Primary Nursing in Dialysis Outpatient Setting Report
VerifiedAdded on 2019/10/18
|11
|3224
|163
Report
AI Summary
This report provides a comprehensive overview of primary nursing in a haemodialysis outpatient setting, focusing on the care of patients with chronic kidney disease. It begins by establishing the significance of haemodialysis as a critical treatment modality and addresses the associated uncertainties from a patient's perspective. The report then employs the PICO (Population, Intervention, Comparator, Outcome) model to frame research questions related to haemodialysis. A literature review is conducted, utilizing databases such as PubMed and Dovepress, to gather evidence on best practices, outcomes, and challenges. The findings are discussed, highlighting variations in dialysis facility practices and the importance of evidence-based practice (EBP) in nursing. Barriers to EBP adoption, such as institutional factors and lack of resources, are identified, along with strategies to overcome these challenges, including staff education, interdisciplinary communication, and supportive management. The report emphasizes the need for nurses to utilize research literature in clinical decision-making and provides a framework for enhancing the quality and effectiveness of haemodialysis care.
PRIMARY NURSING IN DIALYSIS OUTPATIENT SETTING
Task-1: Haemodialysis
Chronic kidney disease (CKD) is now recognized as a common condition that elevates the
risk of cardiovascular disease as well as kidney failure and other complications. The number
of patients with kidney failure treated by dialysis and transplantation (the end stage of CKD)
has increased dramatically in the United States since 1991 (Sarnak et al., 2003). The
occurrence at end stages of renal disease can lead to death unless renal replacement is started.
Unless adequate is provided to the patients with kidney failure, can lead to death of the
patient. The major management strategies include dialysis (Al Wakeel, 2014) and
transplantation (Mosconi et al., 2010). For the vast majority of adult patients with diverse
ages, dialysis will be treatment modality (Korevaar et al., 2003). Two major types of dialysis
are available including haemodialysis and peritoneal dialysis. The processes are used to
remove the biological wastes such as urea, ammonia and toxins forded as the result of
metabolism. Although medical, social, or logistic considerations may preclude one of the
dialysis forms, for most patients a well-considered deliberation has to be made between
starting with haemodialysis or with peritoneal dialysis. It indicates that haemodialysis is one
of the management strategy for kidney failure. Therefore, the topic on ‘haemodialysis’ is
chosen to address the uncertainties associated with the care of patients from patients view.
The uncertainities are addressed utilizing evidences.
Task-2: PICO
This section describes the PICO (Population, Intervention, Comparator, and Outcome) model
as a tool to address health related problems (Huang et al., 2006). The PICO model is
considered as a good approach for framing a “foreground” research question (Aslam &
Emmanuel, 2010). The present case is related to patients with kidney failure and the use of
haemodialysis. Since the procedures and precautions to be taken for initiation of
haemodialysis, a PICO is desired to be in place to handle the cases. The PICO so developed
is shown Table-1
1
Task-1: Haemodialysis
Chronic kidney disease (CKD) is now recognized as a common condition that elevates the
risk of cardiovascular disease as well as kidney failure and other complications. The number
of patients with kidney failure treated by dialysis and transplantation (the end stage of CKD)
has increased dramatically in the United States since 1991 (Sarnak et al., 2003). The
occurrence at end stages of renal disease can lead to death unless renal replacement is started.
Unless adequate is provided to the patients with kidney failure, can lead to death of the
patient. The major management strategies include dialysis (Al Wakeel, 2014) and
transplantation (Mosconi et al., 2010). For the vast majority of adult patients with diverse
ages, dialysis will be treatment modality (Korevaar et al., 2003). Two major types of dialysis
are available including haemodialysis and peritoneal dialysis. The processes are used to
remove the biological wastes such as urea, ammonia and toxins forded as the result of
metabolism. Although medical, social, or logistic considerations may preclude one of the
dialysis forms, for most patients a well-considered deliberation has to be made between
starting with haemodialysis or with peritoneal dialysis. It indicates that haemodialysis is one
of the management strategy for kidney failure. Therefore, the topic on ‘haemodialysis’ is
chosen to address the uncertainties associated with the care of patients from patients view.
The uncertainities are addressed utilizing evidences.
