Point-of-Decision Prompts to Increase Stair Use: A Systematic Review Update
VerifiedAdded on 2023/05/29
|9
|7490
|401
AI Summary
This systematic review update examines the effectiveness of point-of-decision prompts to encourage stair use and enhancements to stairs or stairwells when combined with point-of-decision prompts to increase stair use. The article describes the rationale for these systematic reviews, along with information about the review process and the resulting conclusions.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Point-of-Decision Prompts to Increase
Stair Use
A Systematic Review Update
Robin E. Soler, PhD, Kimberly D. Leeks, PhD, MPH, Leigh Ramsey Buchanan, PhD,
Ross C. Brownson, PhD, Gregory W. Heath, DHSc, MPH, David H. Hopkins, MD, MPH,
the Task Force on Community Preventive Services
Abstract:In 2000, the Guide to Community Preventive Services (Community Guide) completed a
systematic review of the effectiveness of various approaches to increasing physical activity including
informational,behavioraland social,and environmentaland policy approaches.Among these
approaches was the use of signs placed by elevators and escalators to encourage stair use.This
approach was found to be effective based on suffıcient evidence. Over the past 5 years the body of
evidence of this intervention has increased substantially, warranting an updated review. This update
was conducted on 16 peer-reviewed studies (including the six studies in the previous systematic
review),which met specifıed quality criteria and included evaluation outcomes of interest.These
studies evaluated two interventions: point-of-decision prompts to increase stair use and enhance-
ments to stairs or stairwells (e.g., painting walls, laying carpet, adding artwork, playing music) when
combined with point-of-decision prompts to increase stair use.This latter intervention was not
included in the original systematic review.
According to the Community Guide rules of evidence,there is strong evidence that point-of-
decision prompts are effective in increasing the use of stairs. There is insuffıcient evidence, due to a
inadequate number of studies, to determine whether or not enhancements to stairs or stairwells are
an effective addition to point-of-decision prompts.This article describes the rationale for these
systematic reviews, along with information about the review process and the resulting conclusions.
Additionalinformation about applicability,other effects,and barriers to implementation is also
provided.
(Am J Prev Med 2010;38(2S):S292–S300) Published by Elsevier Inc. on behalf of American Journal of Preventive
Medicine
Introduction
The prevalence ofoverweight and obesity in the
U.S. has increased over the past several decades.
In 2003–2004,66.3% of adults in the U.S.were
overweightor obese,and 32.2% were obese.1 Obesity
increases the risk of many diseases and health conditions,
including hypertension,type 2 diabetes,coronary heart
disease,stroke,gallbladder disease,osteoarthritis,and
some cancers.2 The primary cause ofoverweightand
obesity in the U.S. is energy imbalance.2,3Energy imbal-
ance occurs when the number of calories used is not equ
to the number of calories consumed. Energy expenditure
has been on the decline in the U.S. for decades, due in p
to increasing automation of previously manual activi-
ties.In 1996,the U.S.Preventive Services Task Force
(USPSTF) recommended thathealthcareproviders
counsel all patients on the importance of incorporating
physicalactivity into their daily routines.4 One way to
increase energy expenditure,and improve energy bal-
ance, is to incorporate small bouts of physical activity in
daily routines.3
Many intervention approaches are available to increas
engagement in physical activity by adults.5 Each of these
approaches has a set of advantages and disadvantages
can be applied, with differing degrees of success, to peo
with a variety of demographic characteristics and life-
styles in diverse locations. As noted in an earlier review
From the Community Guide Branch, Division of Health Communications
and Marketing Strategy,NationalCenter for Health Marketing,(Soler,
Leeks,Hopkins) and the Chronic Disease Nutrition Branch,Division of
Nutrition,PhysicalActivity,and Obesity,NationalCenter for Chronic
Disease Health Promotion and Prevention (Buchanan),CDC, Atlanta,
Georgia;St.Louis University,Schoolof Public Health (Brownson),St.
Louis, Missouri; and University of Tennessee at Chattanooga, Department
of Health and Human Performance (Heath), Chattanooga, Tennessee
Address correspondence and reprint requests to: Robin E. Soler, PhD,
Community Guide Branch,Centers for Disease Control and Prevention,
1600 Clifton Road, MS-E69, Atlanta GA 30333. E-mail: RSoler@cdc.gov.
0749-3797/00/$17.00
doi: 10.1016/j.amepre.2009.10.028
S292 Am J Prev Med 2010;38(2S):S292–S300Published by Elsevier Inc. on behalf of American Journal of Preventive Medicin
Stair Use
A Systematic Review Update
Robin E. Soler, PhD, Kimberly D. Leeks, PhD, MPH, Leigh Ramsey Buchanan, PhD,
Ross C. Brownson, PhD, Gregory W. Heath, DHSc, MPH, David H. Hopkins, MD, MPH,
the Task Force on Community Preventive Services
Abstract:In 2000, the Guide to Community Preventive Services (Community Guide) completed a
systematic review of the effectiveness of various approaches to increasing physical activity including
informational,behavioraland social,and environmentaland policy approaches.Among these
approaches was the use of signs placed by elevators and escalators to encourage stair use.This
approach was found to be effective based on suffıcient evidence. Over the past 5 years the body of
evidence of this intervention has increased substantially, warranting an updated review. This update
was conducted on 16 peer-reviewed studies (including the six studies in the previous systematic
review),which met specifıed quality criteria and included evaluation outcomes of interest.These
studies evaluated two interventions: point-of-decision prompts to increase stair use and enhance-
ments to stairs or stairwells (e.g., painting walls, laying carpet, adding artwork, playing music) when
combined with point-of-decision prompts to increase stair use.This latter intervention was not
included in the original systematic review.
According to the Community Guide rules of evidence,there is strong evidence that point-of-
decision prompts are effective in increasing the use of stairs. There is insuffıcient evidence, due to a
inadequate number of studies, to determine whether or not enhancements to stairs or stairwells are
an effective addition to point-of-decision prompts.This article describes the rationale for these
systematic reviews, along with information about the review process and the resulting conclusions.
Additionalinformation about applicability,other effects,and barriers to implementation is also
provided.
(Am J Prev Med 2010;38(2S):S292–S300) Published by Elsevier Inc. on behalf of American Journal of Preventive
Medicine
Introduction
The prevalence ofoverweight and obesity in the
U.S. has increased over the past several decades.
In 2003–2004,66.3% of adults in the U.S.were
overweightor obese,and 32.2% were obese.1 Obesity
increases the risk of many diseases and health conditions,
including hypertension,type 2 diabetes,coronary heart
disease,stroke,gallbladder disease,osteoarthritis,and
some cancers.2 The primary cause ofoverweightand
obesity in the U.S. is energy imbalance.2,3Energy imbal-
ance occurs when the number of calories used is not equ
to the number of calories consumed. Energy expenditure
has been on the decline in the U.S. for decades, due in p
to increasing automation of previously manual activi-
ties.In 1996,the U.S.Preventive Services Task Force
(USPSTF) recommended thathealthcareproviders
counsel all patients on the importance of incorporating
physicalactivity into their daily routines.4 One way to
increase energy expenditure,and improve energy bal-
ance, is to incorporate small bouts of physical activity in
daily routines.3
Many intervention approaches are available to increas
engagement in physical activity by adults.5 Each of these
approaches has a set of advantages and disadvantages
can be applied, with differing degrees of success, to peo
with a variety of demographic characteristics and life-
styles in diverse locations. As noted in an earlier review
From the Community Guide Branch, Division of Health Communications
and Marketing Strategy,NationalCenter for Health Marketing,(Soler,
Leeks,Hopkins) and the Chronic Disease Nutrition Branch,Division of
Nutrition,PhysicalActivity,and Obesity,NationalCenter for Chronic
Disease Health Promotion and Prevention (Buchanan),CDC, Atlanta,
Georgia;St.Louis University,Schoolof Public Health (Brownson),St.
Louis, Missouri; and University of Tennessee at Chattanooga, Department
of Health and Human Performance (Heath), Chattanooga, Tennessee
Address correspondence and reprint requests to: Robin E. Soler, PhD,
Community Guide Branch,Centers for Disease Control and Prevention,
1600 Clifton Road, MS-E69, Atlanta GA 30333. E-mail: RSoler@cdc.gov.
0749-3797/00/$17.00
doi: 10.1016/j.amepre.2009.10.028
S292 Am J Prev Med 2010;38(2S):S292–S300Published by Elsevier Inc. on behalf of American Journal of Preventive Medicin
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
the Guide to Community Preventive Services (Community
Guide),which evaluated interventions designed to in-
crease physicalactivity,“the role ofcommunity-based
interventions to promote physical activity has emerged as
a critical piece of an overall strategy to increase physical
activity behaviorsamong thepeopleof the United
States.”5 This 2002 review focused on community-based
intervention approaches, including:
● Informationalapproaches to change knowledge and
attitudes about the benefıts of and opportunities for
physical activity within a community;
● Behavioral and social approaches to teach people the
behavioral management skills necessary both for suc-
cessful adoption and maintenance of behavior change
and for creating social environments that facilitate and
enhance behavioral change; and
● Environmentaland policy approaches to change the
structure of physical and organizational environments
to provide safe,attractive,and convenient places for
physical activity.
This article reports the fındings from an update to the
2002 Point-of-Decision Prompts review,which is a be-
havior and social approach as described above. The up-
dated systematic review examines literature regarding the
effectiveness of prompts on increasing stair use either by
increasing the number of actual stair users or increasing
the frequency of stair use through prompts that relate to
both of these foci, which can be implemented by commu-
nities to help increase levels of physical activity. Point-of-
decision prompts can be used alone or with stairwell
enhancements in an attempt to improve the effectiveness
of the prompt (i.e., by making stairwells more attractive
to potential users).
Guide to Community Preventive Services
The systematic reviews in this report present the fındings
of the independent, nonfederal Task Force on Commu-
nity Preventive Services (Task Force). The Task Force is
developing the Community Guide with the support of the
USDHHS in collaboration with public and private part-
ners. The CDC provides staff support to the Task Force
for development of the Community Guide. The book, The
Guide to Community Preventive Services. What Works to
Promote Health? (Oxford University Press,2005;also
available at www.thecommunityguide.org) presents the
background and the methods used in developing the
Community Guide.The physicalactivity review noted
above was published in the American Journal of Preven-
tive Medicine in 20025,6and describes the broader ana-
lytic framework used to evaluate the effectivenessof
community-based physical activity interventions.
