MSc Paediatrics: Impact of Scientific Advances on Pediatric Cancer
VerifiedAdded on 2022/08/29
|17
|4273
|14
Essay
AI Summary
This essay explores the multifaceted aspects of pediatric cancer, encompassing its epidemiology, understanding, and evolving treatment methodologies. It begins by defining cancer and highlighting its prevalence in children, emphasizing the significance of early symptom recognition. The essay delves into the common types of childhood cancers, including leukemia, neuroblastoma, Wilms' tumor, and brain cancers, providing insights into their characteristics and prevalence. It then examines the advancements in pediatric cancer treatment, such as surgery, chemotherapy, radiation, immunotherapy, and stem cell transplants, while also touching upon the historical context and the shift in perspectives over time. A significant portion of the essay is dedicated to the impact of scientific advancements, including risk-modified therapeutic approaches, multi-center clinical trials, and the development of targeted novel agents. The essay also discusses the emergence of immunotherapy, including CAR-T cell therapy, and the role of genetic alterations in guiding cancer therapy, precision treatments, and hereditary DNA alterations. Finally, the essay highlights milestone trials and the FDA's approval of innovative treatments, such as tisagenlecleucel, and concludes by emphasizing the ongoing research efforts aimed at improving the long-term outcomes and reducing the toxicities associated with pediatric cancer treatment.

Running Head: PC 0
paediatric cANCER
[Document subtitle]
[DATE]
[Company name]
[Company address]
paediatric cANCER
[Document subtitle]
[DATE]
[Company name]
[Company address]
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
PC 1
Table of Contents
Introduction...........................................................................................................................................2
Epidemiology of pediatric cancer......................................................................................................2
Pediatric cancer understanding and treatment....................................................................................3
Impact of scientific advances.............................................................................................................4
Conclusion.............................................................................................................................................9
References...........................................................................................................................................10
Table of Contents
Introduction...........................................................................................................................................2
Epidemiology of pediatric cancer......................................................................................................2
Pediatric cancer understanding and treatment....................................................................................3
Impact of scientific advances.............................................................................................................4
Conclusion.............................................................................................................................................9
References...........................................................................................................................................10

PC 2
Introduction
Cancer is a huge group of ailments that can occur in nearly any organ or body tissue when the
abnormal cells grow wildly, go outside their usual limits to attack connecting parts of the
human body and/or transmit to other different organs. Paediatric cancers are the types of
malignancies that happen in children (Thorp, 2019). Paediatric cancer is recognized as the
second cause of decease in children. Parents need to be conscious of the sign & symptoms of
pediatric cancer: though the paediatrician is possibly a doctor, he/she might have never
diagnosed pediatric cancer. The chief types of childhood cancers come upon are leukemia,
neuroblastomas, different Wilms' tumors, brain type of cancers, rhabdomyosarcomas, the the
lymphomas, retinoblastomas, osteosarcomas and the Ewing's sarcomas (An et al., 2017). The
initial symptoms of pediatric cancer are frequently similar to those that are usually seen in
other different illnesses. These symptoms might include fever, tiredness, or enflamed glands.
Others, for example, bruising or the tender joints or all bones might lead a parent to uncertain
an injury. When these specific signs and symptoms last or are serious, the clinician might
order tests to examine for malignancy or other diseases. the understanding of pediatric
malignancy treatment has enhanced in the past few years (Walker, 2018). This particular
report will discuss how recent scientific advancement has improved the understanding and
the treatment of cancer.
Epidemiology of pediatric cancer
Leukemia is a malignancy of the bone marrow, which is the spongy midpoint of the body
bones that takes part in producing blood cells. Around 35 % of all cancer affected kids are
diagnosed with this pediatric cancer.
Introduction
Cancer is a huge group of ailments that can occur in nearly any organ or body tissue when the
abnormal cells grow wildly, go outside their usual limits to attack connecting parts of the
human body and/or transmit to other different organs. Paediatric cancers are the types of
malignancies that happen in children (Thorp, 2019). Paediatric cancer is recognized as the
second cause of decease in children. Parents need to be conscious of the sign & symptoms of
pediatric cancer: though the paediatrician is possibly a doctor, he/she might have never
diagnosed pediatric cancer. The chief types of childhood cancers come upon are leukemia,
neuroblastomas, different Wilms' tumors, brain type of cancers, rhabdomyosarcomas, the the
lymphomas, retinoblastomas, osteosarcomas and the Ewing's sarcomas (An et al., 2017). The
initial symptoms of pediatric cancer are frequently similar to those that are usually seen in
other different illnesses. These symptoms might include fever, tiredness, or enflamed glands.
Others, for example, bruising or the tender joints or all bones might lead a parent to uncertain
an injury. When these specific signs and symptoms last or are serious, the clinician might
order tests to examine for malignancy or other diseases. the understanding of pediatric
malignancy treatment has enhanced in the past few years (Walker, 2018). This particular
report will discuss how recent scientific advancement has improved the understanding and
the treatment of cancer.
