Nursing Assignment: Hypovolemic Shock and Nursing Interventions
VerifiedAdded on 2022/12/15
|11
|2593
|238
AI Summary
This nursing assignment discusses the problem of hypovolemic shock and provides nursing interventions for its management. It explains the causes and symptoms of hypovolemic shock and emphasizes the importance of prompt nursing interventions. The assignment also includes evidence-based assessments and goals for patient care. The document type is an assignment and the type of assignment is a nursing assignment.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: NURSING ASSIGNMENT
NURSING ASSIGNMENT
Name of the Student
Name of the university
Author’s note
NURSING ASSIGNMENT
Name of the Student
Name of the university
Author’s note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1NURSING ASSIGNMENT
Justification of Nursing Problem Statement
Hypovolemic shock is a severe lethal condition that is caused by the severe blood loss
and fluid loss after a surgery. Patients suffering from hypovolemia have decreased peripheral
perfusion and if it is let untreated, it can develop ischemic injury of the vital organs, causing
multi-organ failure (Gutierrez, Reines & Wulf-Gutierrez, 2014). Hypovolemic shock commonly
occurs in critical care units. This situation is of particular risk for Darren, as considerable loss of
the intravascular volume might lead to hemodynamic instability, reduced perfusion of the tissue,
cellular damage, cellular hypoxia, damaged of the organs and death (Dellinger et al., 2013).
Class I hypovolemic shock is a preterminal complications that requires immediate therapy.
It is evident from the case study Darren Roberts that he had undergone an open
cholecystectomy surgery and is at a risk of developing hypovolemic shock due to the excessive
blood loss. The skin of the patient looks cool and clammy. Patients often feel sluggish and the
skin becomes pale and clammy due to the inadequate pumping of the heart (Noel-Morgan, &
Muir, 2018). The patient also feels sluggishness and sleepiness and confusion because of the
lack of blood flow in to the vital organs. The estimated blood loss is again complicated by many
factors like the renal impairment and the development of tissue edema.
Hypovolemic shock due to the loss of the extracellular fluid can be caused due to the
etiologies like gastrointestinal loss, where the gastrointestinal tract secretes 3-6 liters in a day.
Volume depletion might occur if the fluid from the GI tract are not observed (Noel-Morgan, &
Muir, 2018). The hypovolemic shock occurs due to the reduction of the intravascular volume,
which can be due to extracellular blood loss or loss of fluid from the body. It should be noted in
Justification of Nursing Problem Statement
Hypovolemic shock is a severe lethal condition that is caused by the severe blood loss
and fluid loss after a surgery. Patients suffering from hypovolemia have decreased peripheral
perfusion and if it is let untreated, it can develop ischemic injury of the vital organs, causing
multi-organ failure (Gutierrez, Reines & Wulf-Gutierrez, 2014). Hypovolemic shock commonly
occurs in critical care units. This situation is of particular risk for Darren, as considerable loss of
the intravascular volume might lead to hemodynamic instability, reduced perfusion of the tissue,
cellular damage, cellular hypoxia, damaged of the organs and death (Dellinger et al., 2013).
Class I hypovolemic shock is a preterminal complications that requires immediate therapy.
It is evident from the case study Darren Roberts that he had undergone an open
cholecystectomy surgery and is at a risk of developing hypovolemic shock due to the excessive
blood loss. The skin of the patient looks cool and clammy. Patients often feel sluggish and the
skin becomes pale and clammy due to the inadequate pumping of the heart (Noel-Morgan, &
Muir, 2018). The patient also feels sluggishness and sleepiness and confusion because of the
lack of blood flow in to the vital organs. The estimated blood loss is again complicated by many
factors like the renal impairment and the development of tissue edema.
Hypovolemic shock due to the loss of the extracellular fluid can be caused due to the
etiologies like gastrointestinal loss, where the gastrointestinal tract secretes 3-6 liters in a day.
Volume depletion might occur if the fluid from the GI tract are not observed (Noel-Morgan, &
Muir, 2018). The hypovolemic shock occurs due to the reduction of the intravascular volume,
which can be due to extracellular blood loss or loss of fluid from the body. It should be noted in
2NURSING ASSIGNMENT
this context, that the body tries to compensate with the augmented sympathetic tone causing a
rise in the heart rate, augmented cardiac contractility and peripheral vasoconstriction. In case of a
hypovolemic shock there is an increase in the blood pressure with a narrowed pulse pressure. As
the volume status decreases, the systolic blood pressure drops (Noel-Morgan, & Muir, 2018).
