Nursing Leadership: Analysis, Root Cause Analysis, Risk Management and Required Changes
VerifiedAdded on 2023/06/08
|21
|5207
|267
AI Summary
This report analyses the existing condition of nursing leadership in healthcare facilities and provides a root cause analysis, fishbone analysis, risk management and required changes to improve the system. The report also discusses the implementation of leadership and NHS framework to make the changes sustainable and effective.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: NURSING LEADERSHIP
NURSING LEADERSHIP
Name of the Student
Name of the University
Author note
NURSING LEADERSHIP
Name of the Student
Name of the University
Author note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1NURSING LEADERSHIP
Table of Content
Introduction:...............................................................................................................................2
Analysis existing condition:.......................................................................................................3
Root cause analysis (5 why)...................................................................................................3
Fish-bone analysis..................................................................................................................5
Risk management and matrix:................................................................................................7
Required Changes......................................................................................................................9
PDSA (Plan Do Study Act):.....................................................................................................10
Implementation of leadership...................................................................................................13
Implementation of NHS Framework........................................................................................14
Conclusion:..............................................................................................................................16
Reference:................................................................................................................................18
Table of Content
Introduction:...............................................................................................................................2
Analysis existing condition:.......................................................................................................3
Root cause analysis (5 why)...................................................................................................3
Fish-bone analysis..................................................................................................................5
Risk management and matrix:................................................................................................7
Required Changes......................................................................................................................9
PDSA (Plan Do Study Act):.....................................................................................................10
Implementation of leadership...................................................................................................13
Implementation of NHS Framework........................................................................................14
Conclusion:..............................................................................................................................16
Reference:................................................................................................................................18
2NURSING LEADERSHIP
Introduction:
Intentional rounding is an essential part of healthcare and nursing facility where the
caregivers or nurses perform a direct assistive surveillance to identify any discrepancy in
patient’s health or physical condition such as falling injury, agitation, breathing issues and
others. Intentional rounding is also associated with care rounding every 1 hour during the day
to check on the 5 Ps, meal times, needs of assistance and others. The rounding is also
associated with the appropriate documentation and review of the overall condition
(england.nhs.uk 2014). The rounding can be executed in daytime as well as in nighttimes or
sleep time. Both of these rounding have their individual significance in healthcare service and
assessments. However, in the taken scenario multiple issues are hindering the whole process
and its effectiveness. In this report the cause of these dilemma has been discussed by using
various strategic tools and techniques such as 5why root cause analysis, fishbone analysis.
After that, the possible risks have been also analysed by utilising risk management matrix.
After accumulation of crucial factors, the requirements for changes have been
discussed to formulate the PDSA (Plan Do Study Act) cycle of efficient development. Along
with the formulation of PDSA (Plan Do Study Act), the report has also assessed the required
leadership approach for making the changes sustainable and effective. Throughout this
process, ensuring the healthcare related compliance. With this regards, the appropriate
intervention of NHS regulations and code of conducts within the implementation procedure
of the development planning have been discussed. Moreover, the purpose of this report is to
find an appropriate development planning and implementation technique that can change the
existing condition of ineffective rounding and documentation anomaly. Through this
planning and development procedure, the health care organisation can uplift their entire
Introduction:
Intentional rounding is an essential part of healthcare and nursing facility where the
caregivers or nurses perform a direct assistive surveillance to identify any discrepancy in
patient’s health or physical condition such as falling injury, agitation, breathing issues and
others. Intentional rounding is also associated with care rounding every 1 hour during the day
to check on the 5 Ps, meal times, needs of assistance and others. The rounding is also
associated with the appropriate documentation and review of the overall condition
(england.nhs.uk 2014). The rounding can be executed in daytime as well as in nighttimes or
sleep time. Both of these rounding have their individual significance in healthcare service and
assessments. However, in the taken scenario multiple issues are hindering the whole process
and its effectiveness. In this report the cause of these dilemma has been discussed by using
various strategic tools and techniques such as 5why root cause analysis, fishbone analysis.
After that, the possible risks have been also analysed by utilising risk management matrix.
After accumulation of crucial factors, the requirements for changes have been
discussed to formulate the PDSA (Plan Do Study Act) cycle of efficient development. Along
with the formulation of PDSA (Plan Do Study Act), the report has also assessed the required
leadership approach for making the changes sustainable and effective. Throughout this
process, ensuring the healthcare related compliance. With this regards, the appropriate
intervention of NHS regulations and code of conducts within the implementation procedure
of the development planning have been discussed. Moreover, the purpose of this report is to
find an appropriate development planning and implementation technique that can change the
existing condition of ineffective rounding and documentation anomaly. Through this
planning and development procedure, the health care organisation can uplift their entire
3NURSING LEADERSHIP
facilities and the reputation within the consumers as well. At the same time, the caregivers
would have a new opportunity to enrich their professionalism and competency.
Analysis existing condition:
In this current scenario, multiple issues are hindering the whole process and its effectiveness
where the caregivers, nurses, nursing leaders are also involved. The issues that have been
found are follows:
In the geriatric ward, nurses and health care assistants including the shift leader
completing care rounding shift without physically checking on the patients
Only the patients that rang the bell here attended.
One patient was found lying on her back agitated and extremely wet during the
medication round
The shift leader appeared unworried indicating that it is not always possible to follow
the care plan especially at night when patients were sleeping
During the day shift, staff just ticked boxes without even speaking to the patients
As per the findings mentioned above the following root cause analysis has been performed to
identify the origin of all these dilemmas. In the following section the root causes of this
situation have been analysed with 5 Why analysis.
Root cause analysis (5 why)
Root cause analysis is the procedure of learning from consequences that is usually used by
the healthcare providers to gain acquaintance from near-misses, adverse events, or sentinel
events in the healthcare facility (England 2017). The following questions have been made
keeping the findings and major outcomes in mind.
Why are the patients not checked physically during the night shift?
facilities and the reputation within the consumers as well. At the same time, the caregivers
would have a new opportunity to enrich their professionalism and competency.
Analysis existing condition:
In this current scenario, multiple issues are hindering the whole process and its effectiveness
where the caregivers, nurses, nursing leaders are also involved. The issues that have been
found are follows:
In the geriatric ward, nurses and health care assistants including the shift leader
completing care rounding shift without physically checking on the patients
Only the patients that rang the bell here attended.
One patient was found lying on her back agitated and extremely wet during the
medication round
The shift leader appeared unworried indicating that it is not always possible to follow
the care plan especially at night when patients were sleeping
During the day shift, staff just ticked boxes without even speaking to the patients
As per the findings mentioned above the following root cause analysis has been performed to
identify the origin of all these dilemmas. In the following section the root causes of this
situation have been analysed with 5 Why analysis.
Root cause analysis (5 why)
Root cause analysis is the procedure of learning from consequences that is usually used by
the healthcare providers to gain acquaintance from near-misses, adverse events, or sentinel
events in the healthcare facility (England 2017). The following questions have been made
keeping the findings and major outcomes in mind.
Why are the patients not checked physically during the night shift?
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4NURSING LEADERSHIP
The healthcare governance system of this organisation provided a shift plan for all caregivers,
nurses and shift leader. However, the caregivers show a reluctant behaviour by seating in the
nurse’s room. They all know about the shift timing and procedures, but they have no will to
follow the rule and regulations.
Why do some patients become agitated in spite of having appropriate care plan?
During nighttimes rounding shift the patients only receive attention for the caregivers and
nurses when they ring the bell. Sometime, patients do not have the ability to ring the bell
properly and becomes agitated out of their helpless condition.
Why are there some argument about implementation of nigh shift routine within the staffs?
The management board of the healthcare facility warned the caregivers and nurses of nigh
shift repeatedly. However, the shift leader is equally inactive as the subordinate caregivers
and nurses. This problematic situation is causing the consistent argument within the
healthcare system of the organisation about the rounding procedure, especially in night shift.
Why are only the patients who ring the bell taken into observation and care?
Most of the nurses and caregivers are aware of their negligence and their faults in
professionalism. However, they are less likely to prioritise their duty over their relaxation. At
the same time, if a patient perceives complete ignorance in a vulnerable condition even after
ringing the bell all staffs of night shift will face the legal consequences in any case of lethal
and non lethal outcome (Sharma and Klocke 2014).
