Deakin University HNN108: Delirium Intervention Report
VerifiedAdded on 2022/10/10
|11
|2346
|388
Report
AI Summary
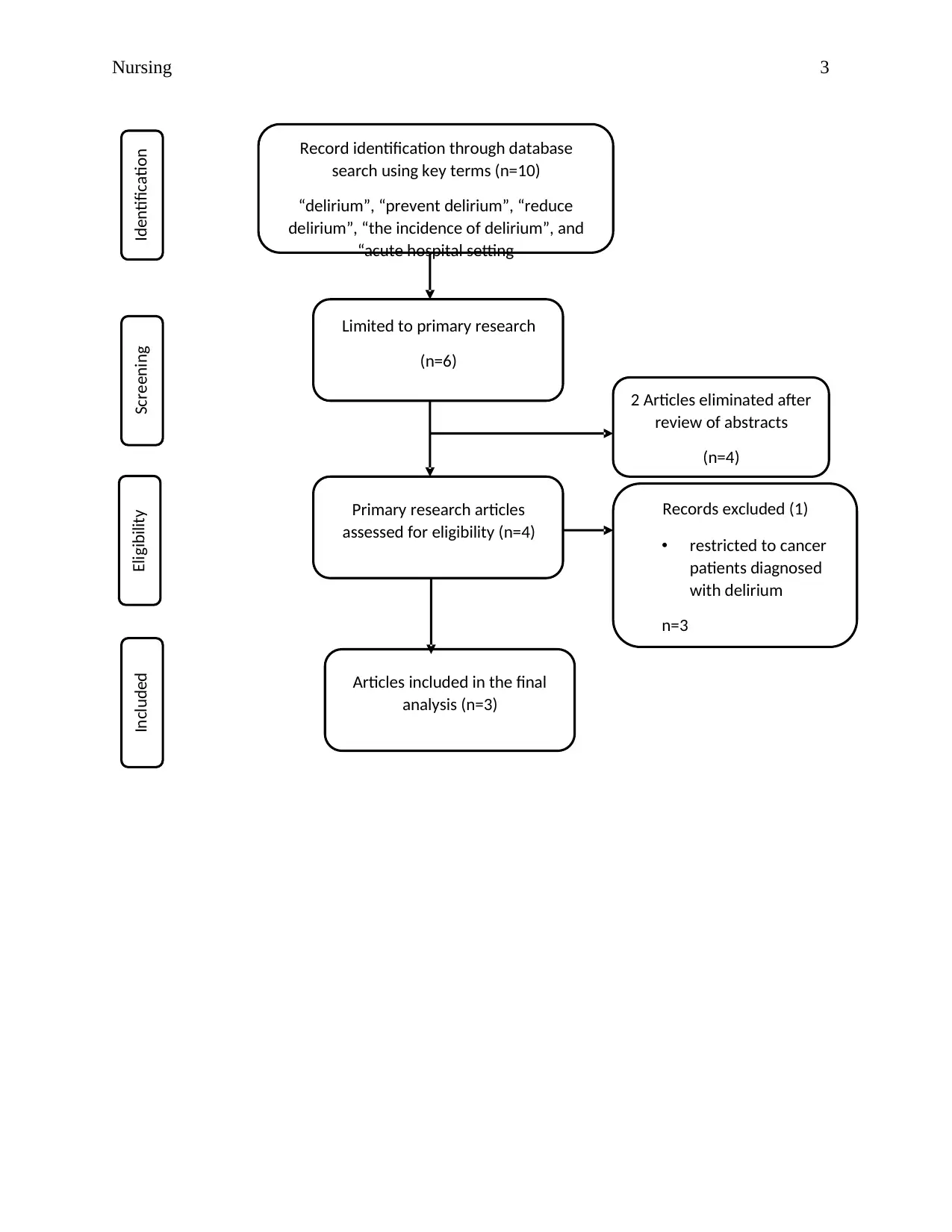
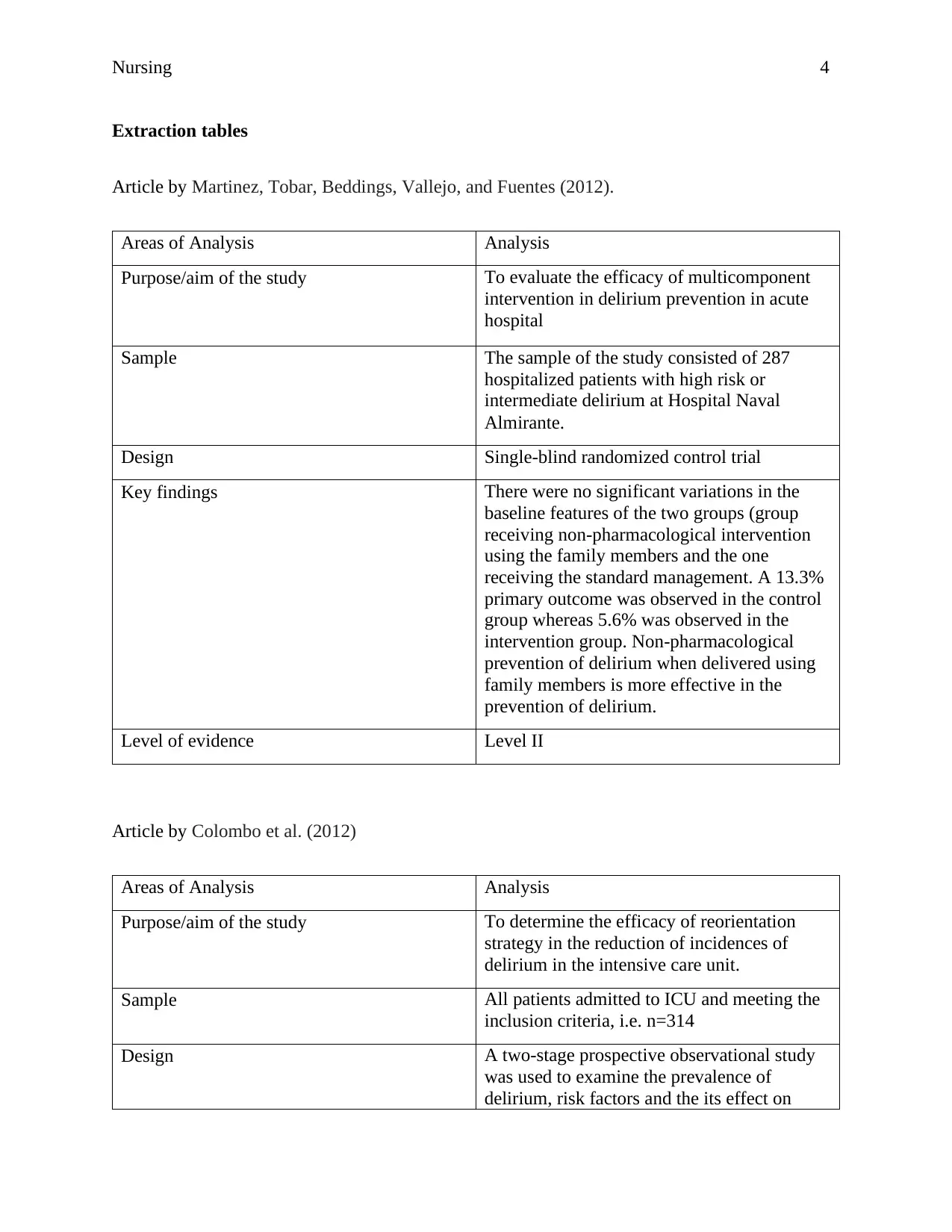
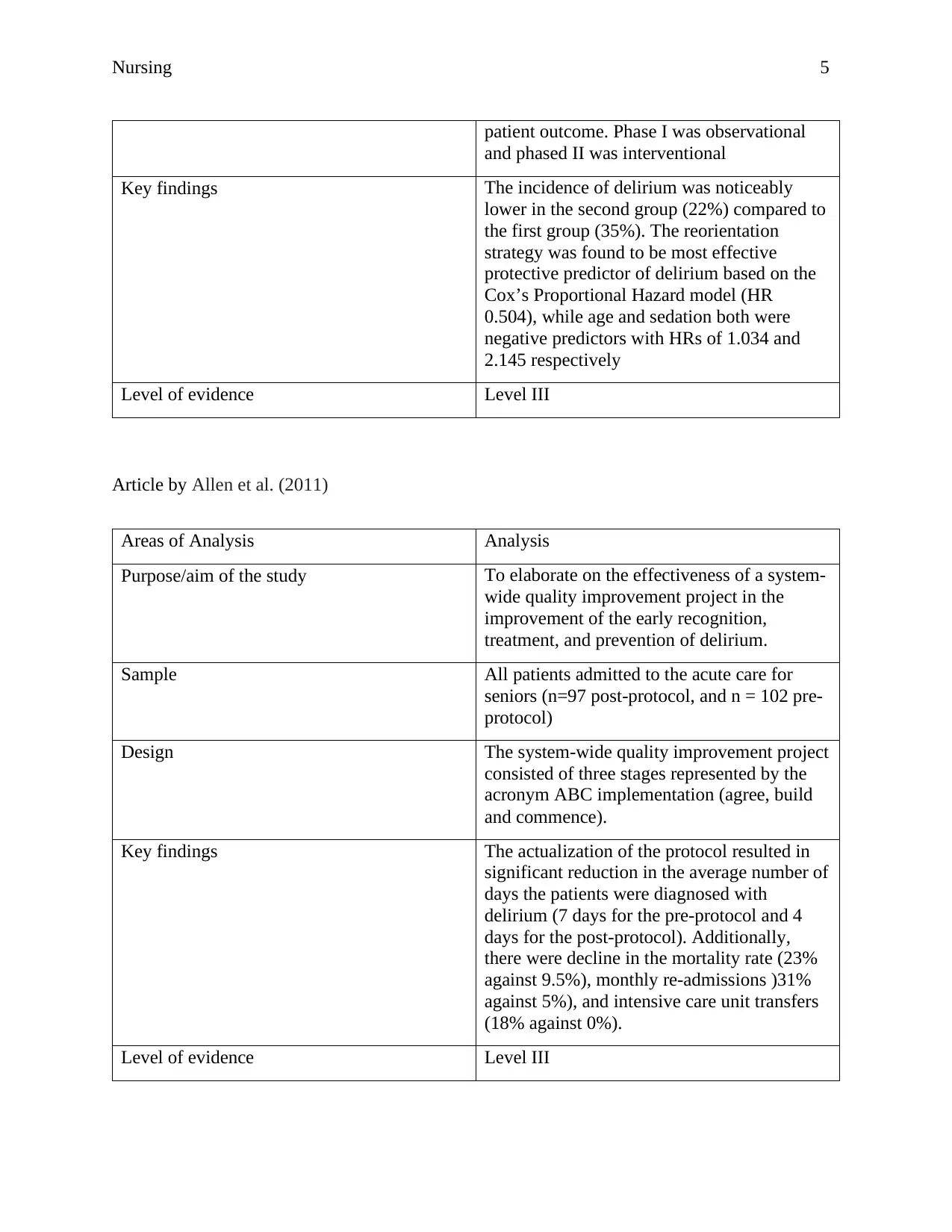
This report critically analyzes the effectiveness of various interventions in preventing and reducing the incidence of delirium in acute hospital settings. The report synthesizes evidence from three primary research articles, focusing on non-pharmacological interventions, reorientation strategies, and system-wide quality improvement projects. The methodology includes an electronic search of databases like PMC, Oxford, MEDLINE, and Cochrane Collaboration, with specific keywords and inclusion/exclusion criteria to identify relevant studies. The analysis evaluates the study designs, samples, key findings, and levels of evidence for each intervention. The report highlights the benefits and limitations of each approach, such as randomized control trials, prospective observational studies, and retrospective observational studies. Ultimately, the report recommends non-pharmacological interventions as the most effective strategy for preventing delirium, supported by the strength of evidence and the reduction in delirium incidence observed in the studies. The report also discusses the implications of the findings, including the need for further research and the importance of implementing evidence-based practices to improve patient outcomes.

1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.