Nursing Case Study: Exogenous Cushing's Syndrome
VerifiedAdded on 2023/04/17
|20
|3053
|174
AI Summary
This nursing case study explores the causes, symptoms, and management of exogenous Cushing's syndrome. Learn about the impact of glucocorticoid medications and the interdisciplinary approach to treatment.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: NURSING CASE STUDY
NURSING CASE STUDY
Name of the Student:
Name of the University:
Author note:
NURSING CASE STUDY
Name of the Student:
Name of the University:
Author note:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

1NURSING CASE STUDY
Question 1
Disease
Maureen is suffering ‘Exogenous Cushing’s syndrome. This disease implies the various
physical and mental alterations that occur due to excessive levels of the hormone cortisol
circulating in the body for a long time period (Wagner-Bartak et al., 2017). Exogenous
Cushing’s syndrome is caused due to external factors, such as consuming large dosages of
glucocorticoids, which further leads to abnormally high levels of cortisol in the blood and hence,
the resultant symptoms as evident in Maureen’s scenario. Maureen has been consuming high
amounts of the medicine prednisolone, a glucocorticoid medication, which can be associated
with her present symptoms (Notay, Fazel & Awasthi, 2019).
Cause
The major cause for exogenous Cushing’s syndrome, is the high intake of glucocorticoid
medications in the body like prednisolone, which results in increased circulating levels of the
hormone, cortisol – which in Maureen’s case is the medicine prednisolone. Glucocorticoids are
prescribed for the mitigation of disease of the autoimmune type, such as lupus, rheumatoid
arthritis, chronic lung diseases, disease of the skin and as well as cancerous tumors (Gottiganti et
al., 2017). Glucocorticoid medicines such as prednisolone as prescribed to Maureen exert
cortisol-like effects in the body such as inducing immune responses, stress regulation through
fight or flight modes, metabolism of macronutrients and regulating of cardiovascular functions
(Scherrer et al., 2015). Despite the therapeutic reasons outlining their prescription, consumption
of glucocorticoids result in circulating levels of cortisol in the blood at levels higher than that of
physiological tolerance. Such an excess leads to health implication such as truncal obesity, face
Question 1
Disease
Maureen is suffering ‘Exogenous Cushing’s syndrome. This disease implies the various
physical and mental alterations that occur due to excessive levels of the hormone cortisol
circulating in the body for a long time period (Wagner-Bartak et al., 2017). Exogenous
Cushing’s syndrome is caused due to external factors, such as consuming large dosages of
glucocorticoids, which further leads to abnormally high levels of cortisol in the blood and hence,
the resultant symptoms as evident in Maureen’s scenario. Maureen has been consuming high
amounts of the medicine prednisolone, a glucocorticoid medication, which can be associated
with her present symptoms (Notay, Fazel & Awasthi, 2019).
Cause
The major cause for exogenous Cushing’s syndrome, is the high intake of glucocorticoid
medications in the body like prednisolone, which results in increased circulating levels of the
hormone, cortisol – which in Maureen’s case is the medicine prednisolone. Glucocorticoids are
prescribed for the mitigation of disease of the autoimmune type, such as lupus, rheumatoid
arthritis, chronic lung diseases, disease of the skin and as well as cancerous tumors (Gottiganti et
al., 2017). Glucocorticoid medicines such as prednisolone as prescribed to Maureen exert
cortisol-like effects in the body such as inducing immune responses, stress regulation through
fight or flight modes, metabolism of macronutrients and regulating of cardiovascular functions
(Scherrer et al., 2015). Despite the therapeutic reasons outlining their prescription, consumption
of glucocorticoids result in circulating levels of cortisol in the blood at levels higher than that of
physiological tolerance. Such an excess leads to health implication such as truncal obesity, face
2NURSING CASE STUDY
rounding or ‘moon shaped’ face, purple striae, fat accumulation in the shoulders and buffalo
hump. The patient also suffers from symptoms like muscles weakness, bone loss, fatigue, weight
gain, hypertension, hyperglycemia, cognitive impairment and abnormally high lipid profiles
(Nieman, 2018).
Exogenous Cushing’s syndrome symptoms can be observed in Maureen through her
symptoms of fatigue, development of a moon face, high levels of LDL cholesterol and adiposity
in her abdominal and truncal regions. Further this disease can result in harmful impacts in
Maureen by further increasing her diabetic conditions like hyperglycemia which will also result
in increased levels of her LDL cholesterol, that is, dyslipidemia, by hindering her fat and
carbohydrate metabolism. This may impact her family with huge medical costs since an inter-
disciplinary approach is necessary to treat Maureen’s multiple disease conditions of Cushing’s
syndrome, rheumatoid arthritis and diabetes (Durrani et al., 2017).
Incidence
Exogenous Cushing’s syndrome is more prevalent in females affecting approximately 8
out of 10 Australian women. Excessive dosages of cortisol-like glucocorticoid medications have
been attributed as the primary cause in approximately 50 to 60% of exogenous Cushing’s
syndrome cases in Australia (Aleksova et al., 2016). High risk populations include individuals
suffering from lymphatic or autoimmune diseases which require glucocorticoid prescription like
prednisone, dexamethasone, prednisolone and methyprednisolone (Manubolu & Nwosu, 2017).
Risk Factor
The major risk factor for exogenous Cushing’s syndrome is the intake of high dosages of
cortisol-like glucocorticoid medicines like prednisolone, as observed in Maureen. The risk
rounding or ‘moon shaped’ face, purple striae, fat accumulation in the shoulders and buffalo
hump. The patient also suffers from symptoms like muscles weakness, bone loss, fatigue, weight
gain, hypertension, hyperglycemia, cognitive impairment and abnormally high lipid profiles
(Nieman, 2018).
Exogenous Cushing’s syndrome symptoms can be observed in Maureen through her
symptoms of fatigue, development of a moon face, high levels of LDL cholesterol and adiposity
in her abdominal and truncal regions. Further this disease can result in harmful impacts in
Maureen by further increasing her diabetic conditions like hyperglycemia which will also result
in increased levels of her LDL cholesterol, that is, dyslipidemia, by hindering her fat and
carbohydrate metabolism. This may impact her family with huge medical costs since an inter-
disciplinary approach is necessary to treat Maureen’s multiple disease conditions of Cushing’s
syndrome, rheumatoid arthritis and diabetes (Durrani et al., 2017).
Incidence
Exogenous Cushing’s syndrome is more prevalent in females affecting approximately 8
out of 10 Australian women. Excessive dosages of cortisol-like glucocorticoid medications have
been attributed as the primary cause in approximately 50 to 60% of exogenous Cushing’s
syndrome cases in Australia (Aleksova et al., 2016). High risk populations include individuals
suffering from lymphatic or autoimmune diseases which require glucocorticoid prescription like
prednisone, dexamethasone, prednisolone and methyprednisolone (Manubolu & Nwosu, 2017).
Risk Factor
The major risk factor for exogenous Cushing’s syndrome is the intake of high dosages of
cortisol-like glucocorticoid medicines like prednisolone, as observed in Maureen. The risk
3NURSING CASE STUDY
factors for the endogenous disease type include, adrenal glandular diseases, familial history,
adenocorticotrophic hormone producing tumors and adenomas in the pituitary (Pivonello et al.,
2016).
