Exploring CAM Use Among Adult Sickle Cell Patients for Pain Relief
VerifiedAdded on 2023/04/23
|6
|5474
|84
Report
AI Summary
This report investigates the use of complementary and alternative medicine (CAM) among adult sickle cell disease (SCD) patients attending a tertiary institution's sickle cell clinic. The cross-sectional survey of 227 patients revealed that a significant majority (91.6%) used CAM in the last six months to manage pain, with prayer being the most common method. The study found that females and individuals with higher education levels were more likely to use CAM. While pharmacologic medications remain a primary component of pain management, an increasing number of patients are turning to CAM for pain relief. The research highlights the need for further investigation into the benefits and accessibility of CAM therapies for adult SCD patients. Desklib provides access to this and other solved assignments to aid students in their studies.
PRIMARY CARE & HEALTH SERVICES SECTION
Original Research Article
Pain Control in Sickle Cell Disease
Patients: Use of Complementary and
Alternative Medicine
Wendy E. Thompson, DrPH, MSW,* and Ike Eriator,
MD, MPH†
*School of Social Work, Andrews University, Berrien
Springs, Michigan;
†School of Medicine, University of Mississippi,
Jackson, Mississippi, USA
Reprint requests to: Wendy E. Thompson, DrPH,
MSW, School of Social Work, Andrews University,
Berrien Springs, MI 49103, USA. Tel: 601-594-0058;
Fax: 269-471-3686; E-mail: thompsow@andrews.edu.
Disclosure: None of the authors has any conflict of
interest or anything to disclose.
Abstract
Objective. To examine the factors associated with
the use of complementary and alternative medicine
(CAM) as reported by patients attending an adult
sickle cell clinic at a tertiary institution.
Design. Cross-sectional survey.
Setting. This study was conducted in a university
tertiary care adult sickle cell clinic.
Subjects. Adult sickle cell patients.
Method. Following Institutional Review Board
approval, a questionnaire was administered to
patients in a sickle cell clinic to examine their use of
CAM for managing pain at home and while admitted
to the hospital.
Results. Of the 227 respondents who completed the
questionnaire, 92% experienced pain lasting from 6
months to more than 2 years. Two hundred and eight
(91.6%) indicated that they have used CAM within
the last 6 months to control pain. The frequency
of CAMs use was higher among females, singles,
those with more education, and higher household
income.
Conclusions. This study shows that a substantial
majority of sickle cell patients live with pain on a
regular basis and that there is substantial CAM use
in the adult Sickle cell disease population. Being
female and having a high school or higher education
were significantly correlated with the use of CAM in
sickle cell patients. A variety of CAM therapies are
used, with the most common being prayer.
Key Words. Complementary Alternative Methods;
Sickle Cell Disease; Coping with Pain; Chronic Pain
Introduction
Sickle cell disease (SCD)remains a significantpublic
health problem in the United States [1]. It is estimated that
approximately 2 million Americans are genetic carriers of
the sickle celltrait [2], and 100,000 people are estimated
to be living with a history of SCD in the United States [3].
The incidence ofSCD is particularly high among African
Americans [4]. Despite the availability of tests to screen for
compatibility ofgenotype [1,5]and programs to increase
individuals’awareness ofthe disease [6],the prevalence
rate ofSCD has continued to rise in the past decade in
some parts of the United States [7]. The prevalence of this
disease is greaterthan that of any other condition
detected by newborn blood screening [2]. Research has
indicated that SCD is linked with severalacute pulmonary
complications including asthma,thromboembolism,and
acute chestsyndrome [8,9].Otherhealth complications
thatoccur as a resultof the disease include blindness,
skin ulcers,gallstones,priapism,bacterialsepticemia,
splenic sequestration, stroke, and chronic organ damage
[10–13]. These complications can be life-threatening and
can affect the whole body [6].
One of the hallmarks of this disease is intermittent, unpre-
dictable pain episodes ofvarying intensities [14].Pain in
SCD presents distinctive challenges for patients, families,
and health-care professionals [15–17].It is the most fre-
quent problem experienced by people with SCD and has
profound effects upon comfortand function in work,
school,play,and socialrelationships [18].A review by
Ballas, Gupta and Graves (2012) examined the frequency
of painfulepisodes experienced by sickle cellpatients and
found that acute painfulepisodes were the most common
bs_bs_banner
Pain Medicine 2014; 15: 241–246
Wiley Periodicals, Inc.
241
Downloaded from https://academic.oup.com/painmedicine/article-abstract/15/2/241/1824660 by guest on 01 March 2019
Original Research Article
Pain Control in Sickle Cell Disease
Patients: Use of Complementary and
Alternative Medicine
Wendy E. Thompson, DrPH, MSW,* and Ike Eriator,
MD, MPH†
*School of Social Work, Andrews University, Berrien
Springs, Michigan;
†School of Medicine, University of Mississippi,
Jackson, Mississippi, USA
Reprint requests to: Wendy E. Thompson, DrPH,
MSW, School of Social Work, Andrews University,
Berrien Springs, MI 49103, USA. Tel: 601-594-0058;
Fax: 269-471-3686; E-mail: thompsow@andrews.edu.
Disclosure: None of the authors has any conflict of
interest or anything to disclose.
Abstract
Objective. To examine the factors associated with
the use of complementary and alternative medicine
(CAM) as reported by patients attending an adult
sickle cell clinic at a tertiary institution.
Design. Cross-sectional survey.
Setting. This study was conducted in a university
tertiary care adult sickle cell clinic.
Subjects. Adult sickle cell patients.
Method. Following Institutional Review Board
approval, a questionnaire was administered to
patients in a sickle cell clinic to examine their use of
CAM for managing pain at home and while admitted
to the hospital.
Results. Of the 227 respondents who completed the
questionnaire, 92% experienced pain lasting from 6
months to more than 2 years. Two hundred and eight
(91.6%) indicated that they have used CAM within
the last 6 months to control pain. The frequency
of CAMs use was higher among females, singles,
those with more education, and higher household
income.
Conclusions. This study shows that a substantial
majority of sickle cell patients live with pain on a
regular basis and that there is substantial CAM use
in the adult Sickle cell disease population. Being
female and having a high school or higher education
were significantly correlated with the use of CAM in
sickle cell patients. A variety of CAM therapies are
used, with the most common being prayer.
Key Words. Complementary Alternative Methods;
Sickle Cell Disease; Coping with Pain; Chronic Pain
Introduction
Sickle cell disease (SCD)remains a significantpublic
health problem in the United States [1]. It is estimated that
approximately 2 million Americans are genetic carriers of
the sickle celltrait [2], and 100,000 people are estimated
to be living with a history of SCD in the United States [3].
The incidence ofSCD is particularly high among African
Americans [4]. Despite the availability of tests to screen for
compatibility ofgenotype [1,5]and programs to increase
individuals’awareness ofthe disease [6],the prevalence
rate ofSCD has continued to rise in the past decade in
some parts of the United States [7]. The prevalence of this
disease is greaterthan that of any other condition
detected by newborn blood screening [2]. Research has
indicated that SCD is linked with severalacute pulmonary
complications including asthma,thromboembolism,and
acute chestsyndrome [8,9].Otherhealth complications
thatoccur as a resultof the disease include blindness,
skin ulcers,gallstones,priapism,bacterialsepticemia,
splenic sequestration, stroke, and chronic organ damage
[10–13]. These complications can be life-threatening and
can affect the whole body [6].
One of the hallmarks of this disease is intermittent, unpre-
dictable pain episodes ofvarying intensities [14].Pain in
SCD presents distinctive challenges for patients, families,
and health-care professionals [15–17].It is the most fre-
quent problem experienced by people with SCD and has
profound effects upon comfortand function in work,
school,play,and socialrelationships [18].A review by
Ballas, Gupta and Graves (2012) examined the frequency
of painfulepisodes experienced by sickle cellpatients and
found that acute painfulepisodes were the most common
bs_bs_banner
Pain Medicine 2014; 15: 241–246
Wiley Periodicals, Inc.
