Case Study Assessment of Cushing's Syndrome in Nursing Practice
VerifiedAdded on 2020/05/08
|8
|2371
|106
Case Study
AI Summary
This case study assesses a 24-year-old female patient, Smith Moureen, presenting with gastrointestinal bleeding, abdominal pain, and fatigue, along with a history of rheumatoid arthritis, type II diabetes, and current corticosteroid and metformin medication use. The assessment reveals potential Cus...
Running Head; Case Study Assessment
UNIVERSITY:
NAME :
STUDENT ID:
COURSE CODE
COURSE NAME
ASSIGNMENT
UNIVERSITY:
NAME :
STUDENT ID:
COURSE CODE
COURSE NAME
ASSIGNMENT
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Nursing case study Assessment Name 2
Introduction
The case study review entails a female Patient, Smith Moureen aged 24 years. She is
experiencing gastrointestinal bleeding, abdominal pain and fatigue which are worsening. The
patient has a history of rheumatoid arthritis and is currently under corticosteroids medication.
Further, she has type II diabetes and she is on metformin medication for the same. On
admission various vital information have been undertaken and the patient’s impression on
assessments exhibits Cushing’s syndrome.
Causes of Cushing’s syndrome
Cushing syndrome is a collection of various signs and symptoms caused by prolonged
exposure of cortisol drug. Accompanying symptoms include high blood pressure, abdominal
obesity characterised by slender arms and legs, fat lumps observed on the shoulders and skin
which is fragile which is occasioned by poor healing process. Women have been observed to
have more hair growth and abnormal menstruation periods. There can also be occasioned
headaches and feeling of tiredness, (Bertagna et al, 2009).
Cushing syndrome is caused by excessive cortisol related drugs like prednisone or tissue
growth which leads to excessive production of cortisol in the adrenal glands. The functions
of cortisol in the body include regulation of blood pressure, reducing the immune system
response on inflammatory system, conversion of carbohydrates, proteins and fats into energy
form, regulation of insulin effects and stress response, (Melmed et al, 2011).
The body can be induced to produce elevated levels of cortisol based on factors such as
stress levels, alcoholism, malnutrition and depression. Thus the most common causes of
Cushing disease is the excessive use of corticosteroid and maintenance of high doses for
longer durations, (Jeffcoate et al, 1979).
Incidences of Cushing syndrome
The incidences of Cushing syndrome have been imprecise and are likely to be under
Introduction
The case study review entails a female Patient, Smith Moureen aged 24 years. She is
experiencing gastrointestinal bleeding, abdominal pain and fatigue which are worsening. The
patient has a history of rheumatoid arthritis and is currently under corticosteroids medication.
Further, she has type II diabetes and she is on metformin medication for the same. On
admission various vital information have been undertaken and the patient’s impression on
assessments exhibits Cushing’s syndrome.
Causes of Cushing’s syndrome
Cushing syndrome is a collection of various signs and symptoms caused by prolonged
exposure of cortisol drug. Accompanying symptoms include high blood pressure, abdominal
obesity characterised by slender arms and legs, fat lumps observed on the shoulders and skin
which is fragile which is occasioned by poor healing process. Women have been observed to
have more hair growth and abnormal menstruation periods. There can also be occasioned
headaches and feeling of tiredness, (Bertagna et al, 2009).
Cushing syndrome is caused by excessive cortisol related drugs like prednisone or tissue
growth which leads to excessive production of cortisol in the adrenal glands. The functions
of cortisol in the body include regulation of blood pressure, reducing the immune system
response on inflammatory system, conversion of carbohydrates, proteins and fats into energy
form, regulation of insulin effects and stress response, (Melmed et al, 2011).
The body can be induced to produce elevated levels of cortisol based on factors such as
stress levels, alcoholism, malnutrition and depression. Thus the most common causes of
Cushing disease is the excessive use of corticosteroid and maintenance of high doses for
longer durations, (Jeffcoate et al, 1979).