Question 2
Pathophysiology of the Disease (tabulated by the Author)
Disease Symptoms Pathology
Symptoms of dyslipidemia such as abdominal
obesity, moon face, subclavicular fat
deposition, buffalo hump
Maureen has been observed to be suffering
from high LDL cholesterol level along with
developing a moon face and gaining fat in her
abdomen as well as between her shoulders.
The steroid hormone cortisol is responsible for
functions like regulating the metabolism of
macronutrients like fats. Cortisol also
mobilizes of energy and nutrients by
metabolizing non-carbohydrate sources like
lipids and fats, by gluconeogenesis processes
for initiating responses of immunity and
inflammation (Sharma, Nieman & Feelders,
(2015). Thus, excessive intake of
glucocorticoid medications (like prednisolone
by Maureen) in exogenous Cushing’s
syndrome leads to uncontrolled
factors for the endogenous disease type include, adrenal glandular diseases, familial history,
adenocorticotrophic hormone producing tumors and adenomas in the pituitary (Pivonello et al.,
2016).
Question 2
Pathophysiology of the Disease (tabulated by the Author)
Disease Symptoms Pathology
Symptoms of dyslipidemia such as abdominal
obesity, moon face, subclavicular fat
deposition, buffalo hump
Maureen has been observed to be suffering
from high LDL cholesterol level along with
developing a moon face and gaining fat in her
abdomen as well as between her shoulders.
The steroid hormone cortisol is responsible for
functions like regulating the metabolism of
macronutrients like fats. Cortisol also
mobilizes of energy and nutrients by
metabolizing non-carbohydrate sources like
lipids and fats, by gluconeogenesis processes
for initiating responses of immunity and
inflammation (Sharma, Nieman & Feelders,
(2015). Thus, excessive intake of
glucocorticoid medications (like prednisolone
by Maureen) in exogenous Cushing’s
syndrome leads to uncontrolled
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4NURSING CASE STUDY
gluconeogenesis and lipid mobilization
resulting in dyslipidemia and facial, abdominal
and truncal obesity as observed in Maureen
(Pineyro et al., 2019).
Hyperglycemia It is evident that Maureen’s blood sugar levels
have spiked excessively, which can be
attributed to her prednisolone consumption.
Cortisols initiate the fight or flight response
towards stress by preventing tissues other than
those of the nervous system to absorb glucose
from the blood stream (Seki et al., 2018). Thus,
high consumption of glucocorticoid
medications like prednisolone results in
inability of the tissues to mobilize glucose
leading to high levels of the same circulating in
the blood and hence, abnormal fasting blood
sugar levels as evident in Maureen (Richmond
& Rogol, 2017).
Hypertension From the case study, we can observe that
Maureen has high blood pressure which again
can be attributed to her excessive dosages of
the glucocorticoid prednisolone. Cortisol
regulates the blood pressure and the
gluconeogenesis and lipid mobilization
resulting in dyslipidemia and facial, abdominal
and truncal obesity as observed in Maureen
(Pineyro et al., 2019).
Hyperglycemia It is evident that Maureen’s blood sugar levels
have spiked excessively, which can be
attributed to her prednisolone consumption.
Cortisols initiate the fight or flight response
towards stress by preventing tissues other than
those of the nervous system to absorb glucose
from the blood stream (Seki et al., 2018). Thus,
high consumption of glucocorticoid
medications like prednisolone results in
inability of the tissues to mobilize glucose
leading to high levels of the same circulating in
the blood and hence, abnormal fasting blood
sugar levels as evident in Maureen (Richmond
& Rogol, 2017).
Hypertension From the case study, we can observe that
Maureen has high blood pressure which again
can be attributed to her excessive dosages of
the glucocorticoid prednisolone. Cortisol
regulates the blood pressure and the
5NURSING CASE STUDY
functioning of the cardiovascular system by
initiating responses from epinephrine,
norepinephrine dopamine – catecholamines
which alleviate low blood pressure by
vasoconstriction (Dubrocq et al., 2017).
Glucocorticoid medication intake results in
excessive cortisol-like functions of
catecholaminses which increase blood pressure
through constriction hence resulting in
Maureen’s condition of high blood pressure
(Isidori et al., 2015). Cortisol also maintains
blood pressure via the anti-diuretic hormone
aldosterone, which increases blood pressure by
increasing uptake and inhibiting excretion of
sodium. Thus, an additional glucocorticoid
effect of sodium uptake may also contribute to
Maureen’s hypertensive symptoms (Raff &
Carroll, 2015).
functioning of the cardiovascular system by
initiating responses from epinephrine,
norepinephrine dopamine – catecholamines
which alleviate low blood pressure by
vasoconstriction (Dubrocq et al., 2017).
Glucocorticoid medication intake results in
excessive cortisol-like functions of
catecholaminses which increase blood pressure
through constriction hence resulting in
Maureen’s condition of high blood pressure
(Isidori et al., 2015). Cortisol also maintains
blood pressure via the anti-diuretic hormone
aldosterone, which increases blood pressure by
increasing uptake and inhibiting excretion of
sodium. Thus, an additional glucocorticoid
effect of sodium uptake may also contribute to
Maureen’s hypertensive symptoms (Raff &
Carroll, 2015).
6NURSING CASE STUDY
Question 3
Glucocorticoids: Pharmacokinetics
Taking insights from Maureen’s case, glucocorticoids are the drug class with highest
relevance. It can be observed that for management of her autoimmune condition of rheumatoid
arthritis, Maureen has been prescribed prednisolone – a glucocorticoid medication, whose high
dosages have resulted in her symptoms of Exogenous Cushing’s syndrome. Prednisolone and
other similar glucorticoids are used for mitigation of symptoms associated with inflammatory
and autoimmune diseases like lymphomas, rheumatoid arthritis, dermal infections, lupus ,
leukemias and symptoms of allergies (Melin et al., 2017). After intake, prednisolone is absorbed
immediately by the digestive tract and achieves its highest plasma concentration within the first
or second hour after its consumption. After being absorbed and metabolized, glucocorticoid
prednisolone have a half life lasting for a maximum of 3 hours. After this, it is excreted in the
urine in the form of glucoconjugates or free substances (Weatherley, McFadyen & Tammara,
2018).
Glucocorticoids: Pharmacodynamics
Glucocorticoids like prednisolone exert anti-inflammatory functions by suppressing
responses exerted by the humoral immune system, by interfering with the mediation of
inflammatory responses and by inhibiting the protective effects of leukocytes at the areas which
are suffering from inflammatory processes (Werkström et al., 2016). Other methods via which
glucocorticoids like prednisolone initiate hinder inflammation by preventing capillaries from
dilating and uptake of substances through membranes of vascular tissues, restricting functions of
polymorphonuclear leukocytes and macrophages and also reducing the secretion of vasoactive
Question 3
Glucocorticoids: Pharmacokinetics
Taking insights from Maureen’s case, glucocorticoids are the drug class with highest
relevance. It can be observed that for management of her autoimmune condition of rheumatoid
arthritis, Maureen has been prescribed prednisolone – a glucocorticoid medication, whose high
dosages have resulted in her symptoms of Exogenous Cushing’s syndrome. Prednisolone and
other similar glucorticoids are used for mitigation of symptoms associated with inflammatory
and autoimmune diseases like lymphomas, rheumatoid arthritis, dermal infections, lupus ,
leukemias and symptoms of allergies (Melin et al., 2017). After intake, prednisolone is absorbed
immediately by the digestive tract and achieves its highest plasma concentration within the first
or second hour after its consumption. After being absorbed and metabolized, glucocorticoid
prednisolone have a half life lasting for a maximum of 3 hours. After this, it is excreted in the
urine in the form of glucoconjugates or free substances (Weatherley, McFadyen & Tammara,
2018).