241
Downloaded from https://academic.oup.com/painmedicine/article-abstract/15/2/241/1824660 by guest on 01 March 2019
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
cause ofhospitalizations.The study also indicated that
50% of hospitaladmissions foracute painfulepisodes
were readmissions within 1 month afterdischarge.This
was associated with pain, suffering, fear, anxiety, depres-
sion, the utilization of relatively high doses of opioids, and
alienationfrom the realitiesof daily living [19]. The
researchers suggested that improvement was needed in
the managementof pain during hospitalization and at
home afterdischarge.Brousseau et al.(2010),using a
retrospective cohort, examined 21,112 sickle cell-related
emergency room treatmentor in-patienthospitalization.
They noted a mean of 2.59 (95% confidence interval[CI])
encounter per patient per year. Utilization was highest for
those in the age group 18–30 years and those with public
insurance.The 30-day rehospitalization rate was 33.4%,
with those in the 18–30-year age group averaging 41.1%
[20]. Pharmacologic medications are a significant compo-
nent ofacute and chronic pain management in the adult
sickle cellpatient.However,recently,more and more
patients have been turning to complementary and alter-
native medicines (CAM)to help manage their painfulepi-
sodes [21–23].
CAM, defined as a group ofdiverse medicaland health
care systems, practices, and products that are not pres-
ently considered part ofconventionalmedicine, is on the
rise universally [24].For the purpose ofthis research,
prayer was defined using the National Center for
Complementary and Alternative Medicine’s definition as
“an active processof appealing to a higherspiritual
power, especially for health reasons: it includes individual
or group prayer on behalfof oneselfor others.” Spiritual
healing is the healing that is transmitted by the spirit, soul
of divine force. Acupuncture is a technique in which prac-
titionersstimulate specific pointson the body—most
often by inserting thin needles through the skin. Massage
therapyincludesmany differenttechniquesin which
practitioners manually manipulate the softtissues ofthe
body.Most meditation techniques involve ways in which
a person learns to focus attention.Relaxation tech-
niques, such as breathing exercises, guided imagery, and
progressive muscle relaxation,are designed to produce
the body’s naturalrelaxation response.
SCD patients seeking to use CAM face a numberof
challenges such as lack of access to these methods and
lack of third party or insurance to cover them as they utilize
CAM [25,26].Sibinga et al.(2006)examined pediatric
patients with SCD and use ofcomplementary and alter-
native therapies and showed that the use ofCAM thera-
pies was common among children with SCD.Prayer,
relaxation techniques, and spiritualhealing were the most
commonly reported CAM therapies [27]. However, there is
a scarcity ofresearch studies on CAM use among adult
sickle cellpatients and the factors thatare associated
its use.
The purpose of our study is to examine the factors asso-
ciated with the use of CAM as reported by patients attend-
ing an adult sickle cellclinic at a tertiary institution in the
United States.
Methods
This is a cross-sectionalstudy carried out using a survey
administered during the months of July through Septem-
ber 2010 at an adultsickle cellclinic.The researcher
invited alladults who were obtaining pain management
treatment for SCD at the clinic (in that 3-month period) to
voluntarily complete a three-page written questionnaire
about CAM use and its benefits. The study protocolwas
approved by InstitutionalReview Boards at Jackson
State University and the University ofMedicalCenter,
Jackson, Mississippi.Written,informed consentforms
were obtained from allparticipants.
Subjects
There were 450 sickle cellpatient registered in the clinic.
The study sample consisted ofa total of 227 patients
invited to participate in the study. Selection criteria for this
study included participants who had been diagnosed with
SCD, were African American, were between ages 18 and
65 years, and had been experiencing pain within the last 6
months.All of the invited patients agreed to participate,
and completed the questionnaire while in the waiting
room. Not allparticipants answered allof the questions.
Survey
Participants completed a three-page survey while they
were waiting to be seen by the hematologist.The ques-
tionnairewas tested for reliability.Cronbach’salpha
coefficientwas greaterthan .80.The questionnaire was
pilot-tested with individuals of similar demographic back-
ground to the study population and was revised based on
theircomments.It was assessed forcontentvalidity by
experts in the field.The survey was written atan eight-
grade reading level and took approximately20–25
minutes to complete. Respondents were informed that the
principalinvestigator and a nurse were available onsite if
they needed assistance with completing the question-
naire. The completed questionnaires were handed back to
the principalinvestigator.The questionnaire consisted of
nine structured items. Participants were asked about their
pain experienced within the past 6 months (when treated
at home and when treated in the hospital),the types of
CAM used and the benefits, and about their demographic
characteristics. There was also a set ofyes–no items on
the types of CAM used and its effectiveness in controlling
painfulepisodes in the last 6 months. A totalof 15 com-
monly used CAMs were provided on the list. A copy of the
questionnaire is attached (Appendix S1).
Data Analysis
The data were analyzed using StatisticalPackage for
SocialSciences version 19.0 [28].Descriptive statistics
was used to determine the frequency ofCAM use. The
influence ofvariousfactors, such as gender,marital
status, age, education, household annualincome, type of
medicalinsurance, and type of SCD, on the use of CAM
were analyzed with binary logistic regression. Results are
242
Thompson and Eriator
Downloaded from https://academic.oup.com/painmedicine/article-abstract/15/2/241/1824660 by guest on 01 March 2019
50% of hospitaladmissions foracute painfulepisodes
were readmissions within 1 month afterdischarge.This
was associated with pain, suffering, fear, anxiety, depres-
sion, the utilization of relatively high doses of opioids, and
alienationfrom the realitiesof daily living [19]. The
researchers suggested that improvement was needed in
the managementof pain during hospitalization and at
home afterdischarge.Brousseau et al.(2010),using a
retrospective cohort, examined 21,112 sickle cell-related
emergency room treatmentor in-patienthospitalization.
They noted a mean of 2.59 (95% confidence interval[CI])
encounter per patient per year. Utilization was highest for
those in the age group 18–30 years and those with public
insurance.The 30-day rehospitalization rate was 33.4%,
with those in the 18–30-year age group averaging 41.1%
[20]. Pharmacologic medications are a significant compo-
nent ofacute and chronic pain management in the adult
sickle cellpatient.However,recently,more and more
patients have been turning to complementary and alter-
native medicines (CAM)to help manage their painfulepi-
sodes [21–23].
CAM, defined as a group ofdiverse medicaland health
care systems, practices, and products that are not pres-
ently considered part ofconventionalmedicine, is on the
rise universally [24].For the purpose ofthis research,
prayer was defined using the National Center for
Complementary and Alternative Medicine’s definition as
“an active processof appealing to a higherspiritual
power, especially for health reasons: it includes individual
or group prayer on behalfof oneselfor others.” Spiritual
healing is the healing that is transmitted by the spirit, soul
of divine force. Acupuncture is a technique in which prac-
titionersstimulate specific pointson the body—most
often by inserting thin needles through the skin. Massage
therapyincludesmany differenttechniquesin which
practitioners manually manipulate the softtissues ofthe
body.Most meditation techniques involve ways in which
a person learns to focus attention.Relaxation tech-
niques, such as breathing exercises, guided imagery, and
progressive muscle relaxation,are designed to produce
the body’s naturalrelaxation response.
SCD patients seeking to use CAM face a numberof
challenges such as lack of access to these methods and
lack of third party or insurance to cover them as they utilize
CAM [25,26].Sibinga et al.(2006)examined pediatric
patients with SCD and use ofcomplementary and alter-
native therapies and showed that the use ofCAM thera-
pies was common among children with SCD.Prayer,
relaxation techniques, and spiritualhealing were the most
commonly reported CAM therapies [27]. However, there is
a scarcity ofresearch studies on CAM use among adult
sickle cellpatients and the factors thatare associated
its use.
The purpose of our study is to examine the factors asso-
ciated with the use of CAM as reported by patients attend-
ing an adult sickle cellclinic at a tertiary institution in the
United States.
Methods
This is a cross-sectionalstudy carried out using a survey
administered during the months of July through Septem-
ber 2010 at an adultsickle cellclinic.The researcher
invited alladults who were obtaining pain management
treatment for SCD at the clinic (in that 3-month period) to
voluntarily complete a three-page written questionnaire
about CAM use and its benefits. The study protocolwas
approved by InstitutionalReview Boards at Jackson
State University and the University ofMedicalCenter,
Jackson, Mississippi.Written,informed consentforms
were obtained from allparticipants.
