Pediatric Oncology Providers Perceptions of Barriers and Facilitators to Early Integration of Pediatric Palliative Care
VerifiedAdded on 2023/06/09
|15
|7619
|233
AI Summary
This study investigates pediatric oncology providers’ perceptions of barriers and facilitators to early integration of a pediatric palliative care team (PPCT) as a standard part of treatment for children with cancer. The study identifies four themes associated with barriers and five themes that served as facilitators of early integration of pediatric palliative care. The barrier themes include provider role, conflicting philosophy, patient readiness, and emotional influence. The facilitator themes include patient eligibility, improved patient care, education, evidence-based medicine, and the potential to improve overall care of children diagnosed with cancer.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Pediatric Oncology Providers Perceptions of Barriers and
Facilitators to Early Integration of Pediatric Palliative Care
Todd Dalberg, DO(1), Elizabeth Jacob-Files, MA(2), Patricia A. Carney, PhD(3), Jeffrey
Meyrowitz, MD(4), Erik Fromme, MD, MCR(5), and Gregory Thomas, MD(1)
(1)Department of Pediatrics Division of Pediatric Hematology-Oncology, Oregon Health & Science
University, Portland, OR
(2)Department of Family Medicine, Oregon Health & Science University, Portland, OR
(3)Departments of Family Medicine and Public Health and Preventive Medicine, Oregon Health &
Science University, Portland, OR
(4)Department of Pediatrics, Oregon Health & Science University, Portland, OR Program Year 2
Pediatric Resident
(5)Division of Hematology and Medical Oncology, Knight Cancer Institute, and Palliative Medicine
& Comfort Care Team, Oregon Health & Science University, Portland, OR
Abstract
Background—Pediatric patients experience significant symptoms during cancer treatment.
Symptom management is frequently inadequate. We studied perceptions of pediatric oncology
care providers regarding early integration of palliative care (PC) for pediatric patients to identify
barriers and facilitators that might assist in understanding how care could be improved.
Procedures—Pediatric oncology providers were recruited to participate in four focus groups. A
proposal for early integration of a pediatric palliative care team (PPCT) was presented and
followed by a facilitated discussion. Data were analytically categorized into themes by three
independent coders using constant comparative analysis and crystallization techniques. A
consensus approach was used to indentify final themes.
Results—Barriers to the proposed care model of early integration of a PPCT included provider
role, conflicting philosophy, patient readiness and emotional influence and were more prevalent in
the physician participants compared to nurse practitioner, nursing, and social work participants.
Facilitators included patient eligibility, improved patient care, education, and evidence-based
medicine. Though all participants were invested in providing optimal patient care, physician
participants believed the current standard of care model is meeting the needs of patients and
family, while the nurse practitioner, nursing, and social work participants working on the same
healthcare team believed the proposed care model would improve the overall care of children
diagnosed with cancer.
Conclusions—Differing perceptions among healthcare providers regarding the care of children
with cancer suggest that team functioning could be improved. Avenues for pilot testing early
integration of PC could provide useful information for a next study.
Keywords
Palliative care; Pediatric; Oncology; Perceptions; Barriers
Correspondence to: Todd Dalberg, DO, Pediatric Hematology-Oncology, Oregon Health & Science University, 3181 SW Sam
Jackson Park Rd., Mailcode: CDRCP, Portland, OR 97239, dalberg@ohsu.edu, Telephone: 503-494-0829, Fax: 503-494-0714.
NIH Public Access
Author Manuscript
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
Published in final edited form as:
Pediatr Blood Cancer. 2013 November ; 60(11): 1875–1881. doi:10.1002/pbc.24673.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Facilitators to Early Integration of Pediatric Palliative Care
Todd Dalberg, DO(1), Elizabeth Jacob-Files, MA(2), Patricia A. Carney, PhD(3), Jeffrey
Meyrowitz, MD(4), Erik Fromme, MD, MCR(5), and Gregory Thomas, MD(1)
(1)Department of Pediatrics Division of Pediatric Hematology-Oncology, Oregon Health & Science
University, Portland, OR
(2)Department of Family Medicine, Oregon Health & Science University, Portland, OR
(3)Departments of Family Medicine and Public Health and Preventive Medicine, Oregon Health &
Science University, Portland, OR
(4)Department of Pediatrics, Oregon Health & Science University, Portland, OR Program Year 2
Pediatric Resident
(5)Division of Hematology and Medical Oncology, Knight Cancer Institute, and Palliative Medicine
& Comfort Care Team, Oregon Health & Science University, Portland, OR
Abstract
Background—Pediatric patients experience significant symptoms during cancer treatment.
Symptom management is frequently inadequate. We studied perceptions of pediatric oncology
care providers regarding early integration of palliative care (PC) for pediatric patients to identify
barriers and facilitators that might assist in understanding how care could be improved.
Procedures—Pediatric oncology providers were recruited to participate in four focus groups. A
proposal for early integration of a pediatric palliative care team (PPCT) was presented and
followed by a facilitated discussion. Data were analytically categorized into themes by three
independent coders using constant comparative analysis and crystallization techniques. A
consensus approach was used to indentify final themes.
Results—Barriers to the proposed care model of early integration of a PPCT included provider
role, conflicting philosophy, patient readiness and emotional influence and were more prevalent in
the physician participants compared to nurse practitioner, nursing, and social work participants.
Facilitators included patient eligibility, improved patient care, education, and evidence-based
medicine. Though all participants were invested in providing optimal patient care, physician
participants believed the current standard of care model is meeting the needs of patients and
family, while the nurse practitioner, nursing, and social work participants working on the same
healthcare team believed the proposed care model would improve the overall care of children
diagnosed with cancer.
Conclusions—Differing perceptions among healthcare providers regarding the care of children
with cancer suggest that team functioning could be improved. Avenues for pilot testing early
integration of PC could provide useful information for a next study.
Keywords
Palliative care; Pediatric; Oncology; Perceptions; Barriers
Correspondence to: Todd Dalberg, DO, Pediatric Hematology-Oncology, Oregon Health & Science University, 3181 SW Sam
Jackson Park Rd., Mailcode: CDRCP, Portland, OR 97239, dalberg@ohsu.edu, Telephone: 503-494-0829, Fax: 503-494-0714.
NIH Public Access
Author Manuscript
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
Published in final edited form as:
Pediatr Blood Cancer. 2013 November ; 60(11): 1875–1881. doi:10.1002/pbc.24673.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Introduction
Although supportive care is improving for pediatric oncology patients,1 many children
experience significant symptoms during cancer treatment and at end of life.2, 3 In 2000,
Wolfe et al. reported that 89% of parents whose child had died of cancer stated their child
experienced “a lot” or “a great deal” of suffering from at least one symptom during the end
of life.3 Parents also reported that successful treatment of these symptoms occurred less than
30% of the time. In another study of children with cancer, uncontrolled suffering at end of
life was more common among children undergoing stem cell transplant compared to those
not receiving a transplant.2 These observations may be a result of discordance between
physicians’ and parents’ perceptions of symptoms in ill children.3 A 2008 follow-up study1
documented a greater emphasis on palliative care (PC) in children who died of cancer which
correlated with better patient experiences, including less suffering and increased parental
preparedness prior to their child’s death.
In 2000, the American Academy of Pediatrics recommended pediatric palliative care (PCC)
be integrated early on as part of care provided to children with life threatening conditions.4
Despite these recommendations and evidence that supports the benefits of early integration
of (PC), barriers to incorporating this service exist. These include concerns about uncertain
prognosis, perceptions that families are not ready to acknowledge their child has a
potentially incurable disease, and a lack of access to PC consultation.5 Thompson, et al.
surveyed pediatricians and found that almost half believed that PC is indicated only at the
end of life when curative treatment is no longer a goal.6 Three of four studies on when to
introduce PC have been conducted with general pediatricians.5, 6, 7, 8 To our knowledge, no
research has focused specifically on perspectives of pediatric oncology providers. One study
examined PC consultation among children who died from cancer and found that 40% of
referrals took place after the first relapse, with 16% occurring within the first 30 days of
diagnosis.9 Our study investigated pediatric oncology providers’ perceptions of barriers and
facilitators to early integration of a pediatric palliative care team (PPCT) as a standard part
of treatment for children with cancer.
Methods
Participants and Procedures
We conducted four focus groups with pediatric oncology providers at an academic
children’s hospital. The Institutional Review Board approved all study activities. Pediatric
oncology providers included attendings, fellows, nurse practitioners, social workers and
nurses. Exclusion criterion included unwillingness or inability to participate in a focus group
session. Participants were recruited through written invitation and were consented
electronically. Participants were divided into three groups: 1) physicians and fellows, 2)
nurse practitioners and social workers, and 3) inpatient and outpatient nurses. This was done
to take advantage of each group’s specific expertise and how this might inform their
perspectives, and to encourage willingness to honestly express viewpoints, which might not
occur if hierarchical persuasion existed. Two focus groups were held with nurses to
accommodate work schedules, for a total of four exploratory focus groups. We conducted
two validation focus groups after initial analysis was performed to verify emergent themes
based on selected exemplars to substantiate our findings. This additional step strengthened
the findings by having participants affirm or clarify any discrepancies in our interpretation
of emerging themes in the initial data set.
Prior to participation in the focus group, participants completed a demographic survey and
clinical practice history, which asked about age, gender, profession, training completion
Dalberg et al. Page 2
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Although supportive care is improving for pediatric oncology patients,1 many children
experience significant symptoms during cancer treatment and at end of life.2, 3 In 2000,
Wolfe et al. reported that 89% of parents whose child had died of cancer stated their child
experienced “a lot” or “a great deal” of suffering from at least one symptom during the end
of life.3 Parents also reported that successful treatment of these symptoms occurred less than
30% of the time. In another study of children with cancer, uncontrolled suffering at end of
life was more common among children undergoing stem cell transplant compared to those
not receiving a transplant.2 These observations may be a result of discordance between
physicians’ and parents’ perceptions of symptoms in ill children.3 A 2008 follow-up study1
documented a greater emphasis on palliative care (PC) in children who died of cancer which
correlated with better patient experiences, including less suffering and increased parental
preparedness prior to their child’s death.
In 2000, the American Academy of Pediatrics recommended pediatric palliative care (PCC)
be integrated early on as part of care provided to children with life threatening conditions.4
Despite these recommendations and evidence that supports the benefits of early integration
of (PC), barriers to incorporating this service exist. These include concerns about uncertain
prognosis, perceptions that families are not ready to acknowledge their child has a
potentially incurable disease, and a lack of access to PC consultation.5 Thompson, et al.
surveyed pediatricians and found that almost half believed that PC is indicated only at the
end of life when curative treatment is no longer a goal.6 Three of four studies on when to
introduce PC have been conducted with general pediatricians.5, 6, 7, 8 To our knowledge, no
research has focused specifically on perspectives of pediatric oncology providers. One study
examined PC consultation among children who died from cancer and found that 40% of
referrals took place after the first relapse, with 16% occurring within the first 30 days of
diagnosis.9 Our study investigated pediatric oncology providers’ perceptions of barriers and
facilitators to early integration of a pediatric palliative care team (PPCT) as a standard part
of treatment for children with cancer.
