Nursing Care Plan for Exogenous Cushing's Syndrome: Causes, Symptoms, and Incidence
VerifiedAdded on 2023/04/25
|22
|4470
|499
AI Summary
In this question we will discuss about nursing care plan and below are the summaries point:-
Maureen has been diagnosed with exogenous Cushing's syndrome due to the consumption of glucocorticoid medication.
Excessive therapeutic consumption of glucocorticoid medications, such as prednisolone, is the primary cause of exogenous Cushing's syndrome.
The symptoms of Cushing's syndrome include fatigue, rounding of the face, high LDL levels, and accumulation of fat in the trunk and abdominal regions.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: NURSING CARE PLAN
NURSING CARE PLAN
Name of the Student:
Name of the University:
Author note:
NURSING CARE PLAN
Name of the Student:
Name of the University:
Author note:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

1NURSING CARE PLAN
Question 1
Disease
Maureen has been diagnosed with exogenous Cushing’s syndrome. Cushing’s syndrome
outlines the psychological and physiological changes that accompany as a resultant of
abnormally high circulating levels of the hormone cortisol for prolonged periods of time
(O'brien, DeKlotz&Silverman, 2018).ExogenousCushing’s syndromeoccurs by an interplay of
external mechanisms underlying the increase in the levels cortisol in the blood which in this case,
can be considered as primarily due to consumption of glucocorticoid medications (Özgüç et al.,
2018).Maureen’s diagnosis of exogenous Cushing’s syndrome can be attributed to her
consumption of high dosage of the glucocorticoid medication prednisolone.
Causes
In the case of exogenous type of this disorder, excessive therapeutic consumption of
medications administering glucocorticoids in the body, namely prednisolone, are the primary
causative factor (Morgan, Hassan-Smith & Lavery, 2016). Glucocorticoid medications are
required for the management of autoimmune disorders such as rheumatoid arthritis, lupus,
asthma, dermal disorders, pulmonary disturbances and even tumor associated conditions such as
cancer (Nieman, 2018).Cortisol-like medicines such as glucocorticoids (as observed in
prednisolone medication given to the Maureen) induce functions similar to cortisol in the body
which include regulation of stress response, maintenance of immune status, cardiovascular
functioning and macronutrient metabolism (Paul et al., 2016). However the recommended
dosages outlined for the consumption of these medications often exceed the circulating levels
beyond that tolerated by the human body. Hence, this results in the administration of side effects
Question 1
Disease
Maureen has been diagnosed with exogenous Cushing’s syndrome. Cushing’s syndrome
outlines the psychological and physiological changes that accompany as a resultant of
abnormally high circulating levels of the hormone cortisol for prolonged periods of time
(O'brien, DeKlotz&Silverman, 2018).ExogenousCushing’s syndromeoccurs by an interplay of
external mechanisms underlying the increase in the levels cortisol in the blood which in this case,
can be considered as primarily due to consumption of glucocorticoid medications (Özgüç et al.,
2018).Maureen’s diagnosis of exogenous Cushing’s syndrome can be attributed to her
consumption of high dosage of the glucocorticoid medication prednisolone.
Causes
In the case of exogenous type of this disorder, excessive therapeutic consumption of
medications administering glucocorticoids in the body, namely prednisolone, are the primary
causative factor (Morgan, Hassan-Smith & Lavery, 2016). Glucocorticoid medications are
required for the management of autoimmune disorders such as rheumatoid arthritis, lupus,
asthma, dermal disorders, pulmonary disturbances and even tumor associated conditions such as
cancer (Nieman, 2018).Cortisol-like medicines such as glucocorticoids (as observed in
prednisolone medication given to the Maureen) induce functions similar to cortisol in the body
which include regulation of stress response, maintenance of immune status, cardiovascular
functioning and macronutrient metabolism (Paul et al., 2016). However the recommended
dosages outlined for the consumption of these medications often exceed the circulating levels
beyond that tolerated by the human body. Hence, this results in the administration of side effects
2NURSING CARE PLAN
and the resultant physiological complications in the form of development of a moon or round
face, obesity in the trunk, buffalo hump, purple striae and superclavicular fat pads (Wagner-
Bartak et al., 2017). Additional symptoms are fatigue, weakness in the muscles, loss of bone
mass, hypertension, dyslipidemia, weight gain, and aggravated diabetics symptoms such as
hyperglycemia and impairments in cognitive abilities (Pereira et al., 2016).
Maureen’s symptoms have begun to manifest as observed in her feelings of fatigue,
rounding of her face, high LDL levels and accumulation of fat in the trunk and abdominal
regions. If left untreated, as researched by Papachan et al., (2017), the symptomatic effects of
this disease can impact an increase in her hyperglycemic symptoms of diabetes which will
further impair her carbohydrate and lipid metabolic processes resulting in distorted lipid profile.
Hence, a multidisciplinary treatment will be required as to treat her diabetes, rheumatoid arthritis
and Cushing’s syndrome disorder further impacting her family through high medical expenses
(Radhakutty et al., 2016).
Incidence
Approximately 60% of Cushing’s disease cases in Australia are attributed to high cortisol
medication consumption and is more susceptible in females than in males (8:1). Cushing’s
syndrome affects almost 40 million of the global population (Torres et al., 2019). The incidence
of this disease is highest in patients suffering from co-existing autoimmune disorders and
proliferative disorders of the lymph requiring administration of glucocorticoid medications such
as prednisolone, prednisone, betamethasone, dexamethasone, methylprednisolone
andtriamcinolone (Sharma, Nieman& Feelders, 2015).
and the resultant physiological complications in the form of development of a moon or round
face, obesity in the trunk, buffalo hump, purple striae and superclavicular fat pads (Wagner-
Bartak et al., 2017). Additional symptoms are fatigue, weakness in the muscles, loss of bone
mass, hypertension, dyslipidemia, weight gain, and aggravated diabetics symptoms such as
hyperglycemia and impairments in cognitive abilities (Pereira et al., 2016).
Maureen’s symptoms have begun to manifest as observed in her feelings of fatigue,
rounding of her face, high LDL levels and accumulation of fat in the trunk and abdominal
regions. If left untreated, as researched by Papachan et al., (2017), the symptomatic effects of
this disease can impact an increase in her hyperglycemic symptoms of diabetes which will
further impair her carbohydrate and lipid metabolic processes resulting in distorted lipid profile.
Hence, a multidisciplinary treatment will be required as to treat her diabetes, rheumatoid arthritis
and Cushing’s syndrome disorder further impacting her family through high medical expenses
(Radhakutty et al., 2016).
Incidence
Approximately 60% of Cushing’s disease cases in Australia are attributed to high cortisol
medication consumption and is more susceptible in females than in males (8:1). Cushing’s
syndrome affects almost 40 million of the global population (Torres et al., 2019). The incidence
of this disease is highest in patients suffering from co-existing autoimmune disorders and
proliferative disorders of the lymph requiring administration of glucocorticoid medications such
as prednisolone, prednisone, betamethasone, dexamethasone, methylprednisolone
andtriamcinolone (Sharma, Nieman& Feelders, 2015).

3NURSING CARE PLAN
Risk factors
While the primary risk factor associated with exogenousCushing’s syndrome, as
observed in Maureen’s case is the excessive consumption of glucocorticoid medications, its
endogenous counterpart can be attributed to various endocrinal and genetic risk factors (Al-Ali et
al., 2016). These include the presence of pituitary adenoma, tumors producing
adenocorticotrophic hormone, diseases in the adrenal glands and a family history of Cushing’s
syndrome (Assié, 2018).
Question 2
Signs, Symptoms and Pathophysiology (As designed by the Author)
Signs and Symptoms Pathophysiology
Dyslipidemia resulting in moon face, obesity,
buffalo hump, subclacicular fat pads
From the case study it can be observed that the
patient in question, Maureen is suffering from
high blood levels of LDL cholesterol coupled
with observable rounding of her face and fat
accumulation in her abdominal and shoulder
regions. Cortisol is a steroid hormone whose
primary functions include regulation of key
macronutrient metabolism of which lipid
metabolism is to be considered here. Cortisol
actively administers the function of
gluconeogenesis, which encompasses
breakdown of non-carbohydrate source such as
Risk factors
While the primary risk factor associated with exogenousCushing’s syndrome, as
observed in Maureen’s case is the excessive consumption of glucocorticoid medications, its
endogenous counterpart can be attributed to various endocrinal and genetic risk factors (Al-Ali et
al., 2016). These include the presence of pituitary adenoma, tumors producing
adenocorticotrophic hormone, diseases in the adrenal glands and a family history of Cushing’s
syndrome (Assié, 2018).
Question 2
Signs, Symptoms and Pathophysiology (As designed by the Author)
Signs and Symptoms Pathophysiology
Dyslipidemia resulting in moon face, obesity,
buffalo hump, subclacicular fat pads
From the case study it can be observed that the
patient in question, Maureen is suffering from
high blood levels of LDL cholesterol coupled
with observable rounding of her face and fat
accumulation in her abdominal and shoulder
regions. Cortisol is a steroid hormone whose
primary functions include regulation of key
macronutrient metabolism of which lipid
metabolism is to be considered here. Cortisol
actively administers the function of
gluconeogenesis, which encompasses
breakdown of non-carbohydrate source such as
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4NURSING CARE PLAN
fats into lipids for conductance of
inflammatory responses (Pineyro et al., 2019).
