Physical Therapy: Blood Pressure Response to Different Exercises
VerifiedAdded on 2023/04/21
|12
|3717
|88
Homework Assignment
AI Summary
This physical therapy assignment examines the effects of various exercises on blood pressure, including aerobic activity, arm curls, bench presses, and leg extensions. It analyzes blood pressure variations based on exercise intensity, duration, and breathing techniques, such as the Valsalva maneuver. The assignment also outlines a comprehensive exercise program for a hypertensive patient and discusses contra-indicated exercises and biomechanically incorrect techniques observed in sports centers. Furthermore, it addresses the increased risk of knee injuries in women and provides exercises to manage patellar tracking problems. The document also covers risk factors for COPD and recommends appropriate exercise regimens, as well as post-operative exercises following ACL surgery. Finally, it suggests suitable exercises for obese patients with gait abnormalities and knee pain, and highlights a progressive strengthening program for athletes after rotator cuff surgery. Desklib offers a range of similar solved assignments and study resources for students.

[School]
[Course title]
Physical therapy
[Course title]
Physical therapy
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

P a g e | 1
Task-01
The resting blood pressure evaluation revealed the reading attributing to 130/82 mmHg. The
systolic/diastolic blood pressure elevation was recorded as 170/96 mmHg during the aerobic
exercise. However, the resting blood pressure recording after 6 hours of undertaking a
moderate to vigorous aerobic exercise was found to be 128/85 mmHg. The findings
concorded with the evidence-based findings that revealed a reduction in diastolic and systolic
blood pressures to 1.8mmHg and 3.2mmHg within 24-hours of aerobic exercise (Carpio-
Rivera, Moncada-Jiménez, Salazar-Rojas, & Solera-Herrera, 2016). The blood pressure
during the execution of mild to moderate arm curls was recorded as 144/89mmHg. The blood
pressure during rigorous bench press was recorded as 140/90mmHg. The resting blood
pressure recorded after 30 minutes of undertaking a rigorous bench press was 126/82mmHg.
The systolic and diastolic blood pressures incrementally increased after each leg press and leg
extension exercise. The peak blood pressure after the accomplishment of four sets of leg
press/extension intervention was recorded as 174/92mmHg. However, the blood pressure was
gradually reduced and recorded as 120/82mmHg after two hours of the bench press/leg
extension exercises. The elevation of the peak blood pressure during double leg press
intervention was based on the acquisition of the concentric phase. This concentric phase
ended after the maximal extension of legs, thereby leading to a decline in the systolic and
diastolic blood pressure values (Gotshall, Gootman, Byrnes, Fleck, & Valovich, 1999). The
blood pressure again experienced a gradual elevation after the initiation of the eccentric
phase.
The stretching extremity exercises elevated the muscle tension that facilitates the
enhancement of the systolic and diastolic blood pressures. This blood pressure elevation
continued until the acquisition of muscle tension failure. The resultant development of fatigue
and muscle relaxation facilitated the decrease in blood pressure pattern. The recorded blood
pressure variations after arm curls, bench press, leg press, and leg extension interventions
affirm the influence of exercise intensity and duration on the blood pressure outcome. The
systolic blood pressure (SBP) initially decreases for a duration of 20 seconds under the
impact of leg press exercise. However, the acquisition of the peak SBP values occurs until the
accomplishment of leg press exercise (de-Sousa et al., 2014). The sequential execution of the
exercise sets (of both extremities) effectively induce the post-exercise hypotensive response.
The exercise-based reduction in blood pressure warrants the utilization of 5-sets of each
exercise by the normotensive individual (Figueiredo, et al., 2015). The breath holding
intervention (or Valsalva maneuver) during the knee extension or single arm curl leads to the
Task-01
The resting blood pressure evaluation revealed the reading attributing to 130/82 mmHg. The
systolic/diastolic blood pressure elevation was recorded as 170/96 mmHg during the aerobic
exercise. However, the resting blood pressure recording after 6 hours of undertaking a
moderate to vigorous aerobic exercise was found to be 128/85 mmHg. The findings
concorded with the evidence-based findings that revealed a reduction in diastolic and systolic
blood pressures to 1.8mmHg and 3.2mmHg within 24-hours of aerobic exercise (Carpio-
Rivera, Moncada-Jiménez, Salazar-Rojas, & Solera-Herrera, 2016). The blood pressure
during the execution of mild to moderate arm curls was recorded as 144/89mmHg. The blood
pressure during rigorous bench press was recorded as 140/90mmHg. The resting blood
pressure recorded after 30 minutes of undertaking a rigorous bench press was 126/82mmHg.
The systolic and diastolic blood pressures incrementally increased after each leg press and leg
extension exercise. The peak blood pressure after the accomplishment of four sets of leg
press/extension intervention was recorded as 174/92mmHg. However, the blood pressure was
gradually reduced and recorded as 120/82mmHg after two hours of the bench press/leg
extension exercises. The elevation of the peak blood pressure during double leg press
intervention was based on the acquisition of the concentric phase. This concentric phase
ended after the maximal extension of legs, thereby leading to a decline in the systolic and
diastolic blood pressure values (Gotshall, Gootman, Byrnes, Fleck, & Valovich, 1999). The
blood pressure again experienced a gradual elevation after the initiation of the eccentric
phase.
The stretching extremity exercises elevated the muscle tension that facilitates the
enhancement of the systolic and diastolic blood pressures. This blood pressure elevation
continued until the acquisition of muscle tension failure. The resultant development of fatigue
and muscle relaxation facilitated the decrease in blood pressure pattern. The recorded blood
pressure variations after arm curls, bench press, leg press, and leg extension interventions
affirm the influence of exercise intensity and duration on the blood pressure outcome. The
systolic blood pressure (SBP) initially decreases for a duration of 20 seconds under the
impact of leg press exercise. However, the acquisition of the peak SBP values occurs until the
accomplishment of leg press exercise (de-Sousa et al., 2014). The sequential execution of the
exercise sets (of both extremities) effectively induce the post-exercise hypotensive response.