Why are not the nursing staffs communicating adequately with the patient even in day shifts?
The lack of monitoring procedure on staff’s activities allows them to perform inadequately
during their daytime shift. In spite of having set of well-structured regulations, the staffs
ignore the procedure and perform only the necessary duties. The healthcare staffs always
want to get rid of their daily work procedure and duties.
The healthcare governance system of this organisation provided a shift plan for all caregivers,
nurses and shift leader. However, the caregivers show a reluctant behaviour by seating in the
nurse’s room. They all know about the shift timing and procedures, but they have no will to
follow the rule and regulations.
Why do some patients become agitated in spite of having appropriate care plan?
During nighttimes rounding shift the patients only receive attention for the caregivers and
nurses when they ring the bell. Sometime, patients do not have the ability to ring the bell
properly and becomes agitated out of their helpless condition.
Why are there some argument about implementation of nigh shift routine within the staffs?
The management board of the healthcare facility warned the caregivers and nurses of nigh
shift repeatedly. However, the shift leader is equally inactive as the subordinate caregivers
and nurses. This problematic situation is causing the consistent argument within the
healthcare system of the organisation about the rounding procedure, especially in night shift.
Why are only the patients who ring the bell taken into observation and care?
Most of the nurses and caregivers are aware of their negligence and their faults in
professionalism. However, they are less likely to prioritise their duty over their relaxation. At
the same time, if a patient perceives complete ignorance in a vulnerable condition even after
ringing the bell all staffs of night shift will face the legal consequences in any case of lethal
and non lethal outcome (Sharma and Klocke 2014).
Why are not the nursing staffs communicating adequately with the patient even in day shifts?
The lack of monitoring procedure on staff’s activities allows them to perform inadequately
during their daytime shift. In spite of having set of well-structured regulations, the staffs
ignore the procedure and perform only the necessary duties. The healthcare staffs always
want to get rid of their daily work procedure and duties.
5NURSING LEADERSHIP
As per the above analysis of 5Why multiple operational anomalies have been found. The
major causes behind this inefficient workforce performance are listed below:
Lack of mentoring and control over the shift system, staffs and even leaders
Lack of effective enforcement of strict regulations and code of conduct
Inefficient leadership process
Lack of professional value and ethics within all staffs and leaders
Lack of effective administration over the execution procedure of duty planning
Lack of respect and dignity towards the patients
Ineffective documentation structure with inaccurate and irregular records
Lack of patient-care giver communication
Fish-bone analysis
Fishbone analysis is a process of examine the interconnections between attributes that
contribute to the result. The attributes are further classified by various operational fields such
as staff, process and others. In this case study, four major fields of attributes are involved that
cause the discrepancies within the care giving facility (Smith and Williams-Jones 2012).
These fields are Patient, Staff, Process and Environment. Here, Patient refers the care
receivers of the organisation who are the main victim of the work process dilemma. Staffs
represent the caregivers and nurses who are responsible to provide adequate care and
assessment to the patient within their shift timings. Process represents the existing execution
process of providing healthcare service to the patient. Environment emphasise the overall
external situation that stimulating the situation to worse.
As per the above analysis of 5Why multiple operational anomalies have been found. The
major causes behind this inefficient workforce performance are listed below:
Lack of mentoring and control over the shift system, staffs and even leaders
Lack of effective enforcement of strict regulations and code of conduct
Inefficient leadership process
Lack of professional value and ethics within all staffs and leaders
Lack of effective administration over the execution procedure of duty planning
Lack of respect and dignity towards the patients
Ineffective documentation structure with inaccurate and irregular records
Lack of patient-care giver communication
Fish-bone analysis
Fishbone analysis is a process of examine the interconnections between attributes that
contribute to the result. The attributes are further classified by various operational fields such
as staff, process and others. In this case study, four major fields of attributes are involved that
cause the discrepancies within the care giving facility (Smith and Williams-Jones 2012).
These fields are Patient, Staff, Process and Environment. Here, Patient refers the care
receivers of the organisation who are the main victim of the work process dilemma. Staffs
represent the caregivers and nurses who are responsible to provide adequate care and
assessment to the patient within their shift timings. Process represents the existing execution
process of providing healthcare service to the patient. Environment emphasise the overall