Hence, in exogenous Cushing’s ’s syndrome,
high consumption of cortisol like medications
results in excessive gluconeogenesis, high
mobilization and excessive circulation levels of
lipids and their accumulation in fatty deposits
in the face, shoulders and abdomen as noted in
Muareen (Raff & Carroll, 2015).
Hypertension Maureen has been observed to report high
blood pressure levels which can be associated
with her high consumption of glucocorticoid
medication prednisolone. An additional key
function of cortisols are regulation of the blood
pressure and cardiovascular functioning
performed through influences exerted on the
vasoconstriction functions of catecholamines
like epinephrine, norepinephrine and
dopamione (Isidori et al., 2016). High
circulatory levels of cortisol, as a result of
glucocorticoid medications result in excessive
stimulation of catecholamine functioning
leading to vasoconstriction and high blood
fats into lipids for conductance of
inflammatory responses (Pineyro et al., 2019).
Hence, in exogenous Cushing’s ’s syndrome,
high consumption of cortisol like medications
results in excessive gluconeogenesis, high
mobilization and excessive circulation levels of
lipids and their accumulation in fatty deposits
in the face, shoulders and abdomen as noted in
Muareen (Raff & Carroll, 2015).
Hypertension Maureen has been observed to report high
blood pressure levels which can be associated
with her high consumption of glucocorticoid
medication prednisolone. An additional key
function of cortisols are regulation of the blood
pressure and cardiovascular functioning
performed through influences exerted on the
vasoconstriction functions of catecholamines
like epinephrine, norepinephrine and
dopamione (Isidori et al., 2016). High
circulatory levels of cortisol, as a result of
glucocorticoid medications result in excessive
stimulation of catecholamine functioning
leading to vasoconstriction and high blood
5NURSING CARE PLAN
pressure as observed in Maureen (Lacroix et
al., 2015).Further, an additional method by
which cortisol initiates its regulatory effect on
blood pressure is through aldosterone, which
increases blood pressure through sodium
reuptake and excretion prevention. Hence, such
high levels of sodium uptake mechanisms may
also contribute to the hypertensive symptoms
in Maureen resulting due to excessive
glucocorticoid consumption (Dubrocq et al.,
2017).
Hyperglycemia High levels of fasting blood glucose has been
observed in Maureen. One of the primary
functions of cortisols include the inhibition of
tissue uptake of glucose for nervous tissue
usage and exhibition of the flight or fight
response to stress (Loriaux, 2017). Hence,
excessive glucocorticoid consumption results
in cortisol-like effects of inhibited glucose
uptake by tissues as a result of which high
circulating levels ensue leading to high fasting
blood glucose levels as observed in Maureen
(Kang et al., 2016).
pressure as observed in Maureen (Lacroix et
al., 2015).Further, an additional method by
which cortisol initiates its regulatory effect on
blood pressure is through aldosterone, which
increases blood pressure through sodium
reuptake and excretion prevention. Hence, such
high levels of sodium uptake mechanisms may
also contribute to the hypertensive symptoms
in Maureen resulting due to excessive
glucocorticoid consumption (Dubrocq et al.,
2017).
Hyperglycemia High levels of fasting blood glucose has been
observed in Maureen. One of the primary
functions of cortisols include the inhibition of
tissue uptake of glucose for nervous tissue
usage and exhibition of the flight or fight
response to stress (Loriaux, 2017). Hence,
excessive glucocorticoid consumption results
in cortisol-like effects of inhibited glucose
uptake by tissues as a result of which high
circulating levels ensue leading to high fasting
blood glucose levels as observed in Maureen
(Kang et al., 2016).
6NURSING CARE PLAN
Question 3
Pharmacokinetics – Glucocorticoids
The class of drug most relevant to the case study of Maureen are glucocorticoids such as
prednisolone which have been prescribed to her for the management of her rheumatoid arthritis
and have also been implicated as a primary causative factor in Cushing’s ’s syndrome.
Glucocorticoids like prednisolone are used primarily for the treatment of autoimmune and
inflammatory conditions such as rheumatoid arthritis, lupus, lymphomas, leukemias, allergic
rhinitis or infections pertaining to the skin (Bunte et al., 2018).Upon consumption, prednisolone
undergoes immediate absorption by the gastrointestinal tract resulting in its highest concentration
in the plasma within the first 2 hours of its intake. Upon absorption and metabolism, the half-life
of glucocorticosteroids like prednisolone last for approximately 2 to 3 hours, followed by which
they may undergo excretion as free compounds in the urine or as glucoconjugates (de Heide et
al., 2018).
Pharmacodynamics – Glucocorticoids
Theanti-inflammatory mechanism of action of glucocorticoid prednisolone can be
attributed to actions such as inhibition of the infiltration of leukocytes at the locations
undergoing inflammation, interference with the mediating procedures underlying the response of
inflammation and suppression of responses underlying humoral immunity (Hosseini et al., 2016).
The anti-inflammatory effects of prednisolone also occur due to mechanism of inhibiting dilation
of capillaries and permeation within vascular tissues. Prednisolone’s pharmacodyanmics for
inflammatory process reduction also encompass restriction of polymorphonuclear leukocytes,
Question 3
Pharmacokinetics – Glucocorticoids
The class of drug most relevant to the case study of Maureen are glucocorticoids such as
prednisolone which have been prescribed to her for the management of her rheumatoid arthritis
and have also been implicated as a primary causative factor in Cushing’s ’s syndrome.
Glucocorticoids like prednisolone are used primarily for the treatment of autoimmune and
inflammatory conditions such as rheumatoid arthritis, lupus, lymphomas, leukemias, allergic
rhinitis or infections pertaining to the skin (Bunte et al., 2018).Upon consumption, prednisolone
undergoes immediate absorption by the gastrointestinal tract resulting in its highest concentration
in the plasma within the first 2 hours of its intake. Upon absorption and metabolism, the half-life
of glucocorticosteroids like prednisolone last for approximately 2 to 3 hours, followed by which
they may undergo excretion as free compounds in the urine or as glucoconjugates (de Heide et
al., 2018).
Pharmacodynamics – Glucocorticoids
Theanti-inflammatory mechanism of action of glucocorticoid prednisolone can be
attributed to actions such as inhibition of the infiltration of leukocytes at the locations
undergoing inflammation, interference with the mediating procedures underlying the response of
inflammation and suppression of responses underlying humoral immunity (Hosseini et al., 2016).
The anti-inflammatory effects of prednisolone also occur due to mechanism of inhibiting dilation
of capillaries and permeation within vascular tissues. Prednisolone’s pharmacodyanmics for
inflammatory process reduction also encompass restriction of polymorphonuclear leukocytes,
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7NURSING CARE PLAN
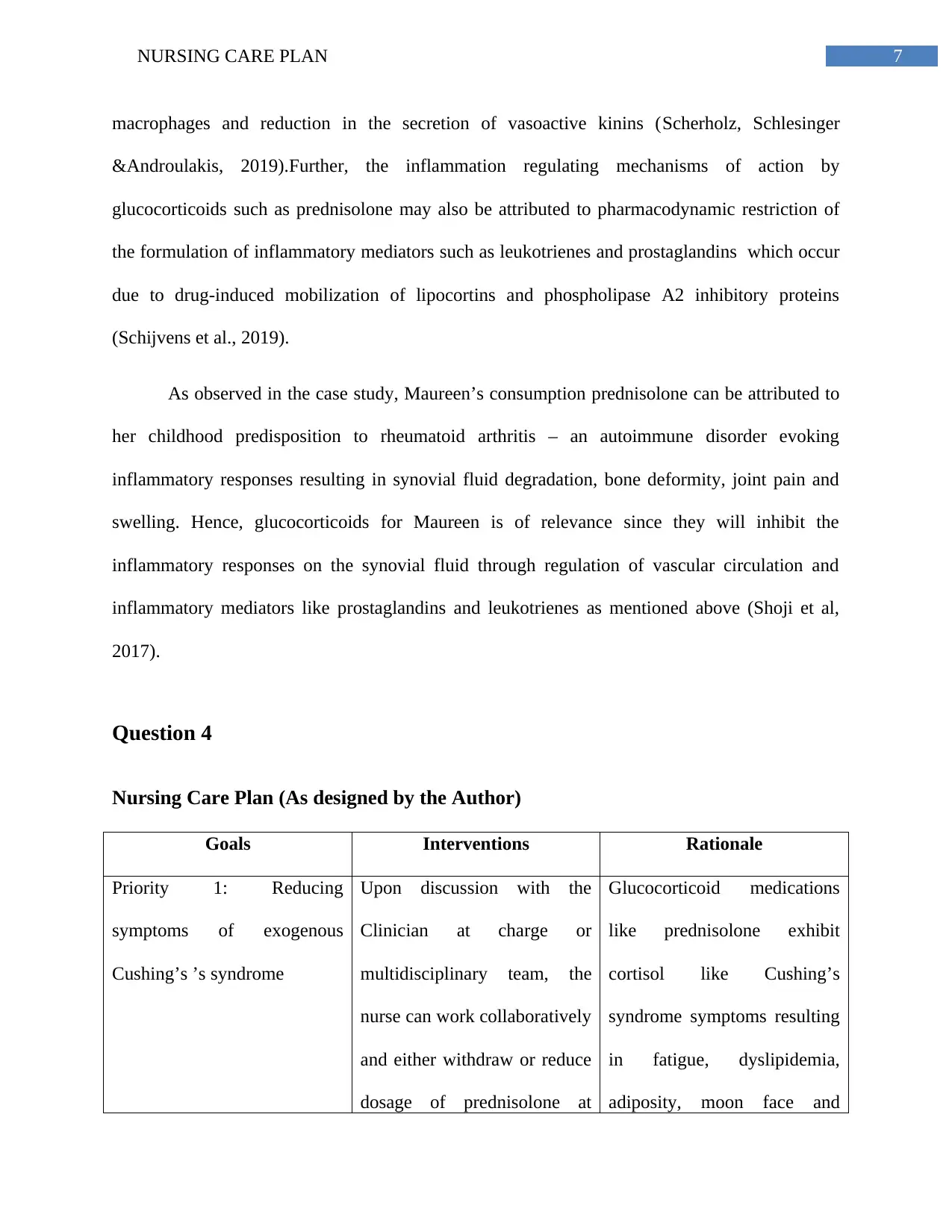
macrophages and reduction in the secretion of vasoactive kinins (Scherholz, Schlesinger
&Androulakis, 2019).Further, the inflammation regulating mechanisms of action by
glucocorticoids such as prednisolone may also be attributed to pharmacodynamic restriction of
the formulation of inflammatory mediators such as leukotrienes and prostaglandins which occur
due to drug-induced mobilization of lipocortins and phospholipase A2 inhibitory proteins
(Schijvens et al., 2019).