Incidences of Cushing syndrome
The incidences of Cushing syndrome have been imprecise and are likely to be under
Nursing case study Assessment Name 3
estimated. Pituitary ACTH Cushing syndrome is approximately 5-6 times common than other
forms caused by benign or malignant tumours, (Govindan et al, 2006). The epidemiologic
reports indicate that there are approximately 5-25 per million cases per year, however with
this statistics, the reported cases are much lower at 1.2-2.4 per million in any given year,
(James et al, 2016).
The associative prevalence of hypercortisolinism has been estimated to be around 2%-
5% among patients with poor control and management of diabetes and hypertension. The
female gender has high prevalence to the male gender in the ratio of 3:1, (Melmed et al,
2011). Cushing syndrome is a rare disease among children. the disease is fatal as it can cause
death and increased morbidity and mortality rate which is characterised by cardiovascular
complications,(Steffensen et al, 2010).
In US, studies have estimated that the incidence was higher than those reported form
European based studies. The results indicated that it affected an estimate of 6.2 to 7.6 per
million persons- years, (Broder et al, 2015).
Risks factors
Cushing syndrome risks factors are well established; however epidemiological studies
have diagnosed more females than males. Further it is common among the age group of 25
years to 40 years. The common risks factors for the disease are;
- Type diabetes, obesity and fluctuating blood glucose levels
- Long term usage of corticosteroid drugs
- Pituitary gland tumours
- Adrenal gland disease and
- Ectopic ACTH forms of secreting tumours
Impacts on the patient and family
Cushing disease has tremendous effects on the patients and the family. Weight
estimated. Pituitary ACTH Cushing syndrome is approximately 5-6 times common than other
forms caused by benign or malignant tumours, (Govindan et al, 2006). The epidemiologic
reports indicate that there are approximately 5-25 per million cases per year, however with
this statistics, the reported cases are much lower at 1.2-2.4 per million in any given year,
(James et al, 2016).
The associative prevalence of hypercortisolinism has been estimated to be around 2%-
5% among patients with poor control and management of diabetes and hypertension. The
female gender has high prevalence to the male gender in the ratio of 3:1, (Melmed et al,
2011). Cushing syndrome is a rare disease among children. the disease is fatal as it can cause
death and increased morbidity and mortality rate which is characterised by cardiovascular
complications,(Steffensen et al, 2010).
In US, studies have estimated that the incidence was higher than those reported form
European based studies. The results indicated that it affected an estimate of 6.2 to 7.6 per
million persons- years, (Broder et al, 2015).
Risks factors
Cushing syndrome risks factors are well established; however epidemiological studies
have diagnosed more females than males. Further it is common among the age group of 25
years to 40 years. The common risks factors for the disease are;
- Type diabetes, obesity and fluctuating blood glucose levels
- Long term usage of corticosteroid drugs
- Pituitary gland tumours
- Adrenal gland disease and
- Ectopic ACTH forms of secreting tumours
Impacts on the patient and family
Cushing disease has tremendous effects on the patients and the family. Weight
You're viewing a preview
Unlock full access by subscribing today!



Nursing case study Assessment Name 4
management of the patients is affected and further it deteriorates the health status of the
patients through increased mortality and morbidity.
The patients often experience sudden increase in weight, poor wound management,
prolong fatigue, anxiety disorders, emotional disturbances, sleep disorders, experiencing
menstrual irregularities.
These impacts have enormous effects on psychological and emotional disturbance on the
patients and their families. The patients often feel increasing signs of sickness but symptoms
seem like depression or hypochondriac lacking diet and exercise fitness. Further often the
family; don’t understand the situation the patient is undergoing and support your getting is
just to advise you to change the lifestyle, further deteriorating the impact on the patient.