Methods
Participants and Procedures
We conducted four focus groups with pediatric oncology providers at an academic
children’s hospital. The Institutional Review Board approved all study activities. Pediatric
oncology providers included attendings, fellows, nurse practitioners, social workers and
nurses. Exclusion criterion included unwillingness or inability to participate in a focus group
session. Participants were recruited through written invitation and were consented
electronically. Participants were divided into three groups: 1) physicians and fellows, 2)
nurse practitioners and social workers, and 3) inpatient and outpatient nurses. This was done
to take advantage of each group’s specific expertise and how this might inform their
perspectives, and to encourage willingness to honestly express viewpoints, which might not
occur if hierarchical persuasion existed. Two focus groups were held with nurses to
accommodate work schedules, for a total of four exploratory focus groups. We conducted
two validation focus groups after initial analysis was performed to verify emergent themes
based on selected exemplars to substantiate our findings. This additional step strengthened
the findings by having participants affirm or clarify any discrepancies in our interpretation
of emerging themes in the initial data set.
Prior to participation in the focus group, participants completed a demographic survey and
clinical practice history, which asked about age, gender, profession, training completion
Dalberg et al. Page 2
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
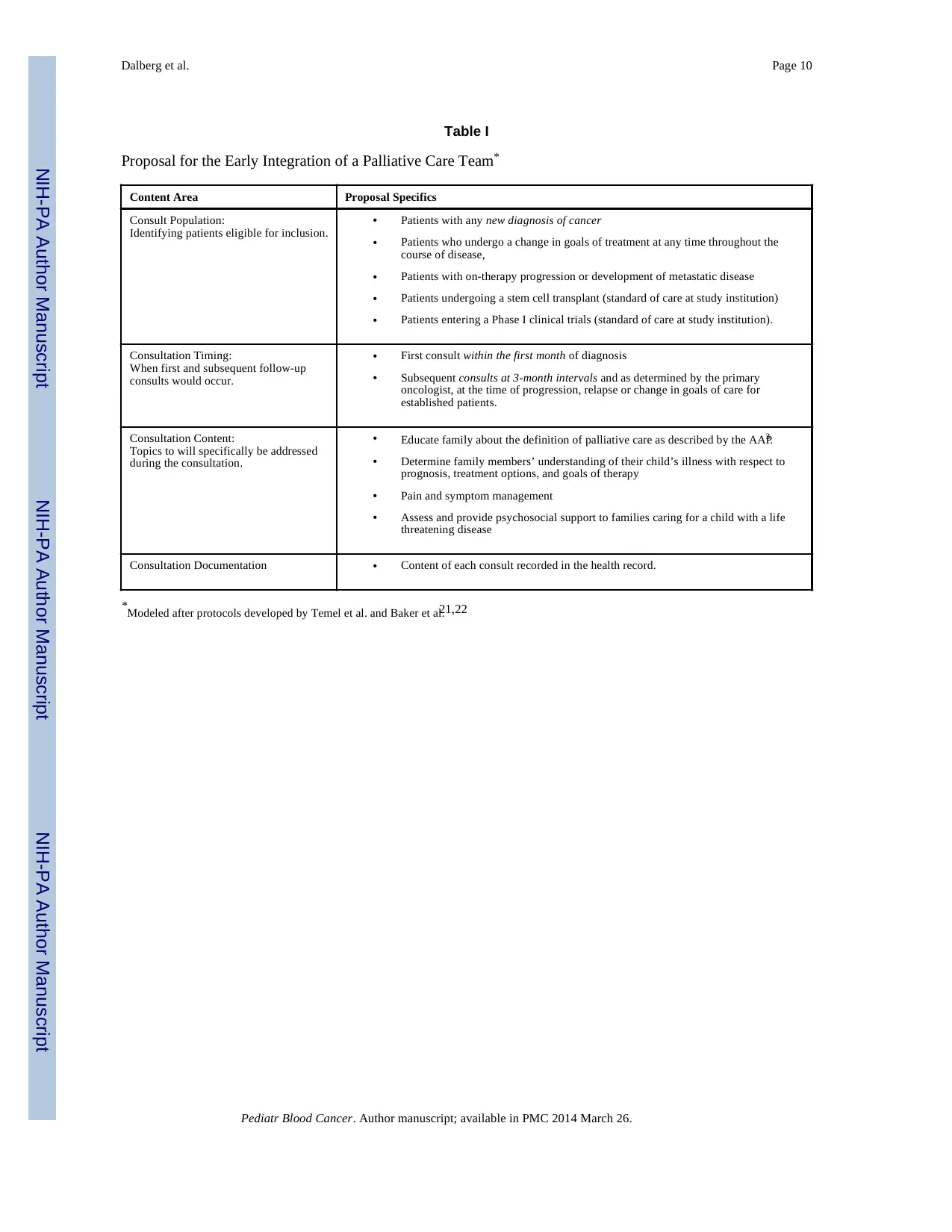
year, and years of clinical practice. At the beginning of each focus group, participants
observed a 10-minute presentation by author TD outlining a proposed model for early
integration of PC, including the study institution’s indications for PC referral (Table I).
Participants were then allowed to ask clarifying questions. Author PAC facilitated the rest of
the focus group using an interview schedule (Supplemental Appendix) designed to elicit
perspectives regarding early integration of palliative care in a neutral, non-leading way
while using prompts to clarify or to delve more deeply into responses. The focus groups
occurred between March and November 2011.
Data Collection and Analyses
Focus groups were audio recorded, de-identified and transcribed verbatim by an independent
transcription service, and double-checked for accuracy. Resultant data files were loaded into
NVivo qualitative analysis software v.8.010 for coding and analysis. The analytic approach
used constant comparative analysis and immersion/crystallization, which involves: 1)
independent identification and reflection of emerging themes, 2) creating a codebook, 3)
merging codes into similar themes, and 4) using a consensus approach to identify final
emerging themes. 11–13 Three authors (TD, EJF, JM) independently coded during the first
immersion/crystallization cycle to develop a preliminary codebook. The codebook was
refined as were themes and relationships among themes during the second immersion/
crystallization cycle until consensus was reached among the analytic team. At designated
intervals, the focus group facilitator met with analysts to review, independently audit, and
assess the validity of emerging findings. The goal of this approach was to group similar
themes together while accounting for each unique code. Once the final codebook was agreed
upon, investigators coded each subsequent transcript using discussion and eventual
consensus.
Results
Demographics
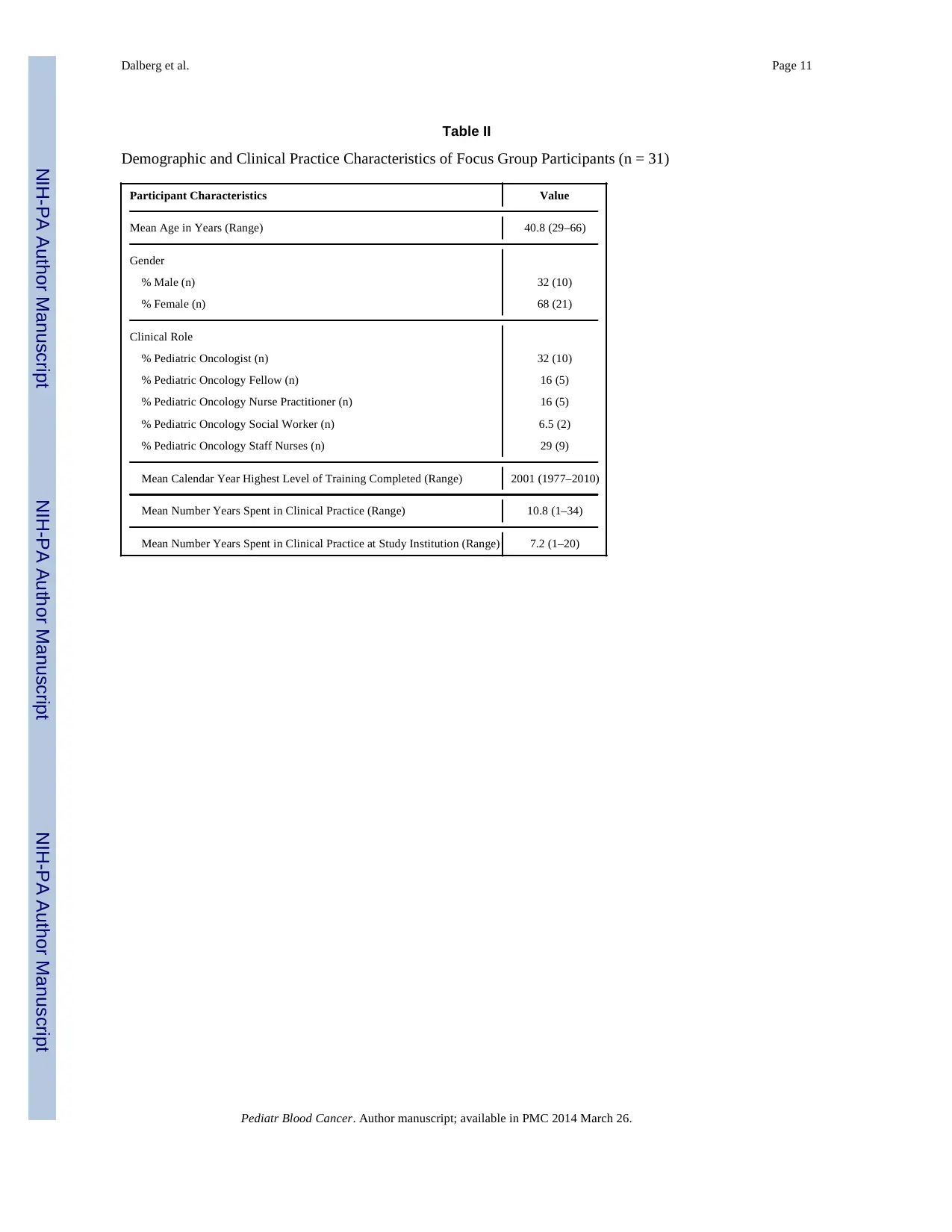
Participants of initial focus groups included 15 physicians, seven nurse practitioners, two
social workers, and nine inpatient and outpatient nurses. Of the original 15 physicians, 12
(80%) participated in the validation focus group. Four of the original five nurse practitioners
(80%), both of the social workers, and two of the original nine nurses (22%) participated in
the validation focus groups. Reasons for not participating in the validation groups included
work schedule conflicts, which affected the nurses disproportionately, as well as providers
who had since taken positions at other institutions.
The mean age of focus group participants was 41 years of age, with a range of 29–66, with
twice as many females as male (Table II). The focus group data analysis identified four
themes associated with barriers and five themes that served as facilitators of early
integration of pediatric palliative care.
