Pharmacokinetics and Pharmacodynamics in Nursing
VerifiedAdded on 2023/03/30
|16
|3283
|385
AI Summary
This document provides an overview of pharmacokinetics and pharmacodynamics in nursing. It explains the concepts of drug absorption, metabolism, and excretion. It also discusses different routes of drug administration and their effects. Additionally, it includes nursing considerations for various medications.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Nursing
Student’s Name:
Student’s ID:
Student’s Code:
Student’s Name:
Student’s ID:
Student’s Code:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1
Table of Contents
Answer 1......................................................................................................................................................2
Answer 2......................................................................................................................................................2
Answer 3......................................................................................................................................................3
Answer 4......................................................................................................................................................4
Answer 5......................................................................................................................................................6
Answer 6......................................................................................................................................................8
Case study 1................................................................................................................................................9
Case study 2................................................................................................................................................9
Case study 3..............................................................................................................................................10
References.................................................................................................................................................12
Table of Contents
Answer 1......................................................................................................................................................2
Answer 2......................................................................................................................................................2
Answer 3......................................................................................................................................................3
Answer 4......................................................................................................................................................4
Answer 5......................................................................................................................................................6
Answer 6......................................................................................................................................................8
Case study 1................................................................................................................................................9
Case study 2................................................................................................................................................9
Case study 3..............................................................................................................................................10
References.................................................................................................................................................12
2
Answer 1
a) Pharmacokinetics is the education of drug captivation, absorption, excretion, metabolism,
and distribution (Ryman & Meibohm, 2017).
b) Pharmacodynamics refers to the learnings of the physiological effects of drugs on the
individual and evaluates how a drug affects the creature (Almazroo, Miah &
Venkataramanan, 2017).
c) Bioavailability means the degree or rate at which the circulatory system of the body
absorbs an administered drug.
d) First pass effect also termed as the first-pass metabolism, occurs when a non-intravenous
drug enters into the liver and decrease concentration quickly before the drug reaches the
target.
e) Drug indication means to use a drug to treat the specific disease. For instance, an
indication of insulin to treat diabetes.
f) Drug contraindication means various health conditions are contraindicated with many
drugs which help the physician to prescribe correct pharmaceutical drugs to the patient.
g) Adverse drug reaction refers to the injury caused by taking improper or inaccurate
medication.
h) The therapeutic range is defined as the range of dosage which expected to achieve
desirable effects of therapeutic.
i) Toxicology is the study of nature and the effects of toxins as well as the treatment of
toxins and discipline that includes the study of hostile effects of chemical substances on
organisms.
Answer 2
a) Three methods of parental administration of drugs are
IM (Intramuscular) – Inserted into the muscle
SC (Subcutaneous) – Inserted under the skin
IV (Intravenous) * It offers 100% bioavailability of a drug – Inserted into the vein
(Hörmann & Zimmer, 2016)
b) Four aspects that affect the absorption of the drug:
Physical forms: Drug exists in the form of liquid, gases, and solid.
Answer 1
a) Pharmacokinetics is the education of drug captivation, absorption, excretion, metabolism,
and distribution (Ryman & Meibohm, 2017).
b) Pharmacodynamics refers to the learnings of the physiological effects of drugs on the
individual and evaluates how a drug affects the creature (Almazroo, Miah &
Venkataramanan, 2017).
c) Bioavailability means the degree or rate at which the circulatory system of the body
absorbs an administered drug.
d) First pass effect also termed as the first-pass metabolism, occurs when a non-intravenous
drug enters into the liver and decrease concentration quickly before the drug reaches the
target.
e) Drug indication means to use a drug to treat the specific disease. For instance, an
indication of insulin to treat diabetes.
f) Drug contraindication means various health conditions are contraindicated with many
drugs which help the physician to prescribe correct pharmaceutical drugs to the patient.
g) Adverse drug reaction refers to the injury caused by taking improper or inaccurate
medication.
h) The therapeutic range is defined as the range of dosage which expected to achieve
desirable effects of therapeutic.
i) Toxicology is the study of nature and the effects of toxins as well as the treatment of
toxins and discipline that includes the study of hostile effects of chemical substances on
organisms.
Answer 2
a) Three methods of parental administration of drugs are
IM (Intramuscular) – Inserted into the muscle
SC (Subcutaneous) – Inserted under the skin
IV (Intravenous) * It offers 100% bioavailability of a drug – Inserted into the vein
(Hörmann & Zimmer, 2016)
b) Four aspects that affect the absorption of the drug:
Physical forms: Drug exists in the form of liquid, gases, and solid.
3
Molecular size: Absorption of drug is more quickly when the molecular size is small.
Liquid water solubility: It means greater liquid water coefficient, higher liquid solubility
and thus, greater absorption of the drug (Pridgen, Alexis & Farokhzad, 2015).
Particle size: The large size of the particle makes the absorption slow.
c) Species and hormones are the two internal factors that affect the metabolism of the drug
(Jones et al., 2015). Diet and environment are the two external factors that affect the
metabolism of the drug.
d) As an individual grows elder, the body organs and tissues start functioning slowly. Due to
the decline in the function of body organs, metabolism, drug absorption, excretion, and
distribution become worse. The drugs are prolonged, and the activity of drug metabolism
decreases in the liver. In an older person, the parenchymal cells reduced that present in
the liver and thus, decrease the blood flow in the liver, which makes the liver unable to
metabolize drugs (Almazroo, Miah & Venkataramanan, 2017).
e) Drugs are excreted by the following four routes such as saliva, kidney, sweat or tears, and
lungs. Liver disease, thyroid disease, kidney disease, and chronic obstructive pulmonary
disease are four chronic diseases that may affect the elimination of drugs (Kawase,
Yamamoto, Egashira & Iwaki, 2016).
f) Polypharmacy refers to the concurrent use of various medicines by an individual patient
(Noale et al., 2016). It is most commonly found in elder persons. Polypharmacy happens
due to multiple pathologies, lack of knowledge about aging, use of repeat prescriptions,
and poor communication between healthcare providers and patient.
