Optimal Use of Medicines: A Comprehensive Questions and Answers Review
VerifiedAdded on 2020/01/07
|30
|7225
|216
Homework Assignment
AI Summary
This assignment provides a detailed analysis of the optimal use of medicines, addressing multiple-choice and short-answer questions. It covers various topics, including different classes of antidepressants (like RIMAs and Heterocyclics), clozapine management (including PBS eligibility, brand names, monitoring requirements, and lifestyle factors), and diabetes management (focusing on insulin types, blood glucose monitoring, hypoglycemia symptoms, and dietary recommendations). The assignment also explores malaria prevention, including vaccination recommendations and counselling points. The analysis includes specific examples, such as the use of Mianserin and Apidrasolostar, and emphasizes the importance of patient counseling, monitoring, and lifestyle factors in ensuring effective and safe medication use. The document references guidelines and resources from reputable sources like the Mayo Clinic, MedicineNet, and the CDC.

Optimal Use of Medicines 1
Optimal Use of Medicines - Questions & Answers
Student’s Name:
Instructor’s Name:
Institution:
Date:
Optimal Use of Medicines - Questions & Answers
Student’s Name:
Instructor’s Name:
Institution:
Date:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Optimal Use of Medicines 2
Part B: Short answer questions
Question one
a) Give TWO examples (including starting dose) from different antidepressant classes
that may be prescribed for Joe.
1. Reversible inhibitors of Monoamine Oxidase-A (RIMAs)
Moclobimide (Aurorix, ARIMA) 450-900mg -divided doses morning preference
Uses:
1. Depression with fatigue
2. Non sedating
3. No- sexual side effects
2. Heterocyclics
Mianserin (tolvon, lumin) 30-90 mg divided doses evening preference
Safety in medically ill patients
Choose ONE option only and provide at least FIVE counselling points for discussion
with Joe on first-time dispensing.
2. Heterocyclics
Mianserin (tolvon, lumin) 30-90 mg divided doses evening preference
Safety in medically ill patients
The five counselling points are:
Cognitive behavioural therapy
Interpersonal therapy
Exercise
Follow good balanced diet
Avoid or restrict alcohol
