Evaluating the Australian Pharmaceutical Benefits Scheme (PBS)
VerifiedAdded on 2023/06/12
|11
|2474
|139
Report
AI Summary
This report examines the Australian Pharmaceutical Benefits Scheme (PBS), a crucial component of Australian healthcare, focusing on government-subsidized medication for residents. It delves into the increasing costs and consumption trends within the PBS, highlighting a significant 11% exp...
The Australian Pharmaceutical Benefits Scheme and the consumption of medicines in Australia
STUDENT ID:
NAME:
Executive Summary
STUDENT ID:
NAME:
Executive Summary
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

Pharmaceutical Benefits Scheme (PBS) is an important feature for defining Australian health
care. The PBS program provides government subsidized medication to Australian residents. The
program enables Australian residents to pay a set price that is much lower than real price with an
objective of providing affordable, reliable, and timely access to medication. The following report
discusses the Australian Pharmaceutical Benefits Scheme increasingly cost and consumption and
outlines recommendations for optimal performance. The report found that the PBS expenditure
has increased by 11% in 2016-0 2017 financial year. This expenditure was caused by increasing
aging population, newly expensive medicines, over prescription and increased patients’
awareness of Medicare. The report concluded that PBS should maintain it expenditure for
sustainability of the program. The report recommends that PBS to embark on preventive and
healthy lifestyle campaign and offer incentives to manufacturers to reduce amount of medicine
required in the country and cost of newly manufactured medicines.
Table of Contents
Executive Summary.....................................................................................................................................2
care. The PBS program provides government subsidized medication to Australian residents. The
program enables Australian residents to pay a set price that is much lower than real price with an
objective of providing affordable, reliable, and timely access to medication. The following report
discusses the Australian Pharmaceutical Benefits Scheme increasingly cost and consumption and
outlines recommendations for optimal performance. The report found that the PBS expenditure
has increased by 11% in 2016-0 2017 financial year. This expenditure was caused by increasing
aging population, newly expensive medicines, over prescription and increased patients’
awareness of Medicare. The report concluded that PBS should maintain it expenditure for
sustainability of the program. The report recommends that PBS to embark on preventive and
healthy lifestyle campaign and offer incentives to manufacturers to reduce amount of medicine
required in the country and cost of newly manufactured medicines.
Table of Contents
Executive Summary.....................................................................................................................................2
Introduction.................................................................................................................................................4
The Pharmaceutical Benefit Scheme...........................................................................................................4
Cost of Medical Consumption and Prescription..........................................................................................5
Reasons for increased Cost of medical consumption..................................................................................8
Type of medicines Prescribed by PBS..........................................................................................................9
Conclusion...................................................................................................................................................9
Recommendation........................................................................................................................................9
References.................................................................................................................................................11
Introduction
Medicine consumption rate and cost is highest in Australia compared to other developed
countries. The government cost of running Pharmaceutical Benefits Scheme is steadily
increasing every year. An increase in cost of medicine increases the government financial
The Pharmaceutical Benefit Scheme...........................................................................................................4
Cost of Medical Consumption and Prescription..........................................................................................5
Reasons for increased Cost of medical consumption..................................................................................8
Type of medicines Prescribed by PBS..........................................................................................................9
Conclusion...................................................................................................................................................9
Recommendation........................................................................................................................................9
References.................................................................................................................................................11
Introduction
Medicine consumption rate and cost is highest in Australia compared to other developed
countries. The government cost of running Pharmaceutical Benefits Scheme is steadily
increasing every year. An increase in cost of medicine increases the government financial
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
burden. The Australian government through the Department of health has a responsibility to
provide its citizens with affordable, accessible, reliable, and timely medicine (Karnon, Edney, &
Sorich, 2017). The government provides subsidized medicines through Pharmaceutical Benefits
Scheme that lists, distributes, and manages prices and costs of medicines in Australia. The cost
of medicine is an important aspect for the government continued provision of affordable
medicine to Australian. Overwhelming increase in medicine cost is unsustainable and can lead to
government PBS program being stopped as a result of underfunding or lack of funds. The
following report discusses the cost of medicine consumption in Australian, type of medicine
consumed and the problems with Pharmaceutical Benefits Scheme (PBS).
The Pharmaceutical Benefit Scheme
Australian Pharmaceutical Benefits Scheme (PBS) is a program under Australian Government
National Medicine policy whose mandate is to provide affordable, reliable, and timely access to
medicine to Australian citizens (Pearson et al., 2015). The program aims to meet Australians
medications and other related services for optimal health and economic objectives for the
country ("Pharmaceutical Benefits Scheme - Australian Government Department of Human
Services", 2018). The PBS first began in 1948 as a limited scheme for pensioners and 139 life-
saving and diseases preventing medical coverage (Mellish et al., 2015). The PBS program is part
o National Health regulation 1960 and National Health Act 1953. The government uses the PSC
to subsidize medicine cost in the country. The program lists medicines that are then dispensed to
citizens by pharmacists. The PBS services are availed to residents who have Medicare cards or
visitors from countries that have Reciprocal Health Care Agreement (RHCA) with Australia. The
services are also eligible to veterans that have DVA cards (Karnon, Edney, & Sorich, 2017).