Methods
This updated review was conducted according to the me
ods developed for the Community Guide, which have bee
described in detail elsewhere.5,7As an update to an existing
Community Guide review,5 some information and guidance
was drawn from the previous review team and resulting
documentation. Inclusion criteria for studies in this revie
were:(1) primary research published in a peer-reviewed
journal;(2) published in English before April20,2005;
(3) met the minimum research quality for study design a
execution7; and (4) evaluated the effects ofpoint-of-decision
prompts to encourage stair use (with or without enhance
ments to the stairwell).The outcome measure remained
stair use, and the search strategy was widened by inclus
additional electronic databases. The systematic review t
(the team) accepted the broader conceptual approach o
original physical activity review5 but developed a new con-
ceptualframework for the interventions evaluated in this
update. The team recalculated the original effect size me
sure (relative change) and calculated a new summary eff
measure (absolute change);reexamined the evidence re-
garding applicability of this intervention;and updated the
overall conclusions based on the original six studies and
additional ten studies found through the updated literatu
search.
Conceptual Approach
Point-of-decision prompts are motivational signs, placed
or near stairwells or at the base of elevators and escalat
encouraging people to use the stairs.These prompts are
typically designed to change a behavior of interest by pr
viding information about a healthier alternative or estab
ing a deterrent to the behavioral standard (e.g., announc
that an elevator is off limits to those capable of using sta
with the intended goal of motivating and enabling peopl
change their behavior and maintain that change over tim
Stairwellenhancements improve the appearance ofstair-
wells by painting walls or laying carpet.A conceptualap-
proach was used to evaluate the effectiveness of point-o
decision prompts and stairwellenhancements to increase
stair use. The approach suggests that extended presenc
point-of-decision promptdesigned to increase stairuse
might work by changing individual knowledge or attitude
about using the stairs. Information provided through sta
prompts might also contribute to an individual’s change
knowledge or attitudes about the value of physical activ
general. As a result, prompts are expected to increase th
of stairs as a mode of transportation and may change at
tudes toward or amount of engagement in physical activ
Walking up or down stairs uses more energy than taking
elevator or escalator,and stair use requires bodily move-
ment. The relationships between stair use and caloric ex
diture and between stair use and physical activity were n
reviewed. This conceptual approach suggests that the sl
Soler et al / Am J Prev Med 2010;38(2S):S292–S300 S293
February 2010
Guide),which evaluated interventions designed to in-
crease physicalactivity,“the role ofcommunity-based
interventions to promote physical activity has emerged as
a critical piece of an overall strategy to increase physical
activity behaviorsamong thepeopleof the United
States.”5 This 2002 review focused on community-based
intervention approaches, including:
● Informationalapproaches to change knowledge and
attitudes about the benefıts of and opportunities for
physical activity within a community;
● Behavioral and social approaches to teach people the
behavioral management skills necessary both for suc-
cessful adoption and maintenance of behavior change
and for creating social environments that facilitate and
enhance behavioral change; and
● Environmentaland policy approaches to change the
structure of physical and organizational environments
to provide safe,attractive,and convenient places for
physical activity.
This article reports the fındings from an update to the
2002 Point-of-Decision Prompts review,which is a be-
havior and social approach as described above. The up-
dated systematic review examines literature regarding the
effectiveness of prompts on increasing stair use either by
increasing the number of actual stair users or increasing
the frequency of stair use through prompts that relate to
both of these foci, which can be implemented by commu-
nities to help increase levels of physical activity. Point-of-
decision prompts can be used alone or with stairwell
enhancements in an attempt to improve the effectiveness
of the prompt (i.e., by making stairwells more attractive
to potential users).
Guide to Community Preventive Services
The systematic reviews in this report present the fındings
of the independent, nonfederal Task Force on Commu-
nity Preventive Services (Task Force). The Task Force is
developing the Community Guide with the support of the
USDHHS in collaboration with public and private part-
ners. The CDC provides staff support to the Task Force
for development of the Community Guide. The book, The
Guide to Community Preventive Services. What Works to
Promote Health? (Oxford University Press,2005;also
available at www.thecommunityguide.org) presents the
background and the methods used in developing the
Community Guide.The physicalactivity review noted
above was published in the American Journal of Preven-
tive Medicine in 20025,6and describes the broader ana-
lytic framework used to evaluate the effectivenessof
community-based physical activity interventions.
Methods
This updated review was conducted according to the me
ods developed for the Community Guide, which have bee
described in detail elsewhere.5,7As an update to an existing
Community Guide review,5 some information and guidance
was drawn from the previous review team and resulting
documentation. Inclusion criteria for studies in this revie
were:(1) primary research published in a peer-reviewed
journal;(2) published in English before April20,2005;
(3) met the minimum research quality for study design a
execution7; and (4) evaluated the effects ofpoint-of-decision
prompts to encourage stair use (with or without enhance
ments to the stairwell).The outcome measure remained
stair use, and the search strategy was widened by inclus
additional electronic databases. The systematic review t
(the team) accepted the broader conceptual approach o
original physical activity review5 but developed a new con-
ceptualframework for the interventions evaluated in this
update. The team recalculated the original effect size me
sure (relative change) and calculated a new summary eff
measure (absolute change);reexamined the evidence re-
garding applicability of this intervention;and updated the
overall conclusions based on the original six studies and
additional ten studies found through the updated literatu
search.
Conceptual Approach
Point-of-decision prompts are motivational signs, placed
or near stairwells or at the base of elevators and escalat
encouraging people to use the stairs.These prompts are
typically designed to change a behavior of interest by pr
viding information about a healthier alternative or estab
ing a deterrent to the behavioral standard (e.g., announc
that an elevator is off limits to those capable of using sta
with the intended goal of motivating and enabling peopl
change their behavior and maintain that change over tim
Stairwellenhancements improve the appearance ofstair-
wells by painting walls or laying carpet.A conceptualap-
proach was used to evaluate the effectiveness of point-o
decision prompts and stairwellenhancements to increase
stair use. The approach suggests that extended presenc
point-of-decision promptdesigned to increase stairuse
might work by changing individual knowledge or attitude
about using the stairs. Information provided through sta
prompts might also contribute to an individual’s change
knowledge or attitudes about the value of physical activ
general. As a result, prompts are expected to increase th
of stairs as a mode of transportation and may change at
tudes toward or amount of engagement in physical activ
Walking up or down stairs uses more energy than taking
elevator or escalator,and stair use requires bodily move-
ment. The relationships between stair use and caloric ex
diture and between stair use and physical activity were n
reviewed. This conceptual approach suggests that the sl
Soler et al / Am J Prev Med 2010;38(2S):S292–S300 S293
February 2010
increase in caloric expenditure (energy expenditure) result-
ing from stair use, which serves to improve energy balance
can,in combination with other forms of physical activity,
contribute to physiologic improvements that are,in turn,
related to longer-term health outcomes.
Selection of Outcomes for Review
The primary outcomes examined in this review were objec-
tive measurements of changes in the use of stairs during two
or more periods of time. Objective measurements were vi-
sual counts of people using the stairs or electronic counts
(from devices such as motion detectors). Some of the quali-
fying studies reported other outcomes which were examined
but are not presented in this report.
Selection of stair use as an outcome assumes that small
amounts ofphysicalactivity on a regular basis willhelp
improve the energy imbalance that affects large numbers of
people (particularly people who are sedentary and those
who are obese).Stair use typically involves ascending or
descending one to four flights per day. Using stairs expends
twice as much energy as using elevators8 with each stair
ascended burning approximately 0.11 kilocalorie and each
stair descended burning approximately 0.05 kilocalorie.9
Regular, substantial stair use (as many as six assents of 199
steps per assent per day for 12 weeks) has been shown to
improve cardiovascular outcomes among previously seden-
tary young women10and Benn et al., in their study of a small
group of older men found that
climbing only three to four flights of stairs at a mod-
erate pace (approximately 50 –70 s) elicits peak circu-
latory demands similar to, but at a much more rapid
rate ofadjustmentthan,10 minutes ofhorizontal
walking at2.5 mph,intermittently carrying a 30-
pound weight, or 4 minutes of walking up a moder-
ately steep slope.11
Over the long-term, this added energy expenditure could
contribute to improved energy balance and longer-term
health outcomes such as weight control.
Search Strategy
The articles considered for this review were obtained from
systematic searches of multiple databases, reviews of biblio-
graphic reference lists, and consultations with experts in the
fıeld. The team’s updated search for evidence encompassed
the period from 2000 to April 2005, which overlapped with
the search conducted for the originalCommunity Guide
review of these interventions (search period 1980 –2000).5
The original review used the following seven databases: En-
viroline, MEDLINE, PsychInfo, Social SciSearch, Sociologi-
cal Abstracts, Sportdiscus, and Transportation Research In-
formation Services (TRIS).For the team’s updated search,
the following 15 databaseswere examined:ArticleFirst,
CINAHL, EMBASE, Enviroline, Health Promotion and Edu-
cation Database, MEDLINE, Ovid, PsycINFO, PubMed, So-
cialSciSearch,SocialScience Citation Index,Sociological
Abstracts,SPORTDiscus,Transportation Research Infor-
mation Services (TRIS),and WorldCat.This list includes
some databases notavailable atthe time ofthe original
review.
Evaluating and Summarizing the Studies
Each study that met the inclusion criteria was evaluated fo
the suitability of the study design and study execution usin
the standardized Community Guide abstraction form.12The
suitability of each study design was rated as greatest, mod
erate, or least depending on the degree to which the desig
protects against threats to validity.The execution of each
study was rated as good,fair,or limited on the basis of
several predetermined factors that could potentially limit a
study’s utility for assessing effectiveness.Each study was
reviewed by at least two trained researchers. Concerns abo
study design and execution were discussed with an expert
physicalactivity interventions and differences in opinion
were resolved by consensus among a team of three system
atic reviewers (the coordination team).Only studies rated
greatest or moderate in design suitability and good or fair i
execution were considered qualifying studies and included
in the team’s fınal assessment of the evidence in this revie
Studies with limited execution are,by Community Guide
methods, excluded from consideration, and studies of least
suitable design were excluded by the coordination team
because the body of literature was adequately represented
with moderate and greatest suitability study designs.