Do things that he will enjoy
Part B: Short answer questions
Question one
a) Give TWO examples (including starting dose) from different antidepressant classes
that may be prescribed for Joe.
1. Reversible inhibitors of Monoamine Oxidase-A (RIMAs)
Moclobimide (Aurorix, ARIMA) 450-900mg -divided doses morning preference
Uses:
1. Depression with fatigue
2. Non sedating
3. No- sexual side effects
2. Heterocyclics
Mianserin (tolvon, lumin) 30-90 mg divided doses evening preference
Safety in medically ill patients
Choose ONE option only and provide at least FIVE counselling points for discussion
with Joe on first-time dispensing.
2. Heterocyclics
Mianserin (tolvon, lumin) 30-90 mg divided doses evening preference
Safety in medically ill patients
The five counselling points are:
Cognitive behavioural therapy
Interpersonal therapy
Exercise
Follow good balanced diet
Avoid or restrict alcohol
Do things that he will enjoy
Optimal Use of Medicines 3
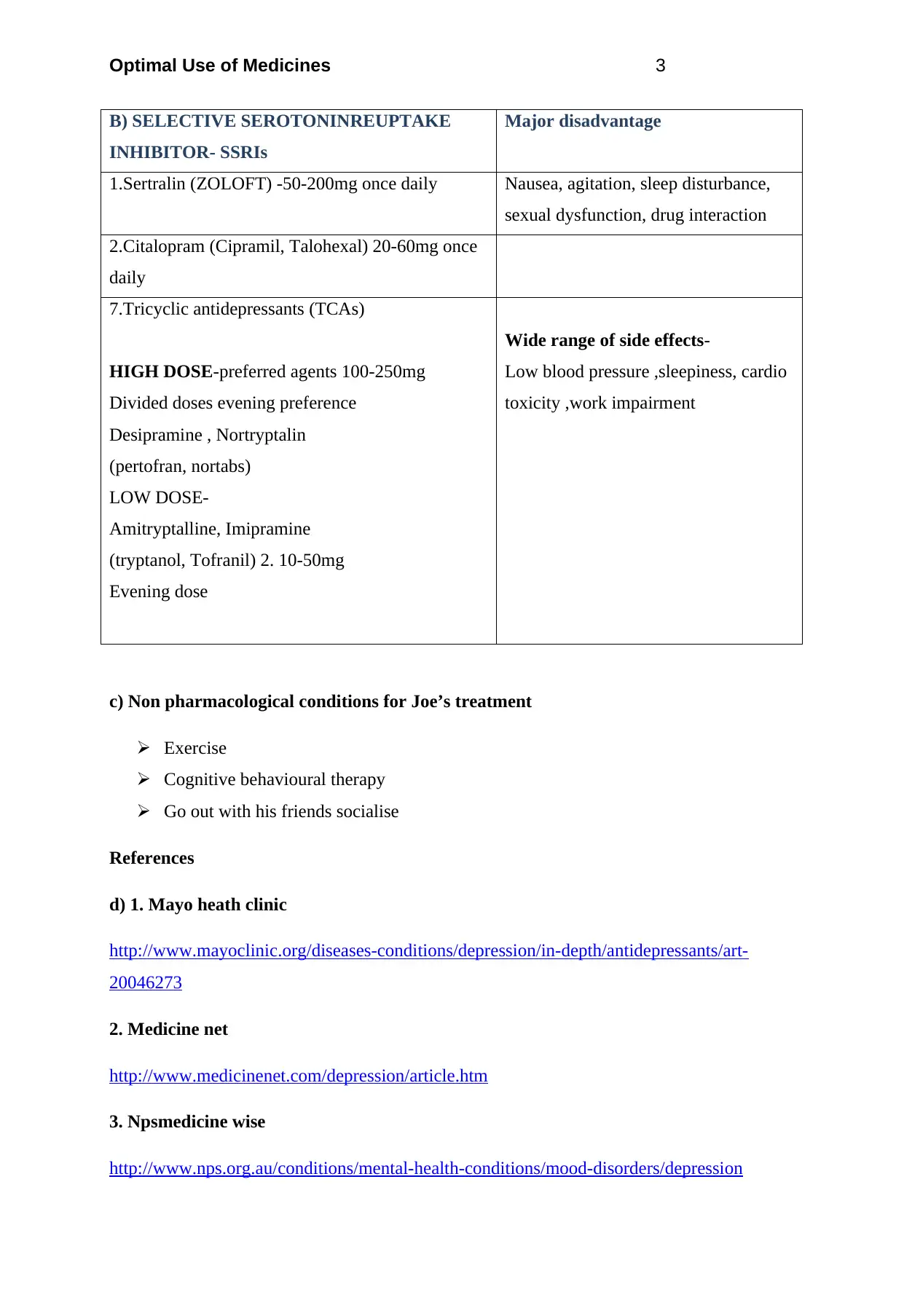
B) SELECTIVE SEROTONINREUPTAKE
INHIBITOR- SSRIs
Major disadvantage
1.Sertralin (ZOLOFT) -50-200mg once daily Nausea, agitation, sleep disturbance,
sexual dysfunction, drug interaction
2.Citalopram (Cipramil, Talohexal) 20-60mg once
daily
7.Tricyclic antidepressants (TCAs)
HIGH DOSE-preferred agents 100-250mg
Divided doses evening preference
Desipramine , Nortryptalin
(pertofran, nortabs)
LOW DOSE-
Amitryptalline, Imipramine
(tryptanol, Tofranil) 2. 10-50mg
Evening dose
Wide range of side effects-
Low blood pressure ,sleepiness, cardio
toxicity ,work impairment
c) Non pharmacological conditions for Joe’s treatment
Exercise
Cognitive behavioural therapy
Go out with his friends socialise
References
d) 1. Mayo heath clinic
http://www.mayoclinic.org/diseases-conditions/depression/in-depth/antidepressants/art-
20046273
2. Medicine net
http://www.medicinenet.com/depression/article.htm
3. Npsmedicine wise
http://www.nps.org.au/conditions/mental-health-conditions/mood-disorders/depression
B) SELECTIVE SEROTONINREUPTAKE
INHIBITOR- SSRIs
Major disadvantage
1.Sertralin (ZOLOFT) -50-200mg once daily Nausea, agitation, sleep disturbance,
sexual dysfunction, drug interaction
2.Citalopram (Cipramil, Talohexal) 20-60mg once
daily
7.Tricyclic antidepressants (TCAs)