Task-2: PICO
This section describes the PICO (Population, Intervention, Comparator, and Outcome) model
as a tool to address health related problems (Huang et al., 2006). The PICO model is
considered as a good approach for framing a “foreground” research question (Aslam &
Emmanuel, 2010). The present case is related to patients with kidney failure and the use of
haemodialysis. Since the procedures and precautions to be taken for initiation of
haemodialysis, a PICO is desired to be in place to handle the cases. The PICO so developed
is shown Table-1
1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
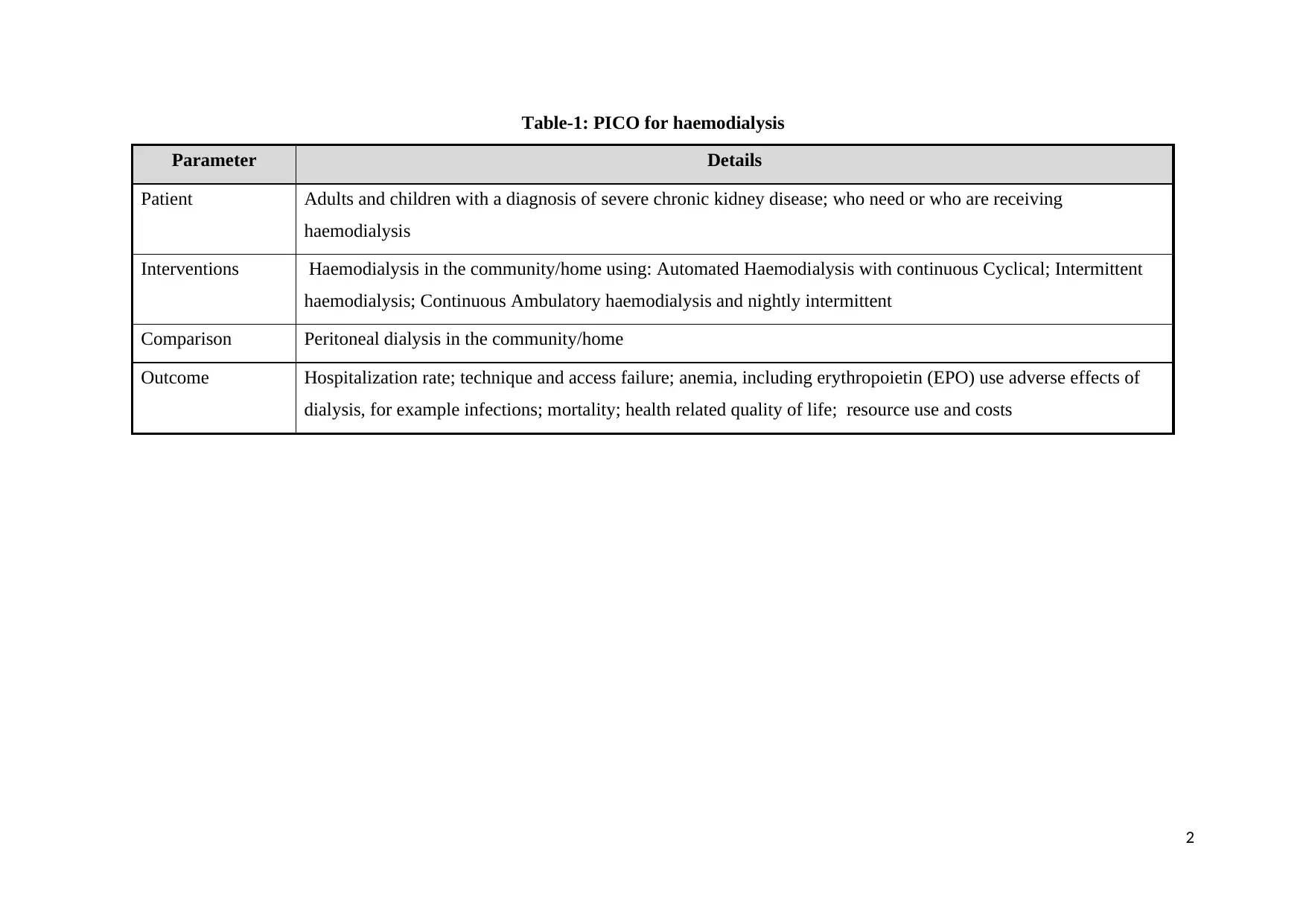
Table-1: PICO for haemodialysis
Parameter Details
Patient Adults and children with a diagnosis of severe chronic kidney disease; who need or who are receiving
haemodialysis
Interventions Haemodialysis in the community/home using: Automated Haemodialysis with continuous Cyclical; Intermittent
haemodialysis; Continuous Ambulatory haemodialysis and nightly intermittent
Comparison Peritoneal dialysis in the community/home
Outcome Hospitalization rate; technique and access failure; anemia, including erythropoietin (EPO) use adverse effects of
dialysis, for example infections; mortality; health related quality of life; resource use and costs
2
Parameter Details
Patient Adults and children with a diagnosis of severe chronic kidney disease; who need or who are receiving
haemodialysis
Interventions Haemodialysis in the community/home using: Automated Haemodialysis with continuous Cyclical; Intermittent
haemodialysis; Continuous Ambulatory haemodialysis and nightly intermittent
Comparison Peritoneal dialysis in the community/home
Outcome Hospitalization rate; technique and access failure; anemia, including erythropoietin (EPO) use adverse effects of
dialysis, for example infections; mortality; health related quality of life; resource use and costs
2
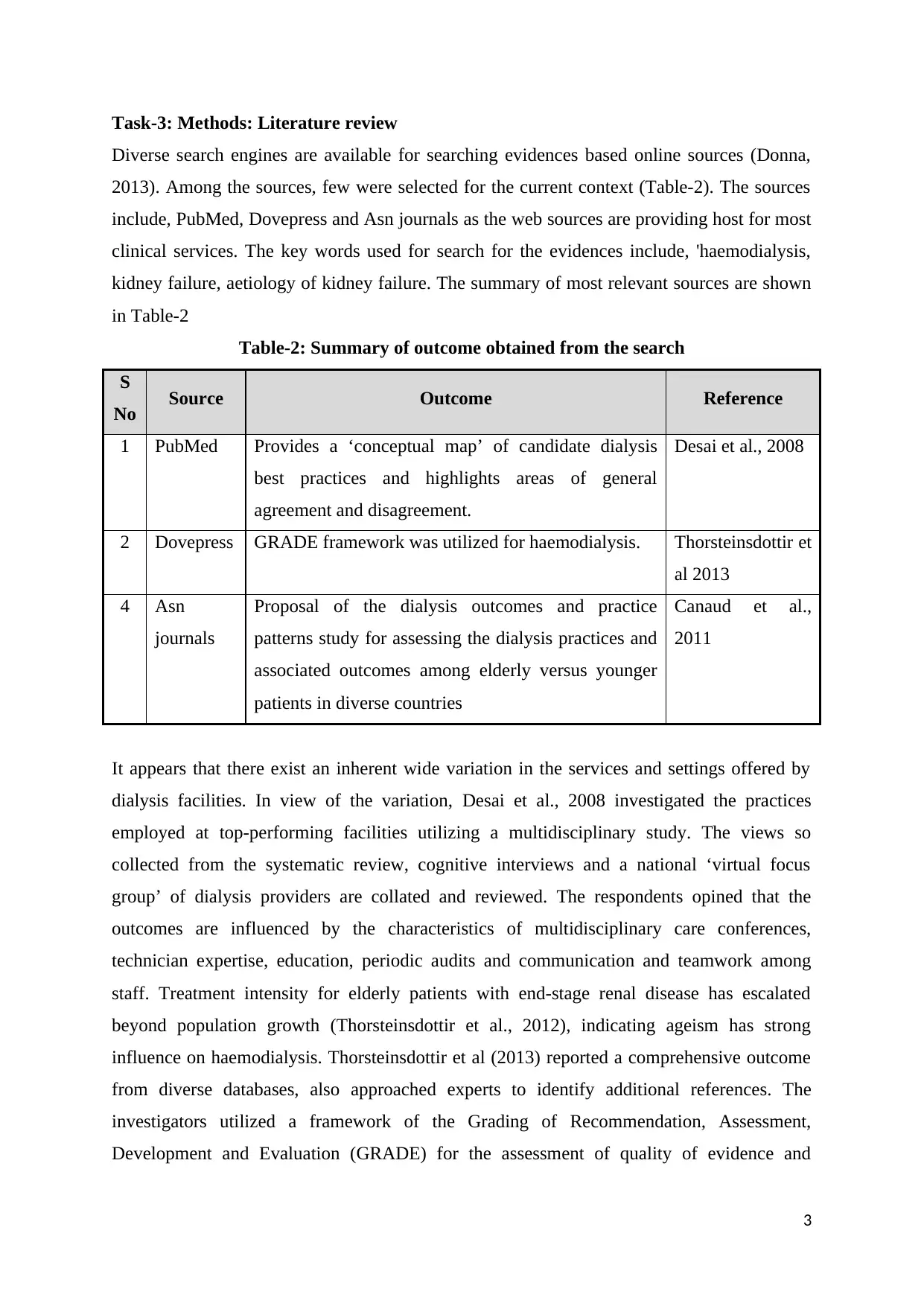
Task-3: Methods: Literature review
Diverse search engines are available for searching evidences based online sources (Donna,
2013). Among the sources, few were selected for the current context (Table-2). The sources
include, PubMed, Dovepress and Asn journals as the web sources are providing host for most
clinical services. The key words used for search for the evidences include, 'haemodialysis,
kidney failure, aetiology of kidney failure. The summary of most relevant sources are shown
in Table-2
Table-2: Summary of outcome obtained from the search
S
No Source Outcome Reference
1 PubMed Provides a ‘conceptual map’ of candidate dialysis
best practices and highlights areas of general
agreement and disagreement.
Desai et al., 2008
2 Dovepress GRADE framework was utilized for haemodialysis. Thorsteinsdottir et
al 2013
4 Asn
journals
Proposal of the dialysis outcomes and practice
patterns study for assessing the dialysis practices and
associated outcomes among elderly versus younger
patients in diverse countries
Canaud et al.,
2011
It appears that there exist an inherent wide variation in the services and settings offered by
dialysis facilities. In view of the variation, Desai et al., 2008 investigated the practices
employed at top-performing facilities utilizing a multidisciplinary study. The views so
collected from the systematic review, cognitive interviews and a national ‘virtual focus
group’ of dialysis providers are collated and reviewed. The respondents opined that the
outcomes are influenced by the characteristics of multidisciplinary care conferences,
