Patient Health History Assessment for Suspected Food Poisoning
VerifiedAdded on 2023/06/15
|11
|2863
|255
AI Summary
This patient health history assessment is for a 42-year-old female nurse who is seeking medical treatment for suspected food poisoning. The assessment covers the patient's identification, reasons for seeking care, history of illness, past health, family history, and review of health systems.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
RUNNING HEAD; PATIENT HEALTH STATUS
UNIVERSITY:
NAME :
STUDENT ID:
COURSE CODE
COURSE NAME
ASSIGNMENT
UNIVERSITY:
NAME :
STUDENT ID:
COURSE CODE
COURSE NAME
ASSIGNMENT
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
PATIENT HEALTH HISTORY ASSESSMENT 2
Patient identification
Patient C.W is aged 42 years female black American living in Los Angelis. She is a
practising nurse. She holds a licence in vocational nurse. She has a one child whom she is
caring. The patient states that she was born in Los Angelis, her parents birthplace is Los
Angelis. Her highest level of education is diploma in Nursing.
Reasons for seeking care
Patient C.W is seeking medical treatment for suspected food poisoning.
History of illness
A 42 years old Black American female came into the ER crying, holding on to her
stomach with a bowl in her hand which contained some light food particles from her vomit.
The patient complained of “severe abdominal pain, cramping, diarrhea, nausea, and vomiting,
mainly around the naval and trunk area of my body, occurring 24 hours at midnight between
12:30am and it’s getting worse.” According to the patient, “I was in good health as I was
socializing with my son all day. We both ate a little portion of Chipotle before going to bed.
Approximately at 12:30am, I started feeling some light dull pain around the trunk of my
body, then visited the restroom six times before daybreak.” According to patient, “The pain
radiated towards my belly button and other parts of my stomach. The abdominal pain got
worse suddenly. Patient stated” I took Tylenol 650mg oral, and I vomited it out, and the
patient stated that her symptoms are triggered by eating, drinking. The symptoms as
described by patient is “unable to sleep, severe weakness, can’t sleep, drink, or eat due to the
pain. Patient denied fever.”
Past health
Patient C.W has a history of gall bladder in 1999 operation and Caesarian assistance 33
years ago. The patient suggests that during the period of C-Section management she didn’t
receive any associative complications such as infections, blood loss, bowel problems organ
Patient identification
Patient C.W is aged 42 years female black American living in Los Angelis. She is a
practising nurse. She holds a licence in vocational nurse. She has a one child whom she is
caring. The patient states that she was born in Los Angelis, her parents birthplace is Los
Angelis. Her highest level of education is diploma in Nursing.
Reasons for seeking care
Patient C.W is seeking medical treatment for suspected food poisoning.
History of illness
A 42 years old Black American female came into the ER crying, holding on to her
stomach with a bowl in her hand which contained some light food particles from her vomit.
The patient complained of “severe abdominal pain, cramping, diarrhea, nausea, and vomiting,
mainly around the naval and trunk area of my body, occurring 24 hours at midnight between
12:30am and it’s getting worse.” According to the patient, “I was in good health as I was
socializing with my son all day. We both ate a little portion of Chipotle before going to bed.
Approximately at 12:30am, I started feeling some light dull pain around the trunk of my
body, then visited the restroom six times before daybreak.” According to patient, “The pain
radiated towards my belly button and other parts of my stomach. The abdominal pain got
worse suddenly. Patient stated” I took Tylenol 650mg oral, and I vomited it out, and the
patient stated that her symptoms are triggered by eating, drinking. The symptoms as
described by patient is “unable to sleep, severe weakness, can’t sleep, drink, or eat due to the
pain. Patient denied fever.”
Past health
Patient C.W has a history of gall bladder in 1999 operation and Caesarian assistance 33
years ago. The patient suggests that during the period of C-Section management she didn’t
receive any associative complications such as infections, blood loss, bowel problems organ
PATIENT HEALTH HISTORY ASSESSMENT 3
injury or blood clots, (Cunningham et al., 2010). During the childhood ages, C.W was
diagnosed with chicken pox, which she states was managed successfully. The patient states
that she has never had any injury as a result of an accident. C.W has only undergone
operation in medical condition stated above; gall bladder and C- section, (Cunningharm et al.,
2010). Her obstetric history condition as stated by her shows that she has 2 gravida children.