Answer 3
a)
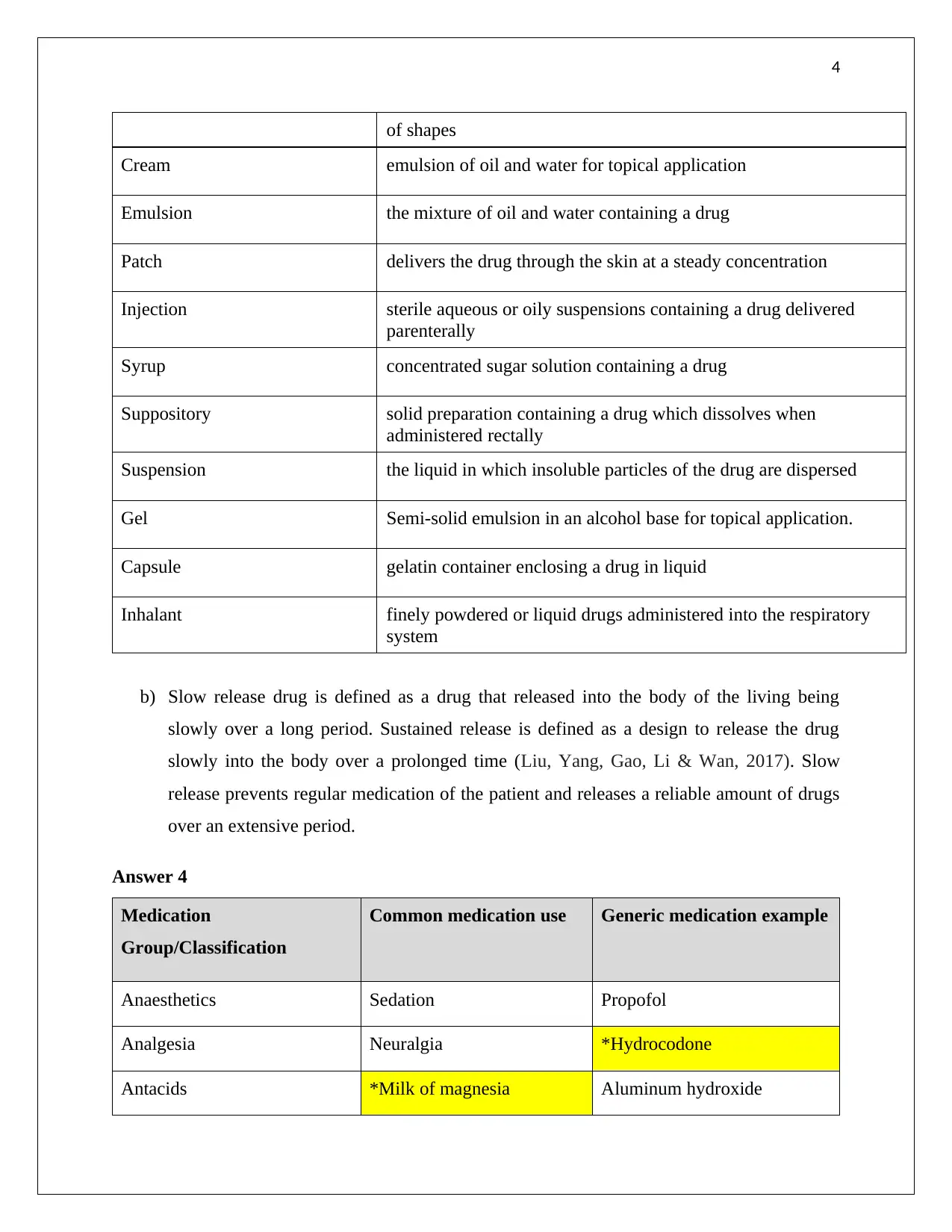
Formulation Description
Wafer orally disintegrating tablet containing medication (Califf, McCall &
Mark, 2017)
Lotion medication dissolved in a water or alcohol base for topical
application – lower viscosity than creams
Drops medication dissolved in sterile liquid for topical application
Tablet a drug mixed with a base compound and compressed into a variety
Molecular size: Absorption of drug is more quickly when the molecular size is small.
Liquid water solubility: It means greater liquid water coefficient, higher liquid solubility
and thus, greater absorption of the drug (Pridgen, Alexis & Farokhzad, 2015).
Particle size: The large size of the particle makes the absorption slow.
c) Species and hormones are the two internal factors that affect the metabolism of the drug
(Jones et al., 2015). Diet and environment are the two external factors that affect the
metabolism of the drug.
d) As an individual grows elder, the body organs and tissues start functioning slowly. Due to
the decline in the function of body organs, metabolism, drug absorption, excretion, and
distribution become worse. The drugs are prolonged, and the activity of drug metabolism
decreases in the liver. In an older person, the parenchymal cells reduced that present in
the liver and thus, decrease the blood flow in the liver, which makes the liver unable to
metabolize drugs (Almazroo, Miah & Venkataramanan, 2017).
e) Drugs are excreted by the following four routes such as saliva, kidney, sweat or tears, and
lungs. Liver disease, thyroid disease, kidney disease, and chronic obstructive pulmonary
disease are four chronic diseases that may affect the elimination of drugs (Kawase,
Yamamoto, Egashira & Iwaki, 2016).
f) Polypharmacy refers to the concurrent use of various medicines by an individual patient
(Noale et al., 2016). It is most commonly found in elder persons. Polypharmacy happens
due to multiple pathologies, lack of knowledge about aging, use of repeat prescriptions,
and poor communication between healthcare providers and patient.
Answer 3
a)
Formulation Description
Wafer orally disintegrating tablet containing medication (Califf, McCall &
Mark, 2017)
Lotion medication dissolved in a water or alcohol base for topical
application – lower viscosity than creams
Drops medication dissolved in sterile liquid for topical application
Tablet a drug mixed with a base compound and compressed into a variety
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4
of shapes
Cream emulsion of oil and water for topical application
Emulsion the mixture of oil and water containing a drug
Patch delivers the drug through the skin at a steady concentration
Injection sterile aqueous or oily suspensions containing a drug delivered
parenterally
Syrup concentrated sugar solution containing a drug
Suppository solid preparation containing a drug which dissolves when
administered rectally
Suspension the liquid in which insoluble particles of the drug are dispersed
Gel Semi-solid emulsion in an alcohol base for topical application.
Capsule gelatin container enclosing a drug in liquid
Inhalant finely powdered or liquid drugs administered into the respiratory
system
b) Slow release drug is defined as a drug that released into the body of the living being
slowly over a long period. Sustained release is defined as a design to release the drug
slowly into the body over a prolonged time (Liu, Yang, Gao, Li & Wan, 2017). Slow
release prevents regular medication of the patient and releases a reliable amount of drugs
over an extensive period.
Answer 4
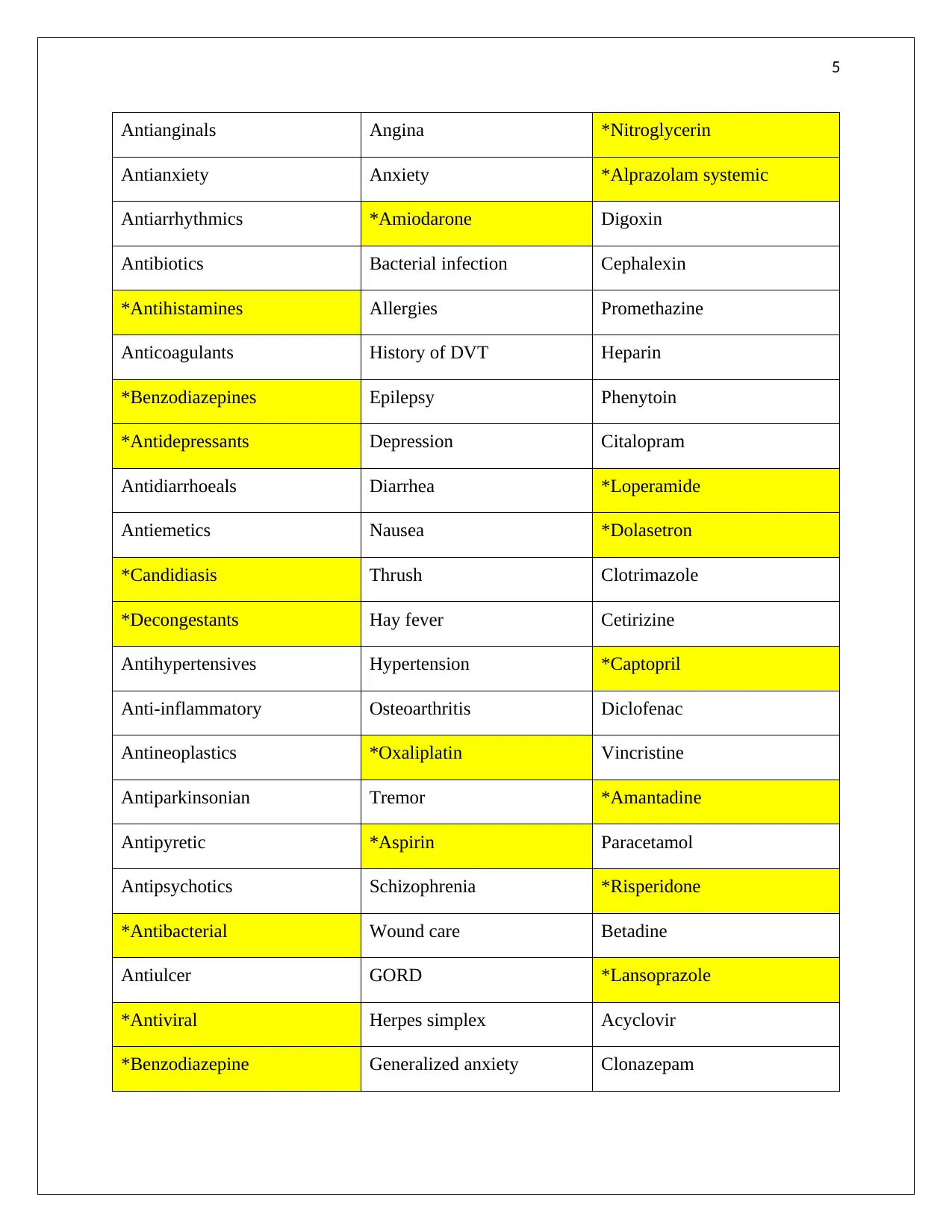
Medication
Group/Classification
Common medication use Generic medication example
Anaesthetics Sedation Propofol
Analgesia Neuralgia *Hydrocodone
Antacids *Milk of magnesia Aluminum hydroxide
of shapes
Cream emulsion of oil and water for topical application
Emulsion the mixture of oil and water containing a drug
Patch delivers the drug through the skin at a steady concentration
Injection sterile aqueous or oily suspensions containing a drug delivered
parenterally
Syrup concentrated sugar solution containing a drug
Suppository solid preparation containing a drug which dissolves when
administered rectally
Suspension the liquid in which insoluble particles of the drug are dispersed
Gel Semi-solid emulsion in an alcohol base for topical application.