external situation that stimulating the situation to worse.
6NURSING LEADERSHIP
Inefficient
rounding and
poor workforce
performance
Patient Staff
Environment Process
Unable to
communicate
Physical and
mental insecurity
Feeling
Agitated
Reluctant
Irresponsible
No monitoring
process
Poor
leadership
Poor
regulation
enforcement
Lack of
teamwork
Poor
workplace
culture
Lack of
morale
and
dignity
Poor
Execution of
work
procedure
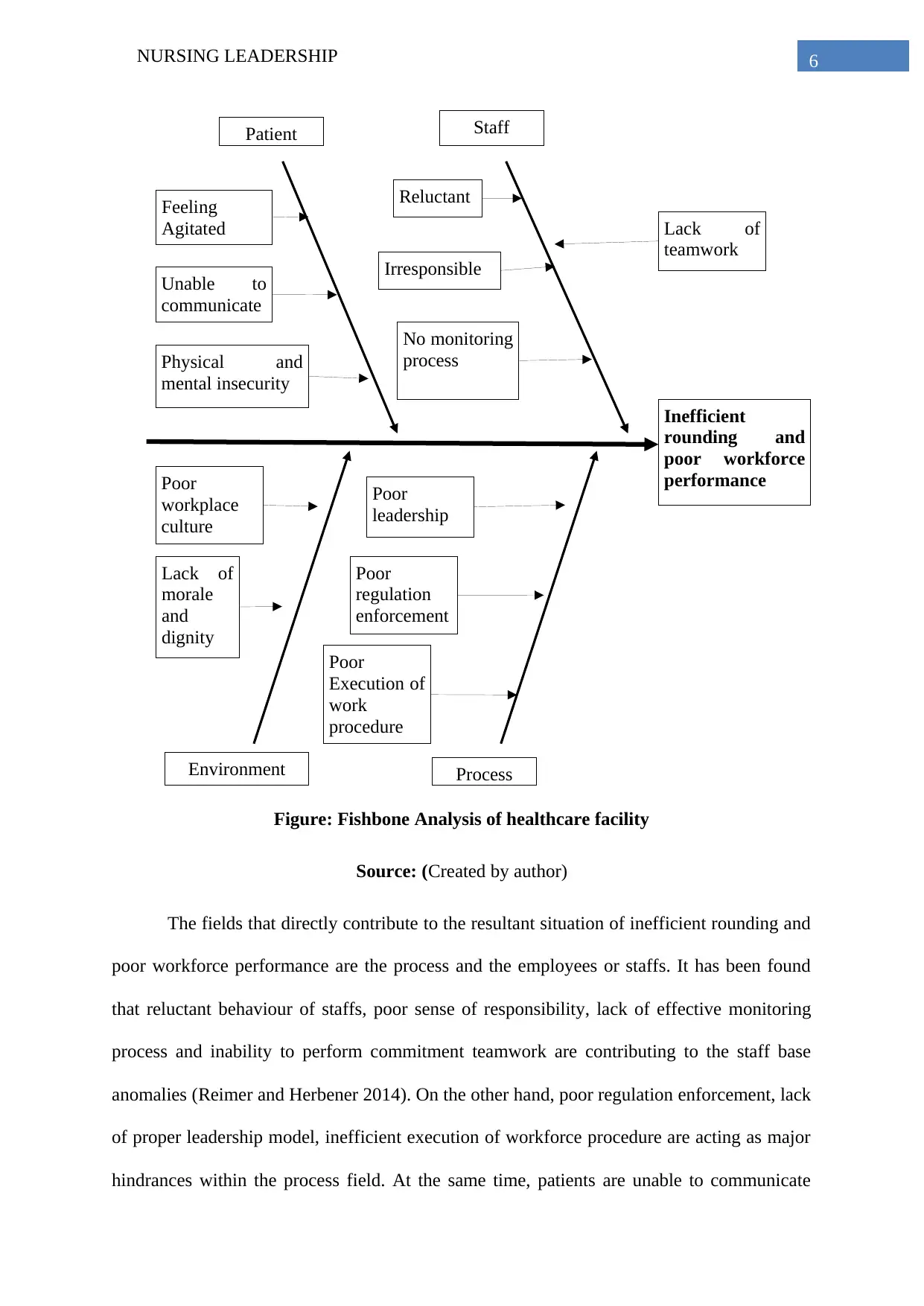
Figure: Fishbone Analysis of healthcare facility
Source: (Created by author)
The fields that directly contribute to the resultant situation of inefficient rounding and
poor workforce performance are the process and the employees or staffs. It has been found
that reluctant behaviour of staffs, poor sense of responsibility, lack of effective monitoring
process and inability to perform commitment teamwork are contributing to the staff base
anomalies (Reimer and Herbener 2014). On the other hand, poor regulation enforcement, lack
of proper leadership model, inefficient execution of workforce procedure are acting as major
hindrances within the process field. At the same time, patients are unable to communicate
Inefficient
rounding and
poor workforce
performance
Patient Staff
Environment Process
Unable to
communicate
Physical and
mental insecurity
Feeling
Agitated
Reluctant
Irresponsible
No monitoring
process
Poor
leadership
Poor
regulation
enforcement
Lack of
teamwork
Poor
workplace
culture
Lack of
morale
and
dignity
Poor
Execution of
work
procedure
Figure: Fishbone Analysis of healthcare facility
Source: (Created by author)
The fields that directly contribute to the resultant situation of inefficient rounding and
poor workforce performance are the process and the employees or staffs. It has been found
that reluctant behaviour of staffs, poor sense of responsibility, lack of effective monitoring
process and inability to perform commitment teamwork are contributing to the staff base
anomalies (Reimer and Herbener 2014). On the other hand, poor regulation enforcement, lack
of proper leadership model, inefficient execution of workforce procedure are acting as major
hindrances within the process field. At the same time, patients are unable to communicate
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7NURSING LEADERSHIP
which is also causing additional distress. Apart from that, consistence agitation and resultant
physical and mental insecurity are causing further dilemma from patient’s side. Another
essential field, which is contributing as a whole, is environment. Poor workforce culture with
lack of ethical consideration and morale are causing significant declination of healthy work
culture (Forde-Johnston 2014.). Along with the poor sense of respect and dignity to the
patients is causing additional hindrance. Therefore, it is clear that most of these causing
attributes have been generated due to the lack of administration, control and law enforcement.
Risk management and matrix:
The inefficient rounding process can cause several risk issues. Therefore, to eliminate
the risk issues the identification of those risks is highly crucial. Risk management is an
essential tool that can help to examine the existing factors that can cause serious hazards. The
risk factors have two separate parameters namely severity and likeliness. The severity
emphasise the impact of the risks on the system or organisation (Olrich, Kalman and Nigolian
2012). On the other hand, the likeliness represents the probability of occurrence of the risks.
A risk factor with higher possibility of occurrence has higher likeliness. Both severity and
likeliness contribute to the magnitude of the riskiness. In other words, the significance of any
risk equals to the product of the severity and the likeliness (Risk=Severity x Likeliness). As
per the existing situation of the healthcare organisation, the risk factors have been analysed
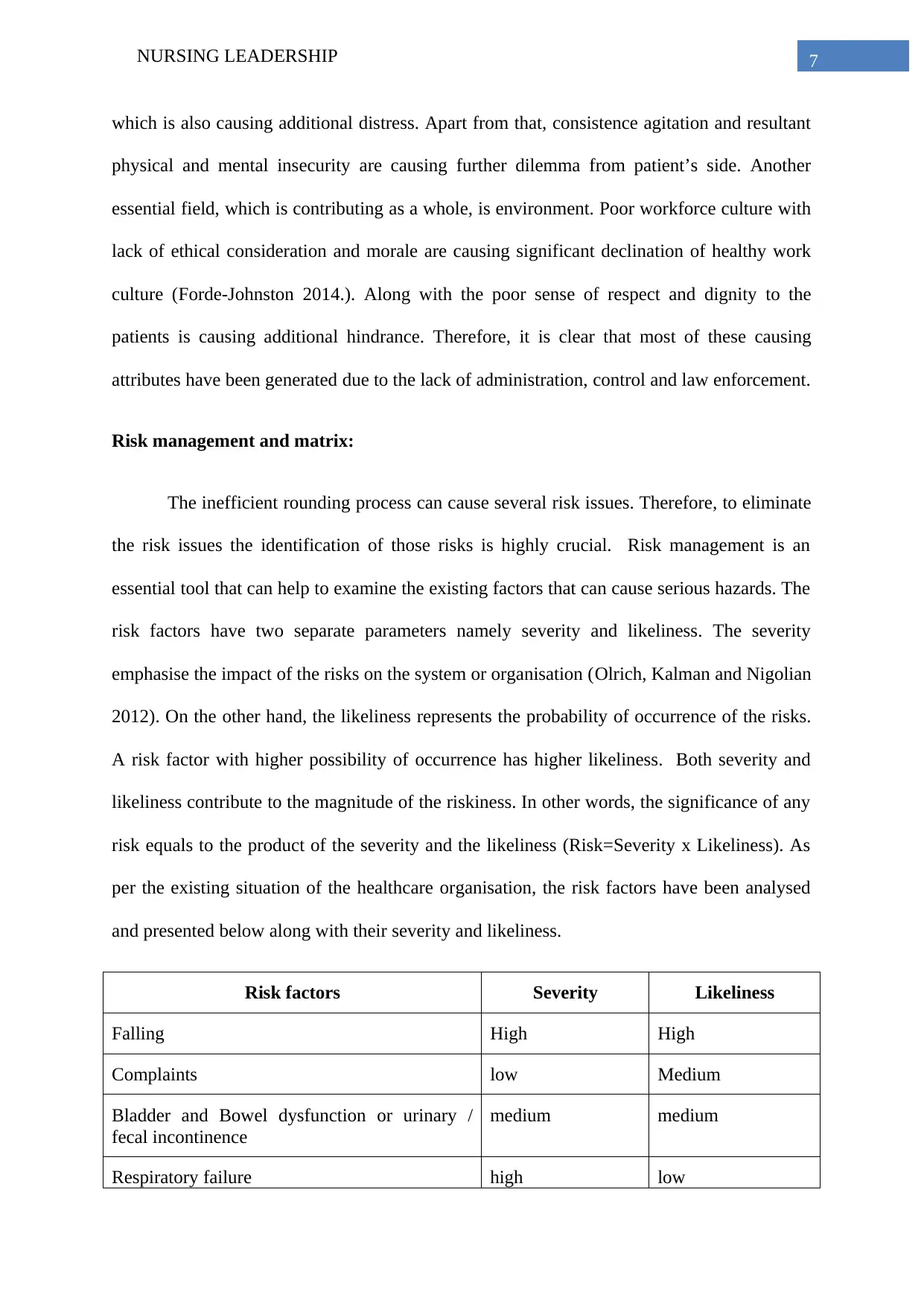
and presented below along with their severity and likeliness.
Risk factors Severity Likeliness
Falling High High
Complaints low Medium
Bladder and Bowel dysfunction or urinary /
fecal incontinence
medium medium
Respiratory failure high low
which is also causing additional distress. Apart from that, consistence agitation and resultant
physical and mental insecurity are causing further dilemma from patient’s side. Another
essential field, which is contributing as a whole, is environment. Poor workforce culture with
lack of ethical consideration and morale are causing significant declination of healthy work
culture (Forde-Johnston 2014.). Along with the poor sense of respect and dignity to the
patients is causing additional hindrance. Therefore, it is clear that most of these causing
attributes have been generated due to the lack of administration, control and law enforcement.
Risk management and matrix:
The inefficient rounding process can cause several risk issues. Therefore, to eliminate
the risk issues the identification of those risks is highly crucial. Risk management is an
essential tool that can help to examine the existing factors that can cause serious hazards. The
risk factors have two separate parameters namely severity and likeliness. The severity
emphasise the impact of the risks on the system or organisation (Olrich, Kalman and Nigolian
2012). On the other hand, the likeliness represents the probability of occurrence of the risks.