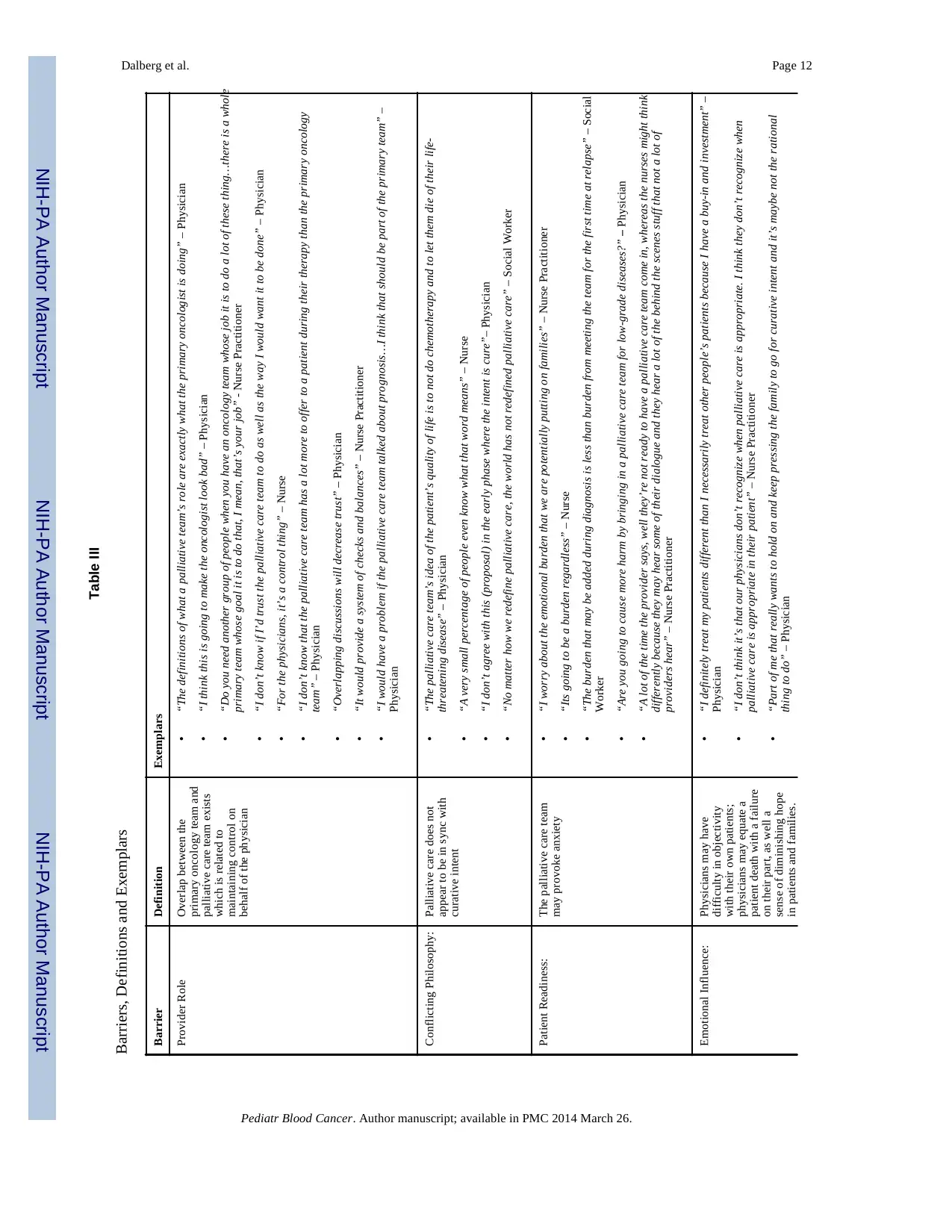
Barriers—Barrier themes included: 1) provider role, 2) conflicting philosophy, 3) patient
readiness, and 4) emotional influence (Table III).
Provider Role: Participants in all provider groups reported concern about overlap in roles
between the primary oncology team and the palliative care team. Physicians expressed views
indicating patients’ PC needs are already adequately addressed by the oncology team, which
typically includes a primary physician, nurse and social worker. Both physicians and nurses
raised concerns that having another team addressing aspects of PC might negatively affect
the physician/patient/family relationship. One physician indicated the proposed early
Dalberg et al. Page 3
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
observed a 10-minute presentation by author TD outlining a proposed model for early
integration of PC, including the study institution’s indications for PC referral (Table I).
Participants were then allowed to ask clarifying questions. Author PAC facilitated the rest of
the focus group using an interview schedule (Supplemental Appendix) designed to elicit
perspectives regarding early integration of palliative care in a neutral, non-leading way
while using prompts to clarify or to delve more deeply into responses. The focus groups
occurred between March and November 2011.
Data Collection and Analyses
Focus groups were audio recorded, de-identified and transcribed verbatim by an independent
transcription service, and double-checked for accuracy. Resultant data files were loaded into
NVivo qualitative analysis software v.8.010 for coding and analysis. The analytic approach
used constant comparative analysis and immersion/crystallization, which involves: 1)
independent identification and reflection of emerging themes, 2) creating a codebook, 3)
merging codes into similar themes, and 4) using a consensus approach to identify final
emerging themes. 11–13 Three authors (TD, EJF, JM) independently coded during the first
immersion/crystallization cycle to develop a preliminary codebook. The codebook was
refined as were themes and relationships among themes during the second immersion/
crystallization cycle until consensus was reached among the analytic team. At designated
intervals, the focus group facilitator met with analysts to review, independently audit, and
assess the validity of emerging findings. The goal of this approach was to group similar
themes together while accounting for each unique code. Once the final codebook was agreed
upon, investigators coded each subsequent transcript using discussion and eventual
consensus.
Results
Demographics
Participants of initial focus groups included 15 physicians, seven nurse practitioners, two
social workers, and nine inpatient and outpatient nurses. Of the original 15 physicians, 12
(80%) participated in the validation focus group. Four of the original five nurse practitioners
(80%), both of the social workers, and two of the original nine nurses (22%) participated in
the validation focus groups. Reasons for not participating in the validation groups included
work schedule conflicts, which affected the nurses disproportionately, as well as providers
who had since taken positions at other institutions.
The mean age of focus group participants was 41 years of age, with a range of 29–66, with
twice as many females as male (Table II). The focus group data analysis identified four
themes associated with barriers and five themes that served as facilitators of early
integration of pediatric palliative care.
Barriers—Barrier themes included: 1) provider role, 2) conflicting philosophy, 3) patient
readiness, and 4) emotional influence (Table III).
Provider Role: Participants in all provider groups reported concern about overlap in roles
between the primary oncology team and the palliative care team. Physicians expressed views
indicating patients’ PC needs are already adequately addressed by the oncology team, which
typically includes a primary physician, nurse and social worker. Both physicians and nurses
raised concerns that having another team addressing aspects of PC might negatively affect
the physician/patient/family relationship. One physician indicated the proposed early
Dalberg et al. Page 3
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
integration care model could make the oncologist, “look bad.” This comment resonated
throughout the physician group.
Conversely, nurse practitioners and social workers indicated that patient needs are not
adequately being met when palliative care is offered only when cure is no longer the goal.
Despite recognizing the potential overlap in patient care by the oncology team and the
PPCT, nurses also believed this model could better meet the complex needs of children with
cancer compared to the current model. Among nurses and nurse practitioners, general
consensus existed that patient symptoms, particularly psychosocial symptoms, contributed to
lower quality of life and could benefit from more focused attention. The validation group
confirmed this finding.
Participants in both validation focus groups identified the physicians’ need to control aspects
of patient care. Most physicians perceived treatment-related symptom management and
discussions of diagnosis, prognosis, and treatment options as responsibilities of the treating
physician alone. Although the PPCT was viewed as a subspecialty with specific expertise, a
subset of physicians commented that consults from other subspecialists (e.g. pediatric
nephrologists) are embraced more willingly than palliative care consults. Physicians also
made a distinction between treatment-related symptoms and disease-related symptoms,
indicating the oncology team could best manage the former, while the latter may or may not
be best managed by the PPCT. In the validation group, physicians clarified the purpose of
the PC consult within the first month of diagnosis as being for educational purposes only.
Conflicting Philosophy: Approximately half of the physician participants believed the
purpose of PC is inconsistent with cure and only appropriate when cure is no longer the
goal. Non-physician focus group participants did not share this belief. There was consensus
among all participants in the latter group that PC was well suited for children who have a
life threatening disease treated with curative intent. Concerns were expressed by many
participants that introducing the PPCT in the first month of diagnosis could lead to
additional parental anxiety, as the lay public often considers -palliative care- to be
synonymous with -hospice care-. Changing the title of the PPCT to the “Supportive Care
Team” or “Quality of Life Team” was proposed as a means of addressing misconceptions.
Patient Readiness: Given the complex information families must digest early in their
child’s diagnosis, nearly all participants expressed concern that introducing the PPCT early
could lead to additional parental burden. Five of 10 attending physicians believed that PC is
inconsistent with curative intent and emphasized that patients and families may not be ready
for a PC consult during the diagnostic period. No attending physicians contradicted this
perception in the initial focus group or the validation group. However, non-physician
participants expressed that the anxiety caused by early integration of a PPCT would be far
less than the anxiety experienced during relapse or disease progression. Overall, provider
groups stated the early integration model places a burden on patient families. Introducing
this model as standard of care was accepted by most participants as a means to alleviate
potential anxiety a family might experience when meeting the PPCT.
Emotional Influence: Several providers, especially nurse practitioners, were concerned that
primary oncologists’ emotions influence patient care. This occurs when physicians’ hope for
cure, even when the prognosis is poor, may bias treatment decisions and how information
regarding therapeutic options is relayed to patients and families. This emotional attachment
and potential bias was perceived to intensify over time. Nurses noted that physicians tend to
be overly optimistic when it comes to their own patients and speculated that the primary
oncologist feels responsible for their patient’s death and that fear of failure influences
decisions. One nurse commented that even with enrollment in a phase I study, where the
Dalberg et al. Page 4
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
throughout the physician group.
Conversely, nurse practitioners and social workers indicated that patient needs are not
adequately being met when palliative care is offered only when cure is no longer the goal.
Despite recognizing the potential overlap in patient care by the oncology team and the
PPCT, nurses also believed this model could better meet the complex needs of children with
cancer compared to the current model. Among nurses and nurse practitioners, general
consensus existed that patient symptoms, particularly psychosocial symptoms, contributed to
lower quality of life and could benefit from more focused attention. The validation group
confirmed this finding.
Participants in both validation focus groups identified the physicians’ need to control aspects
of patient care. Most physicians perceived treatment-related symptom management and
discussions of diagnosis, prognosis, and treatment options as responsibilities of the treating
physician alone. Although the PPCT was viewed as a subspecialty with specific expertise, a
subset of physicians commented that consults from other subspecialists (e.g. pediatric
nephrologists) are embraced more willingly than palliative care consults. Physicians also
made a distinction between treatment-related symptoms and disease-related symptoms,
indicating the oncology team could best manage the former, while the latter may or may not
be best managed by the PPCT. In the validation group, physicians clarified the purpose of
the PC consult within the first month of diagnosis as being for educational purposes only.
Conflicting Philosophy: Approximately half of the physician participants believed the
purpose of PC is inconsistent with cure and only appropriate when cure is no longer the
goal. Non-physician focus group participants did not share this belief. There was consensus
among all participants in the latter group that PC was well suited for children who have a
life threatening disease treated with curative intent. Concerns were expressed by many
participants that introducing the PPCT in the first month of diagnosis could lead to
additional parental anxiety, as the lay public often considers -palliative care- to be
synonymous with -hospice care-. Changing the title of the PPCT to the “Supportive Care
Team” or “Quality of Life Team” was proposed as a means of addressing misconceptions.