HIGH DOSE-preferred agents 100-250mg
Divided doses evening preference
Desipramine , Nortryptalin
(pertofran, nortabs)
LOW DOSE-
Amitryptalline, Imipramine
(tryptanol, Tofranil) 2. 10-50mg
Evening dose
Wide range of side effects-
Low blood pressure ,sleepiness, cardio
toxicity ,work impairment
c) Non pharmacological conditions for Joe’s treatment
Exercise
Cognitive behavioural therapy
Go out with his friends socialise
References
d) 1. Mayo heath clinic
http://www.mayoclinic.org/diseases-conditions/depression/in-depth/antidepressants/art-
20046273
2. Medicine net
http://www.medicinenet.com/depression/article.htm
3. Npsmedicine wise
http://www.nps.org.au/conditions/mental-health-conditions/mood-disorders/depression
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

Optimal Use of Medicines 4
REFERENCE- Hickie et al.Aust NZJ Psychiatry 1999, 33, ,642-649
REFERENCE- Hickie et al.Aust NZJ Psychiatry 1999, 33, ,642-649
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Optimal Use of Medicines 5
Question two
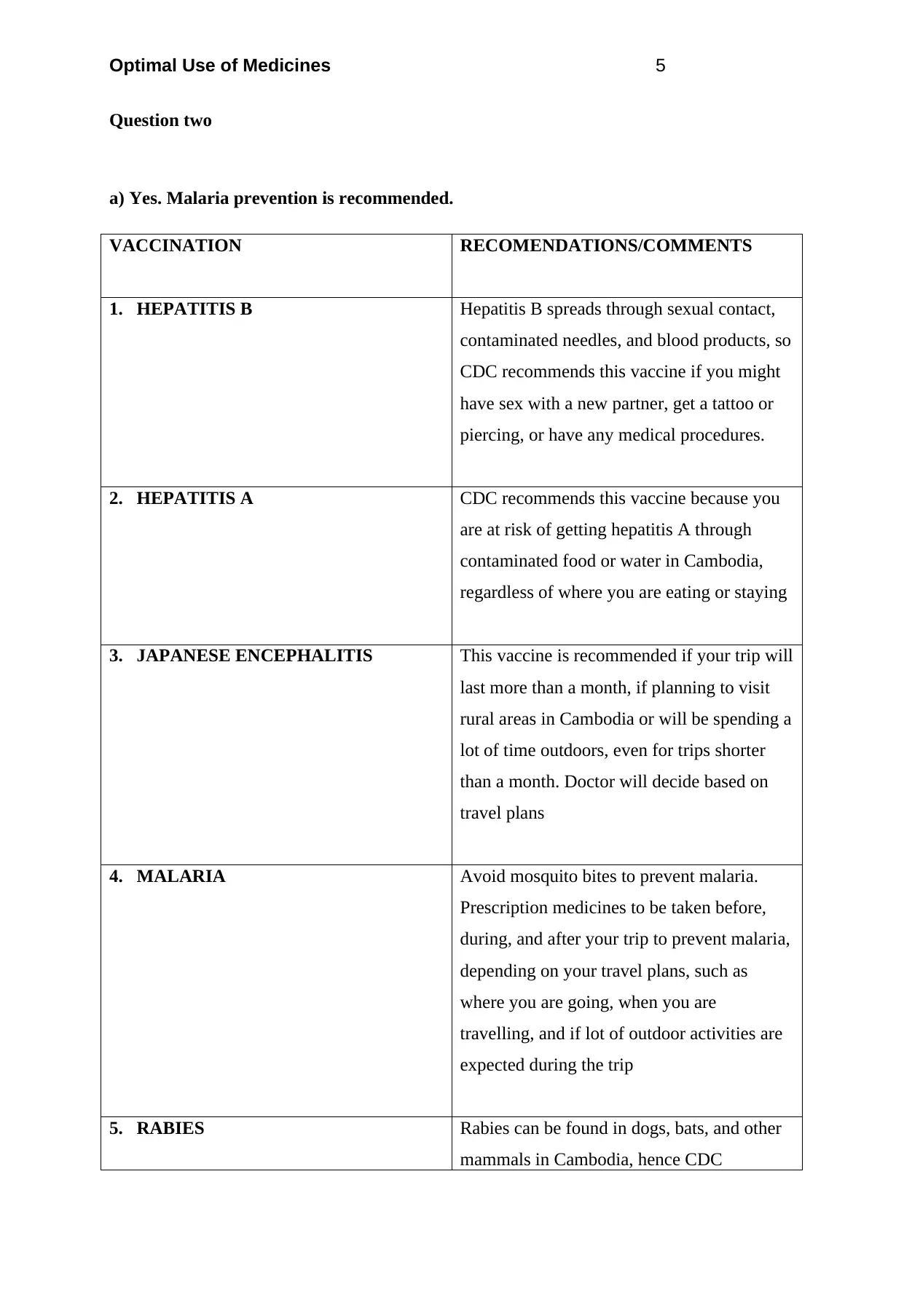
a) Yes. Malaria prevention is recommended.
VACCINATION RECOMENDATIONS/COMMENTS
1. HEPATITIS B Hepatitis B spreads through sexual contact,
contaminated needles, and blood products, so
CDC recommends this vaccine if you might
have sex with a new partner, get a tattoo or
piercing, or have any medical procedures.
2. HEPATITIS A CDC recommends this vaccine because you
are at risk of getting hepatitis A through
contaminated food or water in Cambodia,
regardless of where you are eating or staying
3. JAPANESE ENCEPHALITIS This vaccine is recommended if your trip will
last more than a month, if planning to visit
rural areas in Cambodia or will be spending a
lot of time outdoors, even for trips shorter
than a month. Doctor will decide based on
travel plans
4. MALARIA Avoid mosquito bites to prevent malaria.
Prescription medicines to be taken before,
during, and after your trip to prevent malaria,
depending on your travel plans, such as
where you are going, when you are
travelling, and if lot of outdoor activities are
expected during the trip
5. RABIES Rabies can be found in dogs, bats, and other
mammals in Cambodia, hence CDC
Question two
a) Yes. Malaria prevention is recommended.