The citizens eligible to PBS program pay less to actual medicine price in the market. The co-
payment for concession card is $6.0 as opposed to $39.50 for general public in 2018. The Safety
Net price changed from $378 in 2017 to $384 in 2018 for concession card holders and $1494 in
2017 to $1521.80 in 2018 for other patients (Datta Gupta, & Wilson, 2018). The Australian
government has therefore been able to maintain low cost of medicines by allowing the patients to
pay a small portion while its pay the rest. This has reduced the high medicine burden to
Australians and enabled them to access affordable medicines.
provide its citizens with affordable, accessible, reliable, and timely medicine (Karnon, Edney, &
Sorich, 2017). The government provides subsidized medicines through Pharmaceutical Benefits
Scheme that lists, distributes, and manages prices and costs of medicines in Australia. The cost
of medicine is an important aspect for the government continued provision of affordable
medicine to Australian. Overwhelming increase in medicine cost is unsustainable and can lead to
government PBS program being stopped as a result of underfunding or lack of funds. The
following report discusses the cost of medicine consumption in Australian, type of medicine
consumed and the problems with Pharmaceutical Benefits Scheme (PBS).
The Pharmaceutical Benefit Scheme
Australian Pharmaceutical Benefits Scheme (PBS) is a program under Australian Government
National Medicine policy whose mandate is to provide affordable, reliable, and timely access to
medicine to Australian citizens (Pearson et al., 2015). The program aims to meet Australians
medications and other related services for optimal health and economic objectives for the
country ("Pharmaceutical Benefits Scheme - Australian Government Department of Human
Services", 2018). The PBS first began in 1948 as a limited scheme for pensioners and 139 life-
saving and diseases preventing medical coverage (Mellish et al., 2015). The PBS program is part
o National Health regulation 1960 and National Health Act 1953. The government uses the PSC
to subsidize medicine cost in the country. The program lists medicines that are then dispensed to
citizens by pharmacists. The PBS services are availed to residents who have Medicare cards or
visitors from countries that have Reciprocal Health Care Agreement (RHCA) with Australia. The
services are also eligible to veterans that have DVA cards (Karnon, Edney, & Sorich, 2017).
The citizens eligible to PBS program pay less to actual medicine price in the market. The co-
payment for concession card is $6.0 as opposed to $39.50 for general public in 2018. The Safety
Net price changed from $378 in 2017 to $384 in 2018 for concession card holders and $1494 in
2017 to $1521.80 in 2018 for other patients (Datta Gupta, & Wilson, 2018). The Australian