Hence the oxygen delivery in the vital organ reduces resulting in the switching to anaerobic
metabolism to aerobic metabolism leading to lactic acid metabolism. With the increase of the
sympathetic drive, the flow of the blood is diverted from other organs for preserving the blood
flow to the brain and heart. This helps in the progression of the tissue ischemia and worsens the
occurrence of lactic acidosis. This condition is specifically important to treat for Darren Roberts,
as such situations can worsen the hemodynamic compromise and can bring about mortality.
Again, it can be seen from the case study that Darren Roberts had met the anesthesia
prior to the surgery. Depression of the cardiac performance associated with anesthesia and
arterial vasodilation have a well-recognized hostile effects. The venous circulation, containing
65-70% of the entire volume of the blood, that is a crucial contributor to the stroke volume and
the cardiac output. Vasodilation is the main cause of relative hypovolemia produced by the
anesthetic drugs (Noel-Morgan & Muir, 2018). Impairment of Anesthetic drug is a deceptive and
an appreciated cause of relative hypotension in the patient. It is evident from the case study of
the patients that the patient had mild hypotension, which can be worsened anesthesia related
hypotension.
Patient centered SMART goal
The client will be able to maintain appropriate cardiac output, evidences by strong
peripheral pulses, with a systolic blood pressure within the range 20mm Hg of the baseline, with
this context, that the body tries to compensate with the augmented sympathetic tone causing a
rise in the heart rate, augmented cardiac contractility and peripheral vasoconstriction. In case of a
hypovolemic shock there is an increase in the blood pressure with a narrowed pulse pressure. As
the volume status decreases, the systolic blood pressure drops (Noel-Morgan, & Muir, 2018).
Hence the oxygen delivery in the vital organ reduces resulting in the switching to anaerobic
metabolism to aerobic metabolism leading to lactic acid metabolism. With the increase of the
sympathetic drive, the flow of the blood is diverted from other organs for preserving the blood
flow to the brain and heart. This helps in the progression of the tissue ischemia and worsens the
occurrence of lactic acidosis. This condition is specifically important to treat for Darren Roberts,
as such situations can worsen the hemodynamic compromise and can bring about mortality.
Again, it can be seen from the case study that Darren Roberts had met the anesthesia
prior to the surgery. Depression of the cardiac performance associated with anesthesia and
arterial vasodilation have a well-recognized hostile effects. The venous circulation, containing
65-70% of the entire volume of the blood, that is a crucial contributor to the stroke volume and
the cardiac output. Vasodilation is the main cause of relative hypovolemia produced by the
anesthetic drugs (Noel-Morgan & Muir, 2018). Impairment of Anesthetic drug is a deceptive and
an appreciated cause of relative hypotension in the patient. It is evident from the case study of
the patients that the patient had mild hypotension, which can be worsened anesthesia related
hypotension.
Patient centered SMART goal
The client will be able to maintain appropriate cardiac output, evidences by strong
peripheral pulses, with a systolic blood pressure within the range 20mm Hg of the baseline, with
3NURSING ASSIGNMENT
a heart rate of 60 to 100 beats per minute with a normal rhythm, urinary output 30 ml/hr or more
than that, warm and dry skin and normal level of consciousness.
Nursing interventions
Nursing interventions Rationale
1. Electrolyte replacement can be
prescribed (Sharkawy, Sahota,
Maughan, & Lobo, 2014). Hartmann’s
solution is a balanced crystalloid
solution that can be administered
intravenously.
Imbalance of the electrolytes might cause
dysrhythmias or the other pathological
conditions. Operative trauma imposes a great
impact on the physiology of the fluid and the
electrolytes within the body that is greater
than the changes linked with simple lack of
alimentation (Sharkawy, Sahota, Maughan, &
Lobo, 2014). Crystalloid solutions containing
low molecular weight electrolytes can pass
freely across semi-permeable membrane
(between the intra in water and pass Dextrose
solution are given within 4 hours after the
surgery, because they are metabolized rapidly
(Sweeney, McKendry & Bedi, 2013). Another
reason of giving dextrose, instead of free
water is due to the fact that the administration
of even a small volume of water might cause
intravascular hypotonicity causing hemolysis
of the red blood cells owing to the influx of
a heart rate of 60 to 100 beats per minute with a normal rhythm, urinary output 30 ml/hr or more
than that, warm and dry skin and normal level of consciousness.