Epidemiology of pediatric cancer
Leukemia is a malignancy of the bone marrow, which is the spongy midpoint of the body
bones that takes part in producing blood cells. Around 35 % of all cancer affected kids are
diagnosed with this pediatric cancer.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
PC 3
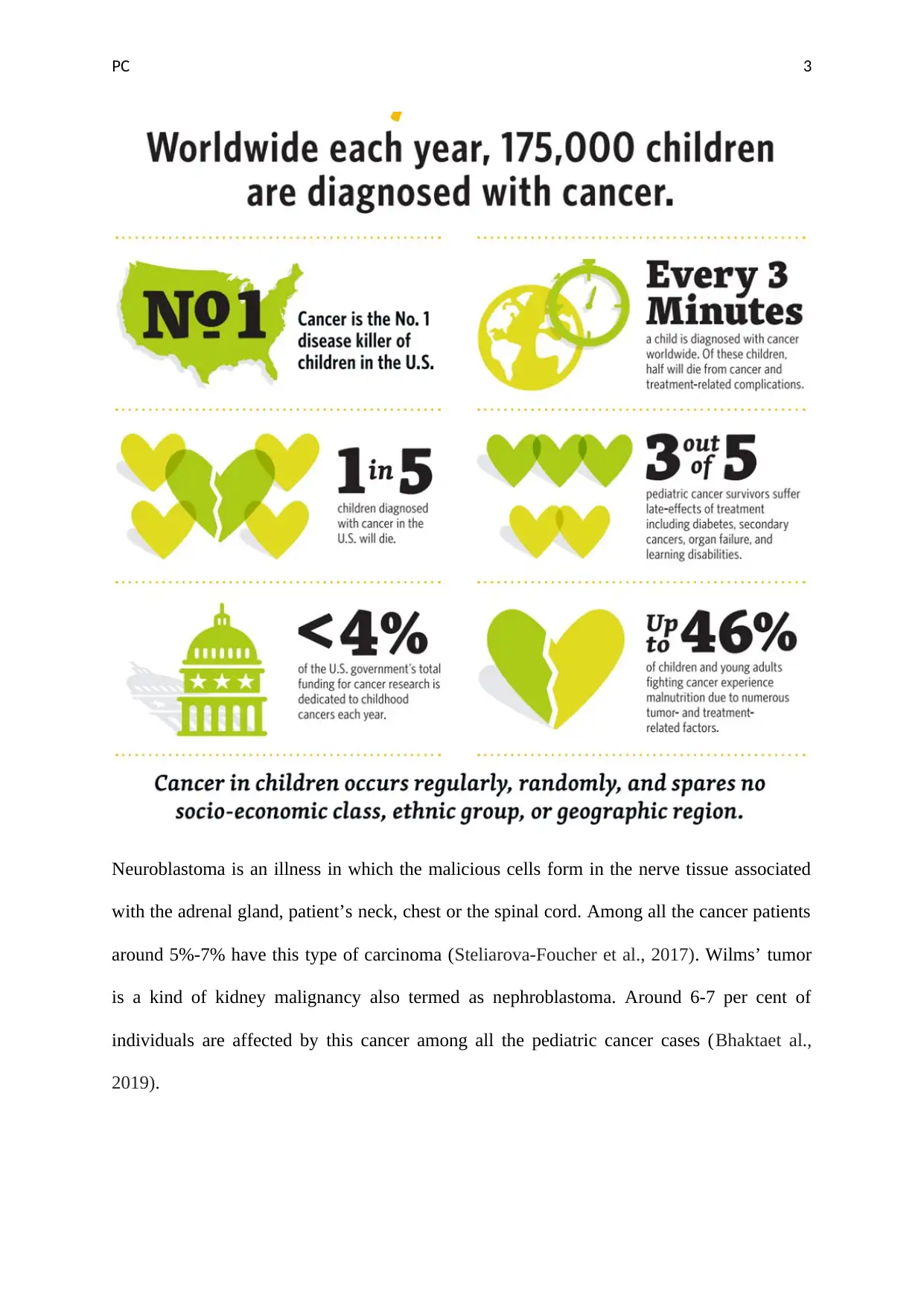
Neuroblastoma is an illness in which the malicious cells form in the nerve tissue associated
with the adrenal gland, patient’s neck, chest or the spinal cord. Among all the cancer patients
around 5%-7% have this type of carcinoma (Steliarova-Foucher et al., 2017). Wilms’ tumor
is a kind of kidney malignancy also termed as nephroblastoma. Around 6-7 per cent of
individuals are affected by this cancer among all the pediatric cancer cases (Bhaktaet al.,
2019).
