Pre & Post Postoperative Management for Stage 1 Colon Cancer
VerifiedAdded on 2022/10/12
|8
|2169
|69
AI Summary
This essay discusses the pre and post postoperative managements required for a patient undergoing resection and anastomosis for stage 1 colon cancer. It includes specific preparations needed for postop management, complications associated with surgery, and supported by extensive evidence from peer-reviewed journals.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Running Head: NURSING 0
PRE & POST POSTOPERATIVE MANAGEMENT.
Stage 1 Colon Cancer
[DATE]
[Company name]
[Company address]
PRE & POST POSTOPERATIVE MANAGEMENT.
Stage 1 Colon Cancer
[DATE]
[Company name]
[Company address]
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
NURSING 1
Introduction
In this essay the pre operational and post postoperative managements which are required
for a patient who is undergoing resection and anastomosis for stage 1 colon cancer. It will further
include the specific preparations needed for the postop management like care in the first 24 hours
of the post-operative period and other complications which may be associated with the surgery.
All the discussion to be done in this assignment will be supported by the extensive evidences
from the journals reviewed by the peer groups and the other relevant resources.
Pre and post operational strategies
Colon cancer is that disease in which malignant cells or the cancer cells are basically
found in the tissues of the colon and it’s the history of the health which basically responsible for
the development of this type of cancer. Its symptoms can be recovery of blood in stool or change
in a bowel habits. Risk factor of this disease include having the history of colon cancer or the
rectal cancer of its own as person or from the family, having been inherited with some germs
which can increase the risk of FAP i.e. familiar adenomatous polyposis., consuming three or
more alcoholic drinks every day, smoking cigarettes, being obese and black. In this cancer there
are four stages, which starts from 0 and extends till IV (Chun, 2019).
For staging process the following procedures may be used like CT scan, MRI, PET scan
i.e. positron emission tomography scan, x-ray of the chest, surgery, lymph node biopsy, complete
blood count i.e. CBC and CEA i.e. carcioembryonic antigen assay. Cancer gets blowout in the
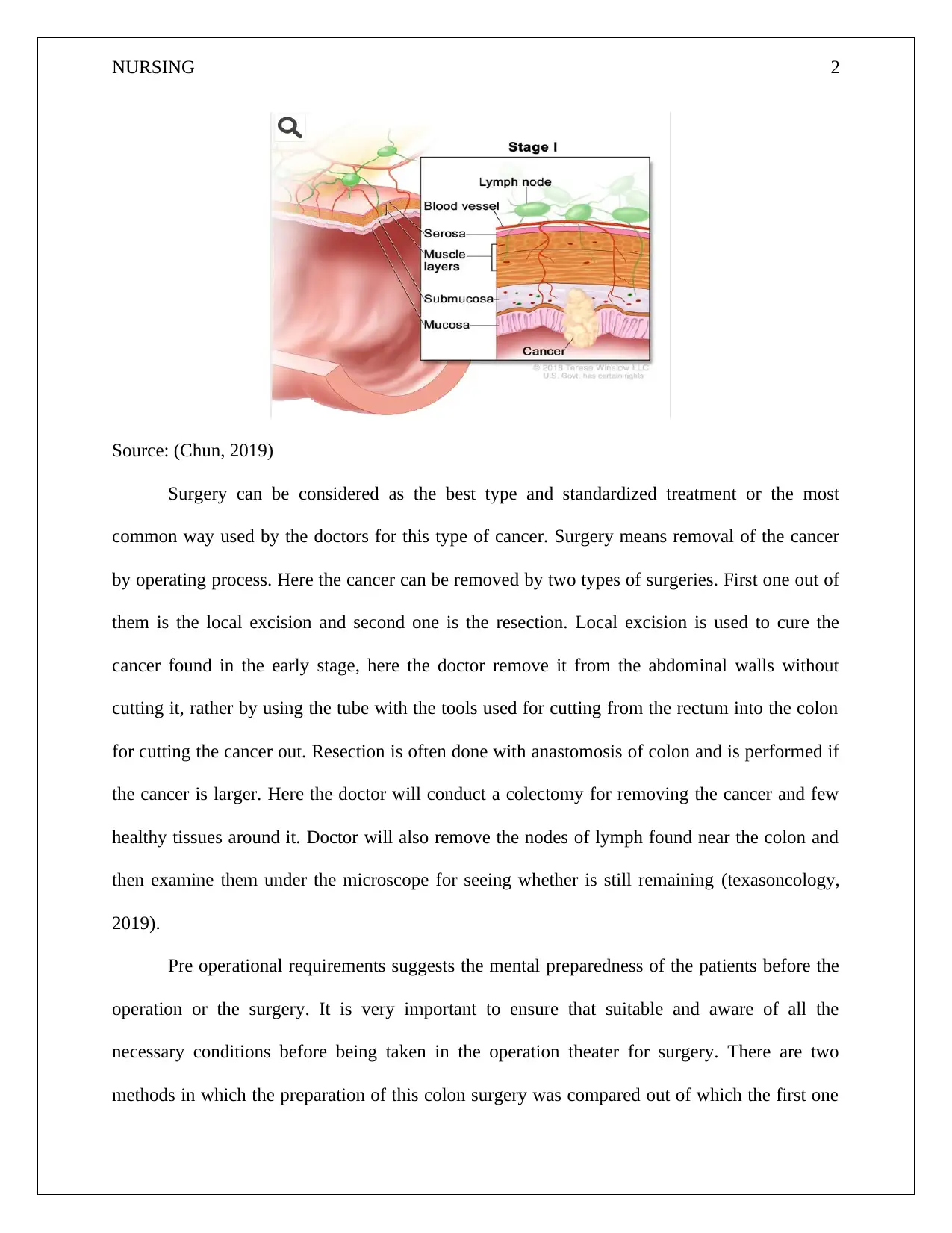
entire body through tissue, blood system and the lymph. In stage 1 of the colon cancer, the
cancer is formed in the innermost layer i.e. mucosa on the walls of the colon and with the help of
the tissue get spread in the sub mucosa or the muscle layer of the colon wall (clinic, 2019).
Introduction
In this essay the pre operational and post postoperative managements which are required
