Nursing Case Study: Wound Assessment, Pathophysiology, and Management
VerifiedAdded on 2022/11/15
|13
|3654
|434
Case Study
AI Summary
This case study presents a comprehensive analysis of a 64-year-old female patient, Mrs. A, with a wound on her right calf muscle, focusing on wound assessment, pathophysiology, and nursing management. The patient's medical history includes anaemia, coronary artery disease, and hypertension, along with lifestyle factors like smoking and a poor diet, which are explored as factors influencing wound healing. The assessment details the wound's characteristics, including dimensions, appearance, and exudate. The study delves into the pathophysiology, identifying potential causes such as pressure ulceration from tight-fitting socks and the impact of diabetes and hypertension on wound healing. It discusses relevant clinical investigations, including blood glucose, iron, and lipoprotein levels, highlighting how these factors interfere with the healing process. Key nursing interventions, such as pain relief, infection prevention, and exudate clearance, are outlined, along with support therapies. The case study emphasizes the importance of a holistic approach to wound management, considering both the physical and psychosocial aspects of patient care.

Running head: NURSING
NURSING
Name of the Student:
Name of the University:
Author Note:
NURSING
Name of the Student:
Name of the University:
Author Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1NURSING
Introduction:
The presented case study deals with a 64 year old female, Mrs. A, who was presented
to the outpatient department by her neighbour Mrs. M, with a medical history of anaemia,
coronary artery disease and hypertension. The patient presented with a wound in the lower
end of her calf muscle on her right leg. On assessing the wound, the wound measured 2cm x
2cm. Mrs. A stated that she was unaware about the exact cause of the wound injury but she
complained of pain and experiencing problem with mobility for the past 2 weeks. She
suspects she might have sustained the injury while gardening and had abstained from visiting
the care facility as she thought it was a minor cut and would recover within a few days with
the use of an antiseptic ointment. On closely assessing the wound, minor swelling was
detected with presence of slight sough near the edge of the lesion. Mrs. A is widowed and has
a daughter who is settled in U.S. She states that her daughter visits her once every two years.
She states experiencing no difficulty in performing her activities of daily living. She however
states feeling lonely without her husband but pleads not to let her daughter know as she does
not want to stress her about her health problems.
Previous Medical History:
The patient has a previous medical history of hypertension and anaemia. She had been
diagnosed with coronary artery disease in the year 2015 and had been under medications. She
however, admits to forgetting to take her medication at times. Her medical history lists no
known allergies. Her current medications include the following:
Acebutolol (Sectral) 400 mg, single dose per day
Atorvastatin (Lipitor) 20 mg, single dose per day
Iron supplements
Introduction:
The presented case study deals with a 64 year old female, Mrs. A, who was presented
to the outpatient department by her neighbour Mrs. M, with a medical history of anaemia,
coronary artery disease and hypertension. The patient presented with a wound in the lower
end of her calf muscle on her right leg. On assessing the wound, the wound measured 2cm x
2cm. Mrs. A stated that she was unaware about the exact cause of the wound injury but she
complained of pain and experiencing problem with mobility for the past 2 weeks. She
suspects she might have sustained the injury while gardening and had abstained from visiting
the care facility as she thought it was a minor cut and would recover within a few days with
the use of an antiseptic ointment. On closely assessing the wound, minor swelling was
detected with presence of slight sough near the edge of the lesion. Mrs. A is widowed and has
a daughter who is settled in U.S. She states that her daughter visits her once every two years.
She states experiencing no difficulty in performing her activities of daily living. She however
states feeling lonely without her husband but pleads not to let her daughter know as she does
not want to stress her about her health problems.
Previous Medical History:
The patient has a previous medical history of hypertension and anaemia. She had been
diagnosed with coronary artery disease in the year 2015 and had been under medications. She
however, admits to forgetting to take her medication at times. Her medical history lists no
known allergies. Her current medications include the following:
Acebutolol (Sectral) 400 mg, single dose per day
Atorvastatin (Lipitor) 20 mg, single dose per day
Iron supplements
2NURSING
Mrs. A admits to smoking 5 cigarettes on an average per day and relying heavily upon take
away meals. Family history of Mrs. A could not be retrieved as she states no genetic diseases
run in her family.