government has therefore been able to maintain low cost of medicines by allowing the patients to
pay a small portion while its pay the rest. This has reduced the high medicine burden to
Australians and enabled them to access affordable medicines.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
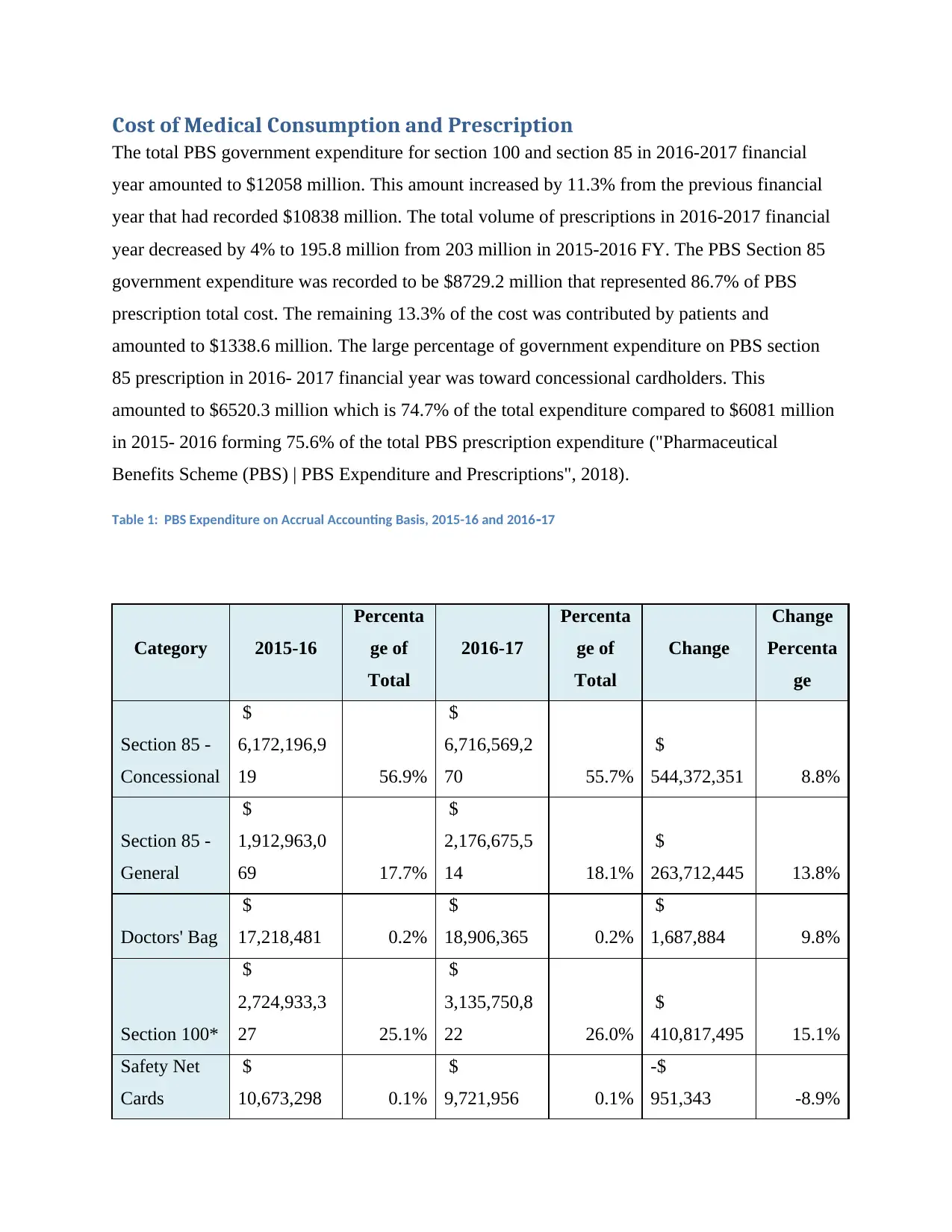
Cost of Medical Consumption and Prescription
The total PBS government expenditure for section 100 and section 85 in 2016-2017 financial
year amounted to $12058 million. This amount increased by 11.3% from the previous financial
year that had recorded $10838 million. The total volume of prescriptions in 2016-2017 financial
year decreased by 4% to 195.8 million from 203 million in 2015-2016 FY. The PBS Section 85
government expenditure was recorded to be $8729.2 million that represented 86.7% of PBS
prescription total cost. The remaining 13.3% of the cost was contributed by patients and
amounted to $1338.6 million. The large percentage of government expenditure on PBS section
85 prescription in 2016- 2017 financial year was toward concessional cardholders. This
amounted to $6520.3 million which is 74.7% of the total expenditure compared to $6081 million
in 2015- 2016 forming 75.6% of the total PBS prescription expenditure ("Pharmaceutical
Benefits Scheme (PBS) | PBS Expenditure and Prescriptions", 2018).
Table 1: PBS Expenditure on Accrual Accounting Basis, 2015-16 and 2016 17‐
Category 2015-16
Percenta
ge of
Total
2016-17
Percenta
ge of
Total
Change
Change
Percenta
ge
Section 85 -
Concessional
$
6,172,196,9
19 56.9%
$
6,716,569,2
70 55.7%
$
544,372,351 8.8%
Section 85 -
General
$
1,912,963,0
69 17.7%
$
2,176,675,5
14 18.1%
$
263,712,445 13.8%
Doctors' Bag
$
17,218,481 0.2%
$
18,906,365 0.2%
$
1,687,884 9.8%
Section 100*
$
2,724,933,3
27 25.1%
$
3,135,750,8
22 26.0%
$
410,817,495 15.1%
Safety Net
Cards
$
10,673,298 0.1%
$
9,721,956 0.1%
-$
951,343 -8.9%
The total PBS government expenditure for section 100 and section 85 in 2016-2017 financial
year amounted to $12058 million. This amount increased by 11.3% from the previous financial
year that had recorded $10838 million. The total volume of prescriptions in 2016-2017 financial
year decreased by 4% to 195.8 million from 203 million in 2015-2016 FY. The PBS Section 85
government expenditure was recorded to be $8729.2 million that represented 86.7% of PBS
prescription total cost. The remaining 13.3% of the cost was contributed by patients and
amounted to $1338.6 million. The large percentage of government expenditure on PBS section
85 prescription in 2016- 2017 financial year was toward concessional cardholders. This
amounted to $6520.3 million which is 74.7% of the total expenditure compared to $6081 million
in 2015- 2016 forming 75.6% of the total PBS prescription expenditure ("Pharmaceutical
Benefits Scheme (PBS) | PBS Expenditure and Prescriptions", 2018).