Neuroblastoma is an illness in which the malicious cells form in the nerve tissue associated
with the adrenal gland, patient’s neck, chest or the spinal cord. Among all the cancer patients
around 5%-7% have this type of carcinoma (Steliarova-Foucher et al., 2017). Wilms’ tumor
is a kind of kidney malignancy also termed as nephroblastoma. Around 6-7 per cent of
individuals are affected by this cancer among all the pediatric cancer cases (Bhaktaet al.,
2019).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
PC 4
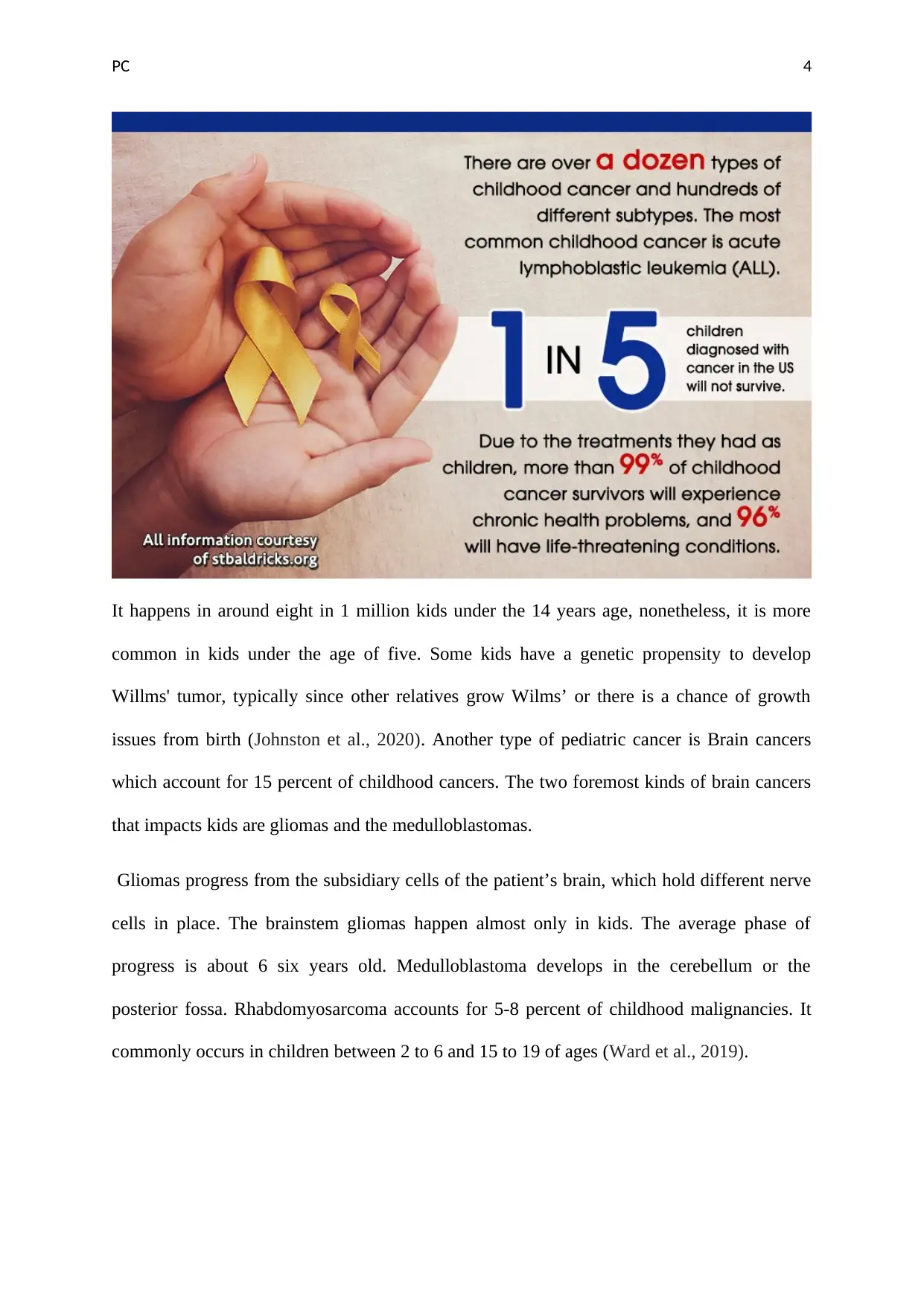
It happens in around eight in 1 million kids under the 14 years age, nonetheless, it is more
common in kids under the age of five. Some kids have a genetic propensity to develop
Willms' tumor, typically since other relatives grow Wilms’ or there is a chance of growth
issues from birth (Johnston et al., 2020). Another type of pediatric cancer is Brain cancers
which account for 15 percent of childhood cancers. The two foremost kinds of brain cancers
that impacts kids are gliomas and the medulloblastomas.
Gliomas progress from the subsidiary cells of the patient’s brain, which hold different nerve
cells in place. The brainstem gliomas happen almost only in kids. The average phase of
progress is about 6 six years old. Medulloblastoma develops in the cerebellum or the
posterior fossa. Rhabdomyosarcoma accounts for 5-8 percent of childhood malignancies. It
commonly occurs in children between 2 to 6 and 15 to 19 of ages (Ward et al., 2019).
It happens in around eight in 1 million kids under the 14 years age, nonetheless, it is more
common in kids under the age of five. Some kids have a genetic propensity to develop
Willms' tumor, typically since other relatives grow Wilms’ or there is a chance of growth
issues from birth (Johnston et al., 2020). Another type of pediatric cancer is Brain cancers
which account for 15 percent of childhood cancers. The two foremost kinds of brain cancers
that impacts kids are gliomas and the medulloblastomas.
