Nursing Principles and Management: COPD Pathophysiology and Care
VerifiedAdded on 2023/04/21
|12
|3262
|241
Report
AI Summary
This report delves into the complexities of Chronic Obstructive Pulmonary Disease (COPD), examining its pathophysiology and the crucial role of nurses in patient care. The introduction highlights COPD's global impact, defining the disease and its symptoms, risk factors, and prevalence, particularly in Australia. The discussion section explores the underlying mechanisms of COPD, including the inflammatory response, oxidative stress, and resulting physiological abnormalities like airflow obstruction and mucous hypersecretion. A schematic diagram illustrates the disease's progression. The report emphasizes the multifaceted role of nurses in COPD management, including spirometry guidance, patient education on self-management and inhaler techniques, smoking cessation support, nutritional guidance, exercise encouragement, and vaccination recommendations. Nurses are vital in helping patients adapt to their condition, identifying exacerbations, and seeking timely assistance, ultimately improving patient outcomes and quality of life.

Running head: NURSING PRINCIPLES AND MANAGEMENT
NURSING PRINCIPLES AND MANAGEMENT
Name of the Student
Name of the University
Author’s Note:
NURSING PRINCIPLES AND MANAGEMENT
Name of the Student
Name of the University
Author’s Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1NURSING PRINCIPLES AND MANAGEMENT
Introduction:
Chronic Obstructive Pulmonary Disease is one of the most hazardous malignancies in the current
world and or Chronic Obstructive Pulmonary Disease has huge impact on the society and
economy all over the world. Chronic obstructive pulmonary disease is a term used to illustrate
progressive lung diseases including chronic bronchitis, emphysema, and refractive asthma (non-
reversible) (Vestbo, 2014). This condition is marked by increasing respiratory failure. The
Chronic obstructive pulmonary disease is a progressive disease, which is at the moment
incurable, but chronic obstructive pulmonary disease can be manageable with the right diagnosis
and treatment. People have been capable to live with chronic obstructive pulmonary disease for
many years. In general, coughing and shortness of breath regards as a sign of aging and this
might be the case of chronic obstructive pulmonary disease (Rennard, Vestbo & Agustí, 2013).
Most common symptoms and signs of Chronic obstructive pulmonary disease consists of
wheezing increased coughing (with or without mucus), shortness of breath, and a feeling of
tightness around the chest. Commonly, chronic obstructive pulmonary disease limits the air flow
in lung which causes the shortness of breath. In general, mostly older people are affected by
chronic obstructive pulmonary disease and most common conditions are chronic bronchitis and
emphysema (Gregersen et al., 2016). The occurrence of chronic obstructive pulmonary disease
increases with age, mostly among the 45 years old or older. Among the age group of 65 years to
74 years old and 75 years to 84 years old, Chronic obstructive pulmonary disease ranks among
the top three causes of overall burden in their health and was the second biggest overall burden
among the men aged 75 years to 84 years old (Australian Institute of Health and Welfare, 2019).
Chronic obstructive pulmonary disease is generally associated by the common risk factors and
effects of chronic obstructive pulmonary disease on other parts of the body might lead to the
Introduction:
Chronic Obstructive Pulmonary Disease is one of the most hazardous malignancies in the current
world and or Chronic Obstructive Pulmonary Disease has huge impact on the society and
economy all over the world. Chronic obstructive pulmonary disease is a term used to illustrate
progressive lung diseases including chronic bronchitis, emphysema, and refractive asthma (non-
reversible) (Vestbo, 2014). This condition is marked by increasing respiratory failure. The
Chronic obstructive pulmonary disease is a progressive disease, which is at the moment
incurable, but chronic obstructive pulmonary disease can be manageable with the right diagnosis
and treatment. People have been capable to live with chronic obstructive pulmonary disease for
many years. In general, coughing and shortness of breath regards as a sign of aging and this
might be the case of chronic obstructive pulmonary disease (Rennard, Vestbo & Agustí, 2013).
Most common symptoms and signs of Chronic obstructive pulmonary disease consists of
wheezing increased coughing (with or without mucus), shortness of breath, and a feeling of
tightness around the chest. Commonly, chronic obstructive pulmonary disease limits the air flow
in lung which causes the shortness of breath. In general, mostly older people are affected by
chronic obstructive pulmonary disease and most common conditions are chronic bronchitis and
emphysema (Gregersen et al., 2016). The occurrence of chronic obstructive pulmonary disease
increases with age, mostly among the 45 years old or older. Among the age group of 65 years to
74 years old and 75 years to 84 years old, Chronic obstructive pulmonary disease ranks among
the top three causes of overall burden in their health and was the second biggest overall burden
among the men aged 75 years to 84 years old (Australian Institute of Health and Welfare, 2019).