Glucocorticoids: Pharmacodynamics
Glucocorticoids like prednisolone exert anti-inflammatory functions by suppressing
responses exerted by the humoral immune system, by interfering with the mediation of
inflammatory responses and by inhibiting the protective effects of leukocytes at the areas which
are suffering from inflammatory processes (Werkström et al., 2016). Other methods via which
glucocorticoids like prednisolone initiate hinder inflammation by preventing capillaries from
dilating and uptake of substances through membranes of vascular tissues, restricting functions of
polymorphonuclear leukocytes and macrophages and also reducing the secretion of vasoactive
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7NURSING CASE STUDY
kinins. Glucocorticoids also reduce inflammation by mobilizing lipocortins and proteins
inhibiting phospholipase A2 which restrict pro-inflammatory prostaglandins and leukotrienes
(Xu et al., 2017).
Maureen’s condition of rheumatoid arthritis is characterized by autoimmune responses
which cause inflammation, damage to the synovial fluid, deformation of bones, joint swelling
pain. Hence, glucocorticoids like prednisolone will alleviate her inflammatory symptoms by
hindering pro-inflammatory leukotrienes and prostaglandins and controlling vascular processes
such as dilation and constriction. For this reason, this class of drugs is most relevant for the
management of her disease conditions (Chatzidionysiou et al., 2017).
Question 4
Care Plan for Maureen (tabulated by the Author)
Goal Intervention Rationale
First Priority: Reduction of
Exogenous Cushing’s
syndrome symptoms
After collaborative nursing
communication with the inter-
disciplinary team or
Maureen’s practitioners, the
nurse and stop or decrease
prednisolone dosages at levels
of tolerance.
High glucorticoid
dosages like
prednisolone result in
Exogenous Cushing’s
syndrome symptoms of
dyslipidemia, adiposity
and moon face.
Symptoms can be
reverse by either
withdrawing or
kinins. Glucocorticoids also reduce inflammation by mobilizing lipocortins and proteins
inhibiting phospholipase A2 which restrict pro-inflammatory prostaglandins and leukotrienes
(Xu et al., 2017).
Maureen’s condition of rheumatoid arthritis is characterized by autoimmune responses
which cause inflammation, damage to the synovial fluid, deformation of bones, joint swelling
pain. Hence, glucocorticoids like prednisolone will alleviate her inflammatory symptoms by
hindering pro-inflammatory leukotrienes and prostaglandins and controlling vascular processes
such as dilation and constriction. For this reason, this class of drugs is most relevant for the
management of her disease conditions (Chatzidionysiou et al., 2017).
Question 4
Care Plan for Maureen (tabulated by the Author)
Goal Intervention Rationale
First Priority: Reduction of
Exogenous Cushing’s
syndrome symptoms
After collaborative nursing
communication with the inter-
disciplinary team or
Maureen’s practitioners, the
nurse and stop or decrease
prednisolone dosages at levels
of tolerance.
High glucorticoid
dosages like
prednisolone result in
Exogenous Cushing’s
syndrome symptoms of
dyslipidemia, adiposity
and moon face.
Symptoms can be
reverse by either
withdrawing or
8NURSING CASE STUDY
reducing the prescribed
intake of the same
(Franke et al., 2017).
To manage rheumatoid
arthritis, the nurse and
practitioner must
prescribe prednisolone
at dosages permitted
by Australian
Government’s Federal
Statement of Principles
for Cushing’s
syndrome, which is
12.5 mg per day
(Australian
Government, 2019).
Second Priority: Alleviation of
gastrointestinal symptoms of
pain and bleeding
The nurse after discussion
with the clinician can
administer acetaminophen and
proton pump inhibitors.
Digestive tract
bleeding can be
prevented by proton
pump inhibitors which
inhibit gastric acid
secretion and permit
healing (Ray et al.,
reducing the prescribed
intake of the same
(Franke et al., 2017).
To manage rheumatoid
arthritis, the nurse and
practitioner must
prescribe prednisolone
at dosages permitted
by Australian
Government’s Federal
Statement of Principles
for Cushing’s
syndrome, which is
12.5 mg per day
(Australian
Government, 2019).
Second Priority: Alleviation of
gastrointestinal symptoms of
pain and bleeding
The nurse after discussion
with the clinician can
administer acetaminophen and
proton pump inhibitors.
Digestive tract
bleeding can be
prevented by proton
pump inhibitors which
inhibit gastric acid
secretion and permit
healing (Ray et al.,
9NURSING CASE STUDY
2016).
Acetaminophen
decrease
gastrointestinal pain by
regulating pro-
inflammatory
cyclooxygenase and
prostaglandin
functioning (Lange te
al., 2018).
Additional medications
include NSAIDS like
aspirin, paracetamol
and ibuprofen, as
stated by the Pharmacy
Guild of Australia
(Ortiz, Calcino &
Dunagan, 2016).
Third Priority: Management of
symptoms of Rheumatoid
Arthritis
The nurse can
administer non-
steroidal anti-
inflammatory drugs
(NSAIDS) to manage
Completely
withdrawing
glucocorticoid
medicines can increase
rheumatoid arthritis
2016).
Acetaminophen
decrease
gastrointestinal pain by
regulating pro-
inflammatory
cyclooxygenase and
prostaglandin
functioning (Lange te
al., 2018).
Additional medications
include NSAIDS like
aspirin, paracetamol
and ibuprofen, as
stated by the Pharmacy
Guild of Australia
(Ortiz, Calcino &
Dunagan, 2016).