technician expertise, education, periodic audits and communication and teamwork among
staff. Treatment intensity for elderly patients with end-stage renal disease has escalated
beyond population growth (Thorsteinsdottir et al., 2012), indicating ageism has strong
influence on haemodialysis. Thorsteinsdottir et al (2013) reported a comprehensive outcome
from diverse databases, also approached experts to identify additional references. The
investigators utilized a framework of the Grading of Recommendation, Assessment,
Development and Evaluation (GRADE) for the assessment of quality of evidence and
3
Diverse search engines are available for searching evidences based online sources (Donna,
2013). Among the sources, few were selected for the current context (Table-2). The sources
include, PubMed, Dovepress and Asn journals as the web sources are providing host for most
clinical services. The key words used for search for the evidences include, 'haemodialysis,
kidney failure, aetiology of kidney failure. The summary of most relevant sources are shown
in Table-2
Table-2: Summary of outcome obtained from the search
S
No Source Outcome Reference
1 PubMed Provides a ‘conceptual map’ of candidate dialysis
best practices and highlights areas of general
agreement and disagreement.
Desai et al., 2008
2 Dovepress GRADE framework was utilized for haemodialysis. Thorsteinsdottir et
al 2013
4 Asn
journals
Proposal of the dialysis outcomes and practice
patterns study for assessing the dialysis practices and
associated outcomes among elderly versus younger
patients in diverse countries
Canaud et al.,
2011
It appears that there exist an inherent wide variation in the services and settings offered by
dialysis facilities. In view of the variation, Desai et al., 2008 investigated the practices
employed at top-performing facilities utilizing a multidisciplinary study. The views so
collected from the systematic review, cognitive interviews and a national ‘virtual focus
group’ of dialysis providers are collated and reviewed. The respondents opined that the
outcomes are influenced by the characteristics of multidisciplinary care conferences,
technician expertise, education, periodic audits and communication and teamwork among
staff. Treatment intensity for elderly patients with end-stage renal disease has escalated
beyond population growth (Thorsteinsdottir et al., 2012), indicating ageism has strong
influence on haemodialysis. Thorsteinsdottir et al (2013) reported a comprehensive outcome
from diverse databases, also approached experts to identify additional references. The
investigators utilized a framework of the Grading of Recommendation, Assessment,
Development and Evaluation (GRADE) for the assessment of quality of evidence and
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

strength of recommendations. There exist certain limitations for the balance of benefits and
risks for the initiation of haemodialysis in elderly patients based on the proposals. In another
investigation, Canaud et al., (2011) derived and proposed certain recommendations. The
investigators observed that malnutrition as one of the common cause in elderly patients along
with a low ultra filtration rate. Despite of increasing threshold for haemodialysis, there are no
standard guidelines for the procedures to be adopted. The Dialysis Outcomes and Practice
Patterns Study (DOPPS) provide a unique opportunity for the assessment of dialysis practices
in elderly and younger patients.