Subjects
There were 450 sickle cellpatient registered in the clinic.
The study sample consisted ofa total of 227 patients
invited to participate in the study. Selection criteria for this
study included participants who had been diagnosed with
SCD, were African American, were between ages 18 and
65 years, and had been experiencing pain within the last 6
months.All of the invited patients agreed to participate,
and completed the questionnaire while in the waiting
room. Not allparticipants answered allof the questions.
Survey
Participants completed a three-page survey while they
were waiting to be seen by the hematologist.The ques-
tionnairewas tested for reliability.Cronbach’salpha
coefficientwas greaterthan .80.The questionnaire was
pilot-tested with individuals of similar demographic back-
ground to the study population and was revised based on
theircomments.It was assessed forcontentvalidity by
experts in the field.The survey was written atan eight-
grade reading level and took approximately20–25
minutes to complete. Respondents were informed that the
principalinvestigator and a nurse were available onsite if
they needed assistance with completing the question-
naire. The completed questionnaires were handed back to
the principalinvestigator.The questionnaire consisted of
nine structured items. Participants were asked about their
pain experienced within the past 6 months (when treated
at home and when treated in the hospital),the types of
CAM used and the benefits, and about their demographic
characteristics. There was also a set ofyes–no items on
the types of CAM used and its effectiveness in controlling
painfulepisodes in the last 6 months. A totalof 15 com-
monly used CAMs were provided on the list. A copy of the
questionnaire is attached (Appendix S1).
Data Analysis
The data were analyzed using StatisticalPackage for
SocialSciences version 19.0 [28].Descriptive statistics
was used to determine the frequency ofCAM use. The
influence ofvariousfactors, such as gender,marital
status, age, education, household annualincome, type of
medicalinsurance, and type of SCD, on the use of CAM
were analyzed with binary logistic regression. Results are
242
Thompson and Eriator
Downloaded from https://academic.oup.com/painmedicine/article-abstract/15/2/241/1824660 by guest on 01 March 2019
presented as percentagesand odds ratios (ORs)
with 95% CI interval.A P value of <0.05 was consid-
ered significant.
Results
Two hundred and twenty-seven participants completed
the questionnaire. Ninety-six (42.3%)were male and 131
(57.7%)were female.The mean age ofthe participants
was 32 years (ranged 18–65). About 32% were between
the ages of 18 and 24, and 56% were older than 24 years.
One hundred and eighty-three (80.6%)identified them-
selves as single. The majority (68.3%)of the participants
had more than a high schoolor generaleducationaldevel-
opment (GED) diploma. The majority (62%) of the respon-
dents had an annualhousehold income ofless than
$15,000, and the majority (64%)of the respondents was
covered by Medicaid as the primary insurance. More than
half of the respondents had Hemoglobin SS.
Duration and Number of PainfulEpisodes Experienced
Ninety-two percentof patients experienced pain lasting
greater than 6 months. The median duration of pain was
25 or more months reported by 136 (65.1%). Pain medi-
cations were taken on a daily basis during the past6
months by 90% ofthe respondents to controlpain. Pain
was more likely to be treated at home than in the hospital.
For pain treated at home, 39.6% indicated that they had
experienced between 1 and 5 painfulepisodes within the
past 6 months (Table 1).When they were treated in the
hospital, 49.1% of the respondents experienced between
1 and 5 painfulepisodes.
When asked to rank the level of pain they felt when treated
at home, 24.2% said that they had experienced mild pain,
42.2% experienced moderate pain,and 34% indicated
that they experienced severe pain.About 11% of the
respondents said thatthey experienced mild pain when
treated in the hospital, 16% experienced moderate pain,
with a larger proportion (73.0%) experiencing severe pain
when treated in the hospital. Severe pain was more likely
to be associated with hospitalization (73%) compared with
33.6% who reported thatthey experienced severe pain
when treated athome.Mild and moderate pains were
more likely to be treated at home (Table 2).
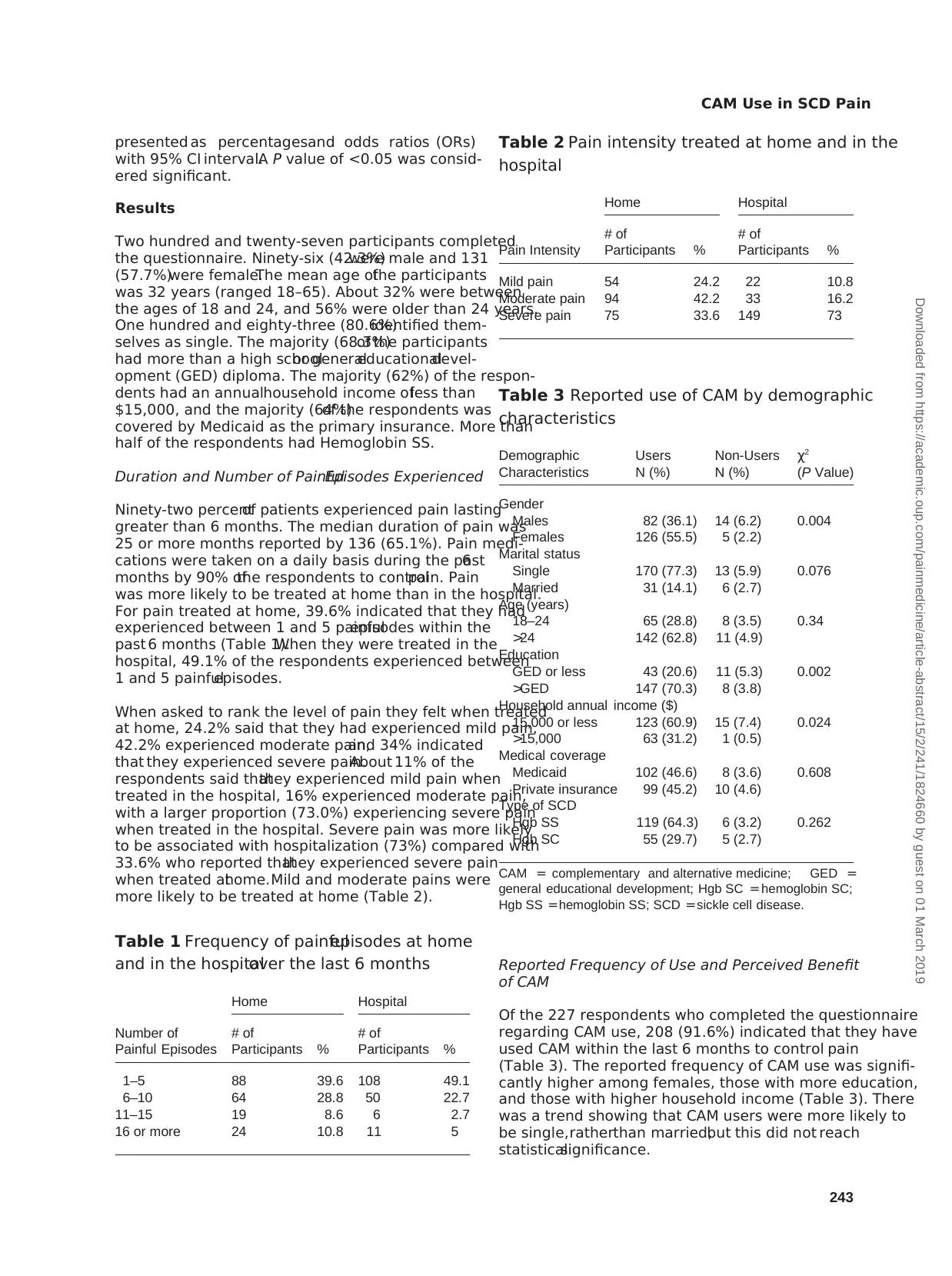
Reported Frequency of Use and Perceived Benefit
of CAM
Of the 227 respondents who completed the questionnaire
regarding CAM use, 208 (91.6%) indicated that they have
used CAM within the last 6 months to control pain
(Table 3). The reported frequency of CAM use was signifi-
cantly higher among females, those with more education,
and those with higher household income (Table 3). There
was a trend showing that CAM users were more likely to
be single,ratherthan married,but this did not reach
statisticalsignificance.