Chronic obstructive pulmonary disease is generally associated by the common risk factors and
effects of chronic obstructive pulmonary disease on other parts of the body might lead to the
2NURSING PRINCIPLES AND MANAGEMENT
other chronic conditions such as respiratory cancers, asthma, cardiac illness and diabetes. Active
smoking or smoking exposure is the principal cause of chronic obstructive pulmonary disease;
however other causes could be involved (Australian Institute of Health and Welfare, 2019).
These causes are outdoor air pollution, fumes and workplace dust from burned fuel of animal or
plant origin, asthma infections and childhood respiratory disease. In Australia, people over the
age of 45 years, chronic obstructive pulmonary disease affects one in 20 Australian individuals.
In the year 2015, it has been reported that chronic obstructive pulmonary disease is Australia's
fifth largest cause of death. In the same year, about 7,100 individuals (3,300 females and 3,800
males) have been reported to have died of chronic obstructive pulmonary disease (Australian
Institute of Health and Welfare, 2019). People who were smoking are 6 times more likely to have
chronic obstructive pulmonary disease in comparison with the non- smokers. Even individuals
who have quit smoking are 5 times more likely to develop emphysema in comparison with the
people who have never smoked (Park et al., 2015).
Along with the physicians, nurses also play an important role in the treatment and caring of
patients with chronic obstructive pulmonary disease. Australia’s population of aged persons
increasing significantly over the years due medical advancements, however general physicians
are not increasing with the same ratio. There physicians are very busy, in here, nurses can help
with the situation. Properly trained and skilled nurses can handle and provide initial treatment to
the patients suffering from chronic obstructive pulmonary disease as well as improve the quality
of health care service by providing timely service to the elderly patients as well as saving and
freeing up time for the doctors (Vestbo et al., 2013).
In 2016, more than 251 million peoples were affected by the chronic obstructive pulmonary
disease worldwide. Additionally, 3.17 million deaths were caused by disease related to chronic
other chronic conditions such as respiratory cancers, asthma, cardiac illness and diabetes. Active
smoking or smoking exposure is the principal cause of chronic obstructive pulmonary disease;
however other causes could be involved (Australian Institute of Health and Welfare, 2019).
These causes are outdoor air pollution, fumes and workplace dust from burned fuel of animal or
plant origin, asthma infections and childhood respiratory disease. In Australia, people over the
age of 45 years, chronic obstructive pulmonary disease affects one in 20 Australian individuals.
In the year 2015, it has been reported that chronic obstructive pulmonary disease is Australia's
fifth largest cause of death. In the same year, about 7,100 individuals (3,300 females and 3,800
males) have been reported to have died of chronic obstructive pulmonary disease (Australian
Institute of Health and Welfare, 2019). People who were smoking are 6 times more likely to have
chronic obstructive pulmonary disease in comparison with the non- smokers. Even individuals
who have quit smoking are 5 times more likely to develop emphysema in comparison with the
people who have never smoked (Park et al., 2015).
Along with the physicians, nurses also play an important role in the treatment and caring of
patients with chronic obstructive pulmonary disease. Australia’s population of aged persons
increasing significantly over the years due medical advancements, however general physicians
are not increasing with the same ratio. There physicians are very busy, in here, nurses can help
with the situation. Properly trained and skilled nurses can handle and provide initial treatment to
the patients suffering from chronic obstructive pulmonary disease as well as improve the quality
of health care service by providing timely service to the elderly patients as well as saving and
freeing up time for the doctors (Vestbo et al., 2013).
In 2016, more than 251 million peoples were affected by the chronic obstructive pulmonary
disease worldwide. Additionally, 3.17 million deaths were caused by disease related to chronic
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3NURSING PRINCIPLES AND MANAGEMENT
obstructive pulmonary disease in the year 2015 (Who.int, 2019). Hence, there is a great need for
the understanding the patho- physiology of chronic obstructive pulmonary disease in order tackle
this situation by understanding the cause and symptoms of the disease. Presently, there is no cure
for chronic obstructive pulmonary disease but it can be manageable through treatment and nurses
play a significant role in this particular scenario. As discussed above, chronic obstructive
pulmonary disease mostly affect the elderly people and they need support for the management of
the disease and nurses can play a role in that scenario. From the judging the high prevalence of
chronic obstructive pulmonary disease and nurses role in this scenario, the purpose of this article
is delve in to the pathophysiology of chronic obstructive pulmonary disease and provide
discussion on the nurses role in the managing and caring for the people who are suffering from
the chronic obstructive pulmonary disease.