The exercise-based reduction in blood pressure warrants the utilization of 5-sets of each
exercise by the normotensive individual (Figueiredo, et al., 2015). The breath holding
intervention (or Valsalva maneuver) during the knee extension or single arm curl leads to the
P a g e | 2
generation of the elevated blood pressure outcomes. Deep inhalation during the concentric
exercise substantially elevates the blood pressure. Eventually, the Valsalva maneuver during
the resistance exercise aggravates the blood pressure outcome (Linsenbardt, Thomas, &
Madsen, 1992). Breath slowdown or holding preserves the autonomic function and elevates
the heart rate variability (Russo, Santarelli, & O’Rourke, 2017). Accordingly, in the
presented scenario the breath holding intervention resulted in the blood pressure elevation
(i.e. 140/89mmHg). The supine position substantially elevates the cardiac pressure as
compared to the seated/inverted leg press. Similarly, the inverted leg press intervention
elevates the systolic and diastolic blood pressures in comparison to the seated exercise
intervention. However, the blood pressures drop down after the acquisition of the resting
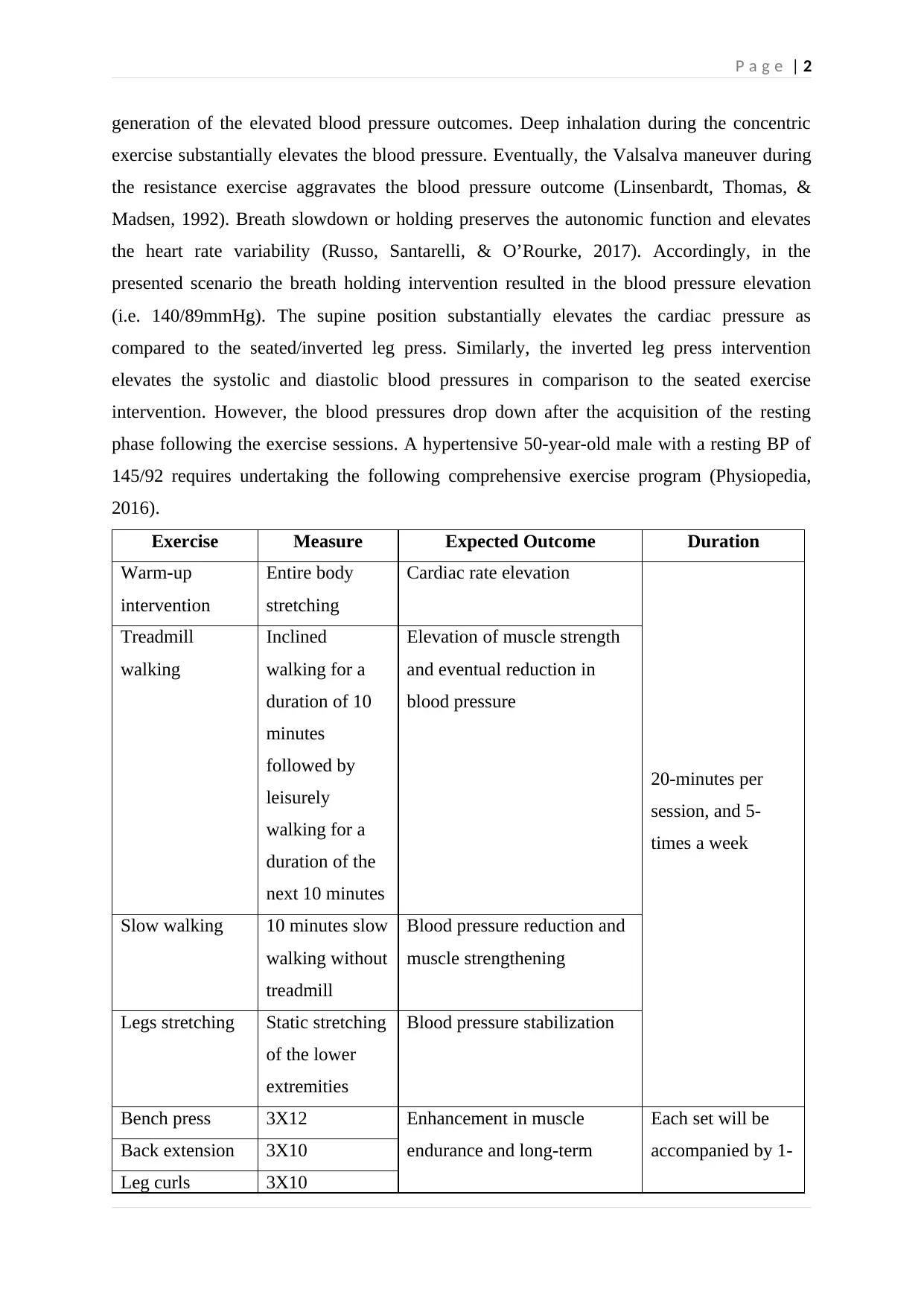
phase following the exercise sessions. A hypertensive 50-year-old male with a resting BP of
145/92 requires undertaking the following comprehensive exercise program (Physiopedia,
2016).
Exercise Measure Expected Outcome Duration
Warm-up
intervention
Entire body
stretching
Cardiac rate elevation
20-minutes per
session, and 5-
times a week
Treadmill
walking
Inclined
walking for a
duration of 10
minutes
followed by
leisurely
walking for a
duration of the
next 10 minutes
Elevation of muscle strength
and eventual reduction in
blood pressure
Slow walking 10 minutes slow
walking without
treadmill
Blood pressure reduction and
muscle strengthening
Legs stretching Static stretching
of the lower
extremities
Blood pressure stabilization
Bench press 3X12 Enhancement in muscle
endurance and long-term
Each set will be
accompanied by 1-Back extension 3X10
Leg curls 3X10
generation of the elevated blood pressure outcomes. Deep inhalation during the concentric
exercise substantially elevates the blood pressure. Eventually, the Valsalva maneuver during
the resistance exercise aggravates the blood pressure outcome (Linsenbardt, Thomas, &
Madsen, 1992). Breath slowdown or holding preserves the autonomic function and elevates
the heart rate variability (Russo, Santarelli, & O’Rourke, 2017). Accordingly, in the
presented scenario the breath holding intervention resulted in the blood pressure elevation
(i.e. 140/89mmHg). The supine position substantially elevates the cardiac pressure as
compared to the seated/inverted leg press. Similarly, the inverted leg press intervention
elevates the systolic and diastolic blood pressures in comparison to the seated exercise
intervention. However, the blood pressures drop down after the acquisition of the resting
phase following the exercise sessions. A hypertensive 50-year-old male with a resting BP of
145/92 requires undertaking the following comprehensive exercise program (Physiopedia,
2016).