Table 3 Reported use of CAM by demographic
characteristics
Demographic
Characteristics
Users Non-Users χ2
N (%) N (%) (P Value)
Gender
Males 82 (36.1) 14 (6.2) 0.004
Females 126 (55.5) 5 (2.2)
Marital status
Single 170 (77.3) 13 (5.9) 0.076
Married 31 (14.1) 6 (2.7)
Age (years)
18–24 65 (28.8) 8 (3.5) 0.34
>24 142 (62.8) 11 (4.9)
Education
GED or less 43 (20.6) 11 (5.3) 0.002
>GED 147 (70.3) 8 (3.8)
Household annual income ($)
15,000 or less 123 (60.9) 15 (7.4) 0.024
>15,000 63 (31.2) 1 (0.5)
Medical coverage
Medicaid 102 (46.6) 8 (3.6) 0.608
Private insurance 99 (45.2) 10 (4.6)
Type of SCD
Hgb SS 119 (64.3) 6 (3.2) 0.262
Hgb SC 55 (29.7) 5 (2.7)
CAM = complementary and alternative medicine; GED =
general educational development; Hgb SC = hemoglobin SC;
Hgb SS =hemoglobin SS; SCD =sickle cell disease.
Table 1 Frequency of painfulepisodes at home
and in the hospitalover the last 6 months
Number of
Painful Episodes
Home Hospital
# of
Participants %
# of
Participants %
1–5 88 39.6 108 49.1
6–10 64 28.8 50 22.7
11–15 19 8.6 6 2.7
16 or more 24 10.8 11 5
Table 2 Pain intensity treated at home and in the
hospital
Pain Intensity
Home Hospital
# of
Participants %
# of
Participants %
Mild pain 54 24.2 22 10.8
Moderate pain 94 42.2 33 16.2
Severe pain 75 33.6 149 73
243
CAM Use in SCD Pain
Downloaded from https://academic.oup.com/painmedicine/article-abstract/15/2/241/1824660 by guest on 01 March 2019
with 95% CI interval.A P value of <0.05 was consid-
ered significant.
Results
Two hundred and twenty-seven participants completed
the questionnaire. Ninety-six (42.3%)were male and 131
(57.7%)were female.The mean age ofthe participants
was 32 years (ranged 18–65). About 32% were between
the ages of 18 and 24, and 56% were older than 24 years.
One hundred and eighty-three (80.6%)identified them-
selves as single. The majority (68.3%)of the participants
had more than a high schoolor generaleducationaldevel-
opment (GED) diploma. The majority (62%) of the respon-
dents had an annualhousehold income ofless than
$15,000, and the majority (64%)of the respondents was
covered by Medicaid as the primary insurance. More than
half of the respondents had Hemoglobin SS.
Duration and Number of PainfulEpisodes Experienced
Ninety-two percentof patients experienced pain lasting
greater than 6 months. The median duration of pain was
25 or more months reported by 136 (65.1%). Pain medi-
cations were taken on a daily basis during the past6
months by 90% ofthe respondents to controlpain. Pain
was more likely to be treated at home than in the hospital.
For pain treated at home, 39.6% indicated that they had
experienced between 1 and 5 painfulepisodes within the
past 6 months (Table 1).When they were treated in the
hospital, 49.1% of the respondents experienced between
1 and 5 painfulepisodes.
When asked to rank the level of pain they felt when treated
at home, 24.2% said that they had experienced mild pain,
42.2% experienced moderate pain,and 34% indicated
that they experienced severe pain.About 11% of the
respondents said thatthey experienced mild pain when
treated in the hospital, 16% experienced moderate pain,
with a larger proportion (73.0%) experiencing severe pain
when treated in the hospital. Severe pain was more likely
to be associated with hospitalization (73%) compared with
33.6% who reported thatthey experienced severe pain
when treated athome.Mild and moderate pains were
more likely to be treated at home (Table 2).
Reported Frequency of Use and Perceived Benefit
of CAM
Of the 227 respondents who completed the questionnaire
regarding CAM use, 208 (91.6%) indicated that they have
used CAM within the last 6 months to control pain
(Table 3). The reported frequency of CAM use was signifi-
cantly higher among females, those with more education,
and those with higher household income (Table 3). There
was a trend showing that CAM users were more likely to
be single,ratherthan married,but this did not reach
statisticalsignificance.
Table 3 Reported use of CAM by demographic
characteristics
Demographic
Characteristics
Users Non-Users χ2
N (%) N (%) (P Value)
Gender
Males 82 (36.1) 14 (6.2) 0.004
Females 126 (55.5) 5 (2.2)
Marital status
Single 170 (77.3) 13 (5.9) 0.076
Married 31 (14.1) 6 (2.7)
Age (years)
18–24 65 (28.8) 8 (3.5) 0.34
>24 142 (62.8) 11 (4.9)
Education
GED or less 43 (20.6) 11 (5.3) 0.002
>GED 147 (70.3) 8 (3.8)
Household annual income ($)
15,000 or less 123 (60.9) 15 (7.4) 0.024
>15,000 63 (31.2) 1 (0.5)
Medical coverage
Medicaid 102 (46.6) 8 (3.6) 0.608
Private insurance 99 (45.2) 10 (4.6)
Type of SCD
Hgb SS 119 (64.3) 6 (3.2) 0.262
Hgb SC 55 (29.7) 5 (2.7)
CAM = complementary and alternative medicine; GED =
general educational development; Hgb SC = hemoglobin SC;
Hgb SS =hemoglobin SS; SCD =sickle cell disease.