VACCINATION RECOMENDATIONS/COMMENTS
1. HEPATITIS B Hepatitis B spreads through sexual contact,
contaminated needles, and blood products, so
CDC recommends this vaccine if you might
have sex with a new partner, get a tattoo or
piercing, or have any medical procedures.
2. HEPATITIS A CDC recommends this vaccine because you
are at risk of getting hepatitis A through
contaminated food or water in Cambodia,
regardless of where you are eating or staying
3. JAPANESE ENCEPHALITIS This vaccine is recommended if your trip will
last more than a month, if planning to visit
rural areas in Cambodia or will be spending a
lot of time outdoors, even for trips shorter
than a month. Doctor will decide based on
travel plans
4. MALARIA Avoid mosquito bites to prevent malaria.
Prescription medicines to be taken before,
during, and after your trip to prevent malaria,
depending on your travel plans, such as
where you are going, when you are
travelling, and if lot of outdoor activities are
expected during the trip
5. RABIES Rabies can be found in dogs, bats, and other
mammals in Cambodia, hence CDC
Optimal Use of Medicines 6
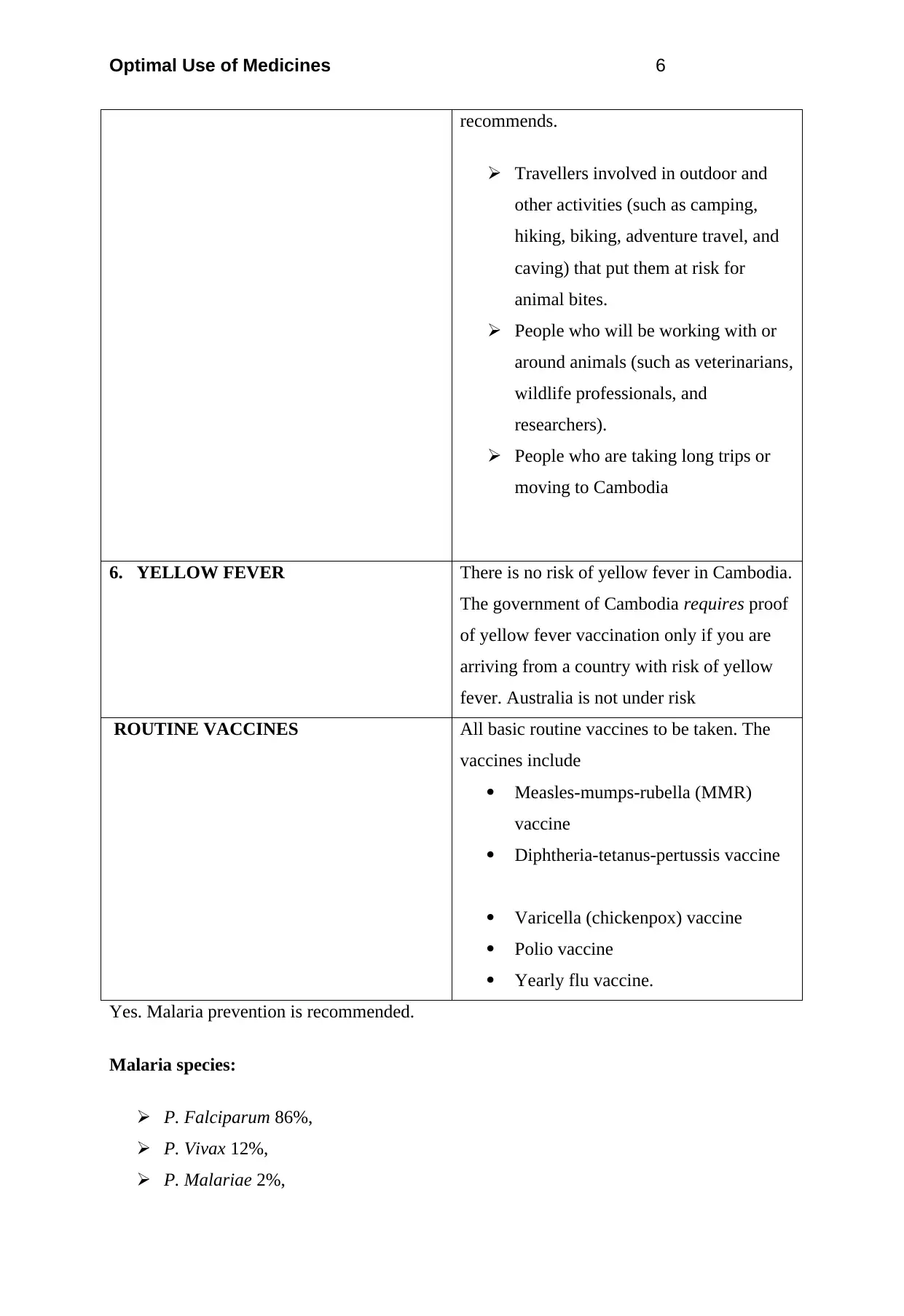
recommends.