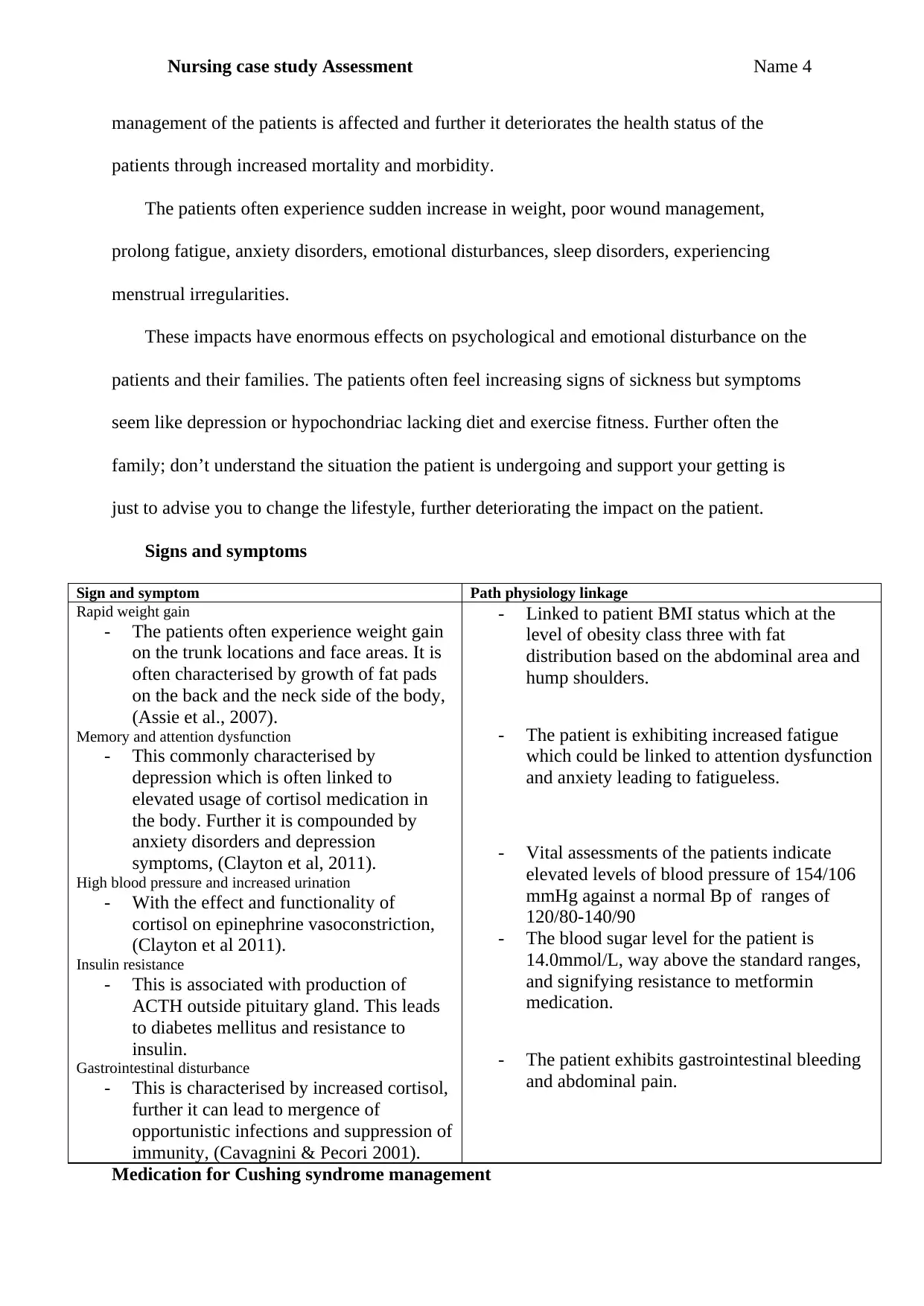
Signs and symptoms
Sign and symptom Path physiology linkage
Rapid weight gain
- The patients often experience weight gain
on the trunk locations and face areas. It is
often characterised by growth of fat pads
on the back and the neck side of the body,
(Assie et al., 2007).
Memory and attention dysfunction
- This commonly characterised by
depression which is often linked to
elevated usage of cortisol medication in
the body. Further it is compounded by
anxiety disorders and depression
symptoms, (Clayton et al, 2011).
High blood pressure and increased urination
- With the effect and functionality of
cortisol on epinephrine vasoconstriction,
(Clayton et al 2011).
Insulin resistance
- This is associated with production of
ACTH outside pituitary gland. This leads
to diabetes mellitus and resistance to
insulin.