Table 1 Frequency of painfulepisodes at home
and in the hospitalover the last 6 months
Number of
Painful Episodes
Home Hospital
# of
Participants %
# of
Participants %
1–5 88 39.6 108 49.1
6–10 64 28.8 50 22.7
11–15 19 8.6 6 2.7
16 or more 24 10.8 11 5
Table 2 Pain intensity treated at home and in the
hospital
Pain Intensity
Home Hospital
# of
Participants %
# of
Participants %
Mild pain 54 24.2 22 10.8
Moderate pain 94 42.2 33 16.2
Severe pain 75 33.6 149 73
243
CAM Use in SCD Pain
Downloaded from https://academic.oup.com/painmedicine/article-abstract/15/2/241/1824660 by guest on 01 March 2019
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
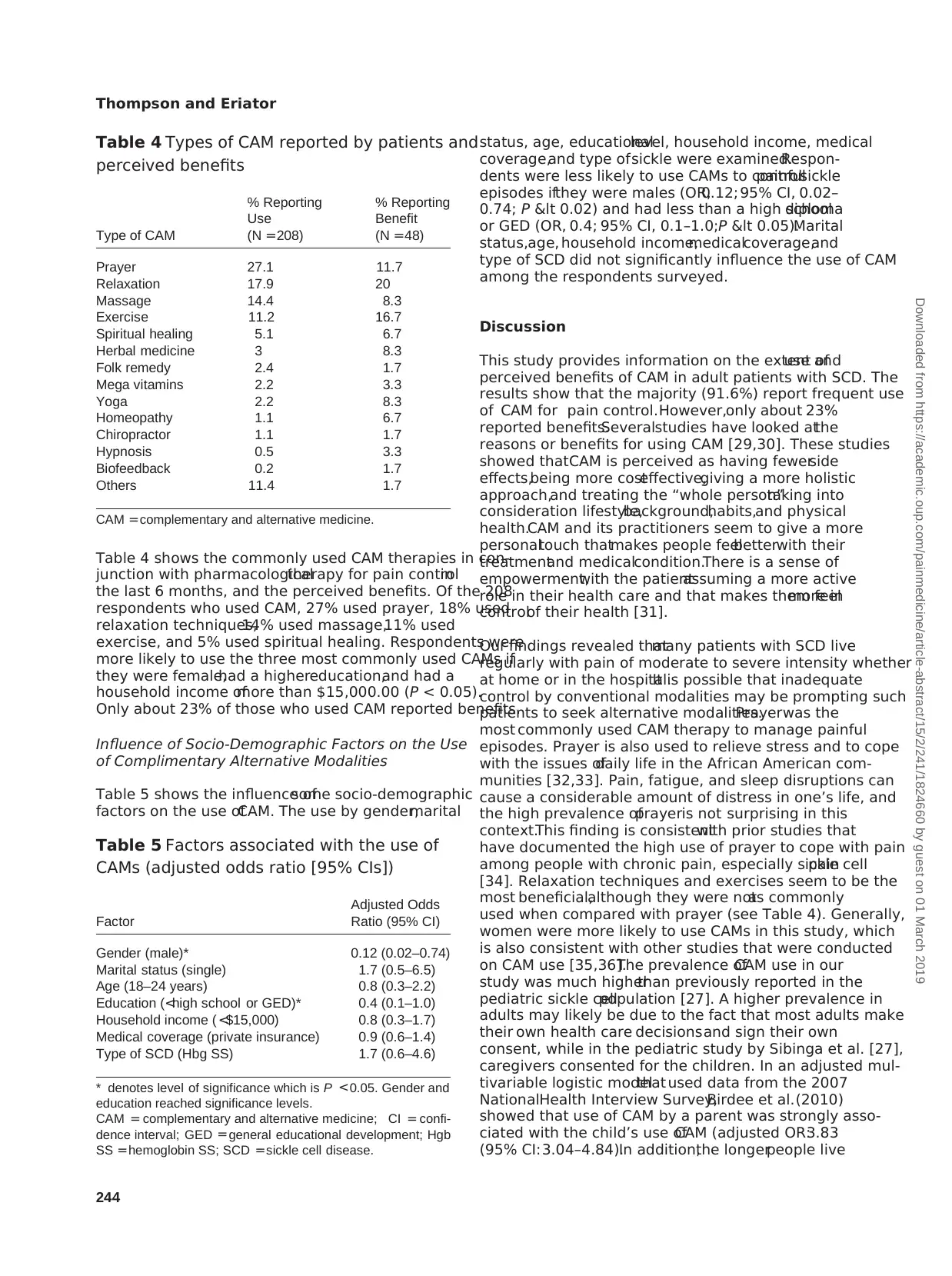
Table 4 shows the commonly used CAM therapies in con-
junction with pharmacologicaltherapy for pain controlin
the last 6 months, and the perceived benefits. Of the 208
respondents who used CAM, 27% used prayer, 18% used
relaxation techniques,14% used massage,11% used
exercise, and 5% used spiritual healing. Respondents were
more likely to use the three most commonly used CAMs if
they were female,had a highereducation,and had a
household income ofmore than $15,000.00 (P < 0.05).
Only about 23% of those who used CAM reported benefits.
Influence of Socio-Demographic Factors on the Use
of Complimentary Alternative Modalities
Table 5 shows the influence ofsome socio-demographic
factors on the use ofCAM. The use by gender,marital
status, age, educationallevel, household income, medical
coverage,and type ofsickle were examined.Respon-
dents were less likely to use CAMs to controlpainfulsickle
episodes ifthey were males (OR,0.12; 95% CI, 0.02–
0.74; P < 0.02) and had less than a high schooldiploma
or GED (OR, 0.4; 95% CI, 0.1–1.0;P < 0.05).Marital
status,age, household income,medicalcoverage,and
type of SCD did not significantly influence the use of CAM
among the respondents surveyed.
Discussion
This study provides information on the extent ofuse and
perceived benefits of CAM in adult patients with SCD. The
results show that the majority (91.6%) report frequent use
of CAM for pain control.However,only about 23%
reported benefits.Severalstudies have looked atthe
reasons or benefits for using CAM [29,30]. These studies
showed thatCAM is perceived as having fewerside
effects,being more costeffective,giving a more holistic
approach,and treating the “whole person”taking into
consideration lifestyle,background,habits,and physical
health.CAM and its practitioners seem to give a more
personaltouch thatmakes people feelbetterwith their
treatmentand medicalcondition.There is a sense of
empowerment,with the patientassuming a more active
role in their health care and that makes them feelmore in
controlof their health [31].
Our findings revealed thatmany patients with SCD live
regularly with pain of moderate to severe intensity whether
at home or in the hospital.It is possible that inadequate
control by conventional modalities may be prompting such
patients to seek alternative modalities.Prayerwas the
most commonly used CAM therapy to manage painful
episodes. Prayer is also used to relieve stress and to cope
with the issues ofdaily life in the African American com-
munities [32,33]. Pain, fatigue, and sleep disruptions can
cause a considerable amount of distress in one’s life, and
the high prevalence ofprayeris not surprising in this
context.This finding is consistentwith prior studies that
have documented the high use of prayer to cope with pain
among people with chronic pain, especially sickle cellpain
[34]. Relaxation techniques and exercises seem to be the
most beneficial,although they were notas commonly
used when compared with prayer (see Table 4). Generally,
women were more likely to use CAMs in this study, which
is also consistent with other studies that were conducted
on CAM use [35,36].The prevalence ofCAM use in our
study was much higherthan previously reported in the
pediatric sickle cellpopulation [27]. A higher prevalence in
adults may likely be due to the fact that most adults make
their own health care decisionsand sign their own
consent, while in the pediatric study by Sibinga et al. [27],
caregivers consented for the children. In an adjusted mul-
tivariable logistic modelthat used data from the 2007
NationalHealth Interview Survey,Birdee et al.(2010)
showed that use of CAM by a parent was strongly asso-
ciated with the child’s use ofCAM (adjusted OR:3.83
(95% CI:3.04–4.84).In addition,the longerpeople live
Table 4 Types of CAM reported by patients and
perceived benefits
Type of CAM
% Reporting
Use
% Reporting
Benefit
(N =208) (N =48)
Prayer 27.1 11.7
Relaxation 17.9 20
Massage 14.4 8.3
Exercise 11.2 16.7
Spiritual healing 5.1 6.7
Herbal medicine 3 8.3
Folk remedy 2.4 1.7
Mega vitamins 2.2 3.3
Yoga 2.2 8.3
Homeopathy 1.1 6.7
Chiropractor 1.1 1.7
Hypnosis 0.5 3.3
Biofeedback 0.2 1.7
Others 11.4 1.7
CAM =complementary and alternative medicine.
Table 5 Factors associated with the use of
CAMs (adjusted odds ratio [95% CIs])
Factor
Adjusted Odds
Ratio (95% CI)
Gender (male)* 0.12 (0.02–0.74)
Marital status (single) 1.7 (0.5–6.5)
Age (18–24 years) 0.8 (0.3–2.2)
Education (<high school or GED)* 0.4 (0.1–1.0)
Household income ( <$15,000) 0.8 (0.3–1.7)
Medical coverage (private insurance) 0.9 (0.6–1.4)
Type of SCD (Hbg SS) 1.7 (0.6–4.6)
* denotes level of significance which is P <0.05. Gender and
education reached significance levels.
CAM = complementary and alternative medicine; CI = confi-
dence interval; GED =general educational development; Hgb
SS =hemoglobin SS; SCD =sickle cell disease.
244
Thompson and Eriator
Downloaded from https://academic.oup.com/painmedicine/article-abstract/15/2/241/1824660 by guest on 01 March 2019
junction with pharmacologicaltherapy for pain controlin
the last 6 months, and the perceived benefits. Of the 208
respondents who used CAM, 27% used prayer, 18% used
relaxation techniques,14% used massage,11% used
exercise, and 5% used spiritual healing. Respondents were
more likely to use the three most commonly used CAMs if
they were female,had a highereducation,and had a
household income ofmore than $15,000.00 (P < 0.05).
Only about 23% of those who used CAM reported benefits.