Gliomas progress from the subsidiary cells of the patient’s brain, which hold different nerve
cells in place. The brainstem gliomas happen almost only in kids. The average phase of
progress is about 6 six years old. Medulloblastoma develops in the cerebellum or the
posterior fossa. Rhabdomyosarcoma accounts for 5-8 percent of childhood malignancies. It
commonly occurs in children between 2 to 6 and 15 to 19 of ages (Ward et al., 2019).
PC 5
Pediatric cancer understanding and treatment
The kinds of treatment that a kid with cancer obtains will be contingent on the kind of
malignancy and how progressive it is. Common treatments comprise operation,
chemotherapy, radiation treatment, immunotherapy, and stem cell transplant. The history of
pediatric cancer is very profound, the treatment of this disorder was rare and most of the
children were died due to the lack of treatment and the negative perspective of people about
childhood cancer. some of the individuals believed that all type of cancer is life-threatening
and leads to death. After the diagnosis, they prefer to avoid searching for treatment options
for their child. But in the past few decades, the understating of individuals and effective
approaches to treating cancer has emerged. This is because of the scientific advancement in
the field of childhood cancer that helped in the development of different types of treatments.
It has been reported that wit the help of effective treatment some of pediatric cancer can be
managed or increase the life expectance of the patient.
Impact of scientific advances
It has been reported that 4 out of five children identified with malignancy can be cured with
current cancer therapy. This signifies a dramatic enhancement in the previous 50 years ago
when the treatment rate of pediatric cancer was <25 per cent in the pre-chemotherapy period
(Hudson et al., 2012). Over the previous ten years, while development in complete survival
(OS) has been bordering, progress in pediatric oncology mendacities with accepting risk-
modified therapeutic method. This has been made probable through classifying clinical and
the biologic prognostic aspects with hard research and stratifying diseased individuals using
these risk aspects, and afterward adapting therapy rendering to risk group project. One of the
encounters of pediatric malignancy research is the minor disease populace, compared with
cancer among grown-up that is forty times more common. To stunned this problem, multi-
center scientific trials were important to produce statistically expressive results. For instance,
Pediatric cancer understanding and treatment
The kinds of treatment that a kid with cancer obtains will be contingent on the kind of
malignancy and how progressive it is. Common treatments comprise operation,
chemotherapy, radiation treatment, immunotherapy, and stem cell transplant. The history of
pediatric cancer is very profound, the treatment of this disorder was rare and most of the
children were died due to the lack of treatment and the negative perspective of people about
childhood cancer. some of the individuals believed that all type of cancer is life-threatening
and leads to death. After the diagnosis, they prefer to avoid searching for treatment options
for their child. But in the past few decades, the understating of individuals and effective
approaches to treating cancer has emerged. This is because of the scientific advancement in
the field of childhood cancer that helped in the development of different types of treatments.
It has been reported that wit the help of effective treatment some of pediatric cancer can be
managed or increase the life expectance of the patient.
Impact of scientific advances
It has been reported that 4 out of five children identified with malignancy can be cured with
current cancer therapy. This signifies a dramatic enhancement in the previous 50 years ago
when the treatment rate of pediatric cancer was <25 per cent in the pre-chemotherapy period
(Hudson et al., 2012). Over the previous ten years, while development in complete survival
(OS) has been bordering, progress in pediatric oncology mendacities with accepting risk-
modified therapeutic method. This has been made probable through classifying clinical and
the biologic prognostic aspects with hard research and stratifying diseased individuals using
these risk aspects, and afterward adapting therapy rendering to risk group project. One of the
encounters of pediatric malignancy research is the minor disease populace, compared with
cancer among grown-up that is forty times more common. To stunned this problem, multi-
center scientific trials were important to produce statistically expressive results. For instance,
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
PC 6
the Children Oncology Group (COG) characterizes the world’s main group keen exclusively
to pediatric cancer investigation (Pritchard-Jones et al., 2013). The conclusion for children
with malignancy has enhanced meaningfully over the past sixty years, with higher than 80
per cent of patients nowadays becoming five-year survivors. Notwithstanding this progress,
malignancy remains the foremost cause of demise from illness in the United States, and
important temporary and long-standing treatment toxicities endure to impact most of the
children with malignancy. The progress of targeted novel agents proposes the outlook of
possibly more effective and less toxic therapy for children. Over a period since imatinib
mesylate was offered into the handling of kids with Philadelphia chromosome, the positive
acute type of lymphoblastic leukemia, converting its outcome, a variety of beleaguered agents
has endured study in pediatric malignancy patients. Early instructions educated from these
includes include a healthier understanding of the opposing event outline of these medications
in kids, the challenge of emerging pediatric- precise preparations, and the sustained reliance
on effective development for grown-up cancer signs on drug development for children
(Saletta, Seng and Lau, 2014).