Gastrointestinal disturbance
- This is characterised by increased cortisol,
further it can lead to mergence of
opportunistic infections and suppression of
immunity, (Cavagnini & Pecori 2001).
- Linked to patient BMI status which at the
level of obesity class three with fat
distribution based on the abdominal area and
hump shoulders.
- The patient is exhibiting increased fatigue
which could be linked to attention dysfunction
and anxiety leading to fatigueless.
- Vital assessments of the patients indicate
elevated levels of blood pressure of 154/106
mmHg against a normal Bp of ranges of
120/80-140/90
- The blood sugar level for the patient is
14.0mmol/L, way above the standard ranges,
and signifying resistance to metformin
medication.
- The patient exhibits gastrointestinal bleeding
and abdominal pain.
Medication for Cushing syndrome management
management of the patients is affected and further it deteriorates the health status of the
patients through increased mortality and morbidity.
The patients often experience sudden increase in weight, poor wound management,
prolong fatigue, anxiety disorders, emotional disturbances, sleep disorders, experiencing
menstrual irregularities.
These impacts have enormous effects on psychological and emotional disturbance on the
patients and their families. The patients often feel increasing signs of sickness but symptoms
seem like depression or hypochondriac lacking diet and exercise fitness. Further often the
family; don’t understand the situation the patient is undergoing and support your getting is
just to advise you to change the lifestyle, further deteriorating the impact on the patient.
Signs and symptoms
Sign and symptom Path physiology linkage
Rapid weight gain
- The patients often experience weight gain
on the trunk locations and face areas. It is
often characterised by growth of fat pads
on the back and the neck side of the body,
(Assie et al., 2007).
Memory and attention dysfunction
- This commonly characterised by
depression which is often linked to
elevated usage of cortisol medication in
the body. Further it is compounded by
anxiety disorders and depression
symptoms, (Clayton et al, 2011).
High blood pressure and increased urination
- With the effect and functionality of
cortisol on epinephrine vasoconstriction,
(Clayton et al 2011).
Insulin resistance
- This is associated with production of
ACTH outside pituitary gland. This leads
to diabetes mellitus and resistance to
insulin.
Gastrointestinal disturbance
- This is characterised by increased cortisol,
further it can lead to mergence of
opportunistic infections and suppression of
immunity, (Cavagnini & Pecori 2001).
- Linked to patient BMI status which at the
level of obesity class three with fat
distribution based on the abdominal area and
hump shoulders.
- The patient is exhibiting increased fatigue
which could be linked to attention dysfunction
and anxiety leading to fatigueless.
- Vital assessments of the patients indicate
elevated levels of blood pressure of 154/106
mmHg against a normal Bp of ranges of
120/80-140/90
- The blood sugar level for the patient is
14.0mmol/L, way above the standard ranges,
and signifying resistance to metformin
medication.
- The patient exhibits gastrointestinal bleeding
and abdominal pain.
Medication for Cushing syndrome management
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Nursing case study Assessment Name 5
The role of medication is to decrease the secretion of cortisol and blockage of receptors of
glucocorticoids and inhibition of ACTH. The various classes of these drugs are;
i) Steroid genesis inhibitors
- Op’DDD drugs are aimed at reducing the cleavage around cholesterol. It inhibits
cortisol secretion among patients with Cushing syndrome. It is effective in half of the
patients and has been shown to induce adrenal atrophy, (Castinetti et al., 2008).
- Another drug inhibitor drug is Ketaconazole which inhibits production of cytochrome
p450 enzymes. It normalizes the levels of cortisols, (Castinetti et al., 2008).
- Metyrapone drug blocks the synthesis of cortisol through inhibiting beta hydroxylase.
It is effective in more than 50% of the patients, it further induces low production of
potassium and hyperandrogenism, (Obinata et al, 2008).
ii) Glucocorticoid receptor antagonist drugs
- Mifepristone drug is a receptor antagonist drug under this class. It is effective clinical
signs control in hypercortisolism, (Castinetti et al., 2009).
iii) ACTH lowering drugs
- The drugs under this class are effective anti secretory and anti tumoral in
prolactinomas disease.