Influence of Socio-Demographic Factors on the Use
of Complimentary Alternative Modalities
Table 5 shows the influence ofsome socio-demographic
factors on the use ofCAM. The use by gender,marital
status, age, educationallevel, household income, medical
coverage,and type ofsickle were examined.Respon-
dents were less likely to use CAMs to controlpainfulsickle
episodes ifthey were males (OR,0.12; 95% CI, 0.02–
0.74; P < 0.02) and had less than a high schooldiploma
or GED (OR, 0.4; 95% CI, 0.1–1.0;P < 0.05).Marital
status,age, household income,medicalcoverage,and
type of SCD did not significantly influence the use of CAM
among the respondents surveyed.
Discussion
This study provides information on the extent ofuse and
perceived benefits of CAM in adult patients with SCD. The
results show that the majority (91.6%) report frequent use
of CAM for pain control.However,only about 23%
reported benefits.Severalstudies have looked atthe
reasons or benefits for using CAM [29,30]. These studies
showed thatCAM is perceived as having fewerside
effects,being more costeffective,giving a more holistic
approach,and treating the “whole person”taking into
consideration lifestyle,background,habits,and physical
health.CAM and its practitioners seem to give a more
personaltouch thatmakes people feelbetterwith their
treatmentand medicalcondition.There is a sense of
empowerment,with the patientassuming a more active
role in their health care and that makes them feelmore in
controlof their health [31].
Our findings revealed thatmany patients with SCD live
regularly with pain of moderate to severe intensity whether
at home or in the hospital.It is possible that inadequate
control by conventional modalities may be prompting such
patients to seek alternative modalities.Prayerwas the
most commonly used CAM therapy to manage painful
episodes. Prayer is also used to relieve stress and to cope
with the issues ofdaily life in the African American com-
munities [32,33]. Pain, fatigue, and sleep disruptions can
cause a considerable amount of distress in one’s life, and
the high prevalence ofprayeris not surprising in this
context.This finding is consistentwith prior studies that
have documented the high use of prayer to cope with pain
among people with chronic pain, especially sickle cellpain
[34]. Relaxation techniques and exercises seem to be the
most beneficial,although they were notas commonly
used when compared with prayer (see Table 4). Generally,
women were more likely to use CAMs in this study, which
is also consistent with other studies that were conducted
on CAM use [35,36].The prevalence ofCAM use in our
study was much higherthan previously reported in the
pediatric sickle cellpopulation [27]. A higher prevalence in
adults may likely be due to the fact that most adults make
their own health care decisionsand sign their own
consent, while in the pediatric study by Sibinga et al. [27],
caregivers consented for the children. In an adjusted mul-
tivariable logistic modelthat used data from the 2007
NationalHealth Interview Survey,Birdee et al.(2010)
showed that use of CAM by a parent was strongly asso-
ciated with the child’s use ofCAM (adjusted OR:3.83
(95% CI:3.04–4.84).In addition,the longerpeople live
Table 4 Types of CAM reported by patients and
perceived benefits
Type of CAM
% Reporting
Use
% Reporting
Benefit
(N =208) (N =48)
Prayer 27.1 11.7
Relaxation 17.9 20
Massage 14.4 8.3
Exercise 11.2 16.7
Spiritual healing 5.1 6.7
Herbal medicine 3 8.3
Folk remedy 2.4 1.7
Mega vitamins 2.2 3.3
Yoga 2.2 8.3
Homeopathy 1.1 6.7
Chiropractor 1.1 1.7
Hypnosis 0.5 3.3
Biofeedback 0.2 1.7
Others 11.4 1.7
CAM =complementary and alternative medicine.
Table 5 Factors associated with the use of
CAMs (adjusted odds ratio [95% CIs])
Factor
Adjusted Odds
Ratio (95% CI)
Gender (male)* 0.12 (0.02–0.74)
Marital status (single) 1.7 (0.5–6.5)
Age (18–24 years) 0.8 (0.3–2.2)
Education (<high school or GED)* 0.4 (0.1–1.0)
Household income ( <$15,000) 0.8 (0.3–1.7)
Medical coverage (private insurance) 0.9 (0.6–1.4)
Type of SCD (Hbg SS) 1.7 (0.6–4.6)
* denotes level of significance which is P <0.05. Gender and
education reached significance levels.
CAM = complementary and alternative medicine; CI = confi-
dence interval; GED =general educational development; Hgb
SS =hemoglobin SS; SCD =sickle cell disease.
244
Thompson and Eriator
Downloaded from https://academic.oup.com/painmedicine/article-abstract/15/2/241/1824660 by guest on 01 March 2019
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
with pain and distress,the more they are likely to seek
alternative approaches [37,38].
Those with higher household incomes were more likely to
use CAMs to controlsickle cellpain than those with a
lower income. This finding is consistent with other studies
on the use of CAM [31,37,38]. People ages 24 and above
were also more likely to report using CAM [39]. Our study
confirms that sickle cellpatients who were 24 years and
older were more likely to report using CAM to controlpain
when compared with those aged 18 to 24 years.
Generally,the respondents suggested some perceived
benefitsattributed to its use including improved life
control, fewer hospitalvisits, fewer schoolabsences, and
less disruption in household activities.
This study has a numberof limitations.The study,
although having alarge sample size, was a cross-
sectionalsurvey and did not examine how these patients
have come to use CAM nor if they willcontinue to do so
into the future. In addition, these were self-reported infor-
mation and may notbe an accurate portrayalof prac-
tice.The sample was obtained from a tertiary institution.
The patients who attend this tertiary care clinic may be
the mostcomplicated and have more pain complaints
when compared with othersickle cell patients in the
community.The findings may nottherefore be general-
izable to allsickle cellpatients in the community. In addi-
tion, this surveywas carried out during the summer
period, and may not be reflective of other seasons. Also,
it is importantto note thatCAM comprises those treat-
mentmodalities thatare not standard partof conven-
tional medicalcare, and as such, there is no strict
limitation ofwhatshould be included in this class.And
there are no strict definitions of allthe included treatment
modalitiesthat are commonlyused by practitioners,
researchers,or patients. Another limitationof our
study is that the population sampled waslimited to
African Americans.
Conclusion
This study shows thata substantialmajority ofadult
sickle cellpatients live with significantpain on a regular
basis and thatthere is significantusage ofCAM in this
population forpain control.A variety ofCAM modalities
are used, with the most common being prayer. However,
relaxation techniquesand exercisesseem to provide
more perceived benefits.This study points to the fact
that adultsickle cellpatients use CAM in conjunction
with standard medicaltherapy.It is more commonly
used by female patients,those with higherhousehold
income,and those with higher levelof education.There
is a great need for health care practitioners to be familiar
with these practices. Health-careproviders should
explore such use ofCAM by their patients—as they are
often used in conjunction with standard medicaltherapy.
Patients find some ofthese complementary and alter-
native modalitieseffective.These should be actively
encouraged and supported.
References
1 Sickle Cell Disease Association ofAmerica.2013.
Sickle celldisease is a GlobalPublic Health Issue.
Availableat: http://www.sicklecelldisease.org/index
.cfm?page=scd-global(accessed July 2013).
2 Hick JL, Nelson SC, Hick K, NwaneriMO. Emergency
managementof sickle cell disease complications:
review and practice guidelines. Minn Med 2006;89(2):
42–4, 47.
3 HassellKL. Population estimates of sickle celldisease
in the U.S. Am J Prev Med 2010;38:S512–21.
4 NationalHeartLung and Blood Institute.2009.Dis-
eases and conditions index: What is sickle cell anemia.
Available at: http://www.nhlbi.nih.gov/health/health
-topics/topics/sca/ (accessed July 2013).
5 NationalHuman Genome Research Institute.2012.
NationalInstitutes ofHealth.Is there a test for sickle
cell disease? Available at:https://www.genome.gov/
10001219 (accessed July 2013).
6 NationalHeartLung Blood Institute.2013.Diseases
and conditions index.Available at:http://www.nhlbi
.nih.gov/health/dci/Diseases/Sca/SCA_WhoIsAtRisk
.html(accessed June 2013).
7 Serjeant GR. One hundred years of sickle celldisease.
Br J Haematol2010;151(5):425–9.
8 Solovieff N, Hartley SW, Baldwin CT, et al. Ancestry of
African Americans with sickle celldisease. Blood Cells
Mol Dis 2011;47(1):41–5.