Discussion:
Patho- physiology of the chronic obstructive pulmonary disease: A poor reversible air flow
obstruction and an abnormal inflammatory response are the characteristics of chronic obstructive
pulmonary disease. All individuals who smokes are infected by inflammation in their lungs, but
chronic obstructive pulmonary disease developers have increased toxicity or abnormal reactions
against the outside toxins (Gea, Agustí & Roca, 2013). This amplified reaction may lead to tissue
damage or emphysema, mucus hyper secretion or chronic bronchitis, and interference in the
normal repair and defense mechanisms which causes inflammation of the air way and fibrosis
also known as bronchiolitis. Increased neutrophil counts, macrophages and T lymphocytes of the
lungs (CD8 more than CD4) characterize chronic obstructive pulmonary disease. The degree of
inflammation is generally associated with the degree of blockage of airflow. Release of a range
of cytokines by these inflammatory cells and mediators are involved in the disease. This pattern
obstructive pulmonary disease in the year 2015 (Who.int, 2019). Hence, there is a great need for
the understanding the patho- physiology of chronic obstructive pulmonary disease in order tackle
this situation by understanding the cause and symptoms of the disease. Presently, there is no cure
for chronic obstructive pulmonary disease but it can be manageable through treatment and nurses
play a significant role in this particular scenario. As discussed above, chronic obstructive
pulmonary disease mostly affect the elderly people and they need support for the management of
the disease and nurses can play a role in that scenario. From the judging the high prevalence of
chronic obstructive pulmonary disease and nurses role in this scenario, the purpose of this article
is delve in to the pathophysiology of chronic obstructive pulmonary disease and provide
discussion on the nurses role in the managing and caring for the people who are suffering from
the chronic obstructive pulmonary disease.
Discussion:
Patho- physiology of the chronic obstructive pulmonary disease: A poor reversible air flow
obstruction and an abnormal inflammatory response are the characteristics of chronic obstructive
pulmonary disease. All individuals who smokes are infected by inflammation in their lungs, but
chronic obstructive pulmonary disease developers have increased toxicity or abnormal reactions
against the outside toxins (Gea, Agustí & Roca, 2013). This amplified reaction may lead to tissue
damage or emphysema, mucus hyper secretion or chronic bronchitis, and interference in the
normal repair and defense mechanisms which causes inflammation of the air way and fibrosis
also known as bronchiolitis. Increased neutrophil counts, macrophages and T lymphocytes of the
lungs (CD8 more than CD4) characterize chronic obstructive pulmonary disease. The degree of
inflammation is generally associated with the degree of blockage of airflow. Release of a range
of cytokines by these inflammatory cells and mediators are involved in the disease. This pattern
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4NURSING PRINCIPLES AND MANAGEMENT
of inflammation is significantly different from the pattern seen in asthma patients. Smoke from
cigarettes and inflammation cause oxidative stress that stimulates multiple inflammatory cells to
release proteases and deactivates various anti- proteases through oxidation (Milne & King,
2014). Proteases which are majorly involved in the process are primarily produced by
neutrophils (including elastase, cathepsin G, and protease 3), macrophages (cathepsins E, A, L
and S and cysteine) and different matrix metalloproteases such as MMP-8, 9, and 12. The most
important anti-proteases involved in emphysema pathogenesis include leukoprotease secretary
inhibitor, α1, and metalloprotease tissue inhibitors. Chronic obstructive pulmonary disease
increases the oxidative burden. This causes an imbalance in antioxidants and oxidants during the
oxidative stress (Kirkham & Barnes, 2013). In stable condition chronic obstructive pulmonary
disease, numerous markers of oxidative stress are increased and in case of exacerbations, it is
increased even further. Oxidative stress might lead to anti- proteases being inactivated or the
stimulation of mucous production (Kirkham & Barnes, 2013). A schematic diagram of the patho-
physiology of the chronic obstructive pulmonary disease can be found in the Figure 1.
of inflammation is significantly different from the pattern seen in asthma patients. Smoke from
cigarettes and inflammation cause oxidative stress that stimulates multiple inflammatory cells to
release proteases and deactivates various anti- proteases through oxidation (Milne & King,
2014). Proteases which are majorly involved in the process are primarily produced by
neutrophils (including elastase, cathepsin G, and protease 3), macrophages (cathepsins E, A, L
and S and cysteine) and different matrix metalloproteases such as MMP-8, 9, and 12. The most
important anti-proteases involved in emphysema pathogenesis include leukoprotease secretary
inhibitor, α1, and metalloprotease tissue inhibitors. Chronic obstructive pulmonary disease
increases the oxidative burden. This causes an imbalance in antioxidants and oxidants during the
oxidative stress (Kirkham & Barnes, 2013). In stable condition chronic obstructive pulmonary
disease, numerous markers of oxidative stress are increased and in case of exacerbations, it is
increased even further. Oxidative stress might lead to anti- proteases being inactivated or the
stimulation of mucous production (Kirkham & Barnes, 2013). A schematic diagram of the patho-
physiology of the chronic obstructive pulmonary disease can be found in the Figure 1.