The practices to treat pediatric cancers started with individual investigators at individual
organizations. Early researchers were Sidney Farber at the Children’s Hospital of Boston and
Joseph H. Burchenal at the Memorial Hospital of Sloan-Kettering Institute, who both
calculated leukemia in the 1940s. As the utmost common kind of pediatric malignancy,
leukemia certainly turns out to be a focus of initial childhood cancer investigation (Kazak et
al., 2015). At that time, kids diagnosed with the leukemia issues expired within weeks of
identification. In the year of 1947, the first partial decrease of pediatric leukemia in a four-
year-old girl applying the medication aminopterin (an analog of the methotrexate). the
supportive model was frequent with other childhood malignancies in the United States. In the
year of 1970, a task force for rhabdomyosarcoma was shaped with representatives from the
the Children Oncology Group (COG) characterizes the world’s main group keen exclusively
to pediatric cancer investigation (Pritchard-Jones et al., 2013). The conclusion for children
with malignancy has enhanced meaningfully over the past sixty years, with higher than 80
per cent of patients nowadays becoming five-year survivors. Notwithstanding this progress,
malignancy remains the foremost cause of demise from illness in the United States, and
important temporary and long-standing treatment toxicities endure to impact most of the
children with malignancy. The progress of targeted novel agents proposes the outlook of
possibly more effective and less toxic therapy for children. Over a period since imatinib
mesylate was offered into the handling of kids with Philadelphia chromosome, the positive
acute type of lymphoblastic leukemia, converting its outcome, a variety of beleaguered agents
has endured study in pediatric malignancy patients. Early instructions educated from these
includes include a healthier understanding of the opposing event outline of these medications
in kids, the challenge of emerging pediatric- precise preparations, and the sustained reliance
on effective development for grown-up cancer signs on drug development for children
(Saletta, Seng and Lau, 2014).
The practices to treat pediatric cancers started with individual investigators at individual
organizations. Early researchers were Sidney Farber at the Children’s Hospital of Boston and
Joseph H. Burchenal at the Memorial Hospital of Sloan-Kettering Institute, who both
calculated leukemia in the 1940s. As the utmost common kind of pediatric malignancy,
leukemia certainly turns out to be a focus of initial childhood cancer investigation (Kazak et
al., 2015). At that time, kids diagnosed with the leukemia issues expired within weeks of
identification. In the year of 1947, the first partial decrease of pediatric leukemia in a four-
year-old girl applying the medication aminopterin (an analog of the methotrexate). the
supportive model was frequent with other childhood malignancies in the United States. In the
year of 1970, a task force for rhabdomyosarcoma was shaped with representatives from the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
PC 7
CCG, Malignancy and Leukemia Group B, and the Southwest Oncology Group wit the
suggestion of NCI (Wasilewski-Masker et al., 2014).
It has been recognised that malignant cells advance the capability to avoid, or hide from, the
person’s resistant system. The supports of malignancy therapy for eras have been operation,
radiation, and chemotherapy. These methods attack the malignancy directly nonetheless are
not positively targeted and destroy healthy along with malicious cells. The potential of cancer
immunotherapy depicts in the element that the treatment uses the immune system of each
patient, is targeted to malignant cells that show the aberrant type of proteins, and may have
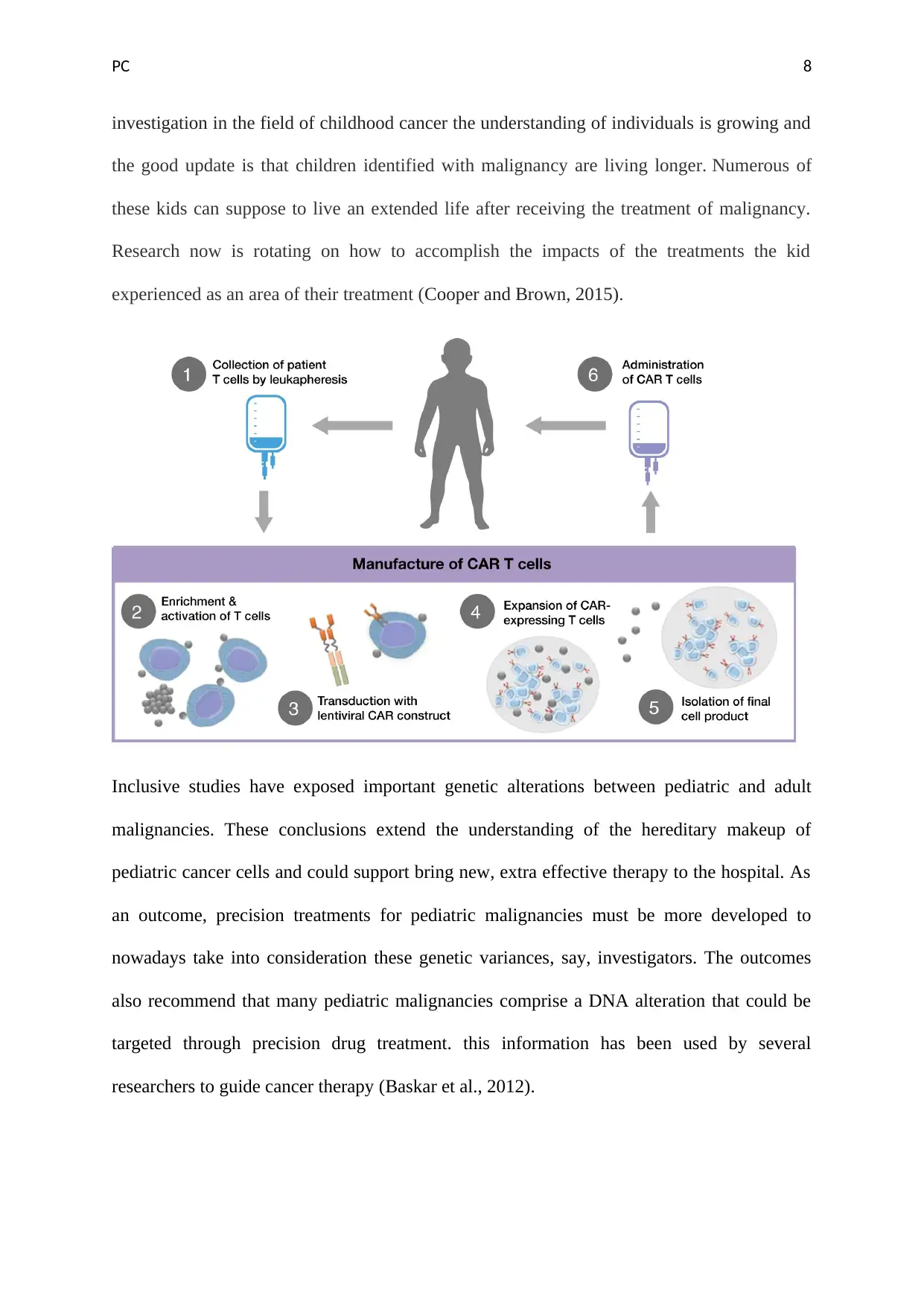
continuing effects (Hudson, Link, and Simone, 2014). Numerous approaches comprise the
dendritic cell treatment (eg, malignancy vaccines), antibody usage (in specific monoclonal