for a patient who is undergoing resection and anastomosis for stage 1 colon cancer. It will further
include the specific preparations needed for the postop management like care in the first 24 hours
of the post-operative period and other complications which may be associated with the surgery.
All the discussion to be done in this assignment will be supported by the extensive evidences
from the journals reviewed by the peer groups and the other relevant resources.
Pre and post operational strategies
Colon cancer is that disease in which malignant cells or the cancer cells are basically
found in the tissues of the colon and it’s the history of the health which basically responsible for
the development of this type of cancer. Its symptoms can be recovery of blood in stool or change
in a bowel habits. Risk factor of this disease include having the history of colon cancer or the
rectal cancer of its own as person or from the family, having been inherited with some germs
which can increase the risk of FAP i.e. familiar adenomatous polyposis., consuming three or
more alcoholic drinks every day, smoking cigarettes, being obese and black. In this cancer there
are four stages, which starts from 0 and extends till IV (Chun, 2019).
For staging process the following procedures may be used like CT scan, MRI, PET scan
i.e. positron emission tomography scan, x-ray of the chest, surgery, lymph node biopsy, complete
blood count i.e. CBC and CEA i.e. carcioembryonic antigen assay. Cancer gets blowout in the
entire body through tissue, blood system and the lymph. In stage 1 of the colon cancer, the
cancer is formed in the innermost layer i.e. mucosa on the walls of the colon and with the help of
the tissue get spread in the sub mucosa or the muscle layer of the colon wall (clinic, 2019).
NURSING 2
Source: (Chun, 2019)
Surgery can be considered as the best type and standardized treatment or the most
common way used by the doctors for this type of cancer. Surgery means removal of the cancer
by operating process. Here the cancer can be removed by two types of surgeries. First one out of
them is the local excision and second one is the resection. Local excision is used to cure the
cancer found in the early stage, here the doctor remove it from the abdominal walls without
cutting it, rather by using the tube with the tools used for cutting from the rectum into the colon
for cutting the cancer out. Resection is often done with anastomosis of colon and is performed if
the cancer is larger. Here the doctor will conduct a colectomy for removing the cancer and few
healthy tissues around it. Doctor will also remove the nodes of lymph found near the colon and
then examine them under the microscope for seeing whether is still remaining (texasoncology,
2019).