5NURSING PRINCIPLES AND MANAGEMENT
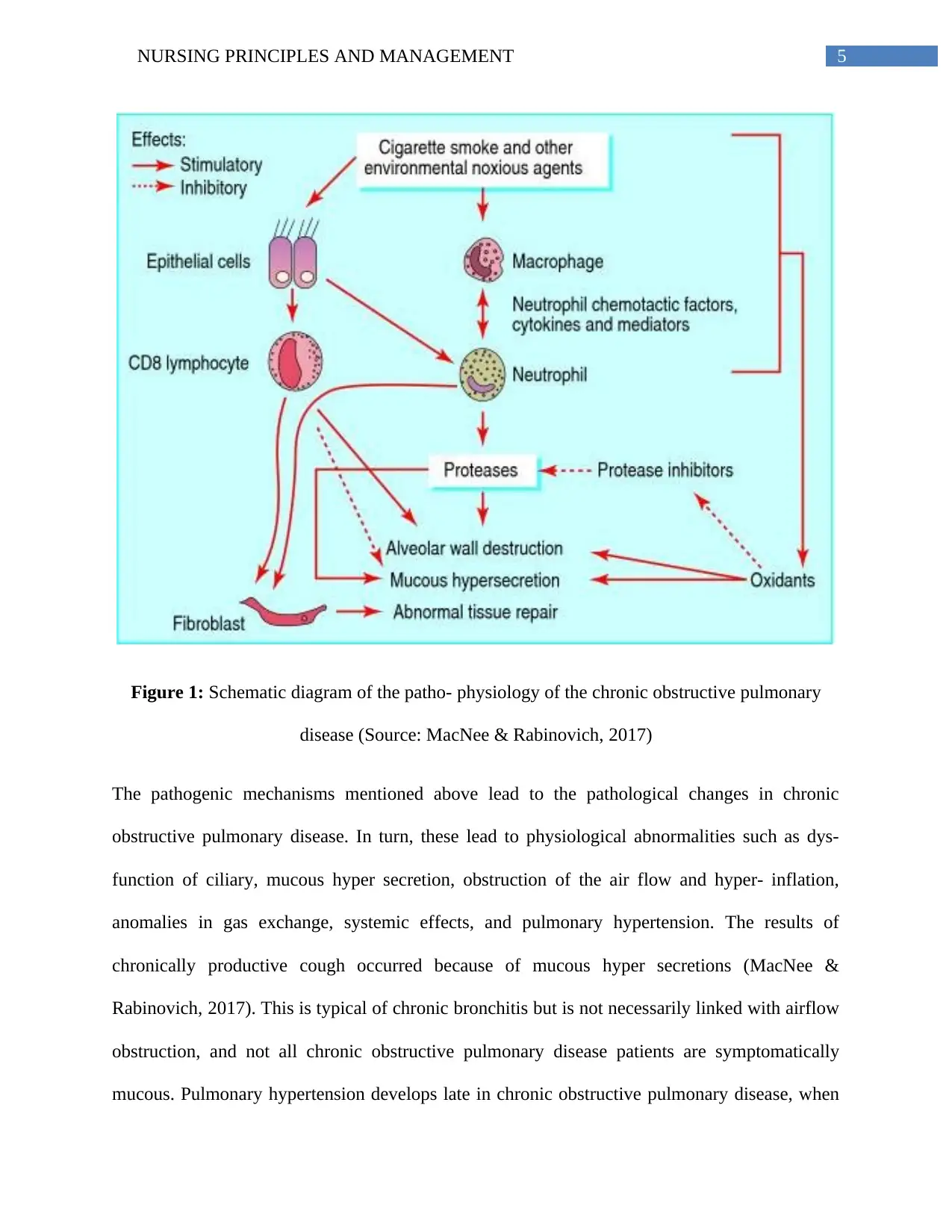
Figure 1: Schematic diagram of the patho- physiology of the chronic obstructive pulmonary
disease (Source: MacNee & Rabinovich, 2017)
The pathogenic mechanisms mentioned above lead to the pathological changes in chronic
obstructive pulmonary disease. In turn, these lead to physiological abnormalities such as dys-
function of ciliary, mucous hyper secretion, obstruction of the air flow and hyper- inflation,
anomalies in gas exchange, systemic effects, and pulmonary hypertension. The results of
chronically productive cough occurred because of mucous hyper secretions (MacNee &
Rabinovich, 2017). This is typical of chronic bronchitis but is not necessarily linked with airflow
obstruction, and not all chronic obstructive pulmonary disease patients are symptomatically
mucous. Pulmonary hypertension develops late in chronic obstructive pulmonary disease, when
Figure 1: Schematic diagram of the patho- physiology of the chronic obstructive pulmonary
disease (Source: MacNee & Rabinovich, 2017)
The pathogenic mechanisms mentioned above lead to the pathological changes in chronic
obstructive pulmonary disease. In turn, these lead to physiological abnormalities such as dys-
function of ciliary, mucous hyper secretion, obstruction of the air flow and hyper- inflation,
anomalies in gas exchange, systemic effects, and pulmonary hypertension. The results of
chronically productive cough occurred because of mucous hyper secretions (MacNee &
Rabinovich, 2017). This is typical of chronic bronchitis but is not necessarily linked with airflow
obstruction, and not all chronic obstructive pulmonary disease patients are symptomatically
mucous. Pulmonary hypertension develops late in chronic obstructive pulmonary disease, when
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6NURSING PRINCIPLES AND MANAGEMENT
abnormalities of gas exchange occur. Abnormalities of gas exchange occur in advanced diseases
and are distinguished by arterial hypoxemia. In a small conducting air way with diameters less
than 2 mm which is the main location for an air flow obstruction. Inflammation and reduction
(remodeling of airways) and inflammatory exudates in the smaller air ways are the reason behind
these. The loss of lungs elastic recoil occurs due to the destruction of alveolar walls and the
destruction of the alveolar support and these are the other factors which contributes to the air
flow obstructions (MacNee & Rabinovich, 2017).
Nurses role in the management and caring of the patients with chronic obstructive pulmonary
disease: Well timed and good preparation of patients are required for precise spirometry and this
is being the routine test for both primary and secondary care, nurses working with chronic
obstructive pulmonary disease patients have to comprehend why and how this is being
performed (Fletcher & Dahl, 2013). Spirometry is very difficult and often stimulates coughs in
patients. A friendly approach is necessary to ensure the patient is as good as he or she can.
Patients conducting reversibility tests must try and ensure that they are guided by a standard
procedure required in this scenario. After the diagnosis has been developed, the medical care of
the patient is designed to support and help the patient to achieve to come in term with the
diagnosis. Some patients might be concerned about the illness itself and hesitating to seek aid, in
specific as they have not been able to resist smoking and fear of disapproval of health workers is