As observed in the case study, Maureen’s consumption prednisolone can be attributed to
her childhood predisposition to rheumatoid arthritis – an autoimmune disorder evoking
inflammatory responses resulting in synovial fluid degradation, bone deformity, joint pain and
swelling. Hence, glucocorticoids for Maureen is of relevance since they will inhibit the
inflammatory responses on the synovial fluid through regulation of vascular circulation and
inflammatory mediators like prostaglandins and leukotrienes as mentioned above (Shoji et al,
2017).
Question 4
Nursing Care Plan (As designed by the Author)
Goals Interventions Rationale
Priority 1: Reducing
symptoms of exogenous
Cushing’s ’s syndrome
Upon discussion with the
Clinician at charge or
multidisciplinary team, the
nurse can work collaboratively
and either withdraw or reduce
dosage of prednisolone at
Glucocorticoid medications
like prednisolone exhibit
cortisol like Cushing’s
syndrome symptoms resulting
in fatigue, dyslipidemia,
adiposity, moon face and
macrophages and reduction in the secretion of vasoactive kinins (Scherholz, Schlesinger
&Androulakis, 2019).Further, the inflammation regulating mechanisms of action by
glucocorticoids such as prednisolone may also be attributed to pharmacodynamic restriction of
the formulation of inflammatory mediators such as leukotrienes and prostaglandins which occur
due to drug-induced mobilization of lipocortins and phospholipase A2 inhibitory proteins
(Schijvens et al., 2019).
As observed in the case study, Maureen’s consumption prednisolone can be attributed to
her childhood predisposition to rheumatoid arthritis – an autoimmune disorder evoking
inflammatory responses resulting in synovial fluid degradation, bone deformity, joint pain and
swelling. Hence, glucocorticoids for Maureen is of relevance since they will inhibit the
inflammatory responses on the synovial fluid through regulation of vascular circulation and
inflammatory mediators like prostaglandins and leukotrienes as mentioned above (Shoji et al,
2017).
Question 4
Nursing Care Plan (As designed by the Author)
Goals Interventions Rationale
Priority 1: Reducing
symptoms of exogenous
Cushing’s ’s syndrome
Upon discussion with the
Clinician at charge or
multidisciplinary team, the
nurse can work collaboratively
and either withdraw or reduce
dosage of prednisolone at
Glucocorticoid medications
like prednisolone exhibit
cortisol like Cushing’s
syndrome symptoms resulting
in fatigue, dyslipidemia,
adiposity, moon face and
8NURSING CARE PLAN
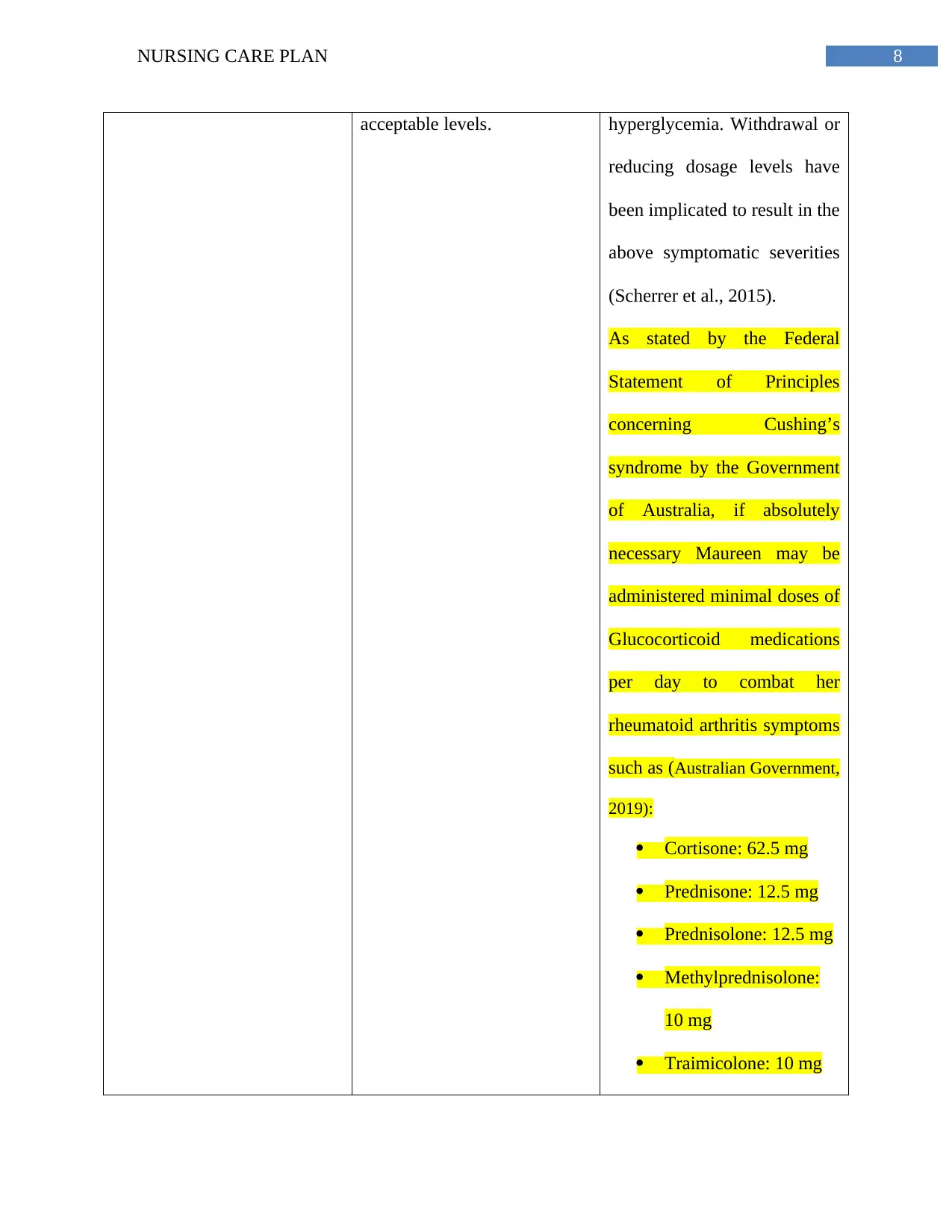
acceptable levels. hyperglycemia. Withdrawal or
reducing dosage levels have
been implicated to result in the
above symptomatic severities
(Scherrer et al., 2015).
As stated by the Federal
Statement of Principles
concerning Cushing’s
syndrome by the Government
of Australia, if absolutely
necessary Maureen may be
administered minimal doses of
Glucocorticoid medications
per day to combat her
rheumatoid arthritis symptoms
such as (Australian Government,
2019):
Cortisone: 62.5 mg
Prednisone: 12.5 mg
Prednisolone: 12.5 mg
Methylprednisolone:
10 mg
Traimicolone: 10 mg
acceptable levels. hyperglycemia. Withdrawal or
reducing dosage levels have
been implicated to result in the
above symptomatic severities
(Scherrer et al., 2015).