Pre operational requirements suggests the mental preparedness of the patients before the
operation or the surgery. It is very important to ensure that suitable and aware of all the
necessary conditions before being taken in the operation theater for surgery. There are two
methods in which the preparation of this colon surgery was compared out of which the first one
Source: (Chun, 2019)
Surgery can be considered as the best type and standardized treatment or the most
common way used by the doctors for this type of cancer. Surgery means removal of the cancer
by operating process. Here the cancer can be removed by two types of surgeries. First one out of
them is the local excision and second one is the resection. Local excision is used to cure the
cancer found in the early stage, here the doctor remove it from the abdominal walls without
cutting it, rather by using the tube with the tools used for cutting from the rectum into the colon
for cutting the cancer out. Resection is often done with anastomosis of colon and is performed if
the cancer is larger. Here the doctor will conduct a colectomy for removing the cancer and few
healthy tissues around it. Doctor will also remove the nodes of lymph found near the colon and
then examine them under the microscope for seeing whether is still remaining (texasoncology,
2019).
Pre operational requirements suggests the mental preparedness of the patients before the
operation or the surgery. It is very important to ensure that suitable and aware of all the
necessary conditions before being taken in the operation theater for surgery. There are two
methods in which the preparation of this colon surgery was compared out of which the first one
NURSING 3
is the one which is normally used i.e. free residue meals of the hospital for five consecutive days,
purgatives for cleansing, laxatives and three liters of polyethylene glycol solution (Bakker,
Cakir, Doodeman, & Houdijk, 2015). But the second or the new method is very simple and easy
one to be implemented. It can be done by the patients at home also which combines intake of
enhanced nutrition along with it excellent level of intra-colon cleansing. It also involves 4 days
exclusive administration of low fiber diet in a variety of flavors and application of two cleansing
purgatives in evening prior to the operation (Du, 2017).
In general the preoperative assessment includes the knowledge of complete medical
history and physical examination. The performance of investigating all the Hematological and
clinical chemistry must be completely done before the conduction of the surgery as well as all
the other appropriate anesthetic investigation must be complete and informed to the patient in an
adequate manner and required amount (Van , et al., 2016). The surgery must be avoided in case
if there are any potential risk appears to overshadow the benefits of procedures of the surgery.
This applies to those patients who are not fit medically for the surgery or the ones who are
having any other advanced disease.
Steps for preoperative management are first the informed consent i.e. all the basic details
must be explained to the patient like the possible outcomes, desired results and other alternatives
etc. Second one is preparation of stoma. It is required for all the patients undergoing the surgery
for colon cancer where all the patients may be completely warned about the possibility of the
surgeon and the basic difference between the temporary and permanent stoma must be explained
in details. The nurses may visit in case of if their role is identified in the stoma therapy, who can
help in developing the physical, social, cultural and psychological factors. They also take
is the one which is normally used i.e. free residue meals of the hospital for five consecutive days,
purgatives for cleansing, laxatives and three liters of polyethylene glycol solution (Bakker,
Cakir, Doodeman, & Houdijk, 2015). But the second or the new method is very simple and easy
one to be implemented. It can be done by the patients at home also which combines intake of
enhanced nutrition along with it excellent level of intra-colon cleansing. It also involves 4 days
exclusive administration of low fiber diet in a variety of flavors and application of two cleansing
purgatives in evening prior to the operation (Du, 2017).
In general the preoperative assessment includes the knowledge of complete medical
history and physical examination. The performance of investigating all the Hematological and
clinical chemistry must be completely done before the conduction of the surgery as well as all
the other appropriate anesthetic investigation must be complete and informed to the patient in an
adequate manner and required amount (Van , et al., 2016). The surgery must be avoided in case
if there are any potential risk appears to overshadow the benefits of procedures of the surgery.
This applies to those patients who are not fit medically for the surgery or the ones who are
having any other advanced disease.
