Haemodialysis Patient Care
Added on 2019-10-18
11 Pages3224 Words163 Views
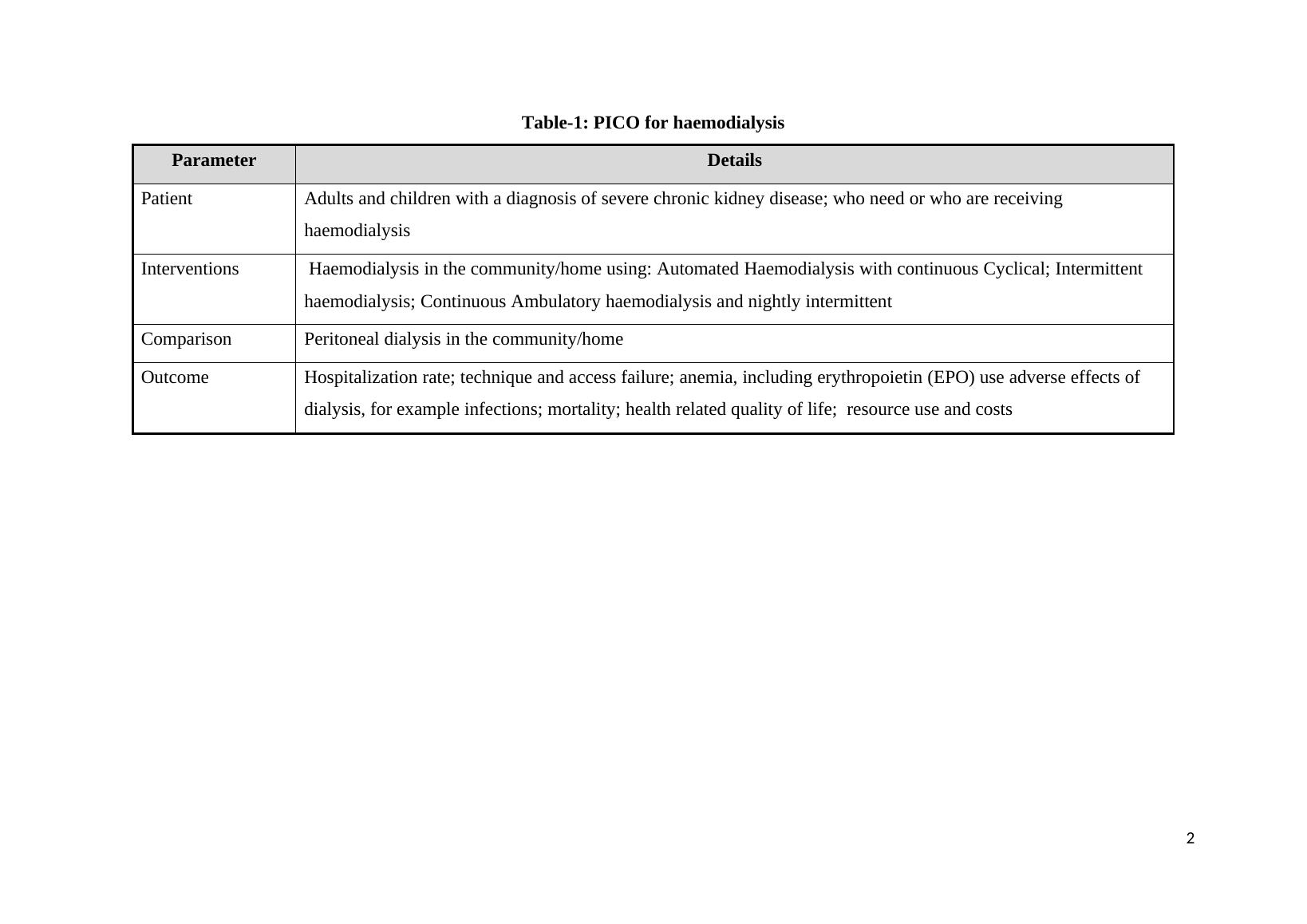
PRIMARY NURSING IN DIALYSIS OUTPATIENT SETTINGTask-1: HaemodialysisChronic kidney disease (CKD) is now recognized as a common condition that elevates therisk of cardiovascular disease as well as kidney failure and other complications. The numberof patients with kidney failure treated by dialysis and transplantation (the end stage of CKD)has increased dramatically in the United States since 1991 (Sarnak et al., 2003). Theoccurrence at end stages of renal disease can lead to death unless renal replacement is started.Unless adequate is provided to the patients with kidney failure, can lead to death of thepatient. The major management strategies include dialysis (Al Wakeel, 2014) andtransplantation (Mosconi et al., 2010). For the vast majority of adult patients with diverseages, dialysis will be treatment modality (Korevaar et al., 2003). Two major types of dialysisare available including haemodialysis and peritoneal dialysis. The processes are used toremove the biological wastes such as urea, ammonia and toxins forded as the result ofmetabolism. Although medical, social, or logistic considerations may preclude one of thedialysis forms, for most patients a well-considered deliberation has to be made betweenstarting with haemodialysis or with peritoneal dialysis. It indicates that haemodialysis is oneof the management strategy for kidney failure. Therefore, the topic on ‘haemodialysis’ ischosen to address the uncertainties associated with the care of patients from patients view.The uncertainities are addressed utilizing evidences.Task-2: PICOThis section describes the PICO (Population, Intervention, Comparator, and Outcome) modelas a tool to address health related problems (Huang et al., 2006). The PICO model isconsidered as a good approach for framing a “foreground” research question (Aslam &Emmanuel, 2010). The present case is related to patients with kidney failure and the use ofhaemodialysis. Since the procedures and precautions to be taken for initiation ofhaemodialysis, a PICO is desired to be in place to handle the cases. The PICO so developedis shown Table-11
Table-1: PICO for haemodialysisParameterDetailsPatientAdults and children with a diagnosis of severe chronic kidney disease; who need or who are receiving haemodialysisInterventionsHaemodialysis in the community/home using: Automated Haemodialysis with continuous Cyclical; Intermittent haemodialysis; Continuous Ambulatory haemodialysis and nightly intermittentComparisonPeritoneal dialysis in the community/homeOutcomeHospitalization rate; technique and access failure; anemia, including erythropoietin (EPO) use adverse effects of dialysis, for example infections; mortality; health related quality of life; resource use and costs2