Further she has had no preterm birth and she underwent full term birth. She currently lives
with her one child.
She normally attends immunization engagement as stated by her records of
immunization indicates that she took DTaP Date 06/25/2014 Pneumonia on date, Influenza
on date 10/12/17, Hepatitis Type B on date e2/2/18, MMR on date 1/5/04, Rotavirus on
date 04/6/17, Hib on date 12/17/17, Varicella Date 1/5/04, IPV Date_2/2/18 and TB on date
12/8/17
The patient is undergoing medication which includes Clarithin, Apro and Ferrous
sulfate. The patients state that she is allergic to pollen and dust. The intake f Claritin, acts as
an anti histamine which acts by reducing the effects of the chemical histamine found in the
body which is linked to sneezing and running nose and watery mucous. Also the Ferrous
sulfate medication is meant for boost in red blood cell count in the body. Her diagnostic lab
tests shows that her CXR, Ekg among others are normal, Jarvis, 2016.
Patient C.W has an history of chronic sinuses which has been itchy since six years ago.
She was referred to a social worker and was placed on Claritin drugs and atropine to manage
the allergies. The patient denies having cervical cancer, heart disease and hypertension. She
denies of any history of smoking nor usage of alcohol. Further despite taking allergy
treatment the patient denies allergy on latex allergies or any form of food allergies.
injury or blood clots, (Cunningham et al., 2010). During the childhood ages, C.W was
diagnosed with chicken pox, which she states was managed successfully. The patient states
that she has never had any injury as a result of an accident. C.W has only undergone
operation in medical condition stated above; gall bladder and C- section, (Cunningharm et al.,
2010). Her obstetric history condition as stated by her shows that she has 2 gravida children.
Further she has had no preterm birth and she underwent full term birth. She currently lives
with her one child.
She normally attends immunization engagement as stated by her records of
immunization indicates that she took DTaP Date 06/25/2014 Pneumonia on date, Influenza
on date 10/12/17, Hepatitis Type B on date e2/2/18, MMR on date 1/5/04, Rotavirus on
date 04/6/17, Hib on date 12/17/17, Varicella Date 1/5/04, IPV Date_2/2/18 and TB on date
12/8/17
The patient is undergoing medication which includes Clarithin, Apro and Ferrous
sulfate. The patients state that she is allergic to pollen and dust. The intake f Claritin, acts as
an anti histamine which acts by reducing the effects of the chemical histamine found in the
body which is linked to sneezing and running nose and watery mucous. Also the Ferrous