Table 1: PBS Expenditure on Accrual Accounting Basis, 2015-16 and 2016 17‐
Category 2015-16
Percenta
ge of
Total
2016-17
Percenta
ge of
Total
Change
Change
Percenta
ge
Section 85 -
Concessional
$
6,172,196,9
19 56.9%
$
6,716,569,2
70 55.7%
$
544,372,351 8.8%
Section 85 -
General
$
1,912,963,0
69 17.7%
$
2,176,675,5
14 18.1%
$
263,712,445 13.8%
Doctors' Bag
$
17,218,481 0.2%
$
18,906,365 0.2%
$
1,687,884 9.8%
Section 100*
$
2,724,933,3
27 25.1%
$
3,135,750,8
22 26.0%
$
410,817,495 15.1%
Safety Net
Cards
$
10,673,298 0.1%
$
9,721,956 0.1%
-$
951,343 -8.9%
Total
$
10,837,985,
095 100.0%
$
12,057,623,
927 100.0%
$
1,219,638,8
33 11.3%
Total
Including
Revenue**
$
10,143,081,
604
$
8,790,109,2
29
Average dispensed price as per PBS Section 85 prescription increased to $51.45 as compared to
$46.15 recorded in 2015-2016 financial year. This average dispended price combined the
government cost plus the patient contribution. The government average cost of dispensed price
increased from $39.45 in 2015- 2016 financial year to $44.58 in 2016- 2017 financial year.
Table 2: PBS S85 Prescription Volume for 4 years
2013-14 2014-15 2015-16 2016-17
-
50,000,000
100,000,000
150,000,000
200,000,000
250,000,000
300,000,000
PBS S85 Prescription Volume for Four
Financial Years
Over Co payment‐ Under Co payment‐
Financial Year
Script Volume ('000)
$
10,837,985,
095 100.0%
$
12,057,623,
927 100.0%
$
1,219,638,8
33 11.3%