Nursing interventions
Nursing interventions Rationale
1. Electrolyte replacement can be
prescribed (Sharkawy, Sahota,
Maughan, & Lobo, 2014). Hartmann’s
solution is a balanced crystalloid
solution that can be administered
intravenously.
Imbalance of the electrolytes might cause
dysrhythmias or the other pathological
conditions. Operative trauma imposes a great
impact on the physiology of the fluid and the
electrolytes within the body that is greater
than the changes linked with simple lack of
alimentation (Sharkawy, Sahota, Maughan, &
Lobo, 2014). Crystalloid solutions containing
low molecular weight electrolytes can pass
freely across semi-permeable membrane
(between the intra in water and pass Dextrose
solution are given within 4 hours after the
surgery, because they are metabolized rapidly
(Sweeney, McKendry & Bedi, 2013). Another
reason of giving dextrose, instead of free
water is due to the fact that the administration
of even a small volume of water might cause
intravascular hypotonicity causing hemolysis
of the red blood cells owing to the influx of
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4NURSING ASSIGNMENT
water in to the cell. 5% dextrose solution can
be given to the patient to treat hypovolemia
(Sweeney, McKendry & Bedi, 2013).
Myburgh, (2015) have argued that infusion of
a large amount of fluid to the patients who
does not have enough preload reserves might
result in unbalanced fluid shift to the
interstitial tissue. Hence before the fluid
resuscitation it is necessary to assess the
actual fluid status. The traditional
haemodynamic parameters does not
adequately quantify the degree of
physiological derangement in the
hypovolemic trauma patient (de Castro
Sajioro Azevedo et al., 2016).
Changes in the water and electrolytes takes
place after the surgery due to two reasons like
The central venous pressure gives information
on the filling pressure of the right side of the
heart (Kayilioglu, Dinc, Sozen, Bostanoglu,
Cete & Coskun, 2015). The pulmonary artery
diastolic pressure and the pulmonary capillary
wedge pressure reflect the fluid volume of the
water in to the cell. 5% dextrose solution can
be given to the patient to treat hypovolemia
(Sweeney, McKendry & Bedi, 2013).
Myburgh, (2015) have argued that infusion of
a large amount of fluid to the patients who
does not have enough preload reserves might
result in unbalanced fluid shift to the
interstitial tissue. Hence before the fluid
resuscitation it is necessary to assess the
actual fluid status. The traditional
haemodynamic parameters does not
adequately quantify the degree of
physiological derangement in the
hypovolemic trauma patient (de Castro
Sajioro Azevedo et al., 2016).
Changes in the water and electrolytes takes
place after the surgery due to two reasons like
The central venous pressure gives information