Patient Readiness: Given the complex information families must digest early in their
child’s diagnosis, nearly all participants expressed concern that introducing the PPCT early
could lead to additional parental burden. Five of 10 attending physicians believed that PC is
inconsistent with curative intent and emphasized that patients and families may not be ready
for a PC consult during the diagnostic period. No attending physicians contradicted this
perception in the initial focus group or the validation group. However, non-physician
participants expressed that the anxiety caused by early integration of a PPCT would be far
less than the anxiety experienced during relapse or disease progression. Overall, provider
groups stated the early integration model places a burden on patient families. Introducing
this model as standard of care was accepted by most participants as a means to alleviate
potential anxiety a family might experience when meeting the PPCT.
Emotional Influence: Several providers, especially nurse practitioners, were concerned that
primary oncologists’ emotions influence patient care. This occurs when physicians’ hope for
cure, even when the prognosis is poor, may bias treatment decisions and how information
regarding therapeutic options is relayed to patients and families. This emotional attachment
and potential bias was perceived to intensify over time. Nurses noted that physicians tend to
be overly optimistic when it comes to their own patients and speculated that the primary
oncologist feels responsible for their patient’s death and that fear of failure influences
decisions. One nurse commented that even with enrollment in a phase I study, where the
Dalberg et al. Page 4
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
purpose of the study is to gain information about an investigational drug rather than cure the
disease, physicians are often overly optimistic in information they provide about
experimental drugs.
Facilitators—Major facilitator themes identified included: 1) patient eligibility and timing
2) improved patient care, 3) education, and 4) evidence-based medicine (Table IV).
Patient Eligibility and Timing: Physician participants indicated that patients with overall
survival of <40 - 50% would likely benefit from early integration of PC. This perspective
differed from all other participants who expressed concerns that presuming who would
benefit from a PPCT based solely on prognosis would exclude some patients in need. Even
if the prognosis is favorable, families may have difficulty coping with their child’s cancer
diagnosis. It was clear among all provider groups that the PPCT would be educating families
at the initial consultation and at transition points (e.g., end of treatment, relapse), when
anxiety may be higher. All providers agreed that the frequency of consultation would be
most appropriate on an as needed basis determined by the primary oncologist.
Improved Patient Care: Non-physician participants were more receptive to integrating the
PPCT within the first month of diagnosis for all children with cancer compared to
physicians. Eight of 10 nurses and social workers believed early integration would address
symptoms and suffering better than current practice. In the validation group this theme
reached consensus among nurses. Nurses believed the PPCT role is currently underutilized
and that patient needs during active treatment often go unmet. They noted that parents
frequently bring concerns to them before they are discussed with other providers as nurses
are more readily available and parents sometimes fear disappointing their oncologist. Both
nurses present in the validation group believed this was an accurate consensus of the
opinions in the two initial focus groups.
There was also consensus among nurses that quality of life is often overlooked in the face of
cancer treatment, and suggested that decision-making incorporate a greater balance between
aggressive therapy and overall patient wellbeing. The proposed early integration care model
was viewed favorably because it would address quality of life at diagnosis and throughout
treatment. Social workers also perceived a relative lack of attention to quality of life
throughout treatment and embraced the proposed care model. This perspective was not as
predominant among physician participants.
Patient Education: All providers agreed that misconceptions about the purpose of PC
abound and that patients and families need to be educated about this service. Individuals in
each focus group suggested a variety of methods including discussion with patients,
providing lay literature, and external media. Nurse practitioners and nurses emphasized the
need for more effective medical education beginning early in medical school and continuing
into residency that clearly addresses the role of PC.
Evidence-based Medicine: Non-physician participants noted the lack of evidence-based
literature regarding trials of early integration of PC. In addition, they believed that
conducting a pilot study, with a select population of patients and physicians, would best
facilitate understanding this care model. The overall risks to patients in such a study were
perceived to be low by this group. They also believed it would provide valuable data about
this complex topic, while physicians did not express such an interest.
Dalberg et al. Page 5
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
disease, physicians are often overly optimistic in information they provide about
experimental drugs.
Facilitators—Major facilitator themes identified included: 1) patient eligibility and timing
2) improved patient care, 3) education, and 4) evidence-based medicine (Table IV).
Patient Eligibility and Timing: Physician participants indicated that patients with overall
survival of <40 - 50% would likely benefit from early integration of PC. This perspective
differed from all other participants who expressed concerns that presuming who would
benefit from a PPCT based solely on prognosis would exclude some patients in need. Even
if the prognosis is favorable, families may have difficulty coping with their child’s cancer
diagnosis. It was clear among all provider groups that the PPCT would be educating families
at the initial consultation and at transition points (e.g., end of treatment, relapse), when
anxiety may be higher. All providers agreed that the frequency of consultation would be
most appropriate on an as needed basis determined by the primary oncologist.
Improved Patient Care: Non-physician participants were more receptive to integrating the
PPCT within the first month of diagnosis for all children with cancer compared to
physicians. Eight of 10 nurses and social workers believed early integration would address
symptoms and suffering better than current practice. In the validation group this theme
reached consensus among nurses. Nurses believed the PPCT role is currently underutilized
and that patient needs during active treatment often go unmet. They noted that parents
frequently bring concerns to them before they are discussed with other providers as nurses
are more readily available and parents sometimes fear disappointing their oncologist. Both
nurses present in the validation group believed this was an accurate consensus of the
opinions in the two initial focus groups.
There was also consensus among nurses that quality of life is often overlooked in the face of
cancer treatment, and suggested that decision-making incorporate a greater balance between
aggressive therapy and overall patient wellbeing. The proposed early integration care model
was viewed favorably because it would address quality of life at diagnosis and throughout
treatment. Social workers also perceived a relative lack of attention to quality of life
throughout treatment and embraced the proposed care model. This perspective was not as
predominant among physician participants.
Patient Education: All providers agreed that misconceptions about the purpose of PC
abound and that patients and families need to be educated about this service. Individuals in
each focus group suggested a variety of methods including discussion with patients,
providing lay literature, and external media. Nurse practitioners and nurses emphasized the
need for more effective medical education beginning early in medical school and continuing
into residency that clearly addresses the role of PC.
Evidence-based Medicine: Non-physician participants noted the lack of evidence-based
literature regarding trials of early integration of PC. In addition, they believed that
conducting a pilot study, with a select population of patients and physicians, would best
facilitate understanding this care model. The overall risks to patients in such a study were
perceived to be low by this group. They also believed it would provide valuable data about
this complex topic, while physicians did not express such an interest.
Dalberg et al. Page 5
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Discussion
This study demonstrates that diverse perspectives exist among pediatric oncology providers
regarding early integration of PC for children diagnosed with cancer. Prior research
indicates concerns about prognosis and family preparedness regarding a potentially
incurable disease were the most common barriers to PC.5, 7 However, other studies indicate
these concerns are unfounded.14, 15
Access to a PPCT in pediatric oncology continues to be an issue as only 58% of Children’s
Oncology Group institutions having a PPCT and only 6% of these institutions discuss PC at
diagnosis.16 Although additional evidence indicates the availability and utilization of PC
services have increased over the past decade, demand for greater involvement of palliative
care for children diagnosed with cancer remains.1
Our study found perceptions about adequacy of PC differ between provider types where
physicians tend not to perceive unmet needs, while nurse practitioners, social workers and
nurses see a significant problem. Solutions identified included improving communication
and documentation. Importantly, many of the facilitators identified could also address
barriers, as suggested by the complex relationships between the barrier and facilitator
themes.
Another important finding in this study is the tension among oncology providers regarding
patients’ needs, suggesting that care for this population can generate significant emotions
about how to improve care, with resistance to changing current practice, especially if it
alters the relationship oncologists have with patients and families. We found resistance
among physicians to give up traditional roles to allow early integration of a PCCT. In
addition, we found conflicting philosophies about whether PC is consistent with curative
therapy, which served as a barrier to early PC, which differed from the non-physician
groups. Although all providers had concerns about patient readiness to receive PC, the non-
physician groups recognized oncologists’ influence in conveying hope for cure in the face of
a poor prognosis. This finding is important as efforts are increasing across the U.S. to
provide team-based care,17, 18 but if competing agendas exist within and between teams,
care will likely be affected.
All providers expressed concern that meeting the PPCT early may increase anxiety in
families, complicating an already stressed family dynamic. Thompson, et al. asked general
pediatricians about their preferred timing of PC referrals for patients with cancer, and 44.2%
believed end of life (EOL), when cure is no longer the goal, was the most appropriate time.6
Most nurses and both social workers felt that basing the timing of referral on prognostic
information alone would limit access to PC for patients who could benefit from this service.
Non-physician groups believed that early integration of a PPCT would improve patient care
by providing an unbiased perspective regarding physical, psychosocial and spiritual
symptom management, and by improving interdisciplinary communication. There are
benefits to patient care even if a PPCT is involved late20, and there may be early benefits as
well. In addition, limiting PC to EOL can place additional burdens on families when code
status, location of death, and symptom management can lead to parents feeling less
prepared1 and less familiar with the PPCT.
Our study participants agreed a family’s aversion to PC is often related to misconceptions
regarding PPCT’s purpose and the services they provide. All providers endorsed educational
opportunities to address misperceptions along with inclusion of educational materials family
members review with nursing staff at diagnosis.
Dalberg et al. Page 6
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
This study demonstrates that diverse perspectives exist among pediatric oncology providers
regarding early integration of PC for children diagnosed with cancer. Prior research
indicates concerns about prognosis and family preparedness regarding a potentially
incurable disease were the most common barriers to PC.5, 7 However, other studies indicate
these concerns are unfounded.14, 15
Access to a PPCT in pediatric oncology continues to be an issue as only 58% of Children’s
Oncology Group institutions having a PPCT and only 6% of these institutions discuss PC at
diagnosis.16 Although additional evidence indicates the availability and utilization of PC
services have increased over the past decade, demand for greater involvement of palliative
care for children diagnosed with cancer remains.1
Our study found perceptions about adequacy of PC differ between provider types where
physicians tend not to perceive unmet needs, while nurse practitioners, social workers and
nurses see a significant problem. Solutions identified included improving communication
and documentation. Importantly, many of the facilitators identified could also address
barriers, as suggested by the complex relationships between the barrier and facilitator
themes.
Another important finding in this study is the tension among oncology providers regarding
patients’ needs, suggesting that care for this population can generate significant emotions
about how to improve care, with resistance to changing current practice, especially if it
alters the relationship oncologists have with patients and families. We found resistance
among physicians to give up traditional roles to allow early integration of a PCCT. In
addition, we found conflicting philosophies about whether PC is consistent with curative
therapy, which served as a barrier to early PC, which differed from the non-physician
groups. Although all providers had concerns about patient readiness to receive PC, the non-
physician groups recognized oncologists’ influence in conveying hope for cure in the face of
a poor prognosis. This finding is important as efforts are increasing across the U.S. to
provide team-based care,17, 18 but if competing agendas exist within and between teams,
care will likely be affected.
