Physiology of Burns and Management - Desklib
Use problem-solving skills to answer questions related to a case study on burn injury and resuscitation priorities in emergency nursing.
13 Pages3501 Words311 Views
Added on 2023-06-09
About This Document
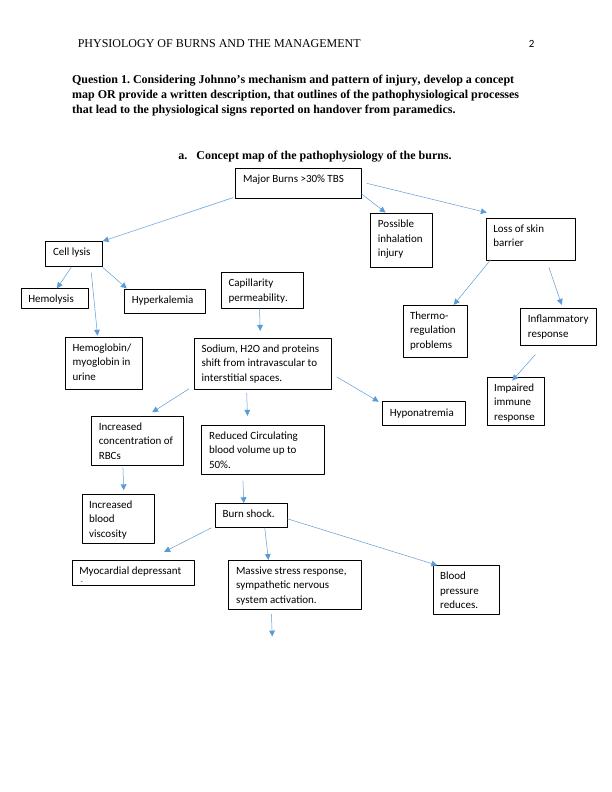
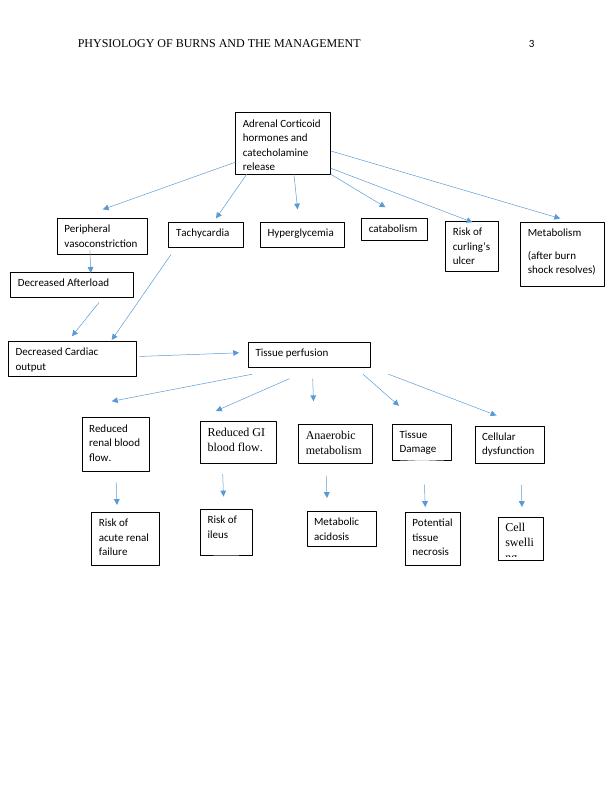
This article discusses the pathophysiology of burns, nursing care priorities, fluid resuscitation, and potential complications. It includes a concept map of the pathophysiology of burns, clinical signs, and immediate nursing care priorities. The article also covers evidence-based research and current recommendations for calculating the percentage of TBSA burned and fluid requirements. Ongoing nursing care to maintain adequate oxygenation and ventilation, circulation, thermoregulation, and managing potential early complications are also discussed.
Physiology of Burns and Management - Desklib
Use problem-solving skills to answer questions related to a case study on burn injury and resuscitation priorities in emergency nursing.
Added on 2023-06-09
ShareRelated Documents

End of preview
Want to access all the pages? Upload your documents or become a member.
Respiratory Acidosis: Causes, Symptoms, and Treatment
|5
|1037
|300
Nursing Case Study: Acute Respiratory Distress Syndrome and Severe Sepsis
|9
|4114
|406
Asthma Management
|6
|1523
|54
Hypovolemic Shock: Causes, Symptoms, and Nursing Interventions
|8
|2371
|61
Oxygen therapy in the pulmonary artery to lower the hypoxic condition in the pulmonary artery
|1
|646
|260
Synchronous Session Reflection on Respiratory and Metabolic Acidosis and Alkalosis
|5
|1198
|147