Task-4: Discussion of findings
Dasia et al., (2008) described the dialysis facilities and their outcomes across the U.S dialysis
facilities for the categorization. Accordingly, the facilities can be grouped as top performing
and bottom performing centres. From the evidences, it can believed that facility-level
outcomes may be related to a series of procedural best practices, including physician-level
practices (e.g., rapidly returning pages), nurse-level practices (e.g., creating nursing teams
that optimally match experience), staff enhancement practices (e.g., appointing a dedicated
anaemia manager), and dialysis scheduling practices (e.g., developing formal systems to
correct short staffing), among many others. The authors have not compared the outcome with
available sources to potentiate the arguments. Despite of lack of clarifications fully, the
investigation gave an insight of needs of dialysis as one of the routine health maintenance
services. Thorsteinsdottir et al (2013) have not made any comparison pertaining to large
cohort data for patients with conservative treatment. The survival aspects were taken into
consideration for the patients who were recommended for palliative care (USRDS, 2008) and
another study looked at looked at median survival for the patients with low glomerular
filtration rate. Another study (Canaud et al., 2011) reveals that the number of elderly patients
are increasing on renal replacement therapy worldwide (Gitto et al., 2008) leading increasing
the health care costs. The available literature lacking the development of health pyramids to
understand the differing approaches and levels of evidence (Rebecca, 2016). EBP includes
respect of patient values, and their needs, whilst delivering high-quality, cost effective health
care. Understanding the differing levels of evidence and their reliability, is paramount to
making correct and appropriate health care decisions pertaining to the setting of care for
haemodialysis. The nurses are required to use EBP as they are responsible for a significant
amount of judgments and decisions every day, and therefore, they must use research literature
as part of their clinical decision-making. Most literature available is lacking the pyramid of
4
risks for the initiation of haemodialysis in elderly patients based on the proposals. In another
investigation, Canaud et al., (2011) derived and proposed certain recommendations. The
investigators observed that malnutrition as one of the common cause in elderly patients along
with a low ultra filtration rate. Despite of increasing threshold for haemodialysis, there are no
standard guidelines for the procedures to be adopted. The Dialysis Outcomes and Practice
Patterns Study (DOPPS) provide a unique opportunity for the assessment of dialysis practices
in elderly and younger patients.
Task-4: Discussion of findings
Dasia et al., (2008) described the dialysis facilities and their outcomes across the U.S dialysis
facilities for the categorization. Accordingly, the facilities can be grouped as top performing
and bottom performing centres. From the evidences, it can believed that facility-level
outcomes may be related to a series of procedural best practices, including physician-level
practices (e.g., rapidly returning pages), nurse-level practices (e.g., creating nursing teams
that optimally match experience), staff enhancement practices (e.g., appointing a dedicated
anaemia manager), and dialysis scheduling practices (e.g., developing formal systems to
correct short staffing), among many others. The authors have not compared the outcome with
available sources to potentiate the arguments. Despite of lack of clarifications fully, the
investigation gave an insight of needs of dialysis as one of the routine health maintenance
services. Thorsteinsdottir et al (2013) have not made any comparison pertaining to large
cohort data for patients with conservative treatment. The survival aspects were taken into
consideration for the patients who were recommended for palliative care (USRDS, 2008) and
another study looked at looked at median survival for the patients with low glomerular
filtration rate. Another study (Canaud et al., 2011) reveals that the number of elderly patients
are increasing on renal replacement therapy worldwide (Gitto et al., 2008) leading increasing