sulfate medication is meant for boost in red blood cell count in the body. Her diagnostic lab
tests shows that her CXR, Ekg among others are normal, Jarvis, 2016.
Patient C.W has an history of chronic sinuses which has been itchy since six years ago.
She was referred to a social worker and was placed on Claritin drugs and atropine to manage
the allergies. The patient denies having cervical cancer, heart disease and hypertension. She
denies of any history of smoking nor usage of alcohol. Further despite taking allergy
treatment the patient denies allergy on latex allergies or any form of food allergies.
PATIENT HEALTH HISTORY ASSESSMENT 4
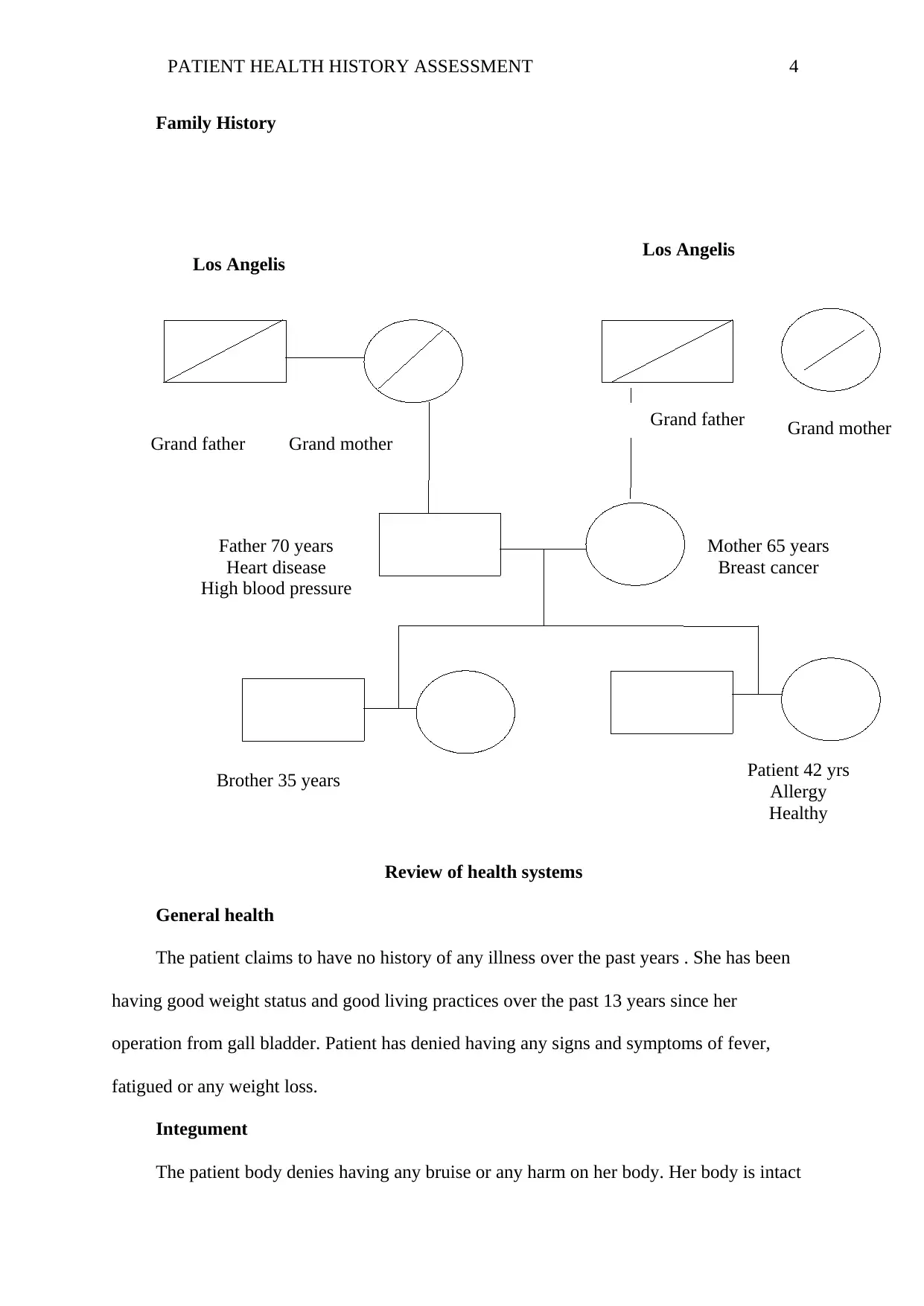
Family History
Review of health systems
General health
The patient claims to have no history of any illness over the past years . She has been
having good weight status and good living practices over the past 13 years since her
operation from gall bladder. Patient has denied having any signs and symptoms of fever,
fatigued or any weight loss.
Integument
The patient body denies having any bruise or any harm on her body. Her body is intact
Grand father Grand mother
Grand father Grand mother
Father 70 years
Heart disease
High blood pressure
Mother 65 years
Breast cancer
Patient 42 yrs
Allergy
Healthy
Brother 35 years
Los Angelis Los Angelis
Family History
Review of health systems
General health
The patient claims to have no history of any illness over the past years . She has been
having good weight status and good living practices over the past 13 years since her
operation from gall bladder. Patient has denied having any signs and symptoms of fever,
fatigued or any weight loss.
Integument
The patient body denies having any bruise or any harm on her body. Her body is intact
Grand father Grand mother
Grand father Grand mother
Father 70 years
Heart disease
High blood pressure
Mother 65 years
Breast cancer
Patient 42 yrs
Allergy
Healthy
Brother 35 years
Los Angelis Los Angelis
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
PATIENT HEALTH HISTORY ASSESSMENT 5
and from the observation, there are no signs of hair loss. She also denies any tattoos. From
observation she has brittle nails in good shape.
Head
C.W denies having any signs of headache or migraine health. Health promotion lan is
to encourage the patient to avoid exposures which precipitate headache
Neck
The patient denies any form of neck swellings of lesions, or any form of thyroid goiter
symptoms. Health promotion plan is to encourage the patient on good sitting and sleeping
postures and to ensure proper hair or seat arrangement.