Capsule gelatin container enclosing a drug in liquid
Inhalant finely powdered or liquid drugs administered into the respiratory
system
b) Slow release drug is defined as a drug that released into the body of the living being
slowly over a long period. Sustained release is defined as a design to release the drug
slowly into the body over a prolonged time (Liu, Yang, Gao, Li & Wan, 2017). Slow
release prevents regular medication of the patient and releases a reliable amount of drugs
over an extensive period.
Answer 4
Medication
Group/Classification
Common medication use Generic medication example
Anaesthetics Sedation Propofol
Analgesia Neuralgia *Hydrocodone
Antacids *Milk of magnesia Aluminum hydroxide
5
Antianginals Angina *Nitroglycerin
Antianxiety Anxiety *Alprazolam systemic
Antiarrhythmics *Amiodarone Digoxin
Antibiotics Bacterial infection Cephalexin
*Antihistamines Allergies Promethazine
Anticoagulants History of DVT Heparin
*Benzodiazepines Epilepsy Phenytoin
*Antidepressants Depression Citalopram
Antidiarrhoeals Diarrhea *Loperamide
Antiemetics Nausea *Dolasetron
*Candidiasis Thrush Clotrimazole
*Decongestants Hay fever Cetirizine
Antihypertensives Hypertension *Captopril
Anti-inflammatory Osteoarthritis Diclofenac
Antineoplastics *Oxaliplatin Vincristine
Antiparkinsonian Tremor *Amantadine
Antipyretic *Aspirin Paracetamol
Antipsychotics Schizophrenia *Risperidone
*Antibacterial Wound care Betadine
Antiulcer GORD *Lansoprazole
*Antiviral Herpes simplex Acyclovir
*Benzodiazepine Generalized anxiety Clonazepam
Antianginals Angina *Nitroglycerin
Antianxiety Anxiety *Alprazolam systemic
Antiarrhythmics *Amiodarone Digoxin
Antibiotics Bacterial infection Cephalexin
*Antihistamines Allergies Promethazine
Anticoagulants History of DVT Heparin
*Benzodiazepines Epilepsy Phenytoin
*Antidepressants Depression Citalopram
Antidiarrhoeals Diarrhea *Loperamide
Antiemetics Nausea *Dolasetron
*Candidiasis Thrush Clotrimazole
*Decongestants Hay fever Cetirizine
Antihypertensives Hypertension *Captopril
Anti-inflammatory Osteoarthritis Diclofenac
Antineoplastics *Oxaliplatin Vincristine
Antiparkinsonian Tremor *Amantadine
Antipyretic *Aspirin Paracetamol
Antipsychotics Schizophrenia *Risperidone
*Antibacterial Wound care Betadine
Antiulcer GORD *Lansoprazole
*Antiviral Herpes simplex Acyclovir
*Benzodiazepine Generalized anxiety Clonazepam
6
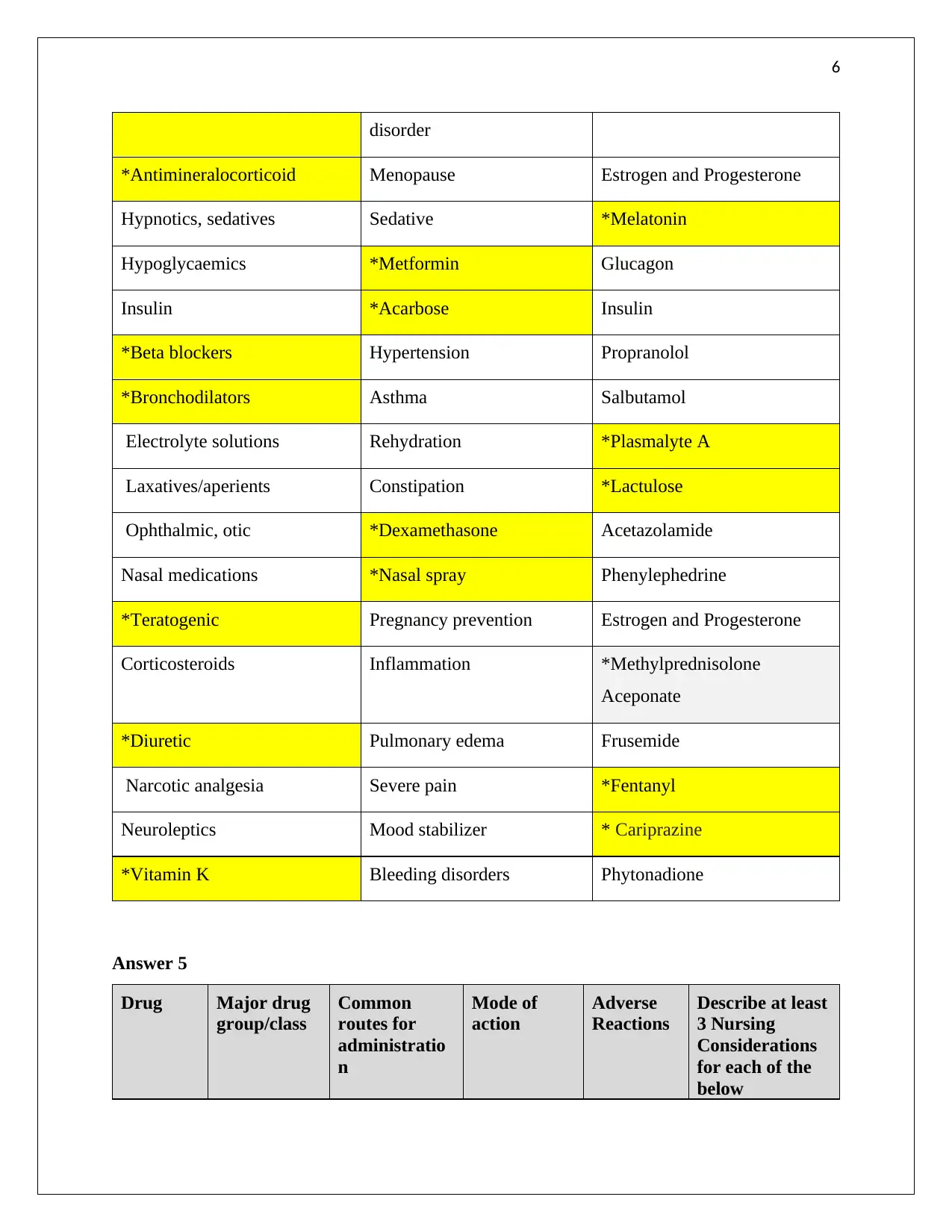
disorder
*Antimineralocorticoid Menopause Estrogen and Progesterone
Hypnotics, sedatives Sedative *Melatonin
Hypoglycaemics *Metformin Glucagon
Insulin *Acarbose Insulin
*Beta blockers Hypertension Propranolol
*Bronchodilators Asthma Salbutamol
Electrolyte solutions Rehydration *Plasmalyte A
Laxatives/aperients Constipation *Lactulose
Ophthalmic, otic *Dexamethasone Acetazolamide
Nasal medications *Nasal spray Phenylephedrine
*Teratogenic Pregnancy prevention Estrogen and Progesterone
Corticosteroids Inflammation *Methylprednisolone
Aceponate
*Diuretic Pulmonary edema Frusemide
Narcotic analgesia Severe pain *Fentanyl
Neuroleptics Mood stabilizer * Cariprazine
*Vitamin K Bleeding disorders Phytonadione