All providers expressed concern that meeting the PPCT early may increase anxiety in
families, complicating an already stressed family dynamic. Thompson, et al. asked general
pediatricians about their preferred timing of PC referrals for patients with cancer, and 44.2%
believed end of life (EOL), when cure is no longer the goal, was the most appropriate time.6
Most nurses and both social workers felt that basing the timing of referral on prognostic
information alone would limit access to PC for patients who could benefit from this service.
Non-physician groups believed that early integration of a PPCT would improve patient care
by providing an unbiased perspective regarding physical, psychosocial and spiritual
symptom management, and by improving interdisciplinary communication. There are
benefits to patient care even if a PPCT is involved late20, and there may be early benefits as
well. In addition, limiting PC to EOL can place additional burdens on families when code
status, location of death, and symptom management can lead to parents feeling less
prepared1 and less familiar with the PPCT.
Our study participants agreed a family’s aversion to PC is often related to misconceptions
regarding PPCT’s purpose and the services they provide. All providers endorsed educational
opportunities to address misperceptions along with inclusion of educational materials family
members review with nursing staff at diagnosis.
Dalberg et al. Page 6
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Loss of hope may result in avoidance of difficult conversations at critical moments in the
course of cancer therapy. Knapp, et al. found that of 81.2% of pediatricians surveyed
reported experiencing difficulty talking about EOL issues, and 77.6% reported not wanting
parents to give up hope for their child.7 Our study identified the possible influence of
physicians’ emotions on treatment decisions, which could potentially lead to unrealistic
goals of therapy. This finding is consistent with previous studies that suggest treatment
decisions for children during the EOL period are highly influenced by the physician,5, 6, 7
with potentially negative consequences. For example, an uncertain prognosis may lead to
suffering from attempts at life prolonging therapies, delayed preparation for the EOL period,
and moral distress on the part of staff if they feel the child is suffering from those
treatments. Nurse practitioners and social workers in our study emphasized how physicians’
emotions influence how they convey information to parents. The addition of an objective
opinion beginning at diagnosis and continuing throughout treatment could improve care for
children diagnosed with cancer, particularly at times of relapse or progression.
Our study addressed pediatric oncology providers’ perceptions of barriers and facilitators to
early integration of a PPCT in pediatric oncology. Our study was novel because few studies
on the use of PC have used qualitative methods.3 Prior studies utilized a survey design
method,2,5–8,14–16 and are limited by the inability to capture in-depth information, which can
be obtained in the dynamic dialogue that often occurs with focus group methodologies.
Furthermore, few studies have investigated barriers or facilitators to a novel proposal, in this
case, early integration of a PPCT. By conducting validation focus groups, coupled with
iterative analyses using NVivo, we further substantiated our findings. Qualitative
methodology focuses on thematic identification, which will inform the next step of our
research, survey formation. These will be designed to capture numerical variables and
relationships. We chose to use the proposal to standardize the stimulus that our focus group
participants reacted to. This technique resulted in very thoughtful responses from
participants. We intend to alter the proposed model for early integration of a PPCT based on
our findings. Though a consensus was not achieved across all provider groups, a revised
care model would continue to focus on addressing the parents understanding of diagnosis,
prognosis, treatment options, pain and symptom management, support systems and
education. In addition, we would change the follow-up time points from every three months,
as described by Temel, et al.21, to within the first month of diagnosis with follow-up on an
as needed basis. There was consensus that end of therapy follow-up with the palliative care
team would be another important check point as families experience anxiety during this
transition to fewer clinical appointments and no cancer-directed therapy.
Our study has several limitations. Although we captured multidisciplinary perceptions, our
study is limited by being from a single institution. Selection bias may have influenced our
findings, as those with strong opinions in favor of or against the topic of PC were likely to
attend. A disproportionately low representation of nurses (29%) is another weakness. We
attributed this to personal obligations and the inability to step away from patient. Though
perspectives were fairly uniform in the initial nursing groups, we can’t be certain we
captured all perspectives in the validation groups. Identifying a time for all of the initial
participants was not possible. Also, hierarchical persuasion may have been present in the
attending/fellow group, which may have altered responses from the fellows. However, over
half the fellows provided in depth perspectives that did not always reflect the sentiment of
the attendings. We plan to conduct additional research based on the current study to
overcome these limitations.
In conclusion, this study provides important insights on the perceptions of pediatric
oncology providers about PC. We found very different perspectives from physician and non-
physician participants, all of whom share the goal of providing excellent care, but differ on
Dalberg et al. Page 7
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
course of cancer therapy. Knapp, et al. found that of 81.2% of pediatricians surveyed
reported experiencing difficulty talking about EOL issues, and 77.6% reported not wanting
parents to give up hope for their child.7 Our study identified the possible influence of
physicians’ emotions on treatment decisions, which could potentially lead to unrealistic
goals of therapy. This finding is consistent with previous studies that suggest treatment
decisions for children during the EOL period are highly influenced by the physician,5, 6, 7
with potentially negative consequences. For example, an uncertain prognosis may lead to
suffering from attempts at life prolonging therapies, delayed preparation for the EOL period,
and moral distress on the part of staff if they feel the child is suffering from those
treatments. Nurse practitioners and social workers in our study emphasized how physicians’
emotions influence how they convey information to parents. The addition of an objective
opinion beginning at diagnosis and continuing throughout treatment could improve care for
children diagnosed with cancer, particularly at times of relapse or progression.
Our study addressed pediatric oncology providers’ perceptions of barriers and facilitators to
early integration of a PPCT in pediatric oncology. Our study was novel because few studies
on the use of PC have used qualitative methods.3 Prior studies utilized a survey design
method,2,5–8,14–16 and are limited by the inability to capture in-depth information, which can
be obtained in the dynamic dialogue that often occurs with focus group methodologies.
Furthermore, few studies have investigated barriers or facilitators to a novel proposal, in this
case, early integration of a PPCT. By conducting validation focus groups, coupled with
iterative analyses using NVivo, we further substantiated our findings. Qualitative
methodology focuses on thematic identification, which will inform the next step of our
research, survey formation. These will be designed to capture numerical variables and
relationships. We chose to use the proposal to standardize the stimulus that our focus group
participants reacted to. This technique resulted in very thoughtful responses from
participants. We intend to alter the proposed model for early integration of a PPCT based on
our findings. Though a consensus was not achieved across all provider groups, a revised
care model would continue to focus on addressing the parents understanding of diagnosis,
prognosis, treatment options, pain and symptom management, support systems and
education. In addition, we would change the follow-up time points from every three months,
as described by Temel, et al.21, to within the first month of diagnosis with follow-up on an
as needed basis. There was consensus that end of therapy follow-up with the palliative care
team would be another important check point as families experience anxiety during this
transition to fewer clinical appointments and no cancer-directed therapy.
Our study has several limitations. Although we captured multidisciplinary perceptions, our
study is limited by being from a single institution. Selection bias may have influenced our
findings, as those with strong opinions in favor of or against the topic of PC were likely to
attend. A disproportionately low representation of nurses (29%) is another weakness. We
attributed this to personal obligations and the inability to step away from patient. Though
perspectives were fairly uniform in the initial nursing groups, we can’t be certain we
captured all perspectives in the validation groups. Identifying a time for all of the initial
participants was not possible. Also, hierarchical persuasion may have been present in the
attending/fellow group, which may have altered responses from the fellows. However, over
half the fellows provided in depth perspectives that did not always reflect the sentiment of
the attendings. We plan to conduct additional research based on the current study to
overcome these limitations.
In conclusion, this study provides important insights on the perceptions of pediatric
oncology providers about PC. We found very different perspectives from physician and non-
physician participants, all of whom share the goal of providing excellent care, but differ on
Dalberg et al. Page 7
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
how to best achieve this despite working on the same healthcare teams. Future research
should address how the barriers and facilitators to early introduction of PC for children with
cancer we have identified can be used to improve the care of these patients.
Supplementary Material
Refer to Web version on PubMed Central for supplementary material.
Acknowledgments
This publication was made possible with support from the Oregon Clinical and Translational Research Institute
(OCTRI), grant number UL1 RR024140 from the National Center for Advancing Translational Sciences (NCATS),
a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Funding was also
supported by the Early Clinical Investigator Award through Medical Research Foundation of Oregon, and through
the Knight Cancer Institute (P30 CA069533C).
References
1. Wolfe J, Hammel J, Edwards K, et al. Easing of Suffering in Children With Cancer at the End of
Life: Is Care Changing? J Clin Oncol. 2008; 26:1717–1723. [PubMed: 18375901]
2. Ullrich C, Dussel V, Hilden J, et al. End-of-Life experience in children undergoing stem cell
transplantation for malignancy: parent and provider perspective and patterns of care. Blood. 2010;
115:3879–3885. [PubMed: 20228275]
3. Wolfe J, Grier H, Klar N, et al. Symptoms and Suffering at The End of Life in Children with
Cancer. New Engl J Med. 2000; 342:326–333. [PubMed: 10655532]
4. Palliative Care for Children. Pediatrics. 2000; 106:351–357. [PubMed: 10920167]
5. Davies B, Sehring S, Partridge C, et al. Barriers to Palliative Care for Children: Perceptions of
Pediatric Health Care Providers. Pediatrics. 2008; 121:282–288. [PubMed: 18245419]
6. Thompson L, Knapp C, Madden V, Shenkman E. Pediatricians’ Perceptions of and Preferred
Timing for Pediatric Palliative Care. Pediatrics. 2009; 123:777–782.
7. Knapp C, Thompson L. Factors associated with perceived barriers to pediatric palliative care: a
survey of pediatricians in Florida and California. Pall Med. 2011; 26(3):268–274.
8. Junger S, Vedder A, Milde S, et al. Peadiatric palliative care home care by general paediatricians: a
multimethod study of perceived barriers and facilitators. BMC Palliative Care. 2010; 9:11.
[PubMed: 20525318]
9. Johnston D, Vadeboncoeur C. Palliatve Care Consultation in Pediatric Oncology. Support Care
Cancer. 2012; 20:799–803. [PubMed: 21479523]
10. QSR International NVivo v.8.0 software
11. Crabtree, BF.; Miller, WL., editors. Doing qualitative research. 2. Thousand Oaks, CA: Sage
Publications; 1999.
12. Crabtree, BF.; Miller, WL., editors. Doing Qualitative Research in Primary Care: Multiple
Strategies. 2. Newbury Park, CA: Sage Publications; 1999.
13. Patton MQ. Enhancing the quality and credibility of qualitative analysis. Health Services Research.
1999; 34:1189–1208. [PubMed: 10591279]
14. Wolfe J, Klar N, Grier H, et al. Understanding of Prognosis Among Parents of Children Who Died
of Cancer. JAMA. 2000; 284:2469–2475. [PubMed: 11074776]
15. Mack J, Wolfe J, Cook E, et al. Hope and Prognostic Disclosure. J Clin Oncol. 2007; 25:5636–
5642. [PubMed: 18065734]
16. Johnston D, Nagel K, et al. Availability and Use of Palliative Care and End-of-Life Services for
Pediatric Oncology Patients. J Clin Oncol. 2008; 26:4646–4650. [PubMed: 18824711]
17. Levit L, Smith AP, Benz EJ Jr, Ferrell B. Ensuring Quality Cancer Care Through the Oncology
Workforce. Journal of Oncology Practice. Jan 1.2010 :7–11. [PubMed: 20539724]
Dalberg et al. Page 8
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
should address how the barriers and facilitators to early introduction of PC for children with
cancer we have identified can be used to improve the care of these patients.
