conclusion
A clinical update has been established that 63.4 % of Australian adults are found to be
overweight. The predominating factor behind the obesity is the life style of the people and
their eating habits. Some obese people also show family history of obesity, although the main
contributing factor will always remain food habits and lack of movement. The risk factors
associated with obesity are some forms of cancers, type 2 diabetes, PCOS in females, chroniv
Behavior changes- Cessation of drugs and alcohol consumption, coping up with stresses
without the help of any addictives (Zhang et al., 2014). Several weight loss programs and
support groups are there for achieving the weight loss goals.
Weight-loss medication- some of the commonly administered weight loss medications are
lorcaserin (Belviq), orlistat (Xenical), topiramate (Qsymia), phentermine, naltrexone
(Contrave) and buproprion , and liraglutide (Saxenda) (Carter et al., 2012, Kushner, 2014).
Weight-loss surgery- Sometimes Weight-loss surgery or bariatric surgery is done. Weigt los
surgery can be done if one is having extreme obesity (40BMI or higher) (Buchwald & Oien,
2013). Some of the weight loss surgeries are Gastric bypass surgery, Laproscopic adjustable
gastric banding, Biliopancreatic diversion with a duodenal switch and gastric sleeve.
Other treatments- Blockage of the vagal nerve can be another treatment of obesity. It
involves implantation of a device under the skin of the abdomen that sends intermittent
electrical pulses to the vagus nerve of the abdomen, which tells the brain whether the
stomach is empty or full (Bagchi & Preuss, (Eds.) 2012).
Prevention of weight regain after obesity treatment- Healthy diet and regular physical
activity and keeping a track of the physical activity can prevent regaining of weight.
Conclusion
A clinical update has been established that 63.4 % of Australian adults are found to be
overweight. The predominating factor behind the obesity is the life style of the people and
their eating habits. Some obese people also show family history of obesity, although the main
contributing factor will always remain food habits and lack of movement. The risk factors
associated with obesity are some forms of cancers, type 2 diabetes, PCOS in females, chroniv
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
11
kidney disease and cardiovascular diseases. Since obesity is a life style disease, Treatments
regarding the management of obesity mainly focuses on the change in the dietary supplement
of the person. Several medications and surgeries are also available for reducing the body
mass index in people suffering from extreme obesity. Regular exercises and physical
activities have been found to be the key component for the management of obesity. It is
believed that 14% of the disease burden of the world could be reduced if the body mass of the
population is dropped slightly.
kidney disease and cardiovascular diseases. Since obesity is a life style disease, Treatments
regarding the management of obesity mainly focuses on the change in the dietary supplement
of the person. Several medications and surgeries are also available for reducing the body
mass index in people suffering from extreme obesity. Regular exercises and physical
activities have been found to be the key component for the management of obesity. It is
believed that 14% of the disease burden of the world could be reduced if the body mass of the
population is dropped slightly.
12
References
Avsar, G., Ham, R., & Tannous, W. K. (2017). Factors influencing the incidence of obesity in
Australia: a generalized ordered probit model. International journal of environmental
research and public health, 14(2), 177.
Bagchi, D., & Preuss, H. G. (Eds.). (2012). Obesity: epidemiology, pathophysiology, and
prevention. CRC press.
Bolton, K. A., Kremer, P., Gibbs, L., Waters, E., Swinburn, B., & de Silva, A. (2017). The
outcomes of health-promoting communities: being active eating well initiative—a
community-based obesity prevention intervention in Victoria, Australia. International
Journal of Obesity.
Buchwald, H., & Oien, D. M. (2013). Metabolic/bariatric surgery worldwide 2011. Obesity
surgery, 23(4), 427-436.
Carter, R., Mouralidarane, A., Ray, S., Soeda, J., & Oben, J. (2012). Recent advancements in
drug treatment of obesity. Clinical Medicine, 12(5), 456-460.
Comans, T. A., Whitty, J. A., Hills, A. P., Kendall, E., Turkstra, E., Gordon, L. G., ... &
Scuffham, P. A. (2013). The cost-effectiveness and consumer acceptability of taxation
strategies to reduce rates of overweight and obesity among children in Australia:
study protocol. BMC public health, 13(1), 1182.
Cushing, D. F., Beazley, H., & Law, L. (2017). 11 Urban green spaces and childhood obesity
in (sub) tropical Queensland, Australia. Children’s Health and Wellbeing in Urban
Environments.
Hall, M. E., do Carmo, J. M., da Silva, A. A., Juncos, L. A., Wang, Z., & Hall, J. E. (2014).
Obesity, hypertension, and chronic kidney disease. International journal of
nephrology and renovascular disease, 7, 75.
References
Avsar, G., Ham, R., & Tannous, W. K. (2017). Factors influencing the incidence of obesity in
Australia: a generalized ordered probit model. International journal of environmental
research and public health, 14(2), 177.
Bagchi, D., & Preuss, H. G. (Eds.). (2012). Obesity: epidemiology, pathophysiology, and
prevention. CRC press.