Third Priority: Management of
symptoms of Rheumatoid
Arthritis
The nurse can
administer non-
steroidal anti-
inflammatory drugs
(NSAIDS) to manage
Completely
withdrawing
glucocorticoid
medicines can increase
rheumatoid arthritis
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10NURSING CASE STUDY
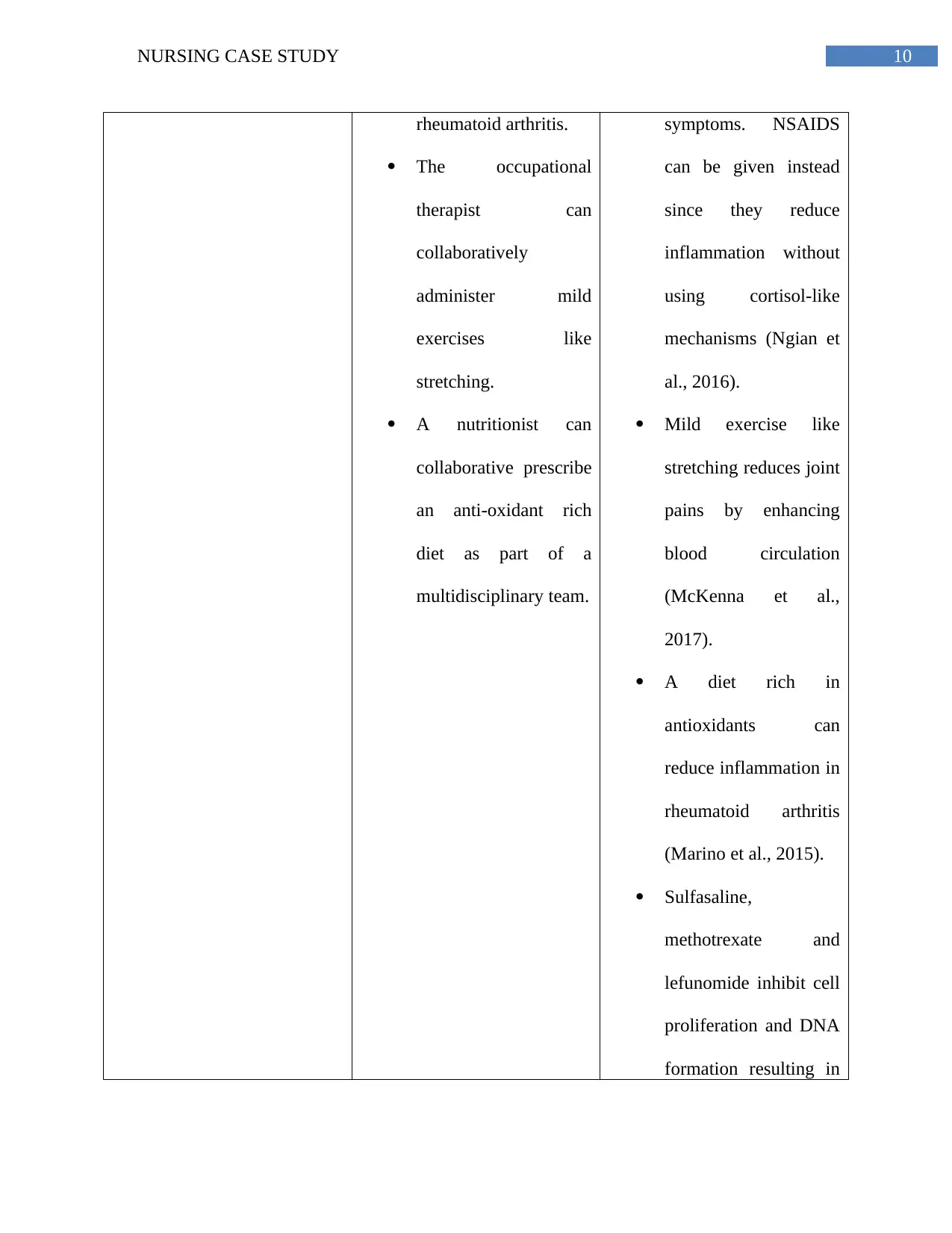
rheumatoid arthritis.
The occupational
therapist can
collaboratively
administer mild
exercises like
stretching.
A nutritionist can
collaborative prescribe
an anti-oxidant rich
diet as part of a
multidisciplinary team.
symptoms. NSAIDS
can be given instead
since they reduce
inflammation without
using cortisol-like
mechanisms (Ngian et
al., 2016).
Mild exercise like
stretching reduces joint
pains by enhancing
blood circulation
(McKenna et al.,
2017).
A diet rich in
antioxidants can
reduce inflammation in
rheumatoid arthritis
(Marino et al., 2015).
Sulfasaline,
methotrexate and
lefunomide inhibit cell
proliferation and DNA
formation resulting in
rheumatoid arthritis.
The occupational
therapist can
collaboratively
administer mild
exercises like
stretching.
A nutritionist can
collaborative prescribe
an anti-oxidant rich
diet as part of a
multidisciplinary team.
symptoms. NSAIDS
can be given instead
since they reduce
inflammation without
using cortisol-like
mechanisms (Ngian et
al., 2016).
Mild exercise like
stretching reduces joint
pains by enhancing
blood circulation
(McKenna et al.,
2017).
A diet rich in
antioxidants can
reduce inflammation in
rheumatoid arthritis
(Marino et al., 2015).
Sulfasaline,
methotrexate and
lefunomide inhibit cell
proliferation and DNA
formation resulting in
11NURSING CASE STUDY
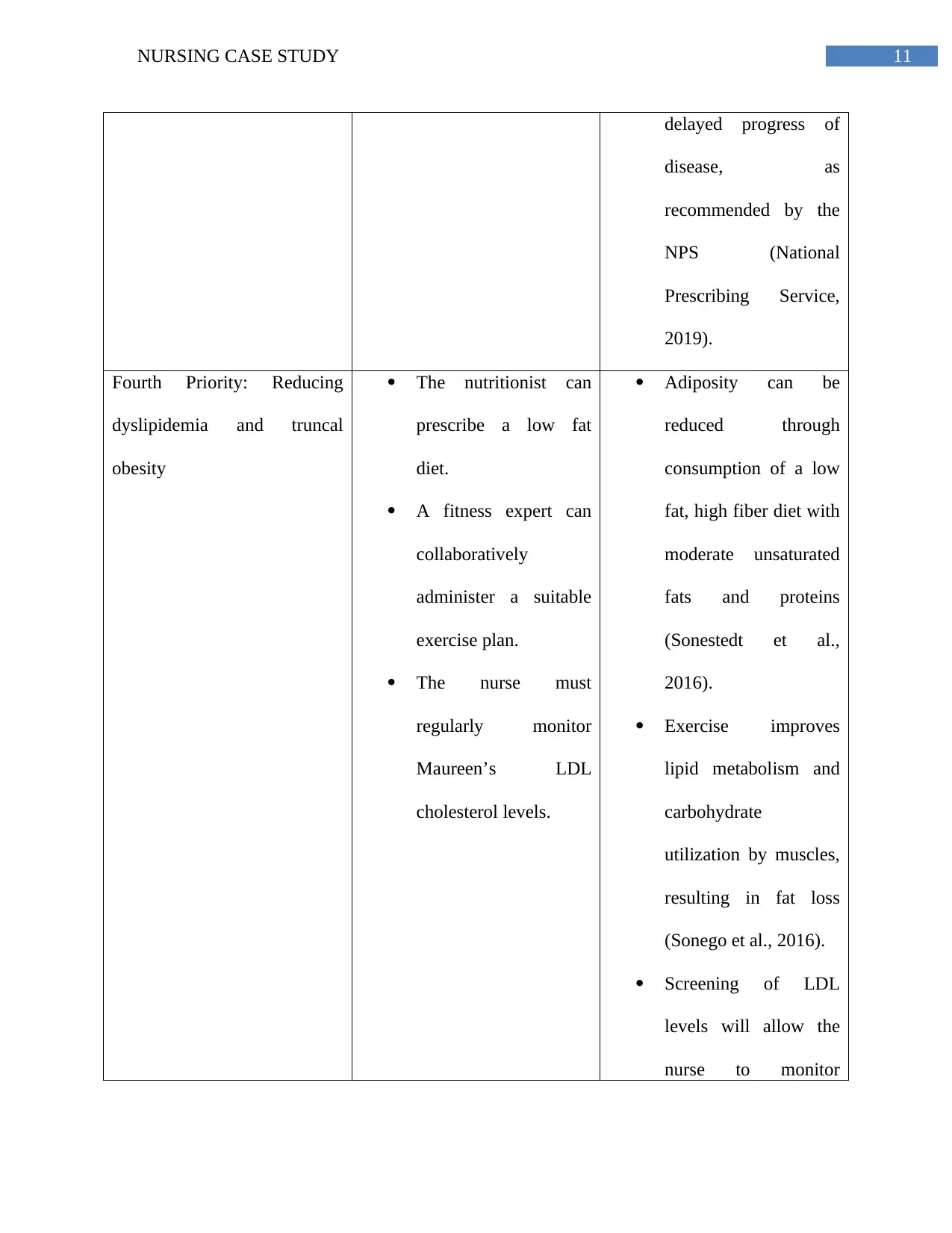
delayed progress of
disease, as
recommended by the
NPS (National
Prescribing Service,
2019).