As stated by the Federal
Statement of Principles
concerning Cushing’s
syndrome by the Government
of Australia, if absolutely
necessary Maureen may be
administered minimal doses of
Glucocorticoid medications
per day to combat her
rheumatoid arthritis symptoms
such as (Australian Government,
2019):
Cortisone: 62.5 mg
Prednisone: 12.5 mg
Prednisolone: 12.5 mg
Methylprednisolone:
10 mg
Traimicolone: 10 mg
9NURSING CARE PLAN
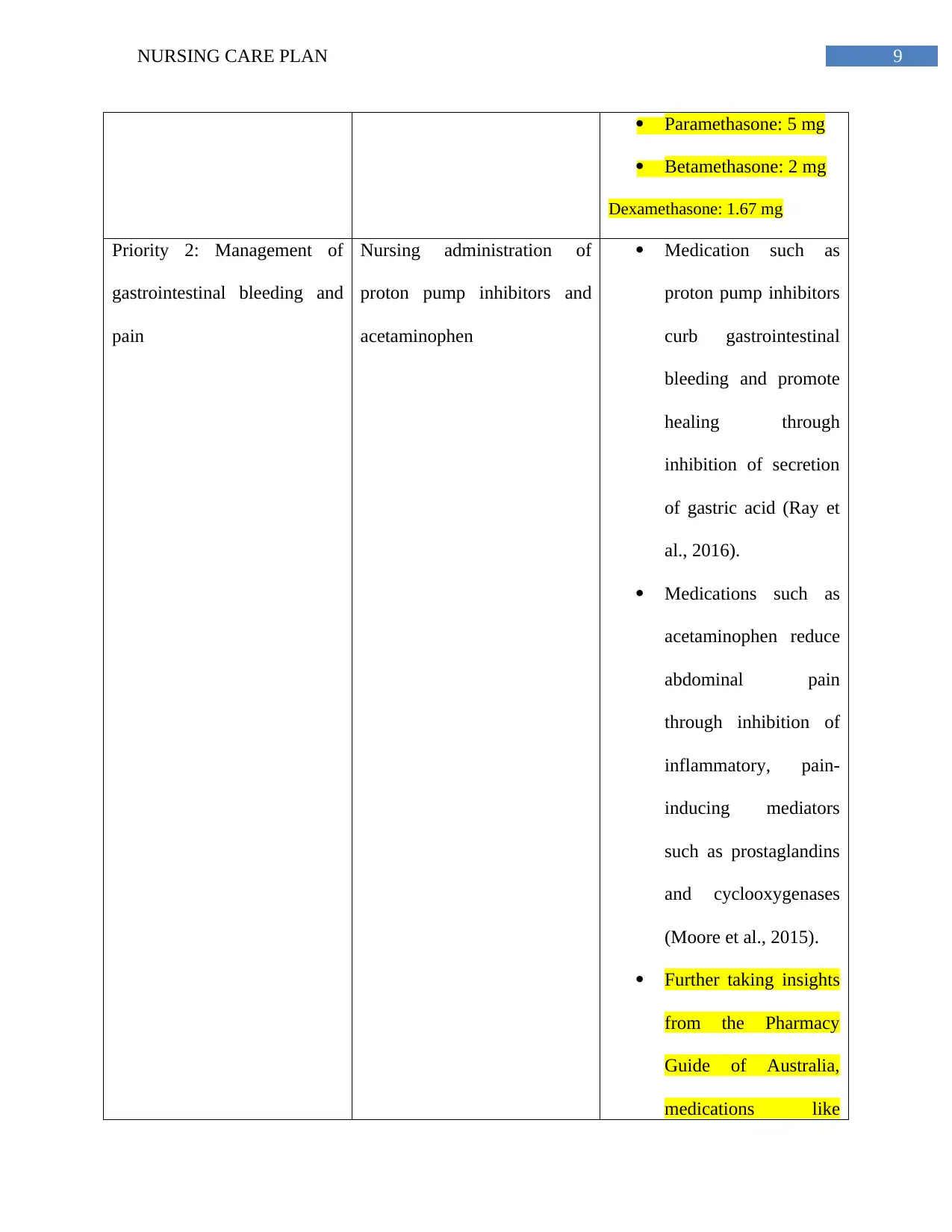
Paramethasone: 5 mg
Betamethasone: 2 mg
Dexamethasone: 1.67 mg
Priority 2: Management of
gastrointestinal bleeding and
pain
Nursing administration of
proton pump inhibitors and
acetaminophen
Medication such as
proton pump inhibitors
curb gastrointestinal
bleeding and promote
healing through
inhibition of secretion
of gastric acid (Ray et
al., 2016).
Medications such as
acetaminophen reduce
abdominal pain
through inhibition of
inflammatory, pain-
inducing mediators
such as prostaglandins
and cyclooxygenases
(Moore et al., 2015).
Further taking insights
from the Pharmacy
Guide of Australia,
medications like
Paramethasone: 5 mg
Betamethasone: 2 mg
Dexamethasone: 1.67 mg
Priority 2: Management of
gastrointestinal bleeding and
pain
Nursing administration of
proton pump inhibitors and
acetaminophen
Medication such as
proton pump inhibitors
curb gastrointestinal
bleeding and promote
healing through
inhibition of secretion
of gastric acid (Ray et
al., 2016).
Medications such as
acetaminophen reduce
abdominal pain
through inhibition of
inflammatory, pain-
inducing mediators
such as prostaglandins
and cyclooxygenases
(Moore et al., 2015).
Further taking insights
from the Pharmacy
Guide of Australia,
medications like
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10NURSING CARE PLAN
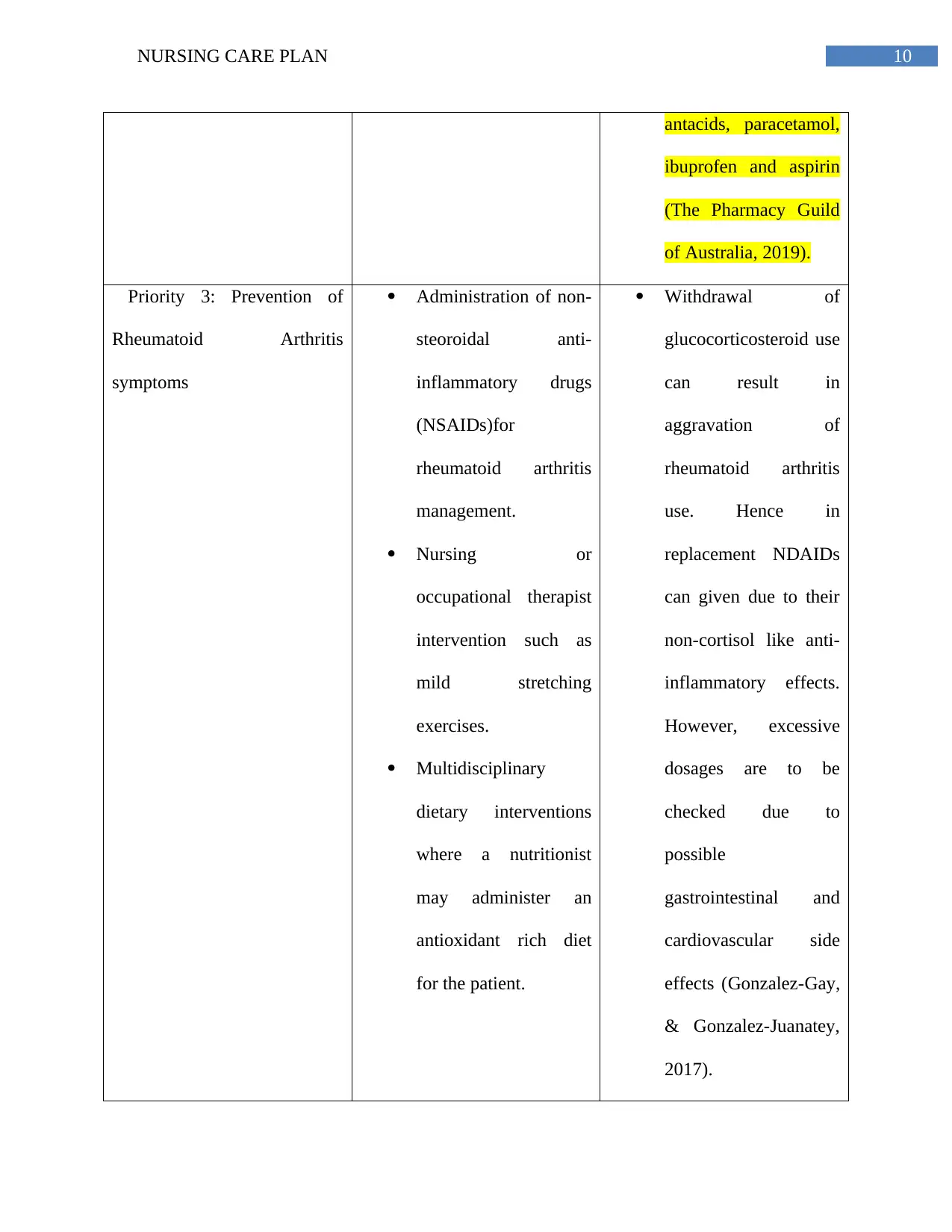
antacids, paracetamol,
ibuprofen and aspirin
(The Pharmacy Guild
of Australia, 2019).
Priority 3: Prevention of
Rheumatoid Arthritis
symptoms
Administration of non-
steoroidal anti-
inflammatory drugs
(NSAIDs)for
rheumatoid arthritis
management.
Nursing or
occupational therapist
intervention such as
mild stretching
exercises.
Multidisciplinary
dietary interventions
where a nutritionist
may administer an
antioxidant rich diet
for the patient.
Withdrawal of
glucocorticosteroid use
can result in
aggravation of
rheumatoid arthritis
use. Hence in
replacement NDAIDs
can given due to their
non-cortisol like anti-
inflammatory effects.
However, excessive
dosages are to be
checked due to
possible
gastrointestinal and
cardiovascular side
effects (Gonzalez-Gay,
& Gonzalez-Juanatey,
2017).
antacids, paracetamol,
ibuprofen and aspirin
(The Pharmacy Guild
of Australia, 2019).
Priority 3: Prevention of
Rheumatoid Arthritis
symptoms
Administration of non-
steoroidal anti-
inflammatory drugs
(NSAIDs)for
rheumatoid arthritis
management.
Nursing or
occupational therapist
intervention such as
mild stretching
exercises.
Multidisciplinary
dietary interventions
where a nutritionist
may administer an
antioxidant rich diet
for the patient.
Withdrawal of
glucocorticosteroid use
can result in
aggravation of
rheumatoid arthritis
use. Hence in
replacement NDAIDs
can given due to their
non-cortisol like anti-
inflammatory effects.