A risk factor with higher possibility of occurrence has higher likeliness. Both severity and
likeliness contribute to the magnitude of the riskiness. In other words, the significance of any
risk equals to the product of the severity and the likeliness (Risk=Severity x Likeliness). As
per the existing situation of the healthcare organisation, the risk factors have been analysed
and presented below along with their severity and likeliness.
Risk factors Severity Likeliness
Falling High High
Complaints low Medium
Bladder and Bowel dysfunction or urinary /
fecal incontinence
medium medium
Respiratory failure high low
8NURSING LEADERSHIP
Cardiac arrest high medium
Missing out treatment Medium low
Thirst or hunger of the patient medium high
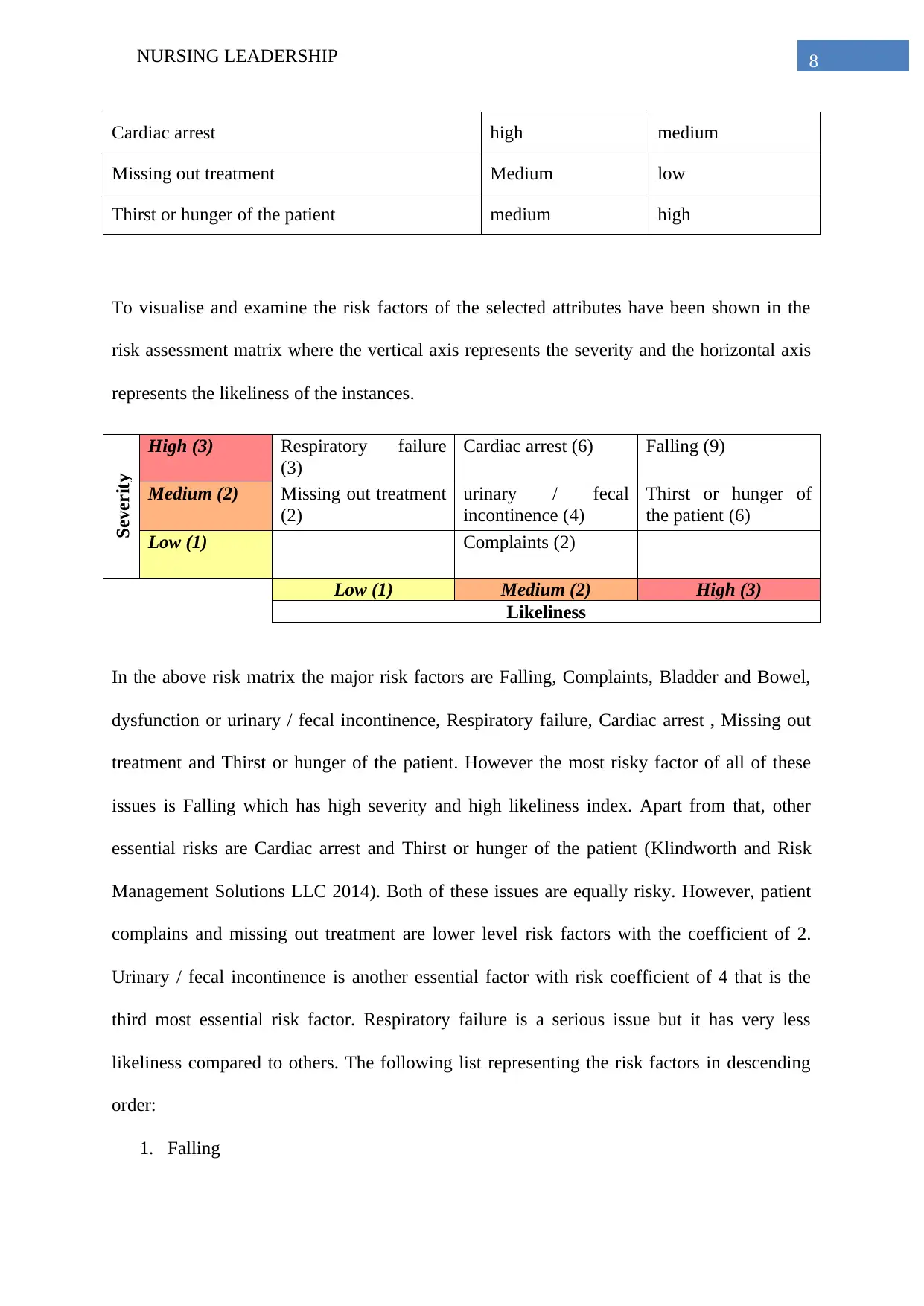
To visualise and examine the risk factors of the selected attributes have been shown in the
risk assessment matrix where the vertical axis represents the severity and the horizontal axis
represents the likeliness of the instances.
Severity
High (3) Respiratory failure
(3)
Cardiac arrest (6) Falling (9)
Medium (2) Missing out treatment
(2)
urinary / fecal
incontinence (4)
Thirst or hunger of
the patient (6)
Low (1) Complaints (2)
Low (1) Medium (2) High (3)
Likeliness
In the above risk matrix the major risk factors are Falling, Complaints, Bladder and Bowel,
dysfunction or urinary / fecal incontinence, Respiratory failure, Cardiac arrest , Missing out
treatment and Thirst or hunger of the patient. However the most risky factor of all of these
issues is Falling which has high severity and high likeliness index. Apart from that, other
essential risks are Cardiac arrest and Thirst or hunger of the patient (Klindworth and Risk
Management Solutions LLC 2014). Both of these issues are equally risky. However, patient
complains and missing out treatment are lower level risk factors with the coefficient of 2.
Urinary / fecal incontinence is another essential factor with risk coefficient of 4 that is the
third most essential risk factor. Respiratory failure is a serious issue but it has very less
likeliness compared to others. The following list representing the risk factors in descending
order:
1. Falling
Cardiac arrest high medium
Missing out treatment Medium low
Thirst or hunger of the patient medium high
To visualise and examine the risk factors of the selected attributes have been shown in the
risk assessment matrix where the vertical axis represents the severity and the horizontal axis
represents the likeliness of the instances.
Severity
High (3) Respiratory failure
(3)
Cardiac arrest (6) Falling (9)
Medium (2) Missing out treatment
(2)
urinary / fecal
incontinence (4)
Thirst or hunger of
the patient (6)
Low (1) Complaints (2)
Low (1) Medium (2) High (3)
Likeliness
In the above risk matrix the major risk factors are Falling, Complaints, Bladder and Bowel,
dysfunction or urinary / fecal incontinence, Respiratory failure, Cardiac arrest , Missing out
treatment and Thirst or hunger of the patient. However the most risky factor of all of these
issues is Falling which has high severity and high likeliness index. Apart from that, other
essential risks are Cardiac arrest and Thirst or hunger of the patient (Klindworth and Risk
Management Solutions LLC 2014). Both of these issues are equally risky. However, patient
complains and missing out treatment are lower level risk factors with the coefficient of 2.