Answer 5
Drug Major drug
group/class
Common
routes for
administratio
n
Mode of
action
Adverse
Reactions
Describe at least
3 Nursing
Considerations
for each of the
below
disorder
*Antimineralocorticoid Menopause Estrogen and Progesterone
Hypnotics, sedatives Sedative *Melatonin
Hypoglycaemics *Metformin Glucagon
Insulin *Acarbose Insulin
*Beta blockers Hypertension Propranolol
*Bronchodilators Asthma Salbutamol
Electrolyte solutions Rehydration *Plasmalyte A
Laxatives/aperients Constipation *Lactulose
Ophthalmic, otic *Dexamethasone Acetazolamide
Nasal medications *Nasal spray Phenylephedrine
*Teratogenic Pregnancy prevention Estrogen and Progesterone
Corticosteroids Inflammation *Methylprednisolone
Aceponate
*Diuretic Pulmonary edema Frusemide
Narcotic analgesia Severe pain *Fentanyl
Neuroleptics Mood stabilizer * Cariprazine
*Vitamin K Bleeding disorders Phytonadione
Answer 5
Drug Major drug
group/class
Common
routes for
administratio
n
Mode of
action
Adverse
Reactions
Describe at least
3 Nursing
Considerations
for each of the
below
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
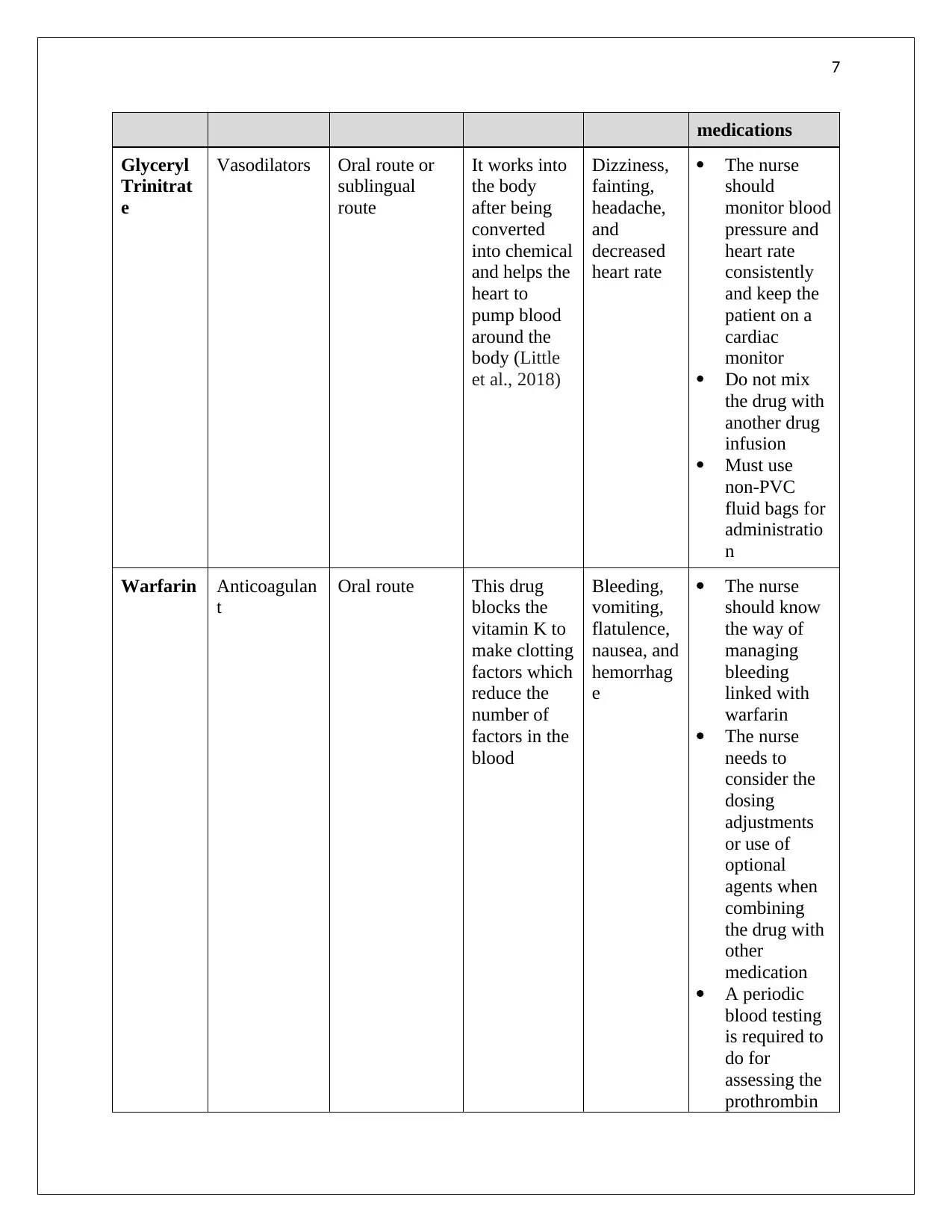
medications
Glyceryl
Trinitrat
e
Vasodilators Oral route or
sublingual
route
It works into
the body
after being
converted
into chemical
and helps the
heart to
pump blood
around the
body (Little
et al., 2018)
Dizziness,
fainting,
headache,
and
decreased
heart rate
The nurse
should
monitor blood
pressure and
heart rate
consistently
and keep the
patient on a
cardiac
monitor
Do not mix
the drug with
another drug
infusion
Must use
non-PVC
fluid bags for
administratio
n
Warfarin Anticoagulan
t
Oral route This drug
blocks the
vitamin K to
make clotting
factors which
reduce the
number of
factors in the
blood
Bleeding,
vomiting,
flatulence,
nausea, and
hemorrhag
e
The nurse
should know
the way of
managing
bleeding
linked with
warfarin
The nurse
needs to
consider the
dosing
adjustments
or use of
optional
agents when
combining
the drug with
other
medication
A periodic
blood testing
is required to
do for
assessing the
prothrombin
medications
Glyceryl
Trinitrat
e
Vasodilators Oral route or
sublingual
route
It works into
the body
after being
converted
into chemical
and helps the
heart to
pump blood
around the
body (Little
et al., 2018)
Dizziness,
fainting,
headache,
and
decreased
heart rate
The nurse
should
monitor blood
pressure and
heart rate
consistently
and keep the
patient on a
cardiac
monitor
Do not mix
the drug with
another drug
infusion
Must use
non-PVC
fluid bags for
administratio
n
Warfarin Anticoagulan
t
Oral route This drug
blocks the
vitamin K to
make clotting
factors which
reduce the
number of
factors in the
blood
Bleeding,
vomiting,
flatulence,
nausea, and
hemorrhag
e
The nurse
should know
the way of
managing
bleeding
linked with
warfarin
The nurse
needs to
consider the
dosing
adjustments
or use of
optional
agents when
combining
the drug with
other
medication
A periodic
blood testing
is required to
do for
assessing the
prothrombin
8
time of the
patients
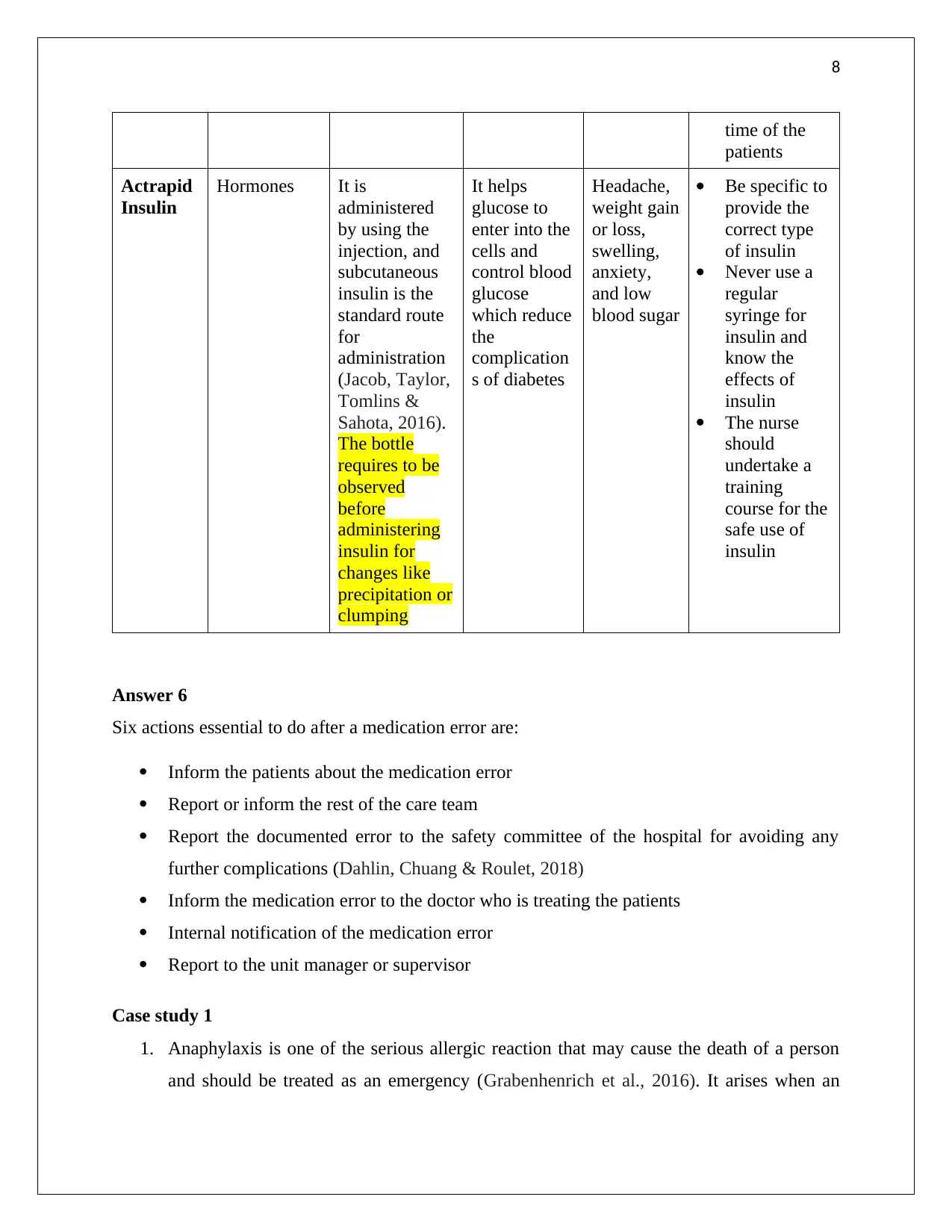
Actrapid
Insulin
Hormones It is
administered