Steps for preoperative management are first the informed consent i.e. all the basic details
must be explained to the patient like the possible outcomes, desired results and other alternatives
etc. Second one is preparation of stoma. It is required for all the patients undergoing the surgery
for colon cancer where all the patients may be completely warned about the possibility of the
surgeon and the basic difference between the temporary and permanent stoma must be explained
in details. The nurses may visit in case of if their role is identified in the stoma therapy, who can
help in developing the physical, social, cultural and psychological factors. They also take
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
NURSING 4
initiatives of teaching the patients etc. Third step is the Bowel preparations i.e. current standard
practice taken place before surgery.
Though, recently randomized controlled trials procedure do not have any such conclusive
benefit. Next step is the cross matching and the blood transfusion and its requirement is
completely dependent upon the preparative hemoglobin and extent of loss of blood in
intraoperative stage. It is then followed by the Thromboembolism prophylaxis. Cancer is
generally shown to have independent risk of developing thromboembolism and its risk is very
much high in colon cancer surgery this is because it’s a long derationed procedure. Next step is
the Antibiotic prophylaxis which is helpful in reducing and shortening the stays in hospitals and
other infection related costs. Last step can be measuring the temperature of the body. Before
taking the patient to the O.T. the normal level of blood temperature must be achieved by the
usages of heated blankets of air and fluid warming (Harvey & Geary, 2018).
While curing the cancer the done treatment may also have some side effects and the
problems which may affect the healthy tissues or the organs. A few out of them are amnesia, loss
of appetite, bleeding and bruising, constipation, diarrhea, swelling, fatigue, symptoms of flu,
infections, problems in the memory or concentration, mouth and throat problems, sexual health
issues in men, sleep problems, urinary and bladder problems etc. (Benson , Chakravarthy,
Hamilton, & Sigurdson, 2013).
An example of the case of colon cancer treated with surgery taken from a report in
Japanese journal determines that there was a 53 years old man who was cured from colon cancer
after conduction of curative surgery for crosswise anastomotic recurrence. While examining he
was first noticed with sub mucosal tumor of 1.3 cm which was located on the line of suture and
during was found to have an annual follow up barium enema and colonoscopy. In a repeat
initiatives of teaching the patients etc. Third step is the Bowel preparations i.e. current standard
practice taken place before surgery.
Though, recently randomized controlled trials procedure do not have any such conclusive
benefit. Next step is the cross matching and the blood transfusion and its requirement is
completely dependent upon the preparative hemoglobin and extent of loss of blood in
intraoperative stage. It is then followed by the Thromboembolism prophylaxis. Cancer is
generally shown to have independent risk of developing thromboembolism and its risk is very
much high in colon cancer surgery this is because it’s a long derationed procedure. Next step is
the Antibiotic prophylaxis which is helpful in reducing and shortening the stays in hospitals and
other infection related costs. Last step can be measuring the temperature of the body. Before
taking the patient to the O.T. the normal level of blood temperature must be achieved by the
usages of heated blankets of air and fluid warming (Harvey & Geary, 2018).
While curing the cancer the done treatment may also have some side effects and the
problems which may affect the healthy tissues or the organs. A few out of them are amnesia, loss
of appetite, bleeding and bruising, constipation, diarrhea, swelling, fatigue, symptoms of flu,
infections, problems in the memory or concentration, mouth and throat problems, sexual health
issues in men, sleep problems, urinary and bladder problems etc. (Benson , Chakravarthy,
Hamilton, & Sigurdson, 2013).
An example of the case of colon cancer treated with surgery taken from a report in
Japanese journal determines that there was a 53 years old man who was cured from colon cancer
after conduction of curative surgery for crosswise anastomotic recurrence. While examining he
was first noticed with sub mucosal tumor of 1.3 cm which was located on the line of suture and
during was found to have an annual follow up barium enema and colonoscopy. In a repeat
NURSING 5
examined after 3 months later reflected lesion which is considered as a typical type of cancer
which was 2.5 cm in size with a large ulcerated area. For the intention of curing right
hemicolectomy was performed. In this report it was seen that it was for the first time that
recurrent lesion was detected as a sub mucosal tumor at the time of annual follow-up
examinations (Rodrigo, 2016).