Calculation of Effect Sizes
The qualifying studies provided measurements of change i
the number or proportion of people using the stairs before
and after the implementation of point-of-decision prompts
(with or without additional enhancements to the stairs or
stairwells).To facilitate comparison across studies and an
evaluation across the body of evidence, individual study ar
results were converted (if necessary) into measurements o
both absolute and relative percentage change.In addition,
whenever possible, a mean effect size was calculated on th
entire sample in each study arm.Studies contained more
than one study arm when there were multiple locations or
mechanismsof implementation forthe intervention.In
some cases,effectmeasures were reported for subgroup
means (e.g.,one for men and one for women).For these
study fındings, the mean of the subgroups was incorporate
into the overallcalculations for median and interquartile
interval (IQI),thus providing only one independent effect
size per study arm (these are referred to as data points). F
time–series studies without a concurrent comparison group
the effectsizes (using pretestmeasurements and the last
postintervention measurement provided) were calculated a
follows:
S294 Soler et al / Am J Prev Med 2010;38(2S):S292–S300
www.ajpm-online.net
ing from stair use, which serves to improve energy balance
can,in combination with other forms of physical activity,
contribute to physiologic improvements that are,in turn,
related to longer-term health outcomes.
Selection of Outcomes for Review
The primary outcomes examined in this review were objec-
tive measurements of changes in the use of stairs during two
or more periods of time. Objective measurements were vi-
sual counts of people using the stairs or electronic counts
(from devices such as motion detectors). Some of the quali-
fying studies reported other outcomes which were examined
but are not presented in this report.
Selection of stair use as an outcome assumes that small
amounts ofphysicalactivity on a regular basis willhelp
improve the energy imbalance that affects large numbers of
people (particularly people who are sedentary and those
who are obese).Stair use typically involves ascending or
descending one to four flights per day. Using stairs expends
twice as much energy as using elevators8 with each stair
ascended burning approximately 0.11 kilocalorie and each
stair descended burning approximately 0.05 kilocalorie.9
Regular, substantial stair use (as many as six assents of 199
steps per assent per day for 12 weeks) has been shown to
improve cardiovascular outcomes among previously seden-
tary young women10and Benn et al., in their study of a small
group of older men found that
climbing only three to four flights of stairs at a mod-
erate pace (approximately 50 –70 s) elicits peak circu-
latory demands similar to, but at a much more rapid
rate ofadjustmentthan,10 minutes ofhorizontal
walking at2.5 mph,intermittently carrying a 30-
pound weight, or 4 minutes of walking up a moder-
ately steep slope.11
Over the long-term, this added energy expenditure could
contribute to improved energy balance and longer-term
health outcomes such as weight control.
Search Strategy
The articles considered for this review were obtained from
systematic searches of multiple databases, reviews of biblio-
graphic reference lists, and consultations with experts in the
fıeld. The team’s updated search for evidence encompassed
the period from 2000 to April 2005, which overlapped with
the search conducted for the originalCommunity Guide
review of these interventions (search period 1980 –2000).5
The original review used the following seven databases: En-
viroline, MEDLINE, PsychInfo, Social SciSearch, Sociologi-
cal Abstracts, Sportdiscus, and Transportation Research In-
formation Services (TRIS).For the team’s updated search,
the following 15 databaseswere examined:ArticleFirst,
CINAHL, EMBASE, Enviroline, Health Promotion and Edu-
cation Database, MEDLINE, Ovid, PsycINFO, PubMed, So-
cialSciSearch,SocialScience Citation Index,Sociological
Abstracts,SPORTDiscus,Transportation Research Infor-
mation Services (TRIS),and WorldCat.This list includes
some databases notavailable atthe time ofthe original
review.
Evaluating and Summarizing the Studies
Each study that met the inclusion criteria was evaluated fo
the suitability of the study design and study execution usin
the standardized Community Guide abstraction form.12The
suitability of each study design was rated as greatest, mod
erate, or least depending on the degree to which the desig
protects against threats to validity.The execution of each
study was rated as good,fair,or limited on the basis of
several predetermined factors that could potentially limit a
study’s utility for assessing effectiveness.Each study was
reviewed by at least two trained researchers. Concerns abo
study design and execution were discussed with an expert
physicalactivity interventions and differences in opinion
were resolved by consensus among a team of three system
atic reviewers (the coordination team).Only studies rated
greatest or moderate in design suitability and good or fair i
execution were considered qualifying studies and included
in the team’s fınal assessment of the evidence in this revie
Studies with limited execution are,by Community Guide
methods, excluded from consideration, and studies of least
suitable design were excluded by the coordination team
because the body of literature was adequately represented
with moderate and greatest suitability study designs.
Calculation of Effect Sizes
The qualifying studies provided measurements of change i
the number or proportion of people using the stairs before
and after the implementation of point-of-decision prompts
(with or without additional enhancements to the stairs or
stairwells).To facilitate comparison across studies and an
evaluation across the body of evidence, individual study ar
results were converted (if necessary) into measurements o
both absolute and relative percentage change.In addition,
whenever possible, a mean effect size was calculated on th
entire sample in each study arm.Studies contained more
than one study arm when there were multiple locations or
mechanismsof implementation forthe intervention.In
some cases,effectmeasures were reported for subgroup
means (e.g.,one for men and one for women).For these
study fındings, the mean of the subgroups was incorporate
into the overallcalculations for median and interquartile
interval (IQI),thus providing only one independent effect
size per study arm (these are referred to as data points). F
time–series studies without a concurrent comparison group
the effectsizes (using pretestmeasurements and the last
postintervention measurement provided) were calculated a
follows:
S294 Soler et al / Am J Prev Med 2010;38(2S):S292–S300
www.ajpm-online.net
absolute percentage change (difference is described as “per-
centage point change”),
Effect size ⫽ Ipost⫺ Ipre;
relative percentage change (result is described as “percent-
age change”),
Effect size ⫽ ((Ipost⫺ Ipre)/I pre) ⫻ 100.
For the study thatincluded a concurrentcomparison
population (not exposed to the intervention), the effect size
was calculated as follows:
absolute percentage change (difference is described as “per-
centage point change”),
Effect size ⫽ (Ipost⫺ Ipre) ⫺ (Cpost⫺ Cpre);
relative percentage change (result is described as “percent-
age change”),
Effect size
⫽ ([(I post⫺ Ipre) ⫺ (Cpost⫺ Cpre)] ⁄ Ipre) ⫻ 100.
For all calculations, I ⫽ intervention group; C ⫽ comparison
group;and “pre” and “post” subscripts indicate measure-
ments taken before and after intervention implementation.
For studies in which multiple postintervention measure-
ments were taken, the measurement most distant from the
end of the intervention is used. In addition to the calculation
of effect sizes for each study,an overall median effect size
and interquartile interval were determined for both absolute
and relative percentage change.
Throughout the results section effect sizes are presented
as both absolute and relative change. The original review of
point-of-decision prompts5 reported relative change only;
thus relative change is reported in this paper to allow for
comparisons across reviews.Absolute change is also re-
ported because it provides an estimate of change that is not
dependent on baseline rates (that may vary according to
setting or other population characteristics).
Results
Part I: Interventions to Increase the Use of
Stairs (Updated)
The team examined the evidence from qualifying studies
for two related interventions:(1) point-of-decision
prompts;and (2)stairwellenhancements when com-
bined with point-of-decision prompts.
Review of Evidence: Point-of-Decision
Prompts
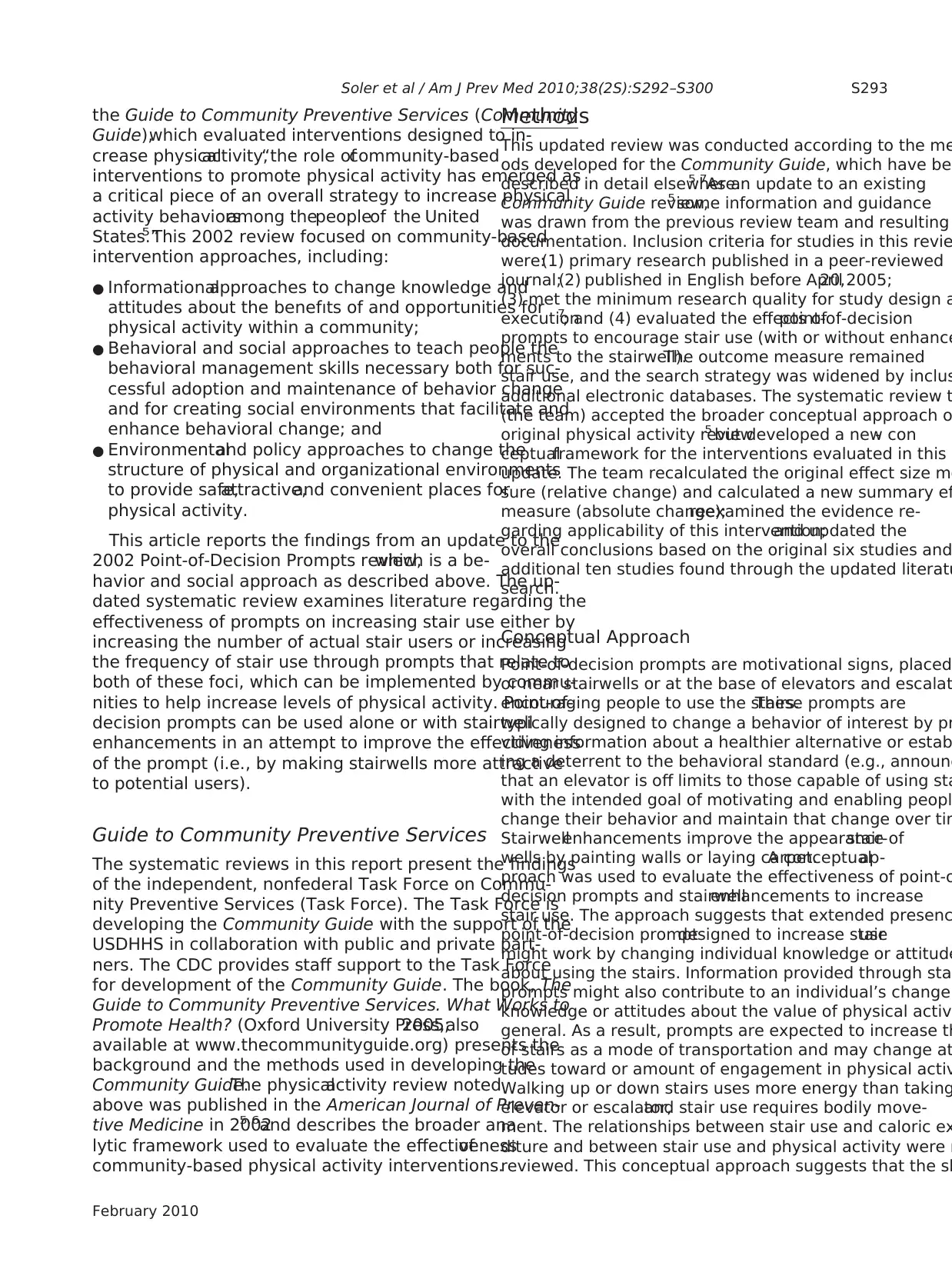
Point-of-decision prompts are motivational signs placed
on or near stairwells or at the base of elevators and esca-
lators encouraging people to use stairs. These signs, such
as the one shown in Figure 1, inform individuals about a
health or weight-loss benefıt from using stairs,about a
nearby opportunity to use stairs, or both. A few examp
of the content of the signs include “improve your wais
line, use the stairs” or “your heart needs exercise, use
stairs.” Point-of-decision signs may be combined with
prompts such as footprints placed to direct individuals
stairwell; the team considered these additional efforts
this review.Point-of-decision prompts when combined
with more elaborate enhancements to the stairs or sta
such as painting stairwell walls or playing music in sta
are reviewed separately below.