Task-3: Methods: Literature review Diverse search engines are available for searching evidences based online sources (Donna,2013). Among the sources, few were selected for the current context (Table-2). The sourcesinclude, PubMed, Dovepress and Asn journals as the web sources are providing host for mostclinical services. The key words used for search for the evidences include, 'haemodialysis,kidney failure, aetiology of kidney failure. The summary of most relevant sources are shownin Table-2Table-2: Summary of outcome obtained from the searchSNoSourceOutcomeReference1PubMedProvides a ‘conceptual map’ of candidate dialysisbest practices and highlights areas of generalagreement and disagreement. Desai et al., 20082DovepressGRADE framework was utilized for haemodialysis. Thorsteinsdottir etal 20134AsnjournalsProposal of the dialysis outcomes and practicepatterns study for assessing the dialysis practices andassociated outcomes among elderly versus youngerpatients in diverse countriesCanaud et al.,2011It appears that there exist an inherent wide variation in the services and settings offered bydialysis facilities. In view of the variation, Desai et al., 2008 investigated the practicesemployed at top-performing facilities utilizing a multidisciplinary study. The views socollected from the systematic review, cognitive interviews and a national ‘virtual focusgroup’ of dialysis providers are collated and reviewed. The respondents opined that theoutcomes are influenced by the characteristics of multidisciplinary care conferences,technician expertise, education, periodic audits and communication and teamwork amongstaff. Treatment intensity for elderly patients with end-stage renal disease has escalatedbeyond population growth (Thorsteinsdottir et al., 2012), indicating ageism has stronginfluence on haemodialysis. Thorsteinsdottir et al (2013) reported a comprehensive outcomefrom diverse databases, also approached experts to identify additional references. Theinvestigators utilized a framework of the Grading of Recommendation, Assessment,Development and Evaluation (GRADE) for the assessment of quality of evidence andstrength of recommendations. There exist certain limitations for the balance of benefits andrisks for the initiation of haemodialysis in elderly patients based on the proposals. In another3
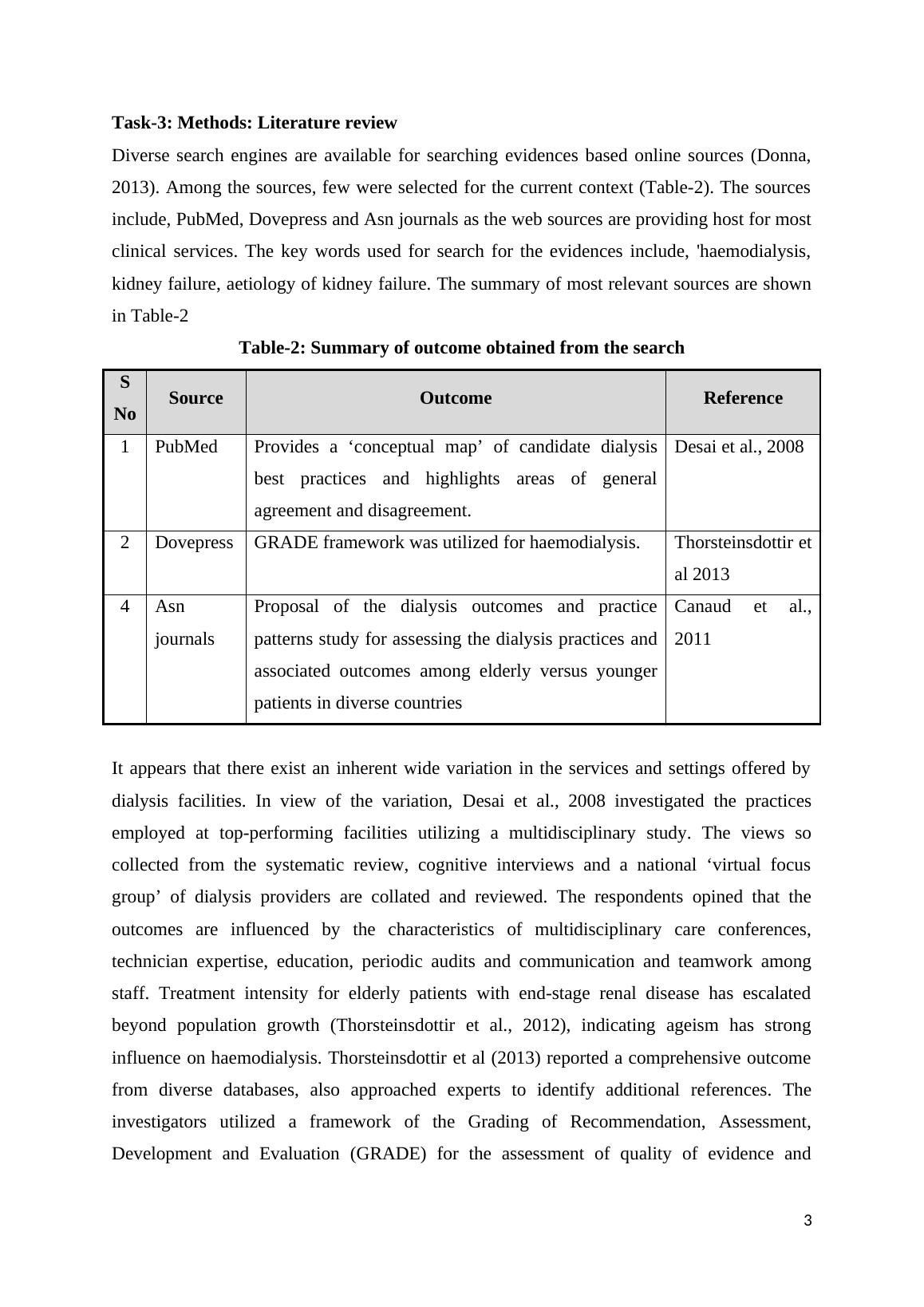
investigation, Canaud et al., (2011) derived and proposed certain recommendations. Theinvestigators observed that malnutrition as one of the common cause in elderly patients alongwith a low ultra filtration rate. Despite of increasing threshold for haemodialysis, there are nostandard guidelines for the procedures to be adopted. The Dialysis Outcomes and PracticePatterns Study (DOPPS) provide a unique opportunity for the assessment of dialysis practicesin elderly and