9 OgunlesiF, Koumbourlis AC.Sickle celldisease and
the lung: Many questions stillremain unanswered. Clin
Pulm Med 2011;18(3):119–28.
10 Miller ST. How I treat acute chest syndrome in children
with sickle celldisease.Blood 2011;117(20):5297–
305.
11 Sickle CellDisease Symptoms,Causes,Treatments.
WebMD – Better information. Better health. N.p., n.d.
Web. 2012. Available at: http://www.webmd.com/
pain-management/pain-management-sickle-cell
-disease (accessed February 2014).
12 Brandow AM, Liem RI. Sickle celldisease in the emer-
gency department:Atypicalcomplications and man-
agement. Clin Pediatr Emerg Med 2011;12(3):202–12.
13 Shilo NR,Lands LC. Asthma and chronic sickle cell
lung disease: A dynamic relationship. Paediatr Respir
Rev 2011;12(1):78–82.
14 Nagalla S, Ballas SK. Drugs for preventing red blood
cell dehydration in people with sickle celldisease.
Cochrane Database SystRev 2010;(1):CD003426,
245
CAM Use in SCD Pain
Downloaded from https://academic.oup.com/painmedicine/article-abstract/15/2/241/1824660 by guest on 01 March 2019
alternative approaches [37,38].
Those with higher household incomes were more likely to
use CAMs to controlsickle cellpain than those with a
lower income. This finding is consistent with other studies
on the use of CAM [31,37,38]. People ages 24 and above
were also more likely to report using CAM [39]. Our study
confirms that sickle cellpatients who were 24 years and
older were more likely to report using CAM to controlpain
when compared with those aged 18 to 24 years.
Generally,the respondents suggested some perceived
benefitsattributed to its use including improved life
control, fewer hospitalvisits, fewer schoolabsences, and
less disruption in household activities.
This study has a numberof limitations.The study,
although having alarge sample size, was a cross-
sectionalsurvey and did not examine how these patients
have come to use CAM nor if they willcontinue to do so
into the future. In addition, these were self-reported infor-
mation and may notbe an accurate portrayalof prac-
tice.The sample was obtained from a tertiary institution.
The patients who attend this tertiary care clinic may be
the mostcomplicated and have more pain complaints
when compared with othersickle cell patients in the
community.The findings may nottherefore be general-
izable to allsickle cellpatients in the community. In addi-
tion, this surveywas carried out during the summer
period, and may not be reflective of other seasons. Also,
it is importantto note thatCAM comprises those treat-
mentmodalities thatare not standard partof conven-
tional medicalcare, and as such, there is no strict
limitation ofwhatshould be included in this class.And
there are no strict definitions of allthe included treatment
modalitiesthat are commonlyused by practitioners,
researchers,or patients. Another limitationof our
study is that the population sampled waslimited to
African Americans.
Conclusion
This study shows thata substantialmajority ofadult
sickle cellpatients live with significantpain on a regular
basis and thatthere is significantusage ofCAM in this
population forpain control.A variety ofCAM modalities
are used, with the most common being prayer. However,
relaxation techniquesand exercisesseem to provide
more perceived benefits.This study points to the fact
that adultsickle cellpatients use CAM in conjunction
with standard medicaltherapy.It is more commonly
used by female patients,those with higherhousehold
income,and those with higher levelof education.There
is a great need for health care practitioners to be familiar
with these practices. Health-careproviders should
explore such use ofCAM by their patients—as they are
often used in conjunction with standard medicaltherapy.
Patients find some ofthese complementary and alter-
native modalitieseffective.These should be actively
encouraged and supported.
References
1 Sickle Cell Disease Association ofAmerica.2013.
Sickle celldisease is a GlobalPublic Health Issue.
Availableat: http://www.sicklecelldisease.org/index
.cfm?page=scd-global(accessed July 2013).
2 Hick JL, Nelson SC, Hick K, NwaneriMO. Emergency
managementof sickle cell disease complications:
review and practice guidelines. Minn Med 2006;89(2):
42–4, 47.
3 HassellKL. Population estimates of sickle celldisease
in the U.S. Am J Prev Med 2010;38:S512–21.
4 NationalHeartLung and Blood Institute.2009.Dis-
eases and conditions index: What is sickle cell anemia.
Available at: http://www.nhlbi.nih.gov/health/health
-topics/topics/sca/ (accessed July 2013).
5 NationalHuman Genome Research Institute.2012.
NationalInstitutes ofHealth.Is there a test for sickle
cell disease? Available at:https://www.genome.gov/
10001219 (accessed July 2013).
6 NationalHeartLung Blood Institute.2013.Diseases
and conditions index.Available at:http://www.nhlbi
.nih.gov/health/dci/Diseases/Sca/SCA_WhoIsAtRisk
.html(accessed June 2013).
7 Serjeant GR. One hundred years of sickle celldisease.
Br J Haematol2010;151(5):425–9.
8 Solovieff N, Hartley SW, Baldwin CT, et al. Ancestry of
African Americans with sickle celldisease. Blood Cells
Mol Dis 2011;47(1):41–5.
9 OgunlesiF, Koumbourlis AC.Sickle celldisease and
the lung: Many questions stillremain unanswered. Clin
Pulm Med 2011;18(3):119–28.
10 Miller ST. How I treat acute chest syndrome in children
with sickle celldisease.Blood 2011;117(20):5297–
305.
11 Sickle CellDisease Symptoms,Causes,Treatments.
WebMD – Better information. Better health. N.p., n.d.
Web. 2012. Available at: http://www.webmd.com/
pain-management/pain-management-sickle-cell
-disease (accessed February 2014).
12 Brandow AM, Liem RI. Sickle celldisease in the emer-
gency department:Atypicalcomplications and man-
agement. Clin Pediatr Emerg Med 2011;12(3):202–12.
13 Shilo NR,Lands LC. Asthma and chronic sickle cell
lung disease: A dynamic relationship. Paediatr Respir
Rev 2011;12(1):78–82.
14 Nagalla S, Ballas SK. Drugs for preventing red blood
cell dehydration in people with sickle celldisease.
Cochrane Database SystRev 2010;(1):CD003426,
245
CAM Use in SCD Pain
Downloaded from https://academic.oup.com/painmedicine/article-abstract/15/2/241/1824660 by guest on 01 March 2019
doi: 10.1002/14651858.CD003426.pub3.(accessed
July 30, 2013).
15 Anie KA. Psychologicalcomplications in sickle cell
disease. Br J Haematol2005;129:723–9.
16 Comer EW.Integrating the health and mentalhealth
needs of the chronically ill. A group of individuals with
depression and sickle celldisease.Soc Work Health
Care 2004;38(4):57–76.
17 GellerAK, O’ConnorMK. The sickle cellcrisis: A
dilemma in pain relief.Mayo Clin Proc 2008;83(3):
320–3.
18 Shapiro BS,Dinges DF,Orne EC,et al.Home man-
agementof sickle cell-related pain in children and
adolescents:Naturalhistory and impacton school
attendance. Pain 1995;61:139–44.
19 Ballas SK, Gupta K, Adams-Graves P. Sickle cellpain:
A criticalreappraisal. Blood 2012;120(18):3647–56.
20 Brousseau DC,Owens PL, Mosso AL, et al.Acute
care utilization and rehospitalizations forsickle cell
disease. JAMA 2010;303:1288–94.
21 A. D. A. M. Sickle cellanemia.2008. Available at:
http://www.nlm.nih.gov/medlineplus/ency/article/
000527.htm (accessed July 2013).
22 Steinberg MH.Managementof sickle celldisease.
NEJM 1999;340(13):1021–30.
23 Eisenberg DM,Davis RB,EttnerSL, et al.Trends in
alternative medicine use in the United States,1990–
1997:Results ofa follow-up nationalsurvey.JAMA
1998;280:1569–75.
24 NationalCenterfor Complementary and Alternative
Medicine.Whatis CAM? 2008. Available at:http://
nccam.nih.gov/health/whatiscam/(accessed July
2013).