the reason behind that (Stridsman, Lindberg & Skär, 2014). Therefore, a constructive approach is
necessary by the nurses that focus on keeping the function and activities of the day to
a minimum the occurrence of the symptoms. One of the crucial roles of the nurses will be to help
patients adapt to their health condition and start teaching self-management. One of the other key
duties of the nurses will be to teach patients how to properly utilize their inhaler. It is
abnormalities of gas exchange occur. Abnormalities of gas exchange occur in advanced diseases
and are distinguished by arterial hypoxemia. In a small conducting air way with diameters less
than 2 mm which is the main location for an air flow obstruction. Inflammation and reduction
(remodeling of airways) and inflammatory exudates in the smaller air ways are the reason behind
these. The loss of lungs elastic recoil occurs due to the destruction of alveolar walls and the
destruction of the alveolar support and these are the other factors which contributes to the air
flow obstructions (MacNee & Rabinovich, 2017).
Nurses role in the management and caring of the patients with chronic obstructive pulmonary
disease: Well timed and good preparation of patients are required for precise spirometry and this
is being the routine test for both primary and secondary care, nurses working with chronic
obstructive pulmonary disease patients have to comprehend why and how this is being
performed (Fletcher & Dahl, 2013). Spirometry is very difficult and often stimulates coughs in
patients. A friendly approach is necessary to ensure the patient is as good as he or she can.
Patients conducting reversibility tests must try and ensure that they are guided by a standard
procedure required in this scenario. After the diagnosis has been developed, the medical care of
the patient is designed to support and help the patient to achieve to come in term with the
diagnosis. Some patients might be concerned about the illness itself and hesitating to seek aid, in
specific as they have not been able to resist smoking and fear of disapproval of health workers is
the reason behind that (Stridsman, Lindberg & Skär, 2014). Therefore, a constructive approach is
necessary by the nurses that focus on keeping the function and activities of the day to
a minimum the occurrence of the symptoms. One of the crucial roles of the nurses will be to help
patients adapt to their health condition and start teaching self-management. One of the other key
duties of the nurses will be to teach patients how to properly utilize their inhaler. It is
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7NURSING PRINCIPLES AND MANAGEMENT
very important to regularly inspect the inhalation techniques of primary and secondary-care
patients before they can be discharged (Sundh et al., 2013). Even to the patients who are
already using inhaler treatment and importance and value of good inhaler techniques must never
be forgotten. The primary role of the nurses is to assist patients suffering with chronic
obstructive pulmonary disease to stop smoking, even if this assistance requires referring the
patient to another specialist services. Several nurses have indeed been instructed on how to
stop of smoking and they can offer necessary assistance to patients. Comparable skills in
secondary care have now been developed, although continuous support in hospitals might be
harder to offer (Spencer & Hanania, 2013). Many of the advanced patients suffering with chronic
obstructive pulmonary disease are weak and some of them are excessively overweight.