Effectiveness.The literature search identifıed 15 stud-
ies thatassessed the effectiveness ofpoint-of-decision
prompts when used alone in changing the frequency o
amount of stair use or the number of stair users.13–27
Four
of these studies were rated as having least suitable st
designs and were excluded from further analysis.21–24
Figure 1.Sample point-of-decision prompt
Soler et al / Am J Prev Med 2010;38(2S):S292–S300 S295
February 2010
centage point change”),
Effect size ⫽ Ipost⫺ Ipre;
relative percentage change (result is described as “percent-
age change”),
Effect size ⫽ ((Ipost⫺ Ipre)/I pre) ⫻ 100.
For the study thatincluded a concurrentcomparison
population (not exposed to the intervention), the effect size
was calculated as follows:
absolute percentage change (difference is described as “per-
centage point change”),
Effect size ⫽ (Ipost⫺ Ipre) ⫺ (Cpost⫺ Cpre);
relative percentage change (result is described as “percent-
age change”),
Effect size
⫽ ([(I post⫺ Ipre) ⫺ (Cpost⫺ Cpre)] ⁄ Ipre) ⫻ 100.
For all calculations, I ⫽ intervention group; C ⫽ comparison
group;and “pre” and “post” subscripts indicate measure-
ments taken before and after intervention implementation.
For studies in which multiple postintervention measure-
ments were taken, the measurement most distant from the
end of the intervention is used. In addition to the calculation
of effect sizes for each study,an overall median effect size
and interquartile interval were determined for both absolute
and relative percentage change.
Throughout the results section effect sizes are presented
as both absolute and relative change. The original review of
point-of-decision prompts5 reported relative change only;
thus relative change is reported in this paper to allow for
comparisons across reviews.Absolute change is also re-
ported because it provides an estimate of change that is not
dependent on baseline rates (that may vary according to
setting or other population characteristics).
Results
Part I: Interventions to Increase the Use of
Stairs (Updated)
The team examined the evidence from qualifying studies
for two related interventions:(1) point-of-decision
prompts;and (2)stairwellenhancements when com-
bined with point-of-decision prompts.
Review of Evidence: Point-of-Decision
Prompts
Point-of-decision prompts are motivational signs placed
on or near stairwells or at the base of elevators and esca-
lators encouraging people to use stairs. These signs, such
as the one shown in Figure 1, inform individuals about a
health or weight-loss benefıt from using stairs,about a
nearby opportunity to use stairs, or both. A few examp
of the content of the signs include “improve your wais
line, use the stairs” or “your heart needs exercise, use
stairs.” Point-of-decision signs may be combined with
prompts such as footprints placed to direct individuals
stairwell; the team considered these additional efforts
this review.Point-of-decision prompts when combined
with more elaborate enhancements to the stairs or sta
such as painting stairwell walls or playing music in sta
are reviewed separately below.
Effectiveness.The literature search identifıed 15 stud-
ies thatassessed the effectiveness ofpoint-of-decision
prompts when used alone in changing the frequency o
amount of stair use or the number of stair users.13–27
Four
of these studies were rated as having least suitable st
designs and were excluded from further analysis.21–24
Figure 1.Sample point-of-decision prompt
Soler et al / Am J Prev Med 2010;38(2S):S292–S300 S295
February 2010
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Two of the studies19,25
were of good execution;the re-
maining nine13–18,20,26,27
were rated as fair.One addi-
tionalpaper provided information on a study already
included in the review.28 Details ofthe 11 qualifying
studies,including a summary ofthe content,delivery,
evaluation design,and outcomes,are available at www.
thecommunityguide.org/pa/environmental-policy/
podp.html.
Study design and implementationcharacteris-
tics. All 11 qualifying studies used time–series designs,
and were rated as being of moderate suitability.13–20,25–27
All of the qualifying studies were conducted between
1980 and 2003, and measured stair use in adult popula-
tions. The types of point-of-decision prompts used in the
qualifyingstudiesweresigns13–19,26,27
or banners,20
which were distinctions used by the authors and not
necessarily related to the size of the prompt, although in
the one study specifying stair banners, the messages were
physically placed on each stair, but like the signs, varied in
design and message.The 11 qualifying studies imple-
mented a variety of point-of-decision prompts messages
such as health benefıts and health promotion,13,14,16 –18,25
weight control,14 and signs (in Spanish and English)
using eitheran individualor family perspective to
specifıcally targetthe Hispanic community.19 One
study focused primarily on African-Americans,and
the point-of-decision prompt was tailored to this partic-
ular community.15Additionally, in one study a deterrent
sign was displayed that limited the elevator to use by the
staff and the physically challenged.26
Outcomes Related to Stair Use
Eleven qualifying studies,13–20,25–27
consisting of 21 study
arms for stair use, provided evidence in terms of absolute
(i.e., percentage point) change. In these studies, the base-
line rates of stair use ranged from 1.7% to 39.7% of po-
tential users (median⫽8.2, IQI⫽5.2, 21.2). Stair use dur-
ing the intervention period in these study arms ranged
from 4.0% to 41.9% ofpotentialusers.The median
change for the 21 study arms representing these studies
was an increase in stair use of2.4 percentage points
(IQI⫽0.83, 6.7 percentage points).Increases in stair
use in 15 of 21 study arms were reported as statistically
signifıcant,14 –20,22–28
while two study arms (from the
same study)reported a signifıcantdecrease in stair
use.19
To examine effects relative to baseline stair use, eleven
qualifying studies that included 21 study arms for stair
use were evaluated in terms of relative (i.e., percentage)
change.13–20,25–27
The majority of studies reported a low
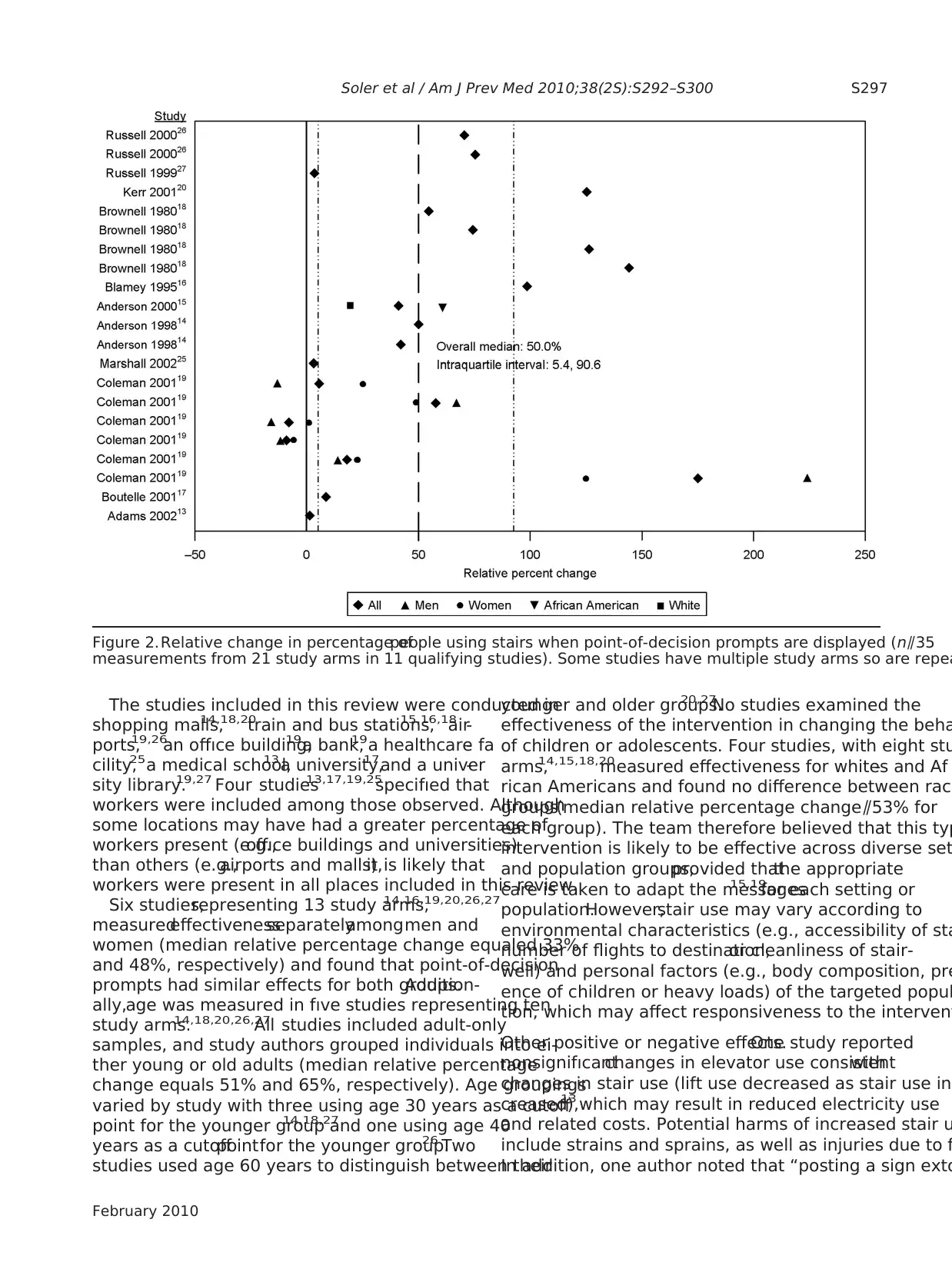
levelof baseline stair use (⬍20%).Overall,in the 11
qualifying studies,the median relative improvement in
observed stair use was 50 percentage points (IQI⫽5.4%,
90.6%) from baseline (Figure 2; note that data points for
subpopulations and simple means for the total sample a
included on this fıgure).