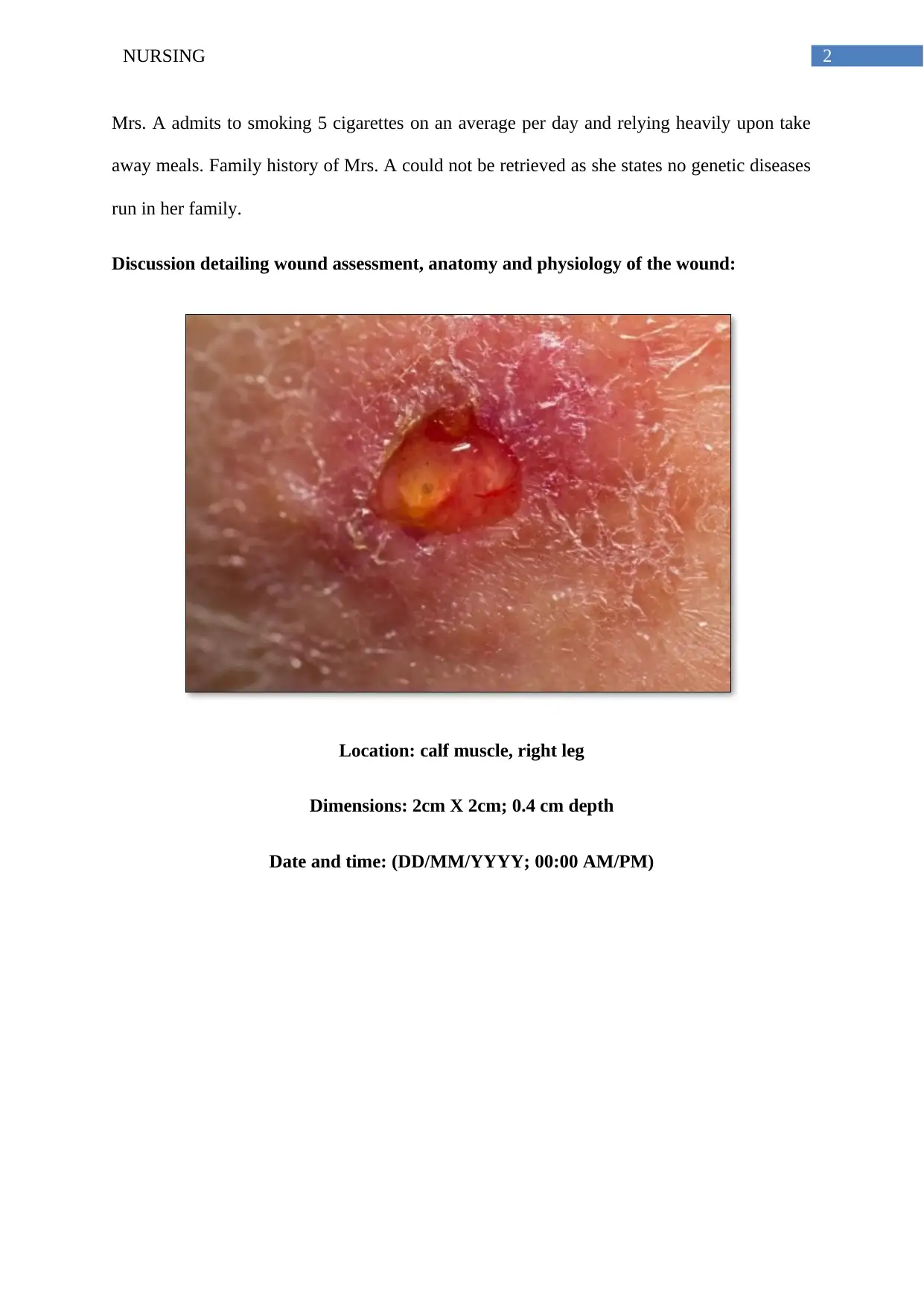
Discussion detailing wound assessment, anatomy and physiology of the wound:
Location: calf muscle, right leg
Dimensions: 2cm X 2cm; 0.4 cm depth
Date and time: (DD/MM/YYYY; 00:00 AM/PM)
Mrs. A admits to smoking 5 cigarettes on an average per day and relying heavily upon take
away meals. Family history of Mrs. A could not be retrieved as she states no genetic diseases
run in her family.
Discussion detailing wound assessment, anatomy and physiology of the wound:
Location: calf muscle, right leg
Dimensions: 2cm X 2cm; 0.4 cm depth
Date and time: (DD/MM/YYYY; 00:00 AM/PM)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3NURSING
Wound assessment:
The initial wound assessment that was conducted revealed the following data:
Type of wound: Acute
Aetiology: Cause of injury unknown
Last tetanus shot: unknown
Location and surrounding skin: Right leg, Stage II, partial thickness that affects the epidermis
and might extend into the dermis
Tissue Loss: Thickness wound that extends up to the subcutaneous tissue but the tendon or
the bone is not visible
Clinical appearance of the wound bed and the stage of healing: The wound appeared to be
moderately contaminated and was assessed to be around 2 cm in length. There was a presence
of moderate soft tissue damage. There was no periosteal stripping and the tendon or bone was
not exposed.