Fourth Priority: Reducing
dyslipidemia and truncal
obesity
The nutritionist can
prescribe a low fat
diet.
A fitness expert can
collaboratively
administer a suitable
exercise plan.
The nurse must
regularly monitor
Maureen’s LDL
cholesterol levels.
Adiposity can be
reduced through
consumption of a low
fat, high fiber diet with
moderate unsaturated
fats and proteins
(Sonestedt et al.,
2016).
Exercise improves
lipid metabolism and
carbohydrate
utilization by muscles,
resulting in fat loss
(Sonego et al., 2016).
Screening of LDL
levels will allow the
nurse to monitor
delayed progress of
disease, as
recommended by the
NPS (National
Prescribing Service,
2019).
Fourth Priority: Reducing
dyslipidemia and truncal
obesity
The nutritionist can
prescribe a low fat
diet.
A fitness expert can
collaboratively
administer a suitable
exercise plan.
The nurse must
regularly monitor
Maureen’s LDL
cholesterol levels.
Adiposity can be
reduced through
consumption of a low
fat, high fiber diet with
moderate unsaturated
fats and proteins
(Sonestedt et al.,
2016).
Exercise improves
lipid metabolism and
carbohydrate
utilization by muscles,
resulting in fat loss
(Sonego et al., 2016).
Screening of LDL
levels will allow the
nurse to monitor
12NURSING CASE STUDY
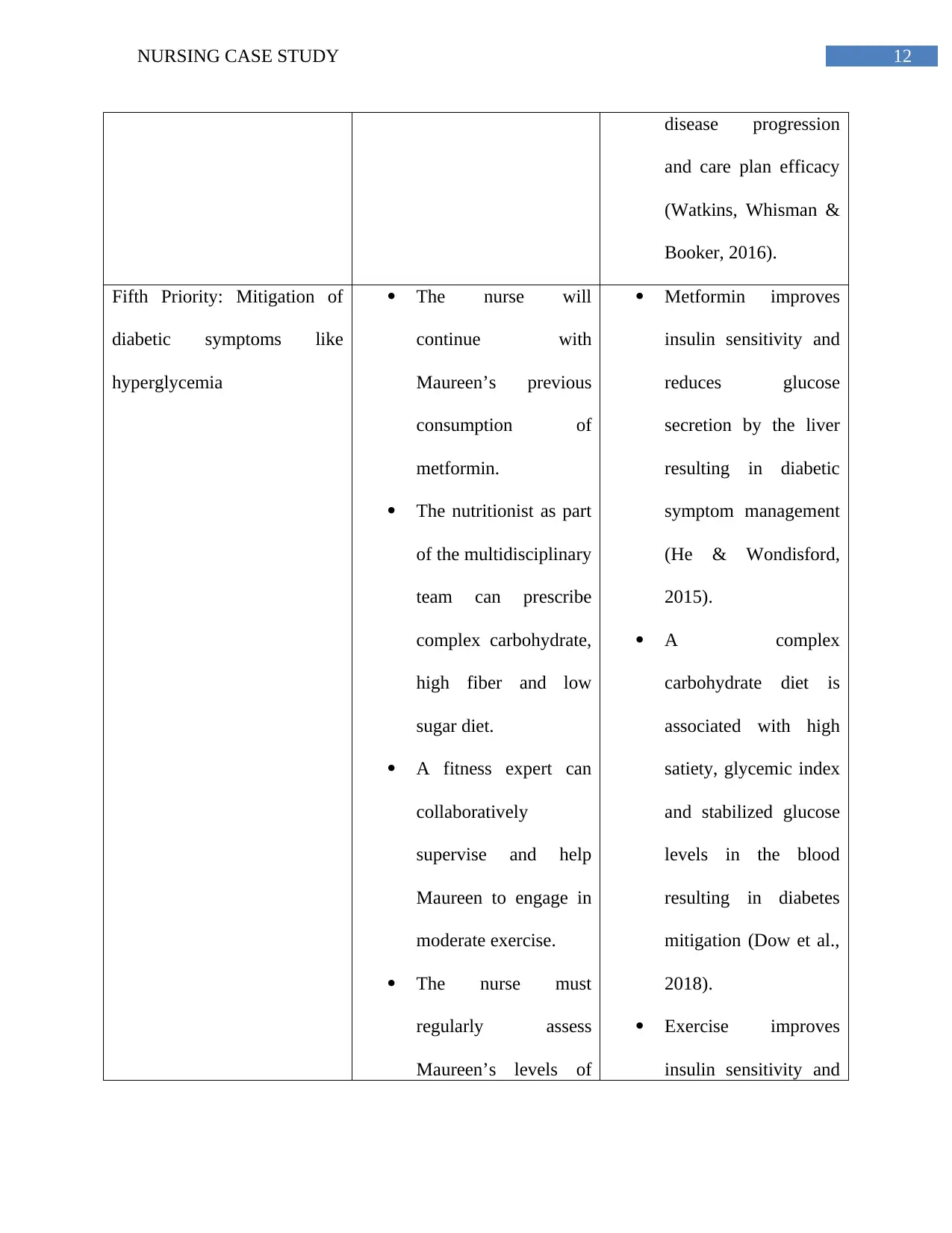
disease progression
and care plan efficacy
(Watkins, Whisman &
Booker, 2016).
Fifth Priority: Mitigation of
diabetic symptoms like
hyperglycemia
The nurse will
continue with
Maureen’s previous
consumption of
metformin.
The nutritionist as part
of the multidisciplinary
team can prescribe
complex carbohydrate,
high fiber and low
sugar diet.
A fitness expert can
collaboratively
supervise and help
Maureen to engage in
moderate exercise.
The nurse must
regularly assess
Maureen’s levels of
Metformin improves
insulin sensitivity and
reduces glucose
secretion by the liver
resulting in diabetic
symptom management
(He & Wondisford,
2015).