Exercise Measure Expected Outcome Duration
Warm-up
intervention
Entire body
stretching
Cardiac rate elevation
20-minutes per
session, and 5-
times a week
Treadmill
walking
Inclined
walking for a
duration of 10
minutes
followed by
leisurely
walking for a
duration of the
next 10 minutes
Elevation of muscle strength
and eventual reduction in
blood pressure
Slow walking 10 minutes slow
walking without
treadmill
Blood pressure reduction and
muscle strengthening
Legs stretching Static stretching
of the lower
extremities
Blood pressure stabilization
Bench press 3X12 Enhancement in muscle
endurance and long-term
Each set will be
accompanied by 1-Back extension 3X10
Leg curls 3X10
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
P a g e | 3
control/reduction/maintenance
of the blood pressure
minutes of rest and
the entire
intervention will
be undertaken
twice a week
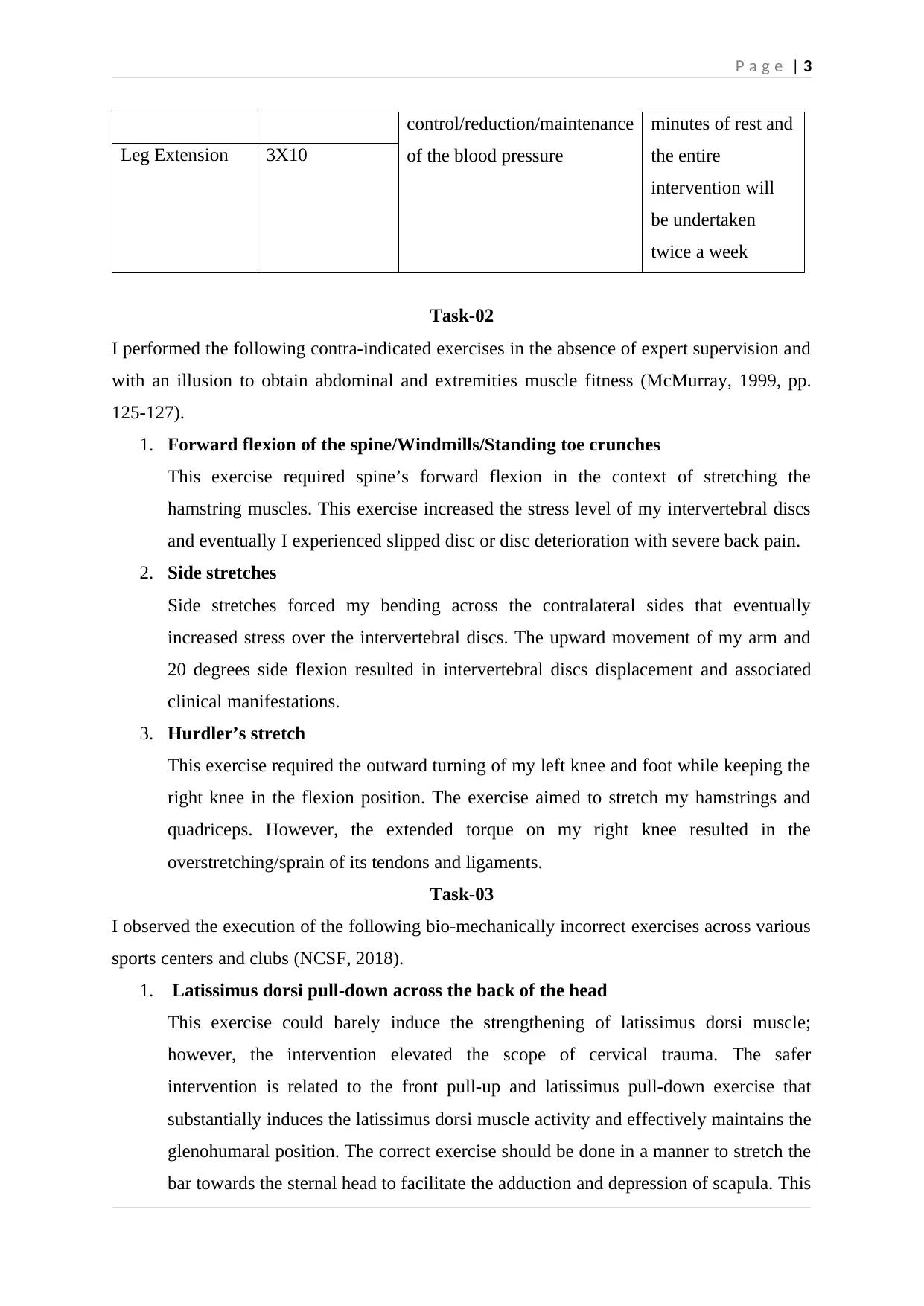
Leg Extension 3X10
Task-02
I performed the following contra-indicated exercises in the absence of expert supervision and
with an illusion to obtain abdominal and extremities muscle fitness (McMurray, 1999, pp.
125-127).
1. Forward flexion of the spine/Windmills/Standing toe crunches
This exercise required spine’s forward flexion in the context of stretching the
hamstring muscles. This exercise increased the stress level of my intervertebral discs
and eventually I experienced slipped disc or disc deterioration with severe back pain.
2. Side stretches
Side stretches forced my bending across the contralateral sides that eventually
increased stress over the intervertebral discs. The upward movement of my arm and
20 degrees side flexion resulted in intervertebral discs displacement and associated
clinical manifestations.
3. Hurdler’s stretch
This exercise required the outward turning of my left knee and foot while keeping the
right knee in the flexion position. The exercise aimed to stretch my hamstrings and
quadriceps. However, the extended torque on my right knee resulted in the
overstretching/sprain of its tendons and ligaments.
Task-03
I observed the execution of the following bio-mechanically incorrect exercises across various
sports centers and clubs (NCSF, 2018).
1. Latissimus dorsi pull-down across the back of the head
This exercise could barely induce the strengthening of latissimus dorsi muscle;
however, the intervention elevated the scope of cervical trauma. The safer
intervention is related to the front pull-up and latissimus pull-down exercise that
substantially induces the latissimus dorsi muscle activity and effectively maintains the
glenohumaral position. The correct exercise should be done in a manner to stretch the
bar towards the sternal head to facilitate the adduction and depression of scapula. This
control/reduction/maintenance
of the blood pressure
minutes of rest and
the entire
intervention will
be undertaken
twice a week
Leg Extension 3X10
Task-02
I performed the following contra-indicated exercises in the absence of expert supervision and
with an illusion to obtain abdominal and extremities muscle fitness (McMurray, 1999, pp.
125-127).
1. Forward flexion of the spine/Windmills/Standing toe crunches
This exercise required spine’s forward flexion in the context of stretching the
hamstring muscles. This exercise increased the stress level of my intervertebral discs
and eventually I experienced slipped disc or disc deterioration with severe back pain.
2. Side stretches
Side stretches forced my bending across the contralateral sides that eventually
increased stress over the intervertebral discs. The upward movement of my arm and
20 degrees side flexion resulted in intervertebral discs displacement and associated
clinical manifestations.
3. Hurdler’s stretch
This exercise required the outward turning of my left knee and foot while keeping the
right knee in the flexion position. The exercise aimed to stretch my hamstrings and
quadriceps. However, the extended torque on my right knee resulted in the
overstretching/sprain of its tendons and ligaments.
Task-03
I observed the execution of the following bio-mechanically incorrect exercises across various
sports centers and clubs (NCSF, 2018).