Nursing Care strategies for the patient
Monitoring and management of associative complications
In the first 24 hours, there is need for management of adrenal hypofunction, which calls
for close monitoring for weak pulse, respiratory rates and body weakness. There is need for
administration of IV fluids to the patient and management of electrolytes and presence of
corticosteroids, before and after treatment. Further close monitoring of lab results to check
statuses of electrolytes is key for the patient. Further since the patient is diabetic, there is need
for close monitoring of blood glucose levels and taking appropriate actions towards increase
The role of medication is to decrease the secretion of cortisol and blockage of receptors of
glucocorticoids and inhibition of ACTH. The various classes of these drugs are;
i) Steroid genesis inhibitors
- Op’DDD drugs are aimed at reducing the cleavage around cholesterol. It inhibits
cortisol secretion among patients with Cushing syndrome. It is effective in half of the
patients and has been shown to induce adrenal atrophy, (Castinetti et al., 2008).
- Another drug inhibitor drug is Ketaconazole which inhibits production of cytochrome
p450 enzymes. It normalizes the levels of cortisols, (Castinetti et al., 2008).
- Metyrapone drug blocks the synthesis of cortisol through inhibiting beta hydroxylase.
It is effective in more than 50% of the patients, it further induces low production of
potassium and hyperandrogenism, (Obinata et al, 2008).
ii) Glucocorticoid receptor antagonist drugs
- Mifepristone drug is a receptor antagonist drug under this class. It is effective clinical
signs control in hypercortisolism, (Castinetti et al., 2009).
iii) ACTH lowering drugs
- The drugs under this class are effective anti secretory and anti tumoral in
prolactinomas disease.
Nursing Care strategies for the patient
Monitoring and management of associative complications
In the first 24 hours, there is need for management of adrenal hypofunction, which calls
for close monitoring for weak pulse, respiratory rates and body weakness. There is need for
administration of IV fluids to the patient and management of electrolytes and presence of
corticosteroids, before and after treatment. Further close monitoring of lab results to check
statuses of electrolytes is key for the patient. Further since the patient is diabetic, there is need
for close monitoring of blood glucose levels and taking appropriate actions towards increase
Nursing case study Assessment Name 6
in blood sugar levels. Further there is need for close monitoring for acute adrenal condition,
which is a life threatening condition characterised by low levels of cortisol hormone from
adrenal glands.
Monitoring the intake and output of the patient is key in ensuring daily weights and
glucose levels and accurate assessment of electrolytes. Urine sample tests will be initiated at
24 hours before medication. Blood samples assessment ensures there is regular management
of the hormone levels for the patient. Normal levels cortisol in both urine and blood needs to
drop after initiation of medication, since the drug initiates signal on pituitary gland to lower
levels of Adrenocorticotropic hormone.
Assessment of late night corticosol in saliva is key in ensuring there is sufficient
production. The level of cortisols at night normally drops and this might be an indicator for
corticosol production management which may require further diagnosis.
Decreasing risk of injury
As a nurse there is need for providing protective environment for the patient to prevent
any fall, fracture and other injuries which are linked to bones and body tissues. Further there
is need to assist the patient, as he is weak in ambulation and to ensure that there is prevention
of falls.
Reduction of risk of infection
There is need to ensure that the patient is kept in an unexposed environment which might
lead to infections. As a nurse, there is need to assess subtle infections. In case the patient has
been scheduled for surgery in the first 24 hours, there is need to monitor frequently the blood
sugar levels and managing it and stool assessments for diabetes mellitus and peptic ulcers
which are predominant problems associated with.
in blood sugar levels. Further there is need for close monitoring for acute adrenal condition,
which is a life threatening condition characterised by low levels of cortisol hormone from
adrenal glands.
Monitoring the intake and output of the patient is key in ensuring daily weights and
glucose levels and accurate assessment of electrolytes. Urine sample tests will be initiated at
24 hours before medication. Blood samples assessment ensures there is regular management
of the hormone levels for the patient. Normal levels cortisol in both urine and blood needs to
drop after initiation of medication, since the drug initiates signal on pituitary gland to lower
levels of Adrenocorticotropic hormone.