Measurement and dimensions of wound: The measurement dimensions include 2cm x 2cm.
The depth of the wound was measured to be 0.2 cm.
Wound edge: Minor swelling was detected with presence of slight sough near the edge of the
exposed lesion. The wound bed appeared to be red in colour
Exudate: viscous and yellow in colour
Presence of infection: Presence of infection which is evident by inflammation and presence
of pus and odour
Pain: 4/10
Wound assessment:
The initial wound assessment that was conducted revealed the following data:
Type of wound: Acute
Aetiology: Cause of injury unknown
Last tetanus shot: unknown
Location and surrounding skin: Right leg, Stage II, partial thickness that affects the epidermis
and might extend into the dermis
Tissue Loss: Thickness wound that extends up to the subcutaneous tissue but the tendon or
the bone is not visible
Clinical appearance of the wound bed and the stage of healing: The wound appeared to be
moderately contaminated and was assessed to be around 2 cm in length. There was a presence
of moderate soft tissue damage. There was no periosteal stripping and the tendon or bone was
not exposed.
Measurement and dimensions of wound: The measurement dimensions include 2cm x 2cm.
The depth of the wound was measured to be 0.2 cm.
Wound edge: Minor swelling was detected with presence of slight sough near the edge of the
exposed lesion. The wound bed appeared to be red in colour
Exudate: viscous and yellow in colour
Presence of infection: Presence of infection which is evident by inflammation and presence
of pus and odour
Pain: 4/10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4NURSING
Previous wound management: Nil
Pathophysiology and nursing management:
According to Woundsaustralia.com.au (2019), it is integral to assess and measure a
wound accurately and precisely. This is primarily on account of the fact that the aetiology of
every wound is different. Also, the treatment for every wound is different and depends on a
number of critical factors. Research studies in this regard mention that the cause of a wound
might be multifactorial which makes it extremely integral to assess the root cause of the
wound formation (Harding and Queen 2019; Silverchain.org.au 2019). As stated by Press
(2019), wounds might be caused on account of mixed aetiologies. This could either be due to
arterial or venous insufficiency or due to Diabetes and pressure characteristics. On closely
analysing the documented wound assessment, it can be said that the wound site contained
distinct edges that were inflamed. This suggests that the wound was a result of pressure
ulceration. The location of wound was on the lower end of the calf muscle on the right leg.
The reason of the wound was assumed to be a minor cut sustained by the patient during
gardening, however the patient was unsure regarding the same. The patient admitted to
wearing tight-fitting socks throughout the major length of the day. The reason for the same
was mentioned as experiencing coldness in her feet. Therefore on the basis of research
findings, it can be anticipated that the external pressure applied by the tight fitting socks
possibly exceeded the capillary pressure within the tissue which interrupted the normal blood
circulation and caused the ulceration (Han and Ceilley 2017). In addition to this, research
studies have also shown that patients diagnosed with a peripheral arterial occlusive disorder
is placed at a high risk of developing pressure wounds (Wong et al. 2015). The underlying
pathophysiology has been explained as a delayed reperfusion time after the removal of the
source of pressure being applied externally (Davidson 2019). In addition to this, damage
Previous wound management: Nil
Pathophysiology and nursing management:
According to Woundsaustralia.com.au (2019), it is integral to assess and measure a
wound accurately and precisely. This is primarily on account of the fact that the aetiology of
every wound is different. Also, the treatment for every wound is different and depends on a
number of critical factors. Research studies in this regard mention that the cause of a wound
might be multifactorial which makes it extremely integral to assess the root cause of the
wound formation (Harding and Queen 2019; Silverchain.org.au 2019). As stated by Press
(2019), wounds might be caused on account of mixed aetiologies. This could either be due to
arterial or venous insufficiency or due to Diabetes and pressure characteristics. On closely
analysing the documented wound assessment, it can be said that the wound site contained
distinct edges that were inflamed. This suggests that the wound was a result of pressure
ulceration. The location of wound was on the lower end of the calf muscle on the right leg.