Total
Including
Revenue**
$
10,143,081,
604
$
8,790,109,2
29
Average dispensed price as per PBS Section 85 prescription increased to $51.45 as compared to
$46.15 recorded in 2015-2016 financial year. This average dispended price combined the
government cost plus the patient contribution. The government average cost of dispensed price
increased from $39.45 in 2015- 2016 financial year to $44.58 in 2016- 2017 financial year.
Table 2: PBS S85 Prescription Volume for 4 years
2013-14 2014-15 2015-16 2016-17
-
50,000,000
100,000,000
150,000,000
200,000,000
250,000,000
300,000,000
PBS S85 Prescription Volume for Four
Financial Years
Over Co payment‐ Under Co payment‐
Financial Year
Script Volume ('000)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
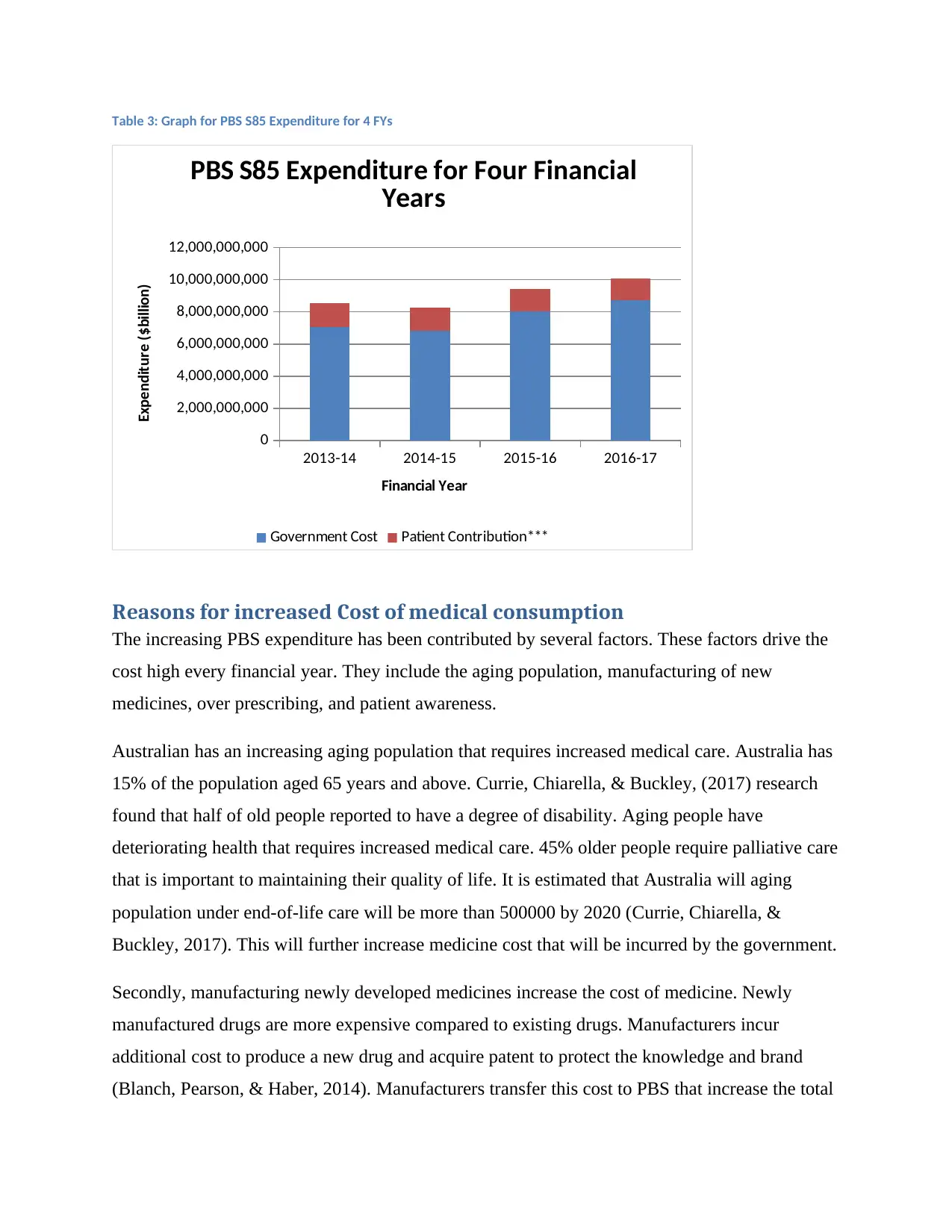
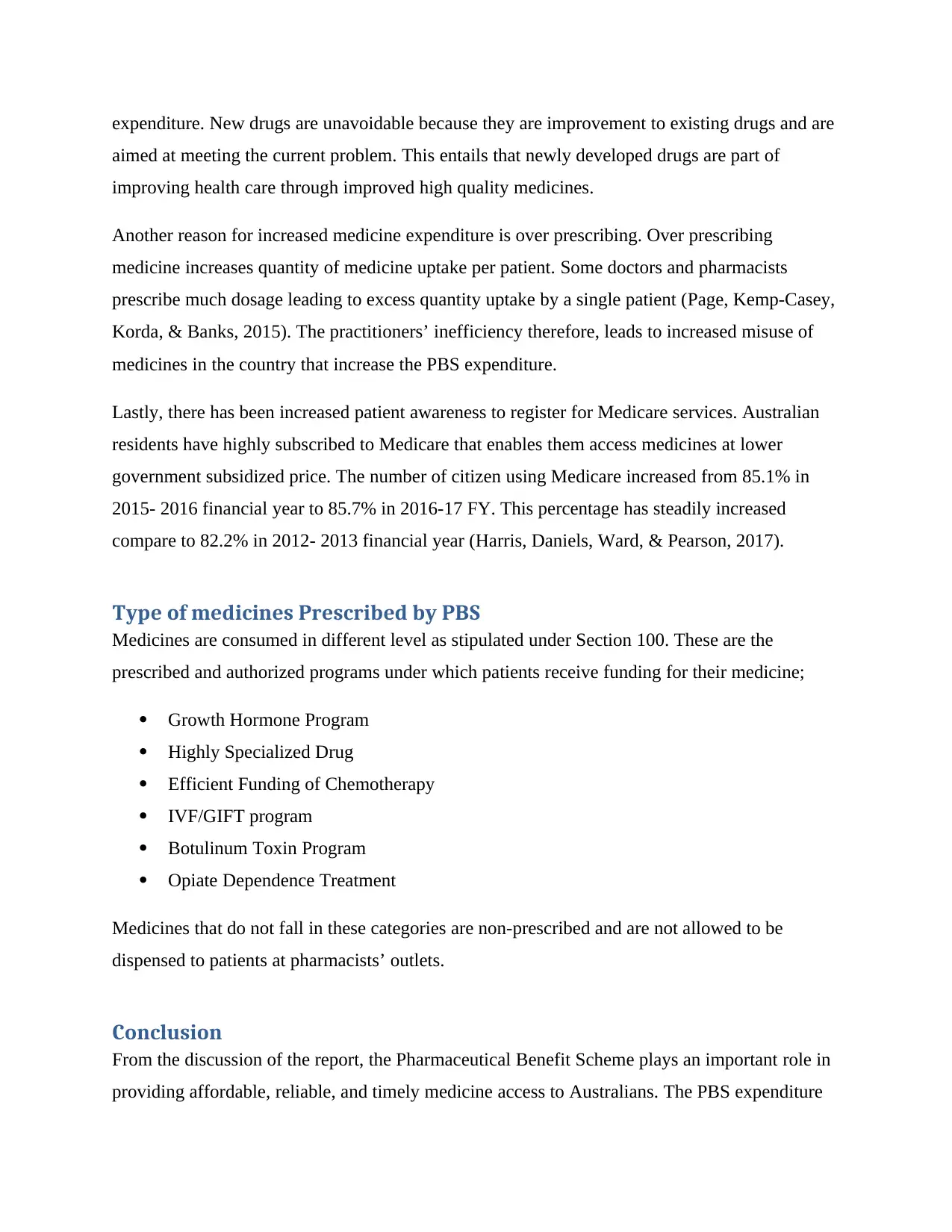
Table 3: Graph for PBS S85 Expenditure for 4 FYs
2013-14 2014-15 2015-16 2016-17
0
2,000,000,000
4,000,000,000
6,000,000,000
8,000,000,000
10,000,000,000
12,000,000,000
PBS S85 Expenditure for Four Financial
Years
Government Cost Patient Contribution***
Financial Year
Expenditure ($billion)
Reasons for increased Cost of medical consumption
The increasing PBS expenditure has been contributed by several factors. These factors drive the
cost high every financial year. They include the aging population, manufacturing of new
medicines, over prescribing, and patient awareness.