Excessive weight increases breathing workload, and weight loss helps patients cope. Nutritional
supplement might be helpful, but it must not replace normal nutrition. Maintaining active fitness
and well-being generally requires for the patients suffering from chronic obstructive pulmonary
disorder. Shortness of breath can be very much painful, and the most natural response in this
scenario is that to stop the activities which causing it. There have to be reassurance for the
patients that even if it is unsettling, shortness of breath is not deadly and practices and self
interests should continue (Spencer & Hanania, 2013). Several patients with relatively moderate
level of diseases must also be encouraged to start working. Patients might need guidance on their
pursuits, and elderly patients at home must be encouraged by basic exercise initiatives to retain
upper and lower limbs power, so that simple as well but essential tasks like bathroom can be
handled by themselves (Tobiano et al., 2015). Aggravations are very common during the winter
and a yearly influenza vaccination should be recommended. Despite a lack of evidence for its
efficacy in chronic obstructive pulmonary disease, many chronic obstructive pulmonary
very important to regularly inspect the inhalation techniques of primary and secondary-care
patients before they can be discharged (Sundh et al., 2013). Even to the patients who are
already using inhaler treatment and importance and value of good inhaler techniques must never
be forgotten. The primary role of the nurses is to assist patients suffering with chronic
obstructive pulmonary disease to stop smoking, even if this assistance requires referring the
patient to another specialist services. Several nurses have indeed been instructed on how to
stop of smoking and they can offer necessary assistance to patients. Comparable skills in
secondary care have now been developed, although continuous support in hospitals might be
harder to offer (Spencer & Hanania, 2013). Many of the advanced patients suffering with chronic
obstructive pulmonary disease are weak and some of them are excessively overweight.
Excessive weight increases breathing workload, and weight loss helps patients cope. Nutritional
supplement might be helpful, but it must not replace normal nutrition. Maintaining active fitness
and well-being generally requires for the patients suffering from chronic obstructive pulmonary
disorder. Shortness of breath can be very much painful, and the most natural response in this
scenario is that to stop the activities which causing it. There have to be reassurance for the
patients that even if it is unsettling, shortness of breath is not deadly and practices and self
interests should continue (Spencer & Hanania, 2013). Several patients with relatively moderate
level of diseases must also be encouraged to start working. Patients might need guidance on their
pursuits, and elderly patients at home must be encouraged by basic exercise initiatives to retain
upper and lower limbs power, so that simple as well but essential tasks like bathroom can be
handled by themselves (Tobiano et al., 2015). Aggravations are very common during the winter
and a yearly influenza vaccination should be recommended. Despite a lack of evidence for its
efficacy in chronic obstructive pulmonary disease, many chronic obstructive pulmonary
8NURSING PRINCIPLES AND MANAGEMENT
disease patients should receive pneumococcal immunization. Educating patients on how to
identify aggravation and seek assistance especially early may lessen the hospitalization (Harrison
et al., 2015). A treatment should be focused on how to maximize bronchodilation, along with
the treatment of any infection and lower inflammation is required. While most of the
aggravations are not microbial in origin, there is frequent use of antibiotics at this kind
of treatment. Short oral steroid courses are advised for all to lessen healing time and increase the
lung function during aggravations. Chronic obstructive pulmonary diseases seem to be running
in families, and patients sometimes report chest issues with a family background. The only
genetic risk factor which is responsible for 1 per cent of chronic obstructive pulmonary disease is
alpha 1-antitrypsin deficiency, but the majority of those with a family history of chronic
obstructive pulmonary disease do not have this abnormality (Gøtzsche & Johansen, 2016).