Bolton, K. A., Kremer, P., Gibbs, L., Waters, E., Swinburn, B., & de Silva, A. (2017). The
outcomes of health-promoting communities: being active eating well initiative—a
community-based obesity prevention intervention in Victoria, Australia. International
Journal of Obesity.
Buchwald, H., & Oien, D. M. (2013). Metabolic/bariatric surgery worldwide 2011. Obesity
surgery, 23(4), 427-436.
Carter, R., Mouralidarane, A., Ray, S., Soeda, J., & Oben, J. (2012). Recent advancements in
drug treatment of obesity. Clinical Medicine, 12(5), 456-460.
Comans, T. A., Whitty, J. A., Hills, A. P., Kendall, E., Turkstra, E., Gordon, L. G., ... &
Scuffham, P. A. (2013). The cost-effectiveness and consumer acceptability of taxation
strategies to reduce rates of overweight and obesity among children in Australia:
study protocol. BMC public health, 13(1), 1182.
Cushing, D. F., Beazley, H., & Law, L. (2017). 11 Urban green spaces and childhood obesity
in (sub) tropical Queensland, Australia. Children’s Health and Wellbeing in Urban
Environments.
Hall, M. E., do Carmo, J. M., da Silva, A. A., Juncos, L. A., Wang, Z., & Hall, J. E. (2014).
Obesity, hypertension, and chronic kidney disease. International journal of
nephrology and renovascular disease, 7, 75.
13
Hardy, O. T., Czech, M. P., & Corvera, S. (2012). What causes the insulin resistance
underlying obesity?. Current opinion in endocrinology, diabetes, and obesity, 19(2),
81.
Illán-Gómez, F., Gonzálvez-Ortega, M., Orea-Soler, I., Alcaraz-Tafalla, M. S., Aragón-
Alonso, A., Pascual-Díaz, M., ... & Lozano-Almela, M. L. (2012). Obesity and
inflammation: change in adiponectin, C-reactive protein, tumour necrosis factor-alpha
and interleukin-6 after bariatric surgery. Obesity surgery, 22(6), 950-955.
Kushner, R. F. (2014). Weight loss strategies for treatment of obesity. Progress in
Cardiovascular Diseases, 56(4), 465-472.
Malik, V. S., Willett, W. C., & Hu, F. B. (2013). Global obesity: trends, risk factors and
policy implications. Nature Reviews Endocrinology, 9(1), 13-27.
Pasco, J. A., Nicholson, G. C., Brennan, S. L., & Kotowicz, M. A. (2012). Prevalence of
obesity and the relationship between the body mass index and body fat: cross-
sectional, population-based data. PloS one, 7(1), e29580.
Walls, H. L., Magliano, D. J., Stevenson, C. E., Backholer, K., Mannan, H. R., Shaw, J. E., &
Peeters, A. (2012). Projected progression of the prevalence of obesity in
Australia. Obesity, 20(4), 872-878.
Wright, S. M., & Aronne, L. J. (2012). Causes of obesity. Abdominal Radiology, 37(5), 730-
732.
Zhang, Y., Liu, J., Yao, J., Ji, G., Qian, L., Wang, J., ... & Gold, M. S. (2014). Obesity:
pathophysiology and intervention. Nutrients, 6(11), 5153-5183.
Hardy, O. T., Czech, M. P., & Corvera, S. (2012). What causes the insulin resistance
underlying obesity?. Current opinion in endocrinology, diabetes, and obesity, 19(2),
81.
Illán-Gómez, F., Gonzálvez-Ortega, M., Orea-Soler, I., Alcaraz-Tafalla, M. S., Aragón-
Alonso, A., Pascual-Díaz, M., ... & Lozano-Almela, M. L. (2012). Obesity and
inflammation: change in adiponectin, C-reactive protein, tumour necrosis factor-alpha
and interleukin-6 after bariatric surgery. Obesity surgery, 22(6), 950-955.
Kushner, R. F. (2014). Weight loss strategies for treatment of obesity. Progress in
Cardiovascular Diseases, 56(4), 465-472.
Malik, V. S., Willett, W. C., & Hu, F. B. (2013). Global obesity: trends, risk factors and
policy implications. Nature Reviews Endocrinology, 9(1), 13-27.
Pasco, J. A., Nicholson, G. C., Brennan, S. L., & Kotowicz, M. A. (2012). Prevalence of
obesity and the relationship between the body mass index and body fat: cross-
sectional, population-based data. PloS one, 7(1), e29580.
Walls, H. L., Magliano, D. J., Stevenson, C. E., Backholer, K., Mannan, H. R., Shaw, J. E., &
Peeters, A. (2012). Projected progression of the prevalence of obesity in
Australia. Obesity, 20(4), 872-878.
Wright, S. M., & Aronne, L. J. (2012). Causes of obesity. Abdominal Radiology, 37(5), 730-
732.
Zhang, Y., Liu, J., Yao, J., Ji, G., Qian, L., Wang, J., ... & Gold, M. S. (2014). Obesity:
pathophysiology and intervention. Nutrients, 6(11), 5153-5183.
1 out of 13
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.