Australian has an increasing aging population that requires increased medical care. Australia has
15% of the population aged 65 years and above. Currie, Chiarella, & Buckley, (2017) research
found that half of old people reported to have a degree of disability. Aging people have
deteriorating health that requires increased medical care. 45% older people require palliative care
that is important to maintaining their quality of life. It is estimated that Australia will aging
population under end-of-life care will be more than 500000 by 2020 (Currie, Chiarella, &
Buckley, 2017). This will further increase medicine cost that will be incurred by the government.
Secondly, manufacturing newly developed medicines increase the cost of medicine. Newly
manufactured drugs are more expensive compared to existing drugs. Manufacturers incur
additional cost to produce a new drug and acquire patent to protect the knowledge and brand
(Blanch, Pearson, & Haber, 2014). Manufacturers transfer this cost to PBS that increase the total
2013-14 2014-15 2015-16 2016-17
0
2,000,000,000
4,000,000,000
6,000,000,000
8,000,000,000
10,000,000,000
12,000,000,000
PBS S85 Expenditure for Four Financial
Years
Government Cost Patient Contribution***
Financial Year
Expenditure ($billion)
Reasons for increased Cost of medical consumption
The increasing PBS expenditure has been contributed by several factors. These factors drive the
cost high every financial year. They include the aging population, manufacturing of new
medicines, over prescribing, and patient awareness.
Australian has an increasing aging population that requires increased medical care. Australia has
15% of the population aged 65 years and above. Currie, Chiarella, & Buckley, (2017) research
found that half of old people reported to have a degree of disability. Aging people have
deteriorating health that requires increased medical care. 45% older people require palliative care
that is important to maintaining their quality of life. It is estimated that Australia will aging
population under end-of-life care will be more than 500000 by 2020 (Currie, Chiarella, &
Buckley, 2017). This will further increase medicine cost that will be incurred by the government.
Secondly, manufacturing newly developed medicines increase the cost of medicine. Newly
manufactured drugs are more expensive compared to existing drugs. Manufacturers incur
additional cost to produce a new drug and acquire patent to protect the knowledge and brand
(Blanch, Pearson, & Haber, 2014). Manufacturers transfer this cost to PBS that increase the total
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
expenditure. New drugs are unavoidable because they are improvement to existing drugs and are
aimed at meeting the current problem. This entails that newly developed drugs are part of
improving health care through improved high quality medicines.
Another reason for increased medicine expenditure is over prescribing. Over prescribing
medicine increases quantity of medicine uptake per patient. Some doctors and pharmacists
prescribe much dosage leading to excess quantity uptake by a single patient (Page, Kemp-Casey,
Korda, & Banks, 2015). The practitioners’ inefficiency therefore, leads to increased misuse of
medicines in the country that increase the PBS expenditure.
Lastly, there has been increased patient awareness to register for Medicare services. Australian
residents have highly subscribed to Medicare that enables them access medicines at lower
government subsidized price. The number of citizen using Medicare increased from 85.1% in
2015- 2016 financial year to 85.7% in 2016-17 FY. This percentage has steadily increased
compare to 82.2% in 2012- 2013 financial year (Harris, Daniels, Ward, & Pearson, 2017).
Type of medicines Prescribed by PBS
Medicines are consumed in different level as stipulated under Section 100. These are the
prescribed and authorized programs under which patients receive funding for their medicine;
Growth Hormone Program
Highly Specialized Drug
Efficient Funding of Chemotherapy
IVF/GIFT program
Botulinum Toxin Program
Opiate Dependence Treatment
Medicines that do not fall in these categories are non-prescribed and are not allowed to be
dispensed to patients at pharmacists’ outlets.