The reason of the wound was assumed to be a minor cut sustained by the patient during
gardening, however the patient was unsure regarding the same. The patient admitted to
wearing tight-fitting socks throughout the major length of the day. The reason for the same
was mentioned as experiencing coldness in her feet. Therefore on the basis of research
findings, it can be anticipated that the external pressure applied by the tight fitting socks
possibly exceeded the capillary pressure within the tissue which interrupted the normal blood
circulation and caused the ulceration (Han and Ceilley 2017). In addition to this, research
studies have also shown that patients diagnosed with a peripheral arterial occlusive disorder
is placed at a high risk of developing pressure wounds (Wong et al. 2015). The underlying
pathophysiology has been explained as a delayed reperfusion time after the removal of the
source of pressure being applied externally (Davidson 2019). In addition to this, damage
5NURSING
caused due to friction on the skin surface by shearing forces also lead to the formation of
pressure wounds (Davidson 2019).
The first nursing wound management priority for the patient would include
envisioning pain relief. In addition to this, the second nursing management priority would
comprise of minimising risk of infection. The third nursing management priority for the
patient would comprise of clearance of exudate so as to facilitate positive recovery.
Pathology findings and clinical investigation:
The accurate diagnosis of a wound is complicated and requires a series of assessments
to be undertaken. In order to complete and confirm the diagnosis, a number of assessments
and clinical investigations need to be conducted. The assessments typically include wound
assessment, skin assessment, pain assessment and vital sign assessment. In addition to this
assessing laboratory values such as nutritional status and other important parameters such as
estimation of the complete blood count, glucose and iron level, protein level and urinalysis,
lipoprotein level, total lymphocyte count, blood urea level and vitamin and mineral level help
in determining the factors that could potentially interfere with the normal healing process. In
order to identify the potential factors that could interfere with the normal healing process, the
patient was referred for the blood glucose level, iron level, protein level, lipoprotein level and
urea level. Typically, the lab results are mentioned as under:
Glucose and iron level: 126/220 mg/dL; 10.0 g/dL
Protein level: 7 g/dL
Lipoprotein level: 30mg/dL
Urea level: 10 mg/dL
caused due to friction on the skin surface by shearing forces also lead to the formation of
pressure wounds (Davidson 2019).
The first nursing wound management priority for the patient would include
envisioning pain relief. In addition to this, the second nursing management priority would
comprise of minimising risk of infection. The third nursing management priority for the
patient would comprise of clearance of exudate so as to facilitate positive recovery.
Pathology findings and clinical investigation:
The accurate diagnosis of a wound is complicated and requires a series of assessments
to be undertaken. In order to complete and confirm the diagnosis, a number of assessments
and clinical investigations need to be conducted. The assessments typically include wound
assessment, skin assessment, pain assessment and vital sign assessment. In addition to this
assessing laboratory values such as nutritional status and other important parameters such as
estimation of the complete blood count, glucose and iron level, protein level and urinalysis,
lipoprotein level, total lymphocyte count, blood urea level and vitamin and mineral level help
in determining the factors that could potentially interfere with the normal healing process. In
order to identify the potential factors that could interfere with the normal healing process, the
patient was referred for the blood glucose level, iron level, protein level, lipoprotein level and
urea level. Typically, the lab results are mentioned as under:
Glucose and iron level: 126/220 mg/dL; 10.0 g/dL
Protein level: 7 g/dL
Lipoprotein level: 30mg/dL
Urea level: 10 mg/dL
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6NURSING
The nutritional assessment of the patient suggested that the patient consumed a diet
high in unsaturated and trans fatty substance. The meals consumed by the patient typically
lacked protein, vitamins and minerals. The carbohydrate level consumed by the patient was
also documented to be high.
On the basis of evaluation of the clinical findings it can be stated that the blood
glucose level of the patient was not within the recommended normal range. This indicated
that patient A was potentially suffering from Diabetes. As stated by Salazar, Ennis and Koh
(2016), the normal blood glucose level of patients must be less than 100 mg/ dL for fasting
and less than 140 mg/dL for the oral glucose tolerance test. The clinical examination report of
the patient suggests that the blood glucose level at fasting was measured equivalent to 126
mg/dL and that for the oral glucose tolerance test was equivalent to 140 mg/dl. This suggests
that the patient is affected by the chronic health condition of Diabetes. Further, the
recommended level of lipoprotein within the blood must be less than 30 mg/ dL (Salazar,
Ennis and Koh 2016). The patient’s clinical evaluation suggests the lipoprotein level to be
equivalent to 30 mg /dL. The reading can be associated with a heightened cholesterol level
which subsequently increases the risk of a stroke or a heart attack. Research studies mention
that the healing process gets delayed with an elevated level of glucose within the blood
(Khalil et al. 2015).