Urinary / fecal incontinence is another essential factor with risk coefficient of 4 that is the
third most essential risk factor. Respiratory failure is a serious issue but it has very less
likeliness compared to others. The following list representing the risk factors in descending
order:
1. Falling
9NURSING LEADERSHIP
2. Cardiac arrest
3. Thirst or hunger of the patient
4. Urinary / fecal incontinence
5. Missing out treatment
6. Complaints
Required Changes
As per the above analysis, it has been found that several issues are causing the
operational discrepancies in rounding system in day as well as nigh shifts. At the same time,
some essential risk factors are also associated with these regulators. According to fish bone
analysis reluctant behaviour of staffs, poor sense of responsibility, lack of effective
monitoring process, inability to perform commitment teamwork, poor regulation
enforcement, lack of proper leadership model, inefficient execution of workforce procedure,
lack of ethical consideration, poor sense of respect and dignity to the patients have been
found to be the major hindrances. Therefore, in further development plan of the healthcare
organisation some major changes are required including:
Persistent and effective workforce training
Appropriate enforcement of regulations and code of conducts
Rescheduling the resource allocation that will allow the employees to alter
their shifts
Increase surveillance and monitoring system on the staffs
Implementing appropriate leadership model to handle the situation and the role
of the caregivers perfectly
Increasing the healthy communication between patients and caregivers to
highlight the key problems
2. Cardiac arrest
3. Thirst or hunger of the patient
4. Urinary / fecal incontinence
5. Missing out treatment
6. Complaints
Required Changes
As per the above analysis, it has been found that several issues are causing the
operational discrepancies in rounding system in day as well as nigh shifts. At the same time,
some essential risk factors are also associated with these regulators. According to fish bone
analysis reluctant behaviour of staffs, poor sense of responsibility, lack of effective
monitoring process, inability to perform commitment teamwork, poor regulation
enforcement, lack of proper leadership model, inefficient execution of workforce procedure,
lack of ethical consideration, poor sense of respect and dignity to the patients have been
found to be the major hindrances. Therefore, in further development plan of the healthcare
organisation some major changes are required including:
Persistent and effective workforce training
Appropriate enforcement of regulations and code of conducts
Rescheduling the resource allocation that will allow the employees to alter
their shifts
Increase surveillance and monitoring system on the staffs
Implementing appropriate leadership model to handle the situation and the role
of the caregivers perfectly
Increasing the healthy communication between patients and caregivers to
highlight the key problems
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10NURSING LEADERSHIP
Conducting repeated meeting to encourage the staffs about their job and
responsibilities
In order to implement the changes the management of the organization should express
the core problems and the potential outcomes of the existing dilemmas in the work process
and execution (Card, Ward and Clarkson 2012). This process could be executed with the
helpful interference of Human Resource Management System. Initially the resistance against
these changes should be minimised through appropriate leadership and communication. Then
the change management process including defreeze, change and freeze phase that allow the
administration to introduce the new policies and process, then incorporating the change and
finally to evaluate the sustainability and accuracy. The recognition and rewarding are other
effective evaluation procedures that will help to increase the proficiency of the workforce
(Wingate 2016). Throughout the change management procedure the essential risk factors
including Patient Falling, Cardiac arrest, Sudden Thirst or hunger of the patient, Urinary /
fecal incontinence, Missing out treatment and Complaints of the patients should be chiefly
considered.
PDSA (Plan Do Study Act):
The PDSA or Plan Do Study Act is a cyclic model of implementing or developing
new process, system and workflow. The plan phase emphasises the designing and finding the
appropriate process of execution that would help to achieve the objectives. The Do phase
refers the execution process where, appropriate control and implementation plan are required.
The Study phase reflects the assessment part of the executed plan that includes the
examination of efficiency, tangibility, affectivity, potentiality and scope of farther
improvement. The major objectives of this PDSA model are incorporating the code of
Conducting repeated meeting to encourage the staffs about their job and
responsibilities
In order to implement the changes the management of the organization should express
the core problems and the potential outcomes of the existing dilemmas in the work process
and execution (Card, Ward and Clarkson 2012). This process could be executed with the
helpful interference of Human Resource Management System. Initially the resistance against
these changes should be minimised through appropriate leadership and communication. Then
the change management process including defreeze, change and freeze phase that allow the
administration to introduce the new policies and process, then incorporating the change and
finally to evaluate the sustainability and accuracy. The recognition and rewarding are other
effective evaluation procedures that will help to increase the proficiency of the workforce
(Wingate 2016). Throughout the change management procedure the essential risk factors
including Patient Falling, Cardiac arrest, Sudden Thirst or hunger of the patient, Urinary /
fecal incontinence, Missing out treatment and Complaints of the patients should be chiefly
considered.
PDSA (Plan Do Study Act):
The PDSA or Plan Do Study Act is a cyclic model of implementing or developing
new process, system and workflow. The plan phase emphasises the designing and finding the
appropriate process of execution that would help to achieve the objectives. The Do phase
refers the execution process where, appropriate control and implementation plan are required.
The Study phase reflects the assessment part of the executed plan that includes the
examination of efficiency, tangibility, affectivity, potentiality and scope of farther
improvement. The major objectives of this PDSA model are incorporating the code of
11NURSING LEADERSHIP
Incorporate the code of
conducts for the staffs
Increasing patient-
caregiver communication
Eliminating potential risks
from inefficient rounding
Do
Executing the process of
training, development and
implementation of
rounding
Act
Finding our required
changes in the existing
process
Plan
Developing effective
regulation and controlling
process
Study
Ensure effective
monitoring and
documentation for
assessment
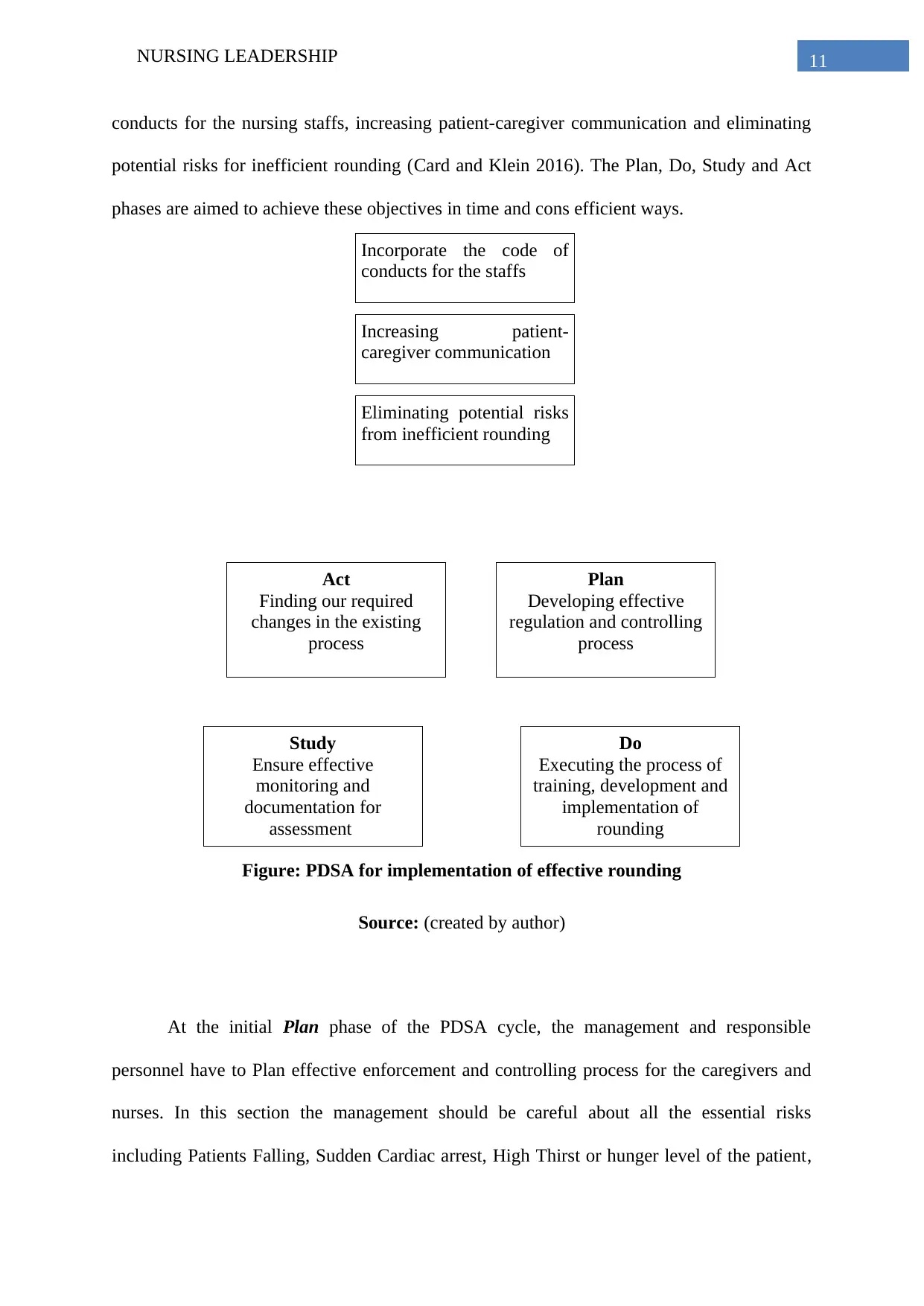
conducts for the nursing staffs, increasing patient-caregiver communication and eliminating
potential risks for inefficient rounding (Card and Klein 2016). The Plan, Do, Study and Act
phases are aimed to achieve these objectives in time and cons efficient ways.