by using the
injection, and
subcutaneous
insulin is the
standard route
for
administration
(Jacob, Taylor,
Tomlins &
Sahota, 2016).
The bottle
requires to be
observed
before
administering
insulin for
changes like
precipitation or
clumping
It helps
glucose to
enter into the
cells and
control blood
glucose
which reduce
the
complication
s of diabetes
Headache,
weight gain
or loss,
swelling,
anxiety,
and low
blood sugar
Be specific to
provide the
correct type
of insulin
Never use a
regular
syringe for
insulin and
know the
effects of
insulin
The nurse
should
undertake a
training
course for the
safe use of
insulin
Answer 6
Six actions essential to do after a medication error are:
Inform the patients about the medication error
Report or inform the rest of the care team
Report the documented error to the safety committee of the hospital for avoiding any
further complications (Dahlin, Chuang & Roulet, 2018)
Inform the medication error to the doctor who is treating the patients
Internal notification of the medication error
Report to the unit manager or supervisor
Case study 1
1. Anaphylaxis is one of the serious allergic reaction that may cause the death of a person
and should be treated as an emergency (Grabenhenrich et al., 2016). It arises when an
time of the
patients
Actrapid
Insulin
Hormones It is
administered
by using the
injection, and
subcutaneous
insulin is the
standard route
for
administration
(Jacob, Taylor,
Tomlins &
Sahota, 2016).
The bottle
requires to be
observed
before
administering
insulin for
changes like
precipitation or
clumping
It helps
glucose to
enter into the
cells and
control blood
glucose
which reduce
the
complication
s of diabetes
Headache,
weight gain
or loss,
swelling,
anxiety,
and low
blood sugar
Be specific to
provide the
correct type
of insulin
Never use a
regular
syringe for
insulin and
know the
effects of
insulin
The nurse
should
undertake a
training
course for the
safe use of
insulin
Answer 6
Six actions essential to do after a medication error are:
Inform the patients about the medication error
Report or inform the rest of the care team
Report the documented error to the safety committee of the hospital for avoiding any
further complications (Dahlin, Chuang & Roulet, 2018)
Inform the medication error to the doctor who is treating the patients
Internal notification of the medication error
Report to the unit manager or supervisor
Case study 1
1. Anaphylaxis is one of the serious allergic reaction that may cause the death of a person
and should be treated as an emergency (Grabenhenrich et al., 2016). It arises when an
9
individual is exposed to an allergen to which he is allergic. At the cellular level, the
antibodies travel to the mast cells and release chemicals that cause symptoms of
anaphylaxis. It is beneficial to know the signs as well as symptoms of anaphylaxis for the
person to avoid the allergic reaction. Food, medicines, latex, insect stings, and exercise
are the five common agents that may trigger anaphylaxis. In the given case, Mr. Brown is
suggested to take adrenaline, which quickly reverses the effects of the anaphylactic
reaction.