However, excessive
dosages are to be
checked due to
possible
gastrointestinal and
cardiovascular side
effects (Gonzalez-Gay,
& Gonzalez-Juanatey,
2017).
11NURSING CARE PLAN
Stretching aids in
enhancement of blood
circulation and
provision of relief
from joint pain and
swelling (Williams et
al., 2015).
An antioxidant rich
diet may help combat
the inflammatory
effects of rheumatoid
arthritis (Hu et al.,
2015).
As per the National
Prescribing Service
(NPS), medications
like methotrexate,
sulfasaline and
lefunomide may be
beneficial which
decrease progression
of disease through
inhibition of DNA
Stretching aids in
enhancement of blood
circulation and
provision of relief
from joint pain and
swelling (Williams et
al., 2015).
An antioxidant rich
diet may help combat
the inflammatory
effects of rheumatoid
arthritis (Hu et al.,
2015).
As per the National
Prescribing Service
(NPS), medications
like methotrexate,
sulfasaline and
lefunomide may be
beneficial which
decrease progression
of disease through
inhibition of DNA
12NURSING CARE PLAN
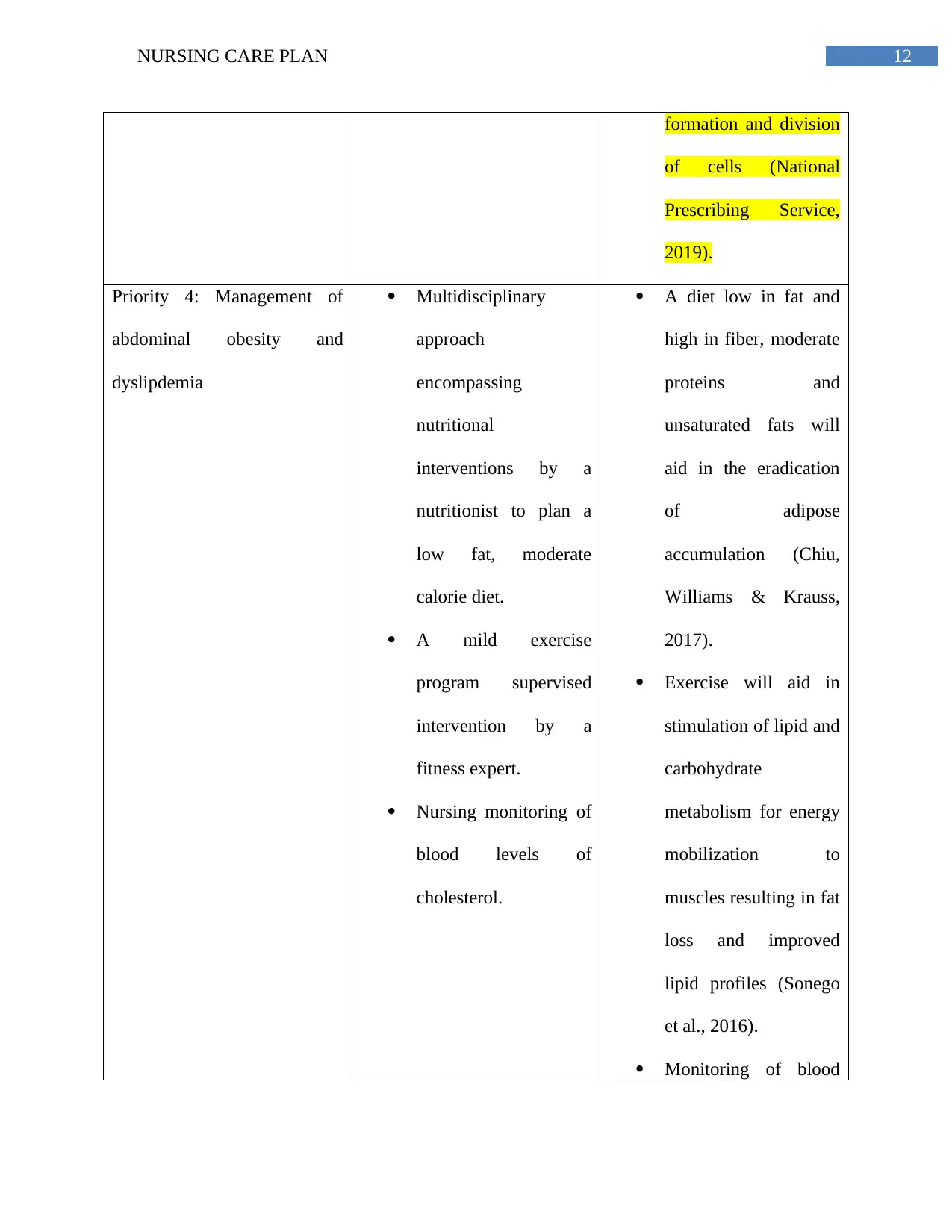
formation and division
of cells (National
Prescribing Service,
2019).
Priority 4: Management of
abdominal obesity and
dyslipdemia
Multidisciplinary
approach
encompassing
nutritional
interventions by a
nutritionist to plan a
low fat, moderate
calorie diet.
A mild exercise
program supervised
intervention by a
fitness expert.
Nursing monitoring of
blood levels of
cholesterol.
A diet low in fat and
high in fiber, moderate
proteins and
unsaturated fats will
aid in the eradication
of adipose
accumulation (Chiu,
Williams & Krauss,
2017).
Exercise will aid in
stimulation of lipid and
carbohydrate
metabolism for energy
mobilization to
muscles resulting in fat
loss and improved
lipid profiles (Sonego
et al., 2016).
Monitoring of blood
formation and division
of cells (National
Prescribing Service,
2019).
Priority 4: Management of
abdominal obesity and
dyslipdemia
Multidisciplinary
approach
encompassing
nutritional
interventions by a
nutritionist to plan a
low fat, moderate
calorie diet.
A mild exercise
program supervised
intervention by a
fitness expert.
Nursing monitoring of
blood levels of
cholesterol.
A diet low in fat and
high in fiber, moderate
proteins and
unsaturated fats will
aid in the eradication
of adipose
accumulation (Chiu,
Williams & Krauss,
2017).
Exercise will aid in
stimulation of lipid and
carbohydrate
metabolism for energy
mobilization to
muscles resulting in fat
loss and improved
lipid profiles (Sonego
et al., 2016).
Monitoring of blood
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
13NURSING CARE PLAN
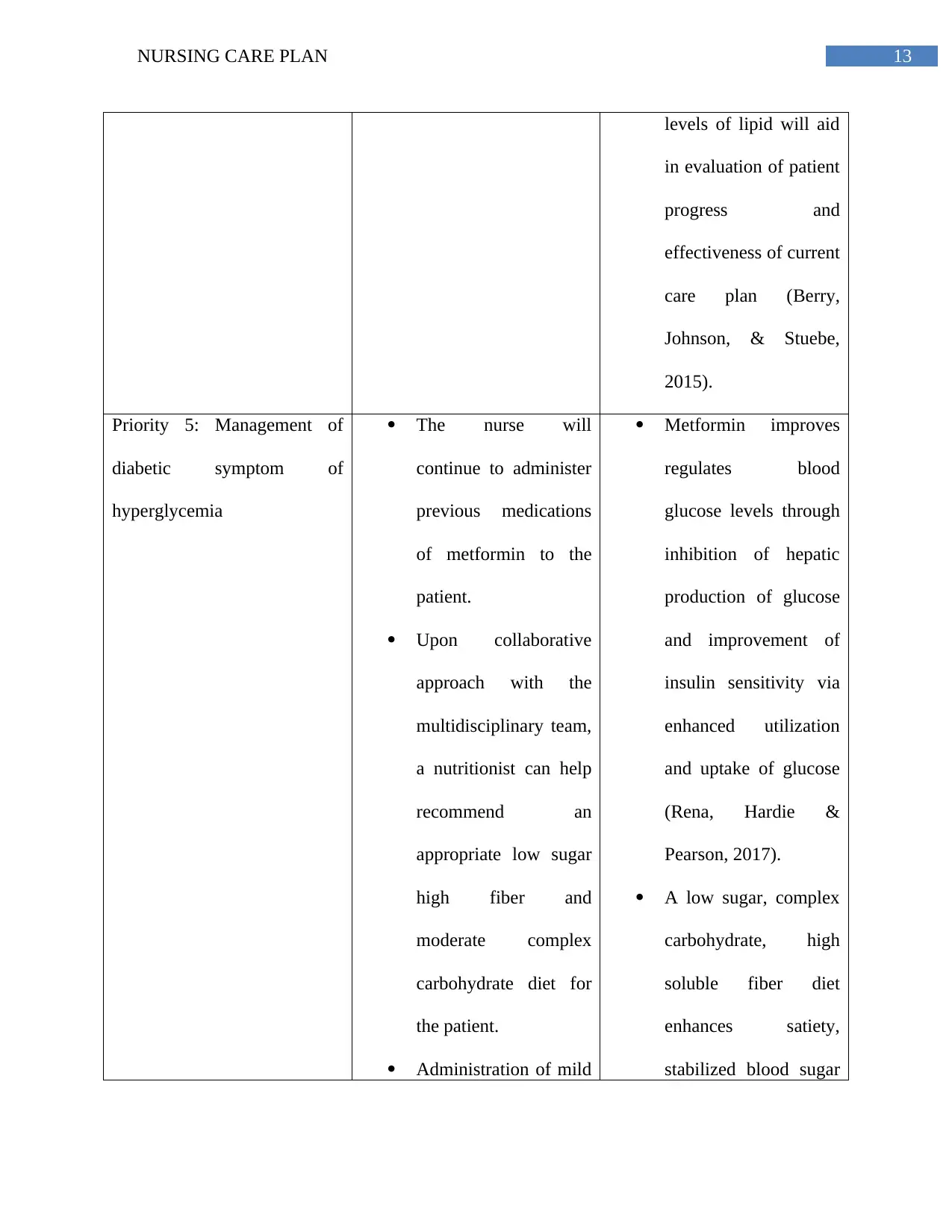
levels of lipid will aid
in evaluation of patient
progress and
effectiveness of current
care plan (Berry,
Johnson, & Stuebe,
2015).