Assessment of late night corticosol in saliva is key in ensuring there is sufficient
production. The level of cortisols at night normally drops and this might be an indicator for
corticosol production management which may require further diagnosis.
Decreasing risk of injury
As a nurse there is need for providing protective environment for the patient to prevent
any fall, fracture and other injuries which are linked to bones and body tissues. Further there
is need to assist the patient, as he is weak in ambulation and to ensure that there is prevention
of falls.
Reduction of risk of infection
There is need to ensure that the patient is kept in an unexposed environment which might
lead to infections. As a nurse, there is need to assess subtle infections. In case the patient has
been scheduled for surgery in the first 24 hours, there is need to monitor frequently the blood
sugar levels and managing it and stool assessments for diabetes mellitus and peptic ulcers
which are predominant problems associated with.
You're viewing a preview
Unlock full access by subscribing today!
Nursing case study Assessment Name 7
References
Assié, G., Bahurel, H., Coste, J., Silvera, S., Kujas, M., Dugué, M. A., ... & Bertagna, X.
(2007). Corticotroph tumor progression after adrenalectomy in Cushing’s disease: a
reappraisal of Nelson’s syndrome. The Journal of Clinical Endocrinology &
Metabolism, 92(1), 172-179.
Bertagna, X., Guignat, L., Groussin, L., & Bertherat, J. (2009). Cushing's disease. Best
Practice & Research Clinical Endocrinology & Metabolism, 23(5), 607-623.
Broder, M. S., Neary, M. P., Chang, E., Cherepanov, D., & Ludlam, W. H. (2015). Incidence
of Cushing’s syndrome and Cushing’s disease in commercially-insured patients< 65
years old in the United States. Pituitary, 18(3), 283-289.
Castinetti, F., Fassnacht, M., Johanssen, S., Terzolo, M., Bouchard, P., Chanson, P., ... &
Young, J. (2009). Merits and pitfalls of mifepristone in Cushing's syndrome. European
journal of endocrinology, 160(6), 1003-1010.
Castinetti, F., Morange, I., Jaquet, P., Conte-Devolx, B., & Brue, T. (2008). Ketoconazole
revisited: a preoperative or postoperative treatment in Cushing's disease. European
Journal of Endocrinology, 158(1), 91-99.
Cavagnini, F., & Pecori, F. G. (2001, April). Epidemiology and follow-up of Cushing's
disease. In Annales d'endocrinologie (Vol. 62, No. 2, pp. 168-172).
Clayton, R. N., Raskauskiene, D., Reulen, R. C., & Jones, P. W. (2011). Mortality and
morbidity in Cushing's disease over 50 years in Stoke-on-Trent, UK: audit and meta-
analysis of literature. The Journal of Clinical Endocrinology & Metabolism, 96(3), 632-
642.
Govindan, R., Page, N., Morgensztern, D., Read, W., Tierney, R., Vlahiotis, A., ... &
Piccirillo, J. (2006). Changing epidemiology of small-cell lung cancer in the United
States over the last 30 years: analysis of the surveillance, epidemiologic, and end results
database. Journal of clinical oncology, 24(28), 4539-4544.
James, B. C., Aschebrook-Kilfoy, B., Cipriani, N., Kaplan, E. L., Angelos, P., & Grogan, R.
H. (2016). The incidence and survival of rare cancers of the Thyroid, Parathyroid,
References
Assié, G., Bahurel, H., Coste, J., Silvera, S., Kujas, M., Dugué, M. A., ... & Bertagna, X.
(2007). Corticotroph tumor progression after adrenalectomy in Cushing’s disease: a
reappraisal of Nelson’s syndrome. The Journal of Clinical Endocrinology &
Metabolism, 92(1), 172-179.
Bertagna, X., Guignat, L., Groussin, L., & Bertherat, J. (2009). Cushing's disease. Best
Practice & Research Clinical Endocrinology & Metabolism, 23(5), 607-623.
Broder, M. S., Neary, M. P., Chang, E., Cherepanov, D., & Ludlam, W. H. (2015). Incidence
of Cushing’s syndrome and Cushing’s disease in commercially-insured patients< 65
years old in the United States. Pituitary, 18(3), 283-289.