antibodies to definite proteins on malignant cells e.g., blockade of checkpoint), and planned T
cells, a procedure in which specific T cells are hereditarily modified to show the chimeric
type of antigen receptors or planned T-cell type of receptors. Though what works in grown-
up malignancies might not work for kids, and although drug producing corporations
frequently emphasis more on adults, immunotherapy is display promise in childhood
malignancy. For instance, the chimeric type of antigen receptor T-cell treatment offers
confidence for worsened or refractory severe lymphoblastic leukemia (Pui et al., 2011).
Significant advances have comprised the first effective transplants using the bone marrow
from the unconnected donor; the overview of T cell reduction as a method to stop graft
against host illness, which is the furthermost frequent severe problem following replacement;
the overview of hyper fractionated entire body irradiation, a technique of transporting
radiation treatment earlier to a resettle to upsurge the antileukemia and the antitumor
properties of radiotherapy while lessening the temporary and long-standing side impacts of
radiation; and the usage of resistant cells resulting from blood to cure viral contaminations or
relapse of illness afterward a transplant (Gupta et al., 2014). Afterward, the decades of
CCG, Malignancy and Leukemia Group B, and the Southwest Oncology Group wit the
suggestion of NCI (Wasilewski-Masker et al., 2014).
It has been recognised that malignant cells advance the capability to avoid, or hide from, the
person’s resistant system. The supports of malignancy therapy for eras have been operation,
radiation, and chemotherapy. These methods attack the malignancy directly nonetheless are
not positively targeted and destroy healthy along with malicious cells. The potential of cancer
immunotherapy depicts in the element that the treatment uses the immune system of each
patient, is targeted to malignant cells that show the aberrant type of proteins, and may have
continuing effects (Hudson, Link, and Simone, 2014). Numerous approaches comprise the
dendritic cell treatment (eg, malignancy vaccines), antibody usage (in specific monoclonal
antibodies to definite proteins on malignant cells e.g., blockade of checkpoint), and planned T
cells, a procedure in which specific T cells are hereditarily modified to show the chimeric
type of antigen receptors or planned T-cell type of receptors. Though what works in grown-
up malignancies might not work for kids, and although drug producing corporations
frequently emphasis more on adults, immunotherapy is display promise in childhood
malignancy. For instance, the chimeric type of antigen receptor T-cell treatment offers
confidence for worsened or refractory severe lymphoblastic leukemia (Pui et al., 2011).
Significant advances have comprised the first effective transplants using the bone marrow
from the unconnected donor; the overview of T cell reduction as a method to stop graft
against host illness, which is the furthermost frequent severe problem following replacement;
the overview of hyper fractionated entire body irradiation, a technique of transporting
radiation treatment earlier to a resettle to upsurge the antileukemia and the antitumor
properties of radiotherapy while lessening the temporary and long-standing side impacts of
radiation; and the usage of resistant cells resulting from blood to cure viral contaminations or
relapse of illness afterward a transplant (Gupta et al., 2014). Afterward, the decades of
PC 8
investigation in the field of childhood cancer the understanding of individuals is growing and
the good update is that children identified with malignancy are living longer. Numerous of
these kids can suppose to live an extended life after receiving the treatment of malignancy.
Research now is rotating on how to accomplish the impacts of the treatments the kid
experienced as an area of their treatment (Cooper and Brown, 2015).