Conclusion
From the discussion of the report, the Pharmaceutical Benefit Scheme plays an important role in
providing affordable, reliable, and timely medicine access to Australians. The PBS expenditure
aimed at meeting the current problem. This entails that newly developed drugs are part of
improving health care through improved high quality medicines.
Another reason for increased medicine expenditure is over prescribing. Over prescribing
medicine increases quantity of medicine uptake per patient. Some doctors and pharmacists
prescribe much dosage leading to excess quantity uptake by a single patient (Page, Kemp-Casey,
Korda, & Banks, 2015). The practitioners’ inefficiency therefore, leads to increased misuse of
medicines in the country that increase the PBS expenditure.
Lastly, there has been increased patient awareness to register for Medicare services. Australian
residents have highly subscribed to Medicare that enables them access medicines at lower
government subsidized price. The number of citizen using Medicare increased from 85.1% in
2015- 2016 financial year to 85.7% in 2016-17 FY. This percentage has steadily increased
compare to 82.2% in 2012- 2013 financial year (Harris, Daniels, Ward, & Pearson, 2017).
Type of medicines Prescribed by PBS
Medicines are consumed in different level as stipulated under Section 100. These are the
prescribed and authorized programs under which patients receive funding for their medicine;
Growth Hormone Program
Highly Specialized Drug
Efficient Funding of Chemotherapy
IVF/GIFT program
Botulinum Toxin Program
Opiate Dependence Treatment
Medicines that do not fall in these categories are non-prescribed and are not allowed to be
dispensed to patients at pharmacists’ outlets.
Conclusion
From the discussion of the report, the Pharmaceutical Benefit Scheme plays an important role in
providing affordable, reliable, and timely medicine access to Australians. The PBS expenditure
has been increasing for the past years that have been caused by increasing aging population,
newly expensive medicines, over prescribing and increased patient awareness of Medicare.
There is importance of controlling the medicine expenditure by PBS to enhance sustainability of
the program. The report recommends that PBS at adopt cost effective strategies that maintain or
minimize the cost of providing medicines in Australia. The report therefore concludes that PBS
has an important role in the health sector and should increase efficiency to minimize cost and
make the program sustainable for the government budget and benefits to citizens.
Recommendation
The report recommends the following to Pharmaceutics Benefit Scheme in order to minimize
cost while optimizing health care delivery;
1. Promoting preventive strategies. This will involve preventing serious conditions from
developing leading palliative care. Preventive strategies will include healthy lifestyle
campaigns and early diagnostic of diseases. This will reduce the number of patients under
serious conditions who require large quantities of medicines. Preventive measure will
also shorten time spent in hospitals.
2. Regulating per prescription. PBS should institute regulation on dosage prescription to
avoid overdosing. This will improve efficiency in utilization thereby reducing the
expenditure.
3. Funding manufacturers’ medical research. This recommendation will ensure that newly
developed medicines are not expensive because there are incentives for new medicine
from the government.
newly expensive medicines, over prescribing and increased patient awareness of Medicare.
There is importance of controlling the medicine expenditure by PBS to enhance sustainability of
the program. The report recommends that PBS at adopt cost effective strategies that maintain or
minimize the cost of providing medicines in Australia. The report therefore concludes that PBS
has an important role in the health sector and should increase efficiency to minimize cost and
make the program sustainable for the government budget and benefits to citizens.
Recommendation
The report recommends the following to Pharmaceutics Benefit Scheme in order to minimize
cost while optimizing health care delivery;
1. Promoting preventive strategies. This will involve preventing serious conditions from
developing leading palliative care. Preventive strategies will include healthy lifestyle
campaigns and early diagnostic of diseases. This will reduce the number of patients under
serious conditions who require large quantities of medicines. Preventive measure will
also shorten time spent in hospitals.
2. Regulating per prescription. PBS should institute regulation on dosage prescription to
avoid overdosing. This will improve efficiency in utilization thereby reducing the
expenditure.
3. Funding manufacturers’ medical research. This recommendation will ensure that newly
developed medicines are not expensive because there are incentives for new medicine
from the government.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

References
Blanch, B., Pearson, S. A., & Haber, P. S. (2014). An overview of the patterns of prescription
opioid use, costs and related harms in Australia. British journal of clinical
pharmacology, 78(5), 1159-1166.
Currie, J., Chiarella, M., & Buckley, T. (2017). Privately practising nurse practitioners’ provision
of care subsidised through the Medicare Benefits Schedule and the Pharmaceutical
Benefits Scheme in Australia: results from a national survey. Australian Health
Review.
Datta Gupta, A., & Wilson, D. H. (2018). Botulinum toxin for spasticity: a case for change to the
Pharmaceutical Benefits Scheme. The Medical Journal of Australia, 208(9), 1.