Supplementary Material
Refer to Web version on PubMed Central for supplementary material.
Acknowledgments
This publication was made possible with support from the Oregon Clinical and Translational Research Institute
(OCTRI), grant number UL1 RR024140 from the National Center for Advancing Translational Sciences (NCATS),
a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Funding was also
supported by the Early Clinical Investigator Award through Medical Research Foundation of Oregon, and through
the Knight Cancer Institute (P30 CA069533C).
References
1. Wolfe J, Hammel J, Edwards K, et al. Easing of Suffering in Children With Cancer at the End of
Life: Is Care Changing? J Clin Oncol. 2008; 26:1717–1723. [PubMed: 18375901]
2. Ullrich C, Dussel V, Hilden J, et al. End-of-Life experience in children undergoing stem cell
transplantation for malignancy: parent and provider perspective and patterns of care. Blood. 2010;
115:3879–3885. [PubMed: 20228275]
3. Wolfe J, Grier H, Klar N, et al. Symptoms and Suffering at The End of Life in Children with
Cancer. New Engl J Med. 2000; 342:326–333. [PubMed: 10655532]
4. Palliative Care for Children. Pediatrics. 2000; 106:351–357. [PubMed: 10920167]
5. Davies B, Sehring S, Partridge C, et al. Barriers to Palliative Care for Children: Perceptions of
Pediatric Health Care Providers. Pediatrics. 2008; 121:282–288. [PubMed: 18245419]
6. Thompson L, Knapp C, Madden V, Shenkman E. Pediatricians’ Perceptions of and Preferred
Timing for Pediatric Palliative Care. Pediatrics. 2009; 123:777–782.
7. Knapp C, Thompson L. Factors associated with perceived barriers to pediatric palliative care: a
survey of pediatricians in Florida and California. Pall Med. 2011; 26(3):268–274.
8. Junger S, Vedder A, Milde S, et al. Peadiatric palliative care home care by general paediatricians: a
multimethod study of perceived barriers and facilitators. BMC Palliative Care. 2010; 9:11.
[PubMed: 20525318]
9. Johnston D, Vadeboncoeur C. Palliatve Care Consultation in Pediatric Oncology. Support Care
Cancer. 2012; 20:799–803. [PubMed: 21479523]
10. QSR International NVivo v.8.0 software
11. Crabtree, BF.; Miller, WL., editors. Doing qualitative research. 2. Thousand Oaks, CA: Sage
Publications; 1999.
12. Crabtree, BF.; Miller, WL., editors. Doing Qualitative Research in Primary Care: Multiple
Strategies. 2. Newbury Park, CA: Sage Publications; 1999.
13. Patton MQ. Enhancing the quality and credibility of qualitative analysis. Health Services Research.
1999; 34:1189–1208. [PubMed: 10591279]
14. Wolfe J, Klar N, Grier H, et al. Understanding of Prognosis Among Parents of Children Who Died
of Cancer. JAMA. 2000; 284:2469–2475. [PubMed: 11074776]
15. Mack J, Wolfe J, Cook E, et al. Hope and Prognostic Disclosure. J Clin Oncol. 2007; 25:5636–
5642. [PubMed: 18065734]
16. Johnston D, Nagel K, et al. Availability and Use of Palliative Care and End-of-Life Services for
Pediatric Oncology Patients. J Clin Oncol. 2008; 26:4646–4650. [PubMed: 18824711]
17. Levit L, Smith AP, Benz EJ Jr, Ferrell B. Ensuring Quality Cancer Care Through the Oncology
Workforce. Journal of Oncology Practice. Jan 1.2010 :7–11. [PubMed: 20539724]
Dalberg et al. Page 8
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
18. Cashavelly BJ, Donean K, Binda KD, Mailhot JR, Clair-Hayes KA, Maramaldi P. The Forgotten
Team Member: Meeting the Needs of Oncology Support Staff. The Oncologist. 2008; 13:530–538.
[PubMed: 18515738]
19. [Accessed 9/26/11] (http://www.qsrinternational.com/products_nvivo.aspx)
20. Zhukovsky DS, Herzog CE, Kaur G, Palmer JL, Bruera E. The impact of palliative care
consultation on symptom assessment, communication needs, and palliatve interventions in
pediatric patients with cancer. J Palliat Med. 2009; 12:343–349. [PubMed: 19327071]
21. Temel J, Greer J, Muzikansky A, et al. Early Palliative Care for Patients with Metastatic Non-
Small-Cell Lung Cancer. N Engl J Med. 2010; 363:733–42. [PubMed: 20818875]
22. Baker J, Barfield R, Hinds P, Kane J. A Process to Facilitate Decision Making in Pediatric Stem
Cell Transplantation: The Individualized Care Planning and Coordination Model. Biology of
Blood and Marrow Transplantation. 2007; 13:245–254. [PubMed: 17317576]
Dalberg et al. Page 9
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Team Member: Meeting the Needs of Oncology Support Staff. The Oncologist. 2008; 13:530–538.
[PubMed: 18515738]
19. [Accessed 9/26/11] (http://www.qsrinternational.com/products_nvivo.aspx)
20. Zhukovsky DS, Herzog CE, Kaur G, Palmer JL, Bruera E. The impact of palliative care
consultation on symptom assessment, communication needs, and palliatve interventions in
pediatric patients with cancer. J Palliat Med. 2009; 12:343–349. [PubMed: 19327071]
21. Temel J, Greer J, Muzikansky A, et al. Early Palliative Care for Patients with Metastatic Non-
Small-Cell Lung Cancer. N Engl J Med. 2010; 363:733–42. [PubMed: 20818875]
22. Baker J, Barfield R, Hinds P, Kane J. A Process to Facilitate Decision Making in Pediatric Stem
Cell Transplantation: The Individualized Care Planning and Coordination Model. Biology of
Blood and Marrow Transplantation. 2007; 13:245–254. [PubMed: 17317576]
Dalberg et al. Page 9
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Dalberg et al. Page 10
Table I
Proposal for the Early Integration of a Palliative Care Team*
Content Area Proposal Specifics
Consult Population:
Identifying patients eligible for inclusion.
• Patients with any new diagnosis of cancer
• Patients who undergo a change in goals of treatment at any time throughout the
course of disease,
• Patients with on-therapy progression or development of metastatic disease
• Patients undergoing a stem cell transplant (standard of care at study institution)
• Patients entering a Phase I clinical trials (standard of care at study institution).
Consultation Timing:
When first and subsequent follow-up
consults would occur.
• First consult within the first month of diagnosis
• Subsequent consults at 3-month intervals and as determined by the primary
oncologist, at the time of progression, relapse or change in goals of care for
established patients.
Consultation Content:
Topics to will specifically be addressed
during the consultation.
• Educate family about the definition of palliative care as described by the AAP3.
• Determine family members’ understanding of their child’s illness with respect to
prognosis, treatment options, and goals of therapy
• Pain and symptom management
• Assess and provide psychosocial support to families caring for a child with a life
threatening disease
Consultation Documentation • Content of each consult recorded in the health record.
*Modeled after protocols developed by Temel et al. and Baker et al.21,22
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
Dalberg et al. Page 10
Table I
Proposal for the Early Integration of a Palliative Care Team*
Content Area Proposal Specifics
Consult Population:
Identifying patients eligible for inclusion.
• Patients with any new diagnosis of cancer
• Patients who undergo a change in goals of treatment at any time throughout the
course of disease,
• Patients with on-therapy progression or development of metastatic disease
• Patients undergoing a stem cell transplant (standard of care at study institution)
• Patients entering a Phase I clinical trials (standard of care at study institution).
Consultation Timing:
When first and subsequent follow-up
consults would occur.
• First consult within the first month of diagnosis
• Subsequent consults at 3-month intervals and as determined by the primary
oncologist, at the time of progression, relapse or change in goals of care for
established patients.
Consultation Content:
Topics to will specifically be addressed
during the consultation.
• Educate family about the definition of palliative care as described by the AAP3.
• Determine family members’ understanding of their child’s illness with respect to
prognosis, treatment options, and goals of therapy
• Pain and symptom management
• Assess and provide psychosocial support to families caring for a child with a life
threatening disease
Consultation Documentation • Content of each consult recorded in the health record.
*Modeled after protocols developed by Temel et al. and Baker et al.21,22
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Dalberg et al. Page 11
Table II
Demographic and Clinical Practice Characteristics of Focus Group Participants (n = 31)
Participant Characteristics Value
Mean Age in Years (Range) 40.8 (29–66)
Gender
% Male (n) 32 (10)
% Female (n) 68 (21)
Clinical Role
% Pediatric Oncologist (n) 32 (10)
% Pediatric Oncology Fellow (n) 16 (5)
% Pediatric Oncology Nurse Practitioner (n) 16 (5)
% Pediatric Oncology Social Worker (n) 6.5 (2)
% Pediatric Oncology Staff Nurses (n) 29 (9)
Mean Calendar Year Highest Level of Training Completed (Range) 2001 (1977–2010)
Mean Number Years Spent in Clinical Practice (Range) 10.8 (1–34)
Mean Number Years Spent in Clinical Practice at Study Institution (Range) 7.2 (1–20)
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
Dalberg et al. Page 11
Table II
Demographic and Clinical Practice Characteristics of Focus Group Participants (n = 31)
Participant Characteristics Value
Mean Age in Years (Range) 40.8 (29–66)
Gender
% Male (n) 32 (10)
% Female (n) 68 (21)
Clinical Role
% Pediatric Oncologist (n) 32 (10)
% Pediatric Oncology Fellow (n) 16 (5)
% Pediatric Oncology Nurse Practitioner (n) 16 (5)
% Pediatric Oncology Social Worker (n) 6.5 (2)
% Pediatric Oncology Staff Nurses (n) 29 (9)
Mean Calendar Year Highest Level of Training Completed (Range) 2001 (1977–2010)
Mean Number Years Spent in Clinical Practice (Range) 10.8 (1–34)
Mean Number Years Spent in Clinical Practice at Study Institution (Range) 7.2 (1–20)
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Dalberg et al. Page 12
Table III
Barriers, Definitions and Exemplars
Barrier Definition Exemplars
Provider Role Overlap between the
primary oncology team and
palliative care team exists
which is related to
maintaining control on
behalf of the physician
• “The definitions of what a palliative team’s role are exactly what the primary oncologist is doing” – Physician
• “I think this is going to make the oncologist look bad” – Physician
• “Do you need another group of people when you have an oncology team whose job it is to do a lot of these thing…there is a whole
primary team whose goal it is to do that, I mean, that’s your job” - Nurse Practitioner
• “I don’t know if I’d trust the palliative care team to do as well as the way I would want it to be done” – Physician
• “For the physicians, it’s a control thing” – Nurse
• “I don’t know that the palliative care team has a lot more to offer to a patient during their therapy than the primary oncology
team” – Physician
• “Overlapping discussions will decrease trust” – Physician
• “It would provide a system of checks and balances” – Nurse Practitioner
• “I would have a problem if the palliative care team talked about prognosis…I think that should be part of the primary team” –
Physician
Conflicting Philosophy: Palliative care does not
appear to be in sync with
curative intent
• “The palliative care team’s idea of the patient’s quality of life is to not do chemotherapy and to let them die of their life-
threatening disease” – Physician
• “A very small percentage of people even know what that word means” – Nurse
• “I don’t agree with this (proposal) in the early phase where the intent is cure”– Physician
• “No matter how we redefine palliative care, the world has not redefined palliative care” – Social Worker
Patient Readiness: The palliative care team
may provoke anxiety
• “I worry about the emotional burden that we are potentially putting on families” – Nurse Practitioner
• “Its going to be a burden regardless” – Nurse
• “The burden that may be added during diagnosis is less than burden from meeting the team for the first time at relapse” – Social
Worker
• “Are you going to cause more harm by bringing in a palliative care team for low-grade diseases?” – Physician
• “A lot of the time the provider says, well they’re not ready to have a palliative care team come in, whereas the nurses might think
differently because they may hear some of their dialogue and they hear a lot of the behind the scenes stuff that not a lot of
providers hear” – Nurse Practitioner
Emotional Influence: Physicians may have
difficulty in objectivity
with their own patients;
physicians may equate a
patient death with a failure
on their part, as well a
sense of diminishing hope
in patients and families.