Priority 5: Management of
diabetic symptom of
hyperglycemia
The nurse will
continue to administer
previous medications
of metformin to the
patient.
Upon collaborative
approach with the
multidisciplinary team,
a nutritionist can help
recommend an
appropriate low sugar
high fiber and
moderate complex
carbohydrate diet for
the patient.
Administration of mild
Metformin improves
regulates blood
glucose levels through
inhibition of hepatic
production of glucose
and improvement of
insulin sensitivity via
enhanced utilization
and uptake of glucose
(Rena, Hardie &
Pearson, 2017).
A low sugar, complex
carbohydrate, high
soluble fiber diet
enhances satiety,
stabilized blood sugar
levels of lipid will aid
in evaluation of patient
progress and
effectiveness of current
care plan (Berry,
Johnson, & Stuebe,
2015).
Priority 5: Management of
diabetic symptom of
hyperglycemia
The nurse will
continue to administer
previous medications
of metformin to the
patient.
Upon collaborative
approach with the
multidisciplinary team,
a nutritionist can help
recommend an
appropriate low sugar
high fiber and
moderate complex
carbohydrate diet for
the patient.
Administration of mild
Metformin improves
regulates blood
glucose levels through
inhibition of hepatic
production of glucose
and improvement of
insulin sensitivity via
enhanced utilization
and uptake of glucose
(Rena, Hardie &
Pearson, 2017).
A low sugar, complex
carbohydrate, high
soluble fiber diet
enhances satiety,
stabilized blood sugar
14NURSING CARE PLAN
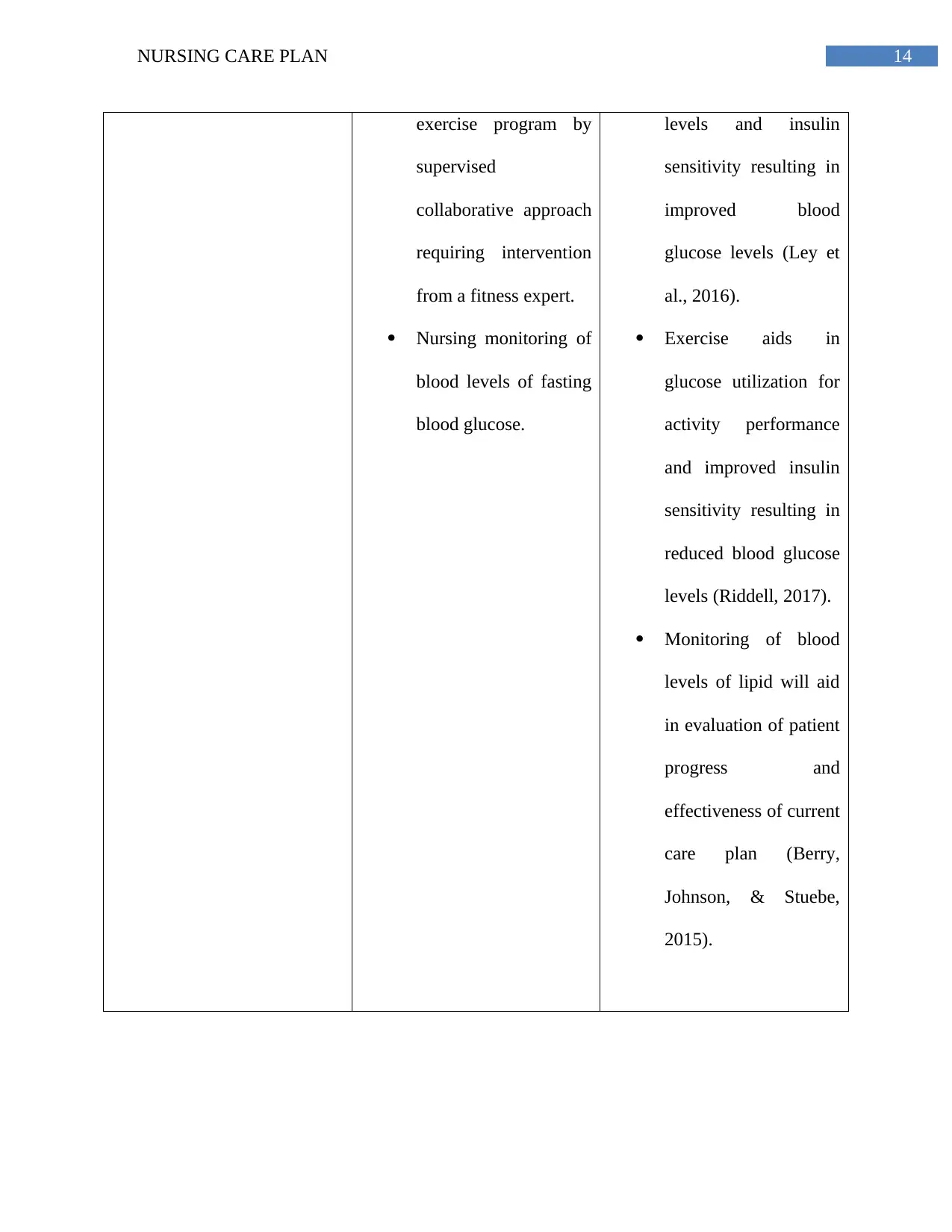
exercise program by
supervised
collaborative approach
requiring intervention
from a fitness expert.
Nursing monitoring of
blood levels of fasting
blood glucose.
levels and insulin
sensitivity resulting in
improved blood
glucose levels (Ley et
al., 2016).
Exercise aids in
glucose utilization for
activity performance
and improved insulin
sensitivity resulting in
reduced blood glucose
levels (Riddell, 2017).
Monitoring of blood
levels of lipid will aid
in evaluation of patient
progress and
effectiveness of current
care plan (Berry,
Johnson, & Stuebe,
2015).
exercise program by
supervised
collaborative approach
requiring intervention
from a fitness expert.
Nursing monitoring of
blood levels of fasting
blood glucose.
levels and insulin
sensitivity resulting in
improved blood
glucose levels (Ley et
al., 2016).
Exercise aids in
glucose utilization for
activity performance
and improved insulin
sensitivity resulting in
reduced blood glucose
levels (Riddell, 2017).
Monitoring of blood
levels of lipid will aid
in evaluation of patient
progress and
effectiveness of current
care plan (Berry,
Johnson, & Stuebe,
2015).
15NURSING CARE PLAN
References
Al-Ali, A. O., Jafaari, S. A., Alhazmi, A. A., Abdulrazzaque, M., & Al Jurayyan, N. A. (2016).
Iatrogenic Cushing’s Syndrome Due to Misuse of Topical Steroids. International Journal
of Health Sciences and Research (IJHSR), 6(7), 403-5.
Assié, G. (2018). Genomic insights into Cushing syndrome. In Annals of Endocrinology, 79(3),
119-122.
Australian Government. (2019). Statement of Principles concerning Cushing's syndrome No. 34
of 2009. Retrieved from https://www.legislation.gov.au/Details/F2009L01601.
Berry, D. C., Johnson, Q. B., & Stuebe, A. M. (2015). Monitoring and managing mothers with
gestational diabetes mellitus: a nursing perspective. Nursing: Research and Reviews, 20,
91-97.
Bunte, K., Smith, D. J., Chappell, M. J., Hassan-Smith, Z. K., Tomlinson, J. W., Arlt, W., &
Tiňo, P. (2018). Learning pharmacokinetic models for in vivo glucocorticoid activation.
Journal of theoretical biology, 455, 222-231.
Chiu, S., Williams, P. T., & Krauss, R. M. (2017). Effects of a very high saturated fat diet on
LDL particles in adults with atherogenic dyslipidemia: A randomized controlled trial.
PloS one, 12(2), e0170664.
de Heide, L. J., de Boer, H. H., van Borren, M., Emous, M., Aarts, E., & de Boer, H. (2018).
Pharmacokinetics of glucocorticoid replacement before and after bariatric surgery in
patients with adrenal insufficiency. Journal of the Endocrine Society, 2(12), 1338-1344.
References
Al-Ali, A. O., Jafaari, S. A., Alhazmi, A. A., Abdulrazzaque, M., & Al Jurayyan, N. A. (2016).
Iatrogenic Cushing’s Syndrome Due to Misuse of Topical Steroids. International Journal
of Health Sciences and Research (IJHSR), 6(7), 403-5.
Assié, G. (2018). Genomic insights into Cushing syndrome. In Annals of Endocrinology, 79(3),
119-122.
Australian Government. (2019). Statement of Principles concerning Cushing's syndrome No. 34
of 2009. Retrieved from https://www.legislation.gov.au/Details/F2009L01601.