Travellers involved in outdoor and
other activities (such as camping,
hiking, biking, adventure travel, and
caving) that put them at risk for
animal bites.
People who will be working with or
around animals (such as veterinarians,
wildlife professionals, and
researchers).
People who are taking long trips or
moving to Cambodia
6. YELLOW FEVER There is no risk of yellow fever in Cambodia.
The government of Cambodia requires proof
of yellow fever vaccination only if you are
arriving from a country with risk of yellow
fever. Australia is not under risk
ROUTINE VACCINES All basic routine vaccines to be taken. The
vaccines include
Measles-mumps-rubella (MMR)
vaccine
Diphtheria-tetanus-pertussis vaccine
Varicella (chickenpox) vaccine
Polio vaccine
Yearly flu vaccine.
Yes. Malaria prevention is recommended.
Malaria species:
P. Falciparum 86%,
P. Vivax 12%,
P. Malariae 2%,
recommends.
Travellers involved in outdoor and
other activities (such as camping,
hiking, biking, adventure travel, and
caving) that put them at risk for
animal bites.
People who will be working with or
around animals (such as veterinarians,
wildlife professionals, and
researchers).
People who are taking long trips or
moving to Cambodia
6. YELLOW FEVER There is no risk of yellow fever in Cambodia.
The government of Cambodia requires proof
of yellow fever vaccination only if you are
arriving from a country with risk of yellow
fever. Australia is not under risk
ROUTINE VACCINES All basic routine vaccines to be taken. The
vaccines include
Measles-mumps-rubella (MMR)
vaccine
Diphtheria-tetanus-pertussis vaccine
Varicella (chickenpox) vaccine
Polio vaccine
Yearly flu vaccine.
Yes. Malaria prevention is recommended.
Malaria species:
P. Falciparum 86%,
P. Vivax 12%,
P. Malariae 2%,
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Optimal Use of Medicines 7
P. Knowlesi Rare
b) Provide her with at least THREE non-pharmacological counselling/advice points on
malaria prevention
Mosquito repellents could be used on skin
Avoid eating and sleeping outdoors
Avoid stagnated water bodies
Three counselling points for the chosen drug protocol.
1. Drug resistance:
Chloroquine
Mefloquine
2. Recommended chemoprophylaxis:
In the provinces of BanteayMeanchey, Battambang, Kampot, Koh Kong, Odder Meanchey,
Pailin, PreahVihear, Pursat, and Siem Reap bordering Thailand: Atovaquone-proguanil or
doxycycline.
All other areas with malaria:
Atovaquone-Proguanil
Doxycycline Or
Mefloquine.
3. Caution to be practised in Areas with malaria: Present throughout the country,
including Siem Reap city. None in the city of Phnom Penh and at the temple complex at
Angkor Wat.
REFERENCE- Centres for Disease Control and Prevention-CDC 24/7 saving lives
protecting people
P. Knowlesi Rare
b) Provide her with at least THREE non-pharmacological counselling/advice points on
malaria prevention
Mosquito repellents could be used on skin
Avoid eating and sleeping outdoors
Avoid stagnated water bodies
Three counselling points for the chosen drug protocol.
1. Drug resistance:
Chloroquine
Mefloquine
2. Recommended chemoprophylaxis:
In the provinces of BanteayMeanchey, Battambang, Kampot, Koh Kong, Odder Meanchey,
Pailin, PreahVihear, Pursat, and Siem Reap bordering Thailand: Atovaquone-proguanil or
doxycycline.
All other areas with malaria:
Atovaquone-Proguanil
Doxycycline Or
Mefloquine.
3. Caution to be practised in Areas with malaria: Present throughout the country,
including Siem Reap city. None in the city of Phnom Penh and at the temple complex at
Angkor Wat.
REFERENCE- Centres for Disease Control and Prevention-CDC 24/7 saving lives
protecting people
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Optimal Use of Medicines 8
Question three
a) PBS patient eligibility requirements for community-based management of people
taking clozapine
Previous initial treatment under a psychiatrist for a period of no less than 18 weeks
The treating psychiatrist agrees the patient is suitable for community-based
management and prescribing
The patient's clozapine dosage is considered stable by the treating psychiatrist
Treatment is under the supervision and direction of the psychiatrist reviewing the
patient at regular intervals.