Conclusion:
Therefore, in a nutshell, it can be deduced from the above discussion that chronic obstructive
pulmonary diseases is one of the frequent malignancies in the world. This is an umbrella term
which covers progressive lung diseases including chronic bronchitis, emphysema, and refractive
asthma (non- reversible). Mainly older peoples are affected by these diseases. Nurses play a vital
role in the care of the patient suffering from chronic obstructive pulmonary diseases as after the
diagnosis, patient primarily need support and assistance regarding the disease. At present there is
no cure for the disease but it is manageable with treatment.
disease patients should receive pneumococcal immunization. Educating patients on how to
identify aggravation and seek assistance especially early may lessen the hospitalization (Harrison
et al., 2015). A treatment should be focused on how to maximize bronchodilation, along with
the treatment of any infection and lower inflammation is required. While most of the
aggravations are not microbial in origin, there is frequent use of antibiotics at this kind
of treatment. Short oral steroid courses are advised for all to lessen healing time and increase the
lung function during aggravations. Chronic obstructive pulmonary diseases seem to be running
in families, and patients sometimes report chest issues with a family background. The only
genetic risk factor which is responsible for 1 per cent of chronic obstructive pulmonary disease is
alpha 1-antitrypsin deficiency, but the majority of those with a family history of chronic
obstructive pulmonary disease do not have this abnormality (Gøtzsche & Johansen, 2016).
Conclusion:
Therefore, in a nutshell, it can be deduced from the above discussion that chronic obstructive
pulmonary diseases is one of the frequent malignancies in the world. This is an umbrella term
which covers progressive lung diseases including chronic bronchitis, emphysema, and refractive
asthma (non- reversible). Mainly older peoples are affected by these diseases. Nurses play a vital
role in the care of the patient suffering from chronic obstructive pulmonary diseases as after the
diagnosis, patient primarily need support and assistance regarding the disease. At present there is
no cure for the disease but it is manageable with treatment.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9NURSING PRINCIPLES AND MANAGEMENT
References:
Australian Institute of Health and Welfare. (2019). COPD (chronic obstructive pulmonary
disease) snapshot, COPD - Australian Institute of Health and Welfare. Retrieved from
https://www.aihw.gov.au/reports/chronic-respiratory-conditions/copd/contents/copd
Fletcher, M. J., & Dahl, B. H. (2013). Expanding nurse practice in COPD: is it key to providing
high quality, effective and safe patient care?. Primary Care Respiratory Journal, 22(2),
230.
Gea, J., Agustí, A., & Roca, J. (2013). Pathophysiology of muscle dysfunction in COPD. Journal
of applied physiology, 114(9), 1222-1234.
Gøtzsche, P. C., & Johansen, H. K. (2016). Intravenous alpha‐1 antitrypsin augmentation therapy
for treating patients with alpha‐1 antitrypsin deficiency and lung disease. Cochrane
database of systematic reviews, (9).
Gregersen, T. L., Green, A., Frausing, E., Ringbaek, T., Brøndum, E., & Ulrik, C. S. (2016). Do
telemedical interventions improve quality of life in patients with COPD? A systematic
review. International journal of chronic obstructive pulmonary disease, 11, 809.
Harrison, S. L., Janaudis-Ferreira, T., Brooks, D., Desveaux, L., & Goldstein, R. S. (2015). Self-
management following an acute exacerbation of COPD: a systematic
review. Chest, 147(3), 646-661.
Kirkham, P. A., & Barnes, P. J. (2013). Oxidative stress in COPD. Chest, 144(1), 266-273.
MacNee, W., & Rabinovich, R. A. (2017). Pathology and pathogenesis. ABC of COPD, Second.
References:
Australian Institute of Health and Welfare. (2019). COPD (chronic obstructive pulmonary
disease) snapshot, COPD - Australian Institute of Health and Welfare. Retrieved from
https://www.aihw.gov.au/reports/chronic-respiratory-conditions/copd/contents/copd
Fletcher, M. J., & Dahl, B. H. (2013). Expanding nurse practice in COPD: is it key to providing
high quality, effective and safe patient care?. Primary Care Respiratory Journal, 22(2),
230.
Gea, J., Agustí, A., & Roca, J. (2013). Pathophysiology of muscle dysfunction in COPD. Journal
of applied physiology, 114(9), 1222-1234.
Gøtzsche, P. C., & Johansen, H. K. (2016). Intravenous alpha‐1 antitrypsin augmentation therapy
for treating patients with alpha‐1 antitrypsin deficiency and lung disease. Cochrane
database of systematic reviews, (9).
Gregersen, T. L., Green, A., Frausing, E., Ringbaek, T., Brøndum, E., & Ulrik, C. S. (2016). Do
telemedical interventions improve quality of life in patients with COPD? A systematic
review. International journal of chronic obstructive pulmonary disease, 11, 809.
Harrison, S. L., Janaudis-Ferreira, T., Brooks, D., Desveaux, L., & Goldstein, R. S. (2015). Self-
management following an acute exacerbation of COPD: a systematic
review. Chest, 147(3), 646-661.