• “I definitely treat my patients different than I necessarily treat other people’s patients because I have a buy-in and investment” –
Physician
• “I don’t think it’s that our physicians don’t recognize when palliative care is appropriate. I think they don’t recognize when
palliative care is appropriate in their patient” – Nurse Practitioner
• “Part of me that really wants to hold on and keep pressing the family to go for curative intent and it’s maybe not the rational
thing to do” – Physician
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
Dalberg et al. Page 12
Table III
Barriers, Definitions and Exemplars
Barrier Definition Exemplars
Provider Role Overlap between the
primary oncology team and
palliative care team exists
which is related to
maintaining control on
behalf of the physician
• “The definitions of what a palliative team’s role are exactly what the primary oncologist is doing” – Physician
• “I think this is going to make the oncologist look bad” – Physician
• “Do you need another group of people when you have an oncology team whose job it is to do a lot of these thing…there is a whole
primary team whose goal it is to do that, I mean, that’s your job” - Nurse Practitioner
• “I don’t know if I’d trust the palliative care team to do as well as the way I would want it to be done” – Physician
• “For the physicians, it’s a control thing” – Nurse
• “I don’t know that the palliative care team has a lot more to offer to a patient during their therapy than the primary oncology
team” – Physician
• “Overlapping discussions will decrease trust” – Physician
• “It would provide a system of checks and balances” – Nurse Practitioner
• “I would have a problem if the palliative care team talked about prognosis…I think that should be part of the primary team” –
Physician
Conflicting Philosophy: Palliative care does not
appear to be in sync with
curative intent
• “The palliative care team’s idea of the patient’s quality of life is to not do chemotherapy and to let them die of their life-
threatening disease” – Physician
• “A very small percentage of people even know what that word means” – Nurse
• “I don’t agree with this (proposal) in the early phase where the intent is cure”– Physician
• “No matter how we redefine palliative care, the world has not redefined palliative care” – Social Worker
Patient Readiness: The palliative care team
may provoke anxiety
• “I worry about the emotional burden that we are potentially putting on families” – Nurse Practitioner
• “Its going to be a burden regardless” – Nurse
• “The burden that may be added during diagnosis is less than burden from meeting the team for the first time at relapse” – Social
Worker
• “Are you going to cause more harm by bringing in a palliative care team for low-grade diseases?” – Physician
• “A lot of the time the provider says, well they’re not ready to have a palliative care team come in, whereas the nurses might think
differently because they may hear some of their dialogue and they hear a lot of the behind the scenes stuff that not a lot of
providers hear” – Nurse Practitioner
Emotional Influence: Physicians may have
difficulty in objectivity
with their own patients;
physicians may equate a
patient death with a failure
on their part, as well a
sense of diminishing hope
in patients and families.
• “I definitely treat my patients different than I necessarily treat other people’s patients because I have a buy-in and investment” –
Physician
• “I don’t think it’s that our physicians don’t recognize when palliative care is appropriate. I think they don’t recognize when
palliative care is appropriate in their patient” – Nurse Practitioner
• “Part of me that really wants to hold on and keep pressing the family to go for curative intent and it’s maybe not the rational
thing to do” – Physician
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
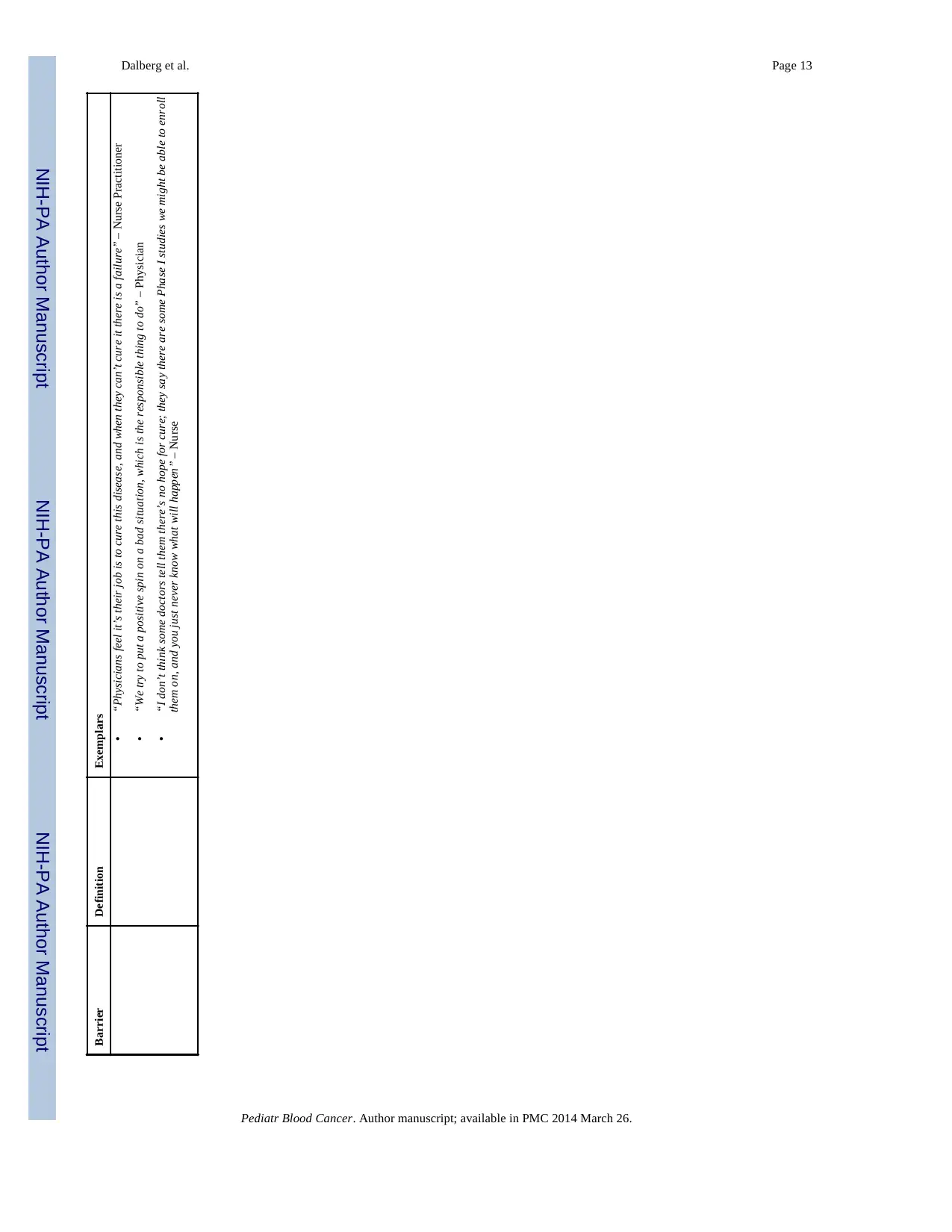
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Dalberg et al. Page 13
Barrier Definition Exemplars
• “Physicians feel it’s their job is to cure this disease, and when they can’t cure it there is a failure” – Nurse Practitioner
• “We try to put a positive spin on a bad situation, which is the responsible thing to do” – Physician
• “I don’t think some doctors tell them there’s no hope for cure; they say there are some Phase I studies we might be able to enroll
them on, and you just never know what will happen” – Nurse
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
Dalberg et al. Page 13
Barrier Definition Exemplars
• “Physicians feel it’s their job is to cure this disease, and when they can’t cure it there is a failure” – Nurse Practitioner
• “We try to put a positive spin on a bad situation, which is the responsible thing to do” – Physician
• “I don’t think some doctors tell them there’s no hope for cure; they say there are some Phase I studies we might be able to enroll
them on, and you just never know what will happen” – Nurse
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
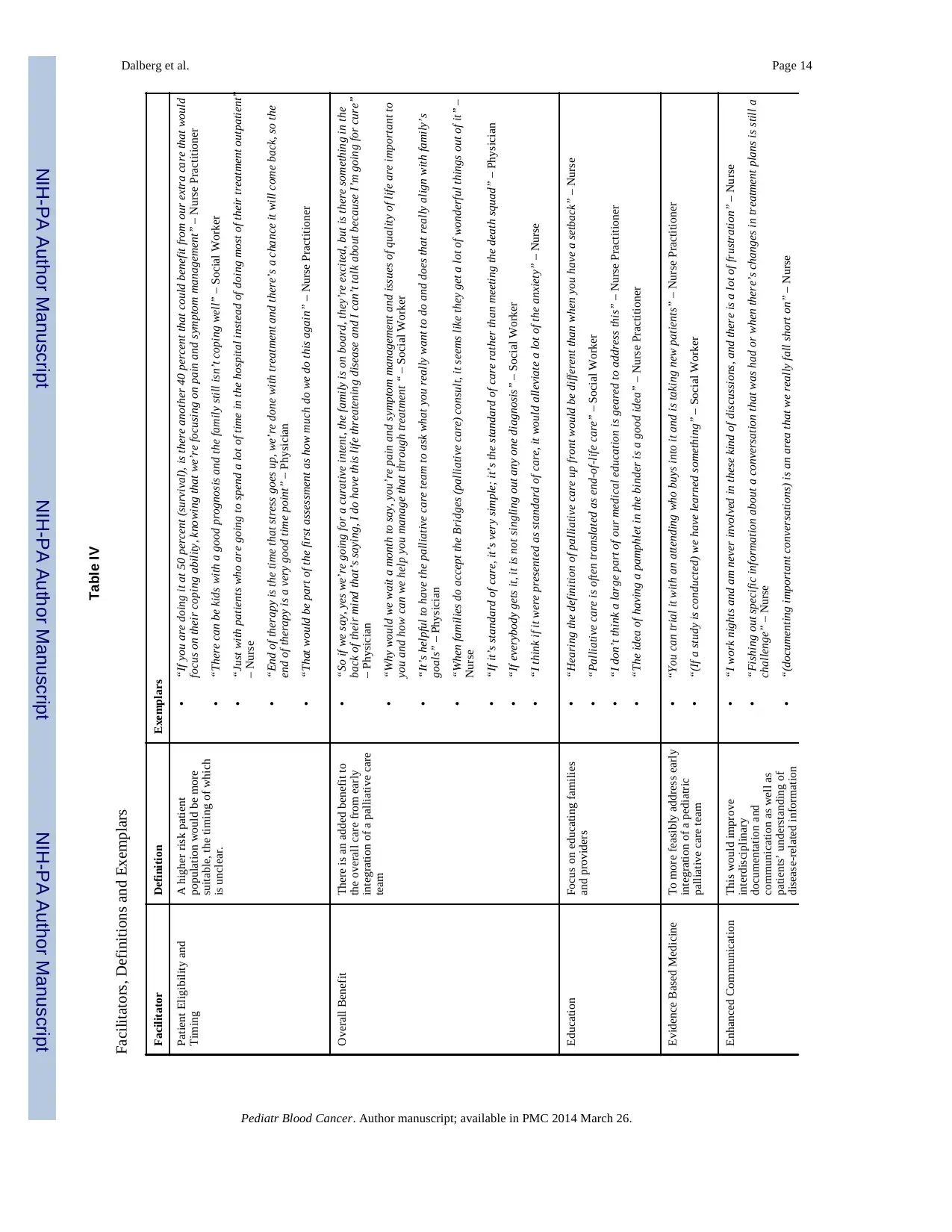
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Dalberg et al. Page 14
Table IV
Facilitators, Definitions and Exemplars
Facilitator Definition Exemplars
Patient Eligibility and
Timing
A higher risk patient
population would be more
suitable, the timing of which
is unclear.