on the filling pressure of the right side of the
heart (Kayilioglu, Dinc, Sozen, Bostanoglu,
Cete & Coskun, 2015). The pulmonary artery
diastolic pressure and the pulmonary capillary
wedge pressure reflect the fluid volume of the
5NURSING ASSIGNMENT
right side.
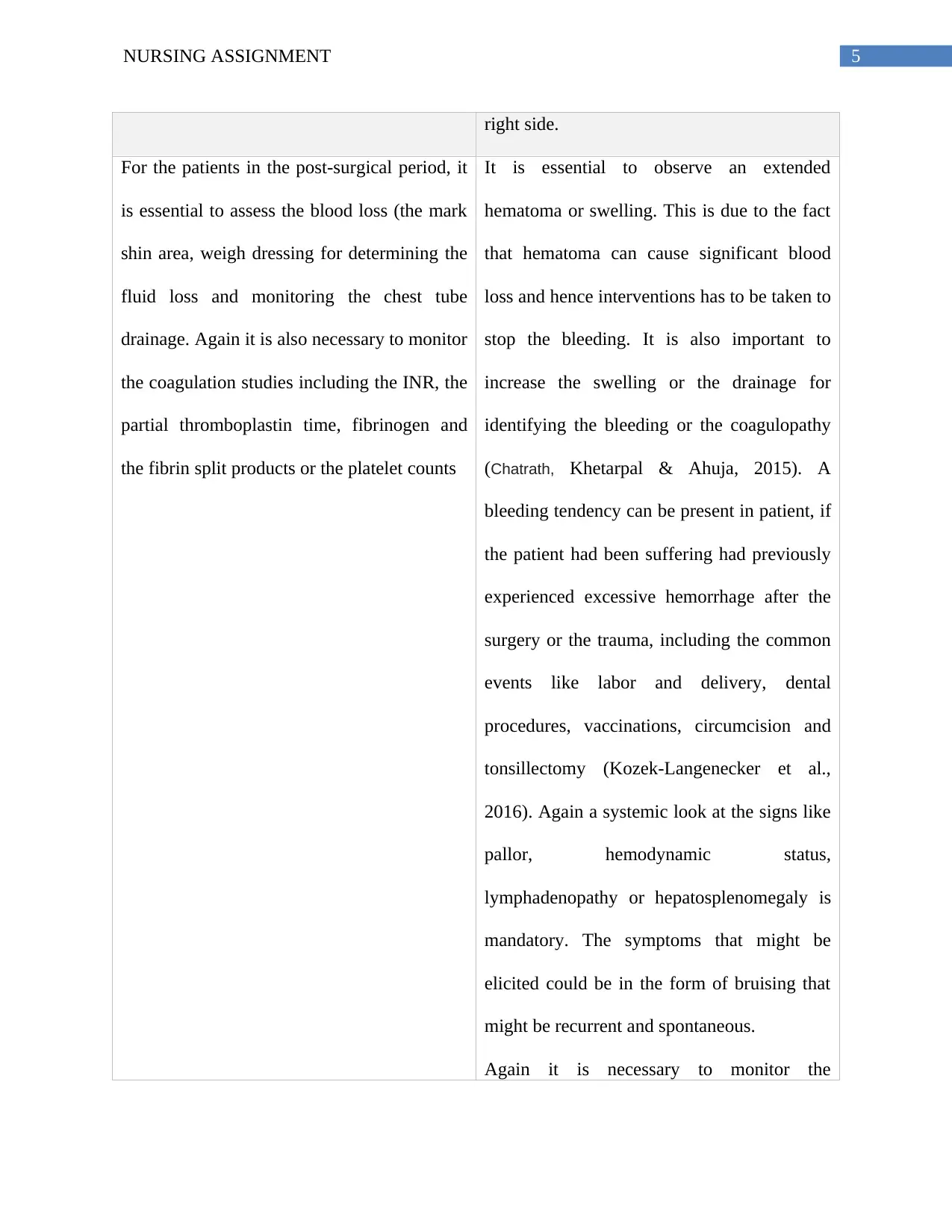
For the patients in the post-surgical period, it
is essential to assess the blood loss (the mark
shin area, weigh dressing for determining the
fluid loss and monitoring the chest tube
drainage. Again it is also necessary to monitor
the coagulation studies including the INR, the
partial thromboplastin time, fibrinogen and
the fibrin split products or the platelet counts
It is essential to observe an extended
hematoma or swelling. This is due to the fact
that hematoma can cause significant blood
loss and hence interventions has to be taken to
stop the bleeding. It is also important to
increase the swelling or the drainage for
identifying the bleeding or the coagulopathy
(Chatrath, Khetarpal & Ahuja, 2015). A
bleeding tendency can be present in patient, if
the patient had been suffering had previously
experienced excessive hemorrhage after the
surgery or the trauma, including the common
events like labor and delivery, dental
procedures, vaccinations, circumcision and
tonsillectomy (Kozek-Langenecker et al.,
2016). Again a systemic look at the signs like
pallor, hemodynamic status,
lymphadenopathy or hepatosplenomegaly is
mandatory. The symptoms that might be
elicited could be in the form of bruising that
might be recurrent and spontaneous.
Again it is necessary to monitor the
right side.
For the patients in the post-surgical period, it
is essential to assess the blood loss (the mark
shin area, weigh dressing for determining the
fluid loss and monitoring the chest tube
drainage. Again it is also necessary to monitor
the coagulation studies including the INR, the
partial thromboplastin time, fibrinogen and
the fibrin split products or the platelet counts
It is essential to observe an extended
hematoma or swelling. This is due to the fact
that hematoma can cause significant blood
loss and hence interventions has to be taken to
stop the bleeding. It is also important to
increase the swelling or the drainage for
identifying the bleeding or the coagulopathy
(Chatrath, Khetarpal & Ahuja, 2015). A
bleeding tendency can be present in patient, if
the patient had been suffering had previously
experienced excessive hemorrhage after the
surgery or the trauma, including the common
events like labor and delivery, dental
procedures, vaccinations, circumcision and
tonsillectomy (Kozek-Langenecker et al.,
2016). Again a systemic look at the signs like
pallor, hemodynamic status,
lymphadenopathy or hepatosplenomegaly is
mandatory. The symptoms that might be
elicited could be in the form of bruising that
might be recurrent and spontaneous.