Post-operative measures undertaken after surgery of colon cancer stage 1 are as follows
first one is mobilization of the patient i.e. initial and liberal patient deployment which is
associated with shorter length of stay. Grade of recommendation: which is strongly
recommended and based upon low-quality evidence, this further includes problems of protracted
stillness along with loss of skeletal muscle and weakness, atelectasis, insulin resistance,
thromboembolic disease, and decreased capacity of exercising. This deconditioning is associated
with bed rest and can reduce the physical activities of the patients (McSorley, Watt, Horgan, &
McMillan, 2016).
Second step is the Ileus anticipation where the patients are to be offered with a regular
diet directly after the surgery. Grade of recommendation is strongly based on the in taking of the
medicines. Third one is the fluid management i.e. Vein fluids should be finished in the early
postoperative period immediately after getting discharged from the room of recovery. Grade of
recommendation is strongly based upon the moderate quality of evidence (Artinyan, et al., 2015),
Fourth one is the urinary catheters i.e. It must be detached within 24 hours of the surgery when
not involving a vesicular fistula, irrespective of the usage of TEA. Grade of recommendation is
strongly based on moderate quality of evidence (Morice, Leary, Creutzberg, Abu-Rustum, &
Darai, 2016).
examined after 3 months later reflected lesion which is considered as a typical type of cancer
which was 2.5 cm in size with a large ulcerated area. For the intention of curing right
hemicolectomy was performed. In this report it was seen that it was for the first time that
recurrent lesion was detected as a sub mucosal tumor at the time of annual follow-up
examinations (Rodrigo, 2016).
Post-operative measures undertaken after surgery of colon cancer stage 1 are as follows
first one is mobilization of the patient i.e. initial and liberal patient deployment which is
associated with shorter length of stay. Grade of recommendation: which is strongly
recommended and based upon low-quality evidence, this further includes problems of protracted
stillness along with loss of skeletal muscle and weakness, atelectasis, insulin resistance,
thromboembolic disease, and decreased capacity of exercising. This deconditioning is associated
with bed rest and can reduce the physical activities of the patients (McSorley, Watt, Horgan, &
McMillan, 2016).
Second step is the Ileus anticipation where the patients are to be offered with a regular
diet directly after the surgery. Grade of recommendation is strongly based on the in taking of the
medicines. Third one is the fluid management i.e. Vein fluids should be finished in the early
postoperative period immediately after getting discharged from the room of recovery. Grade of
recommendation is strongly based upon the moderate quality of evidence (Artinyan, et al., 2015),
Fourth one is the urinary catheters i.e. It must be detached within 24 hours of the surgery when
not involving a vesicular fistula, irrespective of the usage of TEA. Grade of recommendation is
strongly based on moderate quality of evidence (Morice, Leary, Creutzberg, Abu-Rustum, &
Darai, 2016).
NURSING 6
Conclusion
Thus to conclude it can be determined that the patient suffering from the colon cancer
stage 1and undergoing a surgery are to take up following pre and post-operative measures as are
recommended by the peer reviewed articles and journals mentioned above.
References
Artinyan, A., Orcutt, S. T., Anaya, D. A., Richardson, P., Chen, G. J., & Berger, D. H. (2015).
Infectious postoperative complications decrease long-term survival in patients
undergoing curative surgery for colorectal cancer: a study of 12,075 patients. Annals of
surgery, 261(3), 497-505.
Bakker, N., Cakir, H., Doodeman, H. J., & Houdijk, A. J. (2015). Eight years of experience with
enhanced recovery after surgery in patients with colon cancer: impact of measures to
improve adherence. Surgery, 157(6), 1130-1136.
Benson , A., Chakravarthy, A., Hamilton, S., & Sigurdson, E. (2013). Cancers of the Colon and
Rectum: A Multidisciplinary Approach to Diagnosis and Management. Demos Medical
Publishing.
Chun, M. (2019, February 12). Stages of Colon Cancer. Retrieved from Healthline:
https://www.healthline.com/health/colorectal-cancer/stages-of-colon-cancer
clinic, M. (2019, April 16). Diagnosis Screening for colon cancer. Retrieved from cOLON
cANCER: https://www.mayoclinic.org/diseases-conditions/colon-cancer/diagnosis-
treatment/drc-20353674
Du, Y. (2017). PET/CT in Colorectal Cancer. Springer.