1. Latissimus dorsi pull-down across the back of the head
This exercise could barely induce the strengthening of latissimus dorsi muscle;
however, the intervention elevated the scope of cervical trauma. The safer
intervention is related to the front pull-up and latissimus pull-down exercise that
substantially induces the latissimus dorsi muscle activity and effectively maintains the
glenohumaral position. The correct exercise should be done in a manner to stretch the
bar towards the sternal head to facilitate the adduction and depression of scapula. This
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

P a g e | 4
correction will induce the neutral spinal position while reducing the risk of hip angle
changes and premature flexion of the arm.
2. Anchored Sit-ups
This exercise increases the risk of disc decompression through elevated hip flexor
activity. This could result in the development of severe lumbar spine pain. The feet
anchoring increases the pull of hip flexors across the spine and hips. This eventually
increases the risk of sprain across the connective tissues. Therefore, abdominal curl-
ups are highly recommended over anchored sit-ups because of their capacity to stress
the rectus abdominis in a resistive manner. This intervention reduces the risk of low
back pain and disc compression.
Task-04
Women experience greater risk of knee injuries under the impact of estrogen hormone that
weakens their anterior cruciate ligament (University_of_Texas, 2018). A greater frequency of
knee injury episodes is recorded for women during their menstrual cycle that induces
elevated production of estrogen. The elevated Q-angle (i.e. patella mid-point angle formed
between tibial tubercle and anterior superior iliac spine) in females exerts greater pressure
across their knee joints an also increases the extent of foot pronation. Q-angle is indicative of
the frontal plane alignment in females (Nguyen, Boling, Levine, & Shultz, 2009). The greater
width of this alignment in females substantially increases their risk of foot and knee injuries.
Patellar tracking problems occur after the outside shifting of the patella (Blahd, Thompson,
Husney, & McMahon, 2018). This abnormal shifting occurs due to thigh muscle weakness,
tightening of leg muscles, twisting knee activities, and knee trauma. These problems result in
the development of knee joint pain, popping sensation across the knee joint, and knee
buckling. The knee joint eventually fails to bear the body weight. The following exercises
assist in controlling the patella tracking problems and associated signs/symptoms (Sueki &
Brechter, 2010, p. 591) (Peng & Song, 2015).
1. Leg press training
2. Hip adduction
3. Quadricep contraction/strengthening
4. Patellar taping
5. External rotation and hip abduction strengthening
Task-05
The following conditions increase the risk of COPD and associated clinical manifestations
(Qureshi, Sharafkhaneh, & Hanania, 2014).
correction will induce the neutral spinal position while reducing the risk of hip angle
changes and premature flexion of the arm.
2. Anchored Sit-ups
This exercise increases the risk of disc decompression through elevated hip flexor
activity. This could result in the development of severe lumbar spine pain. The feet
anchoring increases the pull of hip flexors across the spine and hips. This eventually
increases the risk of sprain across the connective tissues. Therefore, abdominal curl-
ups are highly recommended over anchored sit-ups because of their capacity to stress
the rectus abdominis in a resistive manner. This intervention reduces the risk of low
back pain and disc compression.
Task-04
Women experience greater risk of knee injuries under the impact of estrogen hormone that
weakens their anterior cruciate ligament (University_of_Texas, 2018). A greater frequency of
knee injury episodes is recorded for women during their menstrual cycle that induces
elevated production of estrogen. The elevated Q-angle (i.e. patella mid-point angle formed
between tibial tubercle and anterior superior iliac spine) in females exerts greater pressure
across their knee joints an also increases the extent of foot pronation. Q-angle is indicative of
the frontal plane alignment in females (Nguyen, Boling, Levine, & Shultz, 2009). The greater
width of this alignment in females substantially increases their risk of foot and knee injuries.
Patellar tracking problems occur after the outside shifting of the patella (Blahd, Thompson,
Husney, & McMahon, 2018). This abnormal shifting occurs due to thigh muscle weakness,
tightening of leg muscles, twisting knee activities, and knee trauma. These problems result in
the development of knee joint pain, popping sensation across the knee joint, and knee
buckling. The knee joint eventually fails to bear the body weight. The following exercises
assist in controlling the patella tracking problems and associated signs/symptoms (Sueki &
Brechter, 2010, p. 591) (Peng & Song, 2015).
1. Leg press training
2. Hip adduction
3. Quadricep contraction/strengthening
4. Patellar taping
5. External rotation and hip abduction strengthening
Task-05
The following conditions increase the risk of COPD and associated clinical manifestations
(Qureshi, Sharafkhaneh, & Hanania, 2014).

P a g e | 5
1. Steroid/antibiotic prescription
2. Consistent and prolonged wheezing/a productive cough
3. Production of chronic bronchial mucus
4. Prolonged airway obstruction
5. Bacterial colonization
6. Cardiovascular comorbidity
7. Asthma exacerbations and previous use of COPD drugs
The client must take into consideration the heat sensitivity profile of the concerned steroids
and antibiotics while undertaking the exercise regimen. The COPD drugs exhibit the capacity
of improving the ventilation capacity of the concerned patient. Therefore, the exercise
capacity of the COPD patient reciprocates with the positive effects of the treatment drugs on
the respiratory functionality (Calverley, 2018). The moderate level COPD patient should
undertake exercise sessions for a duration of 20-30 minutes (Cleveland_Clinic, 2017). The
exercise sessions based on stretching, aerobics, and strengthening interventions should be
repeated 3-4 times a week to improve the fitness level. The comprehensive fitness program
for the COPD patients is mentioned below (Furlanetto, Pinto, Anna, Hernandes, & Pitta,
2016).
Age Exercise Duration Exercise Intensity
65 years or above 30 minutes Greater than 3.2 Mets
Less than 65 years 30 minutes Greater than 4 Mets
Irrespective of age 30 Minutes Greater than 3 Mets
Age 40 years or less 80 Minutes Greater than 3 Mets
Task-06
The following exercises need to be undertaken during the postoperative period after ACL
surgery. The use or knee brace before and after exercise is also recommended to improve the
mechanical-neurosensory anterior cruciate ligament function (Nyland et al., 2016).
Post-ACL Surgery Physical Therapy Rehab Program (CHOC, 2018)
Exercise Measure Duration
Towel Calf Stretch (Long Sitting
Position)
Holding of the foot through
the towel ends
Inward pulling of towel
towards oneself
30 seconds
(Two sets)
Hamstring Stretch (Supine Position) Placement of towel across 30 seconds
1. Steroid/antibiotic prescription
2. Consistent and prolonged wheezing/a productive cough
3. Production of chronic bronchial mucus
4. Prolonged airway obstruction
5. Bacterial colonization
6. Cardiovascular comorbidity
7. Asthma exacerbations and previous use of COPD drugs
The client must take into consideration the heat sensitivity profile of the concerned steroids
and antibiotics while undertaking the exercise regimen. The COPD drugs exhibit the capacity
of improving the ventilation capacity of the concerned patient. Therefore, the exercise
capacity of the COPD patient reciprocates with the positive effects of the treatment drugs on
the respiratory functionality (Calverley, 2018). The moderate level COPD patient should
undertake exercise sessions for a duration of 20-30 minutes (Cleveland_Clinic, 2017). The
exercise sessions based on stretching, aerobics, and strengthening interventions should be
repeated 3-4 times a week to improve the fitness level. The comprehensive fitness program
for the COPD patients is mentioned below (Furlanetto, Pinto, Anna, Hernandes, & Pitta,
2016).