Berry, D. C., Johnson, Q. B., & Stuebe, A. M. (2015). Monitoring and managing mothers with
gestational diabetes mellitus: a nursing perspective. Nursing: Research and Reviews, 20,
91-97.
Bunte, K., Smith, D. J., Chappell, M. J., Hassan-Smith, Z. K., Tomlinson, J. W., Arlt, W., &
Tiňo, P. (2018). Learning pharmacokinetic models for in vivo glucocorticoid activation.
Journal of theoretical biology, 455, 222-231.
Chiu, S., Williams, P. T., & Krauss, R. M. (2017). Effects of a very high saturated fat diet on
LDL particles in adults with atherogenic dyslipidemia: A randomized controlled trial.
PloS one, 12(2), e0170664.
de Heide, L. J., de Boer, H. H., van Borren, M., Emous, M., Aarts, E., & de Boer, H. (2018).
Pharmacokinetics of glucocorticoid replacement before and after bariatric surgery in
patients with adrenal insufficiency. Journal of the Endocrine Society, 2(12), 1338-1344.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
16NURSING CARE PLAN
Dubrocq, G., Estrada, A., Kelly, S., & Rakhmanina, N. (2017). Acute development of Cushing
syndrome in an HIV-infected child on atazanavir/ritonavir based antiretroviral therapy.
Endocrinology, diabetes & metabolism case reports, 2017(1).
Gonzalez-Gay, M. A., & Gonzalez-Juanatey, C. (2017). Inflammation: NSAIDs and
cardiovascular risk in arthritis. Nature Reviews Cardiology, 14(2), 69.
Hosseini, S. H., Maleki, A., Eshraghi, H. R., & Hamidi, M. (2016). Preparation and in
vitro/pharmacokinetic/pharmacodynamic evaluation of a slow-release nano-liposomal
form of prednisolone. Drug delivery, 23(8), 3008-3016.
Hu, Y., Costenbader, K. H., Gao, X., Hu, F. B., Karlson, E. W., & Lu, B. (2015). Mediterranean
diet and incidence of rheumatoid arthritis in women. Arthritis care & research, 67(5),
597-606.
Isidori, A. M., Graziadio, C., Paragliola, R. M., Cozzolino, A., Ambrogio, A. G., Colao, A., ... &
Pivonello, R. (2015). The hypertension of Cushing's syndrome: controversies in the
pathophysiology and focus on cardiovascular complications. Journal of hypertension,
33(1), 44.
Kang, E., Moon, S. J., ho Moon, K., Han, D. J., Lee, J., Ro, S. M., ... & Yoo, S. J. (2016).
Endogenous Cushing's Syndrome in a Patient with Systemic Lupus Erythematosus.
Korean Journal of Obesity (2383-899X), 25(3).
Lacroix, A., Feelders, R. A., Stratakis, C. A., & Nieman, L. K. (2015). Cushing's syndrome. The
lancet, 386(9996), 913-927.
Dubrocq, G., Estrada, A., Kelly, S., & Rakhmanina, N. (2017). Acute development of Cushing
syndrome in an HIV-infected child on atazanavir/ritonavir based antiretroviral therapy.
Endocrinology, diabetes & metabolism case reports, 2017(1).
Gonzalez-Gay, M. A., & Gonzalez-Juanatey, C. (2017). Inflammation: NSAIDs and
cardiovascular risk in arthritis. Nature Reviews Cardiology, 14(2), 69.
Hosseini, S. H., Maleki, A., Eshraghi, H. R., & Hamidi, M. (2016). Preparation and in
vitro/pharmacokinetic/pharmacodynamic evaluation of a slow-release nano-liposomal
form of prednisolone. Drug delivery, 23(8), 3008-3016.
Hu, Y., Costenbader, K. H., Gao, X., Hu, F. B., Karlson, E. W., & Lu, B. (2015). Mediterranean
diet and incidence of rheumatoid arthritis in women. Arthritis care & research, 67(5),
597-606.
Isidori, A. M., Graziadio, C., Paragliola, R. M., Cozzolino, A., Ambrogio, A. G., Colao, A., ... &
Pivonello, R. (2015). The hypertension of Cushing's syndrome: controversies in the
pathophysiology and focus on cardiovascular complications. Journal of hypertension,
33(1), 44.
Kang, E., Moon, S. J., ho Moon, K., Han, D. J., Lee, J., Ro, S. M., ... & Yoo, S. J. (2016).
Endogenous Cushing's Syndrome in a Patient with Systemic Lupus Erythematosus.
Korean Journal of Obesity (2383-899X), 25(3).
Lacroix, A., Feelders, R. A., Stratakis, C. A., & Nieman, L. K. (2015). Cushing's syndrome. The
lancet, 386(9996), 913-927.
17NURSING CARE PLAN
Ley, S. H., Ardisson Korat, A. V., Sun, Q., Tobias, D. K., Zhang, C., Qi, L., ... & Hu, F. B.
(2016). Contribution of the Nurses’ Health Studies to uncovering risk factors for type 2
diabetes: diet, lifestyle, biomarkers, and genetics. American journal of public health,
106(9), 1624-1630.
Loriaux, D. L. (2017). Diagnosis and differential diagnosis of Cushing’s syndrome. New
England Journal of Medicine, 376(15), 1451-1459.
Moore, R. A., Derry, S., Wiffen, P. J., Straube, S., & Aldington, D. J. (2015). Overview review:
Comparative efficacy of oral ibuprofen and paracetamol (acetaminophen) across acute
and chronic pain conditions. European Journal of Pain, 19(9), 1213-1223.
Morgan, S. A., Hassan-Smith, Z. K., & Lavery, G. G. (2016). Mechanisms in endocrinology:
tissue-specific activation of cortisol in Cushing’s syndrome. European journal of
endocrinology, 175(2), R81-R87.
National Prescribing Service. (2019). Disease modifying drugs in adult rheumatoid arthritis.
Retrieved from https://www.nps.org.au/australian-prescriber/articles/disease-modifying-
drugs-in-adult-rheumatoid-arthritis.
Nieman, L. K. (2018). Recent Updates on the Diagnosis and Management of Cushing's
Syndrome. Endocrinology and Metabolism, 33(2), 139-146.
O'brien, K. F., DeKlotz, C. M. C., & Silverman, R. A. (2018). Exogenous Cushing syndrome
from an unexpected source of systemic steroids. Pediatric dermatology, 35(3), e196-
e197.
Ley, S. H., Ardisson Korat, A. V., Sun, Q., Tobias, D. K., Zhang, C., Qi, L., ... & Hu, F. B.
(2016). Contribution of the Nurses’ Health Studies to uncovering risk factors for type 2
diabetes: diet, lifestyle, biomarkers, and genetics. American journal of public health,
106(9), 1624-1630.
Loriaux, D. L. (2017). Diagnosis and differential diagnosis of Cushing’s syndrome. New
England Journal of Medicine, 376(15), 1451-1459.
Moore, R. A., Derry, S., Wiffen, P. J., Straube, S., & Aldington, D. J. (2015). Overview review:
Comparative efficacy of oral ibuprofen and paracetamol (acetaminophen) across acute
and chronic pain conditions. European Journal of Pain, 19(9), 1213-1223.
Morgan, S. A., Hassan-Smith, Z. K., & Lavery, G. G. (2016). Mechanisms in endocrinology:
tissue-specific activation of cortisol in Cushing’s syndrome. European journal of
endocrinology, 175(2), R81-R87.
National Prescribing Service. (2019). Disease modifying drugs in adult rheumatoid arthritis.
Retrieved from https://www.nps.org.au/australian-prescriber/articles/disease-modifying-
drugs-in-adult-rheumatoid-arthritis.
Nieman, L. K. (2018). Recent Updates on the Diagnosis and Management of Cushing's
Syndrome. Endocrinology and Metabolism, 33(2), 139-146.
O'brien, K. F., DeKlotz, C. M. C., & Silverman, R. A. (2018). Exogenous Cushing syndrome
from an unexpected source of systemic steroids. Pediatric dermatology, 35(3), e196-
e197.
18NURSING CARE PLAN
Özgüç Çömlek, F., Örüm, S., Aydın, S., & Tütüncüler, F. (2018). Exogenous Cushing syndrome
due to misuse of potent topical steroid. Pediatric dermatology, 35(2), e121-e123.
Pappachan, J. M., Hariman, C., Edavalath, M., Waldron, J., & Hanna, F. W. (2017). Cushing's
syndrome: a practical approach to diagnosis and differential diagnoses. Journal of
clinical pathology, 70(4), 350-359.
Paul, E. M., Jose, S., Achar, Y., & Raghunath, B. D. (2016). Prednisolone Induced Cushing
Syndrome: A Case Report. Indian Journal of Pharmacy Practice, 9(2), 141.
Pereira, M. T., Ferreira, L., Horta, A. A., & de Carvalho, A. C. (2016). Exogenous Cushing's
syndrome as a result of ritonavir–budesonide interaction–A case report. HIV & AIDS
Review, 15(2), 91-93.
Pineyro, M. M., Redes, L., De Matoos, S., Sanchez, L., Brignardello, E., Bianchi, V., ... & Viola,
M. (2019). Factitious Cushing’s Syndrome: A Diagnosis to Consider when Evaluating
Hypercortisolism. Frontiers in Endocrinology, 10, 129.