The team examined how the effectiveness of point-of-
decision prompts, measured in units of absolute change
varied with baseline stair use and found no signifıcant
relationship between baseline stairuse and absolute
change (Spearman’srho ⫺⫽ 0.39,n⫽21 data points,
p⫽0.77).
The team also examined the effectiveness of point-of-
decision prompts by the period of observation. Research
ers in nine of the studies(representing18 study
arms)13,17–20,25–27
left point-of-decision prompts in place
and observed passersby for different lengths of time, wit
observation periodsranging from 1 week (relative
change⫽81.1%)26to 12 weeks (relative change⫽5.16%).25
The period of observation was not reported for two quali
ing studies representing three study arms.14,15
There was no
signifıcant relationship between the period of observatio
and relative change in stair use (Spearman’s rho ⫺⫽ 0.12
n⫽18 data points, p⫽0.65).
Overall, 25 of the 28 data points representing 17 study
arms (ten studies) in this body of evidence reported fınd
ings in favor of the intervention.For some studies the
statistical signifıcance of the results was not reported, an
for some, the fındings differed by direction for subgroup
Among those studies with fındings in favor of the inter-
vention, at the individual level the actual increase in sta
use was modest. Because using stairs is a physical activ
that can be done by most people in most places where
stairs are present,modest increases in stair use among
populations ofadults across settings (malls,worksites,
libraries,and other such facilities) and across time can
contribute to or extend bouts of physical activity and ma
have a positive effect on energy balance.
Applicability.The body of evidence used to evaluate the
applicability ofthis intervention was the same as that
used to evaluate effectiveness.Seven studies were con-
ducted in the U.S.,14,15,17–19,26,27
two were conducted in
the United Kingdom,13,20
and one study each was con-
ducted in Scotland specifıcally16 and in Australia.25
Point-of-decision prompts were evaluated in a range of
settings, and two studies investigated the effectiveness
the same intervention in different locations.18,19
Baseline
use of stairs differed across settings (e.g., buildings with
single or multiple flights of stairs,public locations and
worksites), and the effectiveness of the intervention also
varied across settings,suggesting that the goal (e.g.,lei-
sure activity or work), or type of dress (e.g., suit or work
shoes) of people in certain types of locations may have a
impact on the effectiveness of the intervention.
S296 Soler et al / Am J Prev Med 2010;38(2S):S292–S300
www.ajpm-online.net
were of good execution;the re-
maining nine13–18,20,26,27
were rated as fair.One addi-
tionalpaper provided information on a study already
included in the review.28 Details ofthe 11 qualifying
studies,including a summary ofthe content,delivery,
evaluation design,and outcomes,are available at www.
thecommunityguide.org/pa/environmental-policy/
podp.html.
Study design and implementationcharacteris-
tics. All 11 qualifying studies used time–series designs,
and were rated as being of moderate suitability.13–20,25–27
All of the qualifying studies were conducted between
1980 and 2003, and measured stair use in adult popula-
tions. The types of point-of-decision prompts used in the
qualifyingstudiesweresigns13–19,26,27
or banners,20
which were distinctions used by the authors and not
necessarily related to the size of the prompt, although in
the one study specifying stair banners, the messages were
physically placed on each stair, but like the signs, varied in
design and message.The 11 qualifying studies imple-
mented a variety of point-of-decision prompts messages
such as health benefıts and health promotion,13,14,16 –18,25
weight control,14 and signs (in Spanish and English)
using eitheran individualor family perspective to
specifıcally targetthe Hispanic community.19 One
study focused primarily on African-Americans,and
the point-of-decision prompt was tailored to this partic-
ular community.15Additionally, in one study a deterrent
sign was displayed that limited the elevator to use by the
staff and the physically challenged.26
Outcomes Related to Stair Use
Eleven qualifying studies,13–20,25–27
consisting of 21 study
arms for stair use, provided evidence in terms of absolute
(i.e., percentage point) change. In these studies, the base-
line rates of stair use ranged from 1.7% to 39.7% of po-
tential users (median⫽8.2, IQI⫽5.2, 21.2). Stair use dur-
ing the intervention period in these study arms ranged
from 4.0% to 41.9% ofpotentialusers.The median
change for the 21 study arms representing these studies
was an increase in stair use of2.4 percentage points
(IQI⫽0.83, 6.7 percentage points).Increases in stair
use in 15 of 21 study arms were reported as statistically
signifıcant,14 –20,22–28
while two study arms (from the
same study)reported a signifıcantdecrease in stair
use.19
To examine effects relative to baseline stair use, eleven
qualifying studies that included 21 study arms for stair
use were evaluated in terms of relative (i.e., percentage)
change.13–20,25–27
The majority of studies reported a low
levelof baseline stair use (⬍20%).Overall,in the 11
qualifying studies,the median relative improvement in
observed stair use was 50 percentage points (IQI⫽5.4%,
90.6%) from baseline (Figure 2; note that data points for
subpopulations and simple means for the total sample a
included on this fıgure).
The team examined how the effectiveness of point-of-
decision prompts, measured in units of absolute change
varied with baseline stair use and found no signifıcant
relationship between baseline stairuse and absolute
change (Spearman’srho ⫺⫽ 0.39,n⫽21 data points,
p⫽0.77).
The team also examined the effectiveness of point-of-
decision prompts by the period of observation. Research
ers in nine of the studies(representing18 study
arms)13,17–20,25–27
left point-of-decision prompts in place
and observed passersby for different lengths of time, wit
observation periodsranging from 1 week (relative
change⫽81.1%)26to 12 weeks (relative change⫽5.16%).25
The period of observation was not reported for two quali
ing studies representing three study arms.14,15
There was no
signifıcant relationship between the period of observatio
and relative change in stair use (Spearman’s rho ⫺⫽ 0.12
n⫽18 data points, p⫽0.65).
Overall, 25 of the 28 data points representing 17 study
arms (ten studies) in this body of evidence reported fınd
ings in favor of the intervention.For some studies the
statistical signifıcance of the results was not reported, an
for some, the fındings differed by direction for subgroup
Among those studies with fındings in favor of the inter-
vention, at the individual level the actual increase in sta
use was modest. Because using stairs is a physical activ
that can be done by most people in most places where
stairs are present,modest increases in stair use among
populations ofadults across settings (malls,worksites,
libraries,and other such facilities) and across time can
contribute to or extend bouts of physical activity and ma
have a positive effect on energy balance.
Applicability.The body of evidence used to evaluate the
applicability ofthis intervention was the same as that
used to evaluate effectiveness.Seven studies were con-
ducted in the U.S.,14,15,17–19,26,27
two were conducted in
the United Kingdom,13,20
and one study each was con-
ducted in Scotland specifıcally16 and in Australia.25
Point-of-decision prompts were evaluated in a range of
settings, and two studies investigated the effectiveness
the same intervention in different locations.18,19
Baseline
use of stairs differed across settings (e.g., buildings with
single or multiple flights of stairs,public locations and
worksites), and the effectiveness of the intervention also
varied across settings,suggesting that the goal (e.g.,lei-
sure activity or work), or type of dress (e.g., suit or work
shoes) of people in certain types of locations may have a
impact on the effectiveness of the intervention.
S296 Soler et al / Am J Prev Med 2010;38(2S):S292–S300
www.ajpm-online.net
The studies included in this review were conducted in
shopping malls,14,18,20
train and bus stations,15,16,18
air-
ports,19,26
an offıce building,19a bank,19a healthcare fa-
cility,25a medical school,13a university,17and a univer-
sity library.19,27 Four studies13,17,19,25
specifıed that
workers were included among those observed. Although
some locations may have had a greater percentage of
workers present (e.g.,offıce buildings and universities)
than others (e.g.,airports and malls),it is likely that
workers were present in all places included in this review.
Six studies,representing 13 study arms,14,16,19,20,26,27
measuredeffectivenessseparatelyamongmen and
women (median relative percentage change equaled 33%
and 48%, respectively) and found that point-of-decision
prompts had similar effects for both groups.Addition-
ally,age was measured in fıve studies representing ten
study arms.14,18,20,26,27
All studies included adult-only
samples, and study authors grouped individuals into ei-
ther young or old adults (median relative percentage
change equals 51% and 65%, respectively). Age groupings
varied by study with three using age 30 years as a cutoff
point for the younger group14,18,27
and one using age 40
years as a cutoffpointfor the younger group.26 Two
studies used age 60 years to distinguish between their
younger and older groups.20,27
No studies examined the
effectiveness of the intervention in changing the beha
of children or adolescents. Four studies, with eight stu
arms,14,15,18,20
measured effectiveness for whites and Af-
rican Americans and found no difference between raci
groups(median relative percentage change⫽53% for
each group). The team therefore believed that this typ
intervention is likely to be effective across diverse set
and population groups,provided thatthe appropriate
care is taken to adapt the messages15,19
for each setting or
population.However,stair use may vary according to
environmental characteristics (e.g., accessibility of sta
number of flights to destination,or cleanliness of stair-
well) and personal factors (e.g., body composition, pre
ence of children or heavy loads) of the targeted popul
tion, which may affect responsiveness to the intervent
Other positive or negative effects.One study reported
nonsignifıcantchanges in elevator use consistentwith
changes in stair use (lift use decreased as stair use in
creased),13 which may result in reduced electricity use
and related costs. Potential harms of increased stair u
include strains and sprains, as well as injuries due to f
In addition, one author noted that “posting a sign exto
Figure 2.Relative change in percentage ofpeople using stairs when point-of-decision prompts are displayed (n⫽35
measurements from 21 study arms in 11 qualifying studies). Some studies have multiple study arms so are repea
Soler et al / Am J Prev Med 2010;38(2S):S292–S300 S297
February 2010
shopping malls,14,18,20
train and bus stations,15,16,18
air-
ports,19,26
an offıce building,19a bank,19a healthcare fa-
cility,25a medical school,13a university,17and a univer-
sity library.19,27 Four studies13,17,19,25
specifıed that
workers were included among those observed. Although
some locations may have had a greater percentage of
workers present (e.g.,offıce buildings and universities)
than others (e.g.,airports and malls),it is likely that
workers were present in all places included in this review.