Inclusive studies have exposed important genetic alterations between pediatric and adult
malignancies. These conclusions extend the understanding of the hereditary makeup of
pediatric cancer cells and could support bring new, extra effective therapy to the hospital. As
an outcome, precision treatments for pediatric malignancies must be more developed to
nowadays take into consideration these genetic variances, say, investigators. The outcomes
also recommend that many pediatric malignancies comprise a DNA alteration that could be
targeted through precision drug treatment. this information has been used by several
researchers to guide cancer therapy (Baskar et al., 2012).
investigation in the field of childhood cancer the understanding of individuals is growing and
the good update is that children identified with malignancy are living longer. Numerous of
these kids can suppose to live an extended life after receiving the treatment of malignancy.
Research now is rotating on how to accomplish the impacts of the treatments the kid
experienced as an area of their treatment (Cooper and Brown, 2015).
Inclusive studies have exposed important genetic alterations between pediatric and adult
malignancies. These conclusions extend the understanding of the hereditary makeup of
pediatric cancer cells and could support bring new, extra effective therapy to the hospital. As
an outcome, precision treatments for pediatric malignancies must be more developed to
nowadays take into consideration these genetic variances, say, investigators. The outcomes
also recommend that many pediatric malignancies comprise a DNA alteration that could be
targeted through precision drug treatment. this information has been used by several
researchers to guide cancer therapy (Baskar et al., 2012).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
PC 9
Current research studies recommend that as a minimum 10 per cent of kids with malignancy
carry a hereditary DNA alteration causing a malignancy predisposition syndrome (Sweet-
Cordero and Biegel, 2019). Consequently, the American Association for Cancer Research
(AACR) printed its first commendations for broadcast and clinical care. Amongst the most
shared syndromes that source an augmented malignancy risk are the Li-Fraumeni syndrome,
the neurofibromatosis and Wilms tumor, GI malignancy predisposition, the leukemia
tendency, and others. In different cases, children might have a germline DNA screen to
search for a congenital predisposition alteration due to an indicative family history
(Rodriguez-Galindo et al., 2015). The commendations provide strategies on when to start
detailed screening measures intended at spotting tumors when they are minor and more
effortlessly treated. In 2018, A less poisonous treatment of the anti- malignancy drug
methotrexate leads to the best results ever stated for children and teenagers with T-cell acute
type of lymphoblastic leukemia. In a federally- sponsored trial, the treatment presented a 5-
year illness-free survival frequency of 91.5 per cent and a complete survival rate of 93.7 per
cent (Cantrell and Ruble 2011). In contrast, the historical general survival frequency for T-
ALL was around 81% grounded on previous medical trials in the pediatric population. In
2017, a milestone trial, the chimeric type of antigen receptor- adapted T cell (CAR-T)
treatment tisagenlecleucel (Kymriah) sources comprehensive remissions in a most of young
people with B-cell acute types lymphoblastic leukemia (ALL) that advanced despite
preceding treatment with typical therapies. Afterward, tisagenlecleucel turn out to be the first
gene treatment to be accepted by the FDA (Vaske and Haussler, 2019)
Targeted therapy for cancer is the usage of medications to classify and eliminate malignancy
cells using their hereditary properties, which is recognized as one of the utmost promising
therapy options for malignancy patients (Vogelzang et al., 2012). “The undertaking in
oncology in over-all, counting pediatrics, is to deliver more modified treatments, researchers
Current research studies recommend that as a minimum 10 per cent of kids with malignancy
carry a hereditary DNA alteration causing a malignancy predisposition syndrome (Sweet-
Cordero and Biegel, 2019). Consequently, the American Association for Cancer Research
(AACR) printed its first commendations for broadcast and clinical care. Amongst the most
shared syndromes that source an augmented malignancy risk are the Li-Fraumeni syndrome,
the neurofibromatosis and Wilms tumor, GI malignancy predisposition, the leukemia
tendency, and others. In different cases, children might have a germline DNA screen to
search for a congenital predisposition alteration due to an indicative family history
(Rodriguez-Galindo et al., 2015). The commendations provide strategies on when to start
detailed screening measures intended at spotting tumors when they are minor and more
effortlessly treated. In 2018, A less poisonous treatment of the anti- malignancy drug
methotrexate leads to the best results ever stated for children and teenagers with T-cell acute
type of lymphoblastic leukemia. In a federally- sponsored trial, the treatment presented a 5-
year illness-free survival frequency of 91.5 per cent and a complete survival rate of 93.7 per
cent (Cantrell and Ruble 2011). In contrast, the historical general survival frequency for T-
ALL was around 81% grounded on previous medical trials in the pediatric population. In
2017, a milestone trial, the chimeric type of antigen receptor- adapted T cell (CAR-T)
treatment tisagenlecleucel (Kymriah) sources comprehensive remissions in a most of young
people with B-cell acute types lymphoblastic leukemia (ALL) that advanced despite
preceding treatment with typical therapies. Afterward, tisagenlecleucel turn out to be the first
gene treatment to be accepted by the FDA (Vaske and Haussler, 2019)
Targeted therapy for cancer is the usage of medications to classify and eliminate malignancy
cells using their hereditary properties, which is recognized as one of the utmost promising
therapy options for malignancy patients (Vogelzang et al., 2012). “The undertaking in
oncology in over-all, counting pediatrics, is to deliver more modified treatments, researchers
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
PC 10
noted. Different other investigators reported that in the future, the researcher will move in the
direction of defining a malignancy through its molecular profile instead of the organ it
includes. Researchers can recognize targets in the body tissue on a molecular level, which is
method deeper, way more detailed than ever beforehand,” said investigators (Dizon et al.,
2016). However, the researcher has not identified the specific treatment for pediatric cancer
and are not reached it yet. But it can be seen that researchers will look to mixture treatment
with targeted treatments. The recent investigation advances support in the growth of different
theories that are presently used extensively throughout the world. Risk-directed treatments
are more regularly used. Patients are nowadays frequently stratified into “low” risk, indicates
that their illness responds healthier to existing therapies, and they need less concentrated
therapy than “high” risk, indicating they are at great risk for deterioration and need more
rigorous rehabilitations to give a healthier chance of treatment (Pishas and Lessnick, 2016).