Ears
The patient denies any form of ear infection which can include bloody discharge,
infection or excessive hair. Health promotion is to encourage her to keep healthy practices
such as avoiding loud music and limiting use of ear phones as they harm the ear drum.
Eyes
The patient denies any form of swelling and redness, cataracts and glaucoma. She states
she has no signs of blurred vision, decrease in visual aspects and bloody eyes. Health
promotion plan is to ensure that she always go for eyes health check in the eye clinic.
Nose and Sinuses
C.W denies any signs of fever and unexplained colds, obstructions, fever, allergies and
changes in the olfactory. Thus the aim of health promotion is to educate the patient of
hygiene and cleanliness of Ear Nose and throat. Further the patient denies or pharynx,
however plan is to educate the patient to offer on oral hygiene and visitation to the dentists,
(Jarvis, 2016).
Respiratory and Cardiovascular
Patient C.W denies any changes on her health with regard to respiratory and
and from the observation, there are no signs of hair loss. She also denies any tattoos. From
observation she has brittle nails in good shape.
Head
C.W denies having any signs of headache or migraine health. Health promotion lan is
to encourage the patient to avoid exposures which precipitate headache
Neck
The patient denies any form of neck swellings of lesions, or any form of thyroid goiter
symptoms. Health promotion plan is to encourage the patient on good sitting and sleeping
postures and to ensure proper hair or seat arrangement.
Ears
The patient denies any form of ear infection which can include bloody discharge,
infection or excessive hair. Health promotion is to encourage her to keep healthy practices
such as avoiding loud music and limiting use of ear phones as they harm the ear drum.
Eyes
The patient denies any form of swelling and redness, cataracts and glaucoma. She states
she has no signs of blurred vision, decrease in visual aspects and bloody eyes. Health
promotion plan is to ensure that she always go for eyes health check in the eye clinic.
Nose and Sinuses
C.W denies any signs of fever and unexplained colds, obstructions, fever, allergies and
changes in the olfactory. Thus the aim of health promotion is to educate the patient of
hygiene and cleanliness of Ear Nose and throat. Further the patient denies or pharynx,
however plan is to educate the patient to offer on oral hygiene and visitation to the dentists,
(Jarvis, 2016).
Respiratory and Cardiovascular
Patient C.W denies any changes on her health with regard to respiratory and
PATIENT HEALTH HISTORY ASSESSMENT 6
cardiovascular health. She denies having any signs of bronchitis, asthma or tuberculosis,
sleep disorder pollution exposure of cough. Plan for health promotion is to educate her to
avoid exposure to harmful environmental substances which can affect her respiratory health.
Further the patient denies having any signs and symptoms of chest pain, congestive heart
failure, stenosis or any heart related pain. However moving forward is to encourage her to
always visit health care facility for screening and tests .
Peripheral vascular and breast tests
C.W denies having any signs of thrombo phlebitis and swelling of the lower
extremities. She says she has no heard any signs of swelling, numbness or ulcers., she also
denies any signs of breasts cancer or any suspicious discharge or rash on her breast. She
asserts that she usually performs self tests breast exam. Health promotion goal is to
encourage to undergoes breast screening and maintaining good practices for the management
of peripheral vascular disease such as avoiding standing for long and crossing of legs while
sitting.
Gastrointestinal & Genitourinary health
C.W denies having any history of gastrointestinal and genitourinary symptoms. She
claims that she has had no urinary tract infections such as hematoruria, dysuria, cloudy urine
or other forms of kidney infections. Health promotion plan is to encourage increasing water
consumption of drinking at least 8 glasses daily. Also she needs to be undergoing regular
assessments and tests Jarvis, 2016.
Reproductive history
C.W states she began her menstruation at the age of 12 years old. She further says that
her LNMP is 1/11/2017. She has regular menstrual cycle of 28 days and usually lats for 5
days. Her menstrual discharge is usually heavy. Her last date of menstrual cycle was on
15/11/2017. The patient denies signs of menopause and she currently uses no contraception.
cardiovascular health. She denies having any signs of bronchitis, asthma or tuberculosis,
sleep disorder pollution exposure of cough. Plan for health promotion is to educate her to
avoid exposure to harmful environmental substances which can affect her respiratory health.
Further the patient denies having any signs and symptoms of chest pain, congestive heart
failure, stenosis or any heart related pain. However moving forward is to encourage her to
always visit health care facility for screening and tests .