Age Exercise Duration Exercise Intensity
65 years or above 30 minutes Greater than 3.2 Mets
Less than 65 years 30 minutes Greater than 4 Mets
Irrespective of age 30 Minutes Greater than 3 Mets
Age 40 years or less 80 Minutes Greater than 3 Mets
Task-06
The following exercises need to be undertaken during the postoperative period after ACL
surgery. The use or knee brace before and after exercise is also recommended to improve the
mechanical-neurosensory anterior cruciate ligament function (Nyland et al., 2016).
Post-ACL Surgery Physical Therapy Rehab Program (CHOC, 2018)
Exercise Measure Duration
Towel Calf Stretch (Long Sitting
Position)
Holding of the foot through
the towel ends
Inward pulling of towel
towards oneself
30 seconds
(Two sets)
Hamstring Stretch (Supine Position) Placement of towel across 30 seconds
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
P a g e | 6
the foot in sitting position
Upward raising of leg with
the support of towel
(Two sets)
Quadriceps Exercise Placement of towel beneath
the knee
Stretching of leg muscles
Holding the leg in same
position
3-5
seconds
(10
repetitions,
2 sets)
Ankle Pumps Body placement in the
supine position
Upward and downward
movement of ankles and toes
10
repetitions
and 2 sets
Heel Slides Placement of towel across
the foot in sitting position
Towel’s backward pulling to
bend the knee
3-5
seconds
(10
repetitions,
2 sets)
Hip Extension (Prone Position) An upward lifting of the leg
while straightening the knee
in prone position
10
repetitions,
2 sets
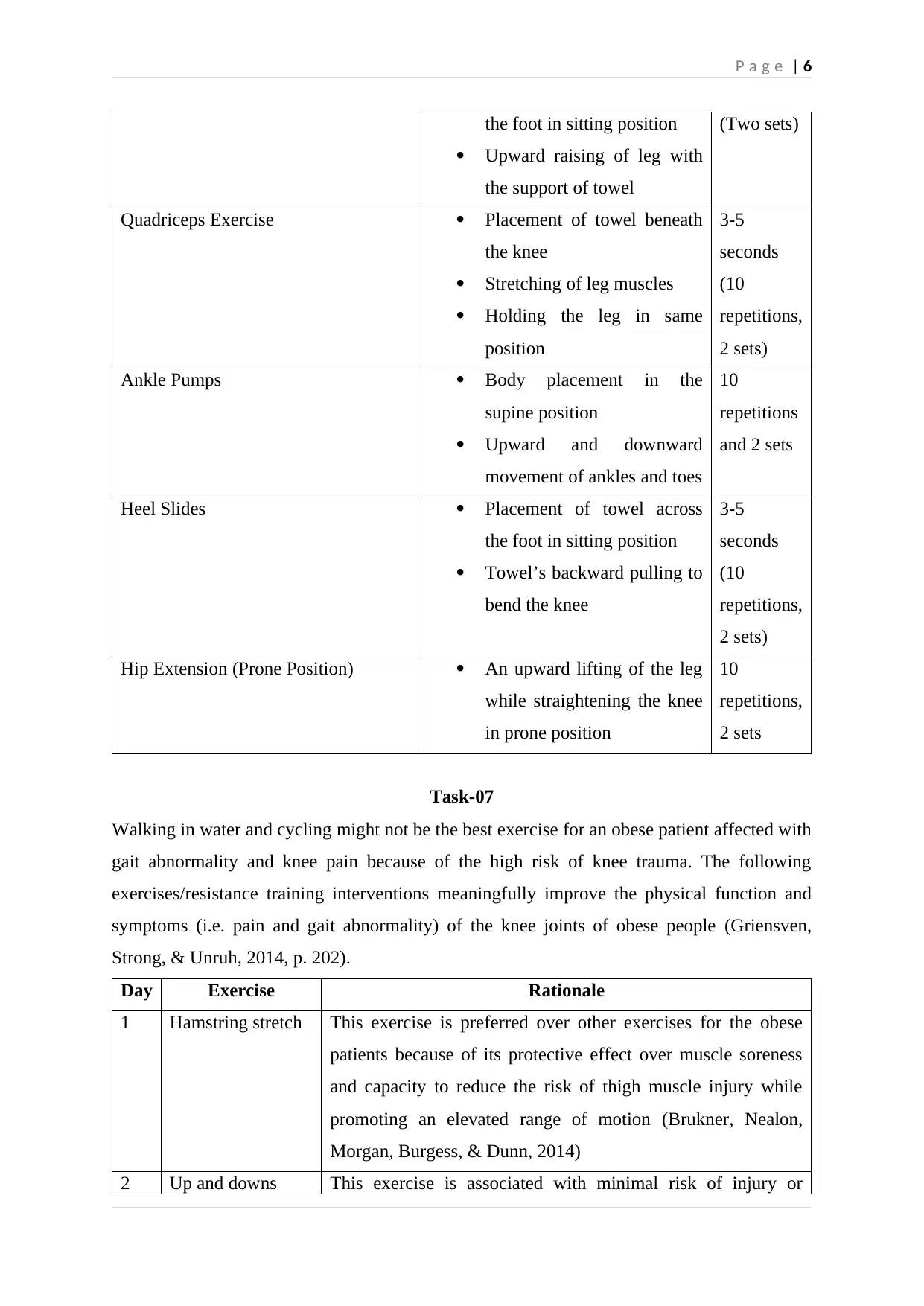
Task-07
Walking in water and cycling might not be the best exercise for an obese patient affected with
gait abnormality and knee pain because of the high risk of knee trauma. The following
exercises/resistance training interventions meaningfully improve the physical function and
symptoms (i.e. pain and gait abnormality) of the knee joints of obese people (Griensven,
Strong, & Unruh, 2014, p. 202).