As per Janis and Harrison (2016), elevated blood glucose level in the diabetes patient
affect their nerves (neuropathy) which leads to the poor circulation of blood in the body.
Blood circulation is needed in the vicinity of the wound area for the skin to repair the wounds
or sores. Hence, from the evidence based research it can be stated that diabetes as co - morbid
factor leads to delayed healing of the wound (Salazar, Ennis and Koh 2016).
The nutritional assessment of the patient suggested that the patient consumed a diet
high in unsaturated and trans fatty substance. The meals consumed by the patient typically
lacked protein, vitamins and minerals. The carbohydrate level consumed by the patient was
also documented to be high.
On the basis of evaluation of the clinical findings it can be stated that the blood
glucose level of the patient was not within the recommended normal range. This indicated
that patient A was potentially suffering from Diabetes. As stated by Salazar, Ennis and Koh
(2016), the normal blood glucose level of patients must be less than 100 mg/ dL for fasting
and less than 140 mg/dL for the oral glucose tolerance test. The clinical examination report of
the patient suggests that the blood glucose level at fasting was measured equivalent to 126
mg/dL and that for the oral glucose tolerance test was equivalent to 140 mg/dl. This suggests
that the patient is affected by the chronic health condition of Diabetes. Further, the
recommended level of lipoprotein within the blood must be less than 30 mg/ dL (Salazar,
Ennis and Koh 2016). The patient’s clinical evaluation suggests the lipoprotein level to be
equivalent to 30 mg /dL. The reading can be associated with a heightened cholesterol level
which subsequently increases the risk of a stroke or a heart attack. Research studies mention
that the healing process gets delayed with an elevated level of glucose within the blood
(Khalil et al. 2015).
As per Janis and Harrison (2016), elevated blood glucose level in the diabetes patient
affect their nerves (neuropathy) which leads to the poor circulation of blood in the body.
Blood circulation is needed in the vicinity of the wound area for the skin to repair the wounds
or sores. Hence, from the evidence based research it can be stated that diabetes as co - morbid
factor leads to delayed healing of the wound (Salazar, Ennis and Koh 2016).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7NURSING
Factors interfering with wound management:
On closely analysing the patient information, it can be said that the blood glucose
level of the patient is not controlled which is one of the factors that has interfered with wound
recovery. The evidence base suggests that the chronic health condition of Diabetes, interferes
with the normal insulin production of the body (Dhivya et al. 2015). The insulin hormone is
responsible for managing the optimal blood glucose level within the body (Boateng and
Catanzano 2015). Further, the insulin hormone dictates the cells to uptake glucose from the
blood stream in order to perform normal physiological functions. If the level of blood glucose
remain predominantly high, the normal functioning of the white blood cell is impaired (Khalil
et al. 2015). White blood cells or WBCs play an integral role in carrying out immunological
functions. The poor functioning of the white blood cells generates poor immunological
response to fight microbial infections and this leads to delay in wound healing (Janis and
Harrison 2016). In addition to this, research studies further reveal that uncontrolled blood
glucose level slows down blood circulation (Han and Ceilley 2017). Poor circulation of blood
curtails the supply of essential nutrients to the wound region which subsequently delays the
recovery process (Wong et al. 2015). Further, Diabetes also leads to neurological impairment
or neuropathy which slows down the wound recovery process (Davidson 2019).
It should also be noted that the previous medical history of the patient suggested that
the patient suffered from hypertension. Further, the vital assessment of the patient also
suggested that the pressure level of the patient was elevated. Research studies state that
hypertension interferes with the normal blood circulation which subsequently results in poor
transportation and availability of nutrients to the damaged tissues of the body (Salazar, Ennis
and Koh 2016). It can therefore be stated that the uncontrolled blood pressure level is one of
the risk factors that has interfered with the normal wound healing process.
Factors interfering with wound management:
On closely analysing the patient information, it can be said that the blood glucose
level of the patient is not controlled which is one of the factors that has interfered with wound
recovery. The evidence base suggests that the chronic health condition of Diabetes, interferes
with the normal insulin production of the body (Dhivya et al. 2015). The insulin hormone is
responsible for managing the optimal blood glucose level within the body (Boateng and
Catanzano 2015). Further, the insulin hormone dictates the cells to uptake glucose from the
blood stream in order to perform normal physiological functions. If the level of blood glucose
remain predominantly high, the normal functioning of the white blood cell is impaired (Khalil
et al. 2015). White blood cells or WBCs play an integral role in carrying out immunological
functions. The poor functioning of the white blood cells generates poor immunological
response to fight microbial infections and this leads to delay in wound healing (Janis and
Harrison 2016). In addition to this, research studies further reveal that uncontrolled blood
glucose level slows down blood circulation (Han and Ceilley 2017). Poor circulation of blood
curtails the supply of essential nutrients to the wound region which subsequently delays the
recovery process (Wong et al. 2015). Further, Diabetes also leads to neurological impairment
or neuropathy which slows down the wound recovery process (Davidson 2019).