Six studies,representing 13 study arms,14,16,19,20,26,27
measuredeffectivenessseparatelyamongmen and
women (median relative percentage change equaled 33%
and 48%, respectively) and found that point-of-decision
prompts had similar effects for both groups.Addition-
ally,age was measured in fıve studies representing ten
study arms.14,18,20,26,27
All studies included adult-only
samples, and study authors grouped individuals into ei-
ther young or old adults (median relative percentage
change equals 51% and 65%, respectively). Age groupings
varied by study with three using age 30 years as a cutoff
point for the younger group14,18,27
and one using age 40
years as a cutoffpointfor the younger group.26 Two
studies used age 60 years to distinguish between their
younger and older groups.20,27
No studies examined the
effectiveness of the intervention in changing the beha
of children or adolescents. Four studies, with eight stu
arms,14,15,18,20
measured effectiveness for whites and Af-
rican Americans and found no difference between raci
groups(median relative percentage change⫽53% for
each group). The team therefore believed that this typ
intervention is likely to be effective across diverse set
and population groups,provided thatthe appropriate
care is taken to adapt the messages15,19
for each setting or
population.However,stair use may vary according to
environmental characteristics (e.g., accessibility of sta
number of flights to destination,or cleanliness of stair-
well) and personal factors (e.g., body composition, pre
ence of children or heavy loads) of the targeted popul
tion, which may affect responsiveness to the intervent
Other positive or negative effects.One study reported
nonsignifıcantchanges in elevator use consistentwith
changes in stair use (lift use decreased as stair use in
creased),13 which may result in reduced electricity use
and related costs. Potential harms of increased stair u
include strains and sprains, as well as injuries due to f
In addition, one author noted that “posting a sign exto
Figure 2.Relative change in percentage ofpeople using stairs when point-of-decision prompts are displayed (n⫽35
measurements from 21 study arms in 11 qualifying studies). Some studies have multiple study arms so are repea
Soler et al / Am J Prev Med 2010;38(2S):S292–S300 S297
February 2010
ling the benefıts of climbing one flight of stairs may con-
vey false information. It may lead people to believe that a
single 30-second climb willsubstantially improve their
health.”29
Economic efficiency.For this updated review, a search
of literature on economic effectiveness was conducted.
No studies were found thatmetthe requirements for
inclusion in a Community Guide review.30
Barriers to intervention implementation.Few studies
reviewed indicated specifıc barriers to successful imple-
mentation of the intervention. One author reported un-
authorized removalof prompts from stairwells.13 An-
otherreported thatthe flooron which an employee
worked affected stair use, suggesting that the more stairs
one has to ascend,the less effective the intervention
might be.24Additionally, some stairwells are locked and
others may be diffıcultto fınd,poorly lit,or notwell
maintained.17Some institutions may have fıre codes and
other policies restricting the placement ofprompts or
posters in public areas. Choice of dress (e.g., high-heeled
shoes) may also serve as barriers to stair use and may
increase general risk of using the stairs.
Summary and Discussion: Effectiveness
of Point-of-Decision Prompts
In general, the qualifying studies identifıed in this review
reported a low level of observed baseline use of stairs, and
small but signifıcant increases in the use of stairs follow-
ing the implementation ofpoint-of-decision prompts.
Although absolute changes were small, these differences
representmodestrelative improvements in the use of
stairs. In general, the lower the level of baseline use, the
greater the improvements in use. The duration of obser-
vation reported in the qualifying studies was relatively
short, with a maximum observation period of 12 weeks.
The team had little evidence with which to evaluate the
long-term impact of these interventions on stair use, and
there was no signifıcant association between length of
observation periods and changes in stair use.
The venue in which the prompt is placed may also
influence the amount of exposure. Some locations, such
as malls and airports,have populations that (with the
exception of a limited number of employees) likely do not
return from one day to the next; whereas other locations,
such as offıce buildings and commuter train stations,
likely have populations that return—and therefore are
exposed to the prompts— day after day.None of these
studies examined the impact that repeated exposure to
prompts may have on stair use— clearly an area for future
research.
Conclusion
According to Community Guide rules of evidence,7 this
review provides strong evidence that point-of-decision
prompts contribute to modest increases in the percentag
of people choosing to take the stairs rather than an elev
tor or escalator. The observed increases in the use of sta
may contribute to a modest improvement in daily physi-
cal activity that would have a cumulative effect on calor
expenditure and, in turn, energy balance.
Review of Evidence: Stair or Stairwell
Enhancements when Combined with
Point-of-Decision Prompts
Enhancement of stairs or stairwells when combined with
point-of-decision prompts was also examined as part of
this update review. This intervention includes modifying
stairwells through one or more of the following: painting
walls, laying carpet, adding artwork, and playing music.
This intervention may indirectly increase the effective-
ness of point-of-decision prompts by changing attitudes
about stair use (or a particular stairwell).
Effectiveness.The team identifıed two studies17,31
that
assessed theeffectivenessof stairwellenhancements
when combined with point-of-decision promptsin
changing frequency of stair use,as measured by mean
number of trips per person per day and percentage of
people using the stairs. Both of these studies used time–
series designs, were rated as moderate in suitability, an
were evaluated as being of fair execution. Details of the
two qualifying studies, including a summary of the con-
tent, delivery, evaluation design, and outcomes, are ava
able atwww.thecommunityguide.org/pa/environmental-
policy/podp.html.
Study design and implementationcharacteris-
tics. Both studies reviewed investigated the impact of
environmental change on stair use. One study31reported
a long-term evaluation during which a stairwellwas
painted and carpeted,artwork was placed on the walls
of landings,point-of-decision promptswereposted
throughout the building and on the computer kiosk in th
lobby, and fınally, music was piped in. This intervention
was implemented in stages where cumulative effects we
examined (effectiveness was evaluated after new carpet
and paint were added,and then again after adding art-
work). In the second study, the effectiveness of prompts
alone and the effectiveness of prompts plus adding art-
work and music to the stairwell were examined.17For this
study, the prompts-alone condition was included in the
review described above. One study was conducted in an
offıce building31and the other was conducted in a univer-
sity building.17Both studies were conducted in the U.S.
S298 Soler et al / Am J Prev Med 2010;38(2S):S292–S300
www.ajpm-online.net
vey false information. It may lead people to believe that a
single 30-second climb willsubstantially improve their
health.”29
Economic efficiency.For this updated review, a search
of literature on economic effectiveness was conducted.
No studies were found thatmetthe requirements for
inclusion in a Community Guide review.30
Barriers to intervention implementation.Few studies
reviewed indicated specifıc barriers to successful imple-
mentation of the intervention. One author reported un-
authorized removalof prompts from stairwells.13 An-
otherreported thatthe flooron which an employee
worked affected stair use, suggesting that the more stairs
one has to ascend,the less effective the intervention
might be.24Additionally, some stairwells are locked and
others may be diffıcultto fınd,poorly lit,or notwell
maintained.17Some institutions may have fıre codes and
other policies restricting the placement ofprompts or
posters in public areas. Choice of dress (e.g., high-heeled
shoes) may also serve as barriers to stair use and may
increase general risk of using the stairs.
Summary and Discussion: Effectiveness
of Point-of-Decision Prompts
In general, the qualifying studies identifıed in this review
reported a low level of observed baseline use of stairs, and
small but signifıcant increases in the use of stairs follow-
ing the implementation ofpoint-of-decision prompts.
Although absolute changes were small, these differences
representmodestrelative improvements in the use of
stairs. In general, the lower the level of baseline use, the
greater the improvements in use. The duration of obser-
vation reported in the qualifying studies was relatively
short, with a maximum observation period of 12 weeks.
The team had little evidence with which to evaluate the
long-term impact of these interventions on stair use, and
there was no signifıcant association between length of
observation periods and changes in stair use.
The venue in which the prompt is placed may also
influence the amount of exposure. Some locations, such
as malls and airports,have populations that (with the
exception of a limited number of employees) likely do not
return from one day to the next; whereas other locations,
such as offıce buildings and commuter train stations,
likely have populations that return—and therefore are
exposed to the prompts— day after day.None of these
studies examined the impact that repeated exposure to
prompts may have on stair use— clearly an area for future
research.
Conclusion
According to Community Guide rules of evidence,7 this
review provides strong evidence that point-of-decision
prompts contribute to modest increases in the percentag
of people choosing to take the stairs rather than an elev
tor or escalator. The observed increases in the use of sta
may contribute to a modest improvement in daily physi-
cal activity that would have a cumulative effect on calor
expenditure and, in turn, energy balance.
Review of Evidence: Stair or Stairwell
Enhancements when Combined with
Point-of-Decision Prompts
Enhancement of stairs or stairwells when combined with
point-of-decision prompts was also examined as part of
this update review. This intervention includes modifying
stairwells through one or more of the following: painting
walls, laying carpet, adding artwork, and playing music.
This intervention may indirectly increase the effective-
ness of point-of-decision prompts by changing attitudes
about stair use (or a particular stairwell).
Effectiveness.The team identifıed two studies17,31
that
assessed theeffectivenessof stairwellenhancements
when combined with point-of-decision promptsin
changing frequency of stair use,as measured by mean
number of trips per person per day and percentage of
people using the stairs. Both of these studies used time–
series designs, were rated as moderate in suitability, an
were evaluated as being of fair execution. Details of the
two qualifying studies, including a summary of the con-
tent, delivery, evaluation design, and outcomes, are ava
able atwww.thecommunityguide.org/pa/environmental-
policy/podp.html.