the health care costs. The available literature lacking the development of health pyramids to
understand the differing approaches and levels of evidence (Rebecca, 2016). EBP includes
respect of patient values, and their needs, whilst delivering high-quality, cost effective health
care. Understanding the differing levels of evidence and their reliability, is paramount to
making correct and appropriate health care decisions pertaining to the setting of care for
haemodialysis. The nurses are required to use EBP as they are responsible for a significant
amount of judgments and decisions every day, and therefore, they must use research literature
as part of their clinical decision-making. Most literature available is lacking the pyramid of
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
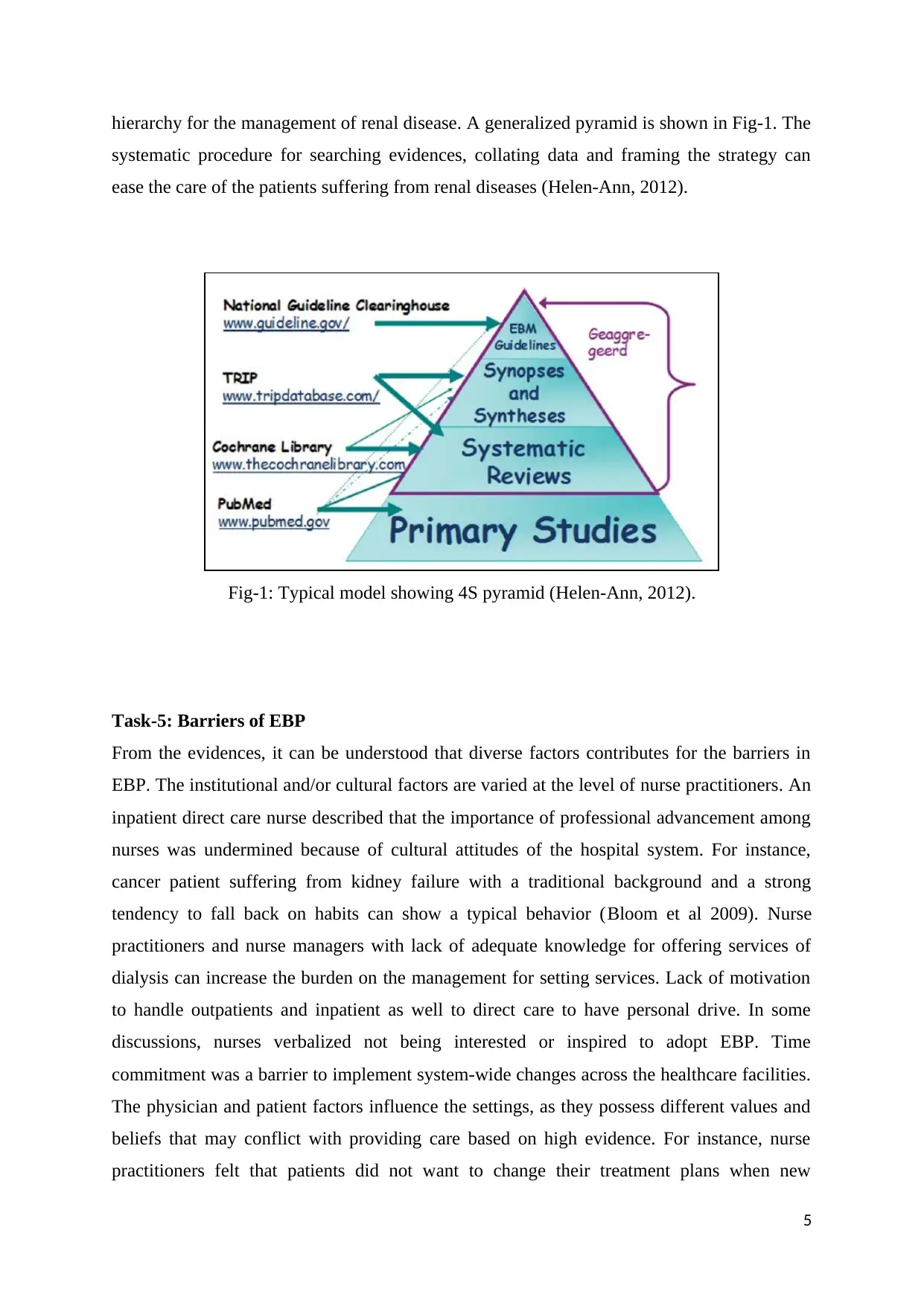
hierarchy for the management of renal disease. A generalized pyramid is shown in Fig-1. The
systematic procedure for searching evidences, collating data and framing the strategy can
ease the care of the patients suffering from renal diseases (Helen-Ann, 2012).
Fig-1: Typical model showing 4S pyramid (Helen-Ann, 2012).
Task-5: Barriers of EBP
From the evidences, it can be understood that diverse factors contributes for the barriers in
EBP. The institutional and/or cultural factors are varied at the level of nurse practitioners. An
inpatient direct care nurse described that the importance of professional advancement among
nurses was undermined because of cultural attitudes of the hospital system. For instance,
cancer patient suffering from kidney failure with a traditional background and a strong
tendency to fall back on habits can show a typical behavior (Bloom et al 2009). Nurse
practitioners and nurse managers with lack of adequate knowledge for offering services of
dialysis can increase the burden on the management for setting services. Lack of motivation
to handle outpatients and inpatient as well to direct care to have personal drive. In some
discussions, nurses verbalized not being interested or inspired to adopt EBP. Time
commitment was a barrier to implement system-wide changes across the healthcare facilities.
The physician and patient factors influence the settings, as they possess different values and
beliefs that may conflict with providing care based on high evidence. For instance, nurse
practitioners felt that patients did not want to change their treatment plans when new
5
systematic procedure for searching evidences, collating data and framing the strategy can
ease the care of the patients suffering from renal diseases (Helen-Ann, 2012).
Fig-1: Typical model showing 4S pyramid (Helen-Ann, 2012).
Task-5: Barriers of EBP
From the evidences, it can be understood that diverse factors contributes for the barriers in
EBP. The institutional and/or cultural factors are varied at the level of nurse practitioners. An
inpatient direct care nurse described that the importance of professional advancement among
nurses was undermined because of cultural attitudes of the hospital system. For instance,
cancer patient suffering from kidney failure with a traditional background and a strong
tendency to fall back on habits can show a typical behavior (Bloom et al 2009). Nurse
practitioners and nurse managers with lack of adequate knowledge for offering services of
dialysis can increase the burden on the management for setting services. Lack of motivation
to handle outpatients and inpatient as well to direct care to have personal drive. In some
discussions, nurses verbalized not being interested or inspired to adopt EBP. Time
commitment was a barrier to implement system-wide changes across the healthcare facilities.
The physician and patient factors influence the settings, as they possess different values and
beliefs that may conflict with providing care based on high evidence. For instance, nurse
practitioners felt that patients did not want to change their treatment plans when new
5
evidence emerged. In addition, the limited access to up-to-date user-friendly technology and
computer systems can also influence the settings for patients with haemodialysis.
The strategies that can be applied to overcome the barriers for the adoption of evidence-based
practice include adequate education of nursing staff to improve their technical and soft skills.