Again it is necessary to monitor the
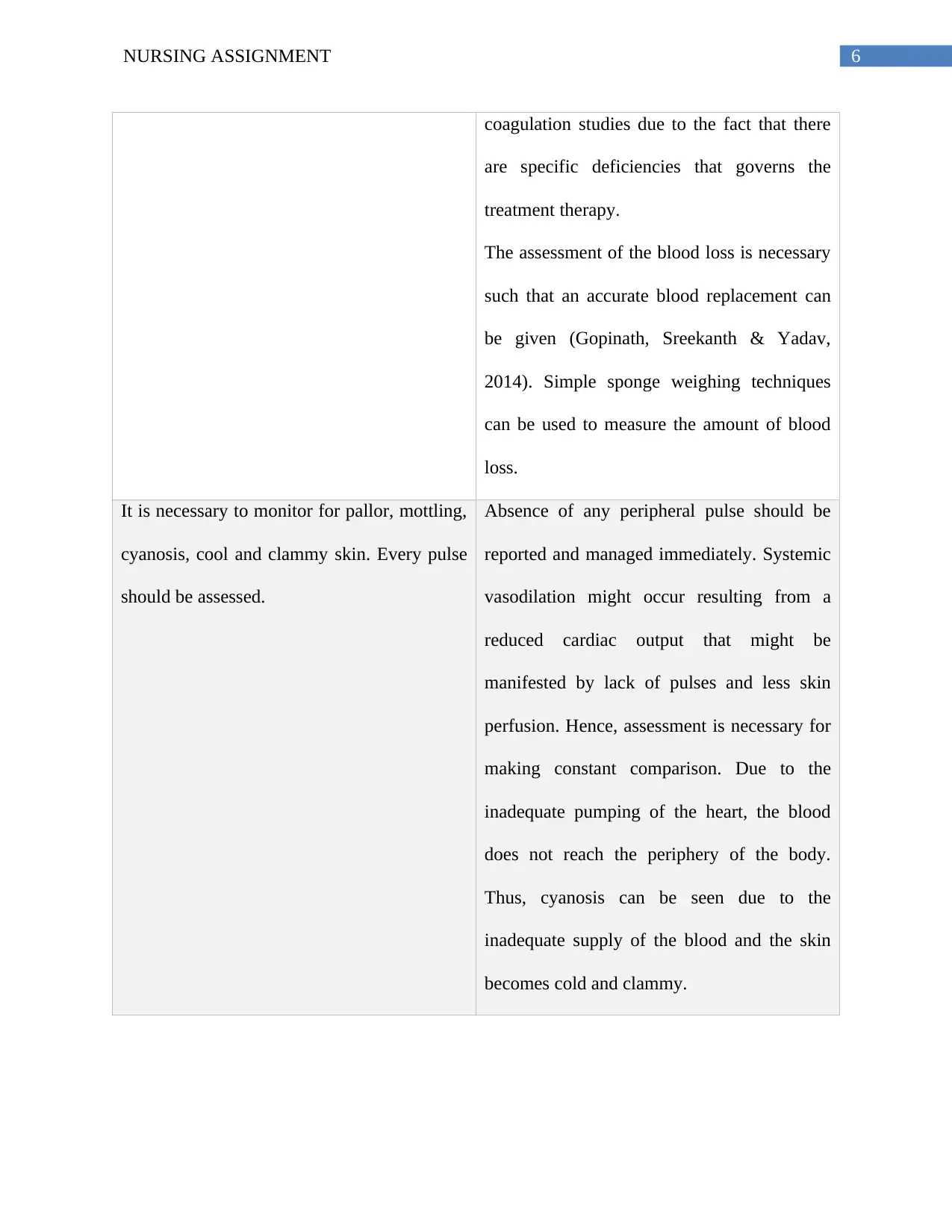
6NURSING ASSIGNMENT
coagulation studies due to the fact that there
are specific deficiencies that governs the
treatment therapy.
The assessment of the blood loss is necessary
such that an accurate blood replacement can
be given (Gopinath, Sreekanth & Yadav,
2014). Simple sponge weighing techniques
can be used to measure the amount of blood
loss.