Study design and implementationcharacteris-
tics. Both studies reviewed investigated the impact of
environmental change on stair use. One study31reported
a long-term evaluation during which a stairwellwas
painted and carpeted,artwork was placed on the walls
of landings,point-of-decision promptswereposted
throughout the building and on the computer kiosk in th
lobby, and fınally, music was piped in. This intervention
was implemented in stages where cumulative effects we
examined (effectiveness was evaluated after new carpet
and paint were added,and then again after adding art-
work). In the second study, the effectiveness of prompts
alone and the effectiveness of prompts plus adding art-
work and music to the stairwell were examined.17For this
study, the prompts-alone condition was included in the
review described above. One study was conducted in an
offıce building31and the other was conducted in a univer-
sity building.17Both studies were conducted in the U.S.
S298 Soler et al / Am J Prev Med 2010;38(2S):S292–S300
www.ajpm-online.net
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Outcomes related to stair use.There was not enough
evidence in this body of literature to draw conclusions
about effectiveness.In the study conducted in an offıce
building,all interventions (paint,carpet,art,signs,and
music) together led to a relative increase in stair use of
8.8% (baseline use: M⫽2.14 trips per day per occupant).31
The other study examined the effectiveness of point-of-
decision prompts with artwork and music and reported a
39.6% relative increase in stair use (percentage of people
using stairs at baseline: 11.1%).17
Barriers to intervention implementation.Fire code
regulations may limit or preclude enhancements to stairs
and stairwells.The qualifying studies did notprovide
additional information on barriers to implementation of
these interventions.
Conclusion
According to the Community Guide’s rules of evidence,7
there is insuffıcient evidence to determine the effective-
ness of point-of-decision prompts in encouraging stair
use when combined with stair or stairwell enhancements.
Two studies of moderate suitability were identifıed.Al-
though both observed improvements in stair use over the
period ofobservation (relative percentage changes of
8.8% in trips per person per day and 39.6% of people
using the stairs),more research is needed to determine
the effects of this intervention on stair use.
Research Issues
Informationalapproachesto increasingphysical
activity.
Effectiveness.This review established the effectiveness
of point-of-decision promptsto encourage stairuse.
However, important research issues regarding the effec-
tiveness ofthese interventions remain.Many research
questions from the fırstCommunity Guide review of
point-of-decision prompts5have been addressed in more
recent studies.However,some questions have not been
addressed and others emerged from this update.
● What effect does varying the message or format of the
prompthave on providing a “booster” to stair use
among the targeted population?
● What type of prompt is most effective? What effect
does format or size have, if any?
● Is there a “critical distance” from the elevator or esca-
lator to the stairs, in which the effect of signage on stair
use is reduced?
● Are there a minimum or maximum number of flights
one must expect stair users to ascend in order for the
prompt to be effective?
● How many individualsread thepoint-of-decision
prompt and react (i.e., increase their use of the stair
a result, as opposed to reacting to other knowledge
the intervention is occurring?
● What strategies can be used to maintain the interve
tion effect after the intervention ends? Are periodic
“boosters” necessary or helpful?
Economic evaluations.The available economic data
were limited.Therefore,considerable research is war-
ranted on the following questions.
● What is the cost effectiveness of each of these seem
ingly low-cost interventions?
● How can effectiveness in terms of health outcomes o
quality adjusted health outcomes be better measure
estimated, or modeled?
Summary
In this article, the team reported results from an upda
review ofpoint-of-decision prompts thatincluded an
additional review of stair or stairwell enhancements w
used with point-of-decision prompts.The inclusion of
more recent studies provides strong evidence of effec
ness of the point-of-decision prompt intervention in in
creasing the use of stairs. On average these improvem
represent a modest improvement in stair use.Point-of-
decision prompts may represent a simple, lower-cost o
tion to increase physical activity in some settings. The
was insuffıcient evidence to draw a conclusion regardi
the effectiveness of stair or stairwell enhancements w
used with point-of-decision prompts. Despite the inclu
sion of additional studies, there remain important gap
understanding of the effectiveness of these interventi
in some settings (such as worksites), and the contribu
of these interventions to overallphysicalactivity and
physical fıtness.
The team thanks the following individuals for their con
tributions to this review: Reba Norman, research librar
ian;Kate W.Harris and Tony Pearson-Clarke,editors;
and the team’s Coordination Team:Nico Pronk,PhD,
Health Partners, Minneapolis MN; Dennis Richling, MD,
CorSolutions, Chicago IL; Deborah R. Bauer, RN, MPH,
NationalCenter for Chronic Disease Prevention and
Health Promotion, CDC, Atlanta GA; Andrew Walker,
Private Consultant,Atlanta GA; Abby Rosenthal,
MPH, Offıce on Smoking and Health, CDC, Atlanta GA;
Curtis S.Florence,II PhD, Emory University,Atlanta
GA; and Deborah MacLean,The Coca-Cola Company,
Atlanta GA.
The names and affıliations of the Task Force membe
are listed in the front of this supplementand at
www.thecommunityguide.org.
Soler et al / Am J Prev Med 2010;38(2S):S292–S300 S299
February 2010
evidence in this body of literature to draw conclusions
about effectiveness.In the study conducted in an offıce
building,all interventions (paint,carpet,art,signs,and
music) together led to a relative increase in stair use of
8.8% (baseline use: M⫽2.14 trips per day per occupant).31
The other study examined the effectiveness of point-of-
decision prompts with artwork and music and reported a
39.6% relative increase in stair use (percentage of people
using stairs at baseline: 11.1%).17
Barriers to intervention implementation.Fire code
regulations may limit or preclude enhancements to stairs
and stairwells.The qualifying studies did notprovide
additional information on barriers to implementation of
these interventions.
Conclusion
According to the Community Guide’s rules of evidence,7
there is insuffıcient evidence to determine the effective-
ness of point-of-decision prompts in encouraging stair
use when combined with stair or stairwell enhancements.
Two studies of moderate suitability were identifıed.Al-
though both observed improvements in stair use over the
period ofobservation (relative percentage changes of
8.8% in trips per person per day and 39.6% of people
using the stairs),more research is needed to determine
the effects of this intervention on stair use.
Research Issues
Informationalapproachesto increasingphysical
activity.
Effectiveness.This review established the effectiveness
of point-of-decision promptsto encourage stairuse.
However, important research issues regarding the effec-
tiveness ofthese interventions remain.Many research
questions from the fırstCommunity Guide review of
point-of-decision prompts5have been addressed in more
recent studies.However,some questions have not been
addressed and others emerged from this update.
● What effect does varying the message or format of the
prompthave on providing a “booster” to stair use
among the targeted population?
● What type of prompt is most effective? What effect
does format or size have, if any?
● Is there a “critical distance” from the elevator or esca-
lator to the stairs, in which the effect of signage on stair
use is reduced?
● Are there a minimum or maximum number of flights
one must expect stair users to ascend in order for the
prompt to be effective?
● How many individualsread thepoint-of-decision
prompt and react (i.e., increase their use of the stair
a result, as opposed to reacting to other knowledge
the intervention is occurring?
● What strategies can be used to maintain the interve
tion effect after the intervention ends? Are periodic
“boosters” necessary or helpful?
Economic evaluations.The available economic data
were limited.Therefore,considerable research is war-
ranted on the following questions.
● What is the cost effectiveness of each of these seem
ingly low-cost interventions?
● How can effectiveness in terms of health outcomes o
quality adjusted health outcomes be better measure
estimated, or modeled?
Summary
In this article, the team reported results from an upda
review ofpoint-of-decision prompts thatincluded an
additional review of stair or stairwell enhancements w
used with point-of-decision prompts.The inclusion of
more recent studies provides strong evidence of effec
ness of the point-of-decision prompt intervention in in
creasing the use of stairs. On average these improvem
represent a modest improvement in stair use.Point-of-
decision prompts may represent a simple, lower-cost o
tion to increase physical activity in some settings. The
was insuffıcient evidence to draw a conclusion regardi
the effectiveness of stair or stairwell enhancements w
used with point-of-decision prompts. Despite the inclu
sion of additional studies, there remain important gap
understanding of the effectiveness of these interventi
in some settings (such as worksites), and the contribu
of these interventions to overallphysicalactivity and
physical fıtness.
The team thanks the following individuals for their con
tributions to this review: Reba Norman, research librar
ian;Kate W.Harris and Tony Pearson-Clarke,editors;
and the team’s Coordination Team:Nico Pronk,PhD,
Health Partners, Minneapolis MN; Dennis Richling, MD,
CorSolutions, Chicago IL; Deborah R. Bauer, RN, MPH,
NationalCenter for Chronic Disease Prevention and
Health Promotion, CDC, Atlanta GA; Andrew Walker,
Private Consultant,Atlanta GA; Abby Rosenthal,
MPH, Offıce on Smoking and Health, CDC, Atlanta GA;
Curtis S.Florence,II PhD, Emory University,Atlanta
GA; and Deborah MacLean,The Coca-Cola Company,
Atlanta GA.
The names and affıliations of the Task Force membe
are listed in the front of this supplementand at
www.thecommunityguide.org.
Soler et al / Am J Prev Med 2010;38(2S):S292–S300 S299
February 2010
No fınancial disclosures were reported by the authors
of this paper.
References
1. Ogden CL, Carrol MD, Curtin LR, McDowell MA, Tabak CJ,
Flegal KM. Prevalence of overweight and obesity in the U.S.,
1999 –2004. JAMA 2006;295(13):1549 –55.
2. CDC. Overweightand obesity:an overview.www.cdc.gov/
nccdphp/dnpa/obesity/contributing_factors.htm.
3. USDHHS. The Surgeon General’s call to action to prevent and
decrease overweightand obesity.www.surgeongeneral.gov/
topics/obesity/.
4. U.S. Preventive Services Task Force. Guide to Clinical Preven-
tive Services: report of the U.S. Preventive Services Task Force.
2nd ed. Baltimore: Williams & Wilkins, 1996.
5. Kahn EB, Ramsey LT, Brownson RC, et al. The effectiveness of
interventions to increase physical activity: a systematic review.
Am J Prev Med 2002;22(4S):S73–107.
6. Task Force on Community Preventive Services.Recommen-
dations to increase physical activity in communities. Am J Prev
Med 2002;22(4S):S67–72.