People taking clozapine need to be regularly assessed. Patients must be monitored for the
development of granulocytopenia and agranulocytosis. It is mandatory that assessment of
white blood cell count and absolute neutrophil count occur at least monthly.
A medical practitioner should request a quantity sufficient for up to one month's supply. Up
to 5 repeats will be authorised.
b) What TWO brands of clozapine are available in Australia and are they
substitutable?
1. CLOPINE 100
2. CLOZARIL 100
Clozapine alternatives are available if you are experiencing bothersome side effects or if the
medication is not adequately controlling your symptoms. These alternatives can include
therapy and medications (such as other atypical antipsychotics and typical antipsychotics).
The newer antipsychotic medications used as clozapine alternatives may have fewer serious
side effects than older, typical antipsychotics, although studies have shown conflicting
results.
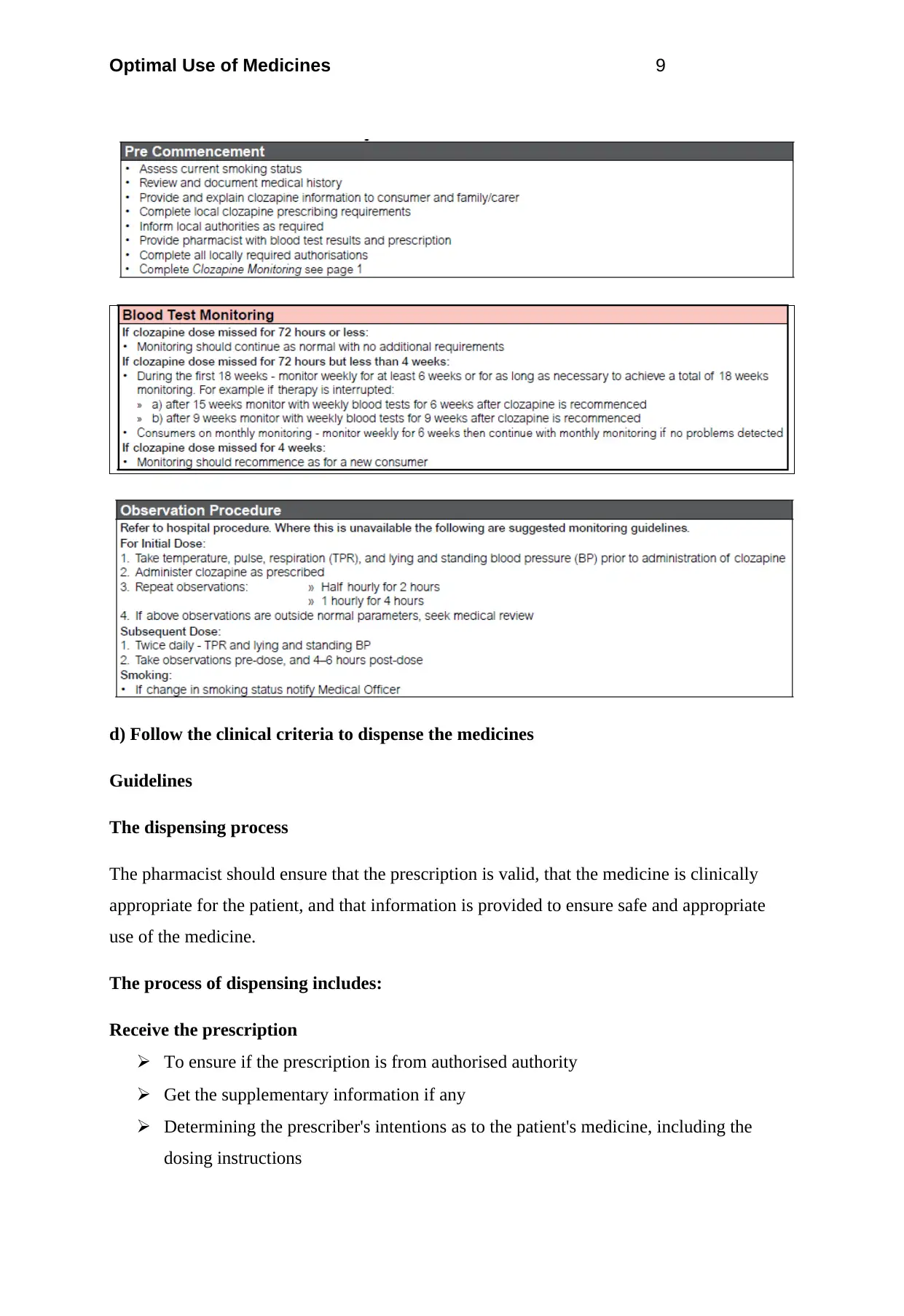
c) What monitoring is required when a patient is on clozapine?