Peripheral vascular and breast tests
C.W denies having any signs of thrombo phlebitis and swelling of the lower
extremities. She says she has no heard any signs of swelling, numbness or ulcers., she also
denies any signs of breasts cancer or any suspicious discharge or rash on her breast. She
asserts that she usually performs self tests breast exam. Health promotion goal is to
encourage to undergoes breast screening and maintaining good practices for the management
of peripheral vascular disease such as avoiding standing for long and crossing of legs while
sitting.
Gastrointestinal & Genitourinary health
C.W denies having any history of gastrointestinal and genitourinary symptoms. She
claims that she has had no urinary tract infections such as hematoruria, dysuria, cloudy urine
or other forms of kidney infections. Health promotion plan is to encourage increasing water
consumption of drinking at least 8 glasses daily. Also she needs to be undergoing regular
assessments and tests Jarvis, 2016.
Reproductive history
C.W states she began her menstruation at the age of 12 years old. She further says that
her LNMP is 1/11/2017. She has regular menstrual cycle of 28 days and usually lats for 5
days. Her menstrual discharge is usually heavy. Her last date of menstrual cycle was on
15/11/2017. The patient denies signs of menopause and she currently uses no contraception.
PATIENT HEALTH HISTORY ASSESSMENT 7
She denies having any premenstrual pain and itching often accompanying menstrual cycle.
Health promotion plan s to encourage the patient on regular annual pap test for any
signs of cancerative cells. This will be key in ensuring that she is advices regularly on healthy
reproductive status.
Musculoskeletal, Neurological and Endocrine health state
The patient denies any signs and symptoms of joints stiffness, fractures, deformities or
any pain. She claims she doesn’t have any signs of knee pain, or spinal cord problems. She
also denies an y history of seizures, paralysis or any form of numbness, memory loss or any
form of nervousneous. Her endocrine health shows negative results the patient, denies any
signs of appetite or polyruia, diabetes and hormone replacement therapy. Health promotion
plan is to educate the patient on regular physical exercises, and having healthy balanced diet
with heavy and regular intake of water daily. Further for good endocrine and hormonal
balance health, is to encourage the patient for normal balance of fruits and vegetables to keep
her body healthy and free from disease.
Psychosocial health
The patient further denies any form of harmful destruction on herself or others. She has
not had any thoughts of depression and suicidal attempts. She claims that se is in peace with
her friends and family who offer family support.
Health promotion plan is encourage her to always be open to friends when feeling of
depression sets in. as this decreases the level of stress and depression.
Hematologic health
C.W denies any form of swelling of lymph nodes and blood transfusions. She has no
history of bleeding and mucous membranes, health promotion for the patient is educate on
health skin check and always seek medical help when there are signs of bruising.
Functional assessment
She denies having any premenstrual pain and itching often accompanying menstrual cycle.
Health promotion plan s to encourage the patient on regular annual pap test for any
signs of cancerative cells. This will be key in ensuring that she is advices regularly on healthy
reproductive status.
Musculoskeletal, Neurological and Endocrine health state
The patient denies any signs and symptoms of joints stiffness, fractures, deformities or
any pain. She claims she doesn’t have any signs of knee pain, or spinal cord problems. She
also denies an y history of seizures, paralysis or any form of numbness, memory loss or any
form of nervousneous. Her endocrine health shows negative results the patient, denies any
signs of appetite or polyruia, diabetes and hormone replacement therapy. Health promotion
plan is to educate the patient on regular physical exercises, and having healthy balanced diet
with heavy and regular intake of water daily. Further for good endocrine and hormonal
balance health, is to encourage the patient for normal balance of fruits and vegetables to keep
her body healthy and free from disease.
Psychosocial health
The patient further denies any form of harmful destruction on herself or others. She has
not had any thoughts of depression and suicidal attempts. She claims that se is in peace with
her friends and family who offer family support.
Health promotion plan is encourage her to always be open to friends when feeling of
depression sets in. as this decreases the level of stress and depression.
Hematologic health
C.W denies any form of swelling of lymph nodes and blood transfusions. She has no
history of bleeding and mucous membranes, health promotion for the patient is educate on
health skin check and always seek medical help when there are signs of bruising.