It should also be noted that the previous medical history of the patient suggested that
the patient suffered from hypertension. Further, the vital assessment of the patient also
suggested that the pressure level of the patient was elevated. Research studies state that
hypertension interferes with the normal blood circulation which subsequently results in poor
transportation and availability of nutrients to the damaged tissues of the body (Salazar, Ennis
and Koh 2016). It can therefore be stated that the uncontrolled blood pressure level is one of
the risk factors that has interfered with the normal wound healing process.
8NURSING
The medical history of the patient also suggests that the patient suffers from anaemia.
Anaemia is primarily caused by iron deficiency throughout the body. Lack of iron interferes
with the optimal oxygen availability to the tissues present within the body. As stated by
Davidson (2019), the process of wound healing and recovery relies heavily on oxygenation
and in cases where the oxygen level is low, the process of recovery is considerably delayed.
This further increases the risk of wound infections.
Other factors that interfere with the wound healing process can be mentioned as
unhealthy lifestyle factors such as increased smoking and unhealthy diet. A number of
research studies have mentioned about an existing relationship between smoking and
Diabetes. As per, Wong et al. (2015), smoking interferes with the normal blood glucose level
within the body which in turn affects the rate of wound recovery. Therefore, the existing
medical history of the patient can be said to have acted as the major risk factors that would
largely interfere with the process of wound recovery.
Key nursing interventions and support therapies:
The following set of nursing interventions were used for envisioning relief to the
patient.
Wound care and management: The wound was cleaned with regular saline and the Alginate
dressing was chosen for dressing the wound. The rationale for the same can be explained as
the effectiveness of the dressing to treat venous leg ulcers. On the basis of the assessed
wound properties, it can be said that wound appeared to be exuding moderately. The Alginate
dressing comprise of calcium ions that directly interact with the sodium ions present within
the exudate of the wound (Dhivya et al. 2015). This reaction enables the fibre present with
the dressing to swell up and dissolve into a gel like substance. Alginate dressings are the best
absorbents that prevent the affected wound from microbial infections and maintain a moist
The medical history of the patient also suggests that the patient suffers from anaemia.
Anaemia is primarily caused by iron deficiency throughout the body. Lack of iron interferes
with the optimal oxygen availability to the tissues present within the body. As stated by
Davidson (2019), the process of wound healing and recovery relies heavily on oxygenation
and in cases where the oxygen level is low, the process of recovery is considerably delayed.
This further increases the risk of wound infections.
Other factors that interfere with the wound healing process can be mentioned as
unhealthy lifestyle factors such as increased smoking and unhealthy diet. A number of
research studies have mentioned about an existing relationship between smoking and
Diabetes. As per, Wong et al. (2015), smoking interferes with the normal blood glucose level
within the body which in turn affects the rate of wound recovery. Therefore, the existing
medical history of the patient can be said to have acted as the major risk factors that would
largely interfere with the process of wound recovery.
Key nursing interventions and support therapies:
The following set of nursing interventions were used for envisioning relief to the
patient.
Wound care and management: The wound was cleaned with regular saline and the Alginate
dressing was chosen for dressing the wound. The rationale for the same can be explained as
the effectiveness of the dressing to treat venous leg ulcers. On the basis of the assessed
wound properties, it can be said that wound appeared to be exuding moderately. The Alginate
dressing comprise of calcium ions that directly interact with the sodium ions present within
the exudate of the wound (Dhivya et al. 2015). This reaction enables the fibre present with
the dressing to swell up and dissolve into a gel like substance. Alginate dressings are the best
absorbents that prevent the affected wound from microbial infections and maintain a moist
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9NURSING
environment that ensures accelerated recovery (Boateng and Catanzano 2015). In addition to
this, this method of dressing was chosen as it is extremely convenient for application and has
no risks associated with allergies (Vowden and Vowden 2017).
Pain management: The pain score of the patient was documented to be 4/10. In order to
envision pain relief, the patient would be administered mild dosage of analgesics and over the
counter Paracetamols. In addition to this, the pain assessment of the patient would be
conducted on a regular basis and in case of an increase in the pain score, a consultation with
the physician would be encouraged (Weller et al. 2016).