Castinetti, F., Fassnacht, M., Johanssen, S., Terzolo, M., Bouchard, P., Chanson, P., ... &
Young, J. (2009). Merits and pitfalls of mifepristone in Cushing's syndrome. European
journal of endocrinology, 160(6), 1003-1010.
Castinetti, F., Morange, I., Jaquet, P., Conte-Devolx, B., & Brue, T. (2008). Ketoconazole
revisited: a preoperative or postoperative treatment in Cushing's disease. European
Journal of Endocrinology, 158(1), 91-99.
Cavagnini, F., & Pecori, F. G. (2001, April). Epidemiology and follow-up of Cushing's
disease. In Annales d'endocrinologie (Vol. 62, No. 2, pp. 168-172).
Clayton, R. N., Raskauskiene, D., Reulen, R. C., & Jones, P. W. (2011). Mortality and
morbidity in Cushing's disease over 50 years in Stoke-on-Trent, UK: audit and meta-
analysis of literature. The Journal of Clinical Endocrinology & Metabolism, 96(3), 632-
642.
Govindan, R., Page, N., Morgensztern, D., Read, W., Tierney, R., Vlahiotis, A., ... &
Piccirillo, J. (2006). Changing epidemiology of small-cell lung cancer in the United
States over the last 30 years: analysis of the surveillance, epidemiologic, and end results
database. Journal of clinical oncology, 24(28), 4539-4544.
James, B. C., Aschebrook-Kilfoy, B., Cipriani, N., Kaplan, E. L., Angelos, P., & Grogan, R.
H. (2016). The incidence and survival of rare cancers of the Thyroid, Parathyroid,
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Nursing case study Assessment Name 8
adrenal, and Pancreas. Annals of surgical oncology, 23(2), 424-433.
Jeffcoate, W. J., Silverstone, J. T., Edwards, C. R. W., & Besser, G. M. (1979). Psychiatric
manifestations of Cushing's syndrome: response to lowering of plasma cortisol. QJM:
An International Journal of Medicine, 48(3), 465-472.
Melmed, S., Polonsky, K. S., Larsen, P. R., & Kronenberg, H. M. (1897). Williams Textbook
of Endocrinology, 2011. Saunders Elsevier, Philadelphia.
Melmed, S., Polonsky, K. S., Larsen, P. R., & Kronenberg, H. M. (1897). Williams Textbook
of Endocrinology, 2011. Saunders Elsevier, Philadelphia.
Obinata, D., Yamaguchi, K., Hirano, D., Yoshida, T., Soma, M., & Takahashi, S. (2008).
Preoperative management of Cushing's syndrome with metyrapone for severe
psychiatric disturbances. International journal of urology, 15(4), 361-362.
Steffensen C, Bak AM, Rubeck KZ, Jorgensen JO: Epidemiology of Cushing's syndrome.
Neuroendocrinology. 2010, 92 (Suppl 1): 1-5.
adrenal, and Pancreas. Annals of surgical oncology, 23(2), 424-433.
Jeffcoate, W. J., Silverstone, J. T., Edwards, C. R. W., & Besser, G. M. (1979). Psychiatric
manifestations of Cushing's syndrome: response to lowering of plasma cortisol. QJM:
An International Journal of Medicine, 48(3), 465-472.
Melmed, S., Polonsky, K. S., Larsen, P. R., & Kronenberg, H. M. (1897). Williams Textbook
of Endocrinology, 2011. Saunders Elsevier, Philadelphia.
Melmed, S., Polonsky, K. S., Larsen, P. R., & Kronenberg, H. M. (1897). Williams Textbook
of Endocrinology, 2011. Saunders Elsevier, Philadelphia.
Obinata, D., Yamaguchi, K., Hirano, D., Yoshida, T., Soma, M., & Takahashi, S. (2008).
Preoperative management of Cushing's syndrome with metyrapone for severe
psychiatric disturbances. International journal of urology, 15(4), 361-362.
Steffensen C, Bak AM, Rubeck KZ, Jorgensen JO: Epidemiology of Cushing's syndrome.
Neuroendocrinology. 2010, 92 (Suppl 1): 1-5.
1 out of 8
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.