Figure: PDSA for implementation of effective rounding
Source: (created by author)
At the initial Plan phase of the PDSA cycle, the management and responsible
personnel have to Plan effective enforcement and controlling process for the caregivers and
nurses. In this section the management should be careful about all the essential risks
including Patients Falling, Sudden Cardiac arrest, High Thirst or hunger level of the patient,
Incorporate the code of
conducts for the staffs
Increasing patient-
caregiver communication
Eliminating potential risks
from inefficient rounding
Do
Executing the process of
training, development and
implementation of
rounding
Act
Finding our required
changes in the existing
process
Plan
Developing effective
regulation and controlling
process
Study
Ensure effective
monitoring and
documentation for
assessment
conducts for the nursing staffs, increasing patient-caregiver communication and eliminating
potential risks for inefficient rounding (Card and Klein 2016). The Plan, Do, Study and Act
phases are aimed to achieve these objectives in time and cons efficient ways.
Figure: PDSA for implementation of effective rounding
Source: (created by author)
At the initial Plan phase of the PDSA cycle, the management and responsible
personnel have to Plan effective enforcement and controlling process for the caregivers and
nurses. In this section the management should be careful about all the essential risks
including Patients Falling, Sudden Cardiac arrest, High Thirst or hunger level of the patient,
12NURSING LEADERSHIP
Urinary / fecal incontinence, Missing out treatment and patient’s Complaints. The further
phase of PDSA cycle depends on this Planning phase. The next phase is the execution phase
also known as Do phase. In this phase, the management and administrator of the organisation
have to execute effective training and development module for new as well as for existing
nursing staffs and caregivers in order to ensure that they have enough knowledge and
reliability to conduct rounding process regularly (Baathe et al. 2014). Apart from that, the
training method should also ensure that the nursing staffs have enough morale, value about
their duties and responsibilities while having appropriate dignity towards the patients needs,
culture and experiences. It will help to increase the communicational efficiency within the
patient and caregivers as well.
The Study phase requires effective monitoring and documentation system that will
help analysing the loop whole within the existing implementation procedure. Both direct and
indirect monitoring is effective in this situation. The direct monitoring can be executing by
direct surveillance by leaders, checking documents and other supervisors (Cornell et al.
2014). On the other hand, indirect monitoring will help to collect data through collecting
feedback from peers and patients. Lastly, the Act phase will help find out required changes in
the existing process that can make the updated execution plan more efficient and effective. It
is the foundation phase of the planning phase. In this section the outcomes of the executed
procedures are analysed by aligning them with the three objectives namely incorporating the
code of conducts for the nursing staffs, increasing patient-caregiver communication and
eliminating potential risks for inefficient rounding.
Implementation of leadership
In healthcare service providing effective leadership is an essential factors that enables
the other factors to achieve the objectives of the organisation. However, in this case study the
Urinary / fecal incontinence, Missing out treatment and patient’s Complaints. The further
phase of PDSA cycle depends on this Planning phase. The next phase is the execution phase
also known as Do phase. In this phase, the management and administrator of the organisation
have to execute effective training and development module for new as well as for existing
nursing staffs and caregivers in order to ensure that they have enough knowledge and
reliability to conduct rounding process regularly (Baathe et al. 2014). Apart from that, the
training method should also ensure that the nursing staffs have enough morale, value about
their duties and responsibilities while having appropriate dignity towards the patients needs,
culture and experiences. It will help to increase the communicational efficiency within the
patient and caregivers as well.
The Study phase requires effective monitoring and documentation system that will
help analysing the loop whole within the existing implementation procedure. Both direct and
indirect monitoring is effective in this situation. The direct monitoring can be executing by
direct surveillance by leaders, checking documents and other supervisors (Cornell et al.
2014). On the other hand, indirect monitoring will help to collect data through collecting
feedback from peers and patients. Lastly, the Act phase will help find out required changes in
the existing process that can make the updated execution plan more efficient and effective. It
is the foundation phase of the planning phase. In this section the outcomes of the executed
procedures are analysed by aligning them with the three objectives namely incorporating the
code of conducts for the nursing staffs, increasing patient-caregiver communication and
eliminating potential risks for inefficient rounding.
Implementation of leadership
In healthcare service providing effective leadership is an essential factors that enables
the other factors to achieve the objectives of the organisation. However, in this case study the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
13NURSING LEADERSHIP
shift leader is supportive to the subordinates about their reluctance to perform the duties and
responsibilities to execute effective and efficient rounding process while making appropriate
interaction with the patients. In this situation, an effective leader should keep the
communication and encouraging interaction with the subordinate to support the management,
to prioritise the patient safety and satisfaction, to sustain the mission, vision and values within
the employees (Al-Sawai 2013). The appropriate time allocation to the caregivers and other
staffs can enhance the overall quality of care giving. Apart from that it is the duty of every
leader to promote the nursing excellence and optional patient outcomes to the tame member
while increasing the awareness of teamwork and integration within the workforce (Delmatoff
and Lazarus, 2014). All of these factors will act together to decrease the patient falls and
other negligence related outcomes such as Cardiac arrest, Thirst or hunger of the patient,
Urinary / fecal incontinence, Missing out treatment and others.
A leader should take care of some of the essential duties such as Valuing the service
ethics while being curious about how to improve services and patient care. Apart from that
the leader should behave in a way that reflects the principles and values of the NHS within
the workforce. A successful leader also creates a shared purpose, where diverse individuals
can do different work and the leader can inspire them to believe in shared values to enable
them delivering benefits for patients, their families and the community. Another crucial factor
of a leader in healthcare service is Staying true to NHS principles and values while holding to
principles and values in own work process to be ideal example of a perfect caregiver (Cliff
2012.). A leader should never hesitate to take personal risks in order to stand up for the
shared purpose or to encourage the team members for the benefit of the service. At the same
time a Leader should understand the underlying emotions of every team members that affect
their team, and care for team members as individuals by helping them to manage unsettling
feelings so that they can focus on their work to deliver a competent service.
shift leader is supportive to the subordinates about their reluctance to perform the duties and
responsibilities to execute effective and efficient rounding process while making appropriate
interaction with the patients. In this situation, an effective leader should keep the
communication and encouraging interaction with the subordinate to support the management,
to prioritise the patient safety and satisfaction, to sustain the mission, vision and values within
the employees (Al-Sawai 2013). The appropriate time allocation to the caregivers and other
staffs can enhance the overall quality of care giving. Apart from that it is the duty of every
leader to promote the nursing excellence and optional patient outcomes to the tame member
while increasing the awareness of teamwork and integration within the workforce (Delmatoff
and Lazarus, 2014). All of these factors will act together to decrease the patient falls and
other negligence related outcomes such as Cardiac arrest, Thirst or hunger of the patient,
Urinary / fecal incontinence, Missing out treatment and others.
A leader should take care of some of the essential duties such as Valuing the service
ethics while being curious about how to improve services and patient care. Apart from that
the leader should behave in a way that reflects the principles and values of the NHS within
the workforce. A successful leader also creates a shared purpose, where diverse individuals
can do different work and the leader can inspire them to believe in shared values to enable
them delivering benefits for patients, their families and the community. Another crucial factor
of a leader in healthcare service is Staying true to NHS principles and values while holding to
principles and values in own work process to be ideal example of a perfect caregiver (Cliff
2012.). A leader should never hesitate to take personal risks in order to stand up for the
shared purpose or to encourage the team members for the benefit of the service. At the same
time a Leader should understand the underlying emotions of every team members that affect
their team, and care for team members as individuals by helping them to manage unsettling
feelings so that they can focus on their work to deliver a competent service.