younger patients.Task-4: Discussion of findings Dasia et al., (2008) described the dialysis facilities and their outcomes across the U.S dialysisfacilities for the categorization. Accordingly, the facilities can be grouped as top performingand bottom performing centres. From the evidences, it can believed that facility-leveloutcomes may be related to a series of procedural best practices, including physician-levelpractices (e.g., rapidly returning pages), nurse-level practices (e.g., creating nursing teamsthat optimally match experience), staff enhancement practices (e.g., appointing a dedicatedanaemia manager), and dialysis scheduling practices (e.g., developing formal systems tocorrect short staffing), among many others. The authors have not compared the outcome withavailable sources to potentiate the arguments. Despite of lack of clarifications fully, theinvestigation gave an insight of needs of dialysis as one of the routine health maintenanceservices. Thorsteinsdottir et al (2013) have not made any comparison pertaining to largecohort data for patients with conservative treatment. The survival aspects were taken intoconsideration for the patients who were recommended for palliative care (USRDS, 2008) andanother study looked at looked at median survival for the patients with low glomerularfiltration rate. Another study (Canaud et al., 2011) reveals that the number of elderly patientsare increasing on renal replacement therapy worldwide (Gitto et al., 2008) leading increasingthe health care costs. The available literature lacking the development of health pyramids tounderstand the differing approaches and levels of evidence (Rebecca, 2016). EBP includesrespect of patient values, and their needs, whilst delivering high-quality, cost effective healthcare. Understanding the differing levels of evidence and their reliability, is paramount tomaking correct and appropriate health care decisions pertaining to the setting of care forhaemodialysis. The nurses are required to use EBP as they are responsible for a significantamount of judgments and decisions every day, and therefore, they must use research literatureas part of their clinical decision-making. Most literature available is lacking the pyramid ofhierarchy for the management of renal disease. A generalized pyramid is shown in Fig-1. The4

End of preview
Want to access all the pages? Upload your documents or become a member.
Related Documents
Chronic Kidney Disease in Tiwi Islandslg...
|12
|2793
|91
Qualitative Research Report- Empathetic Understandinglg...
|11
|3121
|39
Renal Failure and Mortality Trends Post Organ Transplantationlg...
|13
|4598
|490
Evidence Based Practice in Renal Nursinglg...
|11
|3103
|491
Tertiary Hospital in Chinalg...
|9
|2372
|15
Importance of Evidence Based Practice in Renal Systems or Haemodialysislg...
|9
|2390
|140