The implementation of interdisciplinary communication and collaboration, mentorship,
access to professional activities and networks, and supportive management as crucial to EBP
adoption can enhance the adoptability towards services. The nurses should be trained for the
advancements of treatment along with certain diagnostic approaches. These facilitate the
nurses to acquire knowledge and can set the services for outpatients. The hospital
management should conduct periodic assessment programs for the nurse practitioners and
organize the trainings. The decision-making capacities for nurses should be increased and
powers for autonomy can be given to take decisions voluntarily with respect to situation.
6
computer systems can also influence the settings for patients with haemodialysis.
The strategies that can be applied to overcome the barriers for the adoption of evidence-based
practice include adequate education of nursing staff to improve their technical and soft skills.
The implementation of interdisciplinary communication and collaboration, mentorship,
access to professional activities and networks, and supportive management as crucial to EBP
adoption can enhance the adoptability towards services. The nurses should be trained for the
advancements of treatment along with certain diagnostic approaches. These facilitate the
nurses to acquire knowledge and can set the services for outpatients. The hospital
management should conduct periodic assessment programs for the nurse practitioners and
organize the trainings. The decision-making capacities for nurses should be increased and
powers for autonomy can be given to take decisions voluntarily with respect to situation.
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
References
AL WAKEEL, JS (2014) Kidney function and metabolic profile of chronic kidney disease
and hemodialysis patients during Ramadan fasting. Iran J Kidney Dis. 8(4). p. 21-8.
ASLAM, S and EMMANUEL, P. (2010). Formulating a researchable question: A critical
step for facilitating good clinical research. Indian Journal of Sexually Transmitted
Diseases, 31(1), 47–50
BLOOM, H. G., AHMED, I., ALESSI, C. A., ANCOLI-ISRAEL, S., BUYSSE, D. J.,
KRYGER, M. H., BARBARA A.P., MICHAEL, J.T., MICHAEL, V.V AND ZEE, P.
C. (2009). Evidence-Based Recommendations for the Assessment and Management
of Sleep Disorders in Older Persons. Journal of the American Geriatrics Society,
57(5). p. 761–789.
CANAUD, B., TONG, L., TENTORI, F., AKIBA, T., KARABOYAS, A., GILLESPIE, B.,
and PORT, F. K. (2011). Clinical Practices and Outcomes in Elderly Hemodialysis
Patients: Results from the Dialysis Outcomes and Practice Patterns Study
(DOPPS). Clinical Journal of the American Society of Nephrology : CJASN,6(7),
1651–1662. http://doi.org/10.2215/CJN.03530410
DESAI, A. A., BOLUS, R., NISSENSON, A., BOLUS, S., SOLOMON, M. D., KHAWAR,
O., GITLIN, M., TALLEY, J AND SPIEGEL, B. M. R. (2008). Identifying Best
Practices in Dialysis Care: Results of Cognitive Interviews and a National Survey of
Dialysis Providers. Clinical Journal of the American Society of Nephrology 3(4). p.
1066–1076. http://doi.org/10.2215/CJN.04421007
DONNA, W (2013) Searching for the right evidence: how to answer your clinical questions
using the 6S hierarchy Evidence-Based Medicine 18 (3) p. 93-97
GITTO, LSV., SANTORO, D., BELLINGHIERI, G., BIAGIO, DI., LI, VM and SANTO,
NG (2008) Survival in octogenarian dialysis patients: Analysis in two Southern Italian
regions. J Nephrol 21, p.118–123
HELEN-ANN, BE (2012) Let’s Climb an Evidence Pyramid Journal of Hospital
Librarianship, 12, p. 218-228
HUANG, X., LIN, J and DEMNER-FUSHMAN, D. (2006). Evaluation of PICO as a
Knowledge Representation for Clinical Questions. Annual Symposium Proceedings,
2006. P. 359–363.
KOREVAAR, JC., FEITH, GW., DEKKER, FW., VAN MANEN, JG., BOESCHOTEN,
EW., BOSSUYT PM and KREDIET RT. (2003) Effect of starting with hemodialysis
7
AL WAKEEL, JS (2014) Kidney function and metabolic profile of chronic kidney disease
and hemodialysis patients during Ramadan fasting. Iran J Kidney Dis. 8(4). p. 21-8.
ASLAM, S and EMMANUEL, P. (2010). Formulating a researchable question: A critical
step for facilitating good clinical research. Indian Journal of Sexually Transmitted
Diseases, 31(1), 47–50
BLOOM, H. G., AHMED, I., ALESSI, C. A., ANCOLI-ISRAEL, S., BUYSSE, D. J.,
KRYGER, M. H., BARBARA A.P., MICHAEL, J.T., MICHAEL, V.V AND ZEE, P.
C. (2009). Evidence-Based Recommendations for the Assessment and Management
of Sleep Disorders in Older Persons. Journal of the American Geriatrics Society,
57(5). p. 761–789.
CANAUD, B., TONG, L., TENTORI, F., AKIBA, T., KARABOYAS, A., GILLESPIE, B.,
and PORT, F. K. (2011). Clinical Practices and Outcomes in Elderly Hemodialysis
Patients: Results from the Dialysis Outcomes and Practice Patterns Study
(DOPPS). Clinical Journal of the American Society of Nephrology : CJASN,6(7),
1651–1662. http://doi.org/10.2215/CJN.03530410
DESAI, A. A., BOLUS, R., NISSENSON, A., BOLUS, S., SOLOMON, M. D., KHAWAR,
O., GITLIN, M., TALLEY, J AND SPIEGEL, B. M. R. (2008). Identifying Best
Practices in Dialysis Care: Results of Cognitive Interviews and a National Survey of
Dialysis Providers. Clinical Journal of the American Society of Nephrology 3(4). p.