Radhakutty, A., Mangelsdorf, B. L., Drake, S. M., Samocha‐Bonet, D., Heilbronn, L. K., Smith,
M. D., ... & Burt, M. G. (2016). Effects of prednisolone on energy and fat metabolism in
patients with rheumatoid arthritis: tissue‐specific insulin resistance with commonly used
prednisolone doses. Clinical endocrinology, 85(5), 741-747.
Raff, H., & Carroll, T. (2015). Cushing's syndrome: from physiological principles to diagnosis
and clinical care. The Journal of physiology, 593(3), 493-506.
Özgüç Çömlek, F., Örüm, S., Aydın, S., & Tütüncüler, F. (2018). Exogenous Cushing syndrome
due to misuse of potent topical steroid. Pediatric dermatology, 35(2), e121-e123.
Pappachan, J. M., Hariman, C., Edavalath, M., Waldron, J., & Hanna, F. W. (2017). Cushing's
syndrome: a practical approach to diagnosis and differential diagnoses. Journal of
clinical pathology, 70(4), 350-359.
Paul, E. M., Jose, S., Achar, Y., & Raghunath, B. D. (2016). Prednisolone Induced Cushing
Syndrome: A Case Report. Indian Journal of Pharmacy Practice, 9(2), 141.
Pereira, M. T., Ferreira, L., Horta, A. A., & de Carvalho, A. C. (2016). Exogenous Cushing's
syndrome as a result of ritonavir–budesonide interaction–A case report. HIV & AIDS
Review, 15(2), 91-93.
Pineyro, M. M., Redes, L., De Matoos, S., Sanchez, L., Brignardello, E., Bianchi, V., ... & Viola,
M. (2019). Factitious Cushing’s Syndrome: A Diagnosis to Consider when Evaluating
Hypercortisolism. Frontiers in Endocrinology, 10, 129.
Radhakutty, A., Mangelsdorf, B. L., Drake, S. M., Samocha‐Bonet, D., Heilbronn, L. K., Smith,
M. D., ... & Burt, M. G. (2016). Effects of prednisolone on energy and fat metabolism in
patients with rheumatoid arthritis: tissue‐specific insulin resistance with commonly used
prednisolone doses. Clinical endocrinology, 85(5), 741-747.
Raff, H., & Carroll, T. (2015). Cushing's syndrome: from physiological principles to diagnosis
and clinical care. The Journal of physiology, 593(3), 493-506.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
19NURSING CARE PLAN
Ray, W. A., Chung, C. P., Murray, K. T., Smalley, W. E., Daugherty, J. R., Dupont, W. D., &
Stein, C. M. (2016). Association of proton pump inhibitors with reduced risk of warfarin-
related serious upper gastrointestinal bleeding. Gastroenterology, 151(6), 1105-1112.
Rena, G., Hardie, D. G., & Pearson, E. R. (2017). The mechanisms of action of metformin.
Diabetologia, 60(9), 1577-1585.
Riddell, M. C., Gallen, I. W., Smart, C. E., Taplin, C. E., Adolfsson, P., Lumb, A. N., ... &
Annan, F. (2017). Exercise management in type 1 diabetes: a consensus statement. The
lancet Diabetes & endocrinology, 5(5), 377-390.
Scherholz, M. L., Schlesinger, N., & Androulakis, I. P. (2019). Chronopharmacology of
glucocorticoids. Advanced drug delivery reviews.
Scherrer, K. S., Weitz, M., Eisenack, J., Truffer, B., & Konrad, D. (2015). Cushing syndrome
after bilateral lensectomy. European journal of pediatrics, 174(3), 399-401.
Schijvens, A. M., ter Heine, R., de Wildt, S. N., & Schreuder, M. F. (2019). Pharmacology and
pharmacogenetics of prednisone and prednisolone in patients with nephrotic syndrome.
Pediatric Nephrology, 34(3), 389-403.
Sharma, S. T., Nieman, L. K., & Feelders, R. A. (2015). Cushing’s syndrome: epidemiology and
developments in disease management. Clinical epidemiology, 7, 281.
Shoji, S., Suzuki, A., Conrado, D. J., Peterson, M. C., Hey‐Hadavi, J., McCabe, D., ... &
Tammara, B. K. (2017). Dissociated agonist of glucocorticoid receptor or prednisone for
active rheumatoid arthritis: effects on P1NP and osteocalcin pharmacodynamics. CPT:
pharmacometrics & systems pharmacology, 6(7), 439-448.
Ray, W. A., Chung, C. P., Murray, K. T., Smalley, W. E., Daugherty, J. R., Dupont, W. D., &
Stein, C. M. (2016). Association of proton pump inhibitors with reduced risk of warfarin-
related serious upper gastrointestinal bleeding. Gastroenterology, 151(6), 1105-1112.
Rena, G., Hardie, D. G., & Pearson, E. R. (2017). The mechanisms of action of metformin.
Diabetologia, 60(9), 1577-1585.
Riddell, M. C., Gallen, I. W., Smart, C. E., Taplin, C. E., Adolfsson, P., Lumb, A. N., ... &
Annan, F. (2017). Exercise management in type 1 diabetes: a consensus statement. The
lancet Diabetes & endocrinology, 5(5), 377-390.
Scherholz, M. L., Schlesinger, N., & Androulakis, I. P. (2019). Chronopharmacology of
glucocorticoids. Advanced drug delivery reviews.
Scherrer, K. S., Weitz, M., Eisenack, J., Truffer, B., & Konrad, D. (2015). Cushing syndrome
after bilateral lensectomy. European journal of pediatrics, 174(3), 399-401.
Schijvens, A. M., ter Heine, R., de Wildt, S. N., & Schreuder, M. F. (2019). Pharmacology and
pharmacogenetics of prednisone and prednisolone in patients with nephrotic syndrome.
Pediatric Nephrology, 34(3), 389-403.
Sharma, S. T., Nieman, L. K., & Feelders, R. A. (2015). Cushing’s syndrome: epidemiology and
developments in disease management. Clinical epidemiology, 7, 281.
Shoji, S., Suzuki, A., Conrado, D. J., Peterson, M. C., Hey‐Hadavi, J., McCabe, D., ... &
Tammara, B. K. (2017). Dissociated agonist of glucocorticoid receptor or prednisone for
active rheumatoid arthritis: effects on P1NP and osteocalcin pharmacodynamics. CPT:
pharmacometrics & systems pharmacology, 6(7), 439-448.
20NURSING CARE PLAN
Sonego, M., Sagrado, M. J., Escobar, G., Lazzerini, M., Rivas, E., Martín-Cañavate, R., ... &
Custodio, E. (2016). Dyslipidemia, diet and physical exercise in children on treatment
with antiretroviral medication in El Salvador: a cross-sectional study. The Pediatric
infectious disease journal, 35(10), 1111.
The Pharmacy Guild of Australia. (2019). Pain relievers (also known as painkillers or
analgesics). Retrieved from
https://www.guild.org.au/__data/assets/pdf_file/0028/48880/Self-Care-Fact-Cards.pdf.
Torres, S. J., Grimes, C., Nowson, C. A., Jayasinghe, S. U., Bruce, C. R., Mason, S. A., ... &
Turner, A. I. (2019). Urinary sodium is positively associated with urinary free cortisol
and total cortisol metabolites in a cross-sectional sample of Australian schoolchildren
aged 5–12 years and their mothers. British Journal of Nutrition, 121(2), 164-171.
Wagner-Bartak, N. A., Baiomy, A., Habra, M. A., Mukhi, S. V., Morani, A. C., Korivi, B. R., ...
& Elsayes, K. M. (2017). Cushing syndrome: diagnostic workup and imaging features,
with clinical and pathologic correlation. American Journal of Roentgenology, 209(1), 19-
32.
Williams, M. A., Williamson, E. M., Heine, P. J., Nichols, V., Glover, M. J., Dritsaki, M., ... &
McConkey, C. (2015). Strengthening And stretching for Rheumatoid Arthritis of the
Hand (SARAH). A randomised controlled trial and economic evaluation.
Sonego, M., Sagrado, M. J., Escobar, G., Lazzerini, M., Rivas, E., Martín-Cañavate, R., ... &
Custodio, E. (2016). Dyslipidemia, diet and physical exercise in children on treatment
with antiretroviral medication in El Salvador: a cross-sectional study. The Pediatric
infectious disease journal, 35(10), 1111.
The Pharmacy Guild of Australia. (2019). Pain relievers (also known as painkillers or
analgesics). Retrieved from
https://www.guild.org.au/__data/assets/pdf_file/0028/48880/Self-Care-Fact-Cards.pdf.
Torres, S. J., Grimes, C., Nowson, C. A., Jayasinghe, S. U., Bruce, C. R., Mason, S. A., ... &
Turner, A. I. (2019). Urinary sodium is positively associated with urinary free cortisol
and total cortisol metabolites in a cross-sectional sample of Australian schoolchildren
aged 5–12 years and their mothers. British Journal of Nutrition, 121(2), 164-171.
Wagner-Bartak, N. A., Baiomy, A., Habra, M. A., Mukhi, S. V., Morani, A. C., Korivi, B. R., ...
& Elsayes, K. M. (2017). Cushing syndrome: diagnostic workup and imaging features,
with clinical and pathologic correlation. American Journal of Roentgenology, 209(1), 19-
32.
Williams, M. A., Williamson, E. M., Heine, P. J., Nichols, V., Glover, M. J., Dritsaki, M., ... &
McConkey, C. (2015). Strengthening And stretching for Rheumatoid Arthritis of the
Hand (SARAH). A randomised controlled trial and economic evaluation.
21NURSING CARE PLAN
1 out of 22
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.