Day Exercise Rationale
1 Hamstring stretch This exercise is preferred over other exercises for the obese
patients because of its protective effect over muscle soreness
and capacity to reduce the risk of thigh muscle injury while
promoting an elevated range of motion (Brukner, Nealon,
Morgan, Burgess, & Dunn, 2014)
2 Up and downs This exercise is associated with minimal risk of injury or
the foot in sitting position
Upward raising of leg with
the support of towel
(Two sets)
Quadriceps Exercise Placement of towel beneath
the knee
Stretching of leg muscles
Holding the leg in same
position
3-5
seconds
(10
repetitions,
2 sets)
Ankle Pumps Body placement in the
supine position
Upward and downward
movement of ankles and toes
10
repetitions
and 2 sets
Heel Slides Placement of towel across
the foot in sitting position
Towel’s backward pulling to
bend the knee
3-5
seconds
(10
repetitions,
2 sets)
Hip Extension (Prone Position) An upward lifting of the leg
while straightening the knee
in prone position
10
repetitions,
2 sets
Task-07
Walking in water and cycling might not be the best exercise for an obese patient affected with
gait abnormality and knee pain because of the high risk of knee trauma. The following
exercises/resistance training interventions meaningfully improve the physical function and
symptoms (i.e. pain and gait abnormality) of the knee joints of obese people (Griensven,
Strong, & Unruh, 2014, p. 202).
Day Exercise Rationale
1 Hamstring stretch This exercise is preferred over other exercises for the obese
patients because of its protective effect over muscle soreness
and capacity to reduce the risk of thigh muscle injury while
promoting an elevated range of motion (Brukner, Nealon,
Morgan, Burgess, & Dunn, 2014)
2 Up and downs This exercise is associated with minimal risk of injury or
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

P a g e | 7
sprain and improves the endurance of hips flexors. Therefore,
this exercise is preferred over other interventions
3 Calf raises This exercise improves the endurance of soleus and
gastrocnemius muscles and improves gait abnormality. Hence,
this is preferred over other forms of exercise
4 Calf stretch This exercise prevents ankle injury while improving the
endurance and stability of gastrocnemius muscle
5 Hamstring curl This exercise improves knee’s external and internal rotations
while strengthening the semimembranosus, semitendinosus,
and biceps femoris muscles. This intervention stretches the
hip/leg muscles while minimizing the risk of sprain for the
obese patient
Task-08
A progressive strengthening program is highly recommended for an athlete after undergoing
rotator cuff surgery. This program is based on joint mobilization though internal shoulder
rotation to effectively improve the passive range of motion of the glenohumeral joint. The
program also utilizes intramuscular needling to enhance the range of motion of the surgically
intervened shoulder. Furthermore, the progressive strengthening program is based on the
following interventions (Weiss, Wang, Hendel, Buzzerio, & Rodeo, 2018).
ROM Exercise Schedule Outcome
Wall clock exercise
10 repetitions and 4 sets Enhancement of the scapular
stabilityFoam roller exercise
Sidelying external rotation
exercise
15 repetitions and 2 sets Enhancement of the strength
and endurance of teres
minor and infraspinatus
Plyometric chest pass 12 repetitions and 4 sets Enhancement of rotator
cuff’s endurance,
kinesthesia, and
proprioception
Other exercises (based on the published training format) for improving the rotator cuff
strength are mentioned below (v-d-Meijden et al., 2012).
sprain and improves the endurance of hips flexors. Therefore,
this exercise is preferred over other interventions
3 Calf raises This exercise improves the endurance of soleus and
gastrocnemius muscles and improves gait abnormality. Hence,
this is preferred over other forms of exercise
4 Calf stretch This exercise prevents ankle injury while improving the
endurance and stability of gastrocnemius muscle
5 Hamstring curl This exercise improves knee’s external and internal rotations
while strengthening the semimembranosus, semitendinosus,
and biceps femoris muscles. This intervention stretches the
hip/leg muscles while minimizing the risk of sprain for the
obese patient
Task-08
A progressive strengthening program is highly recommended for an athlete after undergoing
rotator cuff surgery. This program is based on joint mobilization though internal shoulder
rotation to effectively improve the passive range of motion of the glenohumeral joint. The
program also utilizes intramuscular needling to enhance the range of motion of the surgically
intervened shoulder. Furthermore, the progressive strengthening program is based on the
following interventions (Weiss, Wang, Hendel, Buzzerio, & Rodeo, 2018).
ROM Exercise Schedule Outcome
Wall clock exercise
10 repetitions and 4 sets Enhancement of the scapular
stabilityFoam roller exercise
Sidelying external rotation
exercise
15 repetitions and 2 sets Enhancement of the strength
and endurance of teres
minor and infraspinatus
Plyometric chest pass 12 repetitions and 4 sets Enhancement of rotator
cuff’s endurance,
kinesthesia, and
proprioception
Other exercises (based on the published training format) for improving the rotator cuff
strength are mentioned below (v-d-Meijden et al., 2012).

P a g e | 8
1. Gentle joint oscillations (arm abduction/short-arm traction)
2. Forward arm flexion for passive range of motion
3. Isolated scapular protraction and depression
4. Active assisted ROM exercise for improving the internal shoulder rotation
5. Salute exercise
6. Open chain proprioceptive exercise
7. Bear hug test
8. Standing sports cord row exercise
9. Conventional biceps curl exercises
10. Triceps extension exercises
Task-09
Outcomes management is based on the administration of rehabilitation and health
improvement measures to improve the health care quality of the treated patient (Durak &
Palmeiri-Jr, 1998). Various outcomes measures focus on enhancing the fitness, health and
wellness outcomes various patients affected with chronic disease conditions. For example,
exercise interventions improve the body mass index while inducing fat loss in the treated
patients. Similarly, stress management helps in improving the range of motion, overall
fitness, and activities of daily living of the chronically ill or surgically intervened patients.
The mandatory outcomes program extends significant implications across trauma
management, pain management, sleep medicine, and other comprehensive health care
specialties (Alkhenizan & Shaw, 2011). These outcomes reveal the positive influence of
mandatory outcomes program on prospective wellness programs and rehabilitation
interventions. The mandatory outcome program offers several professional advantages. The
program proves to be cost effective since it effectively minimizes the use of significant
physician/hospital resources while enhancing the rehabilitation/wellness outcomes. For
example, the use of mandatory physiotherapy program during the postoperative period will
not only facilitate patients’ recovery tenure but also reduce the length of their stay in the
treatment facility, thereby saving the health care expenses to a considerable extent.
1. Gentle joint oscillations (arm abduction/short-arm traction)
2. Forward arm flexion for passive range of motion
3. Isolated scapular protraction and depression
4. Active assisted ROM exercise for improving the internal shoulder rotation
5. Salute exercise
6. Open chain proprioceptive exercise
7. Bear hug test
8. Standing sports cord row exercise
9. Conventional biceps curl exercises
10. Triceps extension exercises
Task-09
Outcomes management is based on the administration of rehabilitation and health
improvement measures to improve the health care quality of the treated patient (Durak &
Palmeiri-Jr, 1998). Various outcomes measures focus on enhancing the fitness, health and
wellness outcomes various patients affected with chronic disease conditions. For example,
exercise interventions improve the body mass index while inducing fat loss in the treated
patients. Similarly, stress management helps in improving the range of motion, overall
fitness, and activities of daily living of the chronically ill or surgically intervened patients.