Functional assessment
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
PATIENT HEALTH HISTORY ASSESSMENT 8
The functional status of the patient shows that she has good self esteem and self
concept. She has attained a diploma level education ad she completed successfully she happy
with hers scores of getting AA degree. She has a wonderful career as a vocational nurse. She
aims at getting a bachelor degree in nursing.
Her financial state is that she has adequate income. Her source of income is in medical
insurance. The patient states that she ascribes to Christian values and beliefs. This are
essential in maintain a positive lifestyle. She has positive self care behaviors which she thinks
keeps her on the right track of medical care.
Activity /Exercise Daily profile
C.W states that she always have a normal busy day with work and during home chores.
She don’t perform any physical exercise and her normal life is characterized by busy life and
performance of her normal duties.
Independent or Needs with ADLs
The patient states that she normally takes care of all her activities of daily life and she
helps her children prepare for school and performances of the normal daily chores.
Leisure activities
C.W states that she has limited time for leisure activities. She likes watching at her free
time and taking nature walks. However with her busy schedule she claims that doesn’t have
enough time for the leisure activities.
Nutrition
C.W states that she rarely prepares her food at home when not at work and often
dislikes preparing food in the house. A 24 hr recall on her nutritional management indicates
that she consumes high among snack foods food from outside outlets.
Prior to the medication protocol, she states that she normally buys food from outside
and she prepares food just in the evening and most of times she buys food from outside and
The functional status of the patient shows that she has good self esteem and self
concept. She has attained a diploma level education ad she completed successfully she happy
with hers scores of getting AA degree. She has a wonderful career as a vocational nurse. She
aims at getting a bachelor degree in nursing.
Her financial state is that she has adequate income. Her source of income is in medical
insurance. The patient states that she ascribes to Christian values and beliefs. This are
essential in maintain a positive lifestyle. She has positive self care behaviors which she thinks
keeps her on the right track of medical care.
Activity /Exercise Daily profile
C.W states that she always have a normal busy day with work and during home chores.
She don’t perform any physical exercise and her normal life is characterized by busy life and
performance of her normal duties.
Independent or Needs with ADLs
The patient states that she normally takes care of all her activities of daily life and she
helps her children prepare for school and performances of the normal daily chores.
Leisure activities
C.W states that she has limited time for leisure activities. She likes watching at her free
time and taking nature walks. However with her busy schedule she claims that doesn’t have
enough time for the leisure activities.
Nutrition
C.W states that she rarely prepares her food at home when not at work and often
dislikes preparing food in the house. A 24 hr recall on her nutritional management indicates
that she consumes high among snack foods food from outside outlets.
Prior to the medication protocol, she states that she normally buys food from outside
and she prepares food just in the evening and most of times she buys food from outside and
PATIENT HEALTH HISTORY ASSESSMENT 9
brings them to house for minimal preparation. Her weight status indicates she is lightly
overweight with BMI index of 25.1. This is due to high snacking and regular consumption of
meals.
Interpersonal relationships
C.W states that she normally has normal cordial relationships with her children. She
states that she often is in good cordial relation with her family and she is a member of church
choir. She sometimes spends time with church members and her peers at work place during
weekends when not at work. She has not had any stressful event in her life of late. She
maintains good relation with friends.
Coping and stress management
C.W states that she has been usual calm life, except when there is small family stress of
children. She states that at times more finances are needed for upkeep of her children.
However she states that she has leant on how to keep up with stress. She says when feeling
stressed up always goes to church to join choir practices. She has observed that this way she
can keep stress away.
Personal habits
C.W states that she normally takes coffee and chocolate in order to make her alert and
always not dull. She denies having smoke cigarette or even smokes. Further she also denies
having any alcohol use over the last 10 years. As mother she does not indulge in drug abuse
or any form of drug abuse. With history of her family she doesn’t have any kind of history of
drug abuse in the family. There is no form of depression and disruptive family patterns
observed at home or at her family in general.
Environmental hazards
C.W states that she is always aware of environmental hazards around her environment
and household. She stays in environmental friendly environment. She always keeps her
brings them to house for minimal preparation. Her weight status indicates she is lightly
overweight with BMI index of 25.1. This is due to high snacking and regular consumption of
meals.
Interpersonal relationships
C.W states that she normally has normal cordial relationships with her children. She
states that she often is in good cordial relation with her family and she is a member of church
choir. She sometimes spends time with church members and her peers at work place during
weekends when not at work. She has not had any stressful event in her life of late. She
maintains good relation with friends.