1066–1076. http://doi.org/10.2215/CJN.04421007
DONNA, W (2013) Searching for the right evidence: how to answer your clinical questions
using the 6S hierarchy Evidence-Based Medicine 18 (3) p. 93-97
GITTO, LSV., SANTORO, D., BELLINGHIERI, G., BIAGIO, DI., LI, VM and SANTO,
NG (2008) Survival in octogenarian dialysis patients: Analysis in two Southern Italian
regions. J Nephrol 21, p.118–123
HELEN-ANN, BE (2012) Let’s Climb an Evidence Pyramid Journal of Hospital
Librarianship, 12, p. 218-228
HUANG, X., LIN, J and DEMNER-FUSHMAN, D. (2006). Evaluation of PICO as a
Knowledge Representation for Clinical Questions. Annual Symposium Proceedings,
2006. P. 359–363.
KOREVAAR, JC., FEITH, GW., DEKKER, FW., VAN MANEN, JG., BOESCHOTEN,
EW., BOSSUYT PM and KREDIET RT. (2003) Effect of starting with hemodialysis
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
compared with peritoneal dialysis in patients new on dialysis treatment: a randomized
controlled trial. Kidney Int. 64(6) p. 2222-8
MOSCONI, G., PANICALI, L., PERSICI, E., CONTE, D., CAPPUCCILLI, ML., CUNA,
V., CAPELLI, I., TODESCHINI, P., D'ARCANGELO, GL and STEFONI, S (2010)
Native kidney function after renal transplantation combined with other solid organs in
pre-emptive patients. Transplant Proc. 42(4) .p. 1017-20. doi:
10.1016/j.transproceed.2010.03.125.
REBECCA, I-B (2016) A nurses’ guide to the hierarchy of research designs and evidence
Australian Journal Advanced Nursing 33(3) 38-43
SARNAK, MJ., LEVEY, AS., SCHOOLWERTH, AC., CORESH, J., CULLETON, B.,
HAMM, LL., MCCULLOUGH, PA., KASISKE, BL., KELEPOURIS, E., KLAG,
MJ., PARFREY, P., PFEFFER, M., RAIJ, L., SPINOSA, DJ and WILSON, PW
(2003) Kidney disease as a risk factor for development of cardiovascular disease: a
statement from the American Heart Association Councils on kidney in cardiovascular
disease, high blood pressure research, clinical cardiology, and epidemiology and
prevention. Hypertension. 42(5). p. 050-65.
THORSTEINSDOTTIR, B., MONTORI, V. M., PROKOP, L. J., & MURAD, M. H. (2013).
Ageism vs the technical imperative, applying the GRADE framework to the evidence
on hemodialysis in very elderly patients. Clinical Interventions in Aging, 8. p. 797–
807. http://doi.org/10.2147/CIA.S43817
THORSTEINSDOTTIR, B., SWETZ, K. M., FEELY, M. A., MUELLER, P. S., &
WILLIAMS, A. W. (2012). Are There Alternatives to Hemodialysis for the Elderly
Patient With End-Stage Renal Failure? Mayo Clinic Proceedings, 87(6), 514–516.
http://doi.org/10.1016/j.mayocp.2012.02.016
USRDS (2008) US Renal Data System Annual Data Report: Atlas of Chronic Kidney
Disease and End-Stage Renal Disease in the United States. Bethesda, MD: National
Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases
8
controlled trial. Kidney Int. 64(6) p. 2222-8
MOSCONI, G., PANICALI, L., PERSICI, E., CONTE, D., CAPPUCCILLI, ML., CUNA,
V., CAPELLI, I., TODESCHINI, P., D'ARCANGELO, GL and STEFONI, S (2010)
Native kidney function after renal transplantation combined with other solid organs in
pre-emptive patients. Transplant Proc. 42(4) .p. 1017-20. doi:
10.1016/j.transproceed.2010.03.125.
REBECCA, I-B (2016) A nurses’ guide to the hierarchy of research designs and evidence
Australian Journal Advanced Nursing 33(3) 38-43
SARNAK, MJ., LEVEY, AS., SCHOOLWERTH, AC., CORESH, J., CULLETON, B.,
HAMM, LL., MCCULLOUGH, PA., KASISKE, BL., KELEPOURIS, E., KLAG,
MJ., PARFREY, P., PFEFFER, M., RAIJ, L., SPINOSA, DJ and WILSON, PW
(2003) Kidney disease as a risk factor for development of cardiovascular disease: a
statement from the American Heart Association Councils on kidney in cardiovascular
disease, high blood pressure research, clinical cardiology, and epidemiology and
prevention. Hypertension. 42(5). p. 050-65.
THORSTEINSDOTTIR, B., MONTORI, V. M., PROKOP, L. J., & MURAD, M. H. (2013).
Ageism vs the technical imperative, applying the GRADE framework to the evidence
on hemodialysis in very elderly patients. Clinical Interventions in Aging, 8. p. 797–
807. http://doi.org/10.2147/CIA.S43817
THORSTEINSDOTTIR, B., SWETZ, K. M., FEELY, M. A., MUELLER, P. S., &
WILLIAMS, A. W. (2012). Are There Alternatives to Hemodialysis for the Elderly
Patient With End-Stage Renal Failure? Mayo Clinic Proceedings, 87(6), 514–516.
http://doi.org/10.1016/j.mayocp.2012.02.016
USRDS (2008) US Renal Data System Annual Data Report: Atlas of Chronic Kidney
Disease and End-Stage Renal Disease in the United States. Bethesda, MD: National
Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases
8
Appendix-I (Desai et al., 2008)
Objectives: To inventory "best practices" that may represent inter facility varieties in results.