The mandatory outcomes program extends significant implications across trauma
management, pain management, sleep medicine, and other comprehensive health care
specialties (Alkhenizan & Shaw, 2011). These outcomes reveal the positive influence of
mandatory outcomes program on prospective wellness programs and rehabilitation
interventions. The mandatory outcome program offers several professional advantages. The
program proves to be cost effective since it effectively minimizes the use of significant
physician/hospital resources while enhancing the rehabilitation/wellness outcomes. For
example, the use of mandatory physiotherapy program during the postoperative period will
not only facilitate patients’ recovery tenure but also reduce the length of their stay in the
treatment facility, thereby saving the health care expenses to a considerable extent.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

P a g e | 9
References
Alkhenizan, A., & Shaw, C. (2011). mpact of Accreditation on the Quality of Healthcare
Services: a Systematic Review of the Literature. Ann Saudi Med, 31(4), 407-416.
doi:10.4103/0256-4947.83204
Blahd, W. H., Thompson, E. G., Husney, A., & McMahon, P. J. (2018, 09 20). Patellar
Tracking Disorder. Retrieved from https://www.uofmhealth.org/health-library/tn7304
Brukner, P., Nealon, A., Morgan, C., Burgess, D., & Dunn, A. (2014). Recurrent hamstring
muscle injury: applying the limited evidence in the professional football setting with a
seven-point programme. Br J Sports Med, 48(11), 929–938. doi:10.1136/bjsports-
2012-091400
Calverley, P. M. (2018). Breathlessness during exercise in COPD: how do the drugs work?
BMJ. doi:http://dx.doi.org/10.1136/thx.2004.023150
Carpio-Rivera, E., Moncada-Jiménez, J., Salazar-Rojas, W., & Solera-Herrera, A. (2016).
Acute Effects of Exercise on Blood Pressure: A Meta-Analytic Investigation. Arq
Bras Cardiol, 106(5), 422-423. doi:0.5935/abc.20160064
CHOC. (2018). Exercises After ACL Surgery. Retrieved from
https://www.choc.org/orthopaedics/surgery/knee-ligament-repair-reconstruction/
exercises-after-acl-surgery/
Cleveland_Clinic. (2017, 09 05). COPD: Exercise & Activity Guidelines. Retrieved from
https://my.clevelandclinic.org/health/articles/9450-copd-exercise--activity-guidelines
de-Sousa, N. M., Magosso , R. F., Dipp, T., Plentz , R. D., Marson , R. A., Montagnolli , A.
N., . . . Baldissera , V. (2014). Continuous blood pressure response at different
intensities in leg press exercise. Eur J Prev Cardiol, 21(11), 1324-1331.
doi:10.1177/2047487313497863
Durak, E. P., & Palmeiri-Jr, A. J. (1998). Fitness and health promotion in the managed care
setting: The emerging role for exercise and health care. ASEPNewsletter, 1(12).
Retrieved from https://www.asep.org/asep/asep/fldr/11b.htm
Figueiredo, T., Rhea , M. R., Peterson , M., Miranda , H., Bentes , C. M., dos-Reis , V. M., &
Simão , R. (2015). Influence of number of sets on blood pressure and heart rate
References
Alkhenizan, A., & Shaw, C. (2011). mpact of Accreditation on the Quality of Healthcare
Services: a Systematic Review of the Literature. Ann Saudi Med, 31(4), 407-416.
doi:10.4103/0256-4947.83204
Blahd, W. H., Thompson, E. G., Husney, A., & McMahon, P. J. (2018, 09 20). Patellar
Tracking Disorder. Retrieved from https://www.uofmhealth.org/health-library/tn7304
Brukner, P., Nealon, A., Morgan, C., Burgess, D., & Dunn, A. (2014). Recurrent hamstring
muscle injury: applying the limited evidence in the professional football setting with a
seven-point programme. Br J Sports Med, 48(11), 929–938. doi:10.1136/bjsports-
2012-091400
Calverley, P. M. (2018). Breathlessness during exercise in COPD: how do the drugs work?
BMJ. doi:http://dx.doi.org/10.1136/thx.2004.023150
Carpio-Rivera, E., Moncada-Jiménez, J., Salazar-Rojas, W., & Solera-Herrera, A. (2016).
Acute Effects of Exercise on Blood Pressure: A Meta-Analytic Investigation. Arq
Bras Cardiol, 106(5), 422-423. doi:0.5935/abc.20160064
CHOC. (2018). Exercises After ACL Surgery. Retrieved from
https://www.choc.org/orthopaedics/surgery/knee-ligament-repair-reconstruction/
exercises-after-acl-surgery/
Cleveland_Clinic. (2017, 09 05). COPD: Exercise & Activity Guidelines. Retrieved from
https://my.clevelandclinic.org/health/articles/9450-copd-exercise--activity-guidelines
de-Sousa, N. M., Magosso , R. F., Dipp, T., Plentz , R. D., Marson , R. A., Montagnolli , A.
N., . . . Baldissera , V. (2014). Continuous blood pressure response at different
intensities in leg press exercise. Eur J Prev Cardiol, 21(11), 1324-1331.
doi:10.1177/2047487313497863
Durak, E. P., & Palmeiri-Jr, A. J. (1998). Fitness and health promotion in the managed care
setting: The emerging role for exercise and health care. ASEPNewsletter, 1(12).
Retrieved from https://www.asep.org/asep/asep/fldr/11b.htm
Figueiredo, T., Rhea , M. R., Peterson , M., Miranda , H., Bentes , C. M., dos-Reis , V. M., &
Simão , R. (2015). Influence of number of sets on blood pressure and heart rate
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

P a g e | 10
variability after a strength training session. J Strength Cond Res, 29(6), 1556-15563.
doi:10.1519/JSC.0000000000000774.
Furlanetto, K. C., Pinto, I. F., Anna, T. S., Hernandes, N. A., & Pitta, F. (2016). Braz J Phys
Ther. Braz J Phys Ther, 20(6), 517-524. doi:10.1590/bjpt-rbf.2014.0185
Gotshall, R. W., Gootman, J., Byrnes, W. C., Fleck, S. J., & Valovich, T. C. (1999).
Noninvasive characterization of the blood pressure response to the double-leg press
exercise. Journal of Exercise Physiology. Retrieved from
https://www.asep.org/asep/asep/Gotshall.html
Griensven, H. V., Strong, J., & Unruh, A. M. (2014). Pain: a textbook for health
professionals. London: Elsevier.
Linsenbardt, S. T., Thomas, T. R., & Madsen, R. W. (1992). Effect of breathing techniques
on blood pressure response to resistance exercise. Br J Sports Med, 26(2), 97-100.
Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1478931/
McMurray, R. G. (1999). Concepts in Fitness Programming. USA: CRC .
NCSF. (2018). Contraindicated Exercises. Retrieved from
https://www.ncsf.org/enew/articles/articles-contraindicatedexercises.aspx
Nguyen, A. D., Boling, M. C., Levine, B., & Shultz, S. J. (2009). Relationships Between
Lower Extremity Alignment and the Quadriceps Angle. Clin J Sport Med, 19(3), 201-
206. doi:10.1097/JSM.0b013e3181a38fb1
Nyland, J., Mattocks, A., Kibbe, S., Kalloub, A., Greene, J. W., & Caborn, D. N. (2016).
Anterior cruciate ligament reconstruction, rehabilitation, and return to play: 2015
updatex`. Open Access J Sports Med, 21-32. doi:10.2147/OAJSM.S72332
Peng, H. T., & Song, C. Y. (2015). Effect of leg press training on patellar realignment in
patients with patellofemoral pain. J Phys Ther Sci, 27(12), 3873-3878.
doi:10.1589/jpts.27.3873
Physiopedia. (2016). A 10-Week Physical Activity Program for a Hypertensive Obese Adult.
Physiopedia. Retrieved from https://www.physio-pedia.com/A_10-
Week_Physical_Activity_Program_for_a_Hypertensive_Obese_Adult
variability after a strength training session. J Strength Cond Res, 29(6), 1556-15563.
doi:10.1519/JSC.0000000000000774.
Furlanetto, K. C., Pinto, I. F., Anna, T. S., Hernandes, N. A., & Pitta, F. (2016). Braz J Phys
Ther. Braz J Phys Ther, 20(6), 517-524. doi:10.1590/bjpt-rbf.2014.0185
Gotshall, R. W., Gootman, J., Byrnes, W. C., Fleck, S. J., & Valovich, T. C. (1999).
Noninvasive characterization of the blood pressure response to the double-leg press
exercise. Journal of Exercise Physiology. Retrieved from
https://www.asep.org/asep/asep/Gotshall.html
Griensven, H. V., Strong, J., & Unruh, A. M. (2014). Pain: a textbook for health
professionals. London: Elsevier.
Linsenbardt, S. T., Thomas, T. R., & Madsen, R. W. (1992). Effect of breathing techniques
on blood pressure response to resistance exercise. Br J Sports Med, 26(2), 97-100.
Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1478931/
McMurray, R. G. (1999). Concepts in Fitness Programming. USA: CRC .
NCSF. (2018). Contraindicated Exercises. Retrieved from
https://www.ncsf.org/enew/articles/articles-contraindicatedexercises.aspx
Nguyen, A. D., Boling, M. C., Levine, B., & Shultz, S. J. (2009). Relationships Between
Lower Extremity Alignment and the Quadriceps Angle. Clin J Sport Med, 19(3), 201-
206. doi:10.1097/JSM.0b013e3181a38fb1
Nyland, J., Mattocks, A., Kibbe, S., Kalloub, A., Greene, J. W., & Caborn, D. N. (2016).
Anterior cruciate ligament reconstruction, rehabilitation, and return to play: 2015
updatex`. Open Access J Sports Med, 21-32. doi:10.2147/OAJSM.S72332
Peng, H. T., & Song, C. Y. (2015). Effect of leg press training on patellar realignment in
patients with patellofemoral pain. J Phys Ther Sci, 27(12), 3873-3878.
doi:10.1589/jpts.27.3873
Physiopedia. (2016). A 10-Week Physical Activity Program for a Hypertensive Obese Adult.
Physiopedia. Retrieved from https://www.physio-pedia.com/A_10-
Week_Physical_Activity_Program_for_a_Hypertensive_Obese_Adult

P a g e | 11
Qureshi, H., Sharafkhaneh, A., & Hanania, N. A. (2014). Chronic obstructive pulmonary
disease exacerbations: latest evidence and clinical implications. Ther Adv Chronic
Dis, 5(5), 212-227. doi:10.1177/2040622314532862
Russo, M. A., Santarelli, D. M., & O’Rourke, D. (2017). The physiological effects of slow
breathing in the healthy human. Breathe (Sheff), 13(4), 298-309.
doi:10.1183/20734735.009817
Sueki, D., & Brechter, J. (2010). Orthopedic Rehabilitation Clinical Advisor. Missouri:
Mosby Elsevier .
University_of_Texas. (2018, 03 18). Science News. Retrieved from Why are women more
prone to knee injuries than men?:
https://www.sciencedaily.com/releases/2016/03/160318131639.htm
v-d-Meijden, O. A., Westgard, P., Chandler, Z., Gaskill, T. R., Kokmeyer, D., & Millett, P. J.
(2012). REHABILITATION AFTER ARTHROSCOPIC ROTATOR CUFF
REPAIR: CURRENT CONCEPTS REVIEW AND EVIDENCE-BASED
GUIDELINES. Int J Sports Phys Ther, 7(2), 197-218. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3325631/
Weiss, L. J., Wang, D., Hendel, M., Buzzerio, P., & Rodeo, S. A. (2018). Management of
Rotator Cuff Injuries in the Elite Athlete. Curr Rev Musculoskelet Med, 11(1), 102-
112. doi:10.1007/s12178-018-9464-5
Qureshi, H., Sharafkhaneh, A., & Hanania, N. A. (2014). Chronic obstructive pulmonary
disease exacerbations: latest evidence and clinical implications. Ther Adv Chronic
Dis, 5(5), 212-227. doi:10.1177/2040622314532862
Russo, M. A., Santarelli, D. M., & O’Rourke, D. (2017). The physiological effects of slow
breathing in the healthy human. Breathe (Sheff), 13(4), 298-309.
doi:10.1183/20734735.009817
Sueki, D., & Brechter, J. (2010). Orthopedic Rehabilitation Clinical Advisor. Missouri:
Mosby Elsevier .
University_of_Texas. (2018, 03 18). Science News. Retrieved from Why are women more
prone to knee injuries than men?:
https://www.sciencedaily.com/releases/2016/03/160318131639.htm
v-d-Meijden, O. A., Westgard, P., Chandler, Z., Gaskill, T. R., Kokmeyer, D., & Millett, P. J.
(2012). REHABILITATION AFTER ARTHROSCOPIC ROTATOR CUFF
REPAIR: CURRENT CONCEPTS REVIEW AND EVIDENCE-BASED
GUIDELINES. Int J Sports Phys Ther, 7(2), 197-218. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3325631/
Weiss, L. J., Wang, D., Hendel, M., Buzzerio, P., & Rodeo, S. A. (2018). Management of
Rotator Cuff Injuries in the Elite Athlete. Curr Rev Musculoskelet Med, 11(1), 102-
112. doi:10.1007/s12178-018-9464-5
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.