Question three
a) PBS patient eligibility requirements for community-based management of people
taking clozapine
Previous initial treatment under a psychiatrist for a period of no less than 18 weeks
The treating psychiatrist agrees the patient is suitable for community-based
management and prescribing
The patient's clozapine dosage is considered stable by the treating psychiatrist
Treatment is under the supervision and direction of the psychiatrist reviewing the
patient at regular intervals.
People taking clozapine need to be regularly assessed. Patients must be monitored for the
development of granulocytopenia and agranulocytosis. It is mandatory that assessment of
white blood cell count and absolute neutrophil count occur at least monthly.
A medical practitioner should request a quantity sufficient for up to one month's supply. Up
to 5 repeats will be authorised.
b) What TWO brands of clozapine are available in Australia and are they
substitutable?
1. CLOPINE 100
2. CLOZARIL 100
Clozapine alternatives are available if you are experiencing bothersome side effects or if the
medication is not adequately controlling your symptoms. These alternatives can include
therapy and medications (such as other atypical antipsychotics and typical antipsychotics).
The newer antipsychotic medications used as clozapine alternatives may have fewer serious
side effects than older, typical antipsychotics, although studies have shown conflicting
results.
c) What monitoring is required when a patient is on clozapine?
Optimal Use of Medicines 9
d) Follow the clinical criteria to dispense the medicines
Guidelines
The dispensing process
The pharmacist should ensure that the prescription is valid, that the medicine is clinically
appropriate for the patient, and that information is provided to ensure safe and appropriate
use of the medicine.
The process of dispensing includes:
Receive the prescription
To ensure if the prescription is from authorised authority
Get the supplementary information if any
Determining the prescriber's intentions as to the patient's medicine, including the
dosing instructions
d) Follow the clinical criteria to dispense the medicines
Guidelines
The dispensing process
The pharmacist should ensure that the prescription is valid, that the medicine is clinically
appropriate for the patient, and that information is provided to ensure safe and appropriate
use of the medicine.
The process of dispensing includes:
Receive the prescription
To ensure if the prescription is from authorised authority
Get the supplementary information if any
Determining the prescriber's intentions as to the patient's medicine, including the
dosing instructions
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Optimal Use of Medicines 10
Reviewing the medication history and other relevant patient information, to ensure
that the medicine is safe, all other relevant considerations of the patient's health,
history of medicines patient is on,
Entering the prescription details on the pharmacy computer and recording to the
requirements of the law
Generating a label for the dispensed medicine and a repeat authorisation where
required
Selection of product preferred by prescriber
Clearly labelling the container of the medicine with the directions for its use as
intended by the prescriber along with any other information that facilitates its proper,
safe and effective use
Carefully checking and re-checking medicines for accuracy and completeness
Counselling the patient, or the patient's agent, sufficiently to allow a proper
understanding of all the information required by the patient to use the medicine safely
and effectively and to motivate the patient to comply with that, and to allow for a final
check of the dispensed medicine.
Dispensing precaution – safety of prescriptions
A pharmacist must take reasonable steps during the dispensing process (detailed in Guideline
1 The dispensing process) to ensure that the dispensing of a medicine in accordance with a
prescription or order is consistent with the safety of the person named in that prescription or
order.
Guideline
In dispensing a prescription, a pharmacist has to follow an independent judgement to ensure
the medicine is safe and appropriate for the patient, as well as that it conforms to the
prescriber’s intentions. When in doubt, the patient or their agent should be consulted and if
necessary, the prescriber contacted.
Good practice involves seeking consent from patients before disclosing information, where
practicable. If the prescriber cannot be contacted, if there is a difference in opinion regarding
the safety of the prescription, professional judgement must be exercised by the pharmacist in
deciding appropriate action to take.
Reviewing the medication history and other relevant patient information, to ensure
that the medicine is safe, all other relevant considerations of the patient's health,
history of medicines patient is on,
Entering the prescription details on the pharmacy computer and recording to the
requirements of the law
Generating a label for the dispensed medicine and a repeat authorisation where
required
Selection of product preferred by prescriber
Clearly labelling the container of the medicine with the directions for its use as
intended by the prescriber along with any other information that facilitates its proper,
safe and effective use
Carefully checking and re-checking medicines for accuracy and completeness
Counselling the patient, or the patient's agent, sufficiently to allow a proper
understanding of all the information required by the patient to use the medicine safely
and effectively and to motivate the patient to comply with that, and to allow for a final
check of the dispensed medicine.
Dispensing precaution – safety of prescriptions
A pharmacist must take reasonable steps during the dispensing process (detailed in Guideline
1 The dispensing process) to ensure that the dispensing of a medicine in accordance with a
prescription or order is consistent with the safety of the person named in that prescription or
order.
Guideline
In dispensing a prescription, a pharmacist has to follow an independent judgement to ensure
the medicine is safe and appropriate for the patient, as well as that it conforms to the
prescriber’s intentions. When in doubt, the patient or their agent should be consulted and if
necessary, the prescriber contacted.