It is necessary to monitor for pallor, mottling,
cyanosis, cool and clammy skin. Every pulse
should be assessed.
Absence of any peripheral pulse should be
reported and managed immediately. Systemic
vasodilation might occur resulting from a
reduced cardiac output that might be
manifested by lack of pulses and less skin
perfusion. Hence, assessment is necessary for
making constant comparison. Due to the
inadequate pumping of the heart, the blood
does not reach the periphery of the body.
Thus, cyanosis can be seen due to the
inadequate supply of the blood and the skin
becomes cold and clammy.
coagulation studies due to the fact that there
are specific deficiencies that governs the
treatment therapy.
The assessment of the blood loss is necessary
such that an accurate blood replacement can
be given (Gopinath, Sreekanth & Yadav,
2014). Simple sponge weighing techniques
can be used to measure the amount of blood
loss.
It is necessary to monitor for pallor, mottling,
cyanosis, cool and clammy skin. Every pulse
should be assessed.
Absence of any peripheral pulse should be
reported and managed immediately. Systemic
vasodilation might occur resulting from a
reduced cardiac output that might be
manifested by lack of pulses and less skin
perfusion. Hence, assessment is necessary for
making constant comparison. Due to the
inadequate pumping of the heart, the blood
does not reach the periphery of the body.
Thus, cyanosis can be seen due to the
inadequate supply of the blood and the skin
becomes cold and clammy.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7NURSING ASSIGNMENT
Evidence based assessment
An intervention can only be completed after a proper assessment is made to evaluate the
effectiveness of the interventions. Nurses can check the tissue perfusion of the vital organs,
which can be checked by the presence of warm and dry skin (He, Long, Liu, Wang & Zhou, 2015).
On effective management, the client will be able to maintain a strong cardiac output. It can be
evidences by the presence of strong peripheral pulses (Baird, 2015). Nurses can be sure about the
effectiveness of the intervention by monitoring the heart beat with normal cardiac rhythms. The
client will become normovolemic with a greater heart rate. Systolic blood pressure will be
greater than equal to about 90 mm Hg. The urinary output of this client is less than that of the
normal value and hence the urinary output of the patient will be restored to 30ml/hr or more. The
skin of the patients will be warm, dry and normal level of consciousness and turgor. The ABG
signs of the patient will display normal value. There would be no edema, alert LOC and no
incidence of the chest pain. Furthermore the pulse rate should be normal and the oxygen
saturation rate should be above 96-98%. The laboratory data has to be reviewed like the
electrolytes, the creatinine, and the international normalized ratio. The prothrombin time and the
partial prothrombin time should show a normal value in case the anticoagulants are used for this
patient.
However, it can be said that post surgical care requires immediate and prompt nursing
interventions, such as fluid resuscitation, assessment of pulse rate , vital signs in order to prevent
premature mortality.
Evidence based assessment
An intervention can only be completed after a proper assessment is made to evaluate the
effectiveness of the interventions. Nurses can check the tissue perfusion of the vital organs,
which can be checked by the presence of warm and dry skin (He, Long, Liu, Wang & Zhou, 2015).
On effective management, the client will be able to maintain a strong cardiac output. It can be
evidences by the presence of strong peripheral pulses (Baird, 2015). Nurses can be sure about the
effectiveness of the intervention by monitoring the heart beat with normal cardiac rhythms. The
client will become normovolemic with a greater heart rate. Systolic blood pressure will be
greater than equal to about 90 mm Hg. The urinary output of this client is less than that of the
normal value and hence the urinary output of the patient will be restored to 30ml/hr or more. The
skin of the patients will be warm, dry and normal level of consciousness and turgor. The ABG
signs of the patient will display normal value. There would be no edema, alert LOC and no
incidence of the chest pain. Furthermore the pulse rate should be normal and the oxygen
saturation rate should be above 96-98%. The laboratory data has to be reviewed like the
electrolytes, the creatinine, and the international normalized ratio. The prothrombin time and the
partial prothrombin time should show a normal value in case the anticoagulants are used for this
patient.
However, it can be said that post surgical care requires immediate and prompt nursing
interventions, such as fluid resuscitation, assessment of pulse rate , vital signs in order to prevent
premature mortality.
8NURSING ASSIGNMENT
References
Annane, D., Siami, S., Jaber, S., Martin, C., Elatrous, S., Declère, A. D., ... & Trouillet, J. L.