A complex
carbohydrate diet is
associated with high
satiety, glycemic index
and stabilized glucose
levels in the blood
resulting in diabetes
mitigation (Dow et al.,
2018).
Exercise improves
insulin sensitivity and
disease progression
and care plan efficacy
(Watkins, Whisman &
Booker, 2016).
Fifth Priority: Mitigation of
diabetic symptoms like
hyperglycemia
The nurse will
continue with
Maureen’s previous
consumption of
metformin.
The nutritionist as part
of the multidisciplinary
team can prescribe
complex carbohydrate,
high fiber and low
sugar diet.
A fitness expert can
collaboratively
supervise and help
Maureen to engage in
moderate exercise.
The nurse must
regularly assess
Maureen’s levels of
Metformin improves
insulin sensitivity and
reduces glucose
secretion by the liver
resulting in diabetic
symptom management
(He & Wondisford,
2015).
A complex
carbohydrate diet is
associated with high
satiety, glycemic index
and stabilized glucose
levels in the blood
resulting in diabetes
mitigation (Dow et al.,
2018).
Exercise improves
insulin sensitivity and
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

13NURSING CASE STUDY
blood glucose. glucose utilization by
muscles in diabetic
patients (Colberg et al.,
2016).
Screening of glucose
levels will allow the
nurse to monitor
disease progression
and care plan efficacy
(Watkins, Whisman &
Booker, 2016).
blood glucose. glucose utilization by
muscles in diabetic
patients (Colberg et al.,
2016).
Screening of glucose
levels will allow the
nurse to monitor
disease progression
and care plan efficacy
(Watkins, Whisman &
Booker, 2016).
14NURSING CASE STUDY
References
Aleksova, J., Ward, G., Taubman, K., Tan, J., Farrell, S., Galloway, S., ... & Sachithanandan, N.
(2016). Cushing's conundrum: an unusual case of primary pigmented nodular adrenal
disease in a 60-year-old woman. The Lancet Diabetes & Endocrinology, 4(7), 630.
Australian Government. (2019). Statement of Principles concerning Cushing's syndrome No. 34
of 2009. Retrieved from https://www.legislation.gov.au/Details/F2009L01601.
Chatzidionysiou, K., Emamikia, S., Nam, J., Ramiro, S., Smolen, J., van der Heijde, D., ... & van
Vollenhoven, R. (2017). Efficacy of glucocorticoids, conventional and targeted synthetic
disease-modifying antirheumatic drugs: a systematic literature review informing the 2016
update of the EULAR recommendations for the management of rheumatoid
arthritis. Annals of the rheumatic diseases, 76(6), 1102-1107.
Colberg, S. R., Sigal, R. J., Yardley, J. E., Riddell, M. C., Dunstan, D. W., Dempsey, P. C., ... &
Tate, D. F. (2016). Physical activity/exercise and diabetes: a position statement of the
American Diabetes Association. Diabetes care, 39(11), 2065-2079.
Dow, C., Mancini, F., Rajaobelina, K., Boutron-Ruault, M. C., Balkau, B., Bonnet, F., &
Fagherazzi, G. (2018). Diet and risk of diabetic retinopathy: A systematic
review. European journal of epidemiology, 33(2), 141-156.
Dubrocq, G., Estrada, A., Kelly, S., & Rakhmanina, N. (2017). Acute development of Cushing
syndrome in an HIV-infected child on atazanavir/ritonavir based antiretroviral
therapy. Endocrinology, diabetes & metabolism case reports, 2017(1).
References
Aleksova, J., Ward, G., Taubman, K., Tan, J., Farrell, S., Galloway, S., ... & Sachithanandan, N.
(2016). Cushing's conundrum: an unusual case of primary pigmented nodular adrenal
disease in a 60-year-old woman. The Lancet Diabetes & Endocrinology, 4(7), 630.
Australian Government. (2019). Statement of Principles concerning Cushing's syndrome No. 34
of 2009. Retrieved from https://www.legislation.gov.au/Details/F2009L01601.
Chatzidionysiou, K., Emamikia, S., Nam, J., Ramiro, S., Smolen, J., van der Heijde, D., ... & van
Vollenhoven, R. (2017). Efficacy of glucocorticoids, conventional and targeted synthetic
disease-modifying antirheumatic drugs: a systematic literature review informing the 2016
update of the EULAR recommendations for the management of rheumatoid
arthritis. Annals of the rheumatic diseases, 76(6), 1102-1107.
Colberg, S. R., Sigal, R. J., Yardley, J. E., Riddell, M. C., Dunstan, D. W., Dempsey, P. C., ... &
Tate, D. F. (2016). Physical activity/exercise and diabetes: a position statement of the
American Diabetes Association. Diabetes care, 39(11), 2065-2079.
Dow, C., Mancini, F., Rajaobelina, K., Boutron-Ruault, M. C., Balkau, B., Bonnet, F., &
Fagherazzi, G. (2018). Diet and risk of diabetic retinopathy: A systematic
review. European journal of epidemiology, 33(2), 141-156.
Dubrocq, G., Estrada, A., Kelly, S., & Rakhmanina, N. (2017). Acute development of Cushing
syndrome in an HIV-infected child on atazanavir/ritonavir based antiretroviral
therapy. Endocrinology, diabetes & metabolism case reports, 2017(1).
15NURSING CASE STUDY
Durrani, M. R. K., Ali, Z., Shafi, T., & Iqbal, M. D. (2017). Iatrogenic cushing syndrome: A
neglected aspect of medical care. Pak J Surg, 33(3), 199-202.
Franke, V., Scholtens, W. F., von Rosenstiel, I. A., & Walenkamp, M. J. (2017). Exogenous
Cushing's syndrome due to a Chinese herbalist’s prescription of ointment containing
dexamethasone. BMJ case reports, 2017, bcr-2016.
Gottiganti, G., Badhvel, J. K., Dornadula, G. R., Petam, A. K., & Pothugunt, B. C. (2017). Case
report on dexamethasone induced iatrogenic cushing syndrome. International Journal of
Pharmaceutical Sciences Review and Research, 45, 29.
He, L., & Wondisford, F. E. (2015). Metformin action: concentrations matter. Cell
metabolism, 21(2), 159-162.
Isidori, A. M., Graziadio, C., Paragliola, R. M., Cozzolino, A., Ambrogio, A. G., Colao, A., ... &
Pivonello, R. (2015). The hypertension of Cushing's syndrome: controversies in the
pathophysiology and focus on cardiovascular complications. Journal of
hypertension, 33(1), 44.
Lange, M., Lee, C. W., Knisely, T., Perla, S., Barber, K., & Kia, M. (2018). Efficacy of
intravenous acetaminophen in length of stay and postoperative pain control in
laparoscopic Roux-en-Y gastric bypass surgery patients. Bariatric surgical practice and
patient care, 13(3), 103-108.
Manubolu, S., & Nwosu, O. (2017). Exogenous Cushing's syndrome secondary to intermittent
high dose oral prednisone for presumed asthma exacerbations in the setting of multiple
emergency department visits. Journal of Clinical and Translational Endocrinology: Case
Reports, 6, 4-8.