14NURSING LEADERSHIP
A System leadership does not enable the leader to working behind the scenes rather
than leading from the front for achieving the success of the team as well as the quality of the
overall healthcare system. However, as per the unprecedented challenges faced by the NHS,
the system leaders need to motivate staff and managers to work differently, across service
and organisational boundaries while aiming towards same purpose of serving the patients
(Edmonstone 2013). The system leadership is the only way to meet the needs and expectation
of the growing number of patient with complex and long-term conditions. Moreover, system
leader should take care of valuing the service ethics while being curious about the
improvement services and patient care through leading the team member abiding by the code
of conducts, rules, regulations and guidance by NHS.
Implementation of NHS Framework
The new regulation and rounding procedure should be aligned with the regulation of
Patient Care Regulation by National Health Service of UK. Therefore for this organisation
the care rounding should be executed in every 1 hour during the day as well as night in order
to check on the 5 Ps – pain, position, pulse, paralysis and paraesthesia of the patients. In night
shift the two hours of frequent rounding is essential event when the patients are awoke. This
procedure cannot be skipped irrespective of the alteration of risk assessments, care plans
(Daly et al. 2014).
Apart from that as per the Healthcare Service Providing Checklist proposed by NHS
the ward managers, as an essential part of the ward documentation audits should regularly
check all of these procedures regarding shift timing, rounding and the implementation of 5p.
Apart from that, the consequences of noncompliance or irregularities should be regularly
usually discussed in staff meetings. Lack of compliance and efficiency may not only
devastating to patients but can result in huge costs by the NHS in terms of treatment, length
A System leadership does not enable the leader to working behind the scenes rather
than leading from the front for achieving the success of the team as well as the quality of the
overall healthcare system. However, as per the unprecedented challenges faced by the NHS,
the system leaders need to motivate staff and managers to work differently, across service
and organisational boundaries while aiming towards same purpose of serving the patients
(Edmonstone 2013). The system leadership is the only way to meet the needs and expectation
of the growing number of patient with complex and long-term conditions. Moreover, system
leader should take care of valuing the service ethics while being curious about the
improvement services and patient care through leading the team member abiding by the code
of conducts, rules, regulations and guidance by NHS.
Implementation of NHS Framework
The new regulation and rounding procedure should be aligned with the regulation of
Patient Care Regulation by National Health Service of UK. Therefore for this organisation
the care rounding should be executed in every 1 hour during the day as well as night in order
to check on the 5 Ps – pain, position, pulse, paralysis and paraesthesia of the patients. In night
shift the two hours of frequent rounding is essential event when the patients are awoke. This
procedure cannot be skipped irrespective of the alteration of risk assessments, care plans
(Daly et al. 2014).
Apart from that as per the Healthcare Service Providing Checklist proposed by NHS
the ward managers, as an essential part of the ward documentation audits should regularly
check all of these procedures regarding shift timing, rounding and the implementation of 5p.
Apart from that, the consequences of noncompliance or irregularities should be regularly
usually discussed in staff meetings. Lack of compliance and efficiency may not only
devastating to patients but can result in huge costs by the NHS in terms of treatment, length
15NURSING LEADERSHIP
of day, continuing care, death and litigation (van Rossum et al. 2016). All of these factors
influence the reputation of the organisation as well as the regulatory operation of the NHS at
national level as well.
As per the published report of NHS digital in 2017, Health safety thermometer, prevalence of
pressure ulcers and falls resulting in harm were approximately 4.4% and 0.6% in 2017
respectively (england.nhs.uk 2014). It is not the situation of a particular area of the nation,
rather it reflects the overall situation of healthcare facilities which are under the governance
of NHS UK. There are many healthcare execution techniques proposed by NICE guidelines
that can be very helpful during the planning and implementation phase. According to NICE
guideline G179 of 2014, some recommend expert assessment and regular reposition of adults
for risk management and developing effective rounding plan can be helpful for the healthcare
organisation to maintain the compliance more easily (England 2017).
According to the Parliamentary and Health Services Ombudsman and Department of
Health and the term “basic nursing care” – attending to patients’ emphasise the needs for
support with feeding, positioning, personal hygiene and skin integrity. Along with that, the
training method should also ensure that the nursing staffs have enough morale, value about
their duties and responsibilities while having appropriate dignity towards the patients needs,
culture and experiences (england.nhs.uk 2014). These procedures also reflect the assessment
part of the executed plan that includes the examination of efficiency, tangibility, affectivity,
potentiality and scope of farther improvement.
Conclusion:
From the above analysis and discussion, it can be said that Intentional rounding is an
essential part of healthcare and nursing facility where the caregivers or nurses perform a
direct assistive surveillance to identify any discrepancy in patient’s health or physical
of day, continuing care, death and litigation (van Rossum et al. 2016). All of these factors
influence the reputation of the organisation as well as the regulatory operation of the NHS at
national level as well.
As per the published report of NHS digital in 2017, Health safety thermometer, prevalence of
pressure ulcers and falls resulting in harm were approximately 4.4% and 0.6% in 2017
respectively (england.nhs.uk 2014). It is not the situation of a particular area of the nation,
rather it reflects the overall situation of healthcare facilities which are under the governance
of NHS UK. There are many healthcare execution techniques proposed by NICE guidelines
that can be very helpful during the planning and implementation phase. According to NICE
guideline G179 of 2014, some recommend expert assessment and regular reposition of adults
for risk management and developing effective rounding plan can be helpful for the healthcare
organisation to maintain the compliance more easily (England 2017).
According to the Parliamentary and Health Services Ombudsman and Department of
Health and the term “basic nursing care” – attending to patients’ emphasise the needs for
support with feeding, positioning, personal hygiene and skin integrity. Along with that, the
training method should also ensure that the nursing staffs have enough morale, value about
their duties and responsibilities while having appropriate dignity towards the patients needs,
culture and experiences (england.nhs.uk 2014). These procedures also reflect the assessment
part of the executed plan that includes the examination of efficiency, tangibility, affectivity,
potentiality and scope of farther improvement.
Conclusion:
From the above analysis and discussion, it can be said that Intentional rounding is an
essential part of healthcare and nursing facility where the caregivers or nurses perform a
direct assistive surveillance to identify any discrepancy in patient’s health or physical
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
16NURSING LEADERSHIP
condition such as falling injury, agitation, breathing issues and others. Throughout this study,
the purpose was to ensure the healthcare related compliance with regards to the appropriate
intervention of NHS regulations and code of conducts within the implementation procedure
of the development planning. In the discussed scenario, multiple issues are hindering the
whole process and its effectiveness where the caregivers, nurses, nursing leaders are also
involved. The caregivers and shift leader show a reluctant behaviour by seating in the nurse’s
room. They all know about the shift timing and procedures, but they have no will to follow
the rule and regulations.
As per the above analysis it can be concluded that the major causes behind the issues are
Lack of mentoring and control over the shift system, Lack of effective enforcement of strict
regulations, Inefficient leadership process, Lack of professional value and ethics within all
staffs, Lack of respect and dignity towards the patients. As per the risk assessment it has been
found that Falling, Cardiac arrest, Thirst or hunger of the patient, Urinary / fecal
incontinence, Missing out treatment, Patient Complaints are the major risks. Some changes
are required to resolve these issues, such as Persistent and effective workforce training,
Appropriate enforcement of regulations and code of conducts, Rescheduling the resource
allocation, Increase surveillance and monitoring system, Implementing appropriate system
leadership model, Increasing the healthy communication between patients and caregivers.
With this regareds, the PDSA or Plan Do Study Act cyclic model will be helpful for
implementing or developing new process, system and workflow. Moreover, it has been found
that in healthcare service providing, effective system leadership is an essential factor that
enables the other factors to achieve the objectives of the organisation.
condition such as falling injury, agitation, breathing issues and others. Throughout this study,
the purpose was to ensure the healthcare related compliance with regards to the appropriate
intervention of NHS regulations and code of conducts within the implementation procedure
of the development planning. In the discussed scenario, multiple issues are hindering the
whole process and its effectiveness where the caregivers, nurses, nursing leaders are also
involved. The caregivers and shift leader show a reluctant behaviour by seating in the nurse’s
room. They all know about the shift timing and procedures, but they have no will to follow
the rule and regulations.