(2013). Effects of fluid resuscitation with colloids vs crystalloids on mortality in critically
ill patients presenting with hypovolemic shock: the CRISTAL randomized
trial. Jama, 310(17), 1809-1817. doi:10.1001/jama.2013.280502
Baird, M. S. (2015). Manual of Critical Care Nursing-E-Book: Nursing Interventions and
Collaborative Management. Elsevier Health Sciences.
Chatrath, V., Khetarpal, R., & Ahuja, J. (2015). Fluid management in patients with trauma:
Restrictive versus liberal approach. Journal of anaesthesiology, clinical
pharmacology, 31(3), 308. doi: 10.4103/0970-9185.161664
de Castro Sajioro Azevedo, A. L., Fazzolo Scarparo, A., & Pedreschi Chaves, L. D. (2013).
Nurses' care and management actions in emergency trauma cases. Investigación y
Educación en Enfermería, 31(1), 36-43.
Dellinger, R. P., Levy, M. M., Rhodes, A., Annane, D., Gerlach, H., Opal, S. M., ... & Osborn, T.
M. (2013). Surviving Sepsis Campaign: international guidelines for management of
severe sepsis and septic shock, 2012. Intensive care medicine, 39(2), 165-228. doi:
10.1097/EJA.0b013e32835f4d5b.
References
Annane, D., Siami, S., Jaber, S., Martin, C., Elatrous, S., Declère, A. D., ... & Trouillet, J. L.
(2013). Effects of fluid resuscitation with colloids vs crystalloids on mortality in critically
ill patients presenting with hypovolemic shock: the CRISTAL randomized
trial. Jama, 310(17), 1809-1817. doi:10.1001/jama.2013.280502
Baird, M. S. (2015). Manual of Critical Care Nursing-E-Book: Nursing Interventions and
Collaborative Management. Elsevier Health Sciences.
Chatrath, V., Khetarpal, R., & Ahuja, J. (2015). Fluid management in patients with trauma:
Restrictive versus liberal approach. Journal of anaesthesiology, clinical
pharmacology, 31(3), 308. doi: 10.4103/0970-9185.161664
de Castro Sajioro Azevedo, A. L., Fazzolo Scarparo, A., & Pedreschi Chaves, L. D. (2013).
Nurses' care and management actions in emergency trauma cases. Investigación y
Educación en Enfermería, 31(1), 36-43.
Dellinger, R. P., Levy, M. M., Rhodes, A., Annane, D., Gerlach, H., Opal, S. M., ... & Osborn, T.
M. (2013). Surviving Sepsis Campaign: international guidelines for management of
severe sepsis and septic shock, 2012. Intensive care medicine, 39(2), 165-228. doi:
10.1097/EJA.0b013e32835f4d5b.
9NURSING ASSIGNMENT
El-Sharkawy, A. M., Sahota, O., Maughan, R. J., & Lobo, D. N. (2014). The pathophysiology of
fluid and electrolyte balance in the older adult surgical patient. Clinical Nutrition, 33(1),
6-13. https://doi.org/10.1016/j.clnu.2013.11.010
Gopinath, R., Sreekanth, Y., & Yadav, M. (2014). Approach to bleeding patient. Indian journal
of anaesthesia, 58(5), 596–602. doi:10.4103/0019-5049.144664
Gutierrez, G., Reines, H. D., & Wulf-Gutierrez, M. E. (2014). Clinical review: hemorrhagic
shock. Critical care (London, England), 8(5), 373–381. doi:10.1186/cc2851
He, H., Long, Y., Liu, D., Wang, X., & Zhou, X. (2015). Clinical classification of tissue
perfusion based on the central venous oxygen saturation and the peripheral perfusion
index. Critical Care, 19(1), 330. https://doi.org/10.1186/s13054-015-1057-8
https://doi.org/10.1111/joim.12326
Kayilioglu, S. I., Dinc, T., Sozen, I., Bostanoglu, A., Cete, M., & Coskun, F. (2015).