• “If you are doing it at 50 percent (survival), is there another 40 percent that could benefit from our extra care that would
focus on their coping ability, knowing that we’re focusing on pain and symptom management” – Nurse Practitioner
• “There can be kids with a good prognosis and the family still isn’t coping well” – Social Worker
• “Just with patients who are going to spend a lot of time in the hospital instead of doing most of their treatment outpatient”
– Nurse
• “End of therapy is the time that stress goes up, we’re done with treatment and there’s a chance it will come back, so the
end of therapy is a very good time point” – Physician
• “That would be part of the first assessment as how much do we do this again” – Nurse Practitioner
Overall Benefit There is an added benefit to
the overall care from early
integration of a palliative care
team
• “So if we say, yes we’re going for a curative intent, the family is on board, they’re excited, but is there something in the
back of their mind that’s saying, I do have this life threatening disease and I can’t talk about because I’m going for cure”
– Physician
• “Why would we wait a month to say, you’re pain and symptom management and issues of quality of life are important to
you and how can we help you manage that through treatment “ – Social Worker
• “It’s helpful to have the palliative care team to ask what you really want to do and does that really align with family’s
goals” – Physician
• “When families do accept the Bridges (palliative care) consult, it seems like they get a lot of wonderful things out of it” –
Nurse
• “If it’s standard of care, it’s very simple; it’s the standard of care rather than meeting the death squad” – Physician
• “If everybody gets it, it is not singling out any one diagnosis” – Social Worker
• “I think if it were presented as standard of care, it would alleviate a lot of the anxiety” – Nurse
Education Focus on educating families
and providers
• “Hearing the definition of palliative care up front would be different than when you have a setback” – Nurse
• “Palliative care is often translated as end-of-life care” – Social Worker
• “I don’t think a large part of our medical education is geared to address this” – Nurse Practitioner
• “The idea of having a pamphlet in the binder is a good idea” – Nurse Practitioner
Evidence Based Medicine To more feasibly address early
integration of a pediatric
palliative care team
• “You can trial it with an attending who buys into it and is taking new patients” – Nurse Practitioner
• “(If a study is conducted) we have learned something” – Social Worker
Enhanced Communication This would improve
interdisciplinary
documentation and
communication as well as
patients’ understanding of
disease-related information
• “I work nights and am never involved in these kind of discussions, and there is a lot of frustration” – Nurse
• “Fishing out specific information about a conversation that was had or when there’s changes in treatment plans is still a
challenge” – Nurse
• “(documenting important conversations) is an area that we really fall short on” – Nurse
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
Dalberg et al. Page 14
Table IV
Facilitators, Definitions and Exemplars
Facilitator Definition Exemplars
Patient Eligibility and
Timing
A higher risk patient
population would be more
suitable, the timing of which
is unclear.
• “If you are doing it at 50 percent (survival), is there another 40 percent that could benefit from our extra care that would
focus on their coping ability, knowing that we’re focusing on pain and symptom management” – Nurse Practitioner
• “There can be kids with a good prognosis and the family still isn’t coping well” – Social Worker
• “Just with patients who are going to spend a lot of time in the hospital instead of doing most of their treatment outpatient”
– Nurse
• “End of therapy is the time that stress goes up, we’re done with treatment and there’s a chance it will come back, so the
end of therapy is a very good time point” – Physician
• “That would be part of the first assessment as how much do we do this again” – Nurse Practitioner
Overall Benefit There is an added benefit to
the overall care from early
integration of a palliative care
team
• “So if we say, yes we’re going for a curative intent, the family is on board, they’re excited, but is there something in the
back of their mind that’s saying, I do have this life threatening disease and I can’t talk about because I’m going for cure”
– Physician
• “Why would we wait a month to say, you’re pain and symptom management and issues of quality of life are important to
you and how can we help you manage that through treatment “ – Social Worker
• “It’s helpful to have the palliative care team to ask what you really want to do and does that really align with family’s
goals” – Physician
• “When families do accept the Bridges (palliative care) consult, it seems like they get a lot of wonderful things out of it” –
Nurse
• “If it’s standard of care, it’s very simple; it’s the standard of care rather than meeting the death squad” – Physician
• “If everybody gets it, it is not singling out any one diagnosis” – Social Worker
• “I think if it were presented as standard of care, it would alleviate a lot of the anxiety” – Nurse
Education Focus on educating families
and providers
• “Hearing the definition of palliative care up front would be different than when you have a setback” – Nurse
• “Palliative care is often translated as end-of-life care” – Social Worker
• “I don’t think a large part of our medical education is geared to address this” – Nurse Practitioner
• “The idea of having a pamphlet in the binder is a good idea” – Nurse Practitioner
Evidence Based Medicine To more feasibly address early
integration of a pediatric
palliative care team
• “You can trial it with an attending who buys into it and is taking new patients” – Nurse Practitioner
• “(If a study is conducted) we have learned something” – Social Worker
Enhanced Communication This would improve
interdisciplinary
documentation and
communication as well as
patients’ understanding of
disease-related information
• “I work nights and am never involved in these kind of discussions, and there is a lot of frustration” – Nurse
• “Fishing out specific information about a conversation that was had or when there’s changes in treatment plans is still a
challenge” – Nurse
• “(documenting important conversations) is an area that we really fall short on” – Nurse
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
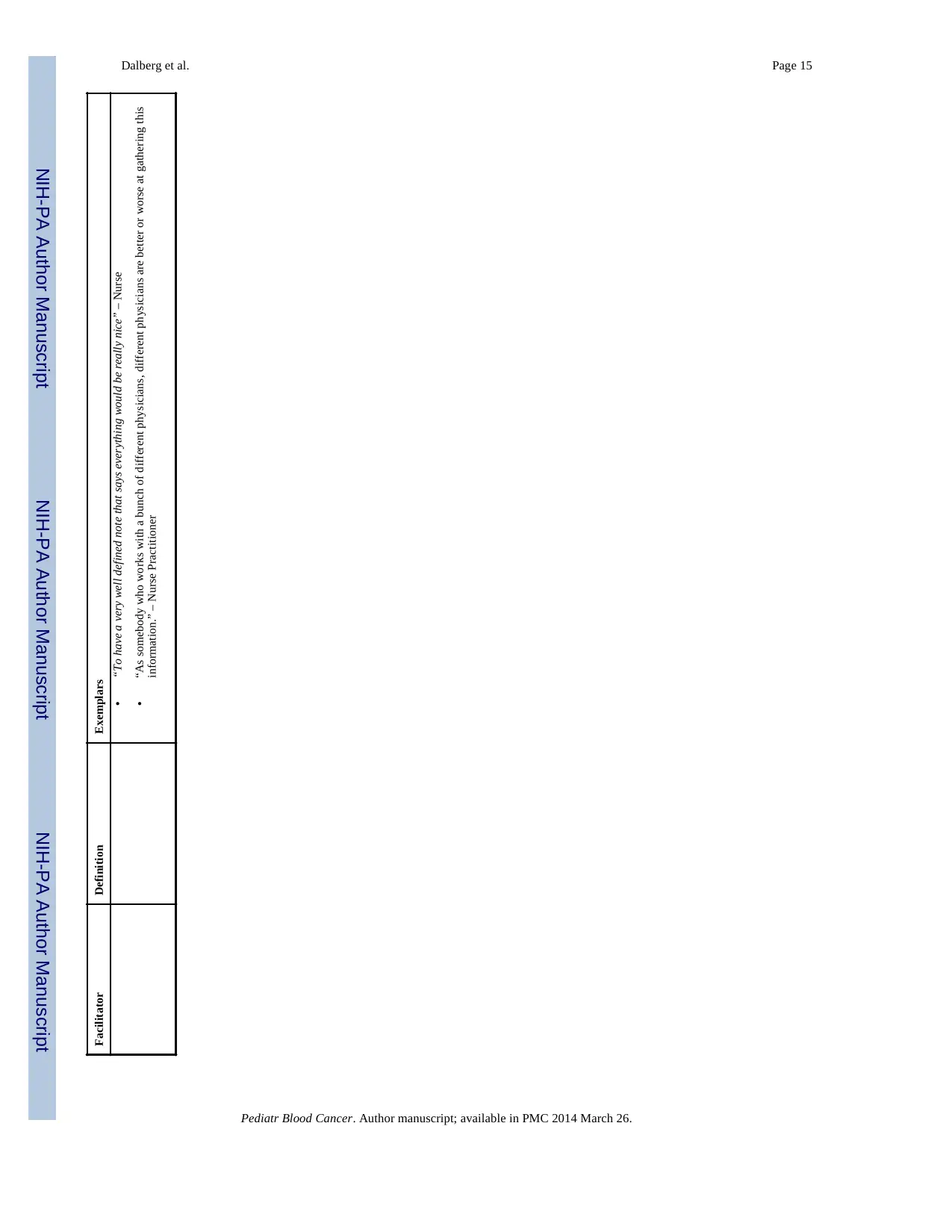
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Dalberg et al. Page 15
Facilitator Definition Exemplars
• “To have a very well defined note that says everything would be really nice” – Nurse
• “As somebody who works with a bunch of different physicians, different physicians are better or worse at gathering this
information.” – Nurse Practitioner
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
Dalberg et al. Page 15
Facilitator Definition Exemplars
• “To have a very well defined note that says everything would be really nice” – Nurse
• “As somebody who works with a bunch of different physicians, different physicians are better or worse at gathering this
information.” – Nurse Practitioner
Pediatr Blood Cancer. Author manuscript; available in PMC 2014 March 26.
1 out of 15
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.