2. The mechanism of action of adrenaline drug: It acts on alpha as well as a beta-adrenergic
receptor. It decreases vasodilation and raises vascular permeability through its action on
receptors. It also relaxes the smooth muscle of bronchial that helps in alleviating
wheezing and bronchospasm that occur during anaphylaxis (Chen & Wang, 2017).
It is administered through auto-injector and reverses the symptoms of anaphylaxis by
acting on both the beta and alpha adrenergic receptors in the body. It prevents the blood
pressure to fall by redirecting the blood to essential organs. It is given by intramuscular
injection to ensure that the drug is injected into the muscle because absorption is more
rapid and reliable through the intramuscular site.
3. As an EN, I will provide emergency care to Mr. Brown, remove the allergen, lay the
patient flat, inject Epinephrine, and provide oxygen. Yes, it is within my scope of practice
to supply oxygen to the patient because any delay in administering oxygen can lead to the
death of the patient. I will communicate with the patient to assess the knowledge of Mr.
Brown regarding the previous allergic reactions and assess the patient for all kinds of
allergies. I would consult with the staff of the emergency department and the doctor who
used to treat Mr. Brown. As an EN, it is required to document the allergy status of Mr.
Brown on the medication chart and respiratory rate.
Case study 2
1. Mrs. Jones is having a low level of hemoglobin, and surgery will take place on Monday
morning. For doing surgery, she requires to administer a blood transfusion. Low
hemoglobin occurs due to anemia, chronic kidney disease, and thalassemia (Rodrigo et
al., 2018).
2. A mild or severe complication can occur during blood transfusion such as blood-borne
infections, acute immune hemolytic reaction, and affect the bone marrow (Tan et al.,
individual is exposed to an allergen to which he is allergic. At the cellular level, the
antibodies travel to the mast cells and release chemicals that cause symptoms of
anaphylaxis. It is beneficial to know the signs as well as symptoms of anaphylaxis for the
person to avoid the allergic reaction. Food, medicines, latex, insect stings, and exercise
are the five common agents that may trigger anaphylaxis. In the given case, Mr. Brown is
suggested to take adrenaline, which quickly reverses the effects of the anaphylactic
reaction.
2. The mechanism of action of adrenaline drug: It acts on alpha as well as a beta-adrenergic
receptor. It decreases vasodilation and raises vascular permeability through its action on
receptors. It also relaxes the smooth muscle of bronchial that helps in alleviating
wheezing and bronchospasm that occur during anaphylaxis (Chen & Wang, 2017).
It is administered through auto-injector and reverses the symptoms of anaphylaxis by
acting on both the beta and alpha adrenergic receptors in the body. It prevents the blood
pressure to fall by redirecting the blood to essential organs. It is given by intramuscular
injection to ensure that the drug is injected into the muscle because absorption is more
rapid and reliable through the intramuscular site.
3. As an EN, I will provide emergency care to Mr. Brown, remove the allergen, lay the
patient flat, inject Epinephrine, and provide oxygen. Yes, it is within my scope of practice
to supply oxygen to the patient because any delay in administering oxygen can lead to the
death of the patient. I will communicate with the patient to assess the knowledge of Mr.
Brown regarding the previous allergic reactions and assess the patient for all kinds of
allergies. I would consult with the staff of the emergency department and the doctor who
used to treat Mr. Brown. As an EN, it is required to document the allergy status of Mr.
Brown on the medication chart and respiratory rate.
Case study 2
1. Mrs. Jones is having a low level of hemoglobin, and surgery will take place on Monday
morning. For doing surgery, she requires to administer a blood transfusion. Low
hemoglobin occurs due to anemia, chronic kidney disease, and thalassemia (Rodrigo et
al., 2018).
2. A mild or severe complication can occur during blood transfusion such as blood-borne
infections, acute immune hemolytic reaction, and affect the bone marrow (Tan et al.,
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10
2017). The other complications of blood transfusion that a person needs to be aware of
are acute kidney failure, lung problems, anemia and shock. If a patient experienced
delayed potential reaction, then the nurse should stop the transfusion and replace the
donor blood with the normal saline.
Blood-borne infections: Blood-borne infections caused by bacteria or viruses
transmitted to the body of a person while transmitting blood. It may also happen if the
blood infections are not tested by the physicians before blood transfusion.
Acute immune hemolytic reaction: It occurs within 24 hours of the blood transfusion
due to the rapid destruction of red blood cells of the donor by host antibodies (IgG). The
reaction is associated with hemolysis and occurs after transfusing a few millilitres of
blood.
Acute kidney failure: It happens when the kidneys of the person lose the ability to
remove waste materials from the blood. Blood transfusion reaction creates clotting of
blood within the blood vessels of the kidney that cause kidney failure.
Lung problems: It happens when the body struggles to get enough oxygen and have
shortness of breath. It refers to the situation in which lungs fill with more fluid at the time
of blood transfusion.
3. I will explain the signs and symptoms of blood transfusion reaction like back pain, fever,
chills, skin flushing, fainting, itching, flank pain, dizziness, shortness of breath, or dark
urine to Mrs. Jones so that she would be aware of the reactions and take immediate
precautions. She should be aware of receiving too much blood, which causes a
transfusion reaction.
4. Blood and blood products are to be transported under the same temperature as when
stored, and the temperature can be maintained by using frozen or chilled packs (Hong et
al., 2016). Minimal physical handling of all the blood components needs to be practised
while handling the products of blood. Blood products are transported under the same
temperature condition as when they are stored which is maintained by using cardboard
boxes with inserted thermal insulation and several configurations of chilled coolant
packs. The laboratories and hospitals also use the shippers of blood service to transport
blood products. The blood components need to be handled by ensuring that the products
are not exposed to an outside temperature for more than 30 minutes and the packaging of
2017). The other complications of blood transfusion that a person needs to be aware of
are acute kidney failure, lung problems, anemia and shock. If a patient experienced
delayed potential reaction, then the nurse should stop the transfusion and replace the
donor blood with the normal saline.
Blood-borne infections: Blood-borne infections caused by bacteria or viruses
transmitted to the body of a person while transmitting blood. It may also happen if the
blood infections are not tested by the physicians before blood transfusion.
Acute immune hemolytic reaction: It occurs within 24 hours of the blood transfusion
due to the rapid destruction of red blood cells of the donor by host antibodies (IgG). The
reaction is associated with hemolysis and occurs after transfusing a few millilitres of
blood.
Acute kidney failure: It happens when the kidneys of the person lose the ability to
remove waste materials from the blood. Blood transfusion reaction creates clotting of
blood within the blood vessels of the kidney that cause kidney failure.
Lung problems: It happens when the body struggles to get enough oxygen and have
shortness of breath. It refers to the situation in which lungs fill with more fluid at the time
of blood transfusion.
3. I will explain the signs and symptoms of blood transfusion reaction like back pain, fever,
chills, skin flushing, fainting, itching, flank pain, dizziness, shortness of breath, or dark
urine to Mrs. Jones so that she would be aware of the reactions and take immediate
precautions. She should be aware of receiving too much blood, which causes a
transfusion reaction.
4. Blood and blood products are to be transported under the same temperature as when
stored, and the temperature can be maintained by using frozen or chilled packs (Hong et
al., 2016). Minimal physical handling of all the blood components needs to be practised
while handling the products of blood. Blood products are transported under the same
temperature condition as when they are stored which is maintained by using cardboard
boxes with inserted thermal insulation and several configurations of chilled coolant
packs. The laboratories and hospitals also use the shippers of blood service to transport
blood products. The blood components need to be handled by ensuring that the products
are not exposed to an outside temperature for more than 30 minutes and the packaging of
11
the products should be checked or examined before sending to other health practitioners.