Techniques: Multidisciplinary study was distinguished in dialysis by means of organized
procedure, including precise survey, intellectual meetings, and a national "virtual center
gathering" of dialysis suppliers took after by positioning the significance as controlled by
mean RAND
Results: The respondents trusted dialysis results are most emphatically identified with
attributes of multidisciplinary consideration gatherings; specialist capability in ensuring
vascular access; preparing of medical attendants to give training in liquid administration,
vascular access, and sustenance; utilization of arbitrary and blinded reviews of staff
execution, and correspondence and collaboration among staff.
Conclusions: The study gives a "reasonable guide" of applicant dialysis best practices and
highlights ranges of general understanding and contradiction.
9
Objectives: To inventory "best practices" that may represent inter facility varieties in results.
Techniques: Multidisciplinary study was distinguished in dialysis by means of organized
procedure, including precise survey, intellectual meetings, and a national "virtual center
gathering" of dialysis suppliers took after by positioning the significance as controlled by
mean RAND
Results: The respondents trusted dialysis results are most emphatically identified with
attributes of multidisciplinary consideration gatherings; specialist capability in ensuring
vascular access; preparing of medical attendants to give training in liquid administration,
vascular access, and sustenance; utilization of arbitrary and blinded reviews of staff
execution, and correspondence and collaboration among staff.
Conclusions: The study gives a "reasonable guide" of applicant dialysis best practices and
highlights ranges of general understanding and contradiction.
9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Appendix-II (Thorsteinsdottir et al 2013)
Goals: To decide the part of "Ageism" (age, forecast, or useful status) on haemodialysis
(HD)
Patients and strategies: A thorough hunt of a few databases was led for methodical audits of
clinical and monetary results of haemodialysis patients' elderly. The techniques are connected
the thorough structure of decisional elements of the Grading of Recommendation,
Assessment, Development and Evaluation (GRADE) to assess the nature of proof and quality
of suggestions.
Results: The nature of the confirmation to bolster the present proposal of HD start for most
elderly patients is low. There is noteworthy instability in a critical position of advantages and
dangers, understanding inclination, and whether defaults HD in this patient populace is an
insightful utilization of assets.
Conclusions: Following the GRADE system, proposal for HD in this populace would be
feeble.
10
Goals: To decide the part of "Ageism" (age, forecast, or useful status) on haemodialysis
(HD)
Patients and strategies: A thorough hunt of a few databases was led for methodical audits of
clinical and monetary results of haemodialysis patients' elderly. The techniques are connected
the thorough structure of decisional elements of the Grading of Recommendation,
Assessment, Development and Evaluation (GRADE) to assess the nature of proof and quality
of suggestions.
Results: The nature of the confirmation to bolster the present proposal of HD start for most
elderly patients is low. There is noteworthy instability in a critical position of advantages and
dangers, understanding inclination, and whether defaults HD in this patient populace is an
insightful utilization of assets.
Conclusions: Following the GRADE system, proposal for HD in this populace would be
feeble.
10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Appendix-III (Canaud et al., 2011)
Background and objectives: Demand for haemodialysis among elderly patients is
expanding around the world. Albeit clinical consideration of this high-chance gathering is
mind boggling and testing, no rules exist to advice haemodialysis rehearses. The Dialysis
Outcomes and Practice Patterns Study (DOPPS) gives a novel chance to evaluate dialysis
hones and related results among elderly versus more youthful patients on endless in-focus
haemodialysis in 12 nations.
Techniques: Clinical attributes, dialysis practices, and results of elderly versus more
youthful patients were looked at among members in four DOPPS locales in 2005 through
2007.
Results: Although member mean age expanded after some time in all DOPPS nations, the
rate of elderly differed broadly. By and large, comorbidities and lack of healthy sustenance
were more basic in the elderly. Fistulae were utilized less as often as possible among elderly
versus more youthful patients in different nations. No distinction in treatment time was seen
amongst elderly and more youthful patients subsequent to normalizing for body weight. In all
locales, ultra filtration rates were lower among elderly patients. Elderly patients reported
poorer personal satisfaction concerning the physical yet not mental segment scores. Mortality
danger was three-to sixfold higher in the elderly gathering, though reasons for death generally
speaking were comparable for elderly and more youthful patients.
Conclusions: Elderly patients speak to an alternate extent of DOPPS members crosswise
over nations, conceivably reflecting contrasts in arrangements and clinical practices. By and
large, haemodialysis rehearses in the elderly mirrored every area's clinical examples, with
some variety by age bunch contingent on the practice.
11
Background and objectives: Demand for haemodialysis among elderly patients is
expanding around the world. Albeit clinical consideration of this high-chance gathering is
mind boggling and testing, no rules exist to advice haemodialysis rehearses. The Dialysis
Outcomes and Practice Patterns Study (DOPPS) gives a novel chance to evaluate dialysis
hones and related results among elderly versus more youthful patients on endless in-focus
haemodialysis in 12 nations.
Techniques: Clinical attributes, dialysis practices, and results of elderly versus more
youthful patients were looked at among members in four DOPPS locales in 2005 through
2007.
Results: Although member mean age expanded after some time in all DOPPS nations, the
rate of elderly differed broadly. By and large, comorbidities and lack of healthy sustenance
were more basic in the elderly. Fistulae were utilized less as often as possible among elderly
versus more youthful patients in different nations. No distinction in treatment time was seen
amongst elderly and more youthful patients subsequent to normalizing for body weight. In all
locales, ultra filtration rates were lower among elderly patients. Elderly patients reported
poorer personal satisfaction concerning the physical yet not mental segment scores. Mortality
danger was three-to sixfold higher in the elderly gathering, though reasons for death generally
speaking were comparable for elderly and more youthful patients.
Conclusions: Elderly patients speak to an alternate extent of DOPPS members crosswise
over nations, conceivably reflecting contrasts in arrangements and clinical practices. By and
large, haemodialysis rehearses in the elderly mirrored every area's clinical examples, with
some variety by age bunch contingent on the practice.
11
1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.