7. BrissPA, Zaza S,Pappaioanou M,et al. Developing an
evidence-based Guide to Community Preventive Services—
methods. Am J Prev Med 2000;18(1S):S35– 43.
8. Lanningham-Foster L, Nysse LJ, Levine JA. Labor saved, calo-
ries lost:the energenic impact of domestic labor-saving de-
vices. Obes Res 2003;11(10):1178 – 81.
9. Teh KC, Aziz AR. Heart rate, oxygen uptake, and energy cost
of ascending and descending the stairs. Med Sci Sports Exerc
2002;34(4):695–9.
10. Boreham CAG,Wallace WFM,NevillA. Training effects of
accumulated daily stair-climbing excercise in previously sed-
entary young women. Prev Med 2000;30:277– 81.
11. Benn SJ, McCartney N, McKelvie RS. Circulatory responses to
weight lifting, walking, and stair climbing in older males. J Am
Geriatr Soc 1996;44(2):121–5.
12. Zaza S, Wright-De Aguero LK, Briss PA, et al. Data collection
instrument and procedure for systematic reviews in the Guide
to Community Preventive Services.Am J Prev Med 2000;
18(1S):44 –74.
13. Adams J, White M. A systematic approach to the development
and evaluation of an intervention promoting stair use. Health
Educ J 2002;61(3):272– 86.
14. Andersen RE, Franckowiak SC, Snyder J, Bartlett SJ, Fontaine
KR. Can inexpensive signs encourage the use of stairs? Results
from a community intervention.Ann Intern Med 1998;
129(5):363–9.
15. Andersen RE,Franckowiak SC,Zuzak KB,Cummings ES,
Crespo CJ.Community intervention to encourage stair use
among African American commuters.Med Sci Sports Exerc
2000;32:38.
16. Blamey A,Mutrie N,Aitchison T.Health promotion by en-
couraged use of stairs. Br Med J 1995;311(7000):289 –90.
17. Boutelle KN,Jeffery RW,Murray DM,Schmitz MK.Using
signs,artwork,and music to promote stair use in a public
building. Am J Public Health 2001;91(12):2004 – 6.
18. Brownell KD, Stunkard AJ, Albaum JM. Evaluation and mod-
ifıcation of exercise patterns in the natural environment. Am J
Psychiatry 1980;137(12):1540 –5.
19. Coleman KJ,Gonzalez EC.Promoting stair use in a U.S.–
Mexico border community. Am J Public Health 2001;91(12):
2007–9.
20. Kerr J, Eves F, Carroll D. Getting more people on the stairs: th
impact of a new message format. J Health Psychol 2001;6(5):
495–500.
21. Kerr J, Eves F,CarrollD. Encouraging stair use:stair-riser
bannersare betterthan posters.Am J Public Health
2001;91(8):1192–3.
22. Kerr J, Eves F, Carroll D. Posters can prompt less active people
to use the stairs. J Epidemiol Community Health 2000;54(12):
942–3.
23. Kerr J, Eves FF, Carroll D. The influence of poster prompts on
stair use:the effects of setting,poster size and content.Br J
Health Psychol 2001;6(Pt 4):397– 405.
24. Kerr J,Eves F,Carroll D.Can posters prompt stair use in a
worksite environment? J Occup Health 2001;43(4):205–7.
25. MarshallAL, Bauman AE,Patch C,Wilson J,Chen J.Can
motivational signs prompt increases in incidental physical ac-
tivity in an Australian healthcare facility? Health Educ Res
2002;17(6):743–9.
26. Russell WD, Hutchinson J. Comparison of health promotion
and deterrent prompts in increasing use of stairs over escala-
tors. Percept Mot Skills 2000;91(1):55– 61.
27. Russell WD, Dzewaltowski DA, Ryan GJ. The effectiveness of a
point-of-decision promptin deterring sedentary behavior.
Am J Health Promot 1999;13(5):257–9.
28. Kerr J,Eves F,CarrollD. Six-month observationalstudy of
prompted stair climbing. Prev Med 2001;33(5):422–7.
29. Reisman A,Gross CP.Increasing stair use.Ann Intern Med
1999;130(7):616 –7.
30. Carande-Kulis VG, Maciosek MV, Briss PA, et al. Methods for
systematic reviews of economic evaluations for the Guide to
CommunityPreventiveServices.Am J Prev Med 2000;
18(1S):S75–91.
31. Kerr NA, Yore MM, Ham SA, Dietz WH. Increasing stair use
in a worksite through environmentalchanges.Am J Health
Promot 2004;18(4):312–5.
S300 Soler et al / Am J Prev Med 2010;38(2S):S292–S300
www.ajpm-online.net
of this paper.
References
1. Ogden CL, Carrol MD, Curtin LR, McDowell MA, Tabak CJ,
Flegal KM. Prevalence of overweight and obesity in the U.S.,
1999 –2004. JAMA 2006;295(13):1549 –55.
2. CDC. Overweightand obesity:an overview.www.cdc.gov/
nccdphp/dnpa/obesity/contributing_factors.htm.
3. USDHHS. The Surgeon General’s call to action to prevent and
decrease overweightand obesity.www.surgeongeneral.gov/
topics/obesity/.
4. U.S. Preventive Services Task Force. Guide to Clinical Preven-
tive Services: report of the U.S. Preventive Services Task Force.
2nd ed. Baltimore: Williams & Wilkins, 1996.
5. Kahn EB, Ramsey LT, Brownson RC, et al. The effectiveness of
interventions to increase physical activity: a systematic review.
Am J Prev Med 2002;22(4S):S73–107.
6. Task Force on Community Preventive Services.Recommen-
dations to increase physical activity in communities. Am J Prev
Med 2002;22(4S):S67–72.
7. BrissPA, Zaza S,Pappaioanou M,et al. Developing an
evidence-based Guide to Community Preventive Services—
methods. Am J Prev Med 2000;18(1S):S35– 43.
8. Lanningham-Foster L, Nysse LJ, Levine JA. Labor saved, calo-
ries lost:the energenic impact of domestic labor-saving de-
vices. Obes Res 2003;11(10):1178 – 81.
9. Teh KC, Aziz AR. Heart rate, oxygen uptake, and energy cost
of ascending and descending the stairs. Med Sci Sports Exerc
2002;34(4):695–9.
10. Boreham CAG,Wallace WFM,NevillA. Training effects of
accumulated daily stair-climbing excercise in previously sed-
entary young women. Prev Med 2000;30:277– 81.
11. Benn SJ, McCartney N, McKelvie RS. Circulatory responses to
weight lifting, walking, and stair climbing in older males. J Am
Geriatr Soc 1996;44(2):121–5.
12. Zaza S, Wright-De Aguero LK, Briss PA, et al. Data collection
instrument and procedure for systematic reviews in the Guide
to Community Preventive Services.Am J Prev Med 2000;
18(1S):44 –74.
13. Adams J, White M. A systematic approach to the development
and evaluation of an intervention promoting stair use. Health
Educ J 2002;61(3):272– 86.
14. Andersen RE, Franckowiak SC, Snyder J, Bartlett SJ, Fontaine
KR. Can inexpensive signs encourage the use of stairs? Results
from a community intervention.Ann Intern Med 1998;
129(5):363–9.
15. Andersen RE,Franckowiak SC,Zuzak KB,Cummings ES,
Crespo CJ.Community intervention to encourage stair use
among African American commuters.Med Sci Sports Exerc
2000;32:38.
16. Blamey A,Mutrie N,Aitchison T.Health promotion by en-
couraged use of stairs. Br Med J 1995;311(7000):289 –90.
17. Boutelle KN,Jeffery RW,Murray DM,Schmitz MK.Using
signs,artwork,and music to promote stair use in a public
building. Am J Public Health 2001;91(12):2004 – 6.
18. Brownell KD, Stunkard AJ, Albaum JM. Evaluation and mod-
ifıcation of exercise patterns in the natural environment. Am J
Psychiatry 1980;137(12):1540 –5.
19. Coleman KJ,Gonzalez EC.Promoting stair use in a U.S.–
Mexico border community. Am J Public Health 2001;91(12):
2007–9.
20. Kerr J, Eves F, Carroll D. Getting more people on the stairs: th
impact of a new message format. J Health Psychol 2001;6(5):
495–500.
21. Kerr J, Eves F,CarrollD. Encouraging stair use:stair-riser
bannersare betterthan posters.Am J Public Health
2001;91(8):1192–3.
22. Kerr J, Eves F, Carroll D. Posters can prompt less active people
to use the stairs. J Epidemiol Community Health 2000;54(12):
942–3.
23. Kerr J, Eves FF, Carroll D. The influence of poster prompts on
stair use:the effects of setting,poster size and content.Br J
Health Psychol 2001;6(Pt 4):397– 405.
24. Kerr J,Eves F,Carroll D.Can posters prompt stair use in a
worksite environment? J Occup Health 2001;43(4):205–7.
25. MarshallAL, Bauman AE,Patch C,Wilson J,Chen J.Can
motivational signs prompt increases in incidental physical ac-
tivity in an Australian healthcare facility? Health Educ Res
2002;17(6):743–9.
26. Russell WD, Hutchinson J. Comparison of health promotion
and deterrent prompts in increasing use of stairs over escala-
tors. Percept Mot Skills 2000;91(1):55– 61.
27. Russell WD, Dzewaltowski DA, Ryan GJ. The effectiveness of a
point-of-decision promptin deterring sedentary behavior.
Am J Health Promot 1999;13(5):257–9.
28. Kerr J,Eves F,CarrollD. Six-month observationalstudy of
prompted stair climbing. Prev Med 2001;33(5):422–7.
29. Reisman A,Gross CP.Increasing stair use.Ann Intern Med
1999;130(7):616 –7.
30. Carande-Kulis VG, Maciosek MV, Briss PA, et al. Methods for
systematic reviews of economic evaluations for the Guide to
CommunityPreventiveServices.Am J Prev Med 2000;
18(1S):S75–91.
31. Kerr NA, Yore MM, Ham SA, Dietz WH. Increasing stair use
in a worksite through environmentalchanges.Am J Health
Promot 2004;18(4):312–5.
S300 Soler et al / Am J Prev Med 2010;38(2S):S292–S300
www.ajpm-online.net
1 out of 9
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.