Non-pharmacological intervention: The patient was advised to keep the wounded region
elevated. The rationale for the same can be explained as facilitating easier fluid drainage from
the affected wound area which could accelerate the recovery process (Finlayson et al. 2017).
In addition to this, the patient was also advised to wear therapeutic shoes that are specifically
designed to reduce risks pertaining to previously existing foot diseases (Weller et al. 2016).
Health Literacy: The patient was educated about his existing physical health condition and
was explained how his uncontrolled blood glucose level delayed the wound recovery process.
Further, the patient was also educated about how smoking interferes with the normal blood
glucose level and slows down the wound healing process.
Referral to Psychotherapist: The patient was also referred to a psychotherapist. The rationale
for the same could be explained as the persisting low mood and affect of the patient. The
psychotherapist could make use of psychological counselling and mindfulness based
therapies for facilitating recovery (Driessen et al. 2015).
Referral to a nutritionist: The patient was also referred to a nutritionist. The rationale for the
same can be explained as devising an appropriate diet plan that could be a source of optimal
haemoglobin level (Goldstein and Muller-Wieland 2016). At the same time, it is also
environment that ensures accelerated recovery (Boateng and Catanzano 2015). In addition to
this, this method of dressing was chosen as it is extremely convenient for application and has
no risks associated with allergies (Vowden and Vowden 2017).
Pain management: The pain score of the patient was documented to be 4/10. In order to
envision pain relief, the patient would be administered mild dosage of analgesics and over the
counter Paracetamols. In addition to this, the pain assessment of the patient would be
conducted on a regular basis and in case of an increase in the pain score, a consultation with
the physician would be encouraged (Weller et al. 2016).
Non-pharmacological intervention: The patient was advised to keep the wounded region
elevated. The rationale for the same can be explained as facilitating easier fluid drainage from
the affected wound area which could accelerate the recovery process (Finlayson et al. 2017).
In addition to this, the patient was also advised to wear therapeutic shoes that are specifically
designed to reduce risks pertaining to previously existing foot diseases (Weller et al. 2016).
Health Literacy: The patient was educated about his existing physical health condition and
was explained how his uncontrolled blood glucose level delayed the wound recovery process.
Further, the patient was also educated about how smoking interferes with the normal blood
glucose level and slows down the wound healing process.
Referral to Psychotherapist: The patient was also referred to a psychotherapist. The rationale
for the same could be explained as the persisting low mood and affect of the patient. The
psychotherapist could make use of psychological counselling and mindfulness based
therapies for facilitating recovery (Driessen et al. 2015).
Referral to a nutritionist: The patient was also referred to a nutritionist. The rationale for the
same can be explained as devising an appropriate diet plan that could be a source of optimal
haemoglobin level (Goldstein and Muller-Wieland 2016). At the same time, it is also
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10NURSING
expected that the recommended diet plan by the nutritionist would help in the regulation of
blood glucose level and cholesterol level.
Social, ethical and legal aspects:
Venous leg wound or ulceration can significantly impact the quality of life. It can
limit the mobility of an individual and can interfere with the normal ability to address the
activities of daily living such as walking, washing or cooking. Further, restricted mobility
affects socialising ability for patients. On the legal front a number of healthcare policies are
available that intend to improve access to healthcare facilities and alleviate the disease
burden associated with wounds and ulceration in the elderly.
Conclusion:
Therefore, to conclude, it can be mentioned that the application of a set of nursing
interventions helped to facilitate holistic recovery of the patient. The set of applied
interventions comprised of undertaking strategies to optimise blood glucose level and making
use of pharmacological and non-pharmacological interventions to dress the wound. In
addition to this, other interventions comprised of arranging referral to a psychotherapist and a
nutritionist. The rationale for the same can be explained as administering counselling and
psychotherapeutic interventions to optimise the mood and affect of the patient and improve
the level of social interaction. At the same time, the rationale for the referral to a nutritionist
can be explained as devising an appropriate diet plan for the patient so as to ensure that the
blood glucose level, cholesterol level and haemoglobin level is managed and is within the
normal range. In addition to this, the patient was also administered health literacy so as to
empower the patient with self-management strategies in order to make healthy lifestyle
changes that could facilitate control of the blood glucose level.
expected that the recommended diet plan by the nutritionist would help in the regulation of
blood glucose level and cholesterol level.
Social, ethical and legal aspects:
Venous leg wound or ulceration can significantly impact the quality of life. It can
limit the mobility of an individual and can interfere with the normal ability to address the
activities of daily living such as walking, washing or cooking. Further, restricted mobility
affects socialising ability for patients. On the legal front a number of healthcare policies are
available that intend to improve access to healthcare facilities and alleviate the disease
burden associated with wounds and ulceration in the elderly.