25 Barnes PM,Bloom B,Nahin R Complementary and
alternative medicine use among adults and children:
United States.2007.CDC NationalHealth Statistics
Report #12. December 10, 2008. Available at: http://
nccam.nih.gov/sites/nccam.nih.gov/files/news/
nhsr12.pdf (accessed July 2013).
26 Konvicka JJ, Meyer TA, McDavid AJ, et al.
Complementary/alternativemedicine use among
chronic pain clinic patients. J PerianesthNurs
2008;23(1):17–23.
27 Sibinga EM, ShindellDL, Casella JF, Duggan AK,
Wilson MH. Pediatric patients with sickle celldisease:
Use of complementaryand alternativetherapies.
J Altern Comp Med 2006;12(3):291–8.
28 IBM Corp. Released 2010.IBM SPSS Statistics for
Windows, Version 19.0. Armonk, NY: IBM Corp.
29 Lee MM, Lin SS, Wrensch MR, et al. Alternative thera-
pies used by women with breast cancer in four ethnic
populations. J NatlCancer Inst 2000;92:42–7.
30 Boyd EL, TaylorSD, Shimp LA, Semler CR. An
assessment of home remedies use by African Ameri-
cans. J NatlMed Assoc 2000;92:341–53.
31 Greene AM,Walsh EG,Sirois FM,McCaffrey A.Per-
ceived benefitsof complementaryand alternative
medicine:A whole systems research perspective.
Open Comp Med J 2009;1:35–45.
32 Barnett MC, Cotroneo M, PurnellJ, et al. Use of CAM
in localAfrican-American communities:Community-
partnered research. J NatlMed Assoc 2003;95:943–
50.
33 Dunn KS,Horgas AL.The prevalence ofprayer as a
spiritualself-care modality in elders.J Holist Nurs
2000;18(4):337–51.
34 AARP and NCCAM. Complementary and alternative
medicine:Whatpeople 50 and olderare using and
discussing with theirphysicians.2007.Available at:
http://www.drhoffman.com/downloads/cam_2007
.pdf (accessed July 2013).
35 Austin JA. Why patients use alternative medicine.
JAMA 1998;279:1548–53.
36 Ndao-Brumblay SK,Green C.Predictors ofcomple-
mentary and alternative medicine use in chronic pain
patients. Pain Med 2010;11:16–24.
37 Birdee GS, Philips RS, Davis RB, Gardiner P. Factors
associated with pediatric use ofcomplementary and
alternative medicine. Pediatrics 2010;125:249–56.
38 NationalCenter for Alternative Complementary Medi-
cine. Chronic pain and CAM: At a glance. 2008. Avail-
able at: http://nccam.nih.gov/health/pain/chronic.htm
(accessed July 2013).
39 Shenfield G,Lim E, Allen H. Survey ofthe use of
complementary medicines and therapies in children
with asthma.J PaediatricChild Health 2002;38:
252–7.
Supporting Information
AdditionalSupporting Information may be found in the
online version of this article at the publisher’s web-site:
Appendix S1 An investigation of complementary alterna-
tive method in conjunction with pharmacologicalmethods
of pain controlfor sickle celldisease patients
246
Thompson and Eriator
Downloaded from https://academic.oup.com/painmedicine/article-abstract/15/2/241/1824660 by guest on 01 March 2019
July 30, 2013).
15 Anie KA. Psychologicalcomplications in sickle cell
disease. Br J Haematol2005;129:723–9.
16 Comer EW.Integrating the health and mentalhealth
needs of the chronically ill. A group of individuals with
depression and sickle celldisease.Soc Work Health
Care 2004;38(4):57–76.
17 GellerAK, O’ConnorMK. The sickle cellcrisis: A
dilemma in pain relief.Mayo Clin Proc 2008;83(3):
320–3.
18 Shapiro BS,Dinges DF,Orne EC,et al.Home man-
agementof sickle cell-related pain in children and
adolescents:Naturalhistory and impacton school
attendance. Pain 1995;61:139–44.
19 Ballas SK, Gupta K, Adams-Graves P. Sickle cellpain:
A criticalreappraisal. Blood 2012;120(18):3647–56.
20 Brousseau DC,Owens PL, Mosso AL, et al.Acute
care utilization and rehospitalizations forsickle cell
disease. JAMA 2010;303:1288–94.
21 A. D. A. M. Sickle cellanemia.2008. Available at:
http://www.nlm.nih.gov/medlineplus/ency/article/
000527.htm (accessed July 2013).
22 Steinberg MH.Managementof sickle celldisease.
NEJM 1999;340(13):1021–30.
23 Eisenberg DM,Davis RB,EttnerSL, et al.Trends in
alternative medicine use in the United States,1990–
1997:Results ofa follow-up nationalsurvey.JAMA
1998;280:1569–75.
24 NationalCenterfor Complementary and Alternative
Medicine.Whatis CAM? 2008. Available at:http://
nccam.nih.gov/health/whatiscam/(accessed July
2013).
25 Barnes PM,Bloom B,Nahin R Complementary and
alternative medicine use among adults and children:
United States.2007.CDC NationalHealth Statistics
Report #12. December 10, 2008. Available at: http://
nccam.nih.gov/sites/nccam.nih.gov/files/news/
nhsr12.pdf (accessed July 2013).
26 Konvicka JJ, Meyer TA, McDavid AJ, et al.
Complementary/alternativemedicine use among
chronic pain clinic patients. J PerianesthNurs
2008;23(1):17–23.
27 Sibinga EM, ShindellDL, Casella JF, Duggan AK,
Wilson MH. Pediatric patients with sickle celldisease:
Use of complementaryand alternativetherapies.
J Altern Comp Med 2006;12(3):291–8.
28 IBM Corp. Released 2010.IBM SPSS Statistics for
Windows, Version 19.0. Armonk, NY: IBM Corp.
29 Lee MM, Lin SS, Wrensch MR, et al. Alternative thera-
pies used by women with breast cancer in four ethnic
populations. J NatlCancer Inst 2000;92:42–7.
30 Boyd EL, TaylorSD, Shimp LA, Semler CR. An
assessment of home remedies use by African Ameri-
cans. J NatlMed Assoc 2000;92:341–53.
31 Greene AM,Walsh EG,Sirois FM,McCaffrey A.Per-
ceived benefitsof complementaryand alternative
medicine:A whole systems research perspective.
Open Comp Med J 2009;1:35–45.
32 Barnett MC, Cotroneo M, PurnellJ, et al. Use of CAM
in localAfrican-American communities:Community-
partnered research. J NatlMed Assoc 2003;95:943–
50.
33 Dunn KS,Horgas AL.The prevalence ofprayer as a
spiritualself-care modality in elders.J Holist Nurs
2000;18(4):337–51.
34 AARP and NCCAM. Complementary and alternative
medicine:Whatpeople 50 and olderare using and
discussing with theirphysicians.2007.Available at:
http://www.drhoffman.com/downloads/cam_2007
.pdf (accessed July 2013).
35 Austin JA. Why patients use alternative medicine.
JAMA 1998;279:1548–53.
36 Ndao-Brumblay SK,Green C.Predictors ofcomple-
mentary and alternative medicine use in chronic pain
patients. Pain Med 2010;11:16–24.
37 Birdee GS, Philips RS, Davis RB, Gardiner P. Factors
associated with pediatric use ofcomplementary and
alternative medicine. Pediatrics 2010;125:249–56.
38 NationalCenter for Alternative Complementary Medi-
cine. Chronic pain and CAM: At a glance. 2008. Avail-
able at: http://nccam.nih.gov/health/pain/chronic.htm
(accessed July 2013).
39 Shenfield G,Lim E, Allen H. Survey ofthe use of
complementary medicines and therapies in children
with asthma.J PaediatricChild Health 2002;38:
252–7.
Supporting Information
AdditionalSupporting Information may be found in the
online version of this article at the publisher’s web-site:
Appendix S1 An investigation of complementary alterna-
tive method in conjunction with pharmacologicalmethods
of pain controlfor sickle celldisease patients
246
Thompson and Eriator
Downloaded from https://academic.oup.com/painmedicine/article-abstract/15/2/241/1824660 by guest on 01 March 2019
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 6
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.