As per the above analysis it can be concluded that the major causes behind the issues are
Lack of mentoring and control over the shift system, Lack of effective enforcement of strict
regulations, Inefficient leadership process, Lack of professional value and ethics within all
staffs, Lack of respect and dignity towards the patients. As per the risk assessment it has been
found that Falling, Cardiac arrest, Thirst or hunger of the patient, Urinary / fecal
incontinence, Missing out treatment, Patient Complaints are the major risks. Some changes
are required to resolve these issues, such as Persistent and effective workforce training,
Appropriate enforcement of regulations and code of conducts, Rescheduling the resource
allocation, Increase surveillance and monitoring system, Implementing appropriate system
leadership model, Increasing the healthy communication between patients and caregivers.
With this regareds, the PDSA or Plan Do Study Act cyclic model will be helpful for
implementing or developing new process, system and workflow. Moreover, it has been found
that in healthcare service providing, effective system leadership is an essential factor that
enables the other factors to achieve the objectives of the organisation.

17NURSING LEADERSHIP
18NURSING LEADERSHIP
Reference:
Al-Sawai, A., 2013. Leadership of healthcare professionals: where do we stand?. Oman
medical journal, 28(4), p.285.
Baathe, F., Ahlborg Jr, G., Lagström, A., Edgren, L. and Nilsson, K., 2014. Physician
experiences of patient-centered and team-based ward rounding–an interview based case-
study. Journal of Hospital Administration, 3(6), p.127.
Card, A.J. and Klein, V.R., 2016. A new frontier in healthcare risk management: working to
reduce avoidable patient suffering. Journal of Healthcare Risk Management, 35(3), pp.31-37.
Card, A.J., Ward, J.R. and Clarkson, P.J., 2012. Getting to Zero: Evidence‐based healthcare
risk management is key. Journal of Healthcare Risk Management, 32(2), pp.20-27.
Cliff, B., 2012. Patient-centered care: The role of healthcare leadership. Journal of
Healthcare Management, 57(6), pp.381-383.
Cornell, P., Gervis, M.T., Yates, L. and Vardaman, J.M., 2014. Impact of SBAR on nurse
shift reports and staff rounding. Medsurg nursing, 23(5), p.334.
Daly, J., Jackson, D., Mannix, J., Davidson, P.M. and Hutchinson, M., 2014. The importance
of clinical leadership in the hospital setting. Journal of Healthcare Leadership, 6, pp.75-83.
Delmatoff, J. and Lazarus, I.R., 2014. The most effective leadership style for the new
landscape of healthcare. Journal of Healthcare Management, 59(4), pp.245-249.
Edmonstone, J., 2013. Healthcare leadership: learning from evaluation. Leadership in Health
Services, 26(2), pp.148-158.
Reference:
Al-Sawai, A., 2013. Leadership of healthcare professionals: where do we stand?. Oman
medical journal, 28(4), p.285.
Baathe, F., Ahlborg Jr, G., Lagström, A., Edgren, L. and Nilsson, K., 2014. Physician
experiences of patient-centered and team-based ward rounding–an interview based case-
study. Journal of Hospital Administration, 3(6), p.127.
Card, A.J. and Klein, V.R., 2016. A new frontier in healthcare risk management: working to
reduce avoidable patient suffering. Journal of Healthcare Risk Management, 35(3), pp.31-37.
Card, A.J., Ward, J.R. and Clarkson, P.J., 2012. Getting to Zero: Evidence‐based healthcare
risk management is key. Journal of Healthcare Risk Management, 32(2), pp.20-27.
Cliff, B., 2012. Patient-centered care: The role of healthcare leadership. Journal of
Healthcare Management, 57(6), pp.381-383.
Cornell, P., Gervis, M.T., Yates, L. and Vardaman, J.M., 2014. Impact of SBAR on nurse
shift reports and staff rounding. Medsurg nursing, 23(5), p.334.
Daly, J., Jackson, D., Mannix, J., Davidson, P.M. and Hutchinson, M., 2014. The importance
of clinical leadership in the hospital setting. Journal of Healthcare Leadership, 6, pp.75-83.
Delmatoff, J. and Lazarus, I.R., 2014. The most effective leadership style for the new
landscape of healthcare. Journal of Healthcare Management, 59(4), pp.245-249.
Edmonstone, J., 2013. Healthcare leadership: learning from evaluation. Leadership in Health
Services, 26(2), pp.148-158.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
19NURSING LEADERSHIP
England, N. 2017. NHS England » Sustainability and transformation partnerships. [online]
England.nhs.uk. Available at: https://www.england.nhs.uk/integratedcare/stps/ [Accessed 16
Aug. 2018].
england.nhs.uk 2014. wp-content. [online] England.nhs.uk. Available at:
https://www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf [Accessed 16 Aug.
2018].
Forde-Johnston, C., 2014. Intentional rounding: a review of the literature. Nursing
Standard, 28(32).
Klindworth, W.A., Risk Management Solutions LLC, 2014. Automated Healthcare Risk
Management System Utilizing Real-time Predictive Models, Risk Adjusted Provider Cost
Index, Edit Analytics, Strategy Management, Managed Learning Environment, Contact
Management, Forensic GUI, Case Management And Reporting System For Preventing And
Detecting Healthcare Fraud, Abuse, Waste And Errors. U.S. Patent Application 14/027,193.
Olrich, T., Kalman, M. and Nigolian, C., 2012. Hourly rounding: a replication
study. Medsurg Nursing, 21(1).
Reimer, N. and Herbener, L., 2014. Round and round we go: rounding strategies to impact
exemplary professional practice. Clinical journal of oncology nursing, 18(6).
Sharma, U. and Klocke, D., 2014. Attitudes of nursing staff toward interprofessional in-
patient-centered rounding. Journal of interprofessional care, 28(5), pp.475-477.
Smith, C.B. and Williams-Jones, P., 2012. Tips to reduce dangerous interruptions by
healthcare staff. Nursing2018, 42(11), pp.65-67.
van Rossum, L., Aij, K.H., Simons, F.E., van der Eng, N. and ten Have, W.D., 2016. Lean
healthcare from a change management perspective: The role of leadership and workforce
England, N. 2017. NHS England » Sustainability and transformation partnerships. [online]
England.nhs.uk. Available at: https://www.england.nhs.uk/integratedcare/stps/ [Accessed 16
Aug. 2018].
england.nhs.uk 2014. wp-content. [online] England.nhs.uk. Available at:
https://www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf [Accessed 16 Aug.
2018].
Forde-Johnston, C., 2014. Intentional rounding: a review of the literature. Nursing
Standard, 28(32).
Klindworth, W.A., Risk Management Solutions LLC, 2014. Automated Healthcare Risk
Management System Utilizing Real-time Predictive Models, Risk Adjusted Provider Cost
Index, Edit Analytics, Strategy Management, Managed Learning Environment, Contact
Management, Forensic GUI, Case Management And Reporting System For Preventing And
Detecting Healthcare Fraud, Abuse, Waste And Errors. U.S. Patent Application 14/027,193.
Olrich, T., Kalman, M. and Nigolian, C., 2012. Hourly rounding: a replication
study. Medsurg Nursing, 21(1).
Reimer, N. and Herbener, L., 2014. Round and round we go: rounding strategies to impact
exemplary professional practice. Clinical journal of oncology nursing, 18(6).
Sharma, U. and Klocke, D., 2014. Attitudes of nursing staff toward interprofessional in-
patient-centered rounding. Journal of interprofessional care, 28(5), pp.475-477.
Smith, C.B. and Williams-Jones, P., 2012. Tips to reduce dangerous interruptions by
healthcare staff. Nursing2018, 42(11), pp.65-67.
van Rossum, L., Aij, K.H., Simons, F.E., van der Eng, N. and ten Have, W.D., 2016. Lean
healthcare from a change management perspective: The role of leadership and workforce
20NURSING LEADERSHIP
flexibility in an operating theatre. Journal of health organization and management, 30(3),
pp.475-493.
Wingate, G., 2016. Computer systems validation: quality assurance, risk management, and
regulatory compliance for pharmaceutical and healthcare companies. CRC Press.
flexibility in an operating theatre. Journal of health organization and management, 30(3),
pp.475-493.
Wingate, G., 2016. Computer systems validation: quality assurance, risk management, and
regulatory compliance for pharmaceutical and healthcare companies. CRC Press.
1 out of 21
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.