The blood can be disposed of by tie a knot in the tubing above the needle and drain the
blood.
Being an EN, an individual would require to check the type of the blood of both donor
and the receiver to avoid transfusion reaction because every person has different blood
types. EN could check blood types by testing the blood in the laboratory of the hospital
and labelled the blood bag with the blood type. It is also necessary to test the donated
blood carefully to find out the blood type and any other infections in the blood.
Case study 3
1. Jack has been prescribed to take IV fluids because he is in a state of depleted water and
normal saline (Baddour et al., 2015). He has low blood volume or if he may be
dehydrated due to cholecystitis. He may be prescribed to take D5W (means 5% Dextrose
in water) IV fluid as it contains hypotonic sugar water.
2. The nurse needs to record the fluid volume, the body weight of the patient, and urinary
output.
3. Several complications included in the IV therapy, which are as follows:
Infiltration: It mainly occurs when there is IV fluid leak into the tissues.
Hematoma: It occurs due to leakage of blood from the blood vessel into the tissues.
Air embolism: It takes place when a bulk of air enters into the vein of the patient through
the set of IV administration.
Phlebitis: It is the swelling of a vein that occurs as a result of a pH agent entered during
IV administration (Ramsay et al., 2018).
Extravasation: It refers to the leaky of vesicant drugs into the adjoining tissues and causes
severe damage to the local tissues.
Hypersensitivity: It can be life-threatening and should be recognized and treated
immediately.
4. The most common electrolyte imbalance identified is potassium (K) that help to conduct
muscle contraction, keep blood pressure and regulate the flow of fluids (Giordano et al.,
2016). Changes in the diet are given to treat potassium electrolyte. It is to be monitored
by doing a potassium blood test to check the increase or decrease in the amount of
potassium in blood.
the products should be checked or examined before sending to other health practitioners.
The blood can be disposed of by tie a knot in the tubing above the needle and drain the
blood.
Being an EN, an individual would require to check the type of the blood of both donor
and the receiver to avoid transfusion reaction because every person has different blood
types. EN could check blood types by testing the blood in the laboratory of the hospital
and labelled the blood bag with the blood type. It is also necessary to test the donated
blood carefully to find out the blood type and any other infections in the blood.
Case study 3
1. Jack has been prescribed to take IV fluids because he is in a state of depleted water and
normal saline (Baddour et al., 2015). He has low blood volume or if he may be
dehydrated due to cholecystitis. He may be prescribed to take D5W (means 5% Dextrose
in water) IV fluid as it contains hypotonic sugar water.
2. The nurse needs to record the fluid volume, the body weight of the patient, and urinary
output.
3. Several complications included in the IV therapy, which are as follows:
Infiltration: It mainly occurs when there is IV fluid leak into the tissues.
Hematoma: It occurs due to leakage of blood from the blood vessel into the tissues.
Air embolism: It takes place when a bulk of air enters into the vein of the patient through
the set of IV administration.
Phlebitis: It is the swelling of a vein that occurs as a result of a pH agent entered during
IV administration (Ramsay et al., 2018).
Extravasation: It refers to the leaky of vesicant drugs into the adjoining tissues and causes
severe damage to the local tissues.
Hypersensitivity: It can be life-threatening and should be recognized and treated
immediately.
4. The most common electrolyte imbalance identified is potassium (K) that help to conduct
muscle contraction, keep blood pressure and regulate the flow of fluids (Giordano et al.,
2016). Changes in the diet are given to treat potassium electrolyte. It is to be monitored
by doing a potassium blood test to check the increase or decrease in the amount of
potassium in blood.
12
5. As a nurse, I will educate Jack by saying or explaining the benefit of administering IV
fluids and assure him of no risks during the treatment. I will kindly tell him that IV fluids
are must to give him for controlling the heartbeat. I would report this to the doctor to talk
to him in getting the IV fluid.
5. As a nurse, I will educate Jack by saying or explaining the benefit of administering IV
fluids and assure him of no risks during the treatment. I will kindly tell him that IV fluids
are must to give him for controlling the heartbeat. I would report this to the doctor to talk
to him in getting the IV fluid.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
13
References
Almazroo, O. A., Miah, M. K., & Venkataramanan, R. (2017). Drug metabolism in the
liver. Clinics in liver disease, 21(1), 1-20.
Baddour, L. M., Wilson, W. R., Bayer, A. S., Fowler Jr, V. G., Tleyjeh, I. M., Rybak, M. J., ... &
Bolger, A. F. (2015). Infective endocarditis in adults: diagnosis, antimicrobial therapy,
and management of complications: a scientific statement for healthcare professionals
from the American Heart Association. Circulation, 132(15), 1435-1486.
Califf, R. M., McCall, J., & Mark, D. B. (2017). Cosmetics, regulations, and the public health:
understanding the safety of medical and other products. JAMA internal medicine, 177(8),
1080-1082.
Chen, D., & Wang, Z. (2017). Adrenaline inhibits osteogenesis via repressing miR‐21
expression. Cell biology international, 41(1), 8-15.
Dahlin, K. B., Chuang, Y. T., & Roulet, T. J. (2018). Opportunity, motivation, and ability to
learn from failures and errors: review, synthesis, and ways to move forward. Academy of
Management Annals, 12(1), 252-277.
Giordano, M., Ciarambino, T., Castellino, P., Malatino, L., Di Somma, S., Biolo, G., ... &
Adinolfi, L. E. (2016). Diseases associated with electrolyte imbalance in the ED: age-
related differences. The American journal of emergency medicine, 34(10), 1923-1926.
Grabenhenrich, L. B., Dölle, S., Moneret-Vautrin, A., Köhli, A., Lange, L., Spindler, T., ... &
Scherer, K. (2016). Anaphylaxis in children and adolescents: the European Anaphylaxis
Registry. Journal of allergy and clinical immunology, 137(4), 1128-1137.
Hong, H., Xiao, W., Lazarus, H. M., Good, C. E., Maitta, R. W., & Jacobs, M. R. (2016).
Detection of septic transfusion reactions to platelet transfusions by active and passive
surveillance. Blood, 127(4), 496-502.
Hörmann, K., & Zimmer, A. (2016). Drug delivery and drug targeting with parenteral lipid
nanoemulsions—A review. Journal of Controlled Release, 223, 85-98.
References
Almazroo, O. A., Miah, M. K., & Venkataramanan, R. (2017). Drug metabolism in the
liver. Clinics in liver disease, 21(1), 1-20.
Baddour, L. M., Wilson, W. R., Bayer, A. S., Fowler Jr, V. G., Tleyjeh, I. M., Rybak, M. J., ... &
Bolger, A. F. (2015). Infective endocarditis in adults: diagnosis, antimicrobial therapy,
and management of complications: a scientific statement for healthcare professionals
from the American Heart Association. Circulation, 132(15), 1435-1486.
Califf, R. M., McCall, J., & Mark, D. B. (2017). Cosmetics, regulations, and the public health:
understanding the safety of medical and other products. JAMA internal medicine, 177(8),
1080-1082.
Chen, D., & Wang, Z. (2017). Adrenaline inhibits osteogenesis via repressing miR‐21
expression. Cell biology international, 41(1), 8-15.
Dahlin, K. B., Chuang, Y. T., & Roulet, T. J. (2018). Opportunity, motivation, and ability to
learn from failures and errors: review, synthesis, and ways to move forward. Academy of
Management Annals, 12(1), 252-277.