Harris, C. A., Daniels, B., Ward, R. L., & Pearson, S. A. (2017). Retrospective comparison of
Australia's Pharmaceutical Benefits Scheme claims data with prescription data in
HER2-positive early breast cancer patients, 2008-2012. Public Health Research and
Practice, 27(5), 1-9.
Home - Australian Institute of Health and Welfare. (2018). Australian Institute of Health and
Welfare. Retrieved 18 April 2018, from https://www.aihw.gov.au/
Karnon, J., Edney, L., & Sorich, M. (2017). Costs of paying higher prices for equivalent effects
on the Pharmaceutical Benefits Scheme. Australian Health Review, 41(1), 1-6.
Blanch, B., Pearson, S. A., & Haber, P. S. (2014). An overview of the patterns of prescription
opioid use, costs and related harms in Australia. British journal of clinical
pharmacology, 78(5), 1159-1166.
Currie, J., Chiarella, M., & Buckley, T. (2017). Privately practising nurse practitioners’ provision
of care subsidised through the Medicare Benefits Schedule and the Pharmaceutical
Benefits Scheme in Australia: results from a national survey. Australian Health
Review.
Datta Gupta, A., & Wilson, D. H. (2018). Botulinum toxin for spasticity: a case for change to the
Pharmaceutical Benefits Scheme. The Medical Journal of Australia, 208(9), 1.
Harris, C. A., Daniels, B., Ward, R. L., & Pearson, S. A. (2017). Retrospective comparison of
Australia's Pharmaceutical Benefits Scheme claims data with prescription data in
HER2-positive early breast cancer patients, 2008-2012. Public Health Research and
Practice, 27(5), 1-9.
Home - Australian Institute of Health and Welfare. (2018). Australian Institute of Health and
Welfare. Retrieved 18 April 2018, from https://www.aihw.gov.au/
Karnon, J., Edney, L., & Sorich, M. (2017). Costs of paying higher prices for equivalent effects
on the Pharmaceutical Benefits Scheme. Australian Health Review, 41(1), 1-6.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Mellish, L., Karanges, E. A., Litchfield, M. J., Schaffer, A. L., Blanch, B., Daniels, B. J., ... &
Pearson, S. A. (2015). The Australian Pharmaceutical Benefits Scheme data
collection: a practical guide for researchers. BMC research notes, 8(1), 634.
Page, E., Kemp-Casey, A., Korda, R., & Banks, E. (2015). Using Australian Pharmaceutical
Benefits Scheme data for pharmacoepidemiological research: challenges and
approaches. Public Health Res Pract, 25(4), e2541546.
Pearson, S. A., Pesa, N., Langton, J. M., Drew, A., Faedo, M., & Robertson, J. (2015). Studies
using Australia's Pharmaceutical Benefits Scheme data for
pharmacoepidemiological research: a systematic review of the published literature
(1987–2013). Pharmacoepidemiology and drug safety, 24(5), 447-455.
Pharmaceutical Benefits Scheme (PBS) | PBS Expenditure and Prescriptions. (2018).
Pbs.gov.au. Retrieved 18 April 2018, from
http://www.pbs.gov.au/info/statistics/expenditure-prescriptions/pbs-expenditure-
and-prescriptions
Pharmaceutical Benefits Scheme - Australian Government Department of Human Services.
(2018). Humanservices.gov.au. Retrieved 18 April 2018, from
https://www.humanservices.gov.au/individuals/services/medicare/pharmaceutical-
benefits-scheme
Pearson, S. A. (2015). The Australian Pharmaceutical Benefits Scheme data
collection: a practical guide for researchers. BMC research notes, 8(1), 634.
Page, E., Kemp-Casey, A., Korda, R., & Banks, E. (2015). Using Australian Pharmaceutical
Benefits Scheme data for pharmacoepidemiological research: challenges and
approaches. Public Health Res Pract, 25(4), e2541546.
Pearson, S. A., Pesa, N., Langton, J. M., Drew, A., Faedo, M., & Robertson, J. (2015). Studies
using Australia's Pharmaceutical Benefits Scheme data for
pharmacoepidemiological research: a systematic review of the published literature
(1987–2013). Pharmacoepidemiology and drug safety, 24(5), 447-455.
Pharmaceutical Benefits Scheme (PBS) | PBS Expenditure and Prescriptions. (2018).
Pbs.gov.au. Retrieved 18 April 2018, from
http://www.pbs.gov.au/info/statistics/expenditure-prescriptions/pbs-expenditure-
and-prescriptions
Pharmaceutical Benefits Scheme - Australian Government Department of Human Services.
(2018). Humanservices.gov.au. Retrieved 18 April 2018, from
https://www.humanservices.gov.au/individuals/services/medicare/pharmaceutical-
benefits-scheme
1 out of 11
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.