The hereditary and biological standards for scheming treatments are repeatedly being better
distinct. New medications are obtainable that are targeted biologically and have a less adverse
reaction, and additionally, these are presently being industrialized. Though, people still
require to learn very much about how to apply them, counting what sicknesses they are
operative in, how to apply them with conservative chemotherapy treatment and with each
other, and duration. In 2010, A modeling investigation based on information from the long-
running pediatric cancer survivor investigation demonstrated that life expectancy for
childhood cancer survivors is around 10 years shorter, overall, than in the common
population (Alewine, Hassan, and Pastan, 2015). This consequence is because of a higher risk
of cardiovascular and lung difficulties and second malignancies later in a patient’s life. The
conclusions upsurge the urgency of longstanding health screenings for survivors of pediatric
cancer, who now more than 300,000 in the U.S. Today, due to advances in the investigation,
the survival frequency for pediatric cancer is just over 80 % in wealthy nations like Canada.
noted. Different other investigators reported that in the future, the researcher will move in the
direction of defining a malignancy through its molecular profile instead of the organ it
includes. Researchers can recognize targets in the body tissue on a molecular level, which is
method deeper, way more detailed than ever beforehand,” said investigators (Dizon et al.,
2016). However, the researcher has not identified the specific treatment for pediatric cancer
and are not reached it yet. But it can be seen that researchers will look to mixture treatment
with targeted treatments. The recent investigation advances support in the growth of different
theories that are presently used extensively throughout the world. Risk-directed treatments
are more regularly used. Patients are nowadays frequently stratified into “low” risk, indicates
that their illness responds healthier to existing therapies, and they need less concentrated
therapy than “high” risk, indicating they are at great risk for deterioration and need more
rigorous rehabilitations to give a healthier chance of treatment (Pishas and Lessnick, 2016).
The hereditary and biological standards for scheming treatments are repeatedly being better
distinct. New medications are obtainable that are targeted biologically and have a less adverse
reaction, and additionally, these are presently being industrialized. Though, people still
require to learn very much about how to apply them, counting what sicknesses they are
operative in, how to apply them with conservative chemotherapy treatment and with each
other, and duration. In 2010, A modeling investigation based on information from the long-
running pediatric cancer survivor investigation demonstrated that life expectancy for
childhood cancer survivors is around 10 years shorter, overall, than in the common
population (Alewine, Hassan, and Pastan, 2015). This consequence is because of a higher risk
of cardiovascular and lung difficulties and second malignancies later in a patient’s life. The
conclusions upsurge the urgency of longstanding health screenings for survivors of pediatric
cancer, who now more than 300,000 in the U.S. Today, due to advances in the investigation,
the survival frequency for pediatric cancer is just over 80 % in wealthy nations like Canada.
PC 11
Still about 90,000 of the 250,000 kids diagnosed with malignancy worldwide per annum
yield to the disease. These kids require investigators to keep functioning in the direction of a
cure (Dancsok, Asleh-Aburaya, and Nielsen, 2017).
Conclusion
Cancer is recognized as a group of illnesses that can affect any part of the body. Pediatric
cancer is a type of cancer that occurs among children. This particular type of cancer is not
restricted to a specific city or nation, it is affecting children from all around the globe. There
a renumber of studies conducted by researchers to emerge new treatment for this health issue.
the understanding of the diseases and treatment has been emerged by advanced research in
this area. pediatric cancer was thought to be as same as other types of cancer and most of the
individuals avoid receiving the treatment for this problem. It has been reported that among all
types of Cancer pediatric cancer accounts for 5 to 7 per cent. some of the subtypes of
Still about 90,000 of the 250,000 kids diagnosed with malignancy worldwide per annum
yield to the disease. These kids require investigators to keep functioning in the direction of a
cure (Dancsok, Asleh-Aburaya, and Nielsen, 2017).
Conclusion
Cancer is recognized as a group of illnesses that can affect any part of the body. Pediatric
cancer is a type of cancer that occurs among children. This particular type of cancer is not
restricted to a specific city or nation, it is affecting children from all around the globe. There
a renumber of studies conducted by researchers to emerge new treatment for this health issue.
the understanding of the diseases and treatment has been emerged by advanced research in
this area. pediatric cancer was thought to be as same as other types of cancer and most of the
individuals avoid receiving the treatment for this problem. It has been reported that among all
types of Cancer pediatric cancer accounts for 5 to 7 per cent. some of the subtypes of
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 17
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.