Durrani, M. R. K., Ali, Z., Shafi, T., & Iqbal, M. D. (2017). Iatrogenic cushing syndrome: A
neglected aspect of medical care. Pak J Surg, 33(3), 199-202.
Franke, V., Scholtens, W. F., von Rosenstiel, I. A., & Walenkamp, M. J. (2017). Exogenous
Cushing's syndrome due to a Chinese herbalist’s prescription of ointment containing
dexamethasone. BMJ case reports, 2017, bcr-2016.
Gottiganti, G., Badhvel, J. K., Dornadula, G. R., Petam, A. K., & Pothugunt, B. C. (2017). Case
report on dexamethasone induced iatrogenic cushing syndrome. International Journal of
Pharmaceutical Sciences Review and Research, 45, 29.
He, L., & Wondisford, F. E. (2015). Metformin action: concentrations matter. Cell
metabolism, 21(2), 159-162.
Isidori, A. M., Graziadio, C., Paragliola, R. M., Cozzolino, A., Ambrogio, A. G., Colao, A., ... &
Pivonello, R. (2015). The hypertension of Cushing's syndrome: controversies in the
pathophysiology and focus on cardiovascular complications. Journal of
hypertension, 33(1), 44.
Lange, M., Lee, C. W., Knisely, T., Perla, S., Barber, K., & Kia, M. (2018). Efficacy of
intravenous acetaminophen in length of stay and postoperative pain control in
laparoscopic Roux-en-Y gastric bypass surgery patients. Bariatric surgical practice and
patient care, 13(3), 103-108.
Manubolu, S., & Nwosu, O. (2017). Exogenous Cushing's syndrome secondary to intermittent
high dose oral prednisone for presumed asthma exacerbations in the setting of multiple
emergency department visits. Journal of Clinical and Translational Endocrinology: Case
Reports, 6, 4-8.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
16NURSING CASE STUDY
Marino, A., Paterniti, I., Cordaro, M., Morabito, R., Campolo, M., Navarra, M., ... & Cuzzocrea,
S. (2015). Role of natural antioxidants and potential use of bergamot in treating
rheumatoid arthritis. PharmaNutrition, 3(2), 53-59.
McKenna, S., Donnelly, A., Fraser, A., Comber, L., & Kennedy, N. (2017). Does exercise
impact on sleep for people who have rheumatoid arthritis? A systematic
review. Rheumatology international, 37(6), 963-974.
Melin, J., Prothon, S., Kloft, C., Cleton, A., Amilon, C., Jorup, C., ... & Hamrén, U. W. (2017).
Pharmacokinetics of the inhaled selective glucocorticoid receptor modulator AZD5423
following inhalation using different devices. The AAPS journal, 19(3), 865-874.
National Prescribing Service. (2019). Disease modifying drugs in adult rheumatoid arthritis.
Retrieved from https://www.nps.org.au/australian-prescriber/articles/disease-
modifyingdrugs-in-adult-rheumatoid-arthritis.
Ngian, G. S., Briggs, A. M., Ackerman, I. N., & Van Doornum, S. (2016). Safety of anti‐
rheumatic drugs for rheumatoid arthritis in pregnancy and lactation. International journal
of rheumatic diseases, 19(9), 834-843.
Nieman, L. K. (2018). Recent Updates on the Diagnosis and Management of Cushing's
Syndrome. Endocrinology and Metabolism, 33(2), 139-146.
Notay, M., Fazel, N., & Awasthi, S. (2019). Cushing Syndrome Induced by Topical
Corticosteroids for the Treatment of Lichen Sclerosus. Journal of pediatric and
adolescent gynecology, 32(1), 83-85.
Marino, A., Paterniti, I., Cordaro, M., Morabito, R., Campolo, M., Navarra, M., ... & Cuzzocrea,
S. (2015). Role of natural antioxidants and potential use of bergamot in treating
rheumatoid arthritis. PharmaNutrition, 3(2), 53-59.
McKenna, S., Donnelly, A., Fraser, A., Comber, L., & Kennedy, N. (2017). Does exercise
impact on sleep for people who have rheumatoid arthritis? A systematic
review. Rheumatology international, 37(6), 963-974.
Melin, J., Prothon, S., Kloft, C., Cleton, A., Amilon, C., Jorup, C., ... & Hamrén, U. W. (2017).
Pharmacokinetics of the inhaled selective glucocorticoid receptor modulator AZD5423
following inhalation using different devices. The AAPS journal, 19(3), 865-874.
National Prescribing Service. (2019). Disease modifying drugs in adult rheumatoid arthritis.
Retrieved from https://www.nps.org.au/australian-prescriber/articles/disease-
modifyingdrugs-in-adult-rheumatoid-arthritis.
Ngian, G. S., Briggs, A. M., Ackerman, I. N., & Van Doornum, S. (2016). Safety of anti‐
rheumatic drugs for rheumatoid arthritis in pregnancy and lactation. International journal
of rheumatic diseases, 19(9), 834-843.
Nieman, L. K. (2018). Recent Updates on the Diagnosis and Management of Cushing's
Syndrome. Endocrinology and Metabolism, 33(2), 139-146.
Notay, M., Fazel, N., & Awasthi, S. (2019). Cushing Syndrome Induced by Topical
Corticosteroids for the Treatment of Lichen Sclerosus. Journal of pediatric and
adolescent gynecology, 32(1), 83-85.
17NURSING CASE STUDY
Ortiz, M., Calcino, G., & Dunagan, F. (2016). Prescription usage patterns of two formulations of
paracetamol in osteoarthritis: Australia-wide experience 2008-11. Australian family
physician, 45(5), 321.
Pineyro, M. M., Redes, L., De Mattos, S., Sanchez, L., Brignardello, E., Bianchi, V., ... & Viola,
M. (2019). Factitious Cushing's Syndrome: A Diagnosis to Consider When Evaluating
Hypercortisolism. Frontiers in Endocrinology, 10.
Pivonello, R., Isidori, A. M., De Martino, M. C., Newell-Price, J., Biller, B. M., & Colao, A.
(2016). Complications of Cushing's syndrome: state of the art. The Lancet Diabetes &
Endocrinology, 4(7), 611-629.
Raff, H., & Carroll, T. (2015). Cushing's syndrome: from physiological principles to diagnosis
and clinical care. The Journal of physiology, 593(3), 493-506.
Ray, W. A., Chung, C. P., Murray, K. T., Smalley, W. E., Daugherty, J. R., Dupont, W. D., &
Stein, C. M. (2016). Association of proton pump inhibitors with reduced risk of warfarin-
related serious upper gastrointestinal bleeding. Gastroenterology, 151(6), 1105-1112.
Richmond, E. J., & Rogol, A. D. (2017). Cushing’s Disease in Children and Adolescents:
Diagnosis and Management. In Cushing's Disease (pp. 187-200). Academic Press.
Scherrer, K. S., Weitz, M., Eisenack, J., Truffer, B., & Konrad, D. (2015). Cushing syndrome
after bilateral lensectomy. European journal of pediatrics, 174(3), 399-401.
Seki, Y., Morimoto, S., Saito, F., Takano, N., Kimura, S., Yamashita, K., ... & Watanabe, D.