Conclusion:
Therefore, to conclude, it can be mentioned that the application of a set of nursing
interventions helped to facilitate holistic recovery of the patient. The set of applied
interventions comprised of undertaking strategies to optimise blood glucose level and making
use of pharmacological and non-pharmacological interventions to dress the wound. In
addition to this, other interventions comprised of arranging referral to a psychotherapist and a
nutritionist. The rationale for the same can be explained as administering counselling and
psychotherapeutic interventions to optimise the mood and affect of the patient and improve
the level of social interaction. At the same time, the rationale for the referral to a nutritionist
can be explained as devising an appropriate diet plan for the patient so as to ensure that the
blood glucose level, cholesterol level and haemoglobin level is managed and is within the
normal range. In addition to this, the patient was also administered health literacy so as to
empower the patient with self-management strategies in order to make healthy lifestyle
changes that could facilitate control of the blood glucose level.
11NURSING
References:
Boateng, J. and Catanzano, O., 2015. Advanced therapeutic dressings for effective wound
healing—a review. Journal of pharmaceutical sciences, 104(11), pp.3653-3680.
Davidson, J. 2019. Wound Repair and Regeneration - Wiley Online Library. [online]
Onlinelibrary.wiley.com. Available at: https://onlinelibrary.wiley.com/journal/1524475x
[Accessed 23 Jul. 2019].
Dhivya, S., Padma, V.V. and Santhini, E., 2015. Wound dressings–a
review. BioMedicine, 5(4).
Driessen, E., Hegelmaier, L.M., Abbass, A.A., Barber, J.P., Dekker, J.J., Van, H.L., Jansma,
E.P. and Cuijpers, P., 2015. The efficacy of short-term psychodynamic psychotherapy for
depression: A meta-analysis update. Clinical psychology review, 42, pp.1-15.
Finlayson, K., Miaskowski, C., Alexander, K., Liu, W.H., Aouizerat, B., Parker, C., Maresco-
Pennisi, D. and Edwards, H., 2017. Distinct wound healing and quality-of-life outcomes in
subgroups of patients with venous leg ulcers with different symptom cluster
experiences. Journal of pain and symptom management, 53(5), pp.871-879.
Goldstein, B.J. and Müller-Wieland, D. eds., 2016. Type 2 diabetes: principles and practice.
CRC Press.
Han, G. and Ceilley, R., 2017. Chronic wound healing: a review of current management and
treatments. Advances in therapy, 34(3), pp.599-610.
Harding, K. and Queen, D. 2019. [online] Available at:
https://www.wiley.com/en-us/International+Wound+Journal-p-9780J [Accessed 23 Jul.
2019].
References:
Boateng, J. and Catanzano, O., 2015. Advanced therapeutic dressings for effective wound
healing—a review. Journal of pharmaceutical sciences, 104(11), pp.3653-3680.
Davidson, J. 2019. Wound Repair and Regeneration - Wiley Online Library. [online]
Onlinelibrary.wiley.com. Available at: https://onlinelibrary.wiley.com/journal/1524475x
[Accessed 23 Jul. 2019].
Dhivya, S., Padma, V.V. and Santhini, E., 2015. Wound dressings–a
review. BioMedicine, 5(4).
Driessen, E., Hegelmaier, L.M., Abbass, A.A., Barber, J.P., Dekker, J.J., Van, H.L., Jansma,
E.P. and Cuijpers, P., 2015. The efficacy of short-term psychodynamic psychotherapy for
depression: A meta-analysis update. Clinical psychology review, 42, pp.1-15.
Finlayson, K., Miaskowski, C., Alexander, K., Liu, W.H., Aouizerat, B., Parker, C., Maresco-
Pennisi, D. and Edwards, H., 2017. Distinct wound healing and quality-of-life outcomes in
subgroups of patients with venous leg ulcers with different symptom cluster
experiences. Journal of pain and symptom management, 53(5), pp.871-879.
Goldstein, B.J. and Müller-Wieland, D. eds., 2016. Type 2 diabetes: principles and practice.
CRC Press.
Han, G. and Ceilley, R., 2017. Chronic wound healing: a review of current management and
treatments. Advances in therapy, 34(3), pp.599-610.
Harding, K. and Queen, D. 2019. [online] Available at:
https://www.wiley.com/en-us/International+Wound+Journal-p-9780J [Accessed 23 Jul.
2019].
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13