Giordano, M., Ciarambino, T., Castellino, P., Malatino, L., Di Somma, S., Biolo, G., ... &
Adinolfi, L. E. (2016). Diseases associated with electrolyte imbalance in the ED: age-
related differences. The American journal of emergency medicine, 34(10), 1923-1926.
Grabenhenrich, L. B., Dölle, S., Moneret-Vautrin, A., Köhli, A., Lange, L., Spindler, T., ... &
Scherer, K. (2016). Anaphylaxis in children and adolescents: the European Anaphylaxis
Registry. Journal of allergy and clinical immunology, 137(4), 1128-1137.
Hong, H., Xiao, W., Lazarus, H. M., Good, C. E., Maitta, R. W., & Jacobs, M. R. (2016).
Detection of septic transfusion reactions to platelet transfusions by active and passive
surveillance. Blood, 127(4), 496-502.
Hörmann, K., & Zimmer, A. (2016). Drug delivery and drug targeting with parenteral lipid
nanoemulsions—A review. Journal of Controlled Release, 223, 85-98.
14
Jacob, D., Taylor, M. J., Tomlins, P., & Sahota, T. S. (2016). Synthesis and identification of
FITC-insulin conjugates produced using human insulin and insulin analogues for
biomedical applications. Journal of fluorescence, 26(2), 617-629.
Jones, H. M., Chen, Y., Gibson, C., Heimbach, T., Parrott, N., Peters, S. A., ... & Hall, S. D.
(2015). Physiologically based pharmacokinetic modeling in drug discovery and
development: a pharmaceutical industry perspective. Clinical Pharmacology &
Therapeutics, 97(3), 247-262.
Kawase, A., Yamamoto, T., Egashira, S., & Iwaki, M. (2016). Stereoselective inhibition of
methotrexate excretion by glucuronides of nonsteroidal anti-inflammatory drugs via
multidrug resistance proteins 2 and 4. Journal of Pharmacology and Experimental
Therapeutics, 356(2), 366-374.
Little, M. W., Macdonald, A. C., Boardman, P., Bratby, M. J., Anthony, S., Hadi, M., &
Tapping, C. R. (2018). Effects of sublingual glyceryl trinitrate administration on the
quality of preprocedure CT angiography performed to plan prostate artery
embolization. Journal of Vascular and Interventional Radiology, 29(2), 225-228.
Liu, X., Yang, Y., Gao, B., Li, Y., & Wan, Y. (2017). Environmentally friendly slow-release
urea fertilizers based on waste frying oil for sustained nutrient release. ACS Sustainable
Chemistry & Engineering, 5(7), 6036-6045.
Noale, M., Veronese, N., Perin, P. C., Pilotto, A., Tiengo, A., Crepaldi, G., & Maggi, S. (2016).
Polypharmacy in elderly patients with type 2 diabetes receiving oral antidiabetic
treatment. Acta diabetologica, 53(2), 323-330.
Pridgen, E. M., Alexis, F., & Farokhzad, O. C. (2015). Polymeric nanoparticle drug delivery
technologies for oral delivery applications. Expert opinion on drug delivery, 12(9), 1459-
1473.
Ramsay, G., Baggaley, A., Shaw, P. V., Soltanmohammadi, E., Ventham, N., Shi, N. G., ... &
Kilkenny, J. (2018). Variability in the prescribing of intravenous fluids: A cross sectional
multicentre analysis of clinical practice. International Journal of Surgery, 51, 199-204.
Jacob, D., Taylor, M. J., Tomlins, P., & Sahota, T. S. (2016). Synthesis and identification of
FITC-insulin conjugates produced using human insulin and insulin analogues for
biomedical applications. Journal of fluorescence, 26(2), 617-629.
Jones, H. M., Chen, Y., Gibson, C., Heimbach, T., Parrott, N., Peters, S. A., ... & Hall, S. D.
(2015). Physiologically based pharmacokinetic modeling in drug discovery and
development: a pharmaceutical industry perspective. Clinical Pharmacology &
Therapeutics, 97(3), 247-262.
Kawase, A., Yamamoto, T., Egashira, S., & Iwaki, M. (2016). Stereoselective inhibition of
methotrexate excretion by glucuronides of nonsteroidal anti-inflammatory drugs via
multidrug resistance proteins 2 and 4. Journal of Pharmacology and Experimental
Therapeutics, 356(2), 366-374.
Little, M. W., Macdonald, A. C., Boardman, P., Bratby, M. J., Anthony, S., Hadi, M., &
Tapping, C. R. (2018). Effects of sublingual glyceryl trinitrate administration on the
quality of preprocedure CT angiography performed to plan prostate artery
embolization. Journal of Vascular and Interventional Radiology, 29(2), 225-228.
Liu, X., Yang, Y., Gao, B., Li, Y., & Wan, Y. (2017). Environmentally friendly slow-release
urea fertilizers based on waste frying oil for sustained nutrient release. ACS Sustainable
Chemistry & Engineering, 5(7), 6036-6045.
Noale, M., Veronese, N., Perin, P. C., Pilotto, A., Tiengo, A., Crepaldi, G., & Maggi, S. (2016).
Polypharmacy in elderly patients with type 2 diabetes receiving oral antidiabetic
treatment. Acta diabetologica, 53(2), 323-330.
Pridgen, E. M., Alexis, F., & Farokhzad, O. C. (2015). Polymeric nanoparticle drug delivery
technologies for oral delivery applications. Expert opinion on drug delivery, 12(9), 1459-
1473.
Ramsay, G., Baggaley, A., Shaw, P. V., Soltanmohammadi, E., Ventham, N., Shi, N. G., ... &
Kilkenny, J. (2018). Variability in the prescribing of intravenous fluids: A cross sectional
multicentre analysis of clinical practice. International Journal of Surgery, 51, 199-204.
15
Rodrigo, R., Allen, A., Manampreri, A., Perera, L., Fisher, C. A., Allen, S., ... &
Premawardhena, A. (2018). Haemoglobin variants, iron status and anaemia in Sri Lankan
adolescents with low red cell indices: A cross sectional survey. Blood Cells, Molecules,
and Diseases, 71, 11-15.
Ryman, J. T., & Meibohm, B. (2017). Pharmacokinetics of monoclonal antibodies. CPT:
pharmacometrics & systems pharmacology, 6(9), 576-588.
Tan, A. J. Q., Lee, C. C. S., Lin, P. Y., Cooper, S., Lau, L. S. T., Chua, W. L., & Liaw, S. Y.
(2017). Designing and evaluating the effectiveness of a serious game for safe
administration of blood transfusion: A randomized controlled trial. Nurse education
today, 55, 38-44.
Rodrigo, R., Allen, A., Manampreri, A., Perera, L., Fisher, C. A., Allen, S., ... &
Premawardhena, A. (2018). Haemoglobin variants, iron status and anaemia in Sri Lankan
adolescents with low red cell indices: A cross sectional survey. Blood Cells, Molecules,
and Diseases, 71, 11-15.
Ryman, J. T., & Meibohm, B. (2017). Pharmacokinetics of monoclonal antibodies. CPT:
pharmacometrics & systems pharmacology, 6(9), 576-588.
Tan, A. J. Q., Lee, C. C. S., Lin, P. Y., Cooper, S., Lau, L. S. T., Chua, W. L., & Liaw, S. Y.
(2017). Designing and evaluating the effectiveness of a serious game for safe
administration of blood transfusion: A randomized controlled trial. Nurse education
today, 55, 38-44.
1 out of 16


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.