Kirkham, P. A., & Barnes, P. J. (2013). Oxidative stress in COPD. Chest, 144(1), 266-273.
MacNee, W., & Rabinovich, R. A. (2017). Pathology and pathogenesis. ABC of COPD, Second.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10NURSING PRINCIPLES AND MANAGEMENT
Milne, S., & King, G. G. (2014). Advanced imaging in COPD: insights into pulmonary
pathophysiology. Journal of thoracic disease, 6(11), 1570.
Park, S. J., Foreman, M. G., Demeo, D. L., Bhatt, S. P., Hansel, N. N., Wise, R. A., ... & Bowler,
R. P. (2015). Menthol cigarette smoking in the COPDG ene cohort: Relationship with
COPD, comorbidities and CT metrics. Respirology, 20(1), 108-114.
Rennard, S. I., Vestbo, J., & Agustí, A. (2013). What Is Chronic Obstructive Pulmonary Disease
Anyway?. Continua, Categories, Cut Points, and Moving beyond Spirometry.
Spencer, P., & Hanania, N. A. (2013). Optimizing safety of COPD treatments: role of the nurse
practitioner. Journal of multidisciplinary healthcare, 6, 53.
Stridsman, C., Lindberg, A., & Skär, L. (2014). Fatigue in chronic obstructive pulmonary
disease: a qualitative study of people's experiences. Scandinavian Journal of Caring
Sciences, 28(1), 130-138.
Sundh, J., Efraimsson, E. Ö., Janson, C., Montgomery, S., Staällberg, B., & Lisspers, K. (2013).
Management of COPD exacerbations in primary care: a clinical cohort study. Primary
Care Respiratory Journal, 22(4), 393.
Tobiano, G., Marshall, A., Bucknall, T., & Chaboyer, W. (2015). Patient participation in nursing
care on medical wards: an integrative review. International Journal of Nursing
Studies, 52(6), 1107-1120.
Vestbo, J. (2014). COPD: definition and phenotypes. Clinics in chest medicine, 35(1), 1-6.
Vestbo, J., Hurd, S. S., Agustí, A. G., Jones, P. W., Vogelmeier, C., Anzueto, A., ... & Stockley,
R. A. (2013). Global strategy for the diagnosis, management, and prevention of chronic
Milne, S., & King, G. G. (2014). Advanced imaging in COPD: insights into pulmonary
pathophysiology. Journal of thoracic disease, 6(11), 1570.
Park, S. J., Foreman, M. G., Demeo, D. L., Bhatt, S. P., Hansel, N. N., Wise, R. A., ... & Bowler,
R. P. (2015). Menthol cigarette smoking in the COPDG ene cohort: Relationship with
COPD, comorbidities and CT metrics. Respirology, 20(1), 108-114.
Rennard, S. I., Vestbo, J., & Agustí, A. (2013). What Is Chronic Obstructive Pulmonary Disease
Anyway?. Continua, Categories, Cut Points, and Moving beyond Spirometry.
Spencer, P., & Hanania, N. A. (2013). Optimizing safety of COPD treatments: role of the nurse
practitioner. Journal of multidisciplinary healthcare, 6, 53.
Stridsman, C., Lindberg, A., & Skär, L. (2014). Fatigue in chronic obstructive pulmonary
disease: a qualitative study of people's experiences. Scandinavian Journal of Caring
Sciences, 28(1), 130-138.
Sundh, J., Efraimsson, E. Ö., Janson, C., Montgomery, S., Staällberg, B., & Lisspers, K. (2013).
Management of COPD exacerbations in primary care: a clinical cohort study. Primary
Care Respiratory Journal, 22(4), 393.
Tobiano, G., Marshall, A., Bucknall, T., & Chaboyer, W. (2015). Patient participation in nursing
care on medical wards: an integrative review. International Journal of Nursing
Studies, 52(6), 1107-1120.
Vestbo, J. (2014). COPD: definition and phenotypes. Clinics in chest medicine, 35(1), 1-6.
Vestbo, J., Hurd, S. S., Agustí, A. G., Jones, P. W., Vogelmeier, C., Anzueto, A., ... & Stockley,
R. A. (2013). Global strategy for the diagnosis, management, and prevention of chronic
11NURSING PRINCIPLES AND MANAGEMENT
obstructive pulmonary disease: GOLD executive summary. American journal of
respiratory and critical care medicine, 187(4), 347-365.
Who.int. (2019). Chronic obstructive pulmonary disease (COPD). Retrieved from
https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-
disease-(copd)
obstructive pulmonary disease: GOLD executive summary. American journal of
respiratory and critical care medicine, 187(4), 347-365.
Who.int. (2019). Chronic obstructive pulmonary disease (COPD). Retrieved from
https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-
disease-(copd)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.