Good practice involves seeking consent from patients before disclosing information, where
practicable. If the prescriber cannot be contacted, if there is a difference in opinion regarding
the safety of the prescription, professional judgement must be exercised by the pharmacist in
deciding appropriate action to take.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Optimal Use of Medicines 11
If the pharmacist decides not to dispense the prescribed medicine, the patient must be
informed about the reasons for the decision and the alternative options available.
Appropriate documentation should be kept to support the action taken.
In conforming to the above principle, dose, frequency and route of administration, duration of
treatment, the presence or absence of other medicines, the patient’s illness, medication
history, allergies, and other relevant circumstances need to be taken into account. When this
information is collected by the pharmacist, relevant details should be recorded in the
dispensing record, and where possible in the patient’s health record, so that the safety of any
future medicines that are prescribed and/or dispensed for that patient can also be assured.
e) What lifestyle factors can influence the therapeutic levels of clozapine?
A change in smoking status can have an adverse effect on the patient’s clozapine blood
levels. Dose adjustment may be necessary as abrupt cessation of smoking may lead to
clozapine intoxication. Patients that smoke should be informed that if they decide to stop
smoking, they are encouraged to do so but must inform their nurse or doctor.
f) Ask him/her if he has constipation or disturbed bowel movements
g) The most common symptom of Myocarditis is
Shortness of breath during exertion
Fatigue
Heart palpitations
Chest pain or pressure
The legs may swell
Rarely, causes a Sudden loss of consciousness that may be due to abnormal heart
rhythms
Signs of infection, such as
Fever
Muscle aches
Sore throat
Headache
Diarrhoea
Painful joints Swollen joints, legs, or neck veins
If the pharmacist decides not to dispense the prescribed medicine, the patient must be
informed about the reasons for the decision and the alternative options available.
Appropriate documentation should be kept to support the action taken.
In conforming to the above principle, dose, frequency and route of administration, duration of
treatment, the presence or absence of other medicines, the patient’s illness, medication
history, allergies, and other relevant circumstances need to be taken into account. When this
information is collected by the pharmacist, relevant details should be recorded in the
dispensing record, and where possible in the patient’s health record, so that the safety of any
future medicines that are prescribed and/or dispensed for that patient can also be assured.
e) What lifestyle factors can influence the therapeutic levels of clozapine?
A change in smoking status can have an adverse effect on the patient’s clozapine blood
levels. Dose adjustment may be necessary as abrupt cessation of smoking may lead to
clozapine intoxication. Patients that smoke should be informed that if they decide to stop
smoking, they are encouraged to do so but must inform their nurse or doctor.
f) Ask him/her if he has constipation or disturbed bowel movements
g) The most common symptom of Myocarditis is
Shortness of breath during exertion
Fatigue
Heart palpitations
Chest pain or pressure
The legs may swell
Rarely, causes a Sudden loss of consciousness that may be due to abnormal heart
rhythms
Signs of infection, such as
Fever
Muscle aches
Sore throat
Headache
Diarrhoea
Painful joints Swollen joints, legs, or neck veins
Optimal Use of Medicines 12
h) List THREE other common side effects of clozapine, include what sign and
symptoms patient may present with
1. Myocarditis- presents with flu like symptoms
2. Constipation- decreased bowel movements
3. Hyper salivation- increased saliva secretion
4. Hypotension and hypertension- dizziness tremors
References-
Https://safetyandquality.gov.au/wp-content/uploads/2013/01/National-Adult-Clozapine-
Titration-Chart-User-Guide.pdf
Http://www.iodine.com/drug/clozaril/alternatives
Http://www.nps.org.au/publications/health-professional/health-news-evidence/2015/new-
S100-supply-arrangements#_Toc423951422
Http://schizophrenia.emedtv.com/clozapine/clozapine-alternatives.html
Http://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/
clinical+resources/clinical+topics/medicines+and+drugs/clozapine
h) List THREE other common side effects of clozapine, include what sign and
symptoms patient may present with
1. Myocarditis- presents with flu like symptoms
2. Constipation- decreased bowel movements
3. Hyper salivation- increased saliva secretion
4. Hypotension and hypertension- dizziness tremors
References-
Https://safetyandquality.gov.au/wp-content/uploads/2013/01/National-Adult-Clozapine-
Titration-Chart-User-Guide.pdf
Http://www.iodine.com/drug/clozaril/alternatives
Http://www.nps.org.au/publications/health-professional/health-news-evidence/2015/new-
S100-supply-arrangements#_Toc423951422
Http://schizophrenia.emedtv.com/clozapine/clozapine-alternatives.html
Http://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/
clinical+resources/clinical+topics/medicines+and+drugs/clozapine
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 30
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.