Postoperative fluid management. World journal of critical care medicine, 4(3), 192–201.
doi:10.5492/wjccm.v4.i3.192
Kozek-Langenecker, S. A., Afshari, A., Albaladejo, P., Santullano, C. A. A., De Robertis, E.,
Filipescu, D. C., ... & Jacob, M. (2013). Management of severe perioperative bleeding:
guidelines from the European Society of Anaesthesiology. European Journal of
Anaesthesiology (EJA), 30(6), 270-382. doi: 10.1097/EJA.0b013e32835f4d5b
Malbrain, M. L., Marik, P. E., Witters, I., Cordemans, C., Kirkpatrick, A. W., Roberts, D. J., &
Van Regenmortel, N. (2014). Fluid overload, de-resuscitation, and outcomes in critically
El-Sharkawy, A. M., Sahota, O., Maughan, R. J., & Lobo, D. N. (2014). The pathophysiology of
fluid and electrolyte balance in the older adult surgical patient. Clinical Nutrition, 33(1),
6-13. https://doi.org/10.1016/j.clnu.2013.11.010
Gopinath, R., Sreekanth, Y., & Yadav, M. (2014). Approach to bleeding patient. Indian journal
of anaesthesia, 58(5), 596–602. doi:10.4103/0019-5049.144664
Gutierrez, G., Reines, H. D., & Wulf-Gutierrez, M. E. (2014). Clinical review: hemorrhagic
shock. Critical care (London, England), 8(5), 373–381. doi:10.1186/cc2851
He, H., Long, Y., Liu, D., Wang, X., & Zhou, X. (2015). Clinical classification of tissue
perfusion based on the central venous oxygen saturation and the peripheral perfusion
index. Critical Care, 19(1), 330. https://doi.org/10.1186/s13054-015-1057-8
https://doi.org/10.1111/joim.12326
Kayilioglu, S. I., Dinc, T., Sozen, I., Bostanoglu, A., Cete, M., & Coskun, F. (2015).
Postoperative fluid management. World journal of critical care medicine, 4(3), 192–201.
doi:10.5492/wjccm.v4.i3.192
Kozek-Langenecker, S. A., Afshari, A., Albaladejo, P., Santullano, C. A. A., De Robertis, E.,
Filipescu, D. C., ... & Jacob, M. (2013). Management of severe perioperative bleeding:
guidelines from the European Society of Anaesthesiology. European Journal of
Anaesthesiology (EJA), 30(6), 270-382. doi: 10.1097/EJA.0b013e32835f4d5b
Malbrain, M. L., Marik, P. E., Witters, I., Cordemans, C., Kirkpatrick, A. W., Roberts, D. J., &
Van Regenmortel, N. (2014). Fluid overload, de-resuscitation, and outcomes in critically
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10NURSING ASSIGNMENT
ill or injured patients: a systematic review with suggestions for clinical
practice. Anaesthesiology intensive therapy, 46(5), 361-380. DOI: 10.5603/AIT.2014.0060
Myburgh, J. A. (2015). Fluid resuscitation in acute medicine: what is the current
situation?. Journal of internal medicine, 277(1), 58-68.
Myburgh, J. A., & Mythen, M. G. (2013). Resuscitation fluids. New England Journal of
Medicine, 369(13), 1243-1251. DOI: 10.1056/NEJMra1208627
Noel-Morgan, J., & Muir, W. W. (2018). Anesthesia-Associated Relative Hypovolemia:
Mechanisms, Monitoring, and Treatment Considerations. Frontiers in veterinary science,
5, 53. doi:10.3389/fvets.2018.00053
Sweeney, R. M., McKendry, R. A., & Bedi, A. (2013). Perioperative intravenous fluid therapy
for adults. The Ulster medical journal, 82(3), 171–178.Retrieved from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3913409/
ill or injured patients: a systematic review with suggestions for clinical
practice. Anaesthesiology intensive therapy, 46(5), 361-380. DOI: 10.5603/AIT.2014.0060
Myburgh, J. A. (2015). Fluid resuscitation in acute medicine: what is the current
situation?. Journal of internal medicine, 277(1), 58-68.
Myburgh, J. A., & Mythen, M. G. (2013). Resuscitation fluids. New England Journal of
Medicine, 369(13), 1243-1251. DOI: 10.1056/NEJMra1208627
Noel-Morgan, J., & Muir, W. W. (2018). Anesthesia-Associated Relative Hypovolemia:
Mechanisms, Monitoring, and Treatment Considerations. Frontiers in veterinary science,
5, 53. doi:10.3389/fvets.2018.00053
Sweeney, R. M., McKendry, R. A., & Bedi, A. (2013). Perioperative intravenous fluid therapy
for adults. The Ulster medical journal, 82(3), 171–178.Retrieved from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3913409/
1 out of 11
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.