Conclusion
Thus to conclude it can be determined that the patient suffering from the colon cancer
stage 1and undergoing a surgery are to take up following pre and post-operative measures as are
recommended by the peer reviewed articles and journals mentioned above.
References
Artinyan, A., Orcutt, S. T., Anaya, D. A., Richardson, P., Chen, G. J., & Berger, D. H. (2015).
Infectious postoperative complications decrease long-term survival in patients
undergoing curative surgery for colorectal cancer: a study of 12,075 patients. Annals of
surgery, 261(3), 497-505.
Bakker, N., Cakir, H., Doodeman, H. J., & Houdijk, A. J. (2015). Eight years of experience with
enhanced recovery after surgery in patients with colon cancer: impact of measures to
improve adherence. Surgery, 157(6), 1130-1136.
Benson , A., Chakravarthy, A., Hamilton, S., & Sigurdson, E. (2013). Cancers of the Colon and
Rectum: A Multidisciplinary Approach to Diagnosis and Management. Demos Medical
Publishing.
Chun, M. (2019, February 12). Stages of Colon Cancer. Retrieved from Healthline:
https://www.healthline.com/health/colorectal-cancer/stages-of-colon-cancer
clinic, M. (2019, April 16). Diagnosis Screening for colon cancer. Retrieved from cOLON
cANCER: https://www.mayoclinic.org/diseases-conditions/colon-cancer/diagnosis-
treatment/drc-20353674
Du, Y. (2017). PET/CT in Colorectal Cancer. Springer.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
NURSING 7
Harvey, M., & Geary, T. (2018). Preoperative assessment and preparation for safe paediatric
anaesthesia. Anaesthesia & Intensive Care Medicine, 19(8), 401-408.
McSorley, S. T., Watt, D. G., Horgan, P. G., & McMillan, D. C. (2016). Postoperative systemic
inflammatory response, complication severity, and survival following surgery for
colorectal cancer. Annals of surgical oncology, 23(9), 2832-2840.
Morice, P., Leary, A., Creutzberg, C., Abu-Rustum, N., & Darai, E. (2016). Endometrial cancer.
The Lancet, 387(10023), 1094-1108.
Rodrigo, L. (2016). Colorectal Cancer: From Pathogenesis to Treatment. BoD – Books on
Demand.
texasoncology. (2019). STAGE I COLON CANCER. Retrieved from Texas Oncology:
https://www.texasoncology.com/types-of-cancer/colon-cancer/stage-i-colon-cancer
Van , C. E., Cervantes, A., Adam, R., Sobrero, A., Van , K. J., Aderka, D., & Ciardiello, F.
(2016). ESMO consensus guidelines for the management of patients with metastatic
colorectal cancer. Annals of Oncology, 27(8), 1386-1422.
Harvey, M., & Geary, T. (2018). Preoperative assessment and preparation for safe paediatric
anaesthesia. Anaesthesia & Intensive Care Medicine, 19(8), 401-408.
McSorley, S. T., Watt, D. G., Horgan, P. G., & McMillan, D. C. (2016). Postoperative systemic
inflammatory response, complication severity, and survival following surgery for
colorectal cancer. Annals of surgical oncology, 23(9), 2832-2840.
Morice, P., Leary, A., Creutzberg, C., Abu-Rustum, N., & Darai, E. (2016). Endometrial cancer.
The Lancet, 387(10023), 1094-1108.
Rodrigo, L. (2016). Colorectal Cancer: From Pathogenesis to Treatment. BoD – Books on
Demand.
texasoncology. (2019). STAGE I COLON CANCER. Retrieved from Texas Oncology:
https://www.texasoncology.com/types-of-cancer/colon-cancer/stage-i-colon-cancer
Van , C. E., Cervantes, A., Adam, R., Sobrero, A., Van , K. J., Aderka, D., & Ciardiello, F.
(2016). ESMO consensus guidelines for the management of patients with metastatic
colorectal cancer. Annals of Oncology, 27(8), 1386-1422.
1 out of 8
Related Documents

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.