(2018). ACTH-dependent Cyclic Cushing's Syndrome Triggered by Glucocorticoid
Ortiz, M., Calcino, G., & Dunagan, F. (2016). Prescription usage patterns of two formulations of
paracetamol in osteoarthritis: Australia-wide experience 2008-11. Australian family
physician, 45(5), 321.
Pineyro, M. M., Redes, L., De Mattos, S., Sanchez, L., Brignardello, E., Bianchi, V., ... & Viola,
M. (2019). Factitious Cushing's Syndrome: A Diagnosis to Consider When Evaluating
Hypercortisolism. Frontiers in Endocrinology, 10.
Pivonello, R., Isidori, A. M., De Martino, M. C., Newell-Price, J., Biller, B. M., & Colao, A.
(2016). Complications of Cushing's syndrome: state of the art. The Lancet Diabetes &
Endocrinology, 4(7), 611-629.
Raff, H., & Carroll, T. (2015). Cushing's syndrome: from physiological principles to diagnosis
and clinical care. The Journal of physiology, 593(3), 493-506.
Ray, W. A., Chung, C. P., Murray, K. T., Smalley, W. E., Daugherty, J. R., Dupont, W. D., &
Stein, C. M. (2016). Association of proton pump inhibitors with reduced risk of warfarin-
related serious upper gastrointestinal bleeding. Gastroenterology, 151(6), 1105-1112.
Richmond, E. J., & Rogol, A. D. (2017). Cushing’s Disease in Children and Adolescents:
Diagnosis and Management. In Cushing's Disease (pp. 187-200). Academic Press.
Scherrer, K. S., Weitz, M., Eisenack, J., Truffer, B., & Konrad, D. (2015). Cushing syndrome
after bilateral lensectomy. European journal of pediatrics, 174(3), 399-401.
Seki, Y., Morimoto, S., Saito, F., Takano, N., Kimura, S., Yamashita, K., ... & Watanabe, D.
(2018). ACTH-dependent Cyclic Cushing's Syndrome Triggered by Glucocorticoid
18NURSING CASE STUDY
Excess Through a Positive-Feedback Mechanism. The Journal of Clinical Endocrinology
& Metabolism.
Sharma, S. T., Nieman, L. K., & Feelders, R. A. (2015). Cushing’s syndrome: epidemiology and
developments in disease management. Clinical epidemiology, 7, 281.
Sonego, M., Sagrado, M. J., Escobar, G., Lazzerini, M., Rivas, E., Martín-Cañavate, R., ... &
Custodio, E. (2016). Dyslipidemia, diet and physical exercise in children on treatment
with antiretroviral medication in El Salvador: a cross-sectional study. The Pediatric
infectious disease journal, 35(10), 1111.
Sonestedt, E., Hellstrand, S., Drake, I., Schulz, C. A., Ericson, U., Hlebowicz, J., ... & Orho-
Melander, M. (2016). Diet quality and change in blood lipids during 16 years of follow-
up and their interaction with genetic risk for dyslipidemia. Nutrients, 8(5), 274.
Wagner-Bartak, N. A., Baiomy, A., Habra, M. A., Mukhi, S. V., Morani, A. C., Korivi, B. R., ...
& Elsayes, K. M. (2017). Cushing syndrome: diagnostic workup and imaging features,
with clinical and pathologic correlation. American Journal of Roentgenology, 209(1), 19-
32.
Watkins, T., Whisman, L., & Booker, P. (2016). Nursing assessment of continuous vital sign
surveillance to improve patient safety on the medical/surgical unit. Journal of clinical
nursing, 25(1-2), 278-281.
Weatherley, B., McFadyen, L., & Tammara, B. (2018). Population Pharmacokinetics of
Fosdagrocorat (PF‐04171327), a Dissociated Glucocorticoid Receptor Agonist, in
Patients With Rheumatoid Arthritis. Clinical and translational science, 11(1), 54-62.
Excess Through a Positive-Feedback Mechanism. The Journal of Clinical Endocrinology
& Metabolism.
Sharma, S. T., Nieman, L. K., & Feelders, R. A. (2015). Cushing’s syndrome: epidemiology and
developments in disease management. Clinical epidemiology, 7, 281.
Sonego, M., Sagrado, M. J., Escobar, G., Lazzerini, M., Rivas, E., Martín-Cañavate, R., ... &
Custodio, E. (2016). Dyslipidemia, diet and physical exercise in children on treatment
with antiretroviral medication in El Salvador: a cross-sectional study. The Pediatric
infectious disease journal, 35(10), 1111.
Sonestedt, E., Hellstrand, S., Drake, I., Schulz, C. A., Ericson, U., Hlebowicz, J., ... & Orho-
Melander, M. (2016). Diet quality and change in blood lipids during 16 years of follow-
up and their interaction with genetic risk for dyslipidemia. Nutrients, 8(5), 274.
Wagner-Bartak, N. A., Baiomy, A., Habra, M. A., Mukhi, S. V., Morani, A. C., Korivi, B. R., ...
& Elsayes, K. M. (2017). Cushing syndrome: diagnostic workup and imaging features,
with clinical and pathologic correlation. American Journal of Roentgenology, 209(1), 19-
32.
Watkins, T., Whisman, L., & Booker, P. (2016). Nursing assessment of continuous vital sign
surveillance to improve patient safety on the medical/surgical unit. Journal of clinical
nursing, 25(1-2), 278-281.
Weatherley, B., McFadyen, L., & Tammara, B. (2018). Population Pharmacokinetics of
Fosdagrocorat (PF‐04171327), a Dissociated Glucocorticoid Receptor Agonist, in
Patients With Rheumatoid Arthritis. Clinical and translational science, 11(1), 54-62.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
19NURSING CASE STUDY
Werkström, V., Prothon, S., Ekholm, E., Jorup, C., & Edsbäcker, S. (2016). Safety,
pharmacokinetics and pharmacodynamics of the selective glucocorticoid receptor
modulator AZD5423 after inhalation in healthy volunteers. Basic & clinical
pharmacology & toxicology, 119(6), 574-581.
Xu, W., Meng, K., Tu, Y., Tanaka, S., Onda, K., Sugiyama, K., ... & Yamada, H. (2017).
Tetrandrine potentiates the glucocorticoid pharmacodynamics via inhibiting P-
glycoprotein and mitogen-activated protein kinase in mitogen-activated human peripheral
blood mononuclear cells. European journal of pharmacology, 807, 102-108.
Werkström, V., Prothon, S., Ekholm, E., Jorup, C., & Edsbäcker, S. (2016). Safety,
pharmacokinetics and pharmacodynamics of the selective glucocorticoid receptor
modulator AZD5423 after inhalation in healthy volunteers. Basic & clinical
pharmacology & toxicology, 119(6), 574-581.
Xu, W., Meng, K., Tu, Y., Tanaka, S., Onda, K., Sugiyama, K., ... & Yamada, H. (2017).
Tetrandrine potentiates the glucocorticoid pharmacodynamics via inhibiting P-
glycoprotein and mitogen-activated protein kinase in mitogen-activated human peripheral
blood mononuclear cells. European journal of pharmacology, 807, 102-108.
1 out of 20
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.