Coping and stress management
C.W states that she has been usual calm life, except when there is small family stress of
children. She states that at times more finances are needed for upkeep of her children.
However she states that she has leant on how to keep up with stress. She says when feeling
stressed up always goes to church to join choir practices. She has observed that this way she
can keep stress away.
Personal habits
C.W states that she normally takes coffee and chocolate in order to make her alert and
always not dull. She denies having smoke cigarette or even smokes. Further she also denies
having any alcohol use over the last 10 years. As mother she does not indulge in drug abuse
or any form of drug abuse. With history of her family she doesn’t have any kind of history of
drug abuse in the family. There is no form of depression and disruptive family patterns
observed at home or at her family in general.
Environmental hazards
C.W states that she is always aware of environmental hazards around her environment
and household. She stays in environmental friendly environment. She always keeps her
PATIENT HEALTH HISTORY ASSESSMENT 10
house always clean and safe. Her dust bin is far end of the house aimed at minimization
contamination of germs within the household. She says she often encounters various health
hazards as a vocational health nurse. She often tries to minimize environmental hazards
exposure for her and her family.
Intimate Partner Violence
C.W states that she has not been a victim of gender based violence in her marriage life.
She states that she is comfortable with her marriage life and bringing up the children,
however the marriage life did not clearly come out.
Occupational health
She states that she is always concern of occupation health status of her job. She says
that her job is always occasioned with various risks which need attention. At times she
exposes herself to harm and infection due to the nature of her career. However she states that
she has put in place enough measures to adopt a healthy work place schedule and coping with
occupational hazards.
Perception of own health
C.W states that her own health physical, spiritual and mental health is of sound state.
She tries much to keep and maintain healthy weight gain. She states that she has no history of
medical illness except for gall bladder, allergy medication and the C-section operation many
years back. She is upkeep of her career and enjoys being and registered licensed vocational
nurse. She has no concerns of care being given but alert on medication o be give. She is
concern of how she consumes food regularly without such symptoms but now it has occurred.
She states that her health goal is achieve healthy weight gain and consume healthy foods,
however she has been having challenges meeting this as she occasionally buys foods from
outside. Her participation in church activities is meant to keep her social and personal relation
with God and church members positive.
house always clean and safe. Her dust bin is far end of the house aimed at minimization
contamination of germs within the household. She says she often encounters various health
hazards as a vocational health nurse. She often tries to minimize environmental hazards
exposure for her and her family.
Intimate Partner Violence
C.W states that she has not been a victim of gender based violence in her marriage life.
She states that she is comfortable with her marriage life and bringing up the children,
however the marriage life did not clearly come out.
Occupational health
She states that she is always concern of occupation health status of her job. She says
that her job is always occasioned with various risks which need attention. At times she
exposes herself to harm and infection due to the nature of her career. However she states that
she has put in place enough measures to adopt a healthy work place schedule and coping with
occupational hazards.
Perception of own health
C.W states that her own health physical, spiritual and mental health is of sound state.
She tries much to keep and maintain healthy weight gain. She states that she has no history of
medical illness except for gall bladder, allergy medication and the C-section operation many
years back. She is upkeep of her career and enjoys being and registered licensed vocational
nurse. She has no concerns of care being given but alert on medication o be give. She is
concern of how she consumes food regularly without such symptoms but now it has occurred.
She states that her health goal is achieve healthy weight gain and consume healthy foods,
however she has been having challenges meeting this as she occasionally buys foods from
outside. Her participation in church activities is meant to keep her social and personal relation
with God and church members positive.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

PATIENT HEALTH HISTORY ASSESSMENT 11
References
Cunningham FG, et al. (2010). Cesarean delivery and peripartum hysterectomy. In Williams
Obstetrics, 23rd ed., pp. 544-564. New York: McGraw-Hill.
Jarvis, C. (2016). Physical examination and health assessment (7th ed.). St. Louis, MO:
Mosby Elsevier
References
Cunningham FG, et al. (2010). Cesarean delivery and peripartum hysterectomy. In Williams
Obstetrics, 23rd ed., pp. 544-564. New York: McGraw-Hill.
Jarvis, C. (2016). Physical examination and health assessment (7th ed.). St. Louis, MO